.png)
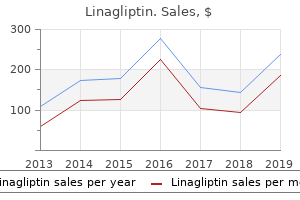
Effective 5 mg linagliptin
Summary: this article discusses causes of altered mental status, an preliminary method to evaluating the affected person, and components of the advanced diagnostic workup. Relationship Disclosure: Dr Douglas has served as editor-in-chief of the Neurohospitalist and has acquired private compensation for medical document review and skilled witness testament. Dr Josephson has acquired private compensation for editorial activities from Annals of Neurology and Journal Watch Neurology. Unlabeled Use of Products/Investigational Use Disclosure: Dr Douglas discusses using of} antipsychotics for the treatment of agitated delirium. It is a standard cause for emergency department visits, hospitalization, and neurology consultation. As many as 5% to 10% of emergency department patients have altered mental status, with considerably greater charges among the elderly; over half of these patients are admitted to the hospital. The differential diagnosis for altered mental status is broad and consists of lifethreatening yet treatable conditions; subsequently, a systematic method to the affected person is critical. Most inner medicine hospitalists and emergency department physicians are snug performing the preliminary workup, and neurologists are often consulted solely when a focal lesion is suspected or no quick trigger can be discovered. This article briefly discusses the preliminary method to the affected person with altered mental status and then delves right into a extra detailed dialogue of the advanced workup and less frequent diagnoses with which the neurologist ought to be acquainted. In the present conception of brain operate, these processes are understood to be carried out by cortical regions and extra widespread neuronal networks. For instance, the power to recognize each written and oral language, interpret its that means, and produce speech is a part of|is part of} consciousness often served by regions in the left temporal and frontal lobes and their connections. Pathologic states of arousal vary from coma, a state of full unresponsiveness with out eye opening, to drowsiness, during which a affected person is arousable however needs stimulation to stay awake, to hypervigilance, the place patients are awake however unable to focus their attention and are easily distracted by extraneous stimuli. If such patients are in a position to} communicate, they nearly universally have a deficit of attention and seem disoriented and confused. Arousal is maintained by varied techniques of neurons, most of that are positioned in the brainstem, hypothalamus, basal forebrain, and thalamus and project diffusely all through the cortex. Altered mental status is a broadly inclusive term used to describe a affected person with a change in both the content material of consciousness or the extent of arousal. Encephalopathy can also be|can be} a nonspecific term, usually used interchangeably with altered mental status, which implies a diffuse course of inflicting a change in the stage of arousal. Delirium is a extra specific term, outlined as an acute change in mental status characterized by a deficit in attention and a fluctuating course with both disorganized pondering or change in the stage of arousal. Occasionally, nevertheless, a focal deficit additionally be} misclassified as delirium by an inexperienced clinician; conversely, delirium could not often be caused by a focal lesion. Examples are basilar meningitis or a big hematoma with mass impact resulting in hemiparesis and decreased responsiveness. A patent airway and intact circulation should be ensured, adopted by measurement of important signs and serum glucose. A targeted neurologic examination is imperative to rule out structural lesions, corresponding to a big stroke or hemorrhage, requiring emergent administration. Naloxone ought to be administered if narcotic overdose is suspected; thiamine and glucose are additionally given routinely. Thiamine ought to all the time be administered with or earlier than glucose to keep away from precipitation of October 2011 968 Once the affected person is stabilized, additional information gathering can be initiated (Table 1-1). After the time course is established, the history ought to dedication of baseline cognitive operate and whether any previous episodes of altered mental status have occurred. Other necessary components of the history embrace symptoms of infection corresponding to fever, headache, stiff neck, cough, or dysuria; current drugs and up to date medication modifications; leisure drug and alcohol use; and history of recent trauma. Specific attention ought to be paid to drugs recognized to trigger delirium, corresponding to these with anticholinergic properties, benzodiazepines, and narcotics. The common physical examination ought to potential medical causes of altered mental status. Percussion and auscultation of the lungs could reveal proof of pneumonia or persistent obstructive pulmonary disease. Examination of the heart and extremities could show signs of endocarditis or congestive coronary heart failure. Inspection of the skin can show signs of liver disease or needle marks indicating injection drug abuse. Signs of meningitis ought to be sought, together with meningismus and the petechial rash associated with meningococcemia. However, the choice relating to whether to pursue a lumbar puncture ought to by no means relaxation solely on the presence or absence of meningismus, outcome of|as a end result of} a number of} research suggest nuchal rigidity, Kernig sign, and Brudzinski sign are insensitive. Patients with psychosis are often oriented and have regular attention despite the presence of delusions, hallucinations, and disorganized pondering. Several stroke subtypes can present with modifications in mental status ranging from abulia (in thalamic or orbital frontal infarcts) to agitation (in posterior cerebral artery infarcts and nondominant parietal lobe infarcts) to Wernicke aphasia (which can be initially mistaken for psychosis or delirium in left middle cerebral artery infarcts) to coma (with basilar artery occlusion). The focal signs that often accompany such lesions additionally be} overlooked by the non-neurologist. Focal deficits accompanying altered mental status can also be seen in lesions inflicting mass impact or hydrocephalus or in these associated with meningitis. The ultimate the preliminary analysis includes laboratory testing to rule out metabolic derangements and common infections that result in altered mental status. This features a full blood depend; measurement of electrolytes together with calcium, magnesium, and phosphorous; and exams of renal and liver operate. An arterial blood fuel additionally be} useful in revealing hypoxia or hypercarbia; a possible clue to the latter is an elevated bicarbonate focus in the routine blood chemistry suggesting persistent respiratory acidosis. However, an extensive workup for altered mental status is pricey, may cause iatrogenic issues, and additionally be} pointless in some instances. Delirium is theorized to occur in the setting of decreased cerebral reserve, resultContinuum Lifelong Learning Neurol 2011;17(5):967983 ing in diminished capability to face up to a variety of|quite a lot of|a big selection of} insults that may trigger the acute confusional state. Advanced age and preexisting cognitive dysfunction are the most persistently recognized threat factors for delirium in potential research. Although some types of neurodegenerative disease, corresponding to Lewy physique dementia, could trigger delirium in and of themselves, most patients with dementia exhibit regular levels of arousal and a spotlight till the very late levels of disease. Occasionally prion disease could progress rapidly sufficient to present with encephalopathy. The insults that may precipitate delirium embrace a wide range|a variety} of pathologic conditions (Table 1-2), many of which may trigger encephalopathy in patients with out threat factors, and iatrogenic insults that the affected person with adequate cognitive reserve can often face up to (Table 1-3). If a affected person with out recognized underlying neurologic disease turns into delirious with a relatively innocuous insult corresponding to a urinary tract infection, follow-up ought to be organized with neurology to display screen for an underlying course of corresponding to an incipient neurodegenerative disease. These patients have essentially failed a ``stress test for the brain,' and an underlying disorder ought to be sought. Patients with out threat factors for delirium and those at excessive threat for intracranial infection or neoplasm generally require additional workup as nicely. Whether brain imaging ought to be routinely obtained in patients with encephalopathy with out focal neurologic signs or the aforementioned threat factors is extra controversial. Several attempts have been made to examine the yield of brain imaging in patients with altered mental status. Although strokes inflicting altered mental status are nearly all the time accompanied by focal deficits, particularly upon cautious neurologic examination, sometimes such localizing signs are absent (Case 1-1). Case 1-1 A 55-year-old right-handed man was delivered to the hospital with confusion. Two weeks ago, he skilled the sudden onset of fluctuating disorientation and forgetfulness. He additionally had exhibited unusual behaviors corresponding to attempting to flip the tv on along with his cellular phone. He underwent a right anterior temporal lobectomy 3 years ago for medically refractory epilepsy however still had one complicated partial seizure per thirty days. He had additionally skilled a steady decline in reminiscence and focus associated with parkinsonism over the past eight years. His drugs included carbamazepine, divalproex, levetiracetam, memantine, venlafaxine, quetiapine, and tamsulosin. On examination he was awake however demonstrated psychomotor slowing, disorientation, and impaired attention and short-term recall.
Buy 5 mg linagliptin
Clinical evidence the condition addressed on this guideline was first described as Primary Ovarian Insufficiency by Fuller Albright in 1942 (Albright, et al. Subsequently several of} completely different terms have been used, with variation between specialities. This would make clear information given to women, improve communication between health professionals, significantly facilitate knowledge collection and audit, and assist future research. The problem of terminology was discussed throughout the guideline development group and the benefits and downsides of the completely different terms used in the literature have been weighed. Several papers have discussed nomenclature, but the terminology used depended on the preference of the writer. This strategy is well argued by Cooper and colleagues and this terminology was adopted by an American consensus meeting (Nelson, 2009; Cooper, et al. It was felt that in Europe the terms "primary" and "secondary" have been extensively used to classify amenorrhea in relation to menarche, and thus "primary ovarian insufficiency" would result in confusion, because it was not synonymous with primary amenorrhoea. This was a minority view of the rule of thumb development group however a clear majority of workshop participants wished to use the terminology "premature ovarian insufficiency". Recommendation the time period "premature ovarian insufficiency" ought to be used to describe this condition in research and clinical follow. It can manifest as primary amenorrhea with onset earlier than menarche or secondary amenorrhea. An instance of the noticed distribution of menopausal ages in a European inhabitants is shown in determine 1. The prevalence of pure menopause earlier than the age of 40 is approximately 1% (Krailo and Pike, 1983; Coulam, et al. Coulam and colleagues established that the rate of pure menopause is ten times larger in the 40 to 44 age group, conventionally this is referred to as "early menopause", as comparability with} the 30 to 39 age group (Coulam, et al. Low ovarian reserve is a condition by which the ovary loses its normal reproductive potential. Women with low ovarian reserve usually reply poorly to controlled ovarian stimulation leading to retrieval of fewer oocytes, producing poorer high quality embryos and reduced implantation charges and pregnancy charges (Narkwichean, et al. Incidence of poor ovarian response, a measure of low ovarian reserve, over all assisted conception cycles ranges from 9 to 24% (Keay, et al. Low ovarian reserve is characterised as common menses 24 and alterations of ovarian reserve checks, and can be caused by situations affecting the ovaries, however in most cases is a consequence of age. The number of oocytes is highest in prenatal life and declines all through reproductive life, falling to a critically low quantity around the age of 50 in most women (see also determine 1. The primordial follicle inhabitants at birth is 701 000 (A), and at menopause is a thousand at 50. Conclusion Premature ovarian insufficiency is a clinical syndrome outlined by loss of ovarian exercise earlier than the age of 40. In this guideline, cessation of ovarian operate in women aged between 40 and forty five will be termed early menopause. This determine was derived from long-term follow-up of a birth cohort of 1858 women in Rochester, Minnesota. The prevalence of early menopause (in the 40 to 44 age group) is ten times larger (Coulam, et al. Lifestyle: smoking is well recognised as a danger issue for earlier onset of menopause (Baron, 1984; van Noord, et al. Socio-economic factors: Later menopause has been shown to be related to larger socio-economic standing (van Noord, et al. Iatrogenic menopause Historically, bilateral oophorectomy has been practised on the time of hysterectomy for benign gynaecological disease. Modifiable factors may include: gynaecological surgical follow lifestyle smoking modified remedy regimens for malignant and persistent diseases. Determinants of age at pure menopause in the Isparta Menopause and Health Study: premenopausal physique mass index acquire fee and episodic weight loss. Ovarian failure in systemic lupus erythematosus patients handled with pulsed intravenous cyclophosphamide. Childhood cognitive ability and age at menopause: evidence from two cohort research. Premature menopause in a multi-ethnic inhabitants study of the menopause transition. Body mass index, train, and different lifestyle factors in relation to age at pure menopause: analyses from the breakthrough generations study. Efficacy of dehydroepiandrosterone to improve ovarian response in women with diminished ovarian reserve: a meta-analysis. Lack of affiliation between age at menarche and age at menopause: Pro-Saude Study, Rio de Janeiro, Brazil. Meta-analysis means that smoking is related to an elevated danger of early pure menopause. Age at pure menopause in a population-based screening cohort: the function of menarche, fecundity, and lifestyle factors. Ovarian reserve and reproductive age determined from measurement of ovarian quantity by transvaginal sonography. Impact of Premature Ovarian Failure on Mortality and Morbidity amongst Chinese Women. Hot flushes and night sweats are characteristic of estrogen deficiency (Conway, 2000). Vaginal symptoms, dyspareunia and dryness, very distressing for the affected person (Davis and Jane, 2011). Other symptoms include sleep disturbance, mood modifications, poor concentration, stiffness, dry eyes (Smith, et al. Women presenting with amenorrhea should be instantly questioned about symptoms, as they may not volunteer these, or certainly remember that their symptoms are related to menstrual disturbance. In distinction, women experiencing surgical menopause usually have severe and persistent symptoms. Young women with primary amenorrhea hardly ever expertise symptoms at presentation, implying that these symptoms are because of of} estrogen withdrawal rather than estrogen deficiency. In untreated women, symptoms usually resolve steadily but the time course is variable and unpredictable. Women may expertise sudden severe symptoms upon cessation of the contraceptive capsule. Anti-Mullerian hormone, inhibin B, and antral follicle count in young women with ovarian failure. Primary ovarian insufficiency: a extra correct time period for premature ovarian failure. In the absence of high quality|of prime of the range|of prime quality} evidence, the rule of thumb development group involves the following recommendations: Recommendations the analysis Premature Ovarian Insufficiency is predicated on the presence of menstrual disturbance and biochemical affirmation. The incidence of an abnormal karyotype is larger in women with primary amenorrhea (21%) than in these presenting with secondary amenorrhea (11%) (Jiao, et al. Recommendations Chromosomal analysis should be carried out in all women with noniatrogenic Premature Ovarian Insufficiency. C Gonadectomy should be recommended for all women with detectable Y chromosomal materials. This requires careful counselling earlier than the test is carried out, including permission from the affected person to perform the test. The penetrance of tremor and ataxia amongst adult premutation carriers elevated with age, exceeding 50% for males aged 70-90 years. Females are also affected however severity and penetrance are less (Jacquemont, et al. B the implications of the fragile-X premutation should be discussed earlier than the test is carried out. For a few of these genes, mutations are identified, while others are listed as candidate genes with a necessity for further investigation. Conclusion and considerations Many genes have been implicated as causative factors in premature ovarian insufficiency. A latest study has shown that coeliac disease and inflammatory bowel disease are significantly extra prevalent (6/224 (2. In the absence of these autoantibodies, no infiltration of ovaries by immune cells has been documented. However, these research are case stories lacking details on the validation and diagnostic accuracy of the antibody assay type used.
Trusted 5mg linagliptin
A Intravitreal injections of antivascular endothelial development factor are indicated for central-involved diabetic macular edema, which happens beneath the foveal middle and will threaten studying imaginative and prescient. A Screening Type 2 Diabetes Diabetic retinopathy is a extremely specific vascular complication of both type 1 and type 2 diabetes, with prevalence strongly associated to both the period of diabetes and the level of glycemic control. In addition to diabetes period, factors that improve the risk of, or are related to, retinopathy include persistent hyperglycemia (49), nephropathy (50), hypertension (51), and dyslipidemia (52). Intensive diabetes administration with the goal of reaching near-normoglycemia has been shown in large potential randomized studies to prevent and/or delay the onset and development of diabetic retinopathy and probably enhance patient-reported visible operate (14,5355). Several case series and a controlled potential research recommend that being pregnant in sufferers with type 1 diabetes could worsen retinopathy and threaten imaginative and prescient, especially when glycemic control is poor on the time of conception (57,58). Exams every 2 years could also be} cost-effective after quantity of} regular eye exams, and in a inhabitants with well-controlled type 2 diabetes, there was basically no risk of improvement of great retinopathy with a 3-year interval after a traditional examination (59). Retinal photography can also improve efficiency and scale back prices when the expertise of ophthalmologists can be utilized for more complex examinations and for therapy (62). Type 1 Diabetes Patients with type 2 diabetes who could have had years of undiagnosed diabetes and have a big risk of prevalent diabetic retinopathy on the time of prognosis should have an initial dilated and complete eye examination on the time of prognosis. [newline]Pregnancy Pregnancy is related to a fast development of diabetic retinopathy (64,65). In addition, fast implementation of intensive glycemic administration in the setting of retinopathy is related to early worsening of retinopathy (58). Treatment Two of the main motivations for screening for diabetic retinopathy are to prevent lack of imaginative and prescient and to intervene with treatment when imaginative and prescient loss may be prevented or reversed. Photocoagulation Surgery Because retinopathy is estimated to take a minimum of|no much less than} 5 years to develop after the onset of hyperglycemia, sufferers with type 1 diabetes should have an initial dilated and complete eye examination inside 5 years after the prognosis of diabetes (63). In both trials, laser photocoagulation surgery was useful in decreasing the risk of further visible loss in affected sufferers but generally not useful in reversing already diminished acuity. The commonest early signs are induced by the involvement of small fibers and include pain and dysesthesias (unpleasant sensations of burning and tingling). Large-fiber operate: vibration perception, 10-g monofilament, and ankle reflexes three. Diabetic Autonomic Neuropathy the diabetic neuropathies are a heterogeneous group of issues with various scientific manifestations. Screening c c All sufferers must be assessed for diabetic peripheral neuropathy starting at prognosis of type 2 diabetes and 5 years after the prognosis of type 1 diabetes and a minimum of|no much less than} yearly thereafter. B Assessment for distal symmetric polyneuropathy should include a cautious historical past and assessment of both temperature or pinprick sensation (small-fiber function) and vibration sensation using a 128-Hz tuning fork (for large-fiber function). B the signs and signs of autonomic neuropathy must be elicited carefully through the historical past and bodily examination. Gastrointestinal Neuropathies Gastrointestinal neuropathies could contain any portion of the gastrointestinal tract with manifestations together with esophageal dysmotility, gastroparesis, constipation, diarrhea, and fecal incontinence. Exclusion of organic causes of gastric outlet obstruction or peptic ulcer disease (with esophagogastroduodenoscopy or a barium research of the stomach) is required before contemplating a prognosis of or specialized testing for gastroparesis. Neuropathic Pain Diabetic autonomic neuropathy can also trigger genitourinary disturbances, together with sexual dysfunction and bladder dysfunction. In males, diabetic autonomic neuropathy could trigger erectile dysfunction and/or retrograde ejaculation (76). Female sexual dysfunction happens more frequently in those with diabetes and presents as decreased sexual want, increased pain throughout intercourse, decreased sexual arousal, and inadequate lubrication (80). Neuropathic pain may be extreme and may influence high quality of life, limit mobility, and contribute to depression and social dysfunction (87). No compelling proof exists in assist of glycemic control or way of life administration as therapies for neuropathic pain in diabetes or prediabetes, which leaves only pharmaceutical interventions. Given the vary of partially efficient treatment options, a tailor-made and stepwise pharmacologic strategy with cautious attention to relative symptom enchancment, treatment adherence, and medicine unwanted side effects} is really helpful to obtain pain reduction and enhance high quality of life (8991). The majority of studies testing pregabalin have reported favorable effects on the proportion of participants with a minimum of|no much less than} 30 50% enchancment in pain (88,ninety,9295). Adverse effects could also be} more extreme in older sufferers (98) and could also be} attenuated by decrease starting doses and more gradual titration. In longer-term studies, a small improve in A1C was reported in people with diabetes handled with duloxetine compared with placebo (100). A recent systematic review and meta-analysis by the Special Interest Group on Neuropathic Pain of the International Association for the Study of Pain found the proof supporting the effectiveness of tapentadol in decreasing neuropathic pain to be inconclusive (88). Withdrawing medicine with opposed effects on gastrointestinal motility together with opioids, anticholinergics, tricyclic antidepressants, glucagon-like peptide 1 receptor agonists, pramlintide, and possibly dipeptidyl peptidase 4 inhibitors, can also enhance intestinal motility (103,104). It must be reserved for extreme instances which might be} unresponsive to other therapies (104). Erectile Dysfunction c c c c Treatments for erectile dysfunction could include phosphodiesterase type 5 inhibitors, intracorporeal or intraurethral prostaglandins, vacuum gadgets, or penile prostheses. C Obtain a prior historical past of ulceration, amputation, Charcot foot, angioplasty or vascular surgery, cigarette smoking, retinopathy, and renal disease and assess current signs of neuropathy (pain, burning, numbness) and vascular disease (leg fatigue, claudication). B the examination should include inspection of the skin, assessment of foot deformities, neurological assessment (10-g monofilament testing with a minimum of|no much less than} one other assessment: pinprick, temperature, vibration, or ankle reflexes), and vascular assessment together with pulses in the legs and feet. B the use specialized therapeutic footwear is really helpful for high-risk sufferers with diabetes together with those with extreme neuropathy, foot deformities, or historical past of amputation. B and treatment of sufferers with diabetes and feet in danger for ulcers and amputations can delay or prevent opposed outcomes. Early recognition All adults with diabetes should endure a complete foot analysis a minimum of|no much less than} yearly. Patients with visible difficulties, bodily constraints preventing movement, or cognitive issues that impair their capability to assess the condition of the foot and to institute appropriate responses will want other people, corresponding to members of the family, to assist with their care. Treatment neuroarthropathy is the best way|one of the only ways|the best way} to prevent deformities that improve the risk of ulceration and amputation. However, sufferers must be supplied enough data to aid in selection of appropriate footwear. Use of custom therapeutic footwear might help scale back the risk of future foot ulcers in high-risk sufferers (106,108). Empiric antibiotic therapy may be narrowly focused at gram-positive cocci in lots of} sufferers with acute infections, but those in danger for an infection with antibiotic-resistant organisms or with persistent, beforehand handled, or extreme infections require broader-spectrum regimens and must be referred to specialized care facilities (109). Foot ulcers and wound care could require care by a podiatrist, orthopedic or vascular surgeon, or rehabilitation specialist skilled in the administration of individuals with diabetes (109). Angiotensinreceptor blockade versus converting-enzyme inhibition in type 2 diabetes and nephropathy. Cardiovascular outcomes in the Irbesartan Diabetic Nephropathy Trial of sufferers with type 2 diabetes and overt nephropathy. The impact of intensive treatment of diabetes on the development and development of long-erm problems in insulin-dependent diabetes mellitus. The sensitivity and specificity of nonmydriatic digital stereoscopic retinal imaging in detecting diabetic retinopathy. Canadian Ophthalmological Society evidence-based scientific practice tips for the administration of diabetic retinopathy. Photocoagulation for diabetic macular edema: Early Treatment Diabetic Retinopathy Study report number one. Randomized trial evaluating ranibizumab plus immediate or deferred laser or triamcinolone plus immediate laser for S98 Microvascular Complications and Foot Care Diabetes Care Volume forty, Supplement 1, January 2017 diabetic macular edema. Expanded 2-year follow-up of ranibizumab plus immediate or deferred laser or triamcinolone plus immediate laser for diabetic macular edema. Neuropathy and associated findings in the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications research. Evidencebased guideline: treatment of painful diabetic neuropathy: report of the American Academy of Neurology, the American Association of Neuromuscular and Electrodiagnostic Medicine, and the American Academy of Physical Medicine and Rehabilitation. The administration of diabetic foot: a scientific practice guideline by the Society for Vascular Surgery in collaboration with the American Podiatric Medical Association and the Society for Vascular Medicine. Type 2 diabetes-related foot care information and foot self-care practice interventions in the United States: a systematic review of the literature. Clin Infect Dis 2012;fifty four:e132e173 Diabetes Care Volume forty, Supplement 1, January 2017 S99 11. C Screening for geriatric syndromes could also be} appropriate in older adults experiencing limitations of their primary and instrumental activities of every day dwelling, as they could result on} diabetes self-management and be associated to health-related high quality of life. C Annual screening for early detection of mild cognitive impairment or dementia is indicated for adults 65 years of age or older.
Trusted 5 mg linagliptin
In these illnesses, the magnitude of proteinuria is often 1,000 mg/g (except in early diabetic kidney disease), and may approach nephrotic vary (spot urine protein-to-creatinine ratio three,000 mg/g). On the other hand, proteinuria is often delicate or absent in vascular illnesses, tubulointerstitial illnesses, and cystic illnesses within the native kidney and in rejection and drug toxicity outcome of} cyclosporine or tacrolimus within the transplant. It is well-known that nephrotic vary proteinuria is related to a large vary of problems, including hypoalbuminemia, edema, hyperlipidemia, and hypercoagulable state; quicker development of kidney illness; and untimely cardiovascular disease. Furthermore, the reduction in proteinuria is correlated with a subsequent slower lack of kidney operate. The factor about} antihypertensive therapy, especially with angiotensin-converting enzyme inhibitors, to sluggish the development of kidney illness is bigger in patients with larger ranges of proteinuria compared to with} patients with decrease ranges of proteinuria. Treatments to sluggish the development of continual kidney illness in adults in are proven in Table 146. However, few patients with continual kidney illness have been included in population-based epidemiologic research of cardiovascular disease or long-term randomized clinical trials. Approach 261 cardiovascular disease threat factors and threat factor reduction methods which might be} probably secure and efficient for patients with continual kidney illness is proven in Table 147. Consultation with a nephrologist may be be} essential to establish the prognosis and therapy of kind of|the sort of} kidney illness. Consultation and/or co-management with a kidney illness care team is advisable during Stage three, and referral to a nephrologist in Stage four is beneficial. A multidisciplinary team approach may be be} essential to implement and coordinate care. This classification could then be remodeled to an ``evidence mannequin' for future development of additional apply pointers regarding specific diagnostic evaluations and therapeutic interventions (Executive Summary). The Work Group sought to develop an ``evidence base' for the classification and clinical action plan, derived from a systematic abstract of the obtainable scientific literature on: the analysis of laboratory measurements for the clinical assessment of kidney illness; association of the extent of kidney operate with problems of continual kidney illness; and stratification of the chance for lack of kidney operate and development of cardiovascular disease. Two products have been developed from this course of: a set of clinical apply pointers regarding the classification and action plan, which are contained in this report; and an evidence report, which consists of the abstract of the literature. The Work Group consisted of ``domain consultants,' including people with experience in nephrology, epidemiology, laboratory medicine, nutrition, social work, pathology, gerontology, and family medicine. In addition, the Work Group had liaison members from the National Institute of Diabetes, Digestive and Kidney Diseases and from the National Institute on Aging. The first task of the Work Group members was to define the general subject and targets, including specifying the target situation, target inhabitants, and audience. They then additional developed and refined every subject, literature search technique, and information extraction kind (described below). The Work Group members have been the principal reviewers of the literature, and from these detailed reviews they summarized the obtainable evidence and took the first roles of writing the guidelines and rationale statements. The Evidence Review Team consisted of nephrologists (one senior nephrologist and three nephrology fellows) and methodologists from New England Medical Center with experience in systematic evaluate of the medical literature. They have been responsible for coordinating the project, including coordinating meetings, refinement of targets and matters, creation of the format of the evidence report, development of literature search methods, initial evaluate and assessment of literature, and coordination of all companions. The Evidence Review Team additionally coordinated the methodological and analytic strategy of the report, coordinated the meetings, and defined and standardized the methodology of performing literature searches, of information extraction, and of summarizing the evidence within the report. They performed literature searches, retrieved and screened abstracts and articles, created varieties to extract relevant information from articles, and tabulated outcomes. Throughout the project, and particularly at meetings, the Evidence Review Team led discussions on systematic evaluate, literature searches, information extraction, assessment of high quality of articles, and abstract reporting. Based on their experience, members of the Work Group focused on the particular questions listed in Table 8 and employed a selective evaluate of evidence: a abstract of reviews for established ideas (review of textbooks, reviews, pointers, and chosen authentic articles familiar to them as domain experts) and a evaluate of primary articles and information model spanking new|for brand new} ideas. The development course of included creation of initial mock-ups by the Work Group Chair and Evidence Review Team followed by iterative refinement by the Work Group members. The refinement course of started prior to literature retrieval and continued through the beginning of reviewing individual articles. The refinement occurred by e-mail, phone, and in-person communication regularly with local consultants and with all consultants during in-person meetings of the Evidence Review Team and Work Group members. Data extraction varieties have been designed to capture info on numerous features of the first articles. Forms for all matters included examine setting and demographics, eligibility standards, causes of kidney illness, numbers of topics, examine design, examine funding source, inhabitants category (see below), examine high quality (based on standards appropriate for every examine design, see below), appropriate selection and definition of measures, outcomes, and sections for comments and assessment of biases. The numerous steps concerned in development of the guideline statements, rationale statements, tables, and information extraction varieties have been piloted on one of the matters (bone disease) with a Work Group member at New England Medical Center. The ``in-person' pilot experience allowed extra efficient development and refinement of subsequent varieties with Work Group members situated at different establishments. It additionally supplied experience within the steps essential for coaching junior members of the Evidence Review Team to develop varieties and to effectively extract relevant info from primary articles. Training of the Work Group members to extract information from primary articles subsequently occurred by e-mail nicely as|in addition to} at meetings. Classification of Stages Defining the phases of severity was an iterative course of, primarily based on experience of the Work Group members and synthesis of evidence developed during the systematic evaluate. The perfect examine design to assess prevalence could be a crosssectional examine of inhabitants consultant of the overall inhabitants. Criteria for analysis of cross-sectional research to assess prevalence are listed in Table 150. Data from baseline assessments of patients enrolled within the Canadian Multicentre cohort examine of patients with continual kidney illness have been used for Figures 28, 29, 36, 37, 38, forty, and forty two. Studies that supplied information for numerous ranges of kidney operate have been preferred; how- 270 Part 10. Members of the Work Group supplied individual affected person information that have been used for some analyses. Stratification of Risk (Prognosis) the appropriate examine to assess the relationship of threat factors to lack of kidney operate and development of cardiovascular disease could be a longitudinal examine of a consultant sample of patients with continual kidney illness with potential assessment of factors at baseline and outcomes during follow-up. Because could be} tough to determine the onset of continual kidney illness and cardiovascular disease, potential cohort research have been preferred to case-control research or retrospective research. Clinical trials have been included, with the understanding that the choice standards for the clinical trial may have result in a non-representative cohort. Appendices 271 recognized association between diabetes and cardiovascular disease, diabetic and nondiabetic patients have been thought-about separately. The association between diabetic kidney illness and different diabetic problems was evaluated utilizing reviews of cross-sectional research and chosen primary articles of cohort research. Studies for the literature evaluate have been identified primarily through Medline searches of English language literature carried out between February and June 2000. These searches have been supplemented by relevant articles recognized to the domain consultants and reviewers. The Medline literature searches have been carried out to determine clinical research printed from 1966 through the search dates. Development of the search methods was an iterative course of that included input from all members of the Work Group. Search methods have been designed to yield roughly 1,000 to 2,000 titles every. The searches have been limited to research on humans and printed in English and focused on both adults or kids, as relevant. In common, research that focused on hemodialysis or peritoneal dialysis have been excluded. Potential papers for retrieval have been identified from printed abstracts and titles, primarily based on examine inhabitants, relevance to subject, and article sort. After retrieval, every paper was screened to confirm relevance and appropriateness for evaluate, primarily based totally on examine design and ascertainment of essential variables. Overall, 18,153 abstracts have been screened, 1,a hundred and ten articles have been reviewed, and outcomes have been extracted from 367 articles. Detailed tables contain information from every area of the parts of the info extraction varieties. Summary tables describe the energy of evidence according to 4 dimensions: examine measurement, applicability depending on kind of|the sort of} examine topics, outcomes, and methodological high quality (see table on the following web page, Example of Format for Evidence Tables). Study Size the examine (sample) measurement is used as a measure of the weight of the evidence. In common, giant research present extra exact estimates of prevalence and associations. A examine that enrolled chosen patients may be be} less generalizable than smaller research that included a broad spectrum of affected person populations. Applicability Applicability (also generalizability or external validity) addresses the difficulty of whether the examine inhabitants is sufficiently broad so that the outcomes can be generalized to the inhabitants of curiosity at giant. The examine inhabitants is often defined by the inclusion and exclusion standards.
5mg linagliptin
Participants randomly assigned to the intensive way of life group achieved equal threat factor management however required fewer glucose-, blood pressure, and lipid-lowering medications than those randomly assigned to standard care. When provided by educated practitioners in medical care settings with close medical monitoring, short-term (3-month) interventions that use very-low-calorie diets (defined as #800 kcal/day) and complete meal replacements could obtain greater short-term weight reduction (1015%) than intensive behavioral way of life interventions that sometimes obtain 5% weight reduction. Phentermine is indicated as short-term (a few weeks) adjunct at the side of} way of life and behavioral weight reduction interventions (29). In scientific trials in overweight sufferers with diabetes, hypoglycemia and abdominal distension had been also noticed. Data of frequent adverse results for Contrave had been derived from 5 double-blind, placebo-controlled scientific trials in mixed-type research populations. Obesity Management for the Treatment of Type 2 Diabetes 14 National Average Drug Acquisition Cost knowledge available at: knowledge. S69 S70 Obesity Management for the Treatment of Type 2 Diabetes Diabetes Care Volume 41, Supplement 1, January 2018 c c and nutritional standing have to be provided to sufferers after surgery, based on pointers for postoperative administration of metabolic surgery by nationwide and worldwide professional societies. Although metabolic surgery has been proven to improve the metabolic profiles of morbidly overweight sufferers with kind 1 diabetes, establishing the role of metabolic surgery in such sufferers would require bigger and longer studies (72). Retrospective analyses and modeling studies suggest that metabolic surgery cost-effective and even cost-saving for sufferers with kind 2 diabetes, but the outcomes are largely dependent on assumptions in regards to the long-term effectiveness and security of the procedures (73,74). Longer-term issues embody dumping syndrome (nausea, colic, diarrhea), vitamin and mineral deficiencies, anemia, osteoporosis, and, not often (75), extreme hypoglycemia from insulin hypersecretion. Lifestyle, diabetes, and cardiovascular threat factors 10 years after bariatric surgery. Clinical outcomes of metabolic surgery: microvascular and macrovascular problems. Ann Surg 2010;251:399405 S72 Obesity Management for the Treatment of Type 2 Diabetes Diabetes Care Volume 41, Supplement 1, January 2018 forty eight. Identifying limitations to acceptable use of metabolic/bariatric surgery for kind 2 diabetes therapy: coverage lab outcomes. A Most people with kind 1 diabetes should use rapid-acting insulin analogs to reduce hypoglycemia threat. Generally, the beginning insulin dose relies on weight, with doses starting from zero. The research was carried out with short-acting and intermediateacting human insulins. These analogs are associated with less hypoglycemia, less weight acquire, and lower A1C than human insulins in individuals with kind 1 diabetes (1618). Longer-acting basal analogs (U-300 glargine or degludec) may additionally convey a lower hypoglycemia threat compared with U-100 glargine in sufferers with kind 1 diabetes (19,20). Postprandial glucose excursions higher controlled by adjusting the timing of prandial (bolus) insulin dose administration. Investigational Agents Metformin Adding metformin to insulin therapy could reduce insulin necessities and improve metabolic management in sufferers with kind 1 diabetes. E In sufferers with kind 2 diabetes and established atherosclerotic heart problems, antihyperglycemic c c c therapy should start with way of life administration and metformin and subsequently incorporate an agent confirmed to reduce major adverse cardiovascular events and cardiovascular mortality (currently empagliflozin and liraglutide), after considering drug-specific and patient factors (Table eight. C* Continuous reevaluation of the medicine routine and adjustment as needed to incorporate patient factors (Table eight. Compared with sulfonylureas, metformin as first-line therapy has beneficial results on A1C, weight, and cardiovascular mortality (33). Combination Therapy Metformin monotherapy ought to be started at analysis of kind 2 diabetes except there are contraindications. A comparative effectiveness meta-analysis (36) suggests that every new class of noninsulin brokers added to preliminary therapy typically lowers A1C roughly zero. Cost-effectiveness models of the newer brokers primarily based on scientific utility and glycemic impact have been reported (38). Rapid-acting secretagogues (meglitinides) used as a substitute of sulfonylureas in sufferers with sulfa allergies or irregular meal schedules or in those that develop late postprandial hypoglycemia when taking a sulfonylurea. Comprehensive training regarding self-monitoring of blood glucose, diet, and the avoidance of and acceptable therapy of hypoglycemia are critically essential in any patient using insulin. [newline]Providers should Basal insulin alone is probably the most convenient preliminary insulin routine, beginning at 10 models per day or zero. Longeracting basal analogs (U-300 glargine or degludec) may additionally convey a lower hypoglycemia threat compared with U-100 glargine when used in combination with oral antihyperglycemic brokers (49 55). There have been substantial increases within the worth of insulin over the previous decade and the cost-effectiveness of different antihyperglycemic brokers is an important consideration in a patientcentered approach to care, together with care. Rapidacting analogs are preferred because of of} their prompt onset of motion after dosing. U-300 glargine and U-200 degludec are three and two instances as concentrated as their U-100 formulations and permit larger doses of basal insulin administration per volume used. These concentrated preparations more comfortable for the patient and may improve adherence for sufferers with insulin resistance who require giant doses of insulin. If a patient continues to be above the A1C goal on basal insulin plus single injection of rapid-acting insulin before the biggest meal, advance to a basal-bolus routine with $2 injections of rapid-acting insulin before meals. Optimized mealtime insulin dosing for fat and protein in kind 1 diabetes: software of a model-based approach to derive insulin doses for open-loop diabetes administration. Outpatient insulin therapy in kind 1 and type 2 diabetes mellitus: scientific evaluate. Comparison of scientific outcomes and adverse events associated with glucose-lowering medicine in sufferers with kind 2 diabetes: a meta-analysis. Diabetes medications as monotherapy or metforminbased combination therapy for kind 2 diabetes: a systematic evaluate and meta-analysis. Metformincontaining medicine: drug security communication revised warnings for certain sufferers with decreased kidney operate [Internet], 2016. Expenditures and prices of antihyperglycemic medications within the United States: 2002-2013. Therapeutic issues for antihyperglycemic brokers in diabetic kidney illness. Accessed 22 September 2017 S86 Diabetes Care Volume 41, Supplement 1, January 2018 9. Therefore, cardiovascular threat factors ought to be systematically assessed at least of|no less than} yearly in all sufferers with diabetes. Screening and Diagnosis Recommendations c c c Blood strain ought to be measured at every routine scientific visit. Home blood strain self-monitoring and 24-h ambulatory blood strain monitoring could present evidence of white coat hypertension, masked hypertension, or different discrepancies between office and "true" blood strain (5). Intensification of antihypertensive therapy to goal blood pressures lower than,140/90 mmHg. Meta-analyses of Trials Most sufferers with diabetes and hypertension ought to be handled to a systolic blood strain objective of,one hundred forty mmHg and a diastolic blood strain objective of,ninety mmHg. Taken collectively, these meta-analyses persistently show that treating sufferers with baseline blood strain $140 mmHg to targets,one hundred forty mmHg is beneficial, whereas more intensive targets could provide further, though in all probability less strong, advantages. Treatment Strategies Lifestyle Intervention Recommendation c chubby or overweight; a Dietary Approaches to Stop Hypertension fashion dietary pattern including decreasing sodium and growing potassium consumption; moderation of alcohol consumption; and increased physical exercise. Single-pill antihypertensive mixtures could improve medicine adherence in some sufferers (25). In two subgroup analyses of a single subsequent randomized controlled trial, shifting at least of|no less than} one antihypertensive medicine to bedtime significantly decreased cardiovascular events, however outcomes had been primarily based on a small number of events (36). Antihypertensive medicine known to be efficient and secure in being pregnant embody methyldopa, labetalol, and long-acting nifedipine, whereas hydralzine thought of within the acute administration of hypertension in being pregnant or extreme preeclampsia (46). Recommendations should give attention to} decreasing saturated fat, ldl cholesterol, and trans fat consumption and growing plant stanols/ sterols, n-3 fatty acids, and viscous fiber (such as in oats, legumes, and citrus) consumption. E Obtain a lipid profile at initiation of statins or different lipid-lowering therapy, 412 weeks after initiation or a change in dose, and yearly thereafter as it may help to monitor the response to therapy and inform adherence. The relative benefit of about} lipid-lowering therapy has been uniform throughout most subgroups examined (53,61), including subgroups that various with respect to age and different threat factors. Recently, threat scores and different cardiovascular biomarkers have been developed for threat stratification of secondary prevention sufferers. Very little scientific trial evidence exists for sufferers with kind 2 diabetes beneath the age of 40 years or for sufferers with kind 1 diabetes of any age. Please refer to "Type 1 Diabetes Mellitus and Cardiovascular Disease: A Scientific Statement From the American Heart Association and American Diabetes Association" (69) for additional discussion. A Combination therapy (statin/niacin) has not been proven to present further cardiovascular benefit above statin therapy alone, could improve the chance of stroke with further aspect effects}, and is generally not beneficial. The threat of rhabdomyolysis is more frequent with larger doses of statins and renal insufficiency and appears to be larger when statins are combined with gemfibrozil (compared with fenofibrate) (80).
Quality linagliptin 5 mg
They are also seen in 85% of patients with X-linked Kallmann syndrome (hypogonadotrophic hypogonadism and anosmia). There is a few neurophysiological evidence from patients with X-linked Kallmann syndrome for the existence of an ipsilateral corticospinal pathway, maintaining with} other evidence that the congenital situation is primarily a disorder of axonal steerage throughout development. Concurrent exercise within ipsilateral and contralateral corticospinal pathways may clarify mirroring of movements. Alternatively, a failure of transcallosal inhibition, acquired at the time of myelination of these pathways, may contribute to the genesis of mirror movements. A deficit of sustained attention has also been postulated as the cause of|the cause for} mirror movements. Failure to acknowledge oneself in a mirror may also be a dissociative symptom, a symptom of depersonalization. This may happen spontaneously, apparently more usually in left-handers, or in right-handers attempting to write with the left hand following left-sided brain harm. The author Lewis Carroll sometimes wrote mirror letters but these differ from his regular script, unlike to|not like} the scenario with Leonardo whose two scripts are trustworthy mirror photographs. The system was also utilized by the author Arthur Ransome in his 1939 novel Secret Water. Jane Austen wrote one letter (1817) to a younger niece during which script runs from proper to left but with word order reversed within words. Various neural mechanisms are proposed to clarify mirror writing, together with bilateral cerebral illustration of language, motor programmes, or visible memory traces or engrams. The mechanisms may differ between a true mirror author like Leonardo and somebody performing the task for amusement like Carroll. The ability to learn mirror reversed text as shortly as normally oriented text has been reported in some autistic people. Misidentification Syndromes these are outlined as delusional situations during which patients incorrectly establish and reduplicate people, places, objects, or occasions. Psychiatric, neurological and medical aspects of misidentification syndromes: a evaluation of 260 patients. It happens with proper parietal region harm (hence left-sided limbs most often involved) and should happen in conjunction with of} anosognosia, left hemispatial neglect, and (so called) constructional apraxia. Cross Reference Negativism Mitmachen A motor disorder during which the patient acquiesces to each passive motion of the physique made by the examiner, but as quickly as the examiner releases the physique part, the patient returns it to the resting place. His speech was fluent with out paraphasia though impoverished in content, with recurrent themes repeated nearly verbatim. Confronted with objects of different colours, he was unable to point to them by colour since all appeared purple to him. The options appear to be distinct from erythropsia (persistent) or phantom chromatopsia (normal visible acuity). Monoparesis of the arm or leg of higher motor neurone type is normally cortical in origin, though may unusually come up from a twine lesion (leg more incessantly than arm). Peripheral problems can sometimes present completely with single limb weakness, similar to monomelic motor neurone illness (Hirayama disease), multifocal motor neuropathy with conduction block, and GuillainBarrй syndrome. In medical usage, the meaning overlaps not only with - 227 - M Motor Neglect that of emotional lability but has also been used in the context of pathological laughter. Cross References Emotionalism, Emotional lability; Pathological crying, Pathological laughter; Witzelsucht Motor Neglect Motor neglect is failure to move the contralesional limbs in the neglect syndrome, a more severe impairment than directional hypokinesia. Cross References Directional hypokinesia; Eastchester clapping sign; Neglect Moving Ear A focal dyskinesia characterised by ear motion has been described. Muscle hypertrophy generalized or focal and happens in response to repetitive voluntary contraction (physiological) or repetitive abnormal electrical exercise (pathological. Muscle enlargement may also end result from substitute of myofibrils by other tissues similar to fat or amyloid, a scenario higher described as pseudohypertrophy. Cross References Calf hypertrophy; Masseter hypertrophy; Myotonia Mutism Mutism is absence of speech output. Thought to be dentatothalamocortical tract damage, bilateral oedema in cerebellar peduncles (rather than surgical trauma or infarction); · Bilateral vocal twine paralysis (although higher termed aphonia); · Autism. American Journal of Psychiatry 1986; 143: 14091414 (erratum: American Journal of Psychiatry 1987; 144: 542). Mydriasis Mydriasis is an abnormal dilatation of the pupil, either unilateral or bilateral. If just one pupil seems massive (anisocoria), necessary to|it is very important|you will want to} distinguish mydriasis from contralateral miosis, when a unique differential will apply. Such problems additional characterised based on whether the responsible lesion lies within or outside the spinal twine: intrinsic or intramedullary lesions are always intradural; extrinsic or extramedullary lesions intradural or extradural. A BrownSйquard syndrome more frequent in extrinsic than intrinsic myelopathies. Pathologies generally causing extrinsic myelopathy include · · · · prolapsed disc, osteophyte bar; tumour (primary, secondary); arteriovenous malformation/haematoma; abscess. Sensory: signs of central (funicular) ache may happen; dissociated sensory loss (spinothalamic > dorsal column involvement, or vice versa), suspended sensory loss, and sacral sparing are characteristic of intramedullary lesions; a BrownSйquard syndrome may happen. Pathologies generally causing intrinsic myelopathy include · · · · · quantity of} sclerosis or other inflammatory course of causing transverse myelitis (complete or partial). Drugs useful in the remedy of myoclonus include clonazepam, sodium valproate, primidone, and piracetam. Cross References Asterixis; Chorea, Choreoathetosis; Dystonia; Fasciculation; Hiccups; Jactitation; Myokymia; Palatal tremor; Tic; Tremor Myoedema Myoedema, or muscle mounding, provoked by mechanical stimuli or stretching of muscle, is a function of rippling muscle illness, during which the muscle contractions are associated with electrical silence. Myokymia Myokymia is an involuntary, spontaneous, wave-like, undulating, flickering motion within a muscle (cf. Neurophysiologically this corresponds to regular groups of motor unit discharges of peripheral nerve origin. Myokymia is thus related to neuromyotonia and stiffness, since there concurrent impairment of muscle leisure and a grievance of muscle cramps. Neurophysiological evidence of myokymia helpful in the evaluation of a brachial plexopathy, since that is found in radiation-induced, but not neoplastic, lesions. Cross References Fasciculation; Myotonia; Neuromyotonia; Stiffness Myopathy the term myopathy means a primary disorder of muscle causing wasting and/or weakness in the absence of sensory abnormalities. Clinically, myopathic processes must be differentiated from neuropathies, notably anterior horn cell diseases and motor neuropathies, and neuromuscular junction problems. Treatment is with antibiotics, normally a 2-week intravenous course of trimethoprimsulphamethoxazole or ceftriaxone adopted by oral remedy for 1 12 months. Cross References Ataxia; Dementia; Myoclonus; Nystagmus Myotonia Myotonia is a stiffness of muscles with incapability to loosen up after voluntary contraction (action myotonia), or induced by electrical or mechanical. Neurophysiology reveals myotonic discharges, with extended twitch leisure part, which can be provoked by motion, percussion, and electrical stimulation of muscle; discharges sometimes wax and wane. Myotonia aggravated by hyperkalaemia, depolarizing neuromuscular blocking medicine. Other factors that may induce myotonia include hypothermia, mechanical or electrical stimulation (including surgical incision and electrocautery), shivering, and use of inhalational anaesthetics. Mutations in genes encoding voltage-gated ion channels have been identified in some of the the} inherited myotonias, therefore these are channelopathies: skeletal muscle voltage-gated Na+ channel mutations have been found in K+ -aggravated myotonia, and also paramyotonia congenita and hyperkalaemic periodic paralysis. Movement of a limb in response to software of strain despite the patient having been advised to resist (mitgehen) is one factor of negativism. The similarity of some of these options to gegenhalten suggests the possibility of|the potential of|the potential for} frontal lobe dysfunction as the underlying cause. Cross References Catatonia; Gegenhalten Neglect Neglect is a failure to orient in the direction of|in course of}, respond to, or report novel or meaningful stimuli. [newline]If failure to reply may be attributed to concurrent sensory or motor deficits. This dichotomy may also be characterised as egocentric (neglecting hemispace outlined by the midplane of the body) and allocentric (neglecting one side of particular person stimuli). Neglect of contralateral hemispace may also be known as unilateral spatial neglect, hemi-inattention, or hemineglect. Lesser levels of neglect manifest as extinction (double simultaneous stimulation). Motor neglect evident as hemiakinesia, hypokinesia, or motor impersistence. Neglect is more frequent after proper rather than left brain damage, normally of vascular origin. The angular gyrus and parahippocampal gyrus central to the development of visible neglect. Hence, type of literal or phonemic paraphasia encountered in aphasic syndromes, most normally these ensuing from left superior temporal lobe damage (Wernicke type).
Best 5mg linagliptin
Know the disturbance in pattern and significance of serum urine, and salivary concentrations in Cushing syndrome o. Know diagnostic tools available to detect pituitary tumors in Cushing syndrome and the indications p. Know indications and contraindications for elimination of pituitary microadenomata in Cushing syndrome r. Know indications for pituitary radiation therapy, both alone or together with different therapeutic modalities s. Understand methods of decreasing or discontinuing hydrocortisone therapy after surgical treatment of Cushing syndrome u. Know that 3-beta-hydroxysteroid dehydrogenase exercise is generally decreased in infancy 2. Know that prematurity is related to higher ranges of Delta 5 steroid hormones than noticed in full-term infants 3. Know the maturational pattern of synthesis and secretion of the adrenal gland (androgens) within the fetus, infant, prepubertal and pubertal child b. Understand the importance of aromatase in intercourse hormone metabolism within the fetus and older people c. Understand that the adrenal androgens are largely bound to albumin and to a small extent to intercourse hormone- binding globulin 2. Understand the relative abundance of various androgens and their biologic sources. Understand that adrenal androgens exert their effect via peripheral conversion to stronger androgens 2. Understand the position of the adrenal androgens at adrenarche within the growth of pubic and axillary hair 2. Know that adrenal androgen deficiency or resistance might contribute to paucity of pubic and axillary hair b. Know that androgen substitute can be used to deal with adrenal androgen deficiency b. Know that elevated adrenal adrogens can suppress pitutiary secretion of gonadotropins 2. Know the clinical options, differential analysis, and laboratory analysis of premature adrenarche c. Understand the long-term outcome of traditional and nonclassic congenital adrenal hyperplasia phrases of|when it comes to|by method of} progress and reproductive operate. Know the long-term outcome of premature adrenarche in that it might be related to later ovarian hyperandrogenism and/or insulin resistance f. Know that androgen excess could also be} present in ladies with insulin resistance syndrome b. Understand the therapeutic choices for androgen excess of adrenal and ovarian derivation C. Know that the adrenal cortex synthesizes and secretes minimal quantities of estrone and estradiol 2. Know nearly all} adrenal estrogens are derived indirectly from peripheral conversion of adrenal androgens 3. Know the clinical and laboratory findings in sufferers with feminizing adrenal tumors b. Know the pathways by which cholesterol is transformed to aldosterone; understand how that is different from cortisol synthesis 2. Know the enzymes and the genes encoding these enzymes essential for the synthesis of aldosterone from cholesterol c. Understand the components that regulate aldosterone secretion, including the reninangiotensin system 2. Know that vasopressin has a transient stimulatory effect on aldosterone secretion d. Understand that aldosterone circulates in both a non-protein bound form or bound to cortisol-binding globulin or albumin. Know that the renin-angiotensin aldosterone system regulates sodium and potassium homeostasis four. Understand the position of 11-beta-hydroxysteroid dehydrogenase in controlling corticosteroid motion on aldosterone-responsive tissues 5. Understand that aldosterone passively crosses cell membranes to bind with receptors 6. Understand that aldosterone promotes lively sodium reabsorption and potassium excretion in its main goal tissues 2. Know the various causes of salt-losing syndromes and differentiate among them d. Know that salt losing crisis could also be} because of of} aldosterone resistance (mineralocorticoid receptor defect) rather than aldosterone deficiency. Know the molecular foundation of pseudohypoaldosteronism and associated salt shedding syndromes 2. Know differentiate mineralocorticoid deficiency from mineralocorticoid unresponsiveness b. Understand the clinical displays of pseudohypoaldosteronism and the variability in aldosterone resistance of various goal tissues c. Know that secondary aldosteronism results from angiotensin stimulation of the zona glomerulosa b. Understand the pathophysiology of hypertension because of of} excess mineralocorticoid secretion or motion 2. Know that renin production is characteristically suppressed in hyperaldosteronism b. Know the clinical presentation of sufferers with excess mineralocorticoid secretion or motion f. Understand the medical treatment of hyperaldosteronism because of of} bilateral adrenal hyperplasia g. Know the treatment of dexamethasone suppressible (glucocorticoid remediable) hyperaldosteronism h. Know the prognosis of hyperaldosteronism because of of} unilateral aldosteronoma, bilateral adrenal hyperplasia, and glucocorticoid remediable aldosteronism c. Know that licorice ingestion can cause hypertension by inhibiting 11beta-hydroxysteroid dehydrogenase enzymatic exercise 2. Understand that familial early onset, severe hypertension deserves a thorough evaluation for endocrine problems E. Know that glucocorticoids are necessary for the event and function of the adrenal medulla b. Understand the measurement of circulating catecholamines and their urinary metabolites 3. Know the different types of the adrenergic receptor system and their mechanism of operate 3. Understand that physiologic catecholamine results are fast in onset and shortly terminated 5. Understand the interrelationship between catecholamines and different hormones similar to insulin, glucagon, renin, parathyroid, calcitonin, thyroxine, cortisol, and aldosterone 2. Know the syndromes and genetic problems underlying extreme production of catecholamines and catecholamine metabolites 2. Know the clinical presentation of problems related to extreme production of catecholamines b. Know the result result} of treatment of lesions related to extreme production of catecholamines c. Know the treatment of problems related to extreme production of catecholamines d. Know the diagnostic evaluation of problems related to extreme production of catecholamines c. Know maturational patterns of particular person hypothalamic/pituitary-target gland axes within the fetus b. Know the final construction of pituitary and hypothalamic hormones including which are brief peptides, which are proteins, and which are glycoproteins c. Understand the processing involved in transport to , storage of, and secretion of pituitary hormones from secretory vesicles 3. Understand the clinical and physiologic importance of pulsatile secretion of pituitary hormones c.
Order 5 mg linagliptin
Technology-assisted weight reduction interventions in primary care: a scientific evaluate. Translating the Diabetes Prevention Program life-style intervention for weight reduction into primary care: a randomized trial. Combined diet and physical exercise promotion applications to stop sort 2 diabetes amongst individuals at increased danger: a scientific evaluate for the Community Preventive Services Task. Long-term security, tolerability, and weight reduction related to metformin within the Diabetes Prevention Program Outcomes Study. Pre-diabetes and the danger for heart problems: a scientific evaluate of the evidence. J Public Health Manag Pract 2011;17:242247 S48 Diabetes Care Volume forty, Supplement 1, January 2017 6. To be helpful, the data must be integrated into medical and selfmanagement plans. For many sufferers, it will require testing 610 (or more) times every day, though particular person wants might differ. These units might offer the chance to scale back hypoglycemia for those with a history of nocturnal hypoglycemia. The security of hybrid closed-loop methods has been supported within the literature (26). E Point-of-care testing for A1C offers the chance for more well timed treatment adjustments. E S50 Glycemic Targets Diabetes Care Volume forty, Supplement 1, January 2017 A1C reflects average glycemia over roughly 3 months and has strong predictive value for diabetes problems (29,30). Thus, A1C testing should be carried out routinely in all sufferers with diabetesdat preliminary evaluation and as part of of} persevering with care. [newline]Other studies have also demonstrated higher A1C ranges in African Amercans than in whites (33). Whether there are clinically meaningful differences in how A1C pertains to average glucose in youngsters or in several ethnicities is an space for further examine (35,36). For the time being, the question has not led to completely different suggestions about testing A1C or to completely different interpretations of the medical which means of given ranges of A1C in those populations. Until further evidence is A reasonable A1C aim so much of} nonpregnant adults is,7% (53 mmol/mol). C Less stringent A1C targets (such as,8% [64 mmol/mol]) appropriate for sufferers with a history of extreme hypoglycemia, restricted life expectancy, advanced microvascular or macrovascular problems, in depth comorbid situations, or long-standing diabetes in whom the aim is difficult to achieve despite diabetes self-management schooling, appropriate glucose monitoring, and effective doses of a number of} glucose-lowering brokers together with insulin. B A1C and Microvascular Complications Hyperglycemia defines diabetes, and glycemic control is fundamental to diabetes management. Given the substantially increased danger of hypoglycemia in sort 1 diabetes trials and with polypharmacy in sort 2 diabetes, the dangers of decrease glycemic targets outweigh the potential advantages on microvascular problems. There is evidence for a cardiovascular benefit of about} intensive glycemic control after long-term follow-up of cohorts treated early in the course of of|in the midst of} sort 1 and type 2 diabetes. The benefit of about} intensive glycemic control on this cohort with sort 1 diabetes has been proven to persist for a number of} decades (49) and to be related to a modest reduction in all-cause mortality (50). Heterogeneity of mortality effects throughout studies was noted, which may reflect differences in glycemic targets, therapeutic approaches, and population characteristics (54). Those sufferers with long length of diabetes, a recognized history of hypoglycemia, advanced atherosclerosis, or advanced age/frailty might benefit from much less aggressive targets (56,57). When potential, such choices should be made with the affected person, reflecting his or her preferences, wants, and values. However, end result studies have clearly proven A1C to be the primary predictor of problems, and landmark trials Table 6. C Glucose (1520 g) is the popular treatment for the acutely aware particular person with hypoglycemia (glucose alert value of #70 mg/dL [3. Recommendations from the International Hypoglycaemia Study Group relating to the classification of hypoglycemia are outlined in Table 6. Severe hypoglycemia is outlined as extreme cognitive impairment requiring help from another individual for recovery (62). Severe hypoglycemia acknowledged or unrecognized and might progress to loss of consciousness, seizure, coma, or dying. Clinically important hypoglycemia could cause acute harm to the individual with diabetes or others, particularly if it causes falls, motor vehicle S54 Glycemic Targets Diabetes Care Volume forty, Supplement 1, January 2017 Table 6. A large cohort examine suggested that amongst older adults with sort 2 diabetes, a history of extreme hypoglycemia was related to larger danger of dementia (63). An affiliation between self-reported extreme hypoglycemia and 5-year mortality has also been reported in medical follow (67). Young youngsters with sort 1 diabetes and the aged are noted as notably susceptible to clinically important hypoglycemia due to their lowered ability to recognize hypoglycemic symptoms and effectively talk their wants. Hypoglycemia Treatment Providers should continue to counsel sufferers to treat hypoglycemia with fast-acting carbohydrates on the blood glucose alert value of 70 mg/dL (3. Hypoglycemia treatment requires ingestion of glucose- or carbohydrate-containing foods. Glucagon the use of of} glucagon is indicated for the treatment of hypoglycemia in folks unable or unwilling to eat carbohydrates by mouth. Those in close contact with, or having custodial care of, folks with hypoglycemia-prone diabetes (family members, roommates, school personnel, child care providers, correctional establishment workers, or coworkers) should be instructed on the use of of} glucagon kits together with the place the equipment is and when and the way to|tips on how to} administer glucagon. A corollary to this "vicious cycle" is that a number of} weeks of avoidance of hypoglycemia has been demonstrated to enhance counterregulation and hypoglycemia awareness in lots of} sufferers (68). Hence, sufferers with one or more of} episodes of clinically important hypoglycemia might benefit from minimal of|no much less than} shortterm relaxation of glycemic targets. For further information on management of sufferers with hyperglycemia within the hospital, please check with Section 14 "Diabetes Care within the Hospital. Any situation resulting in deterioration in glycemic control necessitates more frequent monitoring of blood glucose; ketosis-prone sufferers also require care. A randomised, 52-week, treat-to-target trial evaluating insulin detemir with insulin glargine when administered as add-on to glucose-lowering drugs in insulin-naive folks with sort 2 diabetes. Realtime steady glucose monitoring significantly reduces extreme hypoglycemia in hypoglycemiaunaware sufferers with sort 1 diabetes. The Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Research Group. Intensive glucose control and macrovascular outcomes in sort 2 diabetes [published correction appears in Diabetologia 2009;fifty two: 2470]. Diabetes Care 2009;32:13351343 Diabetes Care Volume forty, Supplement 1, January 2017 S57 7. Obesity Management for the Treatment of Type 2 Diabetes Diabetes Care 2017;40(Suppl. Small studies have demonstrated that in obese sufferers with sort 2 diabetes more extreme dietary power restriction with very low-calorie diets can scale back A1C to ,6. Weight lossinduced enhancements in glycemia are most likely to happen early within the pure history of sort 2 diabetes when obesityassociated insulin resistance has caused reversible b-cell dysfunction however insulin secretory capability stays comparatively preserved (5,8,10). The aim of this section is to present evidence-based suggestions for dietary, pharmacological, and surgical interventions for obesity management as remedies for hyperglycemia in sort 2 diabetes. Strategies embody diet, physical exercise, behavioral remedy, pharmacological remedy, and metabolic surgical procedure (Table 7. A For sufferers who achieve short-term weight reduction targets, long-term ($1-year) comprehensive weight upkeep applications should be prescribed. Such applications should present minimal of|no much less than} month-to-month contact and encourage ongoing monitoring of physique weight (weekly or more frequently), continued Suggested quotation: American Diabetes Association. S58 Obesity Management for the Treatment of Type 2 Diabetes Diabetes Care Volume forty, Supplement 1, January 2017 Table 7. Lifestyle Interventions Among chubby or obese sufferers with sort 2 diabetes and insufficient glycemic, blood strain, and lipid control and/or other obesity-related medical situations, life-style adjustments that lead to modest and sustained weight loss produce clinically meaningful reductions in blood glucose, A1C, and triglycerides (35). Although advantages seen with as little as 5% weight reduction, sustained weight loss of $7% is perfect. These diets might differ within the forms of foods they prohibit (such as high-fat or high-carbohydrate foods) however are effective in the event that they} create the mandatory power deficit (1619). Interventions should be provided by trained interventionists in either particular person or group classes (21). Some industrial and proprietary weight reduction applications have proven promising weight reduction results (22).
References:
- https://www.tn.gov/content/dam/tn/mentalhealth/documents/Pages_from_CY_BPGs_464-472.pdf
- https://naspghan.org/files/documents/pdfs/position-papers/Health_Supervision_in_the_Management_of_Children.19%5B1%5D.pdf
- https://www.engageny.org/file/24091/download/ckla_g1_u1_rdr.pdf?token=sIq5xy4V
- https://www.unco.edu/marie/pdf/resources/2014NTFDBIBiblioStandardPrint.pdf