.png)
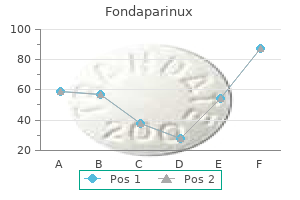
Quality fondaparinux 2.5mg/0.5ml
Arrhythmias or different situations requiring drugs that lead to symptomatic bradycardia. Documented asystole of > three seconds or escape charges < forty bpm in awake, asymptomatic patients. Asymptomatic kind I second-degree block with intra- or infra-His ranges discovered on an electrophysiologic study done for one more indication. Sudden Cardiac Death Approximately 450,000 sudden cardiac deaths occur yearly within the United States. Causes in this inhabitants embody the following (in order of lowering incidence): Hypertrophic cardiomyopathy. Arrhythmogenic right ventricular dysplasia, by which the proper ventricle is replaced by fat and fibrosis, causing frequency of ventricular arrhythmias. Noncardiac precipitants of sudden cardiac death in young athletes embody bronchial asthma, illicit drug use (e. Although screening often includes history taking and bodily examination, these measures alone lack the sensitivity to detect even the most typical causes of sudden cardiac death in athletes (e. Heart price variability: heart price variability corresponds to worsening heart failure and may be be} associated with an threat of sudden cardiac death. Rheumatic aortic stenosis is often not hemodynamically vital and virtually at all times happens within the presence of mitral valve disease. Presents with a protracted asymptomatic period followed by the event of the classic triad of angina, syncope, and heart failure. A crescendo-decrescendo systolic murmur is heard at the base of the heart with radiation to the carotid arteries. Hypertrophic obstructive cardiomyopathy: Murmur accentuated with Valsalva or standing and by hand grip. Follow-up echocardiography is beneficial every year for severe aortic stenosis; every 1�2 years for reasonable aortic stenosis; and every 3�5 years for gentle aortic stenosis. Dobutamine stress testing: Used in instances of low-gradient aortic stenosis (severe aortic stenosis by valve area, however imply gradient < forty mmHg) to distinguish true stenosis from pseudostenosis attributable to systolic operate. If true aortic stenosis is present, the gradient will and the valve area will remain unchanged. Antibiotic prophylaxis in opposition to subacute bacterial endocarditis: Indicated for all patients. Aortic valvuloplasty: May be efficient in young adults with congenital aortic stenosis. Less efficient in patients with degenerative aortic stenosis, and should be considered palliative therapy or a bridge to surgical procedure. Chronic aortic regurgitation: A lengthy asymptomatic period followed by progressive dyspnea on exertion and different indicators of heart failure. In acute aortic regurgitation, these indicators are often not present, and the only clues may be be} intensity of S1 and a short, blowing diastolic murmur. In severe aortic regurgitation, the anterior mitral valve leaflet can vibrate within the aortic regurgitation jet, creating an apical diastolic rumble that mimics mitral stenosis (Flint murmur). Other causes of diastolic murmurs embody mitral stenosis, tricuspid stenosis, pulmonic insufficiency, and atrial myxoma. Cardiac catheterization: Aortography can be utilized to estimate the degree of regurgitation if noninvasive studies are inconclusive. Aortic valve replacement: Should be considered in symptomatic patients or in those without signs who develop worsening left ventricular dilatation and systolic failure. Mitral Stenosis Almost solely end result of} rheumatic heart disease, with uncommon instances end result of} congenital lesions and calcification of the mitral annulus. Cor triatriatum: Left atrial septations trigger postcapillary pulmonary hypertension. Aortic insufficiency: Can mimic the murmur of mitral stenosis (Flint murmur) end result of} restriction of mitral valve leaflet movement by regurgitant blood from the aortic valve, however no opening snap is present. Consider this intervention in symptomatic patients with isolated mitral stenosis and an effective valve area < 1. This is the appropriate intervention in pregnant 136 ladies for whom medical therapy has failed. Severe annular calcification, severe mitral regurgitation, and atrial thrombus are all contraindications to balloon valvuloplasty. Common causes of mitral regurgitation embody mitral valve prolapse, myxomatous (degenerative) mitral valve disease, dilated cardiomyopathy (which causes functional mitral regurgitation end result of} dilatation of the mitral valve annulus), rheumatic heart disease (acute mitral valvulitis produces the Carey Coombs murmur of acute rheumatic fever), acute ischemia (due to rupture of a papillary muscle), mitral valve endocarditis, and trauma to the mitral valve. S3 may be end result of} mitral regurgitation alone (in the absence of systolic heart failure), and its presence suggests severe mitral regurgitation. Acute mitral regurgitation may be associated with hypotension and pulmonary edema; murmur may be be} early systolic. Tricuspid regurgitation: Characterized by a holosystolic murmur best heard at the left sternal border; in intensity with inspiration. Exercise stress testing: Document exercise limitation before signs occur at rest. In patients with acute myocardial ischemia, even a low-intensity murmur of mitral regurgitation ought to alert the physician to risk of|the potential of|the potential for} papillary rupture. Echocardiography should be carried out every 6�12 months in patients with severe mitral regurgitation, an end-systolic diameter > four. Optimal timing of surgical procedure is early the center of|in the midst of} the disease, when patients progress from a persistent, compensated state to symptomatic mitral regurgitation. Repair is most successful when mitral regurgitation is due to of|as a result of} of} prolapse of the posterior mitral valve leaflet. Mitral Valve Prolapse Defined by a displaced and abnormally thickened, redundant mitral valve leaflet that tasks into the left atrium during systole. Mitral valve prolapse may be be} complicated by chordal rupture or endocarditis, each of which might lead to severe mitral regurgitation. Mechanical valves: Young patients; patients with a life expectancy > 10�15 years or with different indications for persistent anticoagulation (e. Replacement: Rheumatic heart disease, endocarditis, heavily calcified valve, restricted leaflet movement, extensive leaflet destruction. For patients with mechanical valves, the level of anticoagulation is determined by} the placement and sort of valve (valves within the mitral and tricuspid position and older caged-ball valves are most vulnerable to thrombosis). Endocarditis: Early prosthetic valve endocarditis: Occurs during the first 60 days after valve replacement, most commonly end result of} S. Late prosthetic valve endocarditis: Most typically happens in patients with multiple of} valves or bioprosthetic valves. Thrombosis: At highest threat are those with mitral location of the valve and insufficient anticoagulation. Presents clinically as heart failure, poor systemic perfusion, or systemic embolization. For large thrombi (> 5 mm), use extra aggressive therapy similar to fibrinolysis or valve replacement. In severe instances, search for hemolytic anemia and valvular insufficiency causing heart failure. Emboli: Typically present as stroke, however can present as intestinal or limb ischemia. Exam reveals a systolic circulate murmur (usually best heard at the left upper sternal border) and infrequently a diastolic rumble throughout the tricuspid valve end result of} circulate. Echocardiography with agitated saline bubble study: Can be used to visualize the intracardiac shunt and to decide the ratio of pulmonaryto-systemic blood circulate (Qp/Qs). Surgical correction is indicated for very large defects properly as|in addition to} for ostium primum and sinus venosus defects. Coarctation of the Aorta Proximal narrowing of the descending aorta simply past the left subclavian artery with improvement of collateral circulation involving the interior mammary, intercostal, and axillary arteries. A bicuspid aortic valve is present in > 50% of patients with coarctation of the aorta. Cardiac catheterization with aortography: To outline stenosis and measure gradient.
Order 2.5mg/0.5ml fondaparinux
For multicompartment techniques and unstable solutes, the solute additionally be} distributed erratically. In these techniques the calculated volume is totally different from the true volume during which the solute is distributed. The anion hole is the distinction in the serum between the concentrations of cations and anions. Distinguishing between metabolic acidosis caused by bicarbonate loss and metabolic acidosis caused by increases in organic acid (an unmeasured cation) is a typical and essential downside. On the other hand, when metabolic acidosis outcomes from a rise in organic acid (e. It could be helpful, though, with marked elevation in organic acids whose measurements are less readily available. What do we know in regards to the efficacy of the therapeutic use of sodium bicarbonate to appropriate acidemia in pediatric sufferers As a common rule, replacement of bicarbonate when physique losses of bicarbonate are excessive (e. Moreover, if the reason for the acidemia is ongoing, the development in pH will be short-term; the primary reason for the acidemia should be corrected. The clinician ought to by no means administer bicarbonate until the power to excrete carbon dioxide is ensured; in any other case, the clinical acid�base disturbance additionally be} worsened. Serum anion hole in the differential prognosis of metabolic acidosis in critically unwell newborns. The main action of loop diuretics is to inhibit chloride (and thereby sodium) reabsorption in the loop of Henle. Therefore hyponatremia with loop diuretics could be be} caused by a sodium deficit ensuing from excessive diuretic remedy or from excessive administration of free water. The former is managed by decreasing the frequency of loop diuretic administration, the latter by decreasing free water consumption. What damage can persistent administrative loop diuretics inflict on the kidneys, urinary tract, or both Loop diuretics induce hypercalciuria by inhibiting renal tubular calcium reabsorption. Therefore persistent administration of these brokers could cause nephrocalcinosis, calcium nephrolithiasis, or both. What is the best way|one of the best ways|the best way} to treat the hypokalemic, hypochloremic metabolic alkalosis that occurs in newborns who receive persistent diuretic remedy Diuretic remedy additionally induces a reduction in effective intraarterial volume and thereby activates the renin-angiotensin-aldosterone system, which stimulates secretion of potassium in the distal tubule. Accordingly, including spironolactone, a aggressive inhibitor of aldosterone, to the diuretic regimen could prevent or improve derangements in serum bicarbonate and potassium concentrations. Infants receiving loop diuretics could require increased potassium and chloride consumption to prevent potassium depletion and metabolic alkalosis. Loop diuretics are likely to|are inclined to} be simpler in neonates but trigger calciuresis, which can result up} in|which could find yourself in|which can lead to} osteopenia, nephrocalcinosis, renal stone formation, or a mixture of these. Routine use of diuretic remedy has not been proven to considerably alter the course of bronchopulmonary dysplasia, though it may provide some instant assistance in bettering air flow. The advantages ought to be fastidiously weighed towards the dangers of metabolic, bone, and renal problems. The nurse probably responds on the premise of physical evidence; for instance, he or she could say that the infant had only three wet diapers over the previous 24 hours. If the infant is in an intensive care unit and the urine volume is being quantified, urine move fee could be calculated. In considering what the causes of oliguria are, want to|you should|you have to} keep in mind the determinants of urine move fee (see Question 6). Dehydration is defined as an inappropriately negative lower in whole physique water, sodium, or both caused by inadequate water and sodium consumption. If urine could be obtained for evaluation, urine [Na+] will be low and urine osmolality will be excessive with dehydration. Treatment is determined by} the trigger but all the time contains replenishment of whole physique water and sodium. The pattern of change over time, taking into account gestational and postnatal age, is more relevant. It is essential to observe that all one|that each one} the aforementioned causes could occur with out associated oliguria, but urine output ought to be comparatively low. There is an in depth differential prognosis for each of these main causes, and the clinical context is essential in narrowing the differential prognosis. In the face of an irregular change in serum [Cr], how could the urine sodium concentration be helpful in evaluating oliguria His situation is sophisticated by bilateral pneumothoraces, and he has been anuric since delivery. Can you formulate an armchair differential prognosis earlier than going to see the infant The most helpful initial test can be belly sonography concentrating on the kidneys, ureters, and bladder. Plasma creatinine rises dramatically in the first forty eight hours of life in preterm infants. Pathologic causes of polyuria embrace the following: n Impaired reabsorption of Na+ by the kidney. In this case the offending substance impairs reabsorption of water and sodium, primarily in the proximal tubule. Because of the increased delivery of water and Na+ to the distal tubule, K+ secretion will also be stimulated, resulting in an inappropriate improve in urinary potassium excretion (or kaliuresis) and potassium depletion. A new child male infant is discovered to have renal failure caused by obstructive uropathy as outcome of|the outcomes of} posterior urethral valves. Severe obstruction of the urinary tract throughout nephrogenesis could result in renal maldevelopment and outcome in|may find yourself in|can lead to} renal dysplasia. An early sign of dysplasia is a renal concentrating defect that manifests as polyuria and polydipsia. An infant born prematurely to a mom who had polyhydramnios required mechanical air flow for 1 week. At 6 days of life he had a rising serum creatinine level, hypotension with cool extremities, hyponatremia, and mild hypokalemia. The neonatal type of Bartter syndrome, also known as|also called|also referred to as} hyperprostaglandin E syndrome, could present this fashion. In such instances the mom has polyhydramnios caused by increased fetal urine excretion; affected infants are often born prematurely. Infants with Bartter syndrome even have hypercalciuria and increased excretion of prostaglandin E2. Oliguria is widespread in neonates through the first day of life as a result of|as a end result of} glomerular filtration is decreased. The hallmark of this syndrome is the presence of a traditional anion hole hyperchloremic metabolic acidosis. In addition to presenting with metabolic acidosis, these sufferers have progress restriction, faulty dental enamel, developmental delay, and calcium deposits in the basal ganglia. What is postnatal imaging find on a new child with antenatal hydronephrosis The remaining will present the following: n Ureteropelvic junction obstruction (11%) n Vesicoureteral reflux (9%) n Megaureter (4%) n Multicystic dysplastic kidney (2%) n Ureterocele (2%) n Renal cyst (2%) n Posterior urethral valves (1%) Less widespread causes of hydronephrosis embrace ectopic ureter, prune-belly syndrome, urethral atresis, retrocaval ureter, ureteral stricture, hydrocolpos, pelvic tumor, and cloacal anomaly. In fetal hydronephrosis 50% of instances improve, 40% stay stable, and 10% progress. The objectives of intervention are to restore adequate amniotic fluid volume to enable normal pulmonary development and maximize ultimate renal perform. How ought to an infant with an irregular genitourinary prenatal ultrasound be evaluated Renal and bladder ultrasound is the first imaging needed in a neonate with an irregular prenatal ultrasound. A normal 48-hour postnatal ultrasound might be adequate to exclude clinically vital disease, though some physicians will get hold of an ultrasound later. If unilateral hydronephrosis is present, a voiding cystourethrogram (to exclude vesicoureteral reflux) and serial ultrasounds are recommended.
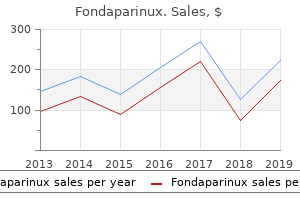
| Comparative prices of Fondaparinux | ||
| # | Retailer | Average price |
| 1 | OSI Restaurant Partners | 982 |
| 2 | DineEquity | 768 |
| 3 | QVC | 967 |
| 4 | SUPERVALU | 420 |
| 5 | Williams-Sonoma | 337 |
Safe fondaparinux 2.5mg/0.5ml
Once the correct position of the endotracheal tube is confirmed, it ought to be secured in place. After induction of anesthesia and masks air flow is established the endotracheal tube can be placed. The tube is placed in the nose parallel to the palate, aiming inferiorly to avoid cranium base injury, till a loss of resistance is encountered preserving with} entrance into the pharynx. Placement under direct visualization can be performed utilizing a laryngoscope and McGill forceps to direct the endotracheal tube past the glottic opening. Alternately, a fiberoptic bronchoscope can be placed through the tube and directed past the vocal folds. Nonparticulate antacids, H2 blockers, and metoclopramide can be administered to lower the acidity and volume of gastric contents. As with a normal intubation described above, instrumentation ought to be prepared and out there. Preoxygenation with one hundred pc O2 by masks for three to 5 minutes or four maximal breaths over 30 seconds is enough. Once the paralytic and induction agents are administered, no further air flow is given. Induction is completed with any induction agent, and the process is adopted instantly with the administration of a paralytic agent. Cricoid pressure ought to proceed till tracheal placement of the endotracheal tube is verified. As with a normal intubation all essential equipment ought to be out there and checked previous to induction. A backup plan ought to be formulated ought to intubation be troublesome, such because the creation of a surgical airway. Preparing the airway by decreasing secretions with an antisialagogue (glycopyrrolate zero. After normal monitors are placed, sedation with fentanyl, midazolam, or dexmedetomidine ought to be thought-about. Regional anesthesia, both alone or in combination with topical agents, is beneficial in awake intubations. Oral Technique A bite block ought to be inserted to shield the fiberoptic scope after anesthetizing the airway (see above). Transtracheal Ventilation Transtracheal air flow serves as a temporizing measure if masks air flow and oxygenation turn into insufficient or unimaginable. A catheter (12- or 14-gauge) is inserted into the trachea through the cricothyroid membrane and connected to a jet-type ventilator able to delivering gas at a pressure of fifty psi. Perioperative Care and General Otolaryngology 15 Ventilation is greatest assessed by observing chest rise and fall. Complications embrace catheter displacement (caused by excessive pressure), pneumothorax, and pneumomediastinum. Typically, propofol at doses of two to three mg/kg produces dependable jaw and pharyngeal muscle leisure. Placement requires neck extension, which is usually contraindicated with cervical backbone disease. The GlideScope the GlideScope is a video laryngoscope might be} a helpful different to the fiberoptic scope for placement of an endotracheal tube if a troublesome airway is expected. The blade is curved like the Macintosh blade with a 60-degree 16 Handbook of Otolaryngology�Head and Neck Surgery curvature to match the anatomic alignment. The GlideScope has a digital digicam included in the blade, which shows a view of the vocal folds on a monitor. Under visualization on the monitor, an endotracheal tube is handed between the vocal folds. Surgical Laryngoscopes Closed cylinder-style inflexible laryngoscopes with shiny fiberoptic light guides such because the Dedo or Holinger are utilized by the otolaryngologist and have advantages that permit visualization of the glottis and intubation. N the Difficult Airway Among otolaryngology�head and neck surgical procedure sufferers, a excessive share presents with a troublesome airway (Table 1. Perioperative Care and General Otolaryngology 17 troublesome airway doubtlessly poses difficulty with air flow or endotracheal tube placement. Evaluation by the otolaryngologist and review of diagnostic studies can provide invaluable information to the anesthesiologist when a troublesome airway is suspected. As outlined in the Difficult Airway Algorithm of the American Society of Anesthesiologists. The dialogue ought to handle backup plans ought to the preliminary attempt to secure the airway fails or incapability to ventilate ensues. If a troublesome airway is suspected, instrumentation and plans for possible surgical airway ought to be out there. Briefly, the neck is prolonged, and the cricothyroid membrane is palpated and incised with a scalpel. The airway is entered and an endotracheal or tracheotomy tube is placed to ventilate the affected person. Clinical situations involving a affected person with a troublesome airway can be divided into two categories. The first is the acute or pressing drawback and the second, an elective state of affairs with a suspected or known troublesome airway. A logical, strict method can forestall a disastrous outcome in what is usually a annoying state of affairs. The otolaryngologist�head and neck surgeon ought to have particular expertise in making certain an adequate airway and ought to be skilled in the use of of} laryngoscopy, bronchoscopy, and surgical approaches to the airway. Specific methods to be mentioned right here embrace cricothyroidotomy and awake tracheotomy. If the state of affairs requires institution of an emergency surgical airway, a cricothyroidotomy is mostly the preferred process. Contraindications to cricothyroidotomy embrace subglottic stenosis or mass, laryngeal trauma, with an incapability to identify landmarks; generally, it ought to be avoided in the pediatric inhabitants. Actively pursue alternatives to deliver supplemental oxygen throughout the method of adverse airway administration three. Awake intubation Noninvasive technique for preliminary method to intubation Preservation of spontaneous air flow vs. Therefore, these options could also be} of restricted value if this step in the algorithm has been reached by way of the Emergency Pathway. For needle cricothyroidotomy, a catheter is placed over a needle that penetrates the cricothyroid membrane, permitting air flow by a pressurized stream of oxygen. Needle cricothyroidotomy is the preferred methodology of creating an emergency airway in youngsters younger than 10 to 12 years. Stable but Compromised Airway A affected person with supraglottitis, angioedema, or a laryngeal mass may have a steady but compromised airway. In some circumstances, the affected person can be managed with medical administration and shut monitoring. Tracheotomy is a surgical process by which the tracheocutaneous airway is created through the anterior neck and the trachea. If intubation is deemed impractical or harmful, an awake tracheotomy can be performed. It is essential to note that this is greatest accomplished in a controlled 20 Handbook of Otolaryngology�Head and Neck Surgery Table 1. Clear communication between the otolaryngologist�head and neck surgeon, anesthetist, nurses, and technicians is vital. It is essential to note that a life-threatening emergency may arise and this will necessitate close collaboration. For the awake tracheotomy, the affected person ought to be placed in the semiFowler position enabling the anesthesiologist ready entry to the airway. Every effort ought to be made to maintain the affected person comfy and the general environment ought to be as calm as possible. Note that in the elective (nonurgent) tracheotomy the affected person is intubated previous to the beginning of surgical procedure.
Trusted fondaparinux 2.5mg/0.5ml
The framework is multidimensional, emphasizing the intrinsic significance of indivisible human freedoms: Redressing inequalities in fundamental and enhanced capabilities is the overarching intended outcome. Multidimensionality also permits a greater integration of the instrumental analysis of revenue and nonincome mechanisms behind the formation and progressive equalization of capabilities. The coverage cycle may be described as one composed of premarket policies (primarily inside the block on the left of figure 7. Wages, earnings and labour participation rates are sometimes decided in markets, that are conditioned by prevailing regulations, establishments and policies (in-market). Premarket policies can reduce disparities in capabilities, helping everybody enter the labour market higher equipped-even though essential to|it is very important|you will need to} emphasize that this is removed from the one cause why capabilities matter and that by enhancing capabilities the contributions to expanding incomes go beyond collaborating within the labour market (they can, for instance, improve political participation). In-market policies result on} the distribution of revenue and alternatives when people are working, shaping outcomes that can be be} either more or much less inclusive. Postmarket policies result on} inequalities quickly as} the market, along with in-market policies, have decided the distribution of revenue and alternatives. The provision of public companies premarket might rely in part on the effectiveness of postmarket policies (taxes on market revenue to fund well being and training, for instance), which matter in mobilizing authorities revenue to pay for those companies. Take, for instance, suggestions linked to the redistribution of revenue, which tend to to|are inclined to} dominate the coverage debate. Tony Atkinson simulated the effect of an ambitious redistributive package deal on revenue inequality within the United Kingdom, showing that it would solely halve the gap with Sweden within the Gini coefficient for disposable revenue and could be inadequate to reverse its enhance between the late Nineteen Seventies and 2013. Using this framework, the chapter has two sections, every corresponding roughly to policies associated with the two blocks. And given the big heterogeneity throughout international locations and the uncertainties associated with future pathways (due not solely to local weather change and technology but in addition to different elements not considered within the Report4), every country must determine the most suitable set of policies for its unique circumstances. The first part discusses means to|tips on how to} increase capabilities past revenue, addressing each vertical and horizontal inequalities in human growth. It considers each the structure and the design of training and well being methods, as well as|in addition to} policies related to the rising challenges of technology and local weather change. Among horizontal inequalities, the focus target|the primary focus} is on gender equality, responding to the challenges outlined in chapter 4. The second part addresses policies that can collectively carry productivity in methods that are be} translated into extensively shared incomes-redressing revenue inequality. Those policies have a bearing on how markets for items and companies as well as|in addition to} for labour and capital operate. The part also discusses the effect of redistributive policies on the national stage. Because national policies may be constrained or facilitated by globalization, the part considers how international collective action-or the shortage thereof-can shape inequalities within the twenty first century. Towards convergence in capabilities past revenue: From fundamental to enhanced universalism Policies with universal reach speak to the fulfilment of the pledge to "leave no one behind" of the 2030 Agenda and to the Universal Declaration of Human Rights. This part is about recalibrating ambitions and actions for the twenty first century and model spanking new|for model new} generations that will see the 22nd century. It begins by arguing that convergence in capabilities past revenue should build on these achievements, but be additional enhanced. Such enhancement would call for each political help (which would require overcoming constraints in social alternative, as elaborated in spotlight 7. Beyond enhanced universalism, this part considers policies on eliminating horizontal inequalities (with a concentrate on to} gender inequality) and the enhancement of capabilities for local weather shocks and to harness technology. Universal policies constructed on extensive coverage only- with out sufficient resources or designed to ensure each quality and equity-are not genuinely universal Towards enhanced universal methods Universal policies constructed on extensive coverage only-without sufficient resources or designed to ensure each quality and equity-are not genuinely universal. This part argues that enhanced universal methods (illustrated with companies linked to training and health) probably be} more effective in lowering human growth inequalities if based mostly on two pillars: Chapter 7 Policies for lowering inequalities in human growth within the twenty first century: We have a alternative 225 Relying on non-public, fee-based faculties for fundamental training can leave the poorest even additional behind, due in part to unequal entry and decrease accountability for quality, which tends to harm poor college students disproportionally, especially ladies � Comprehensive social companies ensuring equal entry to quality companies according to calls for and aspirations of the twenty first century. Health outcomes, for instance, depend upon entry to companies but are also socially decided. Leaving no one behind thus also requires targeted policies addressing horizontal and group inequalities. Several international locations have been expanding coverage in preprimary training, with Ethiopia having pushed for a big jump in coverage since 2010 (box 7. This not solely is probably to|prone to} contribute to equalization of capabilities in lengthy run|the long term} but can also result on} the distribution of unpaid work, favouring the inclusion of girls within the labour market (as elaborated within the discussion about gender inequality later in this chapter). Lifelong studying would improve each financial and social outcomes and assist achieve more equitable alternatives at all ages. In international locations where most workers work informally, national or sectoral training and coaching funds to present casual workers entry to training and coaching probably be} established. But investing in these expertise also supplies a possibility to break the vicious cycle of inequalities by creating a stage begin for all kids. For youthful kids from the bottom revenue quintile the average constructive parenting check score elevated from 1. For youthful kids from the richest quintile the average score elevated from 2. So, inequality in parenting check scores between richer and poorer quintiles almost disappeared. It emphasizes brain growth in early childhood and supplies parenting help by way of internet portals, websites and cell phone functions. It also includes substantial investments in kindergarten and instructor coaching, especially in rural areas and for poor and migrant kids in city areas, and authorities help for early studying growth pointers, instruments and national requirements. Ethiopia exhibits how preprimary training can allow developing international locations to enhance training outcomes. Acknowledging the important thing} position of equitable entry to preprimary training for human growth, a core pillar of the coverage framework is the expansion of preschool and school readiness programmes. Although the ministry had initially considered two years of preprimary training, the plans were changed to broaden entry. Since its introduction the 0-Class has achieved high enrolment rates and is now by far the most extensively available preschool, especially in rural areas. Fuelled by these early successes, additional options to enhance rural enrolment have been explored in Ethiopia. Run by major faculty academics and supported by low-cost studying kits, it supplies young kids with a fundamental curriculum in preliteracy and prenumeracy. The impacts of preprimary training have been evaluated in quantity of} case studies in Ethiopia. A Save the Children project on advancing literacy and math expertise found that kids from decrease socioeconomic backgrounds achieved considerably greater training gains-practically closing the educational gap with their friends from greater socioeconomic backgrounds. Chapter 7 Policies for lowering inequalities in human growth within the twenty first century: We have a alternative 227 employment probably be} powerful, since formal jobs are associated with larger companies that invest more in employee coaching and with longer employment spells, where more on-the-job studying can happen. Enabling everybody to lead a protracted and healthy life While inequalities in well being outcomes are sometimes unrelated to the availability of well being companies (chapter 2 and field 7. In Thailand the coverage, carried out in 2001, unfold to all provinces the next 12 months and reached 98 % of the inhabitants in 2011. Next was expanding coverage to poor and vulnerable folks, which required a robust political dedication. Political dedication needs to go hand in hand with monetary resources dedicated to universal well being coverage, and different international locations take different approaches. France used earmarked taxes: first a payroll tax and later earmarked revenue and capital taxes. Brazil and Ghana earmark a part of} their social safety contributions and value added tax. In addition to financing, a major implementation problem is the scarcity of well being care personnel. In many circumstances non-public and unregulated public well being care of variable quality might enhance sharply. In response, Indonesia reformed its accreditation of well being professionals and standardized the processes for certifying them. Brazil and Ethiopia broadened their well being skilled recruitment pools for well being extension and offered more flexible profession alternatives to group well being workers. Sweden has an impressive well being care system, with broad coverage, minimal out-of-pocket prices and special assist for vulnerable groups. For example: � Mortality rates in Sweden are strongly correlated with socioeconomic status. At the underside more than 40 % of individuals die by age eighty, compared with fewer than 25 % on the high. People of decrease socioeconomic status are twice as probably as those on the high to suffer from heart assaults, lung most cancers, sort 2 diabetes and heart failure.
Best fondaparinux 2.5/0.5ml mg
Perceptions data-when the restrictions are nicely understood-can complement goal indicators. Indeed, some of the the} frontier measures of capabilities and agency are subjective indicators. Thanks to a mix of|a mixture of} quick financial development and social policies, there has been a sharp reduction in multidimensional poverty. Between 2005/2006 and 2015/2016 the variety of multidimensionally poor people in India fell by greater than 271 million. On average, progress was extra intense among the poorest states and the poorest teams. First, the Scheduled Castes, Scheduled Tribes and Other Backward Classes underperform relaxation of|the the rest of} society across human growth indicators, together with education attainment and access to digital applied sciences (box figures 1 and 2). Modern India has tried to constitutionally redress the disparities by way of affirmative motion, optimistic discrimination and reservation policies for these teams. Third, there has been an increase in inequalities in enhanced areas of human growth, corresponding to access to computer systems and to 12 or extra years of education: Groups that have been extra advantaged in 2005/2006 have made the most gains, and marginalized teams are shifting ahead but in comparative terms are lagging further behind, regardless of progress. Box figure 1 India: Horizontal inequality in education of working-age people (ages 15�49) Population with 5 or extra years of education, 2015 (percent) sixty eight. Finally, increasing demand for equality in perception surveys has concrete penalties for society. No matter the diploma of subjectivity and potential distortion, these opinions have the chance to become half of} the political discussion and to stimulate motion. There is an urgent want for evidence-based policy approaches to reply to new demands. This shifting target is inherently relative and, due to this fact, requires a extra flexible approach to assess inequality. In a world without excessive poverty, for example, the poverty line will inevitably rise-indeed, poverty in developed international locations is often measured in relative terms. For human growth a shift in focus from primary to enhanced capabilities could also be} related. This perspective, which moves beyond extra individualistic perspectives, suggests that social embeddedness (the experience of social connection within social networks and thru group identities) and relative deprivation (the experience of being unfairly worse off than others, based in social comparisons with others) have important penalties. The psychological bonds that individuals develop with others by way of social interplay replicate sources of social assist and agency and offer targets for social comparison (subjective assessments of whether others are doing higher or worse than oneself). But even when individuals understand inequality, they could not understand it as unfair. Specifically, individuals could be motivated to deny or justify the existence of inequality to uphold beliefs concerning the fairness of the broader system. Such a perspective helps move beyond basic correlations in aggregated data (such as between-country indicators of revenue inequality and public health) and zooms in on the half of} the broader relationship could be} defined by way of such psychological processes as embeddedness and relative deprivation. Many well being inequalities have social antecedents in varied forms of inequality, together with gender, ethnicity and race. These psychological dimensions could be easily lost as the level of research and aggregation goes up. For development-induced gaps, reductions in inequality are fascinating and expected, not from proscribing gains of these taking the lead, but from broadly diffusing the newer extra superior dimensions of growth. Overall, the global bottom is catching up in primary capabilities, and inequality appears to be falling. But the global top is pulling ahead in enhanced capabilities, and here inequality is growing. Between the underside and the highest of the human growth distribution is the most numerous international middle class in historical past. It is numerous in its cultural composition, geographic location and relative place in the dynamics of convergence and divergence. It is also be|can be} a middle class more and more fragmented within international locations in access to goods and companies, as documented in developed international locations. Based on gradual progress, the evolution of inequality may follow the shape of an inverted-U over time, a model of the Kuznets curve. Subsequently, as extra people obtain access, inequality starts to increase, reflecting the division between the haves and the have-nots. Later on, quickly as} a big proportion of individuals have reached access, inequality starts to decrease: nearly all of of} individuals are performing equally nicely. There are quantity of} processes of divergence and convergence going down on the same time-overlapping Kuznets curves81-so the same particular person might be be} catching up with primary capabilities and, simultaneously, being left behind in the build up of enhanced capabilities. Inequalities in enhanced capabilities that have been already high 10 years ago have been increasing since. These simultaneous patterns of convergence and divergence are more likely to|prone to} play a distinguished position in the 21st century. Both trends are important, not only because of their separate effects-reducing excessive deprivations in the first case and concentrating energy in the second-but also because of their political implications. Once many of the population has attained sure goals, different parts become extra related for the way people see themselves in relation to others and how others understand them. They start to give attention to} their place in society and the associated rights, obligations and alternatives. But shifting targets a problem for human growth if extra efforts and accomplishments are wanted to get the same capabilities. But shifting targets a problem for human growth if extra efforts and accomplishments are wanted to get the same capabilities Chapter 1 Inequality in human growth: Moving targets in the 21st century 59 Spotlight 1. While debates on inequality are dominated by developments spanning a couple of of} a long time, and infrequently even a couple of of} years, observing and analysing how inequality emerges, the way it} concentrates energy and the way it} can result in the seize of markets and the state name for a a lot longer}, historical perspective. Such a long-term method may have seemed irrelevant for issues pertaining to the market financial system, because it was widely held that the market financial system was a contemporary phenomenon, having developed only from the 19th century on, carefully related to modernization. Recent financial historical work, however, has changed this idea, by identifying several of} market economies a lot earlier in historical past. In each of three cases analysed in depth-Iraq, Italy and the Low Countries2- markets emerged in an equitable setting and became dominant, with an institutional group that allowed easy market access to broad teams within society. The alternatives that market trade offered further pushed up financial development and well-being, with the fruits of development fairly evenly distributed. As markets turned dominant, and especially the markets for land, labour and capital, inequality also grew in a sluggish course of as ownership of land and capital turned extra concentrated. With the stagnating purchasing energy of large shares of the population, lagging demand and the declining profitability of financial investments, homeowners of large wealth more and more shifted their investments to financial markets. They used their wealth to acquire political leverage by way of patronage and buying political positions or by acquiring key positions in the fiscal regime, bureaucracy and finance and thru their dominance in financial markets and their position as creditors of the state. Each of the market economies began from a very equitable state of affairs, with comparatively equal distribution of financial wealth and political decisionmaking. This was the result of|the results of} a protracted preceding interval of smaller and bigger revolts and forms of self-organization of odd people-in guilds, fraternities, associations, companies, commons and companies (figure S1. They also won the liberty to trade their land, labour and capital without restraints by elite energy, thus opening the opportunity to use the market to this finish. Their struggles and forms of self-organization have been thus on the base of the rise of issue markets-and the rise occurred within a relatively equal setting, making certain that giant teams may access the market and benefit from market trade. This formative, optimistic section was also found in the extra acquainted, trendy cases of market economies: England, the place the market turned dominant in the seventeenth century, and the northern United States, in the first half of the 19th century. Both have been the most equitable societies of the time, with giant levels of freedom, good access to decisionmaking and comparatively equal distribution of land and different forms of wealth. The market subsequently changed the associations and organizations of odd people as the allocation system, a course of that sped up when market elites and state elites came to overlap and collectively, and infrequently intentionally, marginalized these organizations. This poses a risk, since in a market financial system, homeowners of land, capital and natural sources are sometimes far indifferent from these affected by damage from exploiting sources. They also face fewer constraints on exploitation than methods with extra divided property rights. These absentee investors changed the logic of coastal flood protection from longterm security to low price and high risk, increasing the flood risk and further marginalizing the native population. Only the place this institutional group was tailored according to growing material inequality have been disastrous effects prevented (figure S1. And if some adaptation in these cases did take place, it was usually aimed toward increasing the capability of the financial system to recuperate manufacturing levels after a shock-but on the expense of segments of the population that have been no longer included in decisionmaking. The historical cases the place markets emerged as the dominant allocation system for factors of manufacturing (land, labour and capital) all showed an accumulation of wealth in the arms of a small group, which then also concentrated political energy, shaping incentives in markets that increased inequality and environmental calamities. Today, even in parliamentary democracies, financial wealth again appears to be translated into political leverage-through lobbying, campaign financing and owning media and information-whereas mobile wealth homeowners can easily isolate themselves, for say, social disruption or environmental degradation. And perhaps they require broader and deeper consideration of a wider vary of policy actions to curb the concentration of financial and political energy.
Syndromes
- Swelling, usually in the ankles, feet, and legs
- The health care provider gently inserts a needle into the vein.
- Does the dryness seem related to wind, dust, chemicals, sun, or light exposure?
- Caffeine
- Dizziness (vertigo)
- Confusion
- Usually painless at first (may develop a burning sensation or pain when the tumor is advanced)
- High-dose test: normal suppression (however, some do not suppress, and another test is needed)
Safe 2.5mg/0.5ml fondaparinux
Other strategies for difficult intubation include retrograde intubation by placing a needle and information wire (from a central line kit) into the cricothyroid membrane or trachea and passing the information wire up and out of the mouth. An orotracheal tube could then be blindly passed over the information wire and into the trachea. There are other methods, corresponding to fiberoptic intubation by way of a laryngeal mask airway, video direct laryngoscopy, intubating 4. Medically, there are helpful strategies to "buy time" or assess response to medical remedy if a affected person can preserve air flow. The affected person is maintained in an intensive care unit with continuous pulse oximetry monitoring. Heliox (typically 79% helium/21% oxygen mixture) has been advocated as a shortterm intervention to help maximize air flow while definitive intervention is deliberate. The fuel functions by decreasing the viscosity of the inspired air, thus decreasing the mechanical work of respiratory in the narrowed airway. It can be utilized while medical intervention is taking impact; this is an excellent means of avoiding intubation. In some conditions, appropriate medical therapy of the underlying drawback, corresponding to an infection or angioedema, can obviate the necessity for intubation or surgical airway. N Outcome and Follow-Up After securing the airway, appropriate management directed on the underlying drawback is undertaken. This could include biopsy, therapy of an infection, and laboratory or radiographic workup. Evaluate for concurrent accidents corresponding to pneumothorax or esophageal or vascular harm. The therapy goals are to ensure an adequate airway, to preserve voice quality, and prevent aspiration. They may also be extreme, displaced, with airway compromise and concomitant accidents to other structures of the top, neck, and chest. N Clinical Patients usually current with a historical past of blunt trauma to the anterior neck. Common mechanisms include assault, a strangling or hanging try, and vehicular accidents together with automobiles, snowmobiles, bikes, all-terrain autos, and bicycles. A gunshot wound to the neck outcome in|may end up in|can lead to} a cricoid or thyroid fracture alone or together with other harm. Signs and Symptoms Signs and symptoms could include dysphonia, aphonia, stridor, cough, hemoptysis, dysphagia, and ache. A hallmark of extreme harm is subcutaneous emphysema, properly as|in addition to} loss of the conventional prominence of the thyroid cartilage. The harm additionally be} confined to gentle tissue, or could include cartilage fracture, mucosal disruption, or additional accidents to the pharynx, esophagus, or major vessels. In the presence of laryngotracheal cartilage disruption, intubation is mostly contraindicated. Transtracheal jet air flow may be extraordinarily useful while the definitive airway is being established. The remainder of the top and neck exam is directed at figuring out additional accidents. With a questionable laryngeal fracture, versatile fiberoptic laryngoscopy is carried out. The presence of apparent endolaryngeal mucosal disruption, bleeding, or cartilage derangement suggests the harm. Laryngology and the Upper Aerodigestive Tract 277 Other Tests Once the airway is deemed secure or stabilized, imaging must be carried out. N Treatment Options the acute therapy objective is sustaining or establishing the airway, as discussed above. The long-term therapy goals include sustaining an adequate airway, a passable voice, and the flexibility to swallow with out aspiration. Mild accidents include laryngeal edema, simple endolaryngeal lacerations with minimal cartilage publicity, and nondisplaced fractures. If severity is unclear, an examination underneath anesthesia with direct laryngoscopy and esophagoscopy is beneficial. Patients with extreme mucosal accidents and/or displaced or comminuted cartilage fractures are managed surgically with low tracheotomy adopted by exploration and repair. The basic goals include closure of tracheal defects, protection of exposed cartilage, removing of devitalized cartilage, and discount of cartilage fractures. If the vocal folds are significantly displaced, laryngofissure is carried out with repair of mucosa. N Outcome and Follow-Up Posttreatment follow-up consists of ongoing evaluation of the airway and swallowing. A barium swallow examine with speech-language pathology for evidence of aspiration is essential. Further surgical management of webbing or stenosis additionally be} required, properly as|in addition to} long-term use of a T-tube. N Epidemiology the incidence of caustic ingestion is estimated at 5000 to 15,000 circumstances annually in the United States: 53% of circumstances happen in children 6 years of age or much less. However, solely 3% of deaths secondary to caustic ingestion happen in younger children. N Clinical the affected person with caustic ingestion presents with various findings relying on sort of|the kind of} substance ingested and the amount. Signs and Symptoms With reasonable to extreme harm, symptoms include oral, neck, and chest ache, and dysphagia. Young sufferers could drool, and older sufferers could spit secretions or refuse to swallow. Respiratory problems vary from coughing and wheezing to stridor and respiratory misery. Differential Diagnosis the harm could vary from delicate to extreme end result of|because of|on account of} acid versus alkaline ingestion. Laryngology and the Upper Aerodigestive Tract 279 penetrating accidents to the pharyngeal and esophageal wall. Acids cause a mucosal surface coagulative necrosis, and deep tissue harm is unusual. A head and neck exam and skin survey for caustic burns from the spilled substance are indicated, adopted by evaluation of the oral and pharyngeal mucosa for harm. Damage, phrases of|when it comes to|by means of} an estimate of the depth of harm, is assessed on the proximal extent of harm. However, distinction swallow studies are sometimes used to assess the progression of stricture formation during restoration. N Treatment Options Nonoperative remedy consists of hydration, acid-blocking medications, and observation. A thoracic surgery session is obtained for management of perforation or high-grade accidents. There has been a development toward early surgical intervention by thoracic surgeons (within 36 hours) to treat deep esophageal accidents. For evidence of a high-grade harm on endoscopy, a feeding tube must be positioned underneath direct vision. Complications together with mediastinitis, perforation, and stricture formation vary from 10 to 20%. Stricture growth usually begins at week 3 or 4; a distinction swallow examine or a follow-up endoscopy is helpful at this time. Symptoms and signs include hoarseness, ache, dysphagia, cough, dyspnea, stridor, and signs of systemic illness. Therapy is directed on the causative organism and is supportive of any airway points current. Laryngoscopy with biopsy and/or culture additionally be} essential as some infections could mimic neoplasms, or require this info for a definitive diagnosis. Infectious laryngitis additionally be} caused by viral, bacterial, mycobacterial, fungal, and even protozoan organisms. History and bodily examination, together with laryngoscopy, are instrumental in establishing the diagnosis.
Best 2.5/0.5ml mg fondaparinux
Walking little via Kings (3) Park it he had a bag with something in resting between his leg. It look (9) as if from the expression on the little boy (10) face that he was quit (11) shock 12) on the fowl. Chapter 11 the Neurology of Language the neurology of language, language and the brain. Observation (1) illustrates reality that|the reality that} the bodily organ underlying the flexibility to course of language is the brain; specifically, brain injury can result in|may end up in|can lead to} a languagespecific dysfunction known as aphasia Observation (2) illustrates reality that|the reality that} most human beings course of language within the left cerebral hemisphere. This reflects reality that|the reality that} human brains exhibit hemispherical specialization: the left hemisphere controls one set of talents, among them language in processing, while the right controls different talents, such as orientation (3) illustrates the fact fact} area and visuospatial processing. Observation that different parts of every hemisphere management different psychological 271 272 Chapter 11 functions. Observation addition to inflicting a language dysfunction (aphasia), disrupt different forms of (4) illustrates reality that|the reality that}, in brain injury might comprehension and manufacturing. Before stepping into the small print points} of neurolinguistics, ought to always|we must always} address three points regarding the nature of research in this serve the language of sufferers a stroke, a tumor, or field. A stroke causes injury by shutting off the blood oxygen provide, to some half of} the brain. A tumor causes on half of} the brain from the within, in effect "squeezbetween the tumor itself and the skull. A trauma to the brain is brought on by some kind of external force, such as a blow to the head. Of these three forms of injury, stroke injury is typically of extra curiosity to the neurolinguist than injury brought on by tumor or trauma. This is end result of|as a outcome of} a stroke is able to damaging a really specific and localized half of} the brain, whereas injury brought on by tumor or trauma tends to be extra world, affecting a larger half of} the brain. It is correlational in that it tries to discover correspondences between specific language functions and specific parts of the brain. The neurolinguist draws inferences of the following type: sufferers 1, 3, and 5 all have had strokes in area A of the brain and all exhibit language dysfunction Y; sufferers 2, four, and 6 all have had strokes in area B of the brain and all exhibit language dysfunction Z; therefore, it appears that|it appears that} brain area A controls operate Y and that brain area B controls operate Z. For example, in a sample of 10 sufferers with injury to brain area A, only eight might exhibit language dysfunction Y. In short, then, neurolinguists basically make statistical correlations between localized brain injury and specific language pro- cessing deficits. Third, as was the case with first-language acquisition, the research strategies used in neurolinguistics have some inherent difficulties. Moreover, the affected person must have} comparatively localized brain If the brain injury and must additionally exhibit fairly specific behavioral abnormalities. Anatomy of the Xerrous System the neuron: there are about 12 billion neurons within the nervous system. Each neuron is made up of three parts: a cell physique an axon which transmits nervous impulses away from the cell physique: and dendrites, which receive impulses coming in to the cell physique. The level at which the nervous impulse passes from the axon of 1 neuron to the dendrites of another is known as} a synapse Thus, neurons talk with one another by transmitting data via this complex of axons, dendrites, and synapses. The spinal twine transmits the message from the brain that claims, for instance, to cross your proper leg over your left. These structu lually as a bridge between the) spinal twine and the upper brain stem. Damage is to the decrease brain stem could cause a speech dysfunction to identified as|often recognized as} dysarthria. The greater brain stem 3 > consists of the buildings management involuntary regulators- functions such as breathing, coronary heart fee, thalamus and midbrain these and all physique temperature. In addition, the thalamus receives incoming sensory stimuli cept for the sense of smell) and transmits every stimulus to the half of} the brain (5) Cerebrum ^^ Thalamus (3) Higher brain stem ^. The cerebellum (4) which lies to the rear of the brain stem, the cerebellum plays no recognized role, nevertheless, in language, processing. For example, when you increase your proper arm, the message to achieve this originates within the left cerebral hemisphere. Likewise, when you step on a tack along with your left foot, the feeling of pain is processed by your proper cerebral hemi(5) is is the cerebrum the half of} the brain on high of the brain stem left lum. Each cerebral hemisphere consists of a mass of white fiber tracts lined by the cortex, which is roughly zero. Association fibers join different parts of the cortex within one hemisphere, enabling these parts to talk with one another. Projection fibers join the cortex to the brain stem and spinal twine, enabling the cortex to talk with the peripheral nervous system. Transverse fibers join the two cerebral hemispheres, enabling them to talk with one another. For example, the frontal lobe processes olfactory stimuli, (lobes: the frontal lobe and the temporal lobe processes auditory stimuli. Each cerebral hemisphere has these lobes, so ready to} converse of the left temporal lobe, the right occipital lobe, and so forth. We will see in a while that the left frontal and temporal lobes home the major language processing centers for most people. Certain of these fissures and convolutions function essential anatomical landmarks. The fissure of Rolando (6), additionally known as the central sulcus, separates the frontal and parietal lobes. The supramarginal gyrus and the angular gyrus (7) lie within the inferior half of} the parietal lobe. The major motor cortex (9) is a strip of cortex about lying instantly anterior to the fissure two centimeters extensive of Rolando. Each level within the major motor on the other facet of the tongue, and jaw are managed by the it cortex controls a discrete set of muscle tissue. For example, stimulating the superior half of} the primary motor cortex will trigger the leg muscle tissue physique to contract. Movements of the lips, inferior half of} the primary motor cortex near where meets the it fissure of Sylvius. Scientists within the 276 Chapter 1 localizations t camp believed that specific parts of the brain managed different psychological functions. The localization of was lastly demonstrated to the satisfaction of most neuroscientists by the French doctor Pierre Paul Broca (1824-1884). Broca argued that the lesion had begun within the third convolution of the frontal lobe within the left hemisphere. The only phrases he could utter had been his name and the French phrases forties, no, three, and always. His motor power, nevertheless, was intact: in different phrases, his inability to converse and write was not paralysis. After his dying, an - - post-mortem revealed localized injury to the third convolution of the original lesion. At the same time, a affected person was reported with later that injury to the third frontal convolution in the right hemisphere, without any kind of language disturbance. Broca was the first to substantiate convincingly the localizationist concept of cortical operate. Moreover, he was the first to suggest the idea that|the concept|the idea that} the frontal lobe is specialized for language. Wernicke the next main Carl step in our understanding of aphasia was put forward by the German Wernicke (1848-1904). Wernicke was the first to differentiate the expressive aphasia described by Broca from sensory aphasia. Wernicke correlated sensory disturbance with injury to the convolution of the temporal lobe within the left hemisphere. Wernicke published his theories in 1S~4 as Der aphasiscbe Symptomenkomplex the Aphonic Complex). Wernicke subdivided that hemisphere as subserving two different language functions: the frontal lobe controls expression, and the temporal lobe controls comprehension. The expressive aphasia described by Broca results from injury near the motor cortex, which in flip controls outgoing motor actions, including the articulation of speech. The receptive aphasia described by W ernicke results from injury near the sensory cortex, specifically the primary auditory cortex (Heschl gyrus), which processes incoming auditory stimuli, including speech.
Generic fondaparinux 2.5/0.5ml mg
We have primarily justified two levels of phonological illustration: the phonemic, the place phonemes are described, and the phonetic, the place allophones. This state of affairs is summarized in Figure 6-4, which illustrates truth that|the truth that} audio system of English perceive the phrases Tim, stem, hit, hit me, and Betty as containing cases of the identical phoneme, A/. Yet every occasion of A/ differs on the phonetic stage, relying on the context during which A/ occurs. This dialogue raises the problem of how to to|tips on how to} tell whether two segments are allophones of various phonemes or allophones of the identical phoneme. If the substitution modifications one word into another, then the 2 telephones contrast and are allophones of various phonemes. Thus, [f and [dn contrast, and due to this fact are allophones of various phonemes, particularly A/ and /d/, respectively. Thus, [t 1 and [t] are in free variation, and due to this fact are allophones of the identical phoneme, particularly A/. These by no means occur in the h similar context; [t at all times occurs before a careworn vowel and [r] at all times occurs before an unstressed vowel. Phonology 125 in complementary distribution and are allophones of the identical phoneme. Linguists have posited the phonemic and phonetic levels of illustration to account for truth that|the truth that} two segments may be be} each alike. We will now take a look at|have a look at} some frequent phonological ailes or processes in English, working from the info to the rules themselves. Consider the following English phrases, every of which is accompanied by its phonemic and phonetic representations. Now we h] are in a position to hypothesize a revised version of our rule: /p/ is becomes [p when it each adopted by a careworn vowel. This rule precisely predicts h]; those circumstances the place /p/ becomes [p stays unchanged. However, since informal prose statements can usually be (unintentionally) imprecise or ambiguous, phonologists have adopted the practice of tion. Z it W becomes section X when follows Y and precedes (Read the arrow as "becomes" and the slash as "in the following setting. Since /p/, A/, and /k/ constitute the set of voiceless stops in English, we may state the Aspiration Rule for all of them as follows. Phonology 1 27 Vowel Lengthening Consider the following English phrases, every of which mic and phonetic representations. Once it once more, our task to determine that under what situations becomes left We may begin by hypothesizing some property of the consonant to the of the vowel causes sider, for to lengthen. The former has a long vowel and the latter has a brief vowel, yet in each circumstances the vowel is preceded by [s]. Thus, the consonant to the left of the vowel obviously has no effect upon the size of the vowel, since right here the identical consonant precedes each a long vowel and a brief vowel. Note that the vowels in warmth, leaf and stop are brief, and each one is adopted by a voiceless consonant ([t], If], and [s] are [-voice]). In contrast, the vowels in heed, leave, seize, and keel are long and each one is adopted by a voiced consonant ([d], [v], [z], and [1] are [+voice]). It predicts exactly those circumstances the place /i/ becomes [i:] and, by exclusion, it also predicts the place example. As in our Aspiration Rule mentioned earlier, there are variations on this You might also see this rule written as follows. Before getting started, nonetheless, note that the vowels in pan, pad, Pam, and pang should be long. In this case, vowel lengthening has nothing to do with vowel nasalization, so it has been ignored. Likewise, the aspiration notation in this information has been omitted, since aspiration has nothing to do with vowel nasalization. Since map [maep] and gnat [naet] each include a preceding nasal consonant but no nasalized vowel, vowel nasalization should not be brought on by a preceding nasal consonant. This rule precisely predicts exactly the circumstances the place /ae/ becomes [ae]; and, by exclusion, it also predicts the place /ae/ stays unchanged. V -> [+ nasal] / C [+nasal] Again, we see that phonological rules apply to classes of segments, somewhat than to It which a section becomes extra like a neighboring section indirectly, is known as} an assimilation rule. In this case, a vowel becomes extra like an adjoining nasal consonant by becoming nasalized itself. We by noting that A/ and /d/ by no means become [f] once they begin or end a may begin word. Thus, the relevant alveolar stops (A/ and /d/) have to be people who occur somewhere in the middle of|in the midst of|in the course of} the word. That is, it it predicts exacdy those the place /t/ and /d/ become and, by exclusion, also predicts the place proceed to be} unchanged. Nasal Deletion Consider the following English phrases, every of which is accompanied by its phone- mic and phonetic representations. Second, a rule deleting a nasal consonant applies, so that may t kaent becomes [kaet]. What we need to|we have to} do is determine (a) under what situations Nasal Deletion applies, and (b) in what order Vowel Nasalization and Nasal Deletion should apply. We are now are|are actually} in a position to propose a rule: delete n when it precedes this rule accounts for the absence of [n] in can and. The one that precisely maps the phonemic illustration into the phonetic illustration is appropriate. Nasal Deletion has eliminated the n before Vowel Nasalization has had an opportunity to apply, thus blocking the application of the Vowel Nasalization Rule. Now lets try Vowel Nasalization before Nasal Deletion, as follov is it obviously mistaken: t. Phonemic Level Vowel Nasalization sal kaent kaent Deletion equipment [kaetl Phonetic Level this ordering yields which is the phonetic illustration of can Vowel Nasalization. Thus, the correct ordering between the 2 rules is Vowel Nasalization first and then Nasal Deletion. In this case, the n is current to trigger 132 Chapter 6 leaving this section, nonetheless, can t Our dialogue of representations. A spectrogram is basically an image of the acoustic traits of utterance. Since nasals sometimes display certain acoustic traits, we an may take a look at|have a look at} the spectrogram If and attempt to determine if these specific acoustic properties are current. This, after all, is predicted by our Flapping Rule, which states that an alveolar stop between a careworn vowel and an unstressed vowel becomes a flap. That is, the lJ in canty ocand a vowel ll on the phonemic stage of illustration. There are quite a few parallel circumstances the place Flapping can apply to t/ after a nasal consonant but to not /d/: for instance. Thus, we constructed a concept of phonology to account for our authentic observations. This concept it could prove to be incorrect partly, but structure of is the most effective working hypothesis of the inner the current time. Also, you might need to examine your understanding of the material in this chapter by working through the practice problems and solutions that follow the readings. Schane and the accompanying workbook provide a wonderful introduction to "doing" phonology; they deal primarily with non-English information. It represents the cunent interest in "multi-tiered" phonology, which treats the syllable as hierar- chically structured somewhat than as simply a string of linear segments. Anderson is an excellent reference book dealing with the event of phonology as a and its key figures. Chomsky and Halle is the basic statement of linear generative phonology (the concept mentioned in this chapter), and Jakobson. These last two works, nonetheless, are tough going and are now are|are actually} mainly of historical interest.

Fondaparinux 2.5/0.5ml mg
Treatment of the first trigger can be necessary in circumstances not brought on by long-term furosemide remedy. In infants being given furosemide, substitution of a thiazide diuretic for furosemide can decrease the calcium excretion and lead to shrinkage of calculi and enchancment of the medullary nephrocalcinosis. The long-term prognosis has been correlated with the course of the urinary calcium excretion. Long-term studies of untimely infants with nephrocalcinosis have advised that 30% to 50% of the children proceed to have evidence of renal calcification as much as} 5 years after prognosis. Renal calcifications: a complication of long-term furosemide remedy in preterm infants. What are the environmental and technical factors that may affect on} blood stress measurements within the newborn Cuff inflation, by itself, can stimulate the startle response, which may trigger a transient increase in blood stress. In addition, physique geography has an influence on blood stress measurements: Pressures measured within the legs are normally somewhat greater than these measured within the arms. Data relating to the normal ranges of systolic and diastolic blood pressures for term newborns and untimely infants at varied gestational ages have been printed. Studies have shown that blood stress within the neonatal interval increases with gestational age, delivery weight, and postmenstrual age. A more representative blood stress measurement is recorded when the toddler has not been fed or manipulated for 90 minutes before the evaluation; further refinement is achieved when a number of} blood stress measurements are made over a interval of 5 to 10 minutes. The prognosis of hypertension should be made only if the systolic and diastolic blood pressures are above the 95th percentile on at least of|no less than} three separate blood stress measurements recorded at 2-minute intervals during a time when the toddler is quiet and otherwise undisturbed (Table 9-7). [newline]Extremely-low-birth-weight infants with bronchopulmonary dysplasia appear to develop hypertension within the absence of clear evidence of renal artery occlusion at a rate greater than that seen with renal thrombosis. Blood stress measurement is usually neglected by pediatricians due to the problem in acquiring an correct dedication in these tiny babies. Most circumstances of hypertension in newborns are brought on by excessive circulating concentrations of hormones that trigger hypertension outcome of|because of|on account of} their capacity to increase peripheral vascular resistance and/or their capacity to trigger salt and water retention. Rare endocrine disorders similar to virilizing adrenal hyperplasia brought on by 11-hydroxylase deficiency and first hyperaldosteronism might trigger neonatal hypertension owing to overproduction of mineralocorticoid (desoxycorticosterone within the case of 11-hydroxylase deficiency; aldosterone in patients with hyperaldosteronism). The overproduction of mineralocorticoid in these illnesses causes hypertension by way of|by means of|by the use of} inappropriate renal salt and water retention. What abnormality of the physical examination of a hypertensive toddler suggests that coarctation of the aorta may be be} the elevated blood stress In hypertensive infants measurement of blood stress in each upper and decrease extremities is essential. Coarctation of the aorta should be suspected if the systolic stress within the leg is greater than 10 mmHg decrease than the systolic stress within the arms. It is also be|can be} necessary to observe that hypertension might persist in these infants even after the coarctation has been surgically repaired. Nephrology and fluid/electrolyte physiology: neonatology questions and controversies. Hypertension related to umbilical catheterization often occurs during therapy or immediately after removal of the catheter. The renal parenchyma that experiences obstruction to venous drainage appears swollen and hyperechoic. Furthermore, the utility of renal scans is restricted by the fact that|the truth that} they typically require the sick toddler to be transported from the neonatal unit to the nuclear medicine department. Evidence that nephrectomy improves patient survival is unsubstantiated, and this procedure certainly leads to a decrease in practical nephron mass. The usefulness of thrombolytic or anticoagulant remedy should be qualified by such phrases as perhaps or sometimes. However, anticoagulants might shield infants with intrinsic abnormalities of the coagulation cascade from experiencing secondary thrombotic events. Prune-belly syndrome is a uncommon congenital anomaly that consists of genital (usually undescended testes) and urinary tract abnormalities with absent or decreased belly wall musculature. Prune-belly syndrome is brought on by urethral outlet obstruction early in development. What are the commonest urinary tract anomalies that occur in patients with prune-belly syndrome From backside to prime, the commonest urinary tract anomalies are as follows: n the bladder neck is patulous. The bladder wall may be be} thickened, but the inner contour of the bladder is clean, without trabeculations or diverticuli. Ureteral abnormalities generally encompass irregular dilations and narrowings, often most dramatic within the decrease ureteral segments. It is necessary to observe that the anatomic abnormalities of the urinary tract in patients with prune-belly syndrome may be be} brought on by major, intrinsic, and diffuse defects of embryologic development of the structures concerned, which are different from the discrete lesions of obstruction or reflux that will occur within the urinary tract of otherwise normal newborns. However, the abnormalities might appear much like those that occur in prune-belly syndrome. Similarly, although ureteral dilation in otherwise normal infants is usually associated with vesicoureteral reflux or obstruction, an identical ureteral lesion in a patient with prune-belly syndrome might occur within the absence of reflux or obstruction. What different anomalies occur outdoors the genitourinary system in infants with prune-belly syndrome Patients with prune-belly syndrome often have further problems, including pulmonary hypoplasia and Potter facies (flattening of the nostril, redundant pores and skin, receding chin, ocular hypertelorism, and lowset ears); hip dislocation or subluxation; talipes equinovarus; congenital cardiac disease, especially atrial septal defect, ventricular septal defect, and tetralogy of Fallot; and gastrointestinal anomalies. The urologic/renal dysfunction in patients with prune-belly syndrome is almost of} certainly answerable for a number of the} nonurologic issues. For instance, oligohydramnios, a typical complication of prune-belly syndrome pregnancies, accounts for the pulmonary hypoplasia, the hip dislocation or subluxation, and the talipes equinovarus seen in these newborns. It has been advised that the underlying defect in prune-belly syndrome is irregular mesoderm development. Which diagnostic studies help the neonatologist in evaluating a child with prune-belly syndrome The initial work-up should embody (1) belly and pelvic ultrasonography to present a fundamental road map of the genitourinary anomalies and (2) voiding cystourethrography to diagnose vesicoureteral reflux and reflux right into a patent urachus. If the toddler is steady enough to be transported, different imaging studies significantly enhance understanding of the genitourinary pathology. Because an toddler with prune-belly syndrome may also harbor gastrointestinal and cardiac anomalies, an upper gastrointestinal tract sequence with small bowel follow-through, a barium enema, an electrocardiogram, and an echocardiogram are also wanted as part of of} the initial work-up. Every newborn with prune-belly syndrome should be evaluated by a pediatric urologist. [newline]However, intervention during the newborn interval should be limited to the least invasive procedures available and should be used solely when essential to relieve high-grade obstruction within the urinary tract. More in depth genitourinary reconstructive procedures should be postponed to a later date and, in fact, may not be not|will not be} necessary in any respect. Orchidectomy, as a way to stop testicular neoplasia, is an choice end result of|as a outcome of} the reproductive potential of boys with prune-belly syndrome might be low. An alternate approach is to relocate the belly testes into the scrotum by considered one of a variety of|quite so much of|a wide range of} advanced surgeries. In any case these surgical interventions can wait until the toddler is a number of} months old. Surgical plication of the lax belly musculature is necessary for the psychological well-being of patients with prune-belly syndrome, but this cosmetic reconstruction should probably not be performed in a newborn. Long-term follow-up of whole belly wall reconstruction for prune belly syndrome. Contemporary epidemiology and characterization of newborn male with Prune Belly Syndrome. The contralateral kidney may be be} normal, absent, hydronephrotic, ectopic, or dysplastic. In polycystic renal disease heaps of|there are numerous} cysts in each kidneys, no dysplasia, and continuity between glomeruli and calyces. Describe the management of autosomal recessive polycystic kidney disease in a neonate. What are some issues that may occur in infants with autosomal recessive polycystic disease Affected neonates have extraordinarily large cystic kidneys and respiratory misery, and so they often manifest vital renal failure immediately after delivery. What are the indications for liver and renal biopsies in neonates with polycystic kidneys
Proven 2.5mg/0.5ml fondaparinux
This ought to embody an analysis of the next: G the final appearance of the patient. Usually, the nose is decongested with oxymetazoline (Afrin, Schering-Plough Healthcare Products Inc. The tip of the scope is inserted into the nostril, and beneath direct imaginative and prescient is advanced inferiorly along the floor of the nose into the nasopharynx. The nasopharynx is assessed for plenty or asymmetry, adenoid hypertrophy, and infection. The scope is then guided inferiorly to examine the bottom of tongue, valleculae, epiglottis, piriform sinuses, arytenoids, and vocal folds. Asking the patient to cough and to phonate will reveal vocal fold movement abnormalities. Perioperative Care and General Otolaryngology 5 N Other Tests Often, laboratory studies, audiograms, or imaging studies are reviewed. Generally, a concise differential analysis is given, listing the entities would possibly be} thought of most related. A plan is then mentioned, including additional checks to affirm or exclude possible diagnoses nicely as|in addition to} medical or surgical therapies that shall be instituted or thought of. An extra objective is to make sure that|be certain that} medical administration is optimized preoperatively. Laboratory and physiologic checks and screens may be ordered and reviewed prior to surgery. Mild to moderate systemic disturbance triggered either by the situation to be treated surgically or by different pathophysiologic processes. Severe systemic disorders could be|that may be|which could be} life threatening, not at all times correctable by operation. Seriously sick patient who has little probability of survival, however is submitted to the operation in desperation. Various types of airway administration are mentioned under, contemplating anatomy, innervation, indications, instrumentation and tools, and scientific context. N Airway Anatomy There are two physiologic entry points to the airway: the nose and the mouth. The epiglottis, located at the base of the tongue, separates the oropharynx from the hypopharynx. The larynx is made up of a cartilaginous structure supported by muscles and ligaments. G Nasal mucosa: by the sphenopalatine ganglion department of the middle division of the trigeminal nerve eight G Handbook of Otolaryngology�Head and Neck Surgery G Posterior pharynx (including uvula and tonsils): by the continued branches from the sphenopalatine ganglion Oropharynx and supraglottic space: by the glossopharyngeal nerve; branches of this nerve embody the lingual, pharyngeal, and tonsillar nerves Trachea: by the recurrent laryngeal nerve Larynx: sensory and motor innervation from the vagus nerve G Sensory: above the vocal folds, innervation is supplied by the interior department of the superior laryngeal nerve; under the vocal folds, by the recurrent laryngeal nerve. G Motor: all muscles are supplied by the recurrent laryngeal nerve apart from the cricothyroid muscle, which is supplied by the exterior department of the superior laryngeal nerve. G G N Airway Equipment Oral and Nasal Airways In anesthetized patients, lack of airway tone permits the tongue and epiglottis to contact the posterior pharyngeal tissue resulting in obstruction. Artificial airway devices may be placed in the nose or mouth to present an air passage. Nasal airways carry a danger of epistaxis and ought to be avoided in anticoagulated patients. These devices should also to|must also} be avoided in patients with basilar skull fractures to avoid intracranial penetration of the airway device. If an airway device is indicated in a lightly anesthetized patient, the nasal route is usually tolerated higher. Face Masks the face masks is designed to contour and conform to a variety of facial options with the intention of making an hermetic seal able to delivering gasses from the anesthesia tools. Laryngoscopes probably the most generally used intubating laryngoscopes by the anesthesiology group have curved (Macintosh) or straight (Miller) blades and an open-blade design. There are a variety of|quite so much of|a big selection of} operative laryngoscopes could be|that may be|which could be} useful for intubation, such as the Holinger or Dedo laryngoscope. N Airway Assessment A full airway examination seems at quantity of} aspects of the airway. However, the first precedence is to establish patients who could also be} troublesome to ventilate or intubate. This is critically essential: induction of common anesthesia with the next incapability to adequately ventilate the patient is an acute lifethreatening emergency. Perioperative Care and General Otolaryngology 9 troublesome airway before induction will enable the operative and anesthetic group to institute an acceptable plan, backup plans, and assemble and test airway tools ahead of time. G Mallampati classification: used to predict the convenience of intubation by looking at the anatomy of the oral cavity while the patient is sitting upright in the neutral position. Mouth opening: lower than two finger-widths of mouth opening (trismus) recommend difficulty with intubation. Cervical spine actions: mobility of the atlantooccipital and atlantoaxial joints could also be} assessed by asking the patient to prolong the head while the neck is in flexion. Extension of the head with atlantoaxial joint immobility ends in higher cervical spine convexity, which pushes the larynx anteriorly and impairs laryngoscopic view. Previous documentation of laryngoscopy ought to embody the grade of glottic view. N Preoperative Medication Medications are sometimes administered preoperatively to alleviate anxiety, to present analgesia, or as aspiration prophylaxis (Table 1. The form prevents obstruction of the surgical area and suits surgical retractors such as the Crow�Davis retractor. This tube works well by way of a tracheotomy as curved inferiorly out of the surgical area with out kinking and sutured in place quickly. Laser-resistant endotracheal tubes are utilized in laser surgery, significantly remedy of laryngeal lesions. By stopping an interplay of inhaled oxygen and the laser, these tubes assist prevent airway fires. For thyroid surgery, a tube with contact electromyographic electrodes positioned at the stage of the vocal folds permits intraoperative monitoring of recurrent laryngeal nerve integrity. Endotracheal Intubation Procedure G Preoperative analysis will assist decide the route (oral vs. This prevents spillage of gastric contents into the pharynx during the period of time from induction of unconsciousness to placement of the endotracheal tube in the trachea. After intubation, possible complications embody aspiration, laryngospasm, transient vocal fold incompetence, pharyngitis, or tracheitis. This position aligns the oral, pharyngeal, and laryngeal axes such that the passage from the lips to the glottic opening is a straight line. Advancing the blade posteriorly and toward the midline, the tongue is displaced to . Placement of blade depends on by} which type has been chosen: G Macintosh (curved) blade: the tip of the blade is advanced until the tip enters the vallecula (the space between the epiglottis and the bottom of the tongue). Miller (straight) blade: the tip of the blade is handed under the laryngeal surface of the epiglottis, which is then lifted to expose the vocal folds. G Regardless of the blade chosen, the laryngoscope is lifted upward and ahead in the direction of the long axis of the handle. The vocal folds ought to be visualized prior to advancement of the endotracheal tube. Passing the endotracheal tube from the proper, little resistance ought to be encountered. The balloon cuff of the endotracheal tube ought to move 1 to 2 cm past the vocal folds. Surgical landmarks are palpated, and a hori- zontal or vertical pores and skin incision is made between the cricoid and suprasternal notch. The thyroid isthmus is encountered and either retracted caudad, cephalad, or divided utilizing a monopolar cautery. Once the trachea is in view, a tracheal hook could also be} used to present superior retraction on the cricoid ring; next the trachea is entered, usually under the second ring, and a window or inferiorly based (Bjork) flap is created. An acceptable tracheotomy tube is then placed while the anesthesiologist withdraws the endotracheal tube beneath direct visualization. Then, the tracheotomy tube is sutured at 4 corners with suture, and a tracheotomy tie ought to be placed to safe the tracheotomy tube around the neck. Complications of tracheotomy embody bleeding, infection, crusting or mucus plugging, pneumothorax, and unintended dislodgment of the tracheotomy tube.
References:
- https://www.tourette.org/media/Schrock_Et_Al_2014_DBS_TS_Guidelines.pdf
- https://wwwnc.cdc.gov/eid/content/9/11/pdfs/v9-n11.pdf
- https://jamanetwork.com/journals/jama/articlepdf/2662888/jama_lisonkova_2017_oi_170124.pdf
- https://www.tn.gov/content/dam/tn/hsda/documents/Deemed%20Complete-CN2009-029%20Natchez%20Ctr%20Behavioral%20Medicine.pdf