.png)
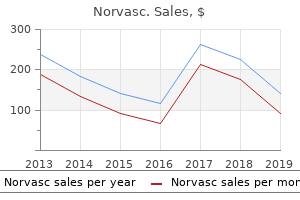
Quality norvasc 2.5 mg
Voluntary genetic testing ought to always be associated with aggressive counseling and assist. Because of the potential changes in life for different household mem bers, every particular person receiving the genetic info must be counseled separately. More than half of girls who inherit mutations will develop breast cancer by the age of fifty compared with less than 2% of girls without the genetic defect. These mutations have an autosomal dominant inheritance pat tern, indicating that women who inherit only one genetic defect can develop the phenotypic cancers. Colon cancer genetic testing There are multiple forms of colon cancer strongly associ ated with household historical past. These genetic defects are inherited in an autosomal dominant style and are essential for genome mismatch repair. The affected person presents with over one hundred polyps in his or her colon-one or more of which may degenerate into can cer. Affected kids turn out to be totally debili tated by 2 to 5 years of age and die by ages 5 to eight. The primary defect in affected patients is a mutation within the hexosaminidase A gene, which is on chromo some 15. Ashkenazi (Eastern European) Jews and nonJewish French Canadians, particularly these within the Cajun population in Louisiana, are affected most. Both the check for the protein and that for the gene mutation are performed on a blood pattern or on chorionic villus samples obtained during amniocentesis (p. This gene encodes the synthesis of a protein that serves as a channel through which chloride enters and leaves some types of epithelial cells. Characteristics of familial melanoma include frequent multiple major melanomas, early age of onset of first melanoma, and frequently the presence of atypical or dys plastic nevi (moles). Family members with the following charac teristics might consider testing for p16 genetic mutations: � Multiple diagnoses of major melanoma � Two or extra relations with melanoma � Melanoma and pancreatic cancer � Melanoma and a personal or household historical past of multiple atypical nevi � Relatives of a affected person with a confirmed p16 genetic mutation Approximately 20% to 40% of families with three or extra affected firstdegree relatives show inheritance of mutations within the p16 gene. The average age at diagnosis is 35 years for these with a mutation in p16 versus 57 years within the general population. Hemochromatosis genetic testing the diagnosis of hemochromatosis is traditionally made through the use of serum iron studies. Increased intestinal iron absorption and intracellular iron accu mulation result in progressive injury of the liver, coronary heart, pancreas, joints, reproductive organs, and endocrine glands. Without ther apy, males might develop symptoms between 40 and 60 years of age and girls after menopause. Early initia tion of phlebotomy remedy reduces the frequency or severity of hemochromatosisrelated symptoms and organ injury. However, lymph node contain ment at diagnosis may be present in as much as 75% of patients for whom a thyroid nodule is the first signal of disease. Cardiac genetic testing Mutations in sarcomeric genes trigger early onset cardiac chan nelopathies and cardiomyopathies. Patients with a sarcomeric gene mutation are nearly three times extra prone to endure an adverse cardiac outcome (cardiovascular dying, nonfatal ischemic stroke, or development to severe coronary heart failure). Many dad and mom are given misinformation on the time of twin births as to whether or not the twins are identical or fraternal. Unfortunately, prenatal testing of the fetal parts for paternity testing requires invasive testing similar to chorionic vil lus sampling or amniocentesis. There are times, particularly in circumstances of rape, when early pregnancy paternity identifica tion is desired. Noninvasive prenatal paternity testing can now be performed precisely by extracting and amplifying fetal chromo some alleles from maternal blood. In a courtroom, the reliability of the proof can defend the person and soci ety as a complete. Inform the affected person of the excessive prices of genetic testing and that it will not be coated by all medical insurance policy. These pro teins are poisonous to the mucosa of the small intestine and trigger characteristic pathologic lesions. The solely therapy is for the affected person to abstain from wheat and wheatcontaining products. When an affected affected person ingests wheatcontaining meals, gluten and gliadin build up within the intestinal mucosa. These gliadin and gluten proteins (and their metabolites) trigger direct mucosal injury. The identification of these antibodies within the blood of patients with malabsorption is useful in sup porting the diagnosis of celiac sprue or dermatitis herpetiformis. However, a definitive diagnosis of celiac disease may be made solely when a affected person with malabsorption is discovered to have the patho logic intestinal lesions characteristic of celiac disease. This may be particularly advantageous within the pediatric population, including the evaluation of children with failure to thrive. In patients with recognized celiac disease, these antibodies can be used to monitor disease status and dietary compliance. As serum glucose ranges rise within the blood, glucagon is inhibited by a unfavorable feedback mechanism. Glucagon deficiency occurs with intensive pancreatic resection or with burnedout pancreatitis. If glu cagon ranges fail to rise even with arginine infusion, a diagnosis of glucagon deficiency as a result of pancreatic insufficiency is confirmed. To differentiate the causes of glucagon insufficiency between pancreatic insuf ficiency and diabetes, arginine stimulation is performed. Patients with diabetes could have an exaggerated elevation of glucagon with arginine. Furthermore, in patients with diabetes, hypogly cemia fails to stimulate glucagon launch as would occur in a non diabetic particular person. Because glucagon is assumed to be metabolized by the kid neys, renal failure is associated with excessive glucagon and, consequently, excessive glucose ranges. When rejection of a transplanted kid ney occurs, one of many first signs of rejection may be elevated serum glucagon ranges. Interfering components � Test results may be invalidated if a affected person has undergone a radioactive scan throughout the earlier forty eight hours. Drugs which will trigger decreased ranges include atenolol, pro pranolol, and secretin. Insulin drives glucose into the cells to be metabolized to glyco gen, amino acids, and fatty acids. Other hormones, similar to adrenocorticosteroids, adrenocortico tropic hormone, epinephrine, progress hormone, and thyroxine, also can affect glucose metabolism. For example, a glucose level of a hundred thirty five mg/dL may be irregular if the affected person is within the fasting state, however this level would be inside normal limits if the affected person had eaten a meal throughout the earlier hour. In general, true glucose elevations point out diabetes mellitus; nonetheless, one must pay attention to many different attainable causes of glucose, blood 475 hyperglycemia. The commonest trigger is inadvertent insulin overdose in patients with brittle diabetes. If diabetes is suspected by elevated fasting blood ranges, glycosylated hemoglobin (p. Glycosylated hemoglobin (web page 483) is now being performed extra frequently to establish diabetes as a result of this blood check rep resents blood sugar ranges over the earlier a hundred and twenty days. That being mentioned, the diagnosis of diabetes must be confirmed with a repeat of the identical checks initially performed however on a unique day to guard in opposition to laboratory error. Glucose determinations must be performed frequently in new patients with diabetes to monitor closely and regulate the insulin dosage to be administered. Fingerstick blood glucose determina tions are often performed earlier than meals and at bedtime. Patients with diabetes can then regulate their insulin doses of rapidacting subcutaneous insulin. For patients with diabetes who experience recurrent epi sodes of severe hypoglycemia or who require greater than three doses of insulin per day, minimally invasive glucose monitoring is available. A small, sterile, disposable glucosesensing gadget is inserted into the subcutaneous tissue (normally the arm). Specialized software then downloads the saved info, and a simpler insulin routine may be developed. To forestall hunger, which may artificially raise the glucose ranges, tell the affected person to not quick much longer than eight hours. However, the affected person must be capable of visually interpret the colour of the reagent strip.
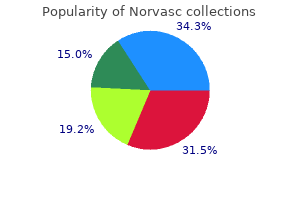
Effective norvasc 5 mg
Setting apart the defense additionally means acknowledging and bearing the helplessness of getting been victimized and dealing through the irrational self-blame that gave such individuals a fantasy of management over occasions throughout which they were helpless. In the past, short-appearing barbiturates similar to sodium amobarbital were used intravenously to reverse functional amnesia, however this technique is no longer employed, largely due to poor results. To date, pharmacological treatment has been restricted to symptom management or the management of comorbid situations. That is because sufferers suffering from dissociation regularly expertise comorbid dysthymic or main depressive dysfunction. Nevertheless, medicine compliance may be an issue with dissociative sufferers because dissociated character states may intervene with medicine taking or may take the medicine in an overdose try. Benzodiazepines have mostly been used to facilitate recall by controlling secondary anxiousness associated with retrieval of traumatic memories. Thus, anticonvulsant brokers may help management the dissociation associated with epileptogenic activity. On the opposite hand, anticonvulsant brokers have proven to be effective within the management of mood problems, in addition to the impulsiveness associated with character problems and brain harm. Also despite their effectiveness, these brokers produce less amnestic unwanted side effects than the benzodiazepines and thus may be most well-liked. Of all pharmacological brokers out there, antipsychotics will be the less desirable. In truth, there have been stories of increased ranges of dissociation and an increased incidence of unwanted side effects when utilized in sufferers suffering from dissociative problems. This is attributed to the influence of a spirit, power, deity, or different particular person, as evidenced by one (or extra) of the following: (a) stereotyped and culturally determined behaviors or actions which are skilled as being controlled by the possessing agent (b) full or partial amnesia for the event B. The trance or possession trance state causes clinically vital misery or impairment in social, occupational, or different essential areas of functioning. Dissociative Trance Disorder Dissociative Trance Dissociative trance dysfunction has been divided into two broad classes, dissociative trance and possession trance (American Psychiatric Association, 2000). Dissociative trance phenomena are characterized by a sudden alteration in consciousness, not accompanied by distinct different identities. In this form the dissociative symptom includes an alteration in consciousness quite than identity. Also, in dissociative trance, the activities carried out are quite easy, usually involving sudden collapse, immobilization, dizziness, shrieking, screaming, or crying. Dissociative trance phenomena regularly contain sudden, excessive modifications in sensory and motor management. A basic instance is the ataque de nervios, prevalent in Latin American nations. For instance, this phenomenon is estimated to have a 12% lifetime prevalence fee in Puerto Rico (Lewis-Fernandez, 1994). A typical episode includes a sudden feeling of tension, adopted by complete physique shakes, which may mimic convulsions. This is then adopted by hyperventilation, unintelligible screaming, agitation and often violent bodily actions. After the episode is over, topics complain of fatigue and having been confused, though this habits is dramatically completely different from basic postictal states. Some topics may expertise amnesia at least to some aspects of the event (Lewis-Fernandez, 1994). In these episodes, troubled individuals usually expertise a sudden vision, mostly of a threatening spirit. The observable habits consists of screaming or crying and bodily manifestation of overtly violent habits which regularly requires the sufferer to be bodily restrained. Possession Trance In contrast to dissociative trance episodes, possession trance includes the assumption of a definite different identity. Different from dissociative trance episodes, which are characterized by quite crude, simplistic, regressive-like behaviors, possession trance victims usually exhibit quite complex habits. During these episodes, topics may, for example, express in any other case forbidden ideas or wants, interact in unusually and uncharacteristic aggressive habits. Cultural Context Dissociative-like phenomena have been described in virtually each culture. Yet they appear to be extra prevalent within the less closely industrialized Second and Third World nations. Studies on the prevalence of dissociative problems in India have suggested that the 1-yr prevalence of dissociative trance dysfunction is roughly three. Trance and possession syndromes are by far the commonest kind of dissociative problems seen around the world. This distinction in prevalence and distribution of dissociative dysfunction across completely different populations may be mediated by cultural in addition to organic factors. Thus, being "possessed" by an out of doors entity would be extra culturally comprehensible and acceptable within the East. On the opposite hand, an obvious proliferation of particular person identities would match higher with the Western preoccupation with individualism. Nonetheless, the underlying dissociative mechanism inhibiting integration of notion, memory and identity may recommend a standard underlying mechanism amongst these dissociative syndromes. Trance dancers benefit from the remarkable privilege of being the only portion of this socially inflexible society capable of elevate their social status. During these altered states of consciousness, which usually occur within the context of a socially acceptable ceremony setting, they dance over sizzling coals, maintain a sword at their throat, or in different ways exhibit supernormal powers of concentration and bodily prowess. By contrast, disordered trance and possession trance are seen by the local community as an aberrant form of habits that requires intervention. Such signs usually arise within the context of household or social misery, for example, discomfort in a new household surroundings. Thus, cultural informants make it clear that individuals with dissociative trance dysfunction are irregular. Treatment Dissociation and Trauma One of the essential developments within the modern understanding of dissociative problems is the institution of a clearer link between trauma and dissociation. There is growing scientific proof that dissociation happens as a defense throughout traumatic experiences, constituting an attempt to maintain mental management at the moment when bodily management has been lost. Assault victims report floating above their physique, feeling sorry for the particular person being assaulted beneath them. Patients, victims of childhood abuse, have reported "taking themselves elsewhere" the place they might "safely play" by themselves or with imaginary associates, while their bodies were brutally abused by a perpetrator. Another means of examining the putative connection between dissociation and trauma is to look at the prevalence of dissociative signs after recent trauma. In the early literature examining responses to trauma, Lindemann (1944), studying the aftermath of the Coconut Grove fireplace, observed that the individuals who acted as though little or nothing had occurred had a particularly poor long-term prognosis. Indeed, it was the absence of publish traumatic signs on this group, in contrast with the agitation, dysphoria, and restlessness that typified the vast majority of survivors, that led him to formulate the normal process of acute grief. Research on survivors of different life-threatening occasions, including hostage taking, indicated that more than half have skilled a sense of detachment, feelings of unreality. However, in others it might become the matrix for later publish traumatic signs, similar to dissociative amnesia for the traumatic episode. Recollection of trauma tends to have an off�on quality involving either intrusion or avoidance (Horowitz, 1976), in which victims either intensively relive the trauma as though it were recurring or have problem remembering it. These diagnostic standards would designate roughly a third of individuals exposed to serious trauma as symptomatic. Most studies demonstrate that 25% or less of those who expertise serious trauma later become symptomatic. This diagnostic category is beneficial not only for research on the normal and irregular processes of adjusting to trauma, but additionally as a means of providing an essential opportunity for early intervention and thus prevention of later psychopathology. Even though dissociation has a role on the time of trauma, if the defense persists too long it might intervene with the working through of traumatic materials. Lindemann (1944) described the term grief work, referring to process needed to put traumatic expertise into perspective and cut back the likelihood of later signs. These neural models assumed that when there are issues with the processing of enter data (a mannequin for traumatic enter), the brain is extra more likely to have problem reaching a coherent and balanced output. Dissociation and Memory Systems There are two broad classes of memory generally known as explicit and implicit, declarative and procedural, or episodic and semantic. Explicit or episodic memory includes recall of private expertise recognized with the self, for example, "I went dancing final night".
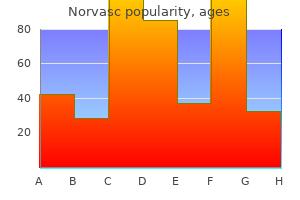
Cheap norvasc 10mg
Combination Drug Therapy �Combinationtherapy could beconsidered afteradequate trialsofmonotherapyand for patients documented to be adherent to the prescribed routine. Management includes dietary fats restriction (10�20% of calories as fats), weightloss,alcoholrestriction,andtreatmentofcoexistingdisorders(eg,diabetes). Drug remedy includes gemfibrozil or fenofibrate, niacin, and higher-efficiency statins(atorvastatin,pitavastatin,rosuvastatin,andsimvastatin). Ventricularhypertrophycanbecausedbypressureoverload(eg,systemicorpulmonary hypertension and aortic or pulmonic valve stenosis) or quantity overload (eg, valvularregurgitation,shunts,high-outputstates). Strategies include smoking cessation and control of hypertension, diabetes mellitus, and dyslipidemia. However, thiazides or the thiazide-like diuretic metolazone canbeusedincombinationwithaloopdiuretictopromoteveryeffectivediuresis. No Concomitant angina a If not already receiving this remedy for earlier If moderately severe to severe signs. Inadditiontoactinginthethickascending limb of the loop of Henle, they induce a prostaglandin-mediated enhance in renal bloodflowthatcontributestotheirnatriureticeffect. Becauseoftheirnegativeinotropiceffects,begin-blockersinverylowdoses with gradual upwarddose titration toavoid symptomaticworsening or acute decompensation. Onthebasis of regimensproven in largeclinical trialsto reducemortality,initialandtargetoraldosesareasfollows: arvedilol,three. Patients with decreased renal function, the aged, or these receiving interactingdrugs(eg,amiodarone)shouldreceive0. Metolazone or spironolactone could also be added if the patient fails to reply to loop diuretics and a second diuretic is required. However,acutereductionsinvenousreturnmayseverely compromise effective preload in patients with vital diastolic dysfunction or intravasculardepletion. However, this lower in preload can be hazardous forpatientswithoutexcessivefillingpressure,leadingtofurtherdecline incardiacindex. However,inotropesmaybeneededwithcertainpatients,suchasthose with low cardiac output states with organ hypoperfusion and cardiogenic shock. Milrinone could also be considered for patients receiving continual -blocker remedy becauseitspositiveinotropiceffectdoesnotinvolvestimulationof-receptors. At doses between 5 and 10 mcg/kg/min, chronotropic and 1-mediatedvasoconstrictingeffectsbecomemoreprominent. Venodilatorsreducepreloadbyincreasingvenouscapacitance,improvingsymptoms of pulmonary congestion in patients with high cardiac filling pressures. Compared with nitroglycerin or nitroprusside, it produces marginal improvement in clinical outcomes and is considerably dearer. Stimulation of V1A receptors (located in vascular smooth muscle cells and myocardium) leads to vasoconstriction, myocyte hypertrophy, coronary vasoconstriction, and optimistic inotropiceffects. ItisasubstrateofcytochromeP450-3A4andis contraindicated with potent inhibitors of this enzyme. Therapymay be restarted at a decrease dose if hyponatremia recurs or persists and/or these aspect effectsresolve. In clinical trials, tolvaptan improved hyponatremia, diuresis, and signs/ symptomsofcongestion. Patients with pheochromocytoma could have headaches, sweating, tachycardia, palpitations, and orthostatic hypotension. In main aldosteronism, hypokalemic signs of muscle cramps and weakness could also be current. Drug remedy recom- mendations are graded with power of advice and quality of evidence in brackets. Strength of suggestions: A, B, C are good, reasonable, and poor evidence to support recommendation, respectively. Quality of evidence: (1) evidence from more than one correctly randomized, managed trial; (2) evidence from no less than one properly-designed clinical trial with randomization, from cohort or case-managed research, or dramatic outcomes from uncontrolled experiments or subgroup analyses; (three) evidence from opinions of revered authorities, primarily based on clinical experience, descriptive research, or stories of professional communities. Start administering doses in such patients, using half the normal dosefollowedby gradual dosetitration. Compelling indications for particular medicine are evidence-primarily based suggestions from end result research or existing clinical tips. Thiseffectmaybeobviatedbyusing sustained-release formulations of nifedipine or other dihydropyridines. Other side effects of dihydropyridines are dizziness, flushing, headache, gingival hyperplasia, andperipheraledema. Theinitialdrop in cardiac output causes a compensatory enhance in peripheral vascular resistance. With continual remedy, extracellular fluid quantity and plasma quantity return to near pretreatment levels, and peripheral vascular resistance falls under baseline. Furthermore, many nondiuretic antihypertensive brokers induce sodium and water retention,whichiscounteractedbyconcurrentdiureticuse. Eplerenonehasan increased risk for hyperkalemia and is contraindicated in patients with impaired renalfunctionortype2diabeteswithproteinuria. Stimulation of presynaptic 2-receptors peripherallymay contributetoreducedsympathetic tone. Discontinue remedy if persistent increases inliverfunctiontestsoccur,becausethismayherald onsetoffulminant, life-threateninghepatitis. Reserpine �Reserpine depletes norepinephrine from sympathetic nerve endings and blocks transportofnorepinephrineintostoragegranules. Direct Arterial Vasodilators �Hydralazine and minoxidil trigger direct arteriolar smooth muscle rest. Compensatory activation of baroreceptor reflexes leads to increased sympatheticoutflowfromthevasomotorcenter,increasingheartrate,cardiacoutput, andreninrelease. Consequently,hypotensiveeffectivenessofdirectvasodilators diminishes over time except the patient can also be taking a sympathetic inhibitor andadiuretic. Lupus-like reactions can often be averted by utilizing whole every day doses less than 200 mg. Because of side effects, hydralazine has restricted usefulnessforchronichypertensionmanagement. Otherwise, management consists of proscribing exercise, bedrest,andclosemonitoring. Onset of hypotensive action is quick and disappears within 1 to 2 minutes ofdiscontinuation. Evaluatemorefrequentlyinpatientswitha history of poor control, nonadherence, progressive target-organ injury, or symptomsofadversedrugeffects. With greater degrees of obstruction, this responseisinadequate,andthecoronaryflowreserveaffordedbyR2vasodilationis insufficienttomeetoxygendemand. Zones of tissue with marginal blood flow could develop that areatriskformoreseveredamageiftheischemicepisodepersistsorbecomesmore severe. Nonischemic areas of myocardium could compensate for severely ischemic andborderzonesofischemiabydevelopingmoretensionthanusualinattemptto maintaincardiacoutput. Unalterableriskfactorsincludegender,age,familyhistoryorgeneticcomposition, environmental influences, and, to some extent, diabetes mellitus. Alterable risk elements include smoking, hypertension, hyperlipidemia, obesity, sedentary lifestyle, hyperuricemia, psychosocial elements similar to stress, and use of medication that may be detrimental(eg,progestins,corticosteroids,calcineurininhibitors). Cardioselective -blockers could reduce adverse results similar to bronchospasm,intermittentclaudication,andsexualdysfunction. Thehalf-lifeofnitroglycerinis1to5minutesregardless of the route, therefore the potential benefit of sustained-release and transdermal products. Dosing of lengthy-appearing preparations should be adjusted to present a hemodynamic response. Ranolazine �Ranolazine reduces calcium overload in ischemic myocytes through inhibition of thelatesodiumcurrent. Lifestyle modifications include every day physical exercise, weight management,dietarytherapy,smokingcessation,psychologicalinterventions,limitationof alcoholintake,andmanagementofbloodpressureanddiabetes. If blood strain is 140/ninety mm Hg or larger, drug remedy should be instituted along with or after lifestyle modifications. Medical Therapy for Relief of Symptoms Sublingual nitroglycerin or nitroglycerin spray for quick reduction of angina. Long-appearing nondihydropyridine calcium antagonists (verapamil, diltiazem) as an alternative of a -blocker as initial remedy. Ranolazine can be useful as a substitute for -blockers if initial treatment with -blockers causes unacceptable adverse results or is ineffective or contraindicated. Ranolazine mixed with a -blocker can be useful when initial -blocker treatment is unsuccessful.
Order 5 mg norvasc
Three separate collections, together with blood samples, are needed for accurate testing. These checks may establish the cause of calculus formation: � Blood calcium and phosphorus ranges detect hyperparathyroidism and show an elevated calcium stage in proportion to normal serum protein ranges. Renal failure, acute Acute renal failure is the sudden interruption of renal perform. How it happens Acute renal failure could also be classified as prerenal, intrarenal, or postrenal. Examples embody hypovolemia, hypotension, vasoconstriction, or inadequate cardiac output. One situation, prerenal azotemia (excess nitrogenous waste merchandise in the blood), accounts for 40% to 80% of all circumstances of acute renal failure. Usually, it can be rapidly reversed by restoring renal blood circulate and glomerular filtration. Causes of acute renal failure Acute renal failure is classified as prerenal, intrarenal, or postrenal. All situations that result in prerenal failure impair blood circulate to the kidneys (renal hypoperfusion), leading to decreased glomerular filtration rate and elevated tubular reabsorption of sodium and water. Intrarenal failure results from harm to the kidneys themselves; postrenal failure, from obstructed urine circulate. Prerenal failure Cardiovascular problems Arrhythmias Cardiac tamponade Cardiogenic shock Heart failure Myocardial infarction Hypovolemia Burns Dehydration Diuretic overuse Hemorrhage Hypovolemic shock Trauma Peripheral vasodilation Antihypertensive medication Sepsis Renovascular obstruction Arterial embolism Arterial or venous thrombosis Tumor Severe vasoconstriction Disseminated intravascular coagulation Eclampsia Malignant hypertension Vasculitis Intrarenal failure Acute tubular necrosis Ischemic harm to renal parenchyma from unrecognized or poorly handled prerenal failure Nephrotoxins, including anesthetics similar to methoxyflurane, antibiotics similar to gentamicin, heavy metals similar to lead, radiographic contrast media, and organic solvents Obstetric issues, similar to eclampsia, postpartum renal failure, septic abortion, and uterine hemorrhage Pigment launch, similar to crush injury, myopathy, sepsis, and transfusion reaction Other parenchymal problems Acute glomerulonephritis Acute interstitial nephritis Acute pyelonephritis Bilateral renal vein thrombosis Malignant nephrosclerosis Papillary necrosis Periarteritis nodosa (inflammatory disease of the arteries) Renal myeloma Sickle cell disease Systemic lupus erythematosus Vasculitis Postrenal failure Bladder obstruction Anticholinergic medication Autonomic nerve dysfunction Infection Trauma Tumor Ureteral obstruction Blood clots Calculi Edema or inflammation Necrotic renal papillae Retroperitoneal fibrosis or hemorrhage Surgery (accidental ligation) Tumor Uric acid crystals Urethral obstruction Prostatic hyperplasia or tumor Strictures Going via phases With therapy, every sort of acute renal failure passes via three distinct phases: oliguric (decreased urine output) diuretic (elevated urine output) restoration (glomerular filtration rate normalizes). Before harm occurs, the kidney responds to decreased blood circulate by conserving sodium and water. The diuretic section may last from 1 to 3 weeks and is marked by urine output that may range from normal (1 to 2 L/day) to as high as 4 to 5 L/day. These situations can result in deficits of potassium, sodium, and water that can be lethal if left untreated. If the cause of the diuresis is corrected, azotemia gradually disappears and the affected person improves significantly-resulting in the restoration stage. Getting complicated Primary harm to the renal tubules or blood vessels results in kidney failure (intrarenal failure). The causes of intrarenal failure are classified as nephrotoxic, inflammatory, or ischemic. When the harm is caused by nephrotoxicity or inflammation, the fragile layer under the epithelium (basement membrane) turns into irreparably damaged, commonly continuing to persistent renal failure. Severe or prolonged lack of blood circulate (isch emia) may result in renal harm (ischemic parenchymal injury) and excess nitrogen in the blood (intrinsic renal azotemia). If the underlying downside is a change in blood stress and volume, the affected person may have: � oliguria � tachycardia � hypotension � dry mucous membranes � flat neck veins � lethargy progressing to coma � decreased cardiac output and funky, clammy skin in a affected person with coronary heart failure. Urine sodium stage is lower than 20 mEq/L if oliguria results from decreased perfusion and greater than 40 mEq/L if it results from an intrarenal downside. Battling illness Treating acute renal failure Supportive measures for acute renal failure embody: a high-calorie food regimen, low in protein, sodium, and potassium fluid and electrolyte stability monitoring for indicators and signs of uremia fluid restriction diuretic therapy in the course of the oliguric section prevention of infection renal-dose dopamine to improve renal perfusion corticosteroids. Halting hyperkalemia Meticulous electrolyte monitoring is required to detect excess potassium in the blood (hyperkalemia). If signs occur, hypertonic glucose, insulin, and sodium bicarbonate are given I. If these measures fail to control uremia, the affected person might have hemodialysis or continuous renal alternative therapy. Renal failure, persistent Chronic renal failure, a normally progressive and irreversible deterioration, is the tip results of gradual tissue destruction and loss of kidney perform. Occasionally, however, persistent renal failure results from a rapidly progressing disease of sudden onset that destroys the nephrons and causes irreversible kidney harm. Healthy nephrons compensate for destroyed nephrons by enlarging and increasing their clearance capacity. The kidneys can preserve comparatively normal perform until about 75% of the nephrons are nonfunctional. Eventually, the healthy glomeruli are so overburdened they turn out to be sclerotic and stiff, resulting in their destruction as nicely. If this situation continues unchecked, toxins accumulate and produce doubtlessly deadly modifications in all major organ systems. What to search for Few signs develop until greater than 75% of glomerular filtration is misplaced. Major findings embody: � hypervolemia (irregular increase in plasma volume) � peripheral edema � hyperphosphatemia � hyperkalemia � hypocalcemia � azotemia � metabolic acidosis � anemia � peripheral neuropathy. Battling illness Treating persistent renal failure Treatment for persistent renal failure may encompass one or more of these remedies, relying on the stage of failure. Dialysis options embody: hemodialysis, which filters blood via a dialysis machine peritoneal dialysis, by which a catheter is placed in the peritoneal cavity for instillation of dialysate. Emergency measures Potassium ranges in the blood have to be monitored to detect hyperkalemia. Emergency therapy consists of dialysis therapy, oral or rectal administration of cation exchange resins, similar to sodium polystyrene sulfonate, and I. Cardiac tamponade resulting from pericardial effusion may require emergency pericardiocentesis or surgery. Intensive dialysis and thoracentesis can relieve pulmonary edema and pleural effusion. Collecting and eliminating waste the kidneys: filter blood flowing via the glomeruli reabsorb filtered fluid via the tubules launch the filtered substance from the tubules. Regulating blood stress the kidneys: produce and secrete renin in response to a decline (actual or perceived) in extracellular fluid volume. Regulating vitamin D and calcium formation the kidneys help convert vitamin D to its lively kind. Renal problems Acute tubular necrosis-destruction of the tubular segment of the nephron, causing renal failure and uremia Benign prostatic hyperplasia-enlarged prostate gland that compresses the urethra and causes urinary obstruction Glomerulonephritis-bilateral inflammation of the glomeruli, commonly following a streptococcal infection Hydronephrosis-irregular dilation of the renal pelvis and the calyces of 1 or both kidneys Prostatitis-inflammation of the prostate gland Renal calculi-substances that usually dissolve in the urine precipitate to kind "kidney stones" Renal failure, acute-sudden interruption of renal perform caused by obstruction, poor circulation, or kidney disease Renal failure, persistent-irreversible deterioration of tissue and eventual loss of kidney perform Quick quiz 1. This is because creatinine is only filtered by the glomeruli and never reabsorbed by the tubules. One such situation, prerenal azotemia, accounts for between 40% and 80% of all circumstances of acute renal failure. Depending on the size of the enlarged prostate and resulting issues, the obstruction could also be handled surgically or symptomatically. Your capacity to concentrate, absorb, and secrete data about the kidneys is wonderful! Pumped by the heart, it constantly circulates via the blood vessels, carrying important elements to each part of the physique. Blood is manufactured from: � a liquid component-plasma � cellular elements-erythrocytes, leukocytes, and thrombocytes suspended in plasma. A downside with any of these elements may have critical and even lethal penalties. Plasma Plasma is a clear, straw-colored fluid that consists primarily of the proteins, albumin, globulin, and fibrinogen held in aqueous suspension. Other elements in plasma embody glucose, lipids, amino acids, electrolytes, pigments, hormones, oxygen, and carbon dioxide. These elements regulate acid-base stability and immune responses as well as carry vitamins to tissues and help to mediate coagulation. About 80% to 90% of erythropoietin is made in the kidneys; the rest comes from the liver. The making of an erythrocyte Erythrocyte formation begins with a precursor, called a stem cell. Development requires vitamin B12, folic acid, and minerals, similar to copper, cobalt, and-especially-iron. Iron is present in food and, when consumed, is absorbed in the duodenum and higher jejunum. After iron is absorbed, it might be transported to the bone marrow for hemoglobin synthesis. Iron can also be transported to needy tissues similar to muscle for myoglobin synthesis.
Cheap 10mg norvasc
Psychosocial Treatments Behavioral Treatment Various behavioral techniques have been tried. The most profitable technique, behavior reversal, relies on designing competitive behaviors that ought to inhibit the behavior of hair-pulling. For example, if hair-pulling requires raising the arm to the scalp and contracting the muscle tissue of the hand to grasp a hair, the behaviorist might design a behavioral program by which the affected person is taught to lower the arm and extend the muscle tissue of the hand. As with behavioral techniques generally, these interventions are most profitable when the affected person is strongly motivated and compliant. In addition, the treating psychiatrist must be experienced in the usage of such techniques. At this time, the potential for the efficacy of this remedy strategy appears good. Clomipramine resulted in symptom reduction greater than that with placebo, however the difference fell short of statistical significance. As with behavioral interventions, the benefits of this strategy are sometimes depending on a highly motivated affected person who can often carry out self-hypnotic measures as instructed by the psychiatrist. Successful use of hypnotherapy for youngsters with trichotillomania has additionally been reported. Dynamic Psychotherapy Many psychoanalytically oriented descriptions of people with trichotillomania have been revealed. Self-assist and Other Groups Self-assist teams for sufferers with trichotillomania have appeared. Some sufferers appear to expertise significant reduction in hair-pulling symptoms after starting participation in such a bunch. Although the efficacy of such teams in reducing symptoms stays to be established, most sufferers with trichotillomania can profit from assembly other people with similar symptoms. Many have experienced parental condemnation for the behavior and have been regularly castigated for a "behavior" which may be considered by others as underneath their voluntary control. The expertise of assembly others with the condition is extremely supportive for such people and will assist to scale back the attendant stress whereas supporting self-esteem. Combined remedy with anxiolytics may be useful for some and will contribute to the reduction in symptoms of trichotillomania. Although fluoxetine may be useful for sufferers with consuming disorders, medication remedy alone is unlikely to be enough and the usual multimodal approaches for the remedy of bulimia nervosa or anorexia are acceptable. Demographical Features When trichotillomania presents in early childhood, the condition may be likely to be inherently self-restricted. Such strategies embody day by day utility of a nonmedicinal ointment to the affected area and reminding the child that the aim is elimination of the hair-pulling behavior. Some suggest that the child be given the duty of making use of the ointment with parental supervision. There have been no systematic research of the benefits of such interventions, but dermatologists who specialize in the remedy of kids have noted that hair-pulling behavior might regularly disappear within a number of weeks of initiating such an strategy. In circumstances by which childhood trichotillomania is extra persistent, the parent and psychiatrist are confronted with a dilemma. Medication must be cautiously thought-about in the remedy of childhood trichotillomania. Although medication may be useful, the absence of knowledge supporting the benefits of such treatments in kids signifies a conservative strategy. Should the psychiatrist be offered with trichotillomania in an individual of superior age, particular consideration must be paid to traditional considerations concerning the usage of these medications in the aged. Lower doses of medication must be thought-about because of potential altered pharmacokinetics in older persons. Medications with anticholinergic unwanted side effects (similar to clomipramine) might present greater hazards for the older individual. Sedative-hypnotic anxiolytics must be used sparingly because of greater vulnerability to cognitive unwanted side effects and the elevated threat of falling. Women of childbearing potential (maybe nearly all of people who might present for remedy) must be advised concerning the potential risks of these medications to a developing fetus. If the affected person is pregnant or considering being pregnant, behavioral treatments may be favored. The psychiatrist must be sensitive to the interaction between cultural values and trichotillomania. Women of certain cultures may be extra prone to distress if trichotillomania is perceived as a hindrance to attaining valued objectives, similar to marriage. It also needs to be noted that in some communities, wigs and other hair accessories are typically acceptable and will present a cushty means of diminishing the cosmetic impact of hair loss. Treatment of Comorbid Conditions Depression, dysthymic disorder and anxiety symptoms occur regularly in sufferers with trichotillomania. Successful remedy of despair may not be related to reduction in trichotillomania. If despair or dysthymic disorder is present and independently offers an indication for medication, one of many antidepressants mentioned earlier must be chosen. If panic disorder is present, either medication should be used, but fluoxetine might initially exacerbate panic attacks in such sufferers and initiation of remedy at low doses (2. In the Standard Edition of the Complete Psychological Works of Sigmund Freud, Vol. Ibanez A, Blanco C, and Saiz-Ruiz J (2002) Neurobiology and genetics of pathological playing. Lee S (1994) the heterogeneity of stealing behaviors in Chinese sufferers with anorexia nervosa in Hong Kong. Lorenz V (1981) Differences discovered amongst Catholic, Protestant, and Jewish households of pathological gamblers, in Fifth National Conference on Gambling and Risk Taking. The symptoms must develop within 3 months after the onset of the stressor (criterion A). No definition adequately specifies precise boundaries for the concept of a "psychological disorder". Whatever its authentic cause, it must presently be thought-about a manifestation of a behavioral, psychological, or organic dysfunction in the individual". There are, in Essentials of Psychiatry Jerald Kay and Allan Tasman � 2006 John Wiley & Sons, Ltd. The improvement of emotional or behavioral symptoms in response to an identifiable stressor(s) occurring within 3 months of the onset of the stressor(s). Specify if: Acute: if the disturbance lasts lower than 6 months Chronic: if the disturbance lasts for 6 months or longer Adjustment disorders are coded primarily based on the subtype, which is selected based on the predominant symptoms. Major affective disorder Yet, in the grey space by which early diagnosis might have monumental value with modest therapeutic funding, tips are the most tenuous. It is the professionals at the "front door" � primary care physicians, triage personnel, emergency division workers, walk-in clinic workers � who need help in making this difficult call: Is there adequate psychiatric morbidity to warrant psychological well being intervention The sex ratio was extra equal in kids and adolescents, though there was still a slight extra of feminine sufferers. Thirty % had symptomatic and practical impairment 6 months following surgery. Since sufferers handled for their psychological states had longer survival time, remedy of despair in cancer sufferers must be thought-about integral to their medical remedy. For example, there may be a number of stressors, insidious or persistent, as opposed to discrete events. Furthermore, relatively minor precipitating events might generate a disturbance in an individual who has beforehand been sensitized to stress. Cohen (1981) argued that acute stresses are totally different from persistent ones in both psychological and physiological terms; that the meaning of the stress is affected by "modifiers" � ego strengths, support methods, prior mastery � and that one must differentiate manifest and latent meaning of the stressors. An objectively overwhelming stress might have little impact on one individual, whereas one other individual might regard a minor one as cataclysmic. A recent minor stress superimposed on a previous underlying (major) stress (which had no observable effect on its own) might have a major impact, not working independently but by its additive effect: the concatenation of events (Hamburg, private communication). Specific forms of annoying events and individual patterns of stress response appear to be preferentially associated to the development of psychiatric symptoms in susceptible people. The linear mannequin Chapter 61 � Adjustment Disorders 781 the ideas of "common expectable surroundings". Such individual cultural�social concerns often require an understanding on the a part of the psychiatrist and thereby often render the evaluation of whether a response is extreme or maladaptive a judgment call. The specific mood and anxiety disorders are often related to and even precipitated by stress. More research is needed carefully to demarcate the boundaries or the meaning of these boundaries among the many problemlevel, subthreshold and threshold disorders, particularly with regard to the function of stressors as etiological precipitants, concomitants, or components primarily unrelated to the prevalence of a selected psychiatric diagnosis.
Saint Ignatius-beans (Ignatius Bean). Norvasc.
- For faintness, use as a tonic, and other uses.
- Dosing considerations for Ignatius Bean.
- How does Ignatius Bean work?
- What is Ignatius Bean?
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96174
Purchase 5 mg norvasc
Preparation of the Patient the cognitive and behavioral therapies explicitly incorporate methods to improve involvement and preparedness of the affected person for remedy. Patients are typically inspired to read related written materials describing the speculation and strategies of the remedy; for widespread issues, such as main depressive dysfunction and panic dysfunction, self-help manuals for patients are now available (Burns, 1990; Greenberger and Padesky, 1995; Wright and Basco, 2001). Outcome Assessment Cognitive and behavioral therapies are, partially, distinguished by their integrated use of goal assessment methods. For despair and the anxiety issues, numerous nicely-established score scales are available. Therapist-administered scales embrace the Hamilton Anxiety Rating Scale (Hamilton, 1959) and the Hamilton Depression Rating Scale (Hamilton, 1960) as well as the Yale-Brown Obsessive�Compulsive Scale (Goodman et al. Self-report assessments of signs embrace the Beck Depression Inventory (Beck et al. These scales are typically administered before treatment Chapter 69 � Cognitive and Behavioral Therapies 883 and repeated periodically. The Dysfunctional Attitudes Scale, the Attributional Style Questionnaire and the Automatic Thoughts Questionnaire may be used to consider distorted cognitions (Dobson and Shaw, 1986). As suggested earlier, high residual ranges of cognitive signs more than likely convey an increased danger for relapse after termination of treatment (Thase et al. No continuation (n = 10) Drug plus continuation (n = eleven) Cognitive remedy (n = 10) Combined cognitive pharmacotherapy (n = thirteen) 50% 32% 21% 60 forty 20 0 0 four 8 12 16 Months in comply with-up 20 15% 24 Augmentation of Therapy One of the major methods of augmenting a cognitive and behavioral remedy is to add an acceptable type of pharmacotherapy. The cognitive and behavioral therapies are the most effective-studied psychological remedies of main depressive, panic, generalized anxiety and obsessive�compulsive issues. Cognitive and behavioral therapies are being adapted for adjunctive use with pharmacotherapy for treatment of bipolar dysfunction and schizophrenia. The cognitive and behavioral therapies have turn into one of the standard psychosocial treatment approaches for mental issues. Furthermore, incomplete remission of despair results in recurrence, and this has many opposed economic, interpersonal and medical penalties (Thase, 1992). In International Handbook of Cognitive and Conclusion the cognitive and habits therapies are based mostly on wellarticulated theories that have a powerful empirical foundation. These therapies emphasize goal assessments and use of directive interventions aimed at decreasing symptomatic distress, enhancing interpersonal skills, and bettering social and vocational functioning. Cognitive interventions are targeted primarily on identifying and modifying distorted ideas and pathological schemas. Behavioral techniques to improve publicity, improve exercise, improve social skills and enhance anxiety administration are helpful modalities, and may complement or amplify the results of cognitive methods. Similarly, the cognitive perspective can add depth to behavioral models for remedy by teaching patients the way to recognize and modify their attitudinal vulnerabilities. Family remedy thus engages relational and communicational processes of households and social networks as a primary context for fixing scientific issues or treating psychiatric issues, even though one family member could be the sole bearer of distress or signs. By educating relations or altering household patterns of relating or communicating, such scientific issues as despair, anxiety, marital battle, or disruptive childhood habits could be resolved or attenuated. The completely different household remedy traditions could be usefully contrasted by comparing how each constructions perceptual, cognitive, and govt processes when clinicians work with households � from each of these perspectives: trates upon motivations, conflicts, defenses and relationships from the past that presently affect the present. Family interactions are explained in terms of internal processes inside individual relations. Therapeutic change is sought through relations gaining acutely aware insight into beforehand unconscious processes that have been producing issues in household relationships. What to Look For Psychodynamic household remedy grounds its work in historic info. These experiential models govern how meanings are attributed to such household patterns as guidelines for how people should respond and models for being a person or a lady, husband or wife, or mother or father. Some of the diagnostic patterns upon which psychodynamic household therapists focus when assessing households embrace the next: � What does a therapist look for Different household remedy traditions are themselves greatest considered completely different units of ideas and interventions to be valued as potential tools inside comprehensive, multimodality treatment programs. We will illustrate the range of perspectives and interventions available within the completely different traditions by analyzing, in turn, how psychodynamic, structural, strategic, cognitive� behavioral and postmodern household remedy traditions each would possibly strategy a scientific drawback. The early psychoanalysts noted that intrapsychic processes of an individual powerfully shape his or her interactions with other people, and most so in emotionally intimate relationships of couples and households. Extending the concepts and language of psychoanalysis to household habits was a logical next step for many who started assembly with parents and children, couples and entire households. In specific, object relations concept supplied a bridge from the individual intrapsychic processes to the interpersonal processes of households (Scharff and Scharff, 1987; Framo, 1991; Slipp, 1991). In projective identification, one family member (a father or mother or couple companion) relates to another family member (a particular youngster or the other couple companion) as if she or he embodied a projected a part of self. The projecting family member then interacts with, or relates to, the projected a part of self as if that part have been an internalized a part of himself or herself. The projecting family member unconsciously prompts the other to conform to the way in which during which she or he is being perceived, evoking within the other the associated emotions and behaviors as if they have been genuine. When considered from the surface by the therapist, it seems as if the 2 are in collusion with one another so as to maintain these mutual, projected perceptions. Projection of disavowed parts of the self, whether or not positive or unfavorable, has the impact of charging the relationship with emotion that has been transposed from an intrapsychic sphere into an interpersonal one. Acted out interpersonally, it serves to lower psychic anxiety on the expense of an increase in rigidity and deadlock within the relationship. Unresolved Grief When a family member, or the household as a complete, has not absolutely grieved losses, the household can turn into developmentally frozen. While so preoccupied with the past, it can be difficult to focus enough time and vitality on present issues. Clarity of Ego Boundaries and Capacity for Intimacy/ Separateness Conflicted household relationships can characterize an alternate technique for stabilizing emotional distance when 886 Chapter 70 � Family Therapy 887 the involved relations lack the emotional maturity to regulate closeness and distance in additional differentiated methods. This has been a common model for understanding couples who chronically struggle yet never separate. What to Do Psychodynamic household therapists employ the fundamental tools of psychodynamic psychotherapy (opening emotional expression, clarifying communications, encouraging relations to speak from the "I" place, and interpretation of unconscious conflicts) to resolve projective processes, cutoff relationships, and difficulties in modulating closeness and distance in household relationships. Psychodramatic techniques, such as doubling and role reversal, can play helpful roles in implementing these interventions (Blatner, 1994). Therapeutic rituals are notably helpful in facilitating grief over losses and in facilitating developmental transitions, such as a young grownup leaving home or a pair transferring into retirement years (Imber-Black and Roberts, 1992). The therapist observes how boundaries, hierarchy, alliances and coalitions are related to the presenting symptom, as well as any repetitive-behavioral sequences (verbal or nonverbal) that contain symptomatic habits. What to Think About the structural household therapist considers the problem to be sustained by the present household structure and its community ecosystem. Important questions to reply in assessing these relationships embrace: � To what parts of household structure � boundaries, hierarchy, � � Structural Family Therapy Structural household remedy considers issues involving a particular family member to be inextricably linked to the organizational context of the complete household. Family structure is the inner group of the household that dictates how, when and to whom relations relate while carrying out the varied features of the household (Aponte and VanDeusen, 1981; Colapinto, 1991). Some necessary parts of household structure for scientific work are boundaries, hierarchy, alliances and coalitions: alliances, coalitions � do occurrences of the presenting drawback seem linked What to Do Structural household therapists ameliorate signs by shifting household structure. Boundaries could be strengthened or weakened by behavioral assignments that exclude a particular family member from sure moments of household life. Alliances are inspired when they support the individual development of relations and strengthen the household as a complete. For instance, a boundary around the parental couple implies that the children are included in discussions of sure matters however not in others; Hierarchy Relative affect of each family member upon the outcome of an exercise. For instance, all relations might have opinions about spending cash, but the parents as a pair typically have the final say; Alliances Family members joining collectively to support another family member. For instance, older kids might be a part of the nicely-father or mother in organizing to father or mother younger kids if the other father or mother have been to turn into critically ill; Coalitions Family members joining collectively in opposition to another family member. The therapist units clear targets that intervene by changing relational and communicational processes within the household (Madanes, 1981; Stanton, 1981). Strategic remedy was designed as a counterpoint to psychodynamic psychotherapy by emphasizing "how" people can behave differently so as to clear up issues, rather than "why" they behave as they do. Problems are considered as persistent efforts by one or more relations to apply an answer that is sensible however is inadequate for the problem at hand, such that "the answer turns into the problem". The household structure should present cohesive and versatile responses to life stresses so that necessary household features � parenting, offering revenue, marital intimacy, recreation and other actions � could be carried out successfully, and relations can grow and mature in their individual lives. At such times when revolutionary drawback-fixing is required, people nevertheless stick with once profitable methods that are now outdated.
Syndromes
- Testicle ultrasound
- Lethargy
- Nutritional counseling
- Loss of self-esteem
- Severe depression
- Heart attack or stroke
- You have problems hearing when there is background noise.
- Muscle weakness
- Increase fats in the diet to increase energy consumption, if you are tolerating fats. Add margarine or butter to breads and vegetables. Add gravies and sauces to foods in large amounts.
Cheap 2.5mg norvasc
These individuals are generally not sleepy until a number of hours after "regular" bedtime. In essence, their rhythm is shifted to a later clock time relative to typical relaxation�activity patterns. Individuals with delayed sleep section usually choose careers that enable them to set their own schedules, such as freelance writers. Delayed sleep section occurs generally in late adolescence and young adulthood, such as in school college students. As many of those individuals age, however, their endogenous sleep�wake rhythm advances and so they ultimately are able to conform themselves to a standard relaxation interval at night time. For others, however, this section shift of the endogenous oscillator could lead at a later age to the advanced sleep section. The etiology of utmost "night time owls" and "larks" might be multifaceted but, in some cases, seems to reflect genetic factors. Chapter fifty nine � Sleep and Sleep�Wake Disorders 745 Treatment Clinical management includes chronobiological methods to shift the section position of the endogenous circadian oscillator in the acceptable direction. Light is normally administered in doses of 2500 lux for a interval of two hours per day, though the ideal depth and length are but to be determined. For some individuals, spending more time outside in brilliant daylight could also be enough to deal with the sleep section. For example, individuals with delayed sleep section must be inspired to remove blinds and curtains from their windows, which might enable the sunlight to pour into their bedrooms in the morning when they need to arise. In addition, gradual adjustments of the timing of the sleep�wake cycle could also be used to readjust the section position of the circadian oscillator. For example, sufferers with delayed section dysfunction can be suggested to delay the onset of sleep by 2 to 3 hours every day. After that, they need to maintain regular sleep�wake patterns, with publicity to brilliant mild in the morning. Modest quantities of coffee could maintain alertness early in the shift but must be avoided near the end of the shift. Traveling east advances the sleep�wake cycle and is typically harder than touring west (which delays the cycle). Jet lag could also be related to issue initiating or sustaining sleep or with daytime sleepiness, impaired efficiency and gastrointestinal disturbance after speedy transmeridian flights. Individuals older than 50 years appear to be more susceptible to jet lag than are younger individuals. Management Considerable research and theorizing are under method better to forestall and handle the problems related to jet lag. Some efforts earlier than departure could also be useful to forestall or ameliorate these problems. For individuals who plan to readjust their circadian clock to the new location, it could be attainable to transfer the sleep� wake and light�dark schedules appropriately earlier than departure. In addition, good sleep hygiene rules must be respected earlier than, throughout and after the journey. For example, many individuals are sleep disadvantaged or in alcohol withdrawal once they step on the airplane due to last-minute preparations or farewell events. Whereas enough fluid intake on the airplane is necessary to avoid dehydration, alcohol consumption must be avoided or minimized as a result of it causes diuresis and may disrupt sleep upkeep. On arriving at the destination, it could be preferable to try to maintain a schedule coinciding with actual residence time if the journey is going to be quick. For example, the person ought to try to sleep at instances that correspond to the usual bedtime or with the traditional midafternoon dip in alertness. In addition, a few of these protocols require avoidance of brilliant mild at certain instances, necessitating carrying dark goggles, for example, when touring. In addition to synchronizing the clock with the new environment, sleep and relaxation must be promoted by good sleep hygiene rules, by avoidance of extreme caffeine and alcohol and, probably, by administration of quick-length hypnotics. Care must be taken, however, to avoid hangover results or amnesia related to hypnotics. Shift Work Shift work problems happen when the circadian sleep�wake rhythm is in conflict with the remaining�activity cycle imposed by the externally determined work schedule. Different patterns embody rotating schedules and more or less permanent evening and night time schedules. Rotating schedules, notably rapidly shifting schedules, are tough as a result of constant readjustment of the endogenous circadian oscillator to the imposed sleep�wake cycle is necessary. In each rotating and shift work schedules, further difficulties are encountered as a result of the worker is normally anticipated to readjust to a standard sleep�wake cycle on weekends and holidays. Even if the worker can adjust his or her circadian system to the work schedule, he or she is then out of synchrony with the rhythm of household and friends throughout off-responsibility hours. These individuals, due to this fact, are continuously sleep disadvantaged and continuously sleepy. They endure impaired efficiency and elevated threat of accidents, somatic complaints and poor morale; hypnotics, stimulants and alcohol are used excessively in relationship to unusual or shifting work schedules. Shift work schedules could have played a task in human errors that contributed to the Three Mile Island and Chernobyl accidents and the Challenger catastrophe. Treatment No totally satisfactory methods currently exist for managing shift work problems. Because people vary in their capability to adjust to these schedules, self-choice or survival of the fittest could also be concerned for individuals who can find other employment or work schedules. Older individuals appear to be much less flexible than younger individuals in adjusting to shift work. Some experiments recommend that the rules of chronobiology could also be useful in reducing the human prices of shift work. For example, as a result of the endogenous pacemaker has a cycle size (tau) longer than 24 hours, rotating shift workers do better when their schedules transfer in a clockwise direction. The lengthened sleep�wake cycle of those sufferers in the natural environment is just like that of regular subjects residing in a time-free environment. The dysfunction seems to be comparatively frequent in sufferers with total blindness, as a result of they no longer understand visible Zeitgebers. Management could embody brilliant mild therapy in the morning to entrain the endogenous oscillator. Administration of vitamin B12 could also be helpful, maybe by enhancing the effectiveness of Zeitgebers. Circadian rhythm disturbances have to be differentiated from sleep-onset insomnia because of other causes (such as pain, caffeine consumption), early morning insomnia because of despair or alcohol use, and modifications in sleep patterns because of lifestyle or lifestyle modifications. Dorsiflexions of the big toe, ankle, knee and sometimes the hip are concerned (Table fifty nine. Patients could also be unaware of those pathological leg movements or arousals, though their mattress companions could also be all too aware of the kicking, frequent movements and restlessness. If these issues are strongly suspected, the patient ought to probably be referred to a sleep issues laboratory for analysis and an in a single day polysomnogram with tibial electromyograms. Diagnosis is made when the periodic limb movement index (number of leg jerks per hour of sleep) is 5 or greater, accompanied by arousals. The jerks happen primarily in the legs but may also appear in much less extreme types in the arms. The movements can be bilateral or unilateral and happen in stage 1 and stage 2 sleep. A associated disturbance, stressed legs syndrome, is related to unpleasant sensations in the lower legs, ft, or thighs that happen in a recumbent or resting position and cause an virtually irresistible urge to transfer the legs. Restless legs syndrome could also be frequent in sufferers with uremia and rheumatoid arthritis or in pregnant ladies. It has been advised that each conditions are familial, maybe because of an autosomal dominant gene. In the elderly, however, this condition is extraordinarily frequent; greater than 45% have no less than 5 leg kicks per hour of sleep. Some studies recommend that the movements arise subcortically from the brain or spinal cord; others recommend subclinical peripheral neuropathy.
Trusted norvasc 10mg
Sensitive, sympathetic, and accepting attitudes towards youngsters and fogeys by the hospital workers are very important. Health care suppliers must do not forget that mother and father have the most effective curiosity of their youngsters at coronary heart and know their youngsters the most effective. Whenever attainable, faculty assignments and tutoring for the hospitalized youngsters should be obtainable in order to have interaction the child intellectually and stop them from falling behind of their scholastic achievements. Anticipated deaths as a result of persistent illness may place a 1 vital pressure on a household, with frequent bouts of illness, hospitalization, disruption of normal residence life, absence of the sick father or mother, and perhaps more duties placed on the child. Additional strains embrace modifications in daily routines, monetary pressures, and the need to address aggressive treatment options. The stresses that a baby will face embrace visualizing the bodily deterioration of the family member, helplessness, and emotional liability. Forewarning the child that the family member may demonstrate bodily modifications, similar to appearing thinner or losing hair will assist the child to modify. Children of a dying father or mother may endure the lack of security and belief on the earth as a safe place, and the surviving father or mother could also be inclined to impose his or her own want for support and luxury onto the child. Sudden, surprising deaths result in more anxiousness and worry, as a result of there was no time for preparation and uncertainty as to explanations. Most bereaved families stay socially related and expect that life will return to some new, albeit completely different, sense of normalcy. The ache and suffering imposed by grief should by no means be automatically deemed "normal" and thus neglected or ignored. In more distressing reactions (similar to these seen in traumatic grief of sudden deaths), the pediatrician could also be a serious, first-line pressure in serving to youngsters and families tackle their loss. Hence, they flip to health care professionals more commonly for recommendation and support. Participation in the care of a child with a life-threatening or terminal illness is a profound experience. Inclusion of multiple disciplines, similar to hospice, clergy, nursing, ache service, child life, and social work, often helps to fully support families during this tough experience. Children have the right to know their diagnosis and should be informed early of their treatment. Parents may wish to be those to inform the child themselves, may select for the pediatric health care supplier to achieve this, or may do it in partnership with the pediatrician. A death, especially the death of a family member, is the most tough loss for a child. Many modifications in normal patterns of functioning may occur, together with lack of love and support from the deceased family member, a change in revenue, the attainable must relocate, much less emotional support from surviving members of the family, altering of routines, and a attainable change in standing from sibling to only child. Relationships between members of the family may turn into strained, and kids may blame themselves or different members of the family for the death of a father or mother or sibling. Bereaved youngsters may exhibit lots of the feelings mentioned earlier as a result of loss, along with behaviors of withdrawal into their very own world, sleep disturbances, nightmares, and signs similar to headache, abdominal pains, or presumably signs similar to these of the family member who has died. School age youngsters may exhibit nonspecific signs similar to headache, abdominal ache, chest ache, fatigue, and lack of vitality. Children and adolescents may also demonstrate enhanced anxiousness should these signs resemble these of the family member who died. The pediatrician should assist the household perceive this essential presence and encourage the protective functioning of the household unit. More frequent visits to the health care professional could also be necessary to tackle these signs and supply reassurance when applicable. Exposure to such disasters happens both instantly or indirectly, where the occasion is experienced through the media. However, youngsters and not using a personal loss watch as a means of participating in the occasion and should thus experience repetitive publicity to traumatic scenes and tales. The loss and devastation for a child who personally lives through a disaster is critical; the effect of the simultaneous incidence of disaster and personal loss complicates the bereavement process as grief reactions turn into interwoven with post-traumatic stress signs. After a death that happens on account of aggressive or traumatic circumstances, entry to skilled assist could also be required. Under circumstances of threat and worry, youngsters seek proximity to safe, steady, protective figures. Instead of the desired protective effect, nonetheless, the child receives the message that demonstrating grief or talking about death is wrong, leading her or him to really feel isolated, to grieve privately, or to delay grieving. Children must know that their mother and father love them and can proceed to protect them. A surviving sibling may really feel responsible just because he or she has survived, especially if the death was as a result of an accident that concerned both youngsters. Parents should be informed of this risk and inspired to discuss the likelihood with their youngsters. Despair, separation anxiousness, and detachment may occur on the withdrawal of nurturing caretakers. Young youngsters also categorical signs and signs of grief of their emotional states, similar to irritability or lethargy, and in severe instances, mutism. Preschool youngsters are in the preoperational cognitive stage, in which communication takes place through play and fantasy. In makes an attempt to master the finality and permanence of death, preschoolers incessantly ask unrelenting, repeated questions on when the person who died shall be returning. Parents and first care suppliers must concentrate on magical pondering and must reassure preschool youngsters that their ideas had nothing to do with the outcome. Children this age are sometimes frightened by extended, powerful expressions of grief by others. Children conceptualize occasions in the context of their very own experiential reality, and subsequently contemplate death by way of sleep, separation, and damage. Young youngsters categorical grief intermittently and present marked affective shifts over temporary periods. Information gathered from the media, friends, and fogeys varieties lasting impressions. Consequently, they could ask candid questions on death that adults will have issue addressing ("He should have been blown to pieces, huh Children 9 yr of age and older do perceive that death is irreversible and that it could involve them or their families. These youngsters are inclined to experience more anxiousness, overt signs of depression, and somatic complaints than do younger youngsters. Contact with the pediatrician may provide great reassurance, especially for the child with somatic signs, and notably when the death followed a medical illness. School and learning problems may also occur, and these reactions are sometimes linked to issue concentrating or preoccupation with the death. At 12-14 yr of age, youngsters begin to use symbolic pondering, reason abstractly, and analyze hypothetical, or "what if," situations systematically. Teenagers are sometimes ambivalent about dependence and independence and should withdraw emotionally from surviving members of the family, only to mourn in isolation. Adolescents begin to perceive complex physiologic systems in relationship to death. Fascination with dramatic, sensational, or romantic death generally happens and should find expression in copycat habits, similar to. Somatic expression of grief may revolve round extremely complex syndromes (eating problems or conversion reactions) as well as signs limited to the more immediate perceptions, as with younger youngsters (stomachaches). Quality of life takes on which means, and the teenager develops a focus on the longer term. Depression, resentment, temper swings, rage, and danger-taking behaviors can emerge as the adolescent seeks answers to questions of values, security, evil, and fairness. Alternately, the adolescent may seek philosophical or spiritual explanations ("being at peace") to ease their sense of loss. Families often battle with the way to inform their youngsters of the death of a family member. Children may be told that the particular person is "no longer residing" or "no longer moving or feeling.
Best 10 mg norvasc
Irrespective of their etiology, adverse emotional states, including frustration, anger, anxiousness, melancholy and tedium, have been shown to contribute to relapse in a substantial proportion of alcoholics. A number of medications have been employed to deal with comorbid psychiatric signs and problems in alcoholics. The use of those medications in alcoholics subsequently entails extra issues that may solely be arrived at through cautious psychiatric prognosis. Alcohol-sensitizing Drugs Medications similar to disulfiram or calcium carbimide trigger an disagreeable response when combined with alcohol. The efficacy of such drugs within the prevention or limitation of relapse in alcoholics has not been demonstrated. However, these drugs could also be of utility in chosen samples of alcoholics with whom particular efforts are made to guarantee compliance. More critical opposed results, similar to optic neuritis, peripheral neuropathy and hepatotoxicity are uncommon. The exacerbation of psychotic signs in sufferers with schizophrenia, and occasionally their look in other individuals as well as the event of melancholy, could also be linked to inhibition of the enzyme dopaminebeta-hydroxylase. As with its neuropathic results, the psychiatric results of disulfiram are unusual and may solely occur at higher dosages of the treatment. However, if a patient has not responded to other pharmacological therapies and is motivated to take disulfi ram, it could be useful. Treatment of Anxiety Symptoms/Disorders A number of research have shown chlordiazepoxide to be effective within the maintenance of alcoholics in lengthy-term outpatient treatment. Furthermore, the use of benzodiazepines could itself end in tolerance and dependence and may enhance depressive signs. Although this concern could also be exaggerated and all benzodiazepines will not be equal of their capacity to produce dependence in alcoholics the use of benzodiazepines in alcoholics is probably greatest restricted to detoxification. When combined with acceptable psychosocial treatment, buspirone seems useful within the treatment of alcoholics with persistent anxiousness. Currently, antipsychotics are indicated solely in alcoholics with a coexistent psychotic dysfunction or for the treatment of alcoholic hallucinosis. Several placebo-managed research have discovered no benefit in the use of phenothiazines for treatment of anxiety, pressure and melancholy following detoxification (Jaffe et al. Because of their capacity to decrease seizure threshold, antipsychotics should be used with caution on this population. Chapter 35 � Substance Abuse: Alcohol Use Disorders 427 Drugs that May Directly Reduce Alcohol Consumption A number of specific neurotransmitter methods have been implicated within the control of alcohol consumption, including endogenous opioids, catecholamines, especially dopamine and serotonin. Although these methods appear to operate interactively of their results on consuming behavior, efforts to use medications to deal with excessive consuming have more and more focused on agents which have selective results on specific neurotransmitter methods. Opioid Antagonists An extensive literature helps the function of opioidergic neurotransmission within the pathophysiology of alcohol consumption and associated phenomena. For instance, small doses of morphine enhance alcohol intake in experimental animals. In contrast, opioid antagonists, similar to naltrexone, lower ethanol consumption and self-administration. Effects similar to these in animals have been reported in some, but not all, research of naltrexone for the treatment of alcohol dependence (Kranzler and Van Kirk, 2001). The considerable variability in findings regarding the efficacy of naltrexone underscores the necessity to identify the circumstances beneath which the treatment exerts its therapeutic results. Naltrexone seems to produce a modest effect on consuming behavior among alcoholics. However, given the comparatively small general effect of the treatment, a variety of other components, including treatment compliance, the severity and chronicity of alcohol dependence, and the selection of concomitant psychotherapy, could determine whether an effect of the treatment is noticed. Further research is required with naltrexone to determine the optimum dosage, duration of treatment and psychosocial treatment methods with which to use the treatment. The query of whether the treatment is most efficacious for alcoholics with high levels of yearning for alcohol stays an important one. In contrast, ondansetron could also be useful in alcoholics with an early onset of drawback consuming. Prospective replication of this serotonergic matching strategy is required, nevertheless, before it can be beneficial for basic medical use. In contrast to this preclinical literature, data on the effects of serotonergic medications on human consuming behavior are more restricted, and the results are less constant. Together, research involving more than 4000 sufferers present constant proof of the efficacy of acamprosate in alcoholism rehabilitation (Kranzler and Van Kirk, 2001). Based on these findings, and the benign aspect-effect profile of the treatment, it seems to maintain considerable value for the treatment of alcohol dependence. Summary Considerable extra research is required before medications are likely to play a significant function within the postwithdrawal treatment of alcohol dependence. One at present useful strategy is the identification of comorbid psychopathology in alcoholics, with pharmacotherapy directed toward reducing both psychiatric signs and alcohol consumption. In addition, the opioid antagonist naltrexone, which is able to yielding a modest effect general in reducing consuming behavior, seems to be of contemplate- 428 Part V � Disorders Table 35. We admitted we have been powerless over alcohol � that our lives had turn into unmanageable. Made a decision to flip our will and our lives over to the care of God as we understood Him. Admitted to God, to ourselves, and to another human being the exact nature of our wrongs. Made an inventory of all individuals we had harmed, and became willing to make amends to them all. Made direct amends to such individuals wherever potential, besides when to accomplish that would injure them or others. Continued to take personal stock and when we have been wrong, promptly admitted it. Sought through prayer and meditation to enhance our conscious contact with God as we understood Him, praying only for information of His will for us and the ability to carry that out. Having had a spiritual awakening as the result of these steps, we tried to carry this message to alcoholics, and to follow these rules in all our affairs. The 12 Steps are reprinted with permission of Alcoholics Anonymous World Services, Inc. Demographic Features Adolescents Despite a paucity of managed, age-specific treatment outcome research of adolescents with alcohol use problems, the necessity for prevention and specialized treatment for this group is clear. However, several components have been related to higher treatment outcome: later onset of drawback consuming, pretreatment attendance at school, voluntary entrance into treatment, lively parental input and availability of ancillary adolescent-specific companies, including these pertaining to faculty, recreation, vocational wants and contraception. Furthermore, the clinician should contemplate the potential impact on treatment of other cognitive problems: learning disabilities, attention-deficit/hyperactivity dysfunction and other psychopathology which may beforehand have gone undiagnosed. Treatment of the adolescent with an alcohol use dysfunction additionally requires an appreciation of the importance of modeling, imitation and peer pressure, which are intrinsic to identity improvement. Geriatric Patients In addition to the high prevalence of medical problems, pharmacokinetic and pharmacodynamic variables can affect treatment outcome in aged alcoholics. For instance, Liskow and colleagues (1989) discovered that aged alcoholics, regardless of having drunk lower than younger sufferers through the month previous to admission, had more severe alcohol withdrawal symptomatology and required a higher dosage of chlordiazepoxide. These investigators speculated that the noticed variations might delay the entry of aged alcoholics into rehabilitation. An important query in treating aged alcoholics is the extent to which specialized treatment companies enhance outcome. Kofoed and colleagues (1987) discovered that sufferers handled in particular aged peer teams remained in treatment longer and have been more likely to complete treatment than these handled in mixedage teams. These investigators concluded that elder-specific treatment has differential therapeutic value. Special Features Influencing Treatment Psychiatric Comorbidity There is considerable proof that links the outcome of alcoholism treatment to comorbid psychopathology. General measures of psychopathology, as well as the precise diagnoses of drug abuse, drug dependence, delinquent character dysfunction and main depressive dysfunction have been shown to predict poorer outcomes in alcoholics. The extent to which treatment of concomitant psychopathology enhances alcoholism treatment outcome is unclear.
References:
- https://entsurrey.com/Download/ENT-SURREY/Dietary%20advice%20for%20Laryngopharyngeal%20Reflux.pdf
- https://cdn.ymaws.com/www.aocd.org/resource/resmgr/jaocd/2010nov.pdf
- https://www.bio.org/sites/default/files/legacy/bioorg/docs/Clinical%20Development%20Success%20Rates%202006-2015%20-%20BIO,%20Biomedtracker,%20Amplion%202016.pdf
- https://www.plannedparenthood.org/files/2613/9611/6275/History_of_BC_Methods.pdf
- https://pkdcure.org/wp-content/uploads/2020-Local-Walk-for-PKD-Sponsorship-packet.pdf