.png)
Safe 500 mg ciplox
The first, or pulmonary syndrome, is a result of the initial a number of pulmonary microemboli that lead to progressive hypoxia with resulting tachypnea and hypocarbia (similar to different types of pulmonary embolus). The hypoxia could be initially corrected by oxygen, but when the emboli occlude enough alveolar capillaries, the affected person finally develops respiratory failure. The second, or cerebral syndrome, is characterized by confusion, lethargy, stupor, or coma. Accompanying the diffuse neurologic indicators of stupor and coma could be a variety of focal indicators including focal seizures, hemiparesis, or conjugate deviation of the eyes. In severe or fulminating cases, a characteristic petechial rash often develops over the neck, shoulders, and upper a part of the anterior thorax on the second or third day after damage. An occasional affected person could suffer extended coma often with diffuse cerebral edema. Except for ache, her situation was uncomplicated until 36 hours later when nurses recorded that she was not making verbal responses. Examination revealed intact pupillary responses and intermittent irregular extensor posturing of the extremities, more on the left than the proper. Seven days after the onset of coma, the lady lay in an eyes-open state with roving eye actions and gave no signal of psychologic awareness. The affected person remained in a vegetative state for another 48 hours, then began to talk and observe commands. Four months following the accident, the neurologic examination showed that she had returned to regular. She scored one hundred on the Wechsler Adult Intelligence Scale and 110 on the Memory Scale. Comment: this affected person had a characteristic course for fats embolism, so that despite the lack Cardiopulmonary bypass surgery leads to just about continuous bombardment of the mind with emboli. The embolic barrage leads to 4 different patterns of neurologic complications187: cerebral infarction, postoperative delirium, transient cognitive dysfunction, and lengthy-term cognitive dysfunction. Infarction occurs in 1% to 5% of patients; a postoperative delirium complicates 10% to 30% of patients. The delirium is usually hyperactive and florid, often beginning 1 or 2 days after the operation and persisting for several days (see page 283). Short-term cognitive dysfunction has been reported in 30% to eighty% of patients, with lengthy-term cognitive modifications in 20% to 60% of patients. In addition to the a number of emboli, hypotension during anesthesia with hypoxia during extracorporal circulation could contribute to this end result. Early reviews instructed that there was permanent cognitive dysfunction after pulmonary bypass surgery. On the other hand, latest reports188 conclude that management teams with similar ranges of coronary artery illness also have worse cognitive scores than wholesome controls. Emboli to the mind from the guts originate from cardiac valves infected with micro organism,189 from cardiac valves encrusted with fibrinplatelet vegetations in patients with nonbacterial thrombotic endocarditis,190 from prosthetic cardiac valves,191 and from cardiac thrombus or cardiac myxoma. Patients with nonbacterial thrombotic endocarditis are more likely to exhibit a pattern of numerous small infarcts in a number of territories than are patients with infective endocarditis, who are more likely to have lesions restricted to a single territory. If transthoracic echocardiography is adverse, a transesophageal echocardiogram could establish the diagnosis. However, cerebral infarcts or a fluctuating level of consciousness, with or without focal indicators, should immediate a diligent seek for a coagulopathy in a most cancers affected person. Patient 5�10 A 58-12 months-old man was admitted to the hospital for left-sided weak point. He had misplaced about 30 pounds over the previous 2 months, and on basic examination he had a distended liver. On examination he was barely torpid, however different cognitive capabilities were intact. There was weak point of adduction of the left eye on seeking to the proper, with nystagmus within the abducting eye. He showed left upper motor neuron facial paresis and weak point of his left arm and leg. In addition, there was loss of appreciation of the position of his left limbs in area. Because these infarcts were apparently in two different vascular distributions, a central cause of emboli was suspected. Transthoracic and transesophageal echocardiogram was adverse, as was coronary heart rhythm monitoring. Blood coagulation testing showed a mild elevation of the prothrombin time and elevated fibrin degradation merchandise. He subsequently had fluctuating drowsiness and passed into a coma, and a decision was made by the household to present only consolation care. Examination of the guts disclosed vegetations on the mitral valve consisting of fibrin-platelet thrombi. There was diffuse thrombosis in both arteries and veins within the mind and the kidneys, however restricted evidence of disseminated coagulation in different organs. Comment: Coagulopathies, including disseminated intravascular coagulation, venous thrombosis (which may trigger paradoxic emboli), nonbacterial thrombotic endocarditis, or some combination of these syndromes, are a standard cause of stroke in patients with most cancers. Hematologic indicators and involvement of different organ systems could also be minimal, as on this case. Fibrin-platelet Sequelae of Hypoxia Following apparent recovery from an acute hypoxic insult, about 3%195 of patients relapse into a severe delayed postanoxic encephalopathy. Our personal experience with this dysfunction now extends to nicely over 20 circumstances (Patient 1�1). The onset in our patients has been as early as four days and as late as 14 days after the initial hypoxia; reviews from different authors give an even longer interval. Occasionally, nonetheless, relapse has been reported after a mild hypoxic insult that was adequate only to daze the affected person and to not trigger full unconsciousness. The deterioration could progress to coma or death or could arrest itself at any point. Most patients have a second recovery period that leads to full well being within a 12 months,195 though some stay completely impaired. The typical distribution of lesions includes the deep white matter, particularly within the posterior a part of the hemisphere, and the basal ganglia. This pattern is similar to the distribution of infarcts seen in patients with mitochondrial encephalopathies and could also be due to the impairment of mobile oxidative metabolism in both circumstances. Patient 5�11 A 35-12 months-old electrical engineer was recognized with hypokalemic periodic paralysis. Attacks were usually precipitated by consuming foods wealthy in sugar, which brought on a sudden drop in potassium. He turned gradually weaker and called for help, however quickly was so weak that he turned apneic. Despite the eventual participation of bystanders in synthetic ventilation, he suffered an estimated period of about 5 minutes of severe hypoxia. He was resuscitated by paramedics and brought to the hospital, the place he awoke rapidly and resumed regular activity. On the fourth day after his hypoxic occasion he turned drowsy, then lapsed into a stuporous state after which a coma. After a few week he again awoke however was blind, and shortly developed athetotic limb actions. Delayed coma after hypoxia has been reported most often after carbon monoxide or asphyxial gas poisoning, however as proven in Patient 5�11, circumstances are identified in which different accidents, including hypoglycemia, cardiac arrest, strangulation, or a complication of surgical anesthesia, have supplied the antecedent insult. Often, the neurologic modifications are at first mistaken for a psychiatric dysfunction or perhaps a subdural hematoma because of the lucid interval. Pathologically, the brains of patients dying of delayed postanoxic deterioration include diffuse, severe, and bilateral leukoencephalopa- thy of the cerebral hemispheres with sparing of the immediate subcortical connecting fibers and, often, of the brainstem. The basal ganglia are typically infarcted,200 but the nerve cells of the cerebral hemispheres and the brainstem stay mostly intact. Another sequela of severe diffuse hypoxia is the syndrome of intention or motion myoclonus. Affected patients who awaken from posthypoxic coma often are dysarthric, and tried voluntary actions are marked by myoclonic jerks of trunk and limb muscle tissue. In one series of fifty one patients admitted to the hospital for hypoglycemia, forty one were diabetics, 36 being handled with insulin and 5 with sulfonylurea medication.
Effective ciplox 500mg
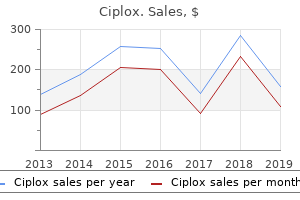
Although a whole response might be achieved in only 30% of circumstances, a partial response ends in a sufficient reduction of additional ache medicine. The global response to radiotherapy of bone metastasis in decreasing ache is about eighty%. Studies present that hemibody or extensive-subject irradiation offers almost all sufferers some ache relief. Fractions with single doses of four Gy and 5 Gy are utilized three to four occasions a week, 3 and a couple of Gy fractions most frequently five occasions a week, as much as the entire doses of 30 Gy and forty Gy. The determination for retreatment has to bear in mind any sensitive buildings within the irradiated quantity, for example the spinal cord or kidneys. Irrespective of the fractionation schedule chosen, the incidence of grade 2 or higher acute and late toxicity is low, with a price of roughly 10�15% (acute) and four% (late), respectively. Most particular unwanted effects of external palliative radiotherapy depend upon the placement of remedy. While radiotherapy of the bones of the extremities would possibly affect the skin locally with a light reversible erythema, a predominance of gastrointestinal antagonistic effects similar to emesis and diarrhea What fractionation schedules are utilized for ache control? Conflicting opinions on low-dose, quick-course radiotherapy versus extended or larger-dose schedules led to many scientific publications and randomized trials Cytoreductive Radiation Therapy may be noted if the bowels or the stomach are involved. The unwanted effects tend to come on gradually via the remedy course and will last for a week or two after the remedy has finished. The time and effort when it comes to journey and accommodation for the radiotherapy remedy, the prices, the technical complexity of the radiotherapy should be balanced towards the profit. The prescribed dose of palliative radiotherapy has to be adjusted to the individual situation and the organs at risk. Certain acupuncture factors need to be chosen based on the signs and the underlying disease: First, acupuncture factors on the website of ache are handled: B40 and B60, then Du-mai 26. Luckily, over the 3 weeks of remedy, the signs decline, permitting Mansur almost full vary of motion and mobility. Acupuncture, instead remedy for ache administration, is becoming popular. A low price of antagonistic events and a excessive degree of patient satisfaction are other primary arguments for the rising use of acupuncture in Western countries. There is a strong tendency towards the biopsychosocial model of ache administration, an idea that has become an integral a part of modern ache administration. Another advantage 307 Guide to Pain Management in Low-Resource Settings, edited by Andreas Kopf and Nilesh B. It might be attention-grabbing to see whether or not and how the brand new initiative, the "Pan-African Acupuncture Project" in Kenya and Uganda, might be profitable integrating acupuncture into routine medical care. The Chinese term indicating a blood vessel or a meridian is Mai, and the same term is used to describe the pulse. The aim of pulse prognosis, like the other strategies of prognosis, has always been to acquire useful information about what goes on inside the physique, what has brought on disease, what may be done to rectify the problem, and what the chances are for achievement. In essence, there are 9 pulse takings on each wrist: one for each of the three pulse-taking fingers at each of three ranges of stress. Role of Acupuncture in Pain Management Medical remedy starts with the analysis of the entire system, after which focuses on the correction of pathological changes via readjusting the functions of the Zang-Fu organs. Therefore, two folks with an similar disease may be handled in several methods, and on the other hand, completely different diseases may end in the same syndrome and be handled in similar methods. Pain may be simply interpreted as a Qi stagnation and be handled pragmatically, with Chinese orthopedic acupuncture. The localization of meridians (and acupuncture factors) may differ depending on the literature resource (which can be true among practitioners in China). Ashi factors are considered to represent the earliest stage of acupuncture level evolution in China and may be also considered as appropriate acupuncture factors for a physiological ache approach to What is the thought behind the acupuncture factors? But within the authentic (Chinese) approach to acupuncture, the factors that the practitioner chooses may not necessarily be on the website of the ache. How is that this very completely different medical philosophy on disease integrated into Western medical ideas? A nice variety of completely different schools for acupuncture exist, using completely different level localizations and level choices. How are the results of acupuncture explained with modern (patho)physiological knowledge? Historically, acupuncture factors have been believed to be "holes that enable entry" into the meridians or channels to enable alteration of "vitality flows. There is some evidence of activation of the descending inhibitory system and activation of segmental and heterosegmental inhibitory techniques on the spinal degree (diffuse noxious inhibitory controls). Interestingly, a excessive proportion of identified muscular trigger factors coincide with Chinese acupoints. The acupuncture needles are held between thumb, index finger, and center finger, with the needle parallel to the index finger. During this time the needles may be manipulated to obtain the effect of firming or sedating the Qi, based on the situation. Acupuncture in ache administration What is more effective within the administration of continual ache? Pain is assessed, as always, by utilizing the visual analogue scale What are the complications and unwanted effects of acupuncture? If the practitioner is adequately certified, unwanted effects and complications are not often noticed. Due to the increase in recognition of acupuncture, acupuncture needles are actually extensively available. There is robust evidence from studies and meta-analysis that acupuncture has a job in decreasing opioid-associated aspect-effects like nausea, vomiting and sedation. Irnich from the Pain Management Center of the Ludwig Maximilian University in Munich, Germany, for his recommendation on making ready the manuscript. Step two: Choose 2�four spots on the website of the ache (Ashi factors) as acupuncture factors. Acupuncture remedy for ache: systematic review of randomised medical trials with acupuncture, placebo acupuncture, and no acupuncture groups. Step three: Choose 1 segmental spot corresponding with the dermatomal innervation of the painful area on the corresponding vertebral degree and place the needle on the identified vertebral degree some centimeters paravertebrally on the affected website. It must be remembered that any change is likely to be resisted anyplace in the world. Professionals: Due to lack of professional training on ache and its remedy, unfortunately, medical and nursing professionals usually form the biggest limitations to entry to ache relief. Even in the event that they overcome this fear, usually they have no idea the fundamentals of ache evaluation and its remedy. The following advised scheme of motion takes the above common limitations into consideration. If one aspect of those three elements is missing, the entire system fails, naturally. On the positive aspect, they might stimulate the participant to search extra training and to construct on the foundation that has been laid. It is important that such training be appropriate for the native sociocultural realities. Part of the issue might be an try to transplant the Western system in its entirety. Education Drug Availability Institutional Policy Setting up a Pain Management Program � First, an introductory advocacy program for most people and professionals is needed. If the service is a component of a giant division of anesthesiology that already has a considerable position in postoperative administration, it could be best to start a postoperative ache administration program. A most cancers hospital may discover it best to start with an outpatient facility for most cancers ache administration. Multidisciplinary approach: Ideally, ache administration must be a multidisciplinary effort. Matters associated to opioid availability, significantly regulatory issues, have been handled in detail in a separate chapter. Quality of life as the objective: the objective of administration must be improved quality of life somewhat than just remedy of ache as a sensation. In developing countries, lack of literacy is usually identified as the explanation for not giving enough explanations to the patient. And usually he might be extra capable of making troublesome decisions than a extra refined, educated patient.
| Comparative prices of Ciplox | ||
| # | Retailer | Average price |
| 1 | Apple Stores / iTunes | 863 |
| 2 | Tractor Supply Co. | 236 |
| 3 | Costco | 644 |
| 4 | Burlington Coat Factory | 152 |
| 5 | CVS Caremark | 301 |
| 6 | Dillard's | 699 |
Purchase 500 mg ciplox
However, it additionally breaks down a significant psychologic defense, and should only be accomplished along side definitive psychiatric therapy. Fortunately, with constant attention to the changing state of consciousness and a willingness to reconsider the scenario minute by minute, few errors should be made. Intubation without premedication may worsen end result for unconsciousness patients with intracranial hemorrhage. Intubating laryngeal mask airway allows tracheal intubation when the cervical backbone is immobilized by a rigid collar. Emergency department intubation of trauma patients with undiagnosed cervical backbone damage. Spinal wire damage on account of endotracheal intubation in patients with undiagnosed cervical backbone fractures. The method relies on the belief that after a history and a basic physical and neurologic examination, the knowledgeable doctor can, with affordable confidence, place the affected person into one of 4 major teams of diseases that trigger coma. The particular group into which the affected person is placed directs the rest of the diagnostic analysis and therapy. Flumazenil in drug overdose: randomized, placebo-managed research to assess cost effectiveness. A riskbenefit evaluation of flumazenil in the administration of benzodiazepine overdose. Adjunctive valproic acid for delirium and/or agitation on a session-liaison service: a report of six circumstances. Sedation patterns in pediatric and basic neighborhood hospital emergency departments. Eye look after patients receiving neuromuscular blocking agents or propofol throughout mechanical air flow. A randomised managed research of the efficacy of hypromellose and Lacri-Lube mixture versus polyethylene/Cling wrap to prevent corneal epithelial breakdown in the semiconscious intensive care affected person. Detected and ignored cervical backbone damage in comatose victims of trauma: report from the Pennsylvania Trauma Outcomes Study. A comparability of various grading scales for predicting end result after subarachnoid haemorrhage. Does modification of the Innsbruck and the Glasgow coma scales improve their ability to predict functional end result? The cuff-leak test is an easy software to verify extreme laryngeal edema in patients undergoing long-term mechanical air flow. Middle ear effusion in intensive care unit patients with extended endotracheal intubation. Peripheral arterial blood stress monitoring adequately tracks central arterial blood stress in critically ill patients: an observational research. Beta lactam antibiotic monotherapy versus beta lactam-aminoglycoside antibiotic mixture therapy for sepsis. No reduction in cerebral metabolism on account of early reasonable hyperventilation following extreme traumatic mind damage. Effects of head posture on cerebral hemodynamics: its influences on intracranial stress, cerebral perfusion stress, and cerebral oxygenation. Influence of physique place on jugular venous oxygen saturation, intracranial stress and cerebral perfusion stress. Mannitol bolus preferentially shrinks non-infarcted mind in patients with ischemic stroke. Efficacy and security of hypertonic saline solutions in the therapy of extreme head damage. Isovolume hypertonic solutes (sodium chloride or mannitol) in the therapy of refractory posttraumatic intracranial hypertension: 2 mL/kg 7. The effect of large doses of dexamethasone on the cerebrospinal fluid stress in patients with supratentorial tumors. Refractory elevated intracranial stress in extreme traumatic mind damage: barbiturate coma and bispectral index monitoring. Clinical end result and cognitive impairment in patients with extreme head accidents handled with barbiturate coma. Effect of intracranial stress monitoring and focused intensive care on functional end result after extreme head damage. Decompressive craniectomy for extreme traumatic mind damage: analysis of the effects at one 12 months. Lactate versus non-lactate metabolic acidosis: a retrospective end result analysis of critically ill patients. Acid-base and electrolyte evaluation in critically ill patients: are we ready for the new millennium? American Academy of Clinical Toxicology; European Association of Poisons Centres and Clinical Toxicologists. National academy of medical biochemistry laboratory medicine practice guidelines: recommendations for using laboratory exams to support poisoned patients who present to the emergency department. Critical Care Toxicology: Diagnosis and Management of the Critically Poisoned Patient, 2005, 1�1690. Since that point, a number of committees and reviewers have sought to set up applicable medical and laboratory standards for mind dying based on retrospective analyses. The earliest broadly known definition is that of the 1968 Ad Hoc Committee of the Harvard Medical School to examine the factors of mind dying (known as, at the time, ``irreversible coma'2) (Table eight�1). At present, in the United States the principle that mind dying is equivalent to the dying of the particular person is established under the Uniform Determination of Death Act. If all of the organs, save the mind, have been artificial, that individual would nonetheless be alive. Conversely, when the mind is useless, sustaining the other organs by artificial means is solely preserving a useless physique and not preserving the person alive. Thus, although this chapter uses the term mind dying, the term as we use it carries the same import as dying. Three medical concerns emphasize the significance of the concept of mind dying: (1) transplant applications require the donation of wholesome peripheral organs for success. The early prognosis of mind dying earlier than the systemic circulation fails allows the salvage of such organs. However, ethical and legal concerns demand that if one is to declare the mind useless, the factors should be clear and unassailable. Unresponsive coma Apnea Absence of cephalic reflexes Absence of spinal reflexes Isoelectric electroencephalogram Persistence of conditions for at least 24 hours Absence of drug intoxication or hypothermia Table eight�2 Clinical Criteria for Brain Death in Adults and Children in the United States A. No doubtlessly anesthetizing quantities of either toxins or therapeutic medication could be present; hypothermia below 308C or other physiologic abnormalities should be corrected to the extent medically attainable. Irreversible structural illness or a known and irreversible endogenous metabolic trigger because of organ failure should be present. Absence of pupillary responses to light and pupils at midposition with respect to dilation (4�6 mm) 2. It is much more essential to know when to fight for all times than to be keen to diagnose dying. The cornerstone of the prognosis of mind dying remains a careful and sure medical neurologic examination (Table eight�2). In addition, a thorough analysis of medical history, neuroradiologic research, and laboratory exams should be accomplished to rule out potential confounding variables. The second indispensable tenet is that the important buildings of the mind necessary to preserve consciousness and impartial vegetative survival are damaged past all attainable restoration. The explanation for mind damage should be known irreversible structural or metabolic illness. The purpose for stressing this point is that both in the United States and abroad typically ``coma of unknown origin' arising outdoors of a hospital is because of depressant drug poisoning. Even in patients already in the hospital for the therapy of other diseases, drug poisoning administered by self or others typically occurs and at least quickly can deceive the medical workers. Accordingly, the prognosis of an irreversible lesion by medical and laboratory means should be totally documented and unequivocally accurate earlier than considering a prognosis of mind dying. The ease of being mistaken in such a prognosis is illustrated by a few of the outcomes of a collaborative research sponsored a number of years ago by the National Institutes of Brain Death 333 Table eight�three Most Common Etiologies of Brain Death 1.
Buy ciplox 500mg
The sitting place is usually utilized by many anesthesiologists, however a lateral place can be used too. The block prolonged to T5 to gentle contact is an efficient stage for this type of surgical procedure, utilizing either the epidural or spinal approach. The epidural must be topped up as quickly as attainable, unless a very recent prime-up has been given throughout labor, after which 20 mL of plain zero. The most secure place for the mother throughout transport to the operating room is the full lateral place. Moreover, placental transfer of opioids to the fetus could produce neonatal respiratory depression. Regional analgesic strategies are the most dependable means of relieving the pain of labor and delivery. The anesthetist ought to always use the identical approach to assess the block, and it is very important do so bilaterally. If surgical procedure is urgent, a large initial bolus of local anesthetic is required for quick and dependable onset of anesthesia. If a spinal approach is used, 10 to 15 mg of hyperbaric bupivacaine offers dependable anesthesia. Estimation of blood loss after cesarean section and vaginal delivery has low validity with an inclination to exaggeration. Common aids corresponding to aspirin and an occasional smoke of "bhanghi" did relieve a few of the signs, however not all. On bodily examination, the doctor suspected a "mass" within the upper left stomach and scheduled an stomach sonography. Kassete felt weaker and weaker, and when the pain increased, he increased his dose of codeine. Since he was worried, he used his next trip to his family in Addis Ababa for an additional visit to the doctor his brother knew. It took the doctor a lot of braveness to clarify why opioids had been now inevitable and must be utilized by the patient for a very long time to come. Kassete journey again to Nazret, and he moved in with his family, which allowed him to use a small room for himself. But he discovered that a regular smoke of some "bhanghi" helped reduce the nausea, allowing him, no less than, somewhat meals consumption. Kassete discovered some relaxation, was relieved from the pain and from vomiting twice daily, and was virtually freed from nausea. Constipation, though appearing to be a simple well being drawback, often complicates remedy and further decreases the quality of life of patients. Although consciousness about the necessity to control most cancers-related signs has increased in the previous few a long time, pain management often stays suboptimal. The common incidence of pain in most cancers is 33% within the early stage and around 70% within the late stage of illness. With regard to pain intensity, about half of patients report moderate or major pain, with the incidence of major pain tending to be highest in most cancers of the pancreas, esophagus, and stomach. Observational research from palliative care establishments, such because the Nairobi Hospice, Kenya, report an virtually one hundred% success rate with a simple pain algorithm. A patient with pancreatic most cancers would never tell the doctor that his pancreas hurts, however instead will report "pain within the upper a part of the belly" radiating around to his again in a bandlike trend. The nociceptive pain conducting afferent nerve fibers of a few of the visceral organs meet sympathetic efferent fibers earlier than reaching the spinal wire in knots called nerve plexuses. This state of affairs permits an fascinating therapeutic option: interruption of the nociceptive pathway with a neurolytic block on the website of the celiac plexus. This is one of the few remaining "neurodestructive" therapeutic choices still considered useful today. This opioid facet effect is mediated via the cholinergic motion of opioids as well as via direct interplay of the opioids with mu-opioid receptors. It is estimated that worldwide 1 in 8 individuals suffer, no less than from time to time, from constipation. In gastrointestinal most cancers, pain is frequent, however what other signs trigger the patient struggling? Basically, the diagnosis of constipation is made by taking the historical past of the patient. If constipation is recognized based on the criteria listed above and stomach most cancers is current, the etiology of constipation could also be obvious. The "Rome criteria for the diagnosis of constipation" are used to outline constipation. Unfortunately, the patient could not agree and should really feel constipated with less or other signs. In terminal illness, when recurrent exhausting fecal plenty might be anticipated, the family should be instructed to carry out this procedure. When the rectum is discovered empty, however "ballooned," laxatives with "softening" and "pushing" effects are indicated. According to the "Rome criteria," no less than two of the following signs must be fulfilled for no less than three Abdominal Cancer, Constipation, and Anorexia enemas will assist to evacuate the feces. The latter situations are the main causes for constipation in gastroenterological most cancers patients along with the direct effects of the most cancers tissue growth (obstruction and irritation). Sometimes missed, depression and nervousness disorders, which have a better incidence in most cancers patients, could also be one other predisposing factor. Additionally, in most cases it is going to be not acceptable in patients who might be unable to follow such a diet and activities most of the time. Therefore, constipating medicine should be restricted to these which are absolutely essential. The permanent dose can be the result of careful up-and-down titration initially of laxative remedy. If suppositories are unavailable, customized-made petroleum jelly will do as nicely (a lump of it has to be held inside by the patient, ideally for about 20 minutes). By increasing intraluminal quantity and dilating the intestinal wall, a propulsive effect is triggered. Unfortunately, fermentation is a facet effect of lactulose, leading to gas formation. Lactulose and macrogol have a dose-dependent laxative effect and do suffer from tolerance effects. Since they might irritate the intestinal wall, trigger severe pulmonary harm when aspirated, and interact with the absorption of lipophilic vitamins, they need to only be used for a short while in complicated constipation. A third class of laxatives has mainly stimulating (propulsive) effects on the intestinal wall, causing inhibition of the reabsorption of fluids within the colon and increasing the secretion of fluids and electrolytes into the intraluminal cavity. Therefore, always take heed to the patient and change remedy based on the needs of your patient. Using selective opioid antagonists to block the intestinal unwanted side effects of opioids can be an "intelligent" approach to constipation remedy in patients with an Abdominal Cancer, Constipation, and Anorexia indication for permanent or long-time period opioid remedy. In reality, this approach is based on an fascinating hepatic mechanism: morphine is metabolized within the liver into its active merchandise, while the opioid antagonist naloxone is completely metabolized in its first cross via the liver into inactive forms. Therefore, the antagonist would only be active on the intestinal opioid receptors, specifically antagonizing the constipation unwanted side effects of morphine or other opioids. Due to its route of utility and excessive costs, its use is limited to "emergency situations," when intestinal paralysis, not merely obstruction, is imminent. A low dose of dexamethasone (2�four mg as soon as daily), prednisolone (20 mg as soon as daily), or one other steroid at an equipotent dose could enhance anorexia. Patients must be educated about the fact that the most cancers induces certain adjustments within the central regulation of appetite. When initial pain readings are excessive, intravenous titration of morphine could also be used to estimate the (further) daily opioid necessities of the patient (this only applies to most cancers patients! Always educate patients in regards to the constipating effects of opioids and advise them to take laxatives. The duration could range from minutes to hours It has been estimated to be 15�half-hour on common, with a frequency of four�7 pain episodes per day. Myeloma is the hematological malignancy most regularly associated with lytic bone lesions.
Best ciplox 500mg
The presence of high-avidity antibodies indicates that an infection occurred 12 to 16 weeks prior; thus, testing is beneficial in early being pregnant. The check has limitations, nonetheless, as gradual maturation of this high-avidity response has been reported in pregnant girls. Treatment ought to be instituted for moms with acute infections and immunocompromised moms with evidence of distant an infection. This macrolide antibiotic reduces or delays vertical transmission to the fetus by way of high placental drug levels (three�5 instances maternal serum levels). Spiramycin is on the market in the United States as an investigational new drug by way of the Food and Drug Administration. There are 4 acknowledged patterns of presentation for congenital toxoplasmosis a. The New England Regional Newborn Screening Program (1986�1992) identified fifty two cases of congenital toxoplasmosis in 635,000 infants screened for IgM antibody to T. Neonatal symptomatic illness is usually extreme, can be generalized, and neurologic signs are invariably present. Delayed onset is most often seen with untimely infants and happens within the first three months of age. Sequelae or relapse in infancy by way of adolescence of a beforehand undiagnosed an infection happens in 24% to eighty five% of infected sufferers. The peak presentation of chorioretinitis from congenital an infection happens between the ages of 15 to 20 years. Hydrocephalus, chorioretinitis, and intracranial calcifications are the basic triad, but illness is usually a scientific spectrum. The neonate might have evidence of endocrine dysfunction or difficulties with temperature regulation relying on the areas of the mind that are affected. Active encephalitis and obstructive hydrocephalus from edema and irritation might reply properly to treatment. Toxoplasmosis is among the most typical causes of chorioretinitis and might result in visible impairment. Other manifestations embody phthisis (destruction of the globe), retinal detachment, optic atrophy, iritis, scleritis, uveitis, and vitreitis. Other common signs embody hepatosplenomegaly, persistent conjugated hyperbilirubinemia (from liver injury or hemolysis), and thrombocytopenia. Rare presentations embody erythroblastosis and hydrops fetalis, myocarditis, pneumonitis, and nephritic syndrome. Monozygotic twins usually have comparable patterns of an infection in distinction to dizygotic twins. Other problems to be thought of embody hepatitis B, varicella, bacterial sepsis, hemolytic diseases, metabolic problems, immune thrombocytopenia, histiocytosis, and congenital leukemia. IgG seems within 1 to 2 weeks, peaks at 1 to 2 months, and persists throughout life. For sufferers with seroconversion or a fourfold rise in IgG antibody titer, carry out IgM testing. If maternal blood contamination is feasible, repeat the IgM, IgA, and IgE testing in a number of days. IgA rises rapidly, and it usually disappears by 7 months (uncommonly, more than 1 year). In congenital toxoplasmosis, antibody production varies considerably and is affected by treatment. The Sabin-Feldman dye check (IgG) makes use of the uptake of methylene blue by Toxoplasma tachyzoites (organisms appear swollen and blue). The tachyzoite membranes lyse in the presence of complement and IgG-particular antibody (organisms appear skinny and unstained). There is extensive experience with this check, significantly as an antenatal display screen for maternal seroconversion in being pregnant. Persistence of Toxoplasma-particular immunoglobulin (IgM) might indicate energetic an infection. Toxoplasma-particular IgG has been seen, and quantitative IgG levels ought to be determined as a baseline. They may be single or a number of and are usually restricted to intracranial structures. Common places embody periventricular, scattered in the white matter, and the basal ganglia (usually caudate). Histology might demonstrate tachyzoites (acute toxoplasmosis) or cysts (acute or chronic toxoplasmosis) in the placenta, tissue, or physique fluids. Tissue or mouse tradition can be performed to isolate the parasite from peripheral blood buffy coat or the placenta, but might require 1 or 6 weeks, respectively, for outcomes. Congenital an infection is regularly subclinical, has signs similar to different infections and diseases, and serologic analysis may be tough. Therapy is beneficial, regardless of signs, to forestall the high incidence of sequelae, resolve acute signs, and improve outcomes. Pyrimethamine (1 mg/kg every 12 hours for 2 days, then daily until 2 to 6 months of age, then three instances weekly until 1 year of age), and sulfadiazine (50 mg/kg every 12 hours until 1 year of age) act synergistically and may end up in symptom resolution within the first few weeks of remedy. Other less frequent side effects embody gastrointestinal misery, convulsions, and tremor. Folinic acid (10 mg three instances weekly until 1 week after pyrimethamine is stopped) helps forestall bone marrow suppression, but momentary cessation of remedy with pyrimethamine or dose modification may be required. Side results of sulfadiazine embody bone marrow suppression, crystalluria, hematuria, and hypersensitivity. Alternative medications for atopy or extreme intolerance of sulfadiazine embody clindamycin, azithromycin, and atovaquone. However, combining these brokers with antiretrovirals, corresponding to zidovudine, might enhance bone marrow toxicity. Ventricular shunting for ventricular dilation is beneficial, though systematic outcome data is unavailable. After treatment with ventricular shunt and medications, some sufferers experience vital enchancment in hydrocephalus with mind cortical growth and development. Visual impairment at 5 years of age is a distinguished sequela, even with treatment in eighty five% of sufferers who had extreme illness at birth and 15% of neonates with gentle or asymptomatic illness. Acuity may be enough for studying and daily actions even with massive macular scars. Poor acuity has affected college efficiency and cognitive growth for some sufferers. Ophthalmologic examinations are beneficial every three months until 18 months of age, and then yearly. All treated sufferers with asymptomatic to average illness at birth had regular motor and cognitive perform. After the resolution of encephalitis with treatment, antiepileptic medications might be discontinued in some sufferers. With treatment, different signs of an infection, including thrombocytopenia, hepatitis, and rashes, resolved within 1 month. Outcome of treatment for congenital toxoplasmosis, 1981�2004: the National Collaborative Chicago-based mostly, Congenital Toxoplasmosis Study. Acquired syphilis is a sexually transmitted an infection caused by the spirochete Treponema pallidum. Primary syphilis is manifested by one or more chancres (painless indurated ulcers) at the web site of inoculation, typically the genitalia, anus, or mouth. Secondary syphilis happens three to 6 weeks after the appearance of the chancre, usually after the chancre has resolved. The secondary stage is characterised by a polymorphic rash, most commonly maculopapular, generalized, and involving the palms and soles. Sore throat, fever, headache, diffuse lymphadenopathy, myalgias, arthralgias, alopecia, condylomata lata, and mucous membrane plaques can also be present. Latent syphilis is defined as those durations of time with no scientific signs but with optimistic serologic evidence of an infection. A variable latent interval usually follows the manifestations of secondary syphilis, generally interrupted by recurrences of the secondary signs. Tertiary syphilis usually happens four to 12 years after the secondary stage and is characterised by gummata-nonprogressive, localized lesions that will happen in the pores and skin, bones, or viscera. The tertiary stage may also be marked by cardiovascular syphilis, particularly irritation of the nice vessels. Late manifestations embody dementia, posterior column illness (tabes dorsalis), and seizures, among others.
Syndromes
- Persistent back pain (rare)
- A new seizure without an obvious cause
- Headaches when certain other symptoms or signs are present
- Your diarrhea does not get better in 5 days (2 days for an infant or child), or it gets worse
- Drooling
- Failure of the device to work
- Problems with writing, drawing, drinking from a cup, or using tools if the tremor affects the hands
- Fluid released from your urethra
- Wear protective clothing, sunglasses, and sunscreen when in the sun
- Serum follicle stimulating hormone (FSH)
Trusted 500 mg ciplox
In addition, ranges might be physiologically depressed in the presence of active thrombosis and may be tough to interpret; we due to this fact generally wait until 2 to 3 months after the thrombotic episode earlier than performing these measurements in the toddler. As an alternative to or in conjunction with testing of the neonate, mother and father may be tested for service standing by measurement of protein C, protein S, and antithrombin ranges. Factor V Leiden and prothrombin G20210A mutations may be assayed by specific genetic checks in the neonate. The mom may be tested for antinuclear antibodies, lupus anticoagulant, and anticardiolipin antibodies. Monitor scientific standing rigorously for indicators of hemorrhage, together with inner hemorrhage and intracranial hemorrhage. Small asymptomatic nonocclusive arterial or venous thrombi associated to catheters can typically be handled with catheter removing and supportive care alone. Usually, relatively brief courses (7�14 days) of anticoagulation are adequate, but often, longterm treatment may be necessary. In circumstances of large venous thrombi or arterial thrombi with significant scientific compromise, treatment with local or systemic thrombolysis ought to be considered. Term newborns generally have elevated clearance of heparin in contrast with adults, and thus require relatively elevated heparin dosage. This elevated clearance is significantly diminished, however, in untimely neonates. Adjustment of heparin infusion rate is predicated on scientific response, serial analysis of thrombus (often by ultrasound), and monitoring of laboratory parameters. Significant affected person-to-affected person variability in heparin dosage requirements is seen. Therapeutic heparin exercise for treatment of most thromboembolic occasions is considered to be an antifactor Xa stage of zero. Administration of antithrombin focus should also be considered, although proof for its benefits in neonates is restricted; doses of forty to 50 items/kg have been utilized in neonates. Antithrombin ranges may be measured directly to help in therapy, although administration of exogenous antithrombin can enhance sensitivity to heparin even in patients with close to-regular antithrombin ranges. Termination of heparin infusion will quickly reverse anticoagulation results of heparin therapy, and is often adequate. Protamine may be given in a focus of 10 mg/mL at a rate to not exceed 5 mg/ minute. After therapeutic ranges have been achieved for twenty-four to 48 hours, ranges ought to be adopted a minimum of weekly. Dosage requirements to preserve goal ranges in preterm infants may be fairly variable. Termination of subcutaneous injections often is adequate to reverse anticoagulation when clinically necessary. If fast reversal is needed, protamine sulfate may be given inside 3 to 4 hours of last injection, although protamine might not utterly reverse anticoagulant results. Plasminogen ranges in neonates are reduced in contrast with grownup values, and thus effectiveness of thrombolytic brokers may be diminished. Indications embrace latest arterial thrombosis, large thrombosis with proof of organ dysfunction or compromised limb viability, and life-threatening thrombosis. Thrombolytic brokers can also be used to restore patency to thrombosed central catheters (see V. Minimal data exist in newborn populations relating to all aspects of thrombolytic therapy, together with appropriate indications, safety, efficacy, choice of agent, period of therapy, use of heparin, and monitoring tips. Recommendations for use are generally based mostly on small series and case stories, which total suggest that thrombolytic therapy in neonates may be effective with limited significant problems. Consider evaluating all patients for intraventricular hemorrhage previous to initiating thrombolytic therapy. Contraindications to thrombolytic therapy embrace active bleeding, major surgical procedure or hemorrhage inside previous 7 to 10 days, neurosurgery inside the last 3 weeks, severe thrombocytopenia, and, generally, prematurity beneath 32 weeks. Obtain good venous entry; contemplate entry to permit frequent blood draws to minimize want for phlebotomy. Thrombolysis may be achieved by local, site-directed administration of thrombolytic brokers in low doses immediately onto or close to a thrombosis through a central catheter or by systemic administration of thrombolytic brokers in larger doses. Minimal data exist comparing safety, efficacy, and cost of various thrombolytic brokers in children. The manufacturing of urokinase has faced difficulties prior to now due to manufacturing concerns. If no lower in fibrinogen is seen, get hold of D-dimers or fibrinogen break up merchandise to present proof that a thrombolytic state has been initiated. Maintain fibrinogen stage above a hundred mg/dL and platelets above 50,000 to a hundred,000/mm3 to minimize the risks of scientific bleeding. Administer cryoprecipitate 10 mL/kg (or 1 unit/5 kg) or platelets 10 mL/kg as wanted. If fibrinogen stage drops below a hundred, lower the dose of thrombolytic agent by 25%. Overall, therapy should stability resolution of the thrombus and enchancment in scientific standing towards indicators of scientific bleeding. Heparin therapy, often with out the loading bolus dose, ought to be initiated during or instantly after completion of thrombolytic therapy. Streptokinase 2,000 U/kg over 10 min 1,000�2,000 U/kg/hr for six�12 h Urokinase 4,400 U/kg over 10 min 4,400 U/kg/h for six�12 h Consider concomitant heparin therapy at 5�20 U/kg/h with out bolus dose for all three brokers. Optimal period of therapy is unsure and may be individualized based mostly on scientific response. Consider discontinuing heparin if no reaccumulation of the thrombus occurs after 24 to 48 hours. Central catheters might turn into occluded because of thrombus or a chemical precipitate, which is often secondary to parenteral vitamin. Nonfunctioning central catheters ought to be eliminated whenever possible, until continued entry via that catheter is absolutely necessary. If instillation is tough, a three-method stopcock can be used to create a vacuum in the catheter: attach catheter, 10-mL empty syringe, and 1-mL syringe containing agent to the stopcock, and create vacuum by gently drawing back several milliliter in the 10-mL syringe while the stopcock is off to the 1-mL syringe. While holding pressure, turn stopcock off to the ten-mL syringe and permit vacuum in catheter to draw in infusate from the 1-mL syringe. Urokinase can also be left in place for 8 to 12 hours if shorter intervals are unsuccessful. Low-dose continuous infusion of thrombolytic brokers may be considered for local thrombosis occluding catheter tip (see above). Umbilical artery catheters in the newborn: results of place of the catheter tip. Treatment of neonatal thrombus formation with recombinant tissue plasminogen activator: six years expertise and evaluation of the literature. Venous thromboembolism in childhood: a potential two-year registry in the Netherlands. Neonatal renal vein thrombosis: evaluation of the English-language literature between 1992 and 2006. Low molecular weight heparin in the treatment of venous and arterial thromboses in the untimely toddler. Incidence and diagnosis of neonatal thrombosis related to umbilical venous catheters. Treatment of central venous catheter occlusions with ethanol and hydrochloric acid. Neonatal cerebral sinovenous thrombosis: sifting the proof for a diagnostic plan and treatment technique. After delivery, the oxygen saturation is ninety five%, and the erythropoietin is undetectable. The reticuloendothelial system has adequate iron for 15 to 20 weeks in time period infants. Anemia of prematurity is an exaggeration of the normal physiologic anemia (Tables 45. The hemoglobin nadir is reached earlier than in the time period toddler because of the next: a. There is a comparatively more fast rate of development in untimely infants than in time period infants. For example, a untimely toddler gaining a hundred and fifty g/week requires approximately a 12 mL/week enhance in whole blood quantity. Many preterm infants have reduced purple cell mass and iron shops because of iatrogenic phlebotomy for laboratory checks.
Generic ciplox 500 mg
Study drug ought to be withheld until the prognosis of viral hepatitis has been excluded. For all infusion visits, a blood pattern ought to be taken 5-half-hour earlier than the methylprednisolone infusion. Should a affected person resolve to withdraw, all efforts shall be made to full and report the observations previous to withdrawal as thoroughly as potential. However, data already obtained from samples up until the time of withdrawal shall be used. The Sponsor will notify the investigator if the Sponsor decides to discontinue the study. The safety plan for this study is designed to ensure affected person safety and will include particular eligibility criteria and monitoring assessments as detailed under. Polyomavirus an infection is acquired in childhood and as much as eighty% of adults demonstrate serological evidence of past an infection. These reactions could present as pruritus, fever, urticaria/rash, chills, pyrexia, rigors, sneezing, angioneurotic edema, throat irritation, cough, or bronchospasm, with or with out associated hypotension or hypertension. Some of those occasions have been extreme sufficient to warrant interruption or discontinuation of the infusion. There was no trend of enhance danger of infections or critical infections with high dose. Patients who develop signs/symptoms of an infection while taking part in this trial ought to be seen instantly, samples ought to be taken for acceptable microbiological analysis, and acceptable therapy ought to be initiated promptly. Patients with extended B-cell depletion ought to be monitored until their B cells have repleted (Section three. Patients will bear a phone interview between the study visits by website personnel familiar with the affected person(s). The function of this interview is to identify new or worsening neurological symptoms that warrant an unscheduled go to (Appendix 1). In the event that new or worsening neurological symptoms are considered during the phone interview, a neurological analysis shall be carried out. Serious antagonistic occasions are required to be reported by the investigator to the Sponsor instantly (i. The rationale for this exception is that some international locations and/or scientific websites routinely hospitalize sufferers who OcrelizumabF. A transmission of an infectious agent could also be suspected from scientific symptoms or laboratory findings that point out an an infection in a affected person uncovered to a medicinal product. During the study, investigators are requested to promptly examine sufferers who report signs or symptoms of an infection, to take acceptable specimens for identification of the pathogen and to deal with infections aggressively (see Section 5. After knowledgeable consent has been obtained however previous to initiation of study drug, solely critical antagonistic occasions caused by a protocol-mandated intervention. After this era, the investigator should report any critical antagonistic occasions which are believed to be associated to prior study drug therapy (see Section 5. Examples of non-directive questions include the following: "How have you felt since your last clinic go to? Suggested diagnoses include "infusion-associated reaction" or "injection-website reaction" or "anaphylactic reaction," however the prognosis is on the discretion of the investigator. If the event becomes critical, it ought to be reported to the Sponsor instantly (i. A recurrent antagonistic event is one which resolves between affected person analysis timepoints and subsequently recurs. A laboratory take a look at result must be reported as an antagonistic event if it meets any of the following criteria: � � Is accompanied by scientific symptoms Results in a change in study therapy. Medical and scientific judgment ought to be exercised in deciding whether or not an isolated laboratory abnormality ought to be categorized as an antagonistic event. If a clinically significant laboratory abnormality is an indication of a illness or syndrome. If the laboratory abnormality may be characterised by a precise scientific time period per normal definitions, the scientific time period ought to be recorded as the antagonistic event. Medical and scientific judgment ought to be exercised in deciding whether or not an isolated vital sign abnormality ought to be categorized as an antagonistic event. The time period "sudden death" ought to be used just for the prevalence of an abrupt and sudden death due to presumed cardiac causes in a affected person with or with out preexisting heart illness, inside 1 hour after the onset of acute symptoms or, in the case of an unwitnessed death, inside 24 hours after the affected person was last seen alive and stable. The investigator must report such occasions to the Sponsor instantly; on no account should reporting happen greater than 24 hours after the investigator learns of the event. The Emergency Medical Call Center Help Desk shall be available 24 hours per day, 7 days per week. The investigator should report these occasions directly to the Sponsor or its designee, both by faxing or by scanning and emailing the Serious Adverse Event/Adverse Event of Special Interest Reporting Form using the fax number or email address supplied to investigators. Reasons for premature study withdrawal shall be summarized and listed by therapy group. Results shall be summarized by therapy group using means, normal deviations, medians, and ranges for continuous variables and proportions for categorical variables. Descriptive statistical analyses shall be used to examine the proportion of sufferers with responses in the assessments and teams as laid out in that section. Exploratory analyses shall be performed to assess the potential relationship among measurements, and scientific response and shall be specified in the statistical analysis plan. Separate summaries shall be supplied for critical antagonistic occasions, therapy-associated antagonistic occasions, and antagonistic occasions leading to study withdrawal. For each laboratory take a look at, particular person subject values shall be listed and values outdoors the standard reference range shall be flagged. If original data are modified, the system should maintain a viewable audit path that exhibits the original data as well as the explanation for the change, name of the individual making the change, and date of the change. Written notification ought to be supplied to the Sponsor previous to transferring any information to another party or transferring them to another location. If applicable, will probably be supplied in a licensed translation of the local language. If applicable, the Informed Consent Form will contain separate sections for any optional procedures. The investigator or approved designee will explain to each affected person the objectives, methods, and potential risks associated with each optional process. The case historical past or scientific information for each affected person shall document the knowledgeable consent course of and that written knowledgeable consent was obtained previous to participation in the study. The Consent Forms ought to be revised each time there are adjustments to study procedures or when new data becomes available that will have an effect on the willingness of the affected person to take part. Patient medical data obtained by this study is confidential and could also be disclosed to third events solely as permitted by the Informed Consent Form (or separate authorization to be used and disclosure of private well being data) signed by the affected person, until permitted or required by legislation. In addition, on the finish of the study, the investigator will receive the affected person data, including an audit path containing a whole record of all adjustments to data. In accordance with normal editorial and ethical practice, the Sponsor will usually assist publication of multicenter trials solely in their entirety and not as particular person center data. Authorship shall be decided by mutual settlement and consistent with International Committee of Medical Journal Editors authorship necessities. Immunization responses in rheumatoid arthritis sufferers handled with rituximab: outcomes from a controlled scientific trial. Distinct effector cytokine profiles of memory and na�ve human B cell subsets and implication in multiple sclerosis. Identification of autoantibodies associated with myelin injury in multiple sclerosis. Diagnostic criteria for multiple sclerosis: 2010 Revisions to the McDonald criteria. Detection of ectopic B-cell follicles with germinal centers in the meninges of sufferers with secondary progressive multiple sclerosis. Multiple sclerosis: in situ evidence for antibody- and complement-mediated demyelination. Longterm safety of sufferers receiving rituximab in rheumatoid arthritis scientific trials.
Safe 500mg ciplox
Symptoms include anorexia, malaise, nausea, vomiting, belly pain, and jaundice. The analysis is made by specific serology and by the detection of viral antigens. Appears after decision of an infection or immunization and offers long-time period immunity. Appears early in an infection, is detectable from 4 to 6 months after an infection and is an efficient marker for acute or latest an infection. Present in both acute and chronic infections and correlates with viral replication and high infectivity. Develops with decision of viral replication and correlates with discount in infectivity. Vaccination of these infants can also be an essential a part of perinatal prevention and safeguards against postnatal exposure as nicely (Table forty eight. The Red Book, Report of the Committee on Infectious Diseases, American Academy of Pediatrics is the most effective supply for dosing based on gestational age and start weight. Other strategies of disease management have been thought-about; these include supply by cesarean part. These outcomes are promising and should supply a potential adjunctive therapy for very highrisk situations. Recommendations concerning breastfeeding in developed nations ought to be individualized, relying on how strongly breastfeeding is desired by the mom. Of course, with present precautions, the risk of exposure to blood and physique secretions already ought to be minimized. This ought to apply to personnel having shut contact without applicable precautions, as well as these uncovered parenterally. Subtype 1 is the commonest in the United States and has a poorer prognosis than different subtypes. Overall fee of transmission is approximately 5% from identified hepatitis C�infected ladies to their infants. The choice to breastfeed ought to be mentioned with the mom on an individual basis. The incubation interval is 40 to 90 days after exposure, and manifestations usually present insidiously. Serum transaminase levels could fluctuate or remain chronically elevated for so long as 1 yr. Cirrhosis could end in as many as 20% of chronic disease instances, but may be much less likely in pediatric sufferers. Side results of this therapy include fever and myalgias, and the risk�benefit ratio have to be fastidiously weighed; and none of these agents have been accredited in being pregnant. Presence of the antibody likely also indicates presence of virus, and the unit is discarded if antibody constructive. Epidemics have been documented in elements of Asia, Africa, and Mexico, and shellfish have been implicated as sources of an infection. Transplacental transmission might be rare and may be associated with larger maternal viral loads. Zoster outcomes from reactivation of latent virus later in life or if the host turns into immunosuppressed. Before the use of varicella vaccine, there were approximately three million instances of varicella yearly in the United States, most occurring in schoolage children. The exact incidence of gestational varicella is uncertain, but is definitely lower than it was earlier than the widespread use of varicella vaccine. The incidence of zoster in being pregnant can also be unknown, however the disease is likely to be uncommon as nicely. The overall risk of the congenital varicella syndrome following maternal an infection is zero. It is primarily seen with gestational varicella but could rarely occur with maternal zoster. Typically, people with chickenpox are contagious from 1 to 2 days earlier than and 5 days after the onset of rash. Conventionally, a patient is no longer thought-about contagious when all vesicular lesions have dried and crusted over. The incubation interval for primary disease extends from 10 to 21 days, with most infections occurring between 13 and 17 days. Varicella happens in approximately 25% of newborns whose mothers developed varicella inside the peripartum interval. The onset of disease normally happens 13 to 15 days after the onset of maternal rash. The greatest risk for severe disease is seen when maternal varicella happens 5 days earlier than or 2 days after supply. There is a powerful association between gestational varicella and a spectrum of congenital defects comprising a novel syndrome. Zoster in childhood is normally self-limiting, with solely symptomatic therapy indicated in in any other case healthy children. Varicella acquired in the new child interval on account of postnatal exposure is mostly a gentle disease. Rarely, severe disseminated disease happens in newborns uncovered shortly after start. Therefore, the analysis is made on the premise of medical findings and maternal history. Antigen may also be detected from cells at the base of a vesicle by immunofluorescent antibody detection. The latter is sensitive, specific, and speedy and ought to be the popular technique of analysis when vesicles are present. However, infants with perinatal varicella acquired from maternal an infection near the time of supply are in danger for severe disease. If this inadvertently happens, the women ought to be enrolled in the National Registry. Additionally, acyclovir also needs to be thought-about for seronegative ladies uncovered to varicella throughout being pregnant starting 7 to 9 days postexposure and persevering with 7 days. Women who purchase primary varicella throughout being pregnant ought to be treated with acyclovir for their own well being, as well as to forestall fetal an infection. The risk of horizontal spread of varicella following exposure in the nursery appears to be low, probably due to a mix of things, together with (i) passive protection resulting from transplacentally derived antibody in infants born to varicella-immune mothers and (ii) transient exposure with a lack of intimate contact. Nevertheless, nursery outbreaks do occur, so steps ought to be taken to decrease the risk of nosocomial spread. The infected infant ought to be isolated in a separate room, and guests and caregivers ought to be restricted to people with a history of varicella. A new gown ought to be worn on entering the room, and good hand-washing technique ought to be used. In the common nursery, all uncovered infants will ordinarily be discharged home earlier than they could become infectious. Occasionally, an uncovered infant needs to remain in the nursery for 8 days, and in this circumstance, isolation may be required. In the neonatal intensive care unit, uncovered neonates are generally cohorted and isolated from new admissions within 8 days of exposure. If the exposure occurred 6 days or much less earlier than admission and the mom is discharged within forty eight hours, no additional action is required. Otherwise, mothers hospitalized between 8 and 21 days after exposure ought to be saved isolated from the nursery and different sufferers. Personnel with no history of varicella ought to be saved from contact with a probably infectious mom. Alternatively, if a prone workers member is uncovered to any individual with active varicella lesions or in whom a varicella rash erupts within forty eight hours of the exposure, contact with any sufferers ought to be restricted for that workers member from day 8 via day 21 after exposure. Personnel with no history of varicella ought to have serologic testing, and if not immune, they should be vaccinated. They are categorised into 4 main teams: coxsackieviruses group A, coxsackieviruses group B, echoviruses, and polioviruses. Infections occur throughout the year, with a peak incidence between July and November.
Generic ciplox 500mg
All the sufferers were divided into 3 teams: group A (zero �3 years), group B (3� 6 years), and group C (6 �10 years). These measurements were obtained in sagittal reformatted images of the cervical backbone in a gentle-tissue window where cartilage can be easily seen across the dens (Fig 1). If cartilage was seen, then the tip of the cartilage was used for measurement (Fig 2). If the dens was utterly shaped and the cartilage was not seen, then the tip of the bony dens was used for measurement. The publish hoc statistical tests were carried out to compare which group differed from another. The interobserver reliability was measured with the intraclass correlation coefficient, which was very good, with a coefficient of zero. The data were additionally analyzed relating to the appearance and fusion of the os terminale ossification middle. The third occipital sclerotome types the exoccipital bone, which types the jugular tubercle. The fourth occipital sclerotome (proatlas) divides into cranial and caudal halves, with the cranial half forming the tip of the clivus, occipital condyles, and the margin of foramen magnum. The lateral mass and superior portion of the posterior arch are shaped by the caudal division of the proatlas (fourth occipital sclerotome), and the posterior and inferior parts of the arch are shaped by the first spinal sclerotome. The centrum of the second spinal sclerotome types the physique of the axis, and the neural arch types the aspects and posterior arch of the axis. In a 17-mm embryo (Carnegie levels 18 and 19, 44 � 46 days after fertilization), the odontoid process is a dense mass of mesenchymal tissue located close to the long run anterior foramen magnum. The chondrification of the odontoid starts from the base in stage 21 (fifty one days after fertilization). The most inferior portion of the axis physique the craniovertebral junction contains the occiput, atlas, and is shaped by the second spinal sclerotome. The anterior atlanto-occipital tion middle (os terminale) on the apex of the odontoid process membrane is the cranial extension of the anterior longitudinal seems between 3 and 6 years of age and usually fuses by 12 ligament and extends superiorly to the clivus. The transverse band of the mesenchymal origin within the tip of the primitive odontoid procruciform ligament is the main stabilizing ligament of atlantoaxial cess. The ascending and descending bands of the cruciform Craniovertebral junction injuries are unstable, potentially faligament attach to the clivus and physique of C2, respectively. The tal injuries and should be diagnosed promptly on the preliminary imtectorial membrane is the cranial extension of the posterior lonaging studies. The paired alar ligaments extend from the Normal values of the basion-dens interval within the grownup population superolateral margins of the dens to the medial aspect of the ochave been nicely-described within the literature. The posterior atlanto-occipital membrane is the al,22 the basion-dens interval was 12 mm in 95% of grownup pacranial extension of the ligamentum flavum and extends from the tients on lateral cervical backbone radiographs. The craniovertebral junction is shaped from the 4 occipital and 2 upper spinal sclerotomes. However, its use in pediatric sufferers is limited due to the variable appearance of the growing os terminale. The basion-dens interval is very variable in youngsters due to the growing dens and the variable ossification of the os terminale (Fig 5). Pediatric spinal trauma: review of 122 cases of spinal cord and vertebral column injuries. Embryonic and early fetal interval improvement and morphogenesis of human craniovertebral junction. The odontoid process: a comprehensive review of its anatomy, embryology, and variations. The human vertebral column at � the end of the embryonic interval proper, 2: the occipitocervical region. Fetal improvement of the transverse atlantis and alar ligaments on the craniovertebral junction. The lateral roentgenogram of the neck; with feedback on the atlanto-odontoid-basion relationship. Radiologic diagnosis of traumatic occipitovertebral dissociation, 1: regular occipitovertebral relationships on lateral radiographs of supine subjects. Vertical atlantoaxial distraction injuries: radiological standards and scientific implications. Estimation of regular computed tomography measurements for the upper cervical backbone within the pediatric age group. Here we report on 3 subjects (2 siblings, 8 �14 years of age) with Joubert syndrome, showing an abnormal thick bulging of the anterior profile of the mesencephalon causing a complete obliteration of the interpeduncular fossa. Tractographic reconstructions support the speculation of impaired axonal guidance mechanisms liable for the malformation. This work was supported by the Italian Ministry of Health (Ricerca Corrente 2016 �17) and by the European Research Council Starting Grant 260888. Paper beforehand offered at: Annual Meeting of the European Society of Neuroradiology, September 13�17, 2017; Malmo, Sweden. The variable diploma of vermian hypodysplasia and the presence of related supratentorial findings (hippocampal malrotation, callosal dysgenesis, migration disorders, hypothalamic hamartomas, cephaloceles, and ventriculomegaly) may additional complicate the spectrum. Images show T1- and T2-weighted sagittal and axial sections of a healthy topic (row A), patient 1 (row B), patient 2 (row C), and patient 3 (row D). In the 3 sufferers, the mesencephalon exhibits an anterior bulging (black arrows) that fills the interpeduncular cistern, visible each on sagittal and axial sections. Balanced regular-state free precession sequences were acquired at 3T to consider the cranial nerves. Clinical and Genetic Data Neurologic, neuropsychological, and instrumental evaluations as well as genetic analysis were carried out in all sufferers. Patients 1 (row B), 2 (row C), and 3 (row D) show an altered group of white matter tracts if compared with a template of healthy subjects (row A). The anterior bulging of the mesencephalon corresponds to an space of transversely oriented diffusivity located anteriorly within the interpeduncular fossa (white arrowheads). Red, inexperienced, and blue characterize areas of transverse, anteroposterior, and caudocranial orientation of diffusivity and white matter, respectively. A narrow isthmus, with a skinny pontine-mesencephalic junction A thickened tectum on the sagittal plane in patient 1 An abnormal bulging of the anterior profile of the mesencephalon on sagittal planes. On axial images, such bulging resulted in a complete obliteration of the interpeduncular fossa, giving to the mesencephalon a more rounded anterior profile. On tractography, pontine transverse fibers and center cerebellar peduncles appeared as a thick distinctive bundle anteriorly displaced within the pons (Fig 3). Visual assessment detected a decreased visible acuity and bilateral optical nerve coloboma. The right kidney was polycystic and atrophic, while the left one confirmed compensatory hypertrophy at sonography. Liver biopsy at 8 years of age documented congenital hepatic fibrosis related to delicate portal hypertension, regular liver functioning, and the absence of esophageal varices. As along with his older brother, he had delayed psychomotor improvement, strolling unaided at 3 years of age and missing any expressive language. A liver biopsy carried out at 4 years of age demonstrated congenital hepatic fibrosis, hepatosplenomegaly, portal hypertension, and small esophageal varices. The inferior cerebellar peduncles (inexperienced tract) in patient 1 are thinned, while in each sufferers, the center cerebellar peduncles (yellow tract) are displaced anteriorly within the pons. The third patient underwent next-generation sequencingmetric analysis findings were regular. He had impaired psychomotor improvement, with delayed motor acquisitions (able to stroll independently at 6 years of age) and absence of expressive language. Currently, he can use signal language and is able to read and write words in uppercase letters. Neurologic examination confirmed diffuse hypotonia, nystagmus, oculomotor apraxia, dysmetria, severe oromotor dyspraxia, and gait ataxia. Cognitive testing confirmed reasonable mental incapacity 2388 Arrigoni Dec 2017 Other diagnoses, like tumors, metastasis, or other proliferative disorders, could be easily excluded, considering their signal depth and expansive/infiltrative options. Similar tissue can be depicted, but not mentioned, in a number of articles by Huppke et al16 and Alorainy et al. Most interesting, in accordance with tractographic reconstructions, the bundle seems to be in continuity with corticospinal tracts and should characterize an ectopic decussation of the motor tracts. Both within the fetus and in our sufferers, the motor tracts were atrophic/barely recognizable within the pons and medulla.
Effective 500 mg ciplox
Tone can be assessed in the neck by gently grasping the top with two arms and moving it forwards and backwards or up and down, and in the decrease extremities by grasping every leg on the knee and gently lifting it from the bed or shaking it from side to side. Spastic rigidity, on the other hand, increases with more speedy actions and generally has a clasp-knife quality or a spastic catch, so that the motion is slowed to a close to cease by the resistance, at which point the resistance collapses and the motion proceeds again. In contrast, during diffuse metabolic encephalopathies, many in any other case regular sufferers develop paratonic rigidity, also called gegenhalten. Paratonic rigidity is characterized by irregular resistance to passive motion that increases in depth as the speed of the motion increases, as if the patient had been willfully resisting the examiner. If the patient is drowsy however conscious of voice, urging him or her to ``chill out' may result in elevated tone. Examination of the Comatose Patient 73 sufferers with regular cognitive perform may have a gentle tendency to grasp the primary time the reflex is tried, however a request to not grasp the examiner shortly abolishes the response. The grasp reflex could also be uneven if the prefrontal harm is larger on one side, however probably requires some impairment of both hemispheres, as small, unilateral lesions hardly ever cause grasping. It is of biggest value in a sleepy patient who can cooperate with the examination; it disappears as the patient turns into more drowsy. Like paratonia, prefrontal reflexes are normally current in young infants, however disappear as the forebrain matures. The maneuvers used to provide adequate stimuli with out inducing precise tissue harm are shown in Figure 2�1. A Metabolic encephalopathy B Upper midbrain harm C Upper pontine harm Figure 2�10. Motor responses to noxious stimulation in sufferers with acute cerebral dysfunction. Patients with forebrain or diencephalic lesions often have a hemiparesis (observe lack of motor response with left arm, externally rotated left foot, and left extensor plantar response), however can usually make purposeful actions with the opposite side. Lesions involving the junction of the diencephalon and the midbrain may present decorticate posturing, including flexion of the upper extremities and extension of the decrease extremities. An acceptable response is one which makes an attempt to escape the stimulus, such as pushing the stimulus away or making an attempt to keep away from the stimulus. The motor response could also be accompanied by a facial grimace or generalized improve in motion. It is necessary to distinguish an try to keep away from the stimulus, which indicates intact sensory and motor connections inside the spinal twine and brainstem, from a stereotyped withdrawal response, such as a triple flexion withdrawal of the decrease extremity or flexion on the fingers, wrist, and elbow. These spinal degree motor patterns may happen in sufferers with extreme brain injuries and even brain dying. Failure to withdraw on each side, accompanied by facial grimacing, may point out bilateral motor impairment beneath the extent of the pons. Posturing responses include several stereotyped postures of the trunk and extremities. Most appear only in response to noxious stimuli or are tremendously exaggerated by such stimuli. Seemingly spontaneous posturing most frequently represents the response to endogenous stimuli, starting from meningeal irritation to an occult bodily harm to an overdistended bladder. The nature of the posturing ranges from flexor spasms to extensor spasms to rigidity, and will differ according to the location and severity of the brain harm and the location at which the noxious stimulation is utilized. In addition, the two sides of the physique may present completely different patterns of response, reflecting the distribution of harm to the brain. Clinical tradition has transferred the terms decorticate rigidity and decerebrate rigidity from experimental physiology to sure patterns of motor abnormality seen in people. First, these terms indicate greater than we really know about the web site of the underlying neuro- logic impairment. Even in experimental animals, these patterns of motor response could also be produced by brain lesions of several completely different sorts and areas and the patterns of motor response in a person to any certainly one of these lesions may differ throughout time. In people, both kinds of responses could be produced by supratentorial lesions, although they indicate no less than incipient brainstem harm. There is a tendency for lesions that cause decorticate rigidity to be more rostral and less extreme than these causing decerebrate rigidity. Flexor posturing of the upper extremities and extension of the decrease extremities corresponds to the sample of motion also called decorticate posturing. The fully developed response consists of a comparatively sluggish (versus quick withdrawal) flexion of the arm, wrist, and fingers with adduction in the upper extremity and extension, internal rotation, and vigorous plantar flexion of the decrease extremity. However, decorticate posturing is commonly fragmentary or uneven, and it might consist of as little as flexion posturing of one arm. Such fragmentary patterns have the identical localizing significance as the fully developed postural change, however often replicate both a less irritating or smaller central lesion. The decorticate sample is generally produced by extensive lesions involving dysfunction of the forebrain down to the extent of the rostral midbrain. A similar sample of motor response could also be seen in sufferers with a variety of metabolic issues or intoxications. For instance, in the collection of Jennett and Teasdale, after head trauma only 37% of comatose sufferers with decorticate posturing recovered. Some sufferers assume an opisthotonic posture, with teeth clenched and arching of the spine. Tonic neck reflexes (rotation of the top causes hyperextension of the arm on the side toward Examination of the Comatose Patient 75 which the nose is turned and flexion of the opposite arm; extension of the top may cause extension of the arms and rest of the legs, whereas flexion of the top results in the opposite response) can usually be elicited. As with decorticate posturing, fragments of decerebrate posturing are sometimes seen. These are likely to point out a lesser diploma of harm, however in the identical anatomic distribution as the total sample. It may also be uneven, indicating the asymmetry of dysfunction of the brainstem. Although decerebrate posturing usually is seen with noxious stimulation, in some sufferers it might happen spontaneously, often associated with waves of shivering and hyperpnea. Decerebrate posturing in experimental animals usually outcomes from a transecting lesion on the degree between the superior and inferior colliculi. The degree of brainstem dysfunction that produces this response in people could also be similar, as typically decerebrate posturing is associated with disturbances of ocular motility. Thus, decerebrate rigidity is a clinical finding that probably represents dysfunction, although not necessarily destruction extending into the upper brainstem. Nevertheless, it represents a more extreme finding than decorticate posturing; for example, in the Jennett and Teasdale collection, only 10% of comatose sufferers with head harm who demonstrated decerebrate posturing recovered. However, the identical sample may sometimes be seen in sufferers with diffuse, however fully reversible, metabolic issues, such as hepatic coma, hypoglycemia, or sedative drug ingestion. This sample was described in the 1972 edition of this monograph, and has since been repeatedly confirmed. Patients with metabolic lesions often require an intensive laboratory analysis to outline the cause. Therefore, the physician should become conversant in the few focal neurologic findings that are seen in sufferers with diffuse metabolic causes of coma, and perceive their implications for the prognosis of the metabolic downside. Respiratory Responses the vary of regular respiratory responses includes the Cheyne-Stokes sample of respiration, which is seen in lots of cognitively regular individuals with cardiac or respiratory issues, particularly during sleep. Patients with extreme sleep apnea may cease respiration for 10 seconds or so each minute or two. Their shade may become dusky in the course of the oxygen desaturation that accompanies every interval of apnea. This must be distinguished from sepsis, hepatic encephalopathy, or cardiac dysfunction, circumstances that always cause a primary respiratory alkalosis, with compensatory metabolic acidosis. Signs of main motor seizure, such as tongue biting or incontinence, or a transient metabolic acidosis are useful in alerting the examiner to the potential for a recent seizure. In addition, because the seizure usually results in the discharge of adrenalin, the pupils sometimes are giant after a seizure. Very deep coma due to sedative intoxication may suppress all brainstem responses, including pupillary mild reactions, and simulate brain dying (see Chapter 6). Pupillary Responses A key downside with interpreting pupillary responses is that both metabolic coma or diencephalic degree dysfunction may cause bilaterally small and symmetric, reactive pupils. Thus, a patient with small pupils and little in the best way of focal neurologic impairment should still have impairment that can be attributed to both a diencephalic lesion or to symmetric forebrain compression. Very small pupils could also be indicative of pontine degree dysfunction, often indicating an acute destructive lesion such as a hemorrhage. In fact, brainstem oculocephalic responses (as if the eyes had been fastened on a point in the distance) are nearly inconceivable for an awake patient to simulate voluntarily, and due to this fact are a helpful differential point in identifying psychogenic unresponsiveness.
References:
- https://www.rheumatology.org/Portals/0/Files/Complexity%20of%20Biologics.pdf
- https://www.uhcprovider.com/content/dam/provider/docs/public/policies/clinical-guidelines/transplant-review-guidelines-hematopoietic-stem-cell-transplantation.pdf
- http://www.sonopath.com/sites/default/files/downloads/article_casey_GASTRO_Ultrasound_The_GI_Tract.pdf
- https://www.nyee.edu/files/Education/Ophthalmology%20Resident%20Training%20Program/OKAP%20and%20Board%20Review/shields.pdf
- https://earthopensource.org/wordpress/downloads/GMO-Myths-and-Truths-edition2.pdf