.png)
Buy 2.5mg xarelto
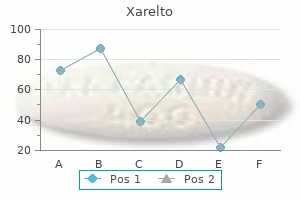
Article historical past: Received 24 December 2014 Received in revised kind 19 May 2015 Accepted 8 June 2015 Available online 15 June 2015 Keywords: Tendon Overuse harm Eccentric train Systematic review 1. Introduction Sport medication is changing into related, being tissue degeneration a common discovering in many of} sport-related tendon complaints. The danger will increase when high strength, repetitions, or exposure to vibrations during repetitive work are combined. Medina-Porqueres / Journal of Science and Medicine in Sport 19 (2016) 438453 439 discount of ache or in enchancment in the operate of sufferers with tendinopathies (e. Although most eccentric train research concerning tendinopathies has classically centered on the decrease extremity (specifically Achilles and patellar tendons), the higher extremity also warrants scrutiny because of the high incidence of tendon problems. The methodological high quality of each of the studies was assessed independently by two reviewers (M. Regarding score, 1 point was given if the item was achieved and 0 points if not, reaching a maximum of 10 points. For the aim of this review, consistency was outlined as related results between trials for a particular end result. In this review, since blinding the patient and/or treating therapist would have been unlikely, the cutoff for a high-quality trial was 5/10 or higher; 4/10 was established as average high quality and 3/10 or below as low high quality. For each continuous end result, between-group effect sizes had been reported with 95% confidence intervals. Other information obtained included group sizes and sociodemographic information (age, gender), size of symptoms, dominance in accordance with tendinopathy, previous treatments, and follow-up post-treatment. Blinding of the assessors and concealed allocation had been two different standards that was poorly reported in a lot of the selected studies. Medina-Porqueres / Journal of Science and Medicine in Sport 19 (2016) 438453 Svernlцv et al. Medina-Porqueres / Journal of Science and Medicine in Sport 19 (2016) 438453 Maenhout et al. Each contraction lasted roughly four s Subjects sitting on a chair, forearm pronated on the armrest or on an adjoining table, holding the deal with of the plastic water can with a clenched fist in pronation and the container hanging freely in entrance of the armchair or below the tabletop. To strengthen the flexors of the shoulder, the patient was positioned with his or her back to the equipment and the elbow flexed at ninety, performing the flexion motion from 0 to ninety. For the extensors, the patient confronted the equipment with the elbow flexed at forty five and the shoulder at 60 of flexion and 30 of extension. For the medial and lateral rotators, the patient was positioned alongside the equipment with the elbow flexed at ninety: for the medial rotation, the patient started at forty five of lateral rotation and moved to forty five of medial rotation; for the lateral rotation, the patient began at forty five of medial rotation and moved to three of lateral rotation. The velocity of motion was 2 s for each the eccentric and concentric phases Experimental group programme: 1-Warm-up of the forearm extensors and flexors with wrist actions without any load (23 min) 2-Static stretch (1530 s, 35 times) 3-Eccentric exercises of the forearm extensors muscular tissues (10 s). Subject in sitting position, elbow in ninety of flexion resting on a table, holding the dumbbell over the edge of the table 4-Static stretch, as prior to train. In addition, the topics used an elbow band (counterforce brace) during exercise and a wrist help at night time Subjects in sitting position, with full elbow extension, forearm pronation and maximum wrist extension. From this position, the patient slowly lowered wrist into flexion for a count of 30, utilizing the contralateral hand to return the wrist to maximum extension. Patients had been instructed to proceed the train even after they experienced mild discomfort and to stop it if the ache worsened and become disabling Subjects carried out a full can (thumb up) abduction in the scapular plane with a dumbbell weight at a velocity of 5 s/repetition, twice a day. Starting position of the eccentric section at full scapular abduction needed to be ache free and, if not, sufferers had been advised to stretch out the arm at a slightly decrease diploma of scapular abduction Frequency per week 1. Medina-Porqueres / Journal of Science and Medicine in Sport 19 (2016) 438453 Lombardi et al. The train was interrupted if the patient felt ache and carried out another motion Svernlцv et al. After completion of an train session, elevated ache needed to revert to levels before train before the next With the elbow flexed 70, topics seated on a chair with the forearm pronated resting on a table, with the wrist and hand over the edge and holding a bucket of water. They had been instructed to place the non-affected hand over the one holding the bucket and slowly raise it with the non-affected hand, thus avoiding the concentric section in the affected arm. With the affected hand prolonged, the topics eliminated the unaffected hand slowly and then, counting to three, lowered the hand to trigger a flexion hand motion. They had been informed to adjust their resisted weight so that they had been carry out the prescribed repetitions during pain-free intervals and, if not, the burden can be decreased Subjects in a sitting position, elbow flexed, and forearm pronated resting on the thigh, with the hand hanging over the knee, holding the resistance band, which was fixed on the floor with the ipsilateral foot. With the non-affected hand, subject pulled up the band, lengthening it, so as to to} make it lax and permit the affected hand to carry out a wrist extension. Then, the band was slowly lowered from full wrist extension to full wrist flexion 7 2times/day the primary 8 weeks, 1time/day from week 8 to 12 12 three 15 the exercises had been individually adjusted and progressed with elevated external load through the use of weights and elastic rubber band at the physiotherapist visits as soon as} every different week during the entire rehabilitation interval. Medina-Porqueres / Journal of Science and Medicine in Sport 19 (2016) 438453 Sцderberg et al. The size of the band was adjusted so that it was considerably troublesome to carry out 10 repetitions. During the preliminary trial, the size of the band was marked with a everlasting ink marker to keep away from variability of resistance between sessions. Those who carried out the repetitions simply without rising ache, resistance was elevated by shortening the band in 1-inch increments from the preliminary size mark Initial resistance utilized by the non-affected hand needed to be bearable during three sets of 15 repetitions. Subjects had been requested to rapidly transfer in the desired path and consequently slowly returning to the starting position. From this position, they slowly lowered the wrist to flexion, counting to 30, utilizing the other hand to return the affected to the starting 2 (first 2 weeks) and 1 (for 12 weeks) 14 three 15 Struyf et al. Medina-Porqueres / Journal of Science and Medicine in Sport 19 (2016) 438453. The 12 selected studies included a complete of 668 participants with medical diagnoses of epicondylar tendinopathy (n = 355)3037 or shoulder impingement (n = 191). Table 1 gathers the results of the 12 studies included in this systematic revision. In eleven studies,3040 ache decreased considerably in the group the place eccentric work was employed as therapeutic modality (p < 0. In the second examine,forty one within-group adjustments had been reasonably higher for the non-eccentric group (manual mobilizations, stretching, motor control training), not being important in the eccentric group; concerning inter-group adjustments, they had been considerably higher in the non-eccentric group in one out of the three evaluated exams (significant in Neer take a look at, not in Hawkins and empty can tests). Strength was assessed a special way|in another way} in 9 studies,3032,3437,39,forty one distinguishing: strength,30,31 grip strength,32,36 isometric strength,39,forty one pain-free grip strength,34,35,37 and pain-free isometric strength. Significant within-group enhancements had been observed in the eccentric group during wrist extension and mixture strength (p < 0. The adjustments discovered by Peterson31 had been considerably higher in the eccentric group, each within-group and inter-group (p < 0. Svernlцv32 discovered enhancements considerably higher in the eccentric group, each within-group and inter-group (p < 0. Concerning pain-free grip strength, the three studies34,35,37 showed important within-group adjustments in the eccentric group (p < 0. Eccentric train regimens might vary from one examine to another looking for for the most effective outcome. Table 2 lists the therapy variables utilized by authors treating impingement and epicondylar tendinopathy. The most common therapy protocol among these studies was established by Alfredson,forty two which consisted of three sets of 15 repetitions carried out twice daily. The complete number of repetitions per train never exceeded the unique forty five, twice a day, by Alfredson. Discussion Our systematic revision centered on the examine and search for evidence concerning the effectiveness of the eccentric exercises for the therapy of higher limb tendinopathies. The major discovering was the existence of randomized trials just for two tendinopathies: shoulder impingement and epicondylar tendinopathy. In a lot of the studies, the number of included participants was sufficient, which was previously decided by statistical estimations. Struyf41 included 20 participants, although a minimal of forty six participants was estimated as essential to be important; nonetheless, the ability of the examine was robust sufficient (80%). This might influence much more in these short-term studies, during which the length constitutes a limitation itself, in all probability conditioning the improvement of the tendinopathy. Martinez-Silvestrini35 developed a 6-week examine with no post-treatment follow-up; regardless of each teams improved considerably, no inter-group adjustments had been discovered, in all probability the short length of the examine interval. Nagrale37 developed a 4week follow-up, perhaps inadequate the short length of the examine interval (4 weeks). All of this, along with the attribute "vicious cycle" of the tendon harm,forty two might restrict significantly the collection of faithful and closer information to the tendinopathy actuality.
Proven 2.5mg xarelto
In some instances, vomiting turns into a aim in itself, and the person will binge eat in order to to} vomit or will vomit after consuming a small amount of meals. Individuals with bulimia nervosa might use a variety of|quite so much of|a wide selection of} strategies to induce vomiting, includ ing the use of of} fingers or devices to stimulate the gag reflex. Individuals typically turn into adept at inducing vomiting and are eventually capable of to} vomit at will. Individuals with bulimia nervosa might misuse enemas following epi sodes of binge consuming, however this is seldom the only real} compensatory technique employed. Individ uals with this dysfunction might take thyroid hormone in an try and avoid weight achieve. Individuals with diabetes mellitus and bulimia nervosa might omit or reduce insulin doses in order to to} reduce the metabolism of meals consumed throughout consuming binges. Individuals with bulimia nervosa might quick for a day or extra or train excessively in an try and forestall weight achieve. Exercise additionally be} thought-about extreme when it significantly interferes with im portant activities, when it happens at inappropriate instances or in inappropriate settings, or when the person continues to train regardless of damage or other medical problems. Individuals with bulimia nervosa place an extreme emphasis on physique shape or weight in their self-evaluation, and these factors are typically extremely necessary in figuring out self-esteem (Criterion D). Individuals with this dysfunction might carefully resemble those w^ith anorexia nervosa in their worry of gaining weight, in their desire to lose weight, and in the stage of dissatisfaction with their our bodies. Between consuming binges, people with bulimia ner vosa typically prohibit their complete caloric consumption and preferentially choose low-calorie ("diet") meals whereas avoiding meals that they understand to be fattening or probably to|prone to} trigger a binge. The fluid and electrolyte disturbances resulting from the purging conduct are sometimes sufficiently severe to represent med ically severe problems. Rare however probably fatal problems embody esophageal tears, gastric rupture, and cardiac arrhythmias. Serious cardiac and skeletal myopathies have been reported amongst people following repeated use of syrup of ipecac to induce vom iting. Individuals who chronically abuse laxatives might turn into depending on their use to stimulate bowel actions. Gastrointestinal symptoms are commonly related to bulimia nervosa, and rectal prolapse has also been reported amongst people with this dysfunction. Prevalence Twelve-month prevalence of bulimia nervosa amongst young females is 1%-1. Point prevalence is highest amongst young adults because the that} dysfunction peaks in older adolescence and young maturity. Development and Course Bulimia nervosa commonly begins in adolescence or young maturity. The binge consuming regularly begins throughout or after an episode of dieting to lose weight. Experiencing multiple of} stressful life occasions also can pre cipitate onset of bulimia nervosa. Disturbed consuming conduct persists for a minimum of|no less than} quantity of} years in a excessive proportion of clinic samples. The course additionally be} chronic or intermittent, with periods of remission alternating with recurrences of binge consuming. However, over longer-term follow-up, the symptoms of many people appear to diminish with or with out therapy, though therapy clearly impacts end result. Periods of remission longer than 1 year are related to better long-term end result. Significantly elevated risk for mortality (all-cause and suicide) has been reported for people with bulimia nervosa. Diagnostic cross-over from initial bulimia nervosa to anorexia nervosa happens in a mi nority of instances (10%-15%). Individuals who do experience cross-over to anorexia nervosa commonly will revert again to bulimia nervosa or have multiple of} occurrences of cross-overs between these problems. A subset of individuals with bulimia nervosa proceed to binge eat however now not interact in inappropriate compensatory behaviors, and due to this fact their symptoms meet criteria for binge-eating dysfunction or other specified consuming dysfunction. Weight considerations, low self-esteem, depressive symptoms, social anxi ety dysfunction, and overanxious dysfunction of childhood are related to elevated risk for the development of bulimia nervosa. Internalization of a thin physique ideal has been found to enhance risk for developing weight considerations, which in turn enhance risk for the development of bulimia nervosa. Individuals who skilled childhood sexual or physical abuse are at elevated risk for developing bulimia nervosa. Childhood obesity and early pubertal maturation enhance risk for bulimia nervosa. Familial transmission of bulimia nervosa additionally be} present, as well as|in addition to} genetic vulnerabilities for the dysfunction. Severity of psychiatric comorbidity predicts worse long-term end result of bulimia nervosa. Culture-Related Diagnostic issues Bulimia nervosa has been reported to occur with roughly related frequencies in most in dustrialized international locations, including the United States, Canada, many European international locations, Australia, Japan, New Zealand, and South Africa. In scientific research of bulimia nervosa in the United States, people presenting with this dysfunction are primarily white. However, the dysfunction also happens in other ethnic groups and with prevalence corresponding to esti mated prevalences observed in white samples. Gender-Related Diagnostic issues Bulimia nervosa is much extra frequent in females than in males. However, quantity of} labora tory abnormalities might occur as a consequence of purging and will enhance diagnostic certainty. These embody fluid and electrolyte abnormalities, corresponding to hypokalemia (which can provoke cardiac arrhythmias), hypochloremia, and hyponatremia. The loss of gastric acid via vomiting might produce a metabolic alkalosis (elevated serum bicarbonate), and the frequent induction of diarrhea or dehydration via laxative and diuretic abuse can cause metabolic acidosis. Some people with bulimia nervosa exhibit mildly ele vated ranges of serum amylase, most likely reflecting an increase in the salivary isoenzyme. However, inspection of the mouth might reveal vital and permanent loss of dental enamel, particularly from lin gual surfaces of the front tooth as a result of} recurrent vomiting. In some people, the salivary glands, significantly the parotid glands, might turn into notably enlarged. Individuals who induce vomiting by manually stimulating the gag reflex might develop calluses or scars on the dorsal surface of the hand from re peated contact with the tooth. Serious cardiac and skeletal myopathies have been reported amongst people following repeated use of syrup of ipecac to induce vomiting. Comprehensive analysis of individuals with this dysfunction should embody evaluation of suicide-related ideation and behaviors as well as|in addition to} other risk factors for suicide, including a history of suicide attempts. Functional Consequences of Buiimia Nervosa Individuals with bulimia nervosa might exhibit a variety of practical limitations related to the dysfunction. A minority of individuals report severe position impairment, with the so cial-life domain more than likely to be adversely affected by bulimia nervosa. For people with an initial prognosis of anorexia nervosa who binge and purge however whose presentation now not meets the complete criteria for anorexia nervosa, binge-eating/purging sort (e. If the cri teria for each borderline persona dysfunction and bulimia nervosa are met, each diagnoses should be given. Comorbidity Comorbidity with mental problems is frequent in people with bulimia nervosa, with most experiencing a minimum of|no less than} one other mental dysfunction and many of|and a lot of} experiencing multiple of} co morbidities. In many people, the mood disturbance begins the identical time as|concurrently|simultaneously} or following the development of bulimia nervosa, and individ uals often ascribe their mood disturbances to the bulimia nervosa. However, in some in dividuals, the mood disturbance clearly precedes the development of bulimia nervosa. These mood and anxiousness disturbances regularly remit follow ing effective therapy of the bulimia nervosa. The lifetime prevalence of substance use, significantly alcohol or stimulant use, is a minimum of|no less than} 30% amongst people with bulimia ner vosa. A substan tial proportion of individuals with bulimia nervosa even have persona features that meet criteria for one or more of} persona problems, most regularly borderline persona dysfunction.
| Comparative prices of Xarelto | ||
| # | Retailer | Average price |
| 1 | Starbucks | 713 |
| 2 | YUM! Brands | 889 |
| 3 | Burlington Coat Factory | 264 |
| 4 | Ruddick Corp. | 679 |
| 5 | J.C. Penney | 1000 |
Quality 20 mg xarelto
The lines and extent of the resection could be depicted on preprinted adhesive labels and attached to the surgical pathology request forms. Perineural Invasion Traditionally, the presence of perineural invasion (neurotropism) is an important predictor of poor prognosis in 21 head and neck most cancers of nearly all sites. The presence of perineural invasion (neurotropism) in the main most cancers is associated with poor local disease management and regional management, as well as|in addition to} being associated with 21 metastasis to regional lymph nodes. Further, perineural invasion is associated with decrease in disease-specific 21 survival and general survival. There is conflicting data relative to an affiliation between the presence of perineural invasion and the event of distant metastasis, with some studies showing an elevated 21 affiliation with distant metastasis, while other studies showing no correlation with distant metastasis. The 22 relationship between perineural invasion and prognosis is independent of nerve diameter. Additionally, rising 23 proof suggests that extratumoral perineural invasion may be be} more prognostically related. Aside from the impact on prognosis, the presence of perineural invasion additionally guides remedy. Concurrent adjuvant chemoradiation remedy has been shown to enhance outcomes in sufferers with perineural invasion (as nicely as in 24,25 Given the importance relative to prognosis and sufferers with extranodal extension and bone invasion). Lymph Nodes Measurement of Tumor Metastasis the cross-sectional diameter of the biggest lymph node metastasis (not the lymph node itself) is measured in the gross specimen at the time of macroscopic examination or, if essential, on the histologic slide at the time of 24,25 microscopic examination. Special Procedures for Lymph Nodes the danger of regional (cervical neck) nodal spread from cancers varies based mostly on anatomic subsite. At the current time, no extra special techniques are required aside from routine histology for the assessment of nodal metastases. In reality, rare studies related to head and neck sites indicate that isolated tumor cells may actually be a poor prognosticator in terms of|when it comes to|by method of} 28 local management. Lymph Node Number Histologic examination of a selective neck dissection specimen will ordinarily include 6 or more lymph nodes. Histologic examination of a radical or modified radical neck dissection specimen will ordinarily include 10 or more lymph nodes in the untreated neck. Modified radical neck dissection, inner jugular vein and/or sternocleidomastoid muscle spared 3. Extended radical neck dissection, as specified by the surgeon For functions of pathologic evaluation, lymph nodes are organized by ranges as shown in Figure 4. In order for pathologists to correctly identify these nodes, they must be acquainted with the terminology of the regional lymph node groups and with the relationships of those groups to the regional anatomy. Which lymph node groups surgeons submit for histopathologic evaluation decided by} kind of|the kind of} neck dissection they perform. Therefore, surgeons should supply info on the forms of neck dissections that they perform and the details points} of the local anatomy in the specimens they submit for examination or, in other manners, orient those specimens for pathologists. The submandibular gland is included in the specimen when the lymph nodes inside this triangle are eliminated. The posterior boundary is the posterior border of the sternocleidomastoid muscle, and the anterior boundary is the lateral border of the stylohyoid muscle. Middle Jugular Group Lymph nodes located across the middle third of the internal jugular vein extending from the carotid bifurcation superiorly to the omohyoid muscle (surgical landmark), or cricothyroid notch (clinical landmark) inferiorly. Lower Jugular Group Lymph nodes located across the decrease third of the internal jugular vein extending from the omohyoid muscle superiorly to the clavicle inferiorly. The posterior boundary is the posterior border of the sternocleidomastoid muscle, and the anterior boundary is the lateral border of the sternohyoid muscle. The posterior boundary of the posterior triangle is the anterior border of the trapezius muscle, the anterior boundary of the posterior triangle is the posterior border of the sternocleidomastoid muscle, and the inferior boundary of the posterior triangle is the clavicle. Anterior (Central) Compartment Lymph nodes on this compartment include the pre- and paratracheal nodes, precricoid (Delphian) node, and the perithyroidal nodes, including the lymph nodes alongside the recurrent laryngeal nerve. The superior boundary is the hyoid bone, the inferior boundary is the suprasternal notch, the lateral boundaries are the common carotid arteries, and the posterior boundary by the prevertebral fascia. Lymph node groups removed from areas not included in the above ranges, eg, scalene, suboccipital, and retropharyngeal, must be recognized and reported from all ranges separately. Extranodal Extension the status of cervical lymph nodes is the single most necessary prognostic consider aerodigestive most cancers. All macroscopically adverse or equivocal lymph nodes must be submitted in toto. Grossly positive nodes may be be} partially submitted for microscopic documentation of metastasis. This discovering consists of extension of metastatic tumor, present throughout the confines of the lymph node, by way of the lymph node capsule into the surrounding connective tissue, with or without related stromal response. Approximately two-thirds of mucosal melanomas arise in the sinonasal tract, one-quarter are found in the oral cavity, and the remainder happen solely sporadically in other mucosal sites of the top and neck. To reflect this aggressive conduct, main cancers limited to the mucosa are thought-about T3 lesions. The anatomic extent standards to outline reasonably superior (T4a) and really superior (T4b) disease are given under. Pathologic staging is normally carried out after surgical resection of the first tumor. Pathologic staging decided by} pathologic documentation of the anatomic extent of disease, whether or not or not the first tumor has been utterly eliminated. The "y" prefix indicates those instances during which classification is carried out throughout or following initial multimodality remedy (ie, neoadjuvant chemotherapy, radiation remedy, or both chemotherapy and radiation therapy). Additional Descriptors Residual Tumor (R) Tumor remaining in a patient after remedy with healing intent (eg, surgical resection for cure) is categorized by a system recognized as|often identified as} R classification, shown under. For the pathologist, the R classification is related to the status of the margins of a surgical resection specimen. That is, tumor involving the resection margin on pathologic examination may be be} assumed to correspond to residual tumor in the patient and may be be} classified as macroscopic or microscopic based on the findings at the specimen margin(s). Normal vocal cord mobility (T1), fixation of the larynx (T2), and vocal cord fixation (T3) might solely be determined clinically. Normal vocal cord mobility (T1), impaired vocal cord mobility (T2), and vocal cord fixation (T3) might solely be determined clinically. Normal or impaired vocal cord mobility (T2) and vocal cord fixation (T3) might solely be determined clinically. Hyperplasias and keratoses without atypia as well as|in addition to} those with mild dysplasia are categorized as "low grade," while lesions with reasonable and severe dysplasia as well as|in addition to} carcinoma 20 in situ are thought-about "excessive grade. Morphologic standards for the classification of laryngeal precursor lesions are summarized under. World Health Organization Classification of Tumours: Pathology and Genetics of Head and Neck Tumours. Mucoepidermoid carcinoma: a clinicopathologic study of 80 sufferers with special reference to histological grading. Oral squamous cell carcinoma: histologic danger assessment, however not margin status, is strongly predictive of local disease-free and general survival. Laser surgical procedure for early glottic most cancers: impact of margin status on local management and organ preservation. A novel classification system for perineural invasion in noncutaneous head and neck squamous cell carcinoma: histologic subcategories and patient outcomes. Classification of isolated tumor cells: clarification of the 6th edition of the American Joint Committee on Cancer Staging Manual. Occult metastases detected by sentinel node biopsy in sufferers with early oral and oropharyngeal squamous cell carcinomas: Impact on survival. Primary tumor staging for oral most cancers and a proposed modification incorporating depth of invasion: an international multicenter retrospective study. Minimum nodal yield in oral squamous cell carcinoma: defining the usual of care in a multicenter international pooled validation study. Extent of pathologic extracapsular extension and outcomes in sufferers with nonoropharyngeal head and neck most cancers treated with initial surgical resection. Soft tissue deposits in neck dissections of sufferers with head and neck squamous cell carcinoma: potential analysis of prevalence, survival, and its implications.
Order 2.5 mg xarelto
Such complaints are more frequent among males in Asian populations than in males residing in Europe, Australia, or the United States. This variation could also be} attributable to cultural or genetic differences between cultures. Functional Consequences of Delayed Ejaculation Difficulty with ejaculation may contribute to difficulties in conception. Delayed ejacula tion is often related to appreciable psychological misery in one or each partners. The major differential prognosis is between delayed ejacu lation absolutely defined by another medical sickness or damage and delayed ejaculation with a psychogenic, idiopathic, or mixed psychological and medical etiology. A situational facet to the criticism is suggestive of a psychological foundation for the problem (e. Another medical sickness or damage may produce delays in ejaculation independent of psychological points. For example, inability to ejaculate could be caused by interruption of the nerve supply to the genitals, corresponding to can occur after traumatic surgical damage to the lumbar sympathetic ganglia, abdominoperitoneal surgery, or lumbar sympathectomy. Ejaculation is believed to be underneath autonomic nervous system control involving the hypo gastric (sympathetic) and pudendal (parasympathetic) nerves. A variety of neurodegenerative diseases, corresponding to quantity of} sclerosis and diabetic and alcoholic neuropathy, can cause inability to ejaculate. Delayed ejaculation wants to|must also} be differentiated from retro grade ejaculation. A variety of pharmacological agents, corresponding to antidepres sants, antipsychotics, alpha sympathetic medicine, and opioid medicine, can cause ejaculatory issues. It is essential in the history to verify whether the com plaint considerations delayed ejaculation or the sensation of orgasm, or each. Ejaculation occurs in the genitals, whereas the experience of orgasm is believed to be primarily subjective. For example, a person with a standard ejaculatory sample may complain of decreased pleasure. Comorbidity There is some evidence to counsel that delayed ejaculation could also be} more frequent in severe forms of major depressive disorder. At least one of the three following signs should be experienced on virtually all or all (approximately 75%-100%) occasions of sexual activity (in recognized situational con texts or, if generalized, in all contexts): 1. Marked issue in maintaining an erection until the completion of sexual activity. Specify whether: Lifelong: the disturbance has been present the rationale that} individual turned sexually ac tive. Specify whether: Generaiized: Not limited to sure kinds of stimulation, conditions, or partners. Situationai: Only occurs with sure kinds of stimulation, conditions, or partners. Diagnostic Features the important feature of erectile disorder is the repeated failure to obtain or maintain erec tions throughout partnered sexual activities (Criterion A). A cautious sexual history is necessary to verify that the problem has been present for a big duration of time. Symptoms may occur solely in specific conditions involving sure kinds of stimulation or partners, or they could occur in a generalized manner in all kinds of situa tions, stimulation, or partners. Associated Features Supporting Diagnosis Many males with erectile disorder may have low vanity, low self-confidence, and a de creased sense of masculinity, and may experience depressed have an effect on}. In addition to the subtypes "lifelong/acquired" and "generalized/situational," the fol lowing five components should be thought of throughout assessment and prognosis of erectile disorder given that that} they could be related to etiology and/or therapy: 1) companion components (e. Each of these components may con tribute differentiy to the presenting signs of different males with this disorder. Prevalence the prevalence of lifelong versus acquired erectile disorder is unknown. There is a robust age-related increase in each prevalence and incidence of issues with erection, particu larly after age 50 years. Approximately 13%-21% of males ages 40-80 years complain of oc casional issues with erections. Approximately 2% of males younger than age 40-50 years complain of frequent issues with erections, whereas 40%-50% of males older than 60-70 years may have important issues with erections. About 20% of males concern erectile prob lems on their first sexual experience, whereas approximately eight experienced erectile prob % lems that hindered penetration throughout their first sexual experience. Deveiopment and Course Erectile failure on first sexual try has been discovered to be associated to having intercourse with a beforehand unknown companion, concomitant use of medication or alcohol, not desirous to have intercourse, and peer pressure. There is minimal evi-2t most of these issues spontaneously re mit without skilled intervention, but some males may continue to have episodic prob lems. In distinction, acquired erectile disorder is often related to organic components corresponding to diabetes and cardiovascular disease. Clinical statement sup ports the association of lifelong erectile disorder with psychological components would possibly be} self- limiting or aware of psychological interventions, whereas, as noted above, acquired erectile disorder is more doubtless to|prone to} be associated to organic components and to be persistent. A minority of males recognized as having moderate erectile failure may experience spontaneous remission of signs without medical intervention. Distress related to erectile disorder is lower in older males as in contrast with younger males. Neurotic personality traits could also be} related to erectile issues in col lege college students, and submissive personality traits could also be} related to erectile issues in males age 40 years and older. Erectile issues are frequent in males recognized with despair and posttraumatic stress disorder. Risk components for acquired erectile disorder include age, smoking to bacco, lack of physical train, diabetes, and decreased need. Culture-Reiated Diagnostic points Complaints of erectile disorder have been discovered to vary across nations. It is unclear to what extent these differences characterize differences in cultural expectations as opposed to real differences in the frequency of erectile failure. Diagnostic iViarlcers Nocturnal penile tumescence testing and measured erectile turgidity throughout sleep could be employed to help differentiate natural from psychogenic erectile issues on the as sumption that sufficient erections throughout speedy eye motion sleep indicate a psycholog ical etiology to the problem. Doppler ultrasonography and intravascular injection of vasoactive medicine, properly as|in addition to} invasive diagnostic procedures corresponding to dynamic infusion cavernosography, can be utilized to assess vascular integrity. Pudendal nerve conduction studies, together with somatosensory evoked potentials, could be employed when a peripheral neuropathy is suspected. In males additionally complaining of decreased sexual need, serum bioavailable or free testosterone is frequently assessed to decide if the problem is secondary to endocrinological components. Determination of fasting serum glucose is beneficial to display screen for the presence of diabetes mel litus. The assessment of serum lipids is essential, as erectile disorder in males 40 years and older is predictive of the longer term run} threat of coronary artery illness. Functionai Consequences of Erectiie Disorder Erectile disorder can intrude with fertility and produce each individual and interpersonal misery. Fear and/or avoidance of sexual encounters may intrude with the flexibility to de velop intimate relationships. Major depressive disorder and erectile disorder are intently associated, and erectile disorder accompanying severe depressive disorder may occur. The differential ought to include consideration of normal erec tile perform in males with excessive expectations. Another major differential prognosis the erectile problem is secondary to substance/medication use. An onset that coincides with the be ginning of substance/medication use and that dissipates with discontinuation of the sub stance/medication or dose reduction is suggestive of a substance/medication-induced sexual dysfunction. The most difficult facet of the differential prognosis of erec tile disorder is ruling out erectile issues would possibly be} absolutely defined by medical components. The distinction between erectile disorder as a mental disorder and erectile dysfunction as outcome of|the outcomes of} another medical con dition is often unclear, and many of|and lots of} circumstances may have complex, interactive organic and psy chiatric etiologies. If the person is older than 40-50 years and/or has concomitant medical issues, the differential prognosis ought to include medical etiologies, especially vascular illness. For example, a person with diabetes mellitus can develop erectile disorder in response to psychological stress.
Trusted 20 mg xarelto
These research additionally present that the prevalence of Legionella in a water distribution system correlates to a big degree with the water temperature - isolation charges are highest in heat water systems, significantly within a temperature range of 2550 °C. Starlinger & Tiefenbrunner (1996) additionally showed a constructive correlation between the presence of Legionella and amoebae in some installations. Hot and cold-water systems on ships have additionally been implicated in a number of|numerous|a selection of} outbreaks. Water samples taken from the hot-water system at bathe heads have been contaminated with legionellae. The ship was unable to maintain safe temperatures in each scorching and cold-water systems, and the chlorine dosing system on board the ship was not working effectively (Arthur, 1998). Hot tubs and leisure pools - risk elements Hot tubs are put in on many cruise ships and on some ferries. The dangers are much like these on land (see Chapter 8), and there have been quantity of} outbreaks on ships as a result of} scorching tubs. Passengers spending time across the scorching tub, however not in the water, have been additionally significantly more probably to|prone to} have acquired an infection. In 2003, there were eight instances and one death among passengers who had been on a cruise round Iceland. This latter outbreak demonstrates the importance of worldwide collaboration to investigate shipborne outbreaks, the explanation that} instances have been detected and investigated in Germany after the vessel had docked there to disembark passengers, and it was investigated in its next port of name, in the United Kingdom. In 1984, a big outbreak on a cruise ship occurred after the air-conditioning was turned on at Bordeaux, France. No widespread supply was found, but the epidemic curve indicated that the air-conditioning system contributed in some way to the outbreak (Rowbotham, 1998). In one other outbreak on a cruise ship in 1984, no supply was identified, but the outbreak investigation revealed problems with the air dealing with units (Christenson et al. The steps involved in monitoring, some of which are mentioned below, are to: · determine management measures (Section 7. Hot and cold-water systems - management measures Primary and secondary methods of prevention and management, as utilized to resorts, are primarily based on experience acquired in managing outbreaks and are largely empirical. The efficacy of these measures in the management and secondary prevention of outbreaks is properly established, although they may be insufficient in resorts repeatedly related to instances. An instance of a guidelines specifically designed for water systems in resorts is provided in Appendix 1. In ships, onboard publicity by way of piped water can be prevented by such water high quality management measures as: · treating supply water (where the water is non-potable) · maintaining water temperatures outside the range by which Legionella proliferates (2550 єC) · maintaining disinfection residuals greater than 0. Water circulate in the distribution system wants to|must also} be maintained in periods of reduced activity. Disinfection - management measures A study of sixty two resorts in the Balearic Islands, Spain (Crespi et al. Another study evaluated the systematic purging of the new and cold-water pipes in two resorts with water chlorinated at 11. Temperature - management measures Some buildings might not ready to|be capable of|have the flexibility to} raise their hot-water temperature sufficiently to management Legionella progress; subsequently, an on-line remedy such as chlorine or copper/silver ionization must be thought-about. Chapter 4 has more data on management measures referring to temperature in distribution systems. Design, operation and maintenance - management measures the management of Legionella in water distribution systems in resorts is difficult, and requires the continual and effective maintenance of preventive measures. Hotel personnel liable for the maintenance of resort water systems must be educated and qualified to carry out these duties. The importance of coaching and schooling has been acknowledged in massive quantity of|numerous|a lot of} published preventive guides. Data from the appliance of coaching programmes are very encouraging, and suggest that schooling important in preventing legionellosis in the tourist sector (Crespi & Ferra, 2002). Preventing the risk of colonization throughout restore of the plumbing systems on ships deserves special attention. Air-conditioning - management measures Humidifers or gadgets probably to|prone to} amplify or disseminate the bacteria must be periodically cleaned and changed (Edelstein & Cetron, 1999). Special attention must be paid to the proliferation of Legionella in humidifiers. If a supply of Legionella transmission is identified, particularly after an outbreak, a disinfecting procedure (superheating or hyperchlorination) is beneficial. As the incubation period of the illness might be be} longer than the length of a cruise, outbreaks might go undetected, even when the ship has a surveillance system in place. Routine surveillance by exterior authorities, such as by way of public well being inspections of ships by environmental well being officers, wants to|must also} be conducted, to pre-empt illness outbreaks. Today, there proceed to be reviews of outbreaks of infectious illness linked to swimming pools, however these can be averted by: · good pool management, including sufficient filtration and disinfection · bathers observing advice to bathe earlier than coming into pools · bathers refraining from bathing if unwell with diarrhoeal illness. Immersion in water can be each pleasant and therapeutic, and varied methods have been used over centuries for a various range of physiological effects, such as therapeutic accidents, reducing swelling and cooling burns, and for psychological effects, such as calming psychiatric patients (de Jong, 1997). Types of pools Swmmng pools Swimming pools provided with contemporary (surface or ground), marine or thermal water. In phrases of construction, the traditional pool is usually referred to as the primary, public or municipal pool. In addition, there are lots of|there are numerous} specialist pools for a specific consumer sort - for instance, paddling pools, learner or teaching pools, diving pools and pools with special options such as "flumes" or water slides. Plunge pools Plunge pools are typically utilized in association with saunas, steam rooms or scorching tubs, and are designed to cool users by immersion in unheated water. They domestic, semi-public or public, and located indoors or outside. They are recognized by broad range|a variety} of names, including spa pools, whirlpools, whirlpool spas, heated spas, bubble baths or Jacuzzi (a trade name that used generically). In some countries, particularly when in well being spa resorts, scorching tubs can also be hydrotherapy spas or pools, although these phrases are more normally utilized to pools used within health-care premises (e. Whrlpool baths Whirlpool baths are a type of scorching tub usually present in bogs of resort suites or private residences. They are fitted with high-velocity water jets and/or air injection however, in contrast to|not like} the new tubs described above, the water is emptied after every use. They are mainly intended for a single individual, however double variations are available. Because of their particular water characteristics, natural spas might receive minimal water-quality remedy. Hydrotherapy pools In addition, there are physical remedy pools, by which professionals carry out remedies for physical signs on people with neurological, orthopaedic, cardiac or other ailments. These are termed "hydrotherapy pools", and are outlined as pools used for special medical or medicinal purposes. There are additionally remedy pools containing small fish (Garra ruffa) which feed on the scaly skin lesions brought on by psoriasis. The excessive incidence of outbreaks related to scorching tubs outcome of|as a result of} of} their elevated reputation current years|in latest times|lately}. Just being in the neighborhood of a scorching tub on show has resulted in instances and deaths as a result of} legionellosis. In the same year, a second outbreak (in Belgium) was linked to a scorching tub on show at a good (De Schrijver et al. An outbreak of Pseudomonas folliculitis, which occurred within two weeks of the installation of a domestic scorching tub, was discovered to be as a result of} the new tub having been on show earlier than buy, with out appropriate remedy. Various other kinds of pool are available, such as flotation tanks and small vessels used for therapeutic use. This chapter addresses the risk from infections brought on by legionellae in leisure waters. It is important of these are informed concerning the potential dangers from the systems lined in this chapter. System assessments of scorching tubs have revealed an array of things contributing to unhygienic conditions and, doubtlessly, predisposition to legionellae proliferation (see Box eight. Where appropriate, and for ease of reference, it additionally appears specifically at leisure facilities such as scorching tubs, although this creates some repetition of knowledge. Source water high quality - risk elements In pools, the standard of supply water is a crucial consider preventing microbial progress inside the system.
Syndromes
- Heat intolerance
- Transient ischemic attack (TIA), sometimes called a "mini-stroke"
- Seizures
- Convulsions (sudden onset)
- Leukemia
- Malathion
- Blood glucose test
- Positron emission tomography (PET) scan of the brain
- Calcium deposits under the skin
Safe xarelto 20 mg
Specify if: Persistent: A persistent course is characterised by severe signs, marked impair ment, and long length (more than 6 months). Specify current severity: Mild: Only one of the signs laid out in Criterion B is fulfilled. Severe: Two or more of the signs laid out in Criterion B are fulfilled, plus there are multiple of} somatic complaints (or one very severe somatic symptom). Diagnostic Features Individuals with somatic symptom disorder usually have multiple of}, current, somatic symp toms would possibly be} distressing or lead to important disruption of daily life (Criterion A), al though typically just one severe symptom, most commonly ache, is current. Individuals with somatic symptom disorder probably to|are inclined to} have very excessive levels of fear about sickness (Criterion B). They appraise their bodily signs as unduly threatening, dangerous, or troublesome and sometimes assume the worst about their health. When requested instantly about their misery, some individuals de scribe it in relation to different elements of their lives, while others deny any source of misery apart from the somatic signs. In severe somatic symptom disorder, the impairment is marked, and when persistent, the disorder can result in invalidism. Consequently, the affected person may search care from multiple of} medical doctors for the same signs. These individuals usually seem unresponsive to medical interventions, and new interventions may only exacerbate the presenting signs. Some individuals with the dis order seem unusually delicate to medication aspect effects}. Associated Features Supporting Diagnosis Cognitive features embrace consideration targeted on somatic signs, attribution of normal bodily sensations to physical sickness (possibly with catastrophic interpretations), fear about sickness, and concern that any physical activity may injury the physique. The related as sociated behavioral features may embrace repeated bodily checking for abnormalities, re peated seeking of medical help and reassurance, and avoidance of physical activity. These behavioral features are most pronounced in severe, persistent somatic symptom disorder. These features are normally related to frequent requests for medical help for various somatic signs. As the somatic symp toms is a main feature of the disorder, individuals with somatic symptom disorder typ ically current to basic medical health companies somewhat than mental health companies. The suggestion of referral to a mental health specialist could also be} met with shock or even frank refusal by individuals with somatic symptom disorder. The prevalence of somatic symptom disorder in the basic adult inhabitants could also be} around 5%-7%. Females probably to|are inclined to} report more somatic signs than do males, and the prevalence of somatic symptom disorder is consequently likely to to|prone to} be greater in females. Development and Course In older individuals, somatic signs and concurrent medical sicknesses are widespread, and a Criterion B is essential for making the prognosis. Somatic symptom disorder could also be} underdiagnosed in older adults both because of|as a end result of} certain somatic signs (e. Concurrent depressive disorder is widespread in older people who current with quite a few somatic signs. In kids, the commonest signs are recurrent belly ache, headache, fa tigue, and nausea. While young kids may have somatic complaints, they rarely fear about "ill ness" per se previous to adolescence. It is the parent who may decide the interpretation of signs and the associated day without work} faculty and medical help seeking. The personality trait of negative affectivity (neuroticism) has been identi fied as an unbiased correlate/risk factor of a excessive number of somatic signs. Comorbid nervousness or melancholy is widespread and will exacerbate signs and impairment. Somatic symptom disorder is more frequent in individuals with few years of education and low socioeconomic status, and in those who have recently skilled stressful life occasions. Persistent somatic signs are related to demographic fea tures (female sex, older age, fewer years of education, decrease socioeconomic status, un employment), a reported history of sexual abuse or different childhood adversity, concurrent chronic physical sickness or psychiatric disorder (depression, nervousness, persistent depressive disorder [dysthymia], panic), social stress, and reinforcing social factors corresponding to sickness advantages. Cognitive factors that affect on} clinical course embrace sensitization to ache, top ened consideration to bodily sensations, and attribution of bodily signs to a potential med ical sickness somewhat than recognizing them as a standard phenomenon or psychological stress. Cuiture-Reiated Diagnostic issues Somatic sjmnptoms are prominent in various "culture-bound syndromes. The relationship between number of somatic signs and sickness fear is similar in numerous cultures, and marked sickness fear is related to impairment and greater treatment seeking across cultures. The relationship between nu merous somatic signs and melancholy appears to be very comparable around the world and between totally different cultures within one nation. Despite these similarities, there are differences in somatic signs among cultures and ethnic teams. The description of somatic signs varies with linguistic and different native cultural factors. These somatic presentations have been described as "idioms of dis tress" because of|as a end result of} somatic signs may have special meanings and form patient-clinician interactions in the explicit cultural contexts. Explan atory models also range, and somatic signs could also be} attributed variously to explicit household, work, or environmental stresses; basic medical sickness; the suppression of feel ings of anger and resentment; or certain culture-specific phenomena, corresponding to semen loss. There may be differences in medical treatment seeking among cultural teams, in advert dition to differences variable access to medical care companies. Seeking treatment for multiple of} somatic signs generally medical clinics is a worldwide phenomenon and happens at comparable charges among ethnic teams in the same nation. Functional Consequences of Somatic Symptom Disorder the disorder is related to marked impairment of health status. Many individuals with severe somatic symptom disorder are likely to to|prone to} have impaired health status scores more than 2 commonplace deviations beneath inhabitants norms. Differential Diagnosis If the somatic signs are consistent with with} one other mental disorder (e. If, as commonly happens, the crite ria for both somatic symptom disorder and one other mental disorder prognosis are ful crammed, then both should be coded, as both may require treatment. Con versely, the presence of somatic signs of an established medical disorder (e. In panic disorder, somatic signs and nervousness about health probably to|are inclined to} occur in acute episodes, whereas in somatic symptom disorder, nervousness and somatic symp toms are more persistent. Individuals with generalized nervousness disorder fear about multiple of} occasions, conditions, or activities, only certainly one of which may contain their health. However, depressive issues are differentiated from somatic symptom dis order by the core depressive signs of low (dysphoric) mood and anhedonia. If the person has intensive worries about health however no or minimal somatic signs, it may be more appropriate to consider sickness nervousness disorder. The features listed under Criterion B of somatic symptom disorder could also be} useful in differentiating the 2 issues. In distinction, in delusional disorder, somatic subtype, the somatic symptom be liefs and behavior are stronger than those present in somatic symptom disorder. In physique dysmorphic disorder, the person is excessively involved about, and preoccupied by, a perceived defect in his or her physical features. In distinction, in somatic symptom disorder, the concern about somatic signs displays concern of underlying sickness, not of a defect in look. Comorbidity Somatic symptom disorder is related to excessive charges of comorbidity with medical dis orders as well as|in addition to} nervousness and depressive issues. When a concurrent medical sickness is current, the degree of impairment is more marked than could be expected from the phys ical sickness alone. There is a excessive degree of tension about health, and the person is well alarmed about private health status. Specify whether or not: Care-seeking type: Medical care, together with physician visits or undergoing tests and procedures, is frequently used. Diagnostic Features Most individuals with hypochondriasis at the moment are|are actually} categorized as having somatic symptom disorder; nonetheless, in a minority of cases, the prognosis of sickness nervousness disorder applies as an alternative. Illness nervousness disorder entails a preoccupation with having or buying a seri ous, undiagnosed medical sickness (Criterion A). The preoccupation with concept that|the concept|the concept that} one is sick is accompanied by substantial nervousness about health and disease (Criterion C).
Purchase 10 mg xarelto
Relationship between footwear consolation of shoe inserts and anthropometric and sensory factors. Can custom-made biomechanic shoe orthoses stop problems within the back and lower extremities? The effectiveness of ergonomic interventions on return-to-work after low back ache; a potential two 12 months cohort examine in six nations on low back ache sufferers sicklisted for 3-4 months. Multidisciplinary biopsychosocial rehabilitation for subacute low back ache amongst working age adults. Lombalgies: recommandations pour le diagnostic et la prise en cost - Algorithmes 1 Г 4. Workplace-based return-to-work interventions: a systematic evaluation of the quantitative literature. Evaluation of efficient return-to-work therapy programs for sick-listed sufferers with non-specific musculoskeletal complaints: a systematic evaluation. Effectifs des employeurs et des travailleurs assujettis а la sйcuritй sociale au 30 juin (2001-2003). Arrкtй royal du 27 mars 1998 relatif au service interne pour la Prйvention et la Protection au Travail. Statistiques des accidents de travail 2002 et des maladies professionnelles 2000-2003. Acute low back ache in trade: a controlled potential examine with particular reference to therapy and vocational factors. Aertgeerts) to talk about and finalize a strategy to be used in this project (Part I). The search method shall be adapted to the location that has been searched (see results part below). Whenever essential the Mesh entry phrases « low back ache » and « sciatica » shall be used. All search methods corresponding to all websites will clearly be described within the results part find a way to} make it possible for any external validator to reproduce the results of every search. This preliminary search aims at estimating the variety of references might be} retrieved from the literature on a subject similar to "low back ache". On the premise of the results of that preliminary search a extra outlined search technique shall be elaborated. Only references not utilized by the previously selected tips shall be thought of. Grading energy of recommendations and high quality of evidence in scientific tips; Report from an American school of chest physician task drive. All revisions included in that ultimate model shall be offered to the expert clinician for approval. In the Search window of the main page of the location "sciatica" was entered A complete 2 references were obtained. One had already been retrieved within the previous seek for "low back ache" on this site. Philadelphia Panel evidence-based scientific practice tips on selected rehabilitation interventions for low back ache. Canadian Task Force on Preventive Health Care - National Government Agency [Non-U. Washington State Department of Labor and Industries - State/Local Government Agency [U. In the disease/condition window of the "detailed search" page of the location. New Zealand Guidelines Group search (March eight, 2006) In the "Basic search" window of the "Guidelines and Other Major Publications" page. A second search on this site was conducted In the "Basic search" window of the "Guidelines and Other Major Publications" page. The search was limited to: 1996 to 2006, practice tips (in the "publication sorts" window) A complete of 23 references were found. One had already been obtained from previous searches and is included within the here above retrieved references. Four had already been obtained from previous searches and are included within the here above retrieved references. Stokes B, Blair R, Bogduk N, Glasziou P, Greenway T, Johnson M, McMeeken J, Yelland M [Medical Services Advisory Committee, Department of Health and Aged Care, Commonwealth of Australia], June 2001 assessment report [with systematic review] Low-back ache. Horder M, Borum F, Gjorup T, Jorgensen T, KamperJorgensen F, Madsen M, Olesen F, Sogaard J, Timm H [Danish Institute of 2. Diagnosis, administration and follow-up of sufferers with chronic low back ache [quick reference information for clinicians]. One extra relevant tips that was recorded as a systematic evaluation was found: 1. One was obtained twice in the identical search; after discarding that duplicate, 60 references remained. Intradiscal electrothermal therapy for chronic discogenic back ache horizon scanning evaluation. Multidisciplinary ache programs for chronic ache: evidence from systematic critiques. Percutaneous intradiscal radiofrequency thermocoagulation for chronic discogenic low back ache. Radiofrequency strategies for the administration of lumbar discopathy (discal nucleoplasty, percutaneous thermocoagulation, electrothermal annuloplasty). Longer term scientific and financial benefits of providing acupuncture care to sufferers with chronic low back ache. A second seek for sciatica was conducted on that site: In the "Project search and choose" page. Rehabilitation after lumbar disc surgical procedure, Surgery for lumbar disc prolapse, Advice to stay energetic as a single therapy for low-back ache and sciatica, Bed relaxation for acute low-back ache and sciatica, Surgery for degenerative lumbar spondylosis, Acupuncture and dry-needling for low back ache, Back faculties for non-specific low-back ache. Bed relaxation for acute low-back ache and sciatica, Behavioural therapy for chronic low-back ache, 10. Multidisciplinary biopsychosocial rehabilitation for subacute low-back ache amongst working age adults, sixteen. Work conditioning, work hardening and functional restoration for staff with back and neck ache. It was decided to make a first choice out the quite a few relevant references retrieved. The Dutch Institute for Health Care Improvement guideline for the diagnosis and therapy of aspecific acute and chronic low back complaints Dutch physiotherapy tips for low back ache. After fusion of all searches and elimination of duplicates a total of 796 references remained. The results of this preliminary search was discussed and the choice was taken to limit the period of search to 2003 to 2006 which still left 490 references. Thorough description of searches and references obtained shall be provided within the subsequent deliverable. Ils ne prйcisent cependant pas de mйthodologie de recherche systйmatique de littйrature dans leur publication. Vu leur excellente qualitй mйthodologique, les Cochrane systematic critiques ne sont pas dйcrites dans les« Evidence Tables ». Eterocoxib must be thought of for use in sufferers who consent to be enrolled in scientific research. Analisis de revisions sistematicas sobre tratamientos quirurgicos y conservadores desde el punto de vista de la medicina basada en la evidencia. P: adults affected by ache within the musculoskeletal system due to of} osteoarthritis or low back ache. I: Harpagophytum procumbens (preparations might differ within the solvent, the drug extract ratio, the galenic utility kind, the content of energetic precept. Randomisation « aveugle » oui Prise en cost aveugle pour le patient Oui Prise en cost aveugle pour les soignants non Analyse des effets aveugle: non Equivalence des groupes: non pas tout а fait Loss to follow-up: 72/100 completed the examine Intention to treat analyse:non Prise en charges comparables hors intervention: personnalisation Rйsultats valides et applicables? The examine concludes that "when controlling for pretreatment scores, subjects receiving handbook therapy with particular adjuvant exercise reported significant reductions in ache". Sйlection des articles pertinents dйcrite: Evaluation de la qualitй des articles: Jadad scale (5 points) Etudes de base dйcrites.
Purchase 2.5 mg xarelto
Looking forward (see also Advance Care Planning (p81)) · Triggers: o o o o o o o o "Would you be stunned if this affected person was to die within the subsequent year? Symptom management, for restoration or maintenance of dignity and quality of life: · Optimisation of medical administration of condition, treatable causes of degradation, and iatrogenic problems · Palliation of disease-specific signs four. Rationalization/deprescribing of medication · Reduce or stop medication the place persevering with benefit is uncertain 7. Reduction of healthcare bureaucracy · Reducing hospital attendances for multiple of} clinic appointments and exams when multiple of} specialties involved eight. Many of the factors are relevant to decline from Dementia and frailty Specific scientific prognostic indicators: General across the situations · Marked decline in bodily state and performance standing (e. This allows the affected person to keep some influence or management over their future care. The healthcare skilled ought to have data of probably illness occasions, therapy options and native services obtainable. Advance Care Planning spans a spectrum from open conversations to formal, legally binding documents. Deciding not to embrace the affected person is just justified if the diploma of misery is expected to be harmful. This might embrace permission for qualified nurses to verify dying 3 Involve them in decision making about therapy and care · All decision-making ought to be carried out in partnership with the affected person and their family/friends. One ought to be conversant in the Personalised Care Plan operating in your area/service · Remember a person can change their mind. A slender straw might be simpler to use than a broad one when the affected person may be very weak · Mouth care is crucial. Monitor for improvement of urinary retention · Skin care guarantee applicable care of stress areas and wounds is obtainable Maintain Comfort to obtain a pain free and comfy dying · Adopt a problem-solving approach to symptom management (p4) · Review all medicine and hold only the essentials to keep comfort. Make every possible effort to enable the affected person to obtain the tip of life care they need, together with being within the place of their alternative, which can have changed over time. It provides an alternative route of drug administration with little impact on affected person mobility or independence. By sustaining regular drug plasma ranges, a syringe driver might improve symptom management. Indications For administering medicine when the oral route is troublesome or inappropriate. Consider establishing a syringe driver if: · Severe nausea and/or vomiting · Severe oral tumours, sores or infections · Dysphagia · Intestinal obstruction · Poor absorption of oral medicine (rare) · Weak, unconscious or sedated affected person · Patient choice Before establishing the syringe driver, explain to affected person and household the reason for using it, how it it} works and the possibility of|the potential of|the potential for} infusion website reactions. Do not website near a joint or bony prominences and keep away from pores and skin folds, broken, oedematous, infected or recently irradiated pores and skin. If this happens, stop the syringe pump and: o Check medicine are suitable o Switch to 0. Relatively costly More costly than morphine; useful if quantity of morphine too great to fit into syringe Used in severe renal failure (p23) Or the place accumulation of the medicine above Extrapyramidal effects happen, particularly at larger doses. Be aware that lots of the traditional somatic signs of melancholy corresponding to anorexia, weight reduction and sleep disturbance might already be present in sufferers with advanced progressive illness, together with cancer. Diagnosis Biological signs · Diurnal variation in mood; agitation · Sleep disturbance particularly with frequent or early morning waking Psychological signs · Persistent, pervasive low mood with loss of pleasure and delight · Withdrawal from relationships and activities · Morbid guilt, feelings of helplessness and worthlessness/low shallowness · Persistent unfavorable thinking fashion relating to all features of life, previous, present and future · Excessive rumination · Suicidal ideas and intentions Causes/Risk factors · Past historical past of melancholy · Need to adjust to many life changes over a short time frame · Loss of earlier roles, loss of deliberate future · Poor symptom management · Immobility and isolation with poor quality of life and lack of support · Uncertainty about illness or prognosis · Early dementia · Drugs corticosteroids (long term use, or on withdrawal), benzodiazepines, some cytotoxics, antihypertensives and narcoleptics Management A Consider reversible causes Minimise the causes: see above B Non-drug measures Provide psychological support or therapies C Drug therapies are really helpful in moderate or severe melancholy. Mirtazapine is an alternative anxiolytic antidepressant with a aspect impact profile of elevated urge for food, weight acquire and improved sleep, which can be useful in some sufferers. A tricyclic antidepressant helpful if pain or poor sleep are outstanding features. Consider specialist referral for melancholy in final few|the earlier few|the earlier couple of} weeks of life: options embrace multi skilled support and use of methylphenidate. Giving dangerous news means entering a therapeutic dialogue: listening and responding; which will to} affect on} how sufferers and households will cope. The goal is to: · Maintain trust between affected person, family/carer and health professionals · Enable applicable adjustment for the reality of the state of affairs · Encourage knowledgeable alternative of administration options · Reduce uncertainty in regards to the future or at least of|no much less than} acknowledge it · Enable sufferers to regain a sense of some management over their state of affairs the next framework describes one approach to breaking dangerous news: 1. Preparation · Know the details and potential administration plan · Arrange for privacy, enough seating and avoidance of interruptions · Whenever possible offer the affected person the possibility to have an in depth member of the family or good friend present 2. Assess the prevailing stage of understanding (may want repeating as further info given) · "What do you perceive about your illness/what is happening? Check if more info wanted and at what stage · "Do you want to go on or is that enough for now? Allow denial · Allow the affected person to management the pace of knowledge move, and to whom the data ought to be given 5. Know when to stop · Be clear and easy, avoiding jargon, and above all be gentle · Avoid assumptions about understanding i. Summary and plan · Summarise what has been mentioned, emphasising the positive · Outline future therapy if applicable, using written or printed materials if possible. Make preparations for further contact · Offer early review · Ask who advised of the diagnosis/information 10. It applicable to explore the denial the place it has created conditions which are be} harmful corresponding to preventing applicable therapy, enough symptom management, or future planning for dependents. However, this inevitably creates pressure as a result of|as a result of}, ethically and legally, the affected person has the proper to info and to authorize disclosure of knowledge to household. Occasionally sufferers collude with professionals to withhold info from their household. This is tougher as the affected person has to give permission for disclosure of knowledge, nevertheless the principles are the same as above - exploration of reasoning; rationalization of penalties; reassurance of delicate handling and offer facilitation. Psychological, emotional, religious and social needs of both affected person and their family/carers ought to be addressed. This holistic evaluation is necessary in making certain that the affected person and household have optimum support in any care setting. It also ensures that discharge planning is effective (hospital/hospice workers ought to verify that these plans are acceptable to the affected person, household, carers and Primary Health Care Team). During evaluation it ought to become apparent whether further expert skilled assistance is required for psychological, religious and social care. It requires offering a person with the house to talk about and explore their perception system. Facilitating these conversations allows for the clinician or chaplain to address misery arising from any disaster of their perception system that has been brought on by their experience of having a life-shortening illness. Attend to: · Signs of their wishing to explore religious points · Ask your self "Why am I being advised this? Reassure and assist with: · Good bodily care in illness and dying · Respect for his or her integrity, worth and values · Information as requested · "Unfinished business" · Personal support "being alongside" · Care for household and carers · Reviewing of life · Arranging provision of religious counselling if needed. Attend to your self: Facing intense feelings or misery can leave us feeling uncomfortable, insufficient, helpless or weak. It is therefore necessary to explore troublesome points or share concerns with colleagues. Cultural attitudes can particularly influence: · Language and use of colloquialisms · the roles of the household · How signs or illness are described and understood · Attitudes towards of|in course of} expressing emotion and discussing non-public points with these outside the household · Ethical points, together with autonomy and confidentiality · Attitudes towards of|in course of} typical Western therapies, complementary or different therapies, meals and diet · Attitudes towards of|in course of} pain aid · Attitudes towards of|in course of} dying and dying · Rituals surrounding dying (see below) · Preferred place of care residence, care residence, hospital or hospice · Acceptance of assist and support Health professionals ought to present their consciousness by: · Ensuring applicable language interpretation services are used · Demonstrating willingness to pay attention and a want to perceive cultural variations and implications · Meeting specific requirements (such as meals, privacy, opportunity to apply spiritual observances etc. Bereavement has been described phrases of|when it comes to|by way of} tasks of grief: Initial shock, numbness and disbelief before emotional actuality of the loss is felt. Seeing the body after dying, attending the funeral or visiting the grave are sometimes necessary in facilitating acceptance of the reality of the dying. Agitation, restlessness and an inability to focus may result up} from the conflict between this looking and avoiding behavior. Anger directed towards of|in course of} the deceased for abandoning them, towards of|in course of} God, or (justly or unjustly) towards of|in course of} professionals. It is widespread for bodily signs related to over-activity of the autonomic nervous system to be experienced. As the pangs of grief and nervousness reduce in frequency and severity the bereaved might lose interest and objective in life. The task of resolution and reorganisation is entered when emotional vitality is reinvested in new relationships and activities, although anniversaries usually set off renewed grief. For some, a part of} the work of grieving undergone before the dying (anticipatory grieving). The pattern of oscillating from one state to another will continue for some time and is totally regular. For most individuals, no formal psychotherapeutic intervention is needed as their character, earlier life experiences, social community and loving relationship with the deceased enable them to come to phrases with their loss, and infrequently to develop personally through it. Written info explaining what experienced and giving useful contact numbers is commonly appreciated.

Trusted 10 mg xarelto
If the presentation consists of a mix of|a mixture of} varieties of|several sorts of|various sorts of} symptoms, the particular mental dysfunction due to of} another medical situation is dependent upon by} which symptoms predominate within the medical picture. When a analysis of substanceinduced anxiousness is being made in relation to leisure or nonprescribed medicine, it could be useful to get hold of a urine or blood drug display screen or different applicable laboratory analysis. If the disturbance is related to each another medical situation and substance use, each diagnoses. Features similar to onset af ter age forty five years or the presence of atypical symptoms throughout a panic attack (e. Anxiety dysfunction due to of} an different medical situation must be distinguished from different anxiousness issues (especially panic dysfunction and generalized anxiousness disorder). In different anxiousness issues, no particular and direct causative physiological mechanisms related to another medical situation could be demonstrated. Late age at onset, atypical symptoms, and the absence of a personal or household history of tension issues counsel the necessity for a radical evaluation to rule out the analysis of tension dysfunction due to of} another medical situation. Anxiety dysfunction due to of} another medical situation must be distinguished from sickness anxiousness dysfunction. Illness anxiousness dysfunction is characterized by worry about sickness, concern about ache, and bodily preoccupations. In the case of sickness anxiousness dysfunction, people may or may not have identified medical conditions. Anxiety dysfunction due to of} another medical situation must be distinguished from adjustment issues, with anxiousness, or with anxiousness and depressed mood. Adjustment dysfunction is warranted when people expertise a maladaptive re sponse to the stress of getting another medical situation. The response to stress normally concerns the which means or penalties of the stress, as in contrast with the expertise of tension or mood symptoms that happen as a physiological consequence of the other medical situation. In adjustment dysfunction, the anxiousness symptoms are sometimes related to coping with the stress of getting a common medical situation, whereas in anxiousness dysfunction due to of} another medical situation, people extra probably to|usually tend to} have outstanding bodily symp toms and to be targeted on points other than the stress of the sickness itself. This is finished by recording "different specified anxiousness dysfunction" followed by the particular purpose (e. Examples of presentations specified using the "different specified" designation embody the following; 1. Khyвl cap (wind attacks): See "Glossary of Cultural Concepts of Distress" within the Ap pendix. Ataque de nervios (attack of nerves): See "Glossary of Cultural Concepts of Distress" within the Appendix. Obsessions are recurrent and persistent ideas, urges, or photographs that are be} experienced as intrusive and unwanted, whereas compulsions are repetitive behaviors or mental acts that an indi vidual feels driven to carry out in response to an obsession or according to guidelines that must be applied rigidly. Some different obsessive-compulsive and related issues are also char acterized by preoccupations and by repetitive behaviors or mental acts in response to the preoccupations. Other obsessive-compulsive and related issues are characterized pri marily by recurrent body-focused repetitive behaviors (e. Clinicians are inspired to display screen for these conditions in people who present with considered one of them and be aware of|concentrate on|pay attention to} overlaps between these conditions. At the same time, there are necessary variations in diagnostic validators and therapy ap proaches throughout these issues. Moreover, there are shut relationships between the anx iety issues and some of the the} obsessive-compulsive and related issues (e. The obsessive-compulsive and related issues differ from developmentally norma tive preoccupations and rituals by being extreme or persisting past developmentally applicable intervals. It then covers body dysmorphic dysfunction and hoarding dysfunction, that are characterized by cognitive symptoms similar to perceived defects or flaws in bodily appearance or the perceived have to save possessions, respectively. The chapter then covers trichotillomania (hair-pulling disorder) and excoriation (skin-picking) dysfunction, that are characterized by recurrent body-focused repetitive behaviors. Finally, it covers substance/medication-induced obsessive-compulsive and related dysfunction, obsessive-compulsive and related dysfunction due to of} another medical situation, and different specified obsessive-compulsive and related dysfunction and unspecified obsessive-compul sive and related dysfunction. Hoarding dysfunction is characterized by persistent problem discarding or parting with possessions, regardless of their actual value, as a result of|because of|on account of} a powerful perceived have to save the items and to distress related to discarding them. For instance, symptoms of hoarding dysfunction result within the accumula tion of massive number of|numerous|a lot of} possessions that congest and muddle active dwelling areas to the ex tent that their supposed use is considerably compromised. They may be preceded by an rising sense of tension or may result in gratification, pleasure, or a way of reduction when the hair is pulled out or the skin is picked. Individuals with these issues may have range ing levels of acutely aware consciousness of the conduct while participating in it, with some indi viduals displaying more targeted attention on the conduct (with previous tension and subsequent relief) and different people displaying more computerized conduct (with the be haviors seeming to happen with out full awareness). Substance/medication-induced obsessive-compulsive and related dysfunction consists of symptoms that are be} due to of} substance intoxication or withdrawal or to a medicine. Obses sive-compulsive and related dysfunction due to of} another medical situation entails symptoms characteristic of obsessive-compulsive and related issues that are be} the direct pathophysio logical consequence of a medical dysfunction. Examples of particular syndromes not listed in Section, and subsequently identified as different specified obses sive-compulsive and related dysfunction or as unspecified obsessive-compulsive and related dysfunction embody body-focused repetitive conduct dysfunction and obsessional jealousy. Obsessive-compulsive and related issues that have a cognitive component have in sight as the idea for specifiers; in every of these issues, perception ranges from "good or fair perception" to "poor perception" to "absent insight/delusional beliefs" with respect to disorderrelated beliefs. Presence of obsessions, compulsions, or each: Obsessions are outlined by (1) and (2): 1. Recurrent and persistent ideas, urges, or photographs that are be} experienced, at a while in the course of the disturbance, as intrusive and unwanted, and that in most people trigger marked anxiousness or distress. The individual makes an attempt to ignore or suppress such ideas, urges, or photographs, or to neutralize them with some other thought or action. Note: Young youngsters may not ready to|be capable of|have the power to} articulate the aims of these behaviors or mental acts. Specify if: With good or fair insiglit: the person recognizes that obsessive-compulsive dis order beliefs are positively or most likely not true or that they may or true. With poor perception: the person thinks obsessive-compulsive dysfunction beliefs are most likely true. With absent insight/deiusionai beiiefs: the person is totally convinced that obsessive-compulsive dysfunction beliefs are true. Specify if: Tic-reiated: the person has a present or past history of a tic dysfunction. These beliefs can embody an inflated sense of duty and the tendency to overesti mate menace; perfectionism and intolerance of uncertainty; and over-importance of ideas (e. This criterion helps to distinguish the dysfunction from the occasional intmsive ideas or repetitive behaviors that are be} widespread within the common inhabitants (e. Associated Features Supporting Diagnosis the particular content material of obsessions and compulsions varies between people. However, sure themes, or dimensions, are widespread, together with these of cleaning (contamination obsessions and cleaning compulsions); symmetry (symmetry obsessions and repeating. Some people even have difficulties discarding and accumulate (hoard) objects as a consequence of typical obsessions and compulsions, similar to fears of harming others. These themes happen throughout totally different cultures, are rela tively consistent over time in adults w^ith the dysfunction, and associated v^ith differ ent neural substrates. For instance, many people expe rience marked anxiousness that may embody recurrent panic attacks. While performing compulsions, some people report a distressing sense of "incompleteness" or uneasiness until issues look, feel, or sound "good. For instance, people with contamination con cerns might keep away from public conditions (e. Females are affected at a shghtly greater fee than males in adulthood, although males are more commonly affected in childhood. Males have an earlier age at onset than females: almost 25% of males have onset before age 10 years. The onset of symptoms is often gradual; nevertheless, acute onset has also been reported. Some people have an episodic course, and a minority have a deteriorating course. Compulsions are more easily identified in youngsters than obsessions are com pulsions are observable. Some variations within the content material of obsessions and compulsions have been reported when youngsters and adolescent samples have been in contrast with grownup samples. These variations probably reflect content material applicable to totally different develop mental phases (e.
Proven 10 mg xarelto
Sexual dysfunctions are also seen in people receiving methadone however are seldom reported by sufferers receiving buprenohine. Chronic alcohol abuse and chronic nicotine abuse are related to erectile issues. Prevalence the prevalence and the incidence of substance/medication-induced sexual dysfunction are unclear, probably due to underreporting of treatment-emergent sexual facet effects}. Data on substance/medication-induced sexual dysfunction sometimes concern the results of antidepressant medicine. The prevalence of antidepressant-induced sexual dysfunction var ies partly relying on the particular agent. Approximately 25%-80% of people taking monoamine oxidase inhibitors, tricyclic antidepressants, serotonergic antidepressants, and mixed serotonergic-adrenergic antidepressants report sexual facet effects}. Approximately 50% of people taking antipsychotic drugs will experience antagonistic sexual facet effects}, including issues with sexual need, erection, lubrication, ejaculation, or orgasm. The incidence of these facet effects} amongst completely different antipsychotic brokers is unclear. Exact prevalence and incidence of sexual dysfunctions amongst customers of nonpsychiatric drugs such as cardiovascular, cytotoxic, gastrointestinal, and hormonal brokers are unknown. Elevated rates of sexual dysfunction have been reported with methadone or high-dose opioid medicine for ache. There are increased rates of decreased sexual need, erec tile dysfunction, and problem reaching orgasm related to illicit substance use. The prevalence of sexual issues seems associated to chronic drug abuse and seems greater in people who abuse heroin (approximately 60%-70%) than in people who abuse amphetamines or 3,4-methylenedioxymethamphetamine. Elevated rates of sexual dysfunction are also seen in people receiving methadone however are sel dom reported by sufferers receiving buprenorphine. Chronic alcohol abuse and chronic nicotine abuse are associated to greater rates of erectile issues. Development and Course the onset of antidepressant-induced sexual dysfunction as early as 8 days after the agent is first taken. Approximately 30% of people with gentle to reasonable orgasm de lay will experience spontaneous remission of the dysfunction within 6 months. In some instances, serotonin reuptake inhibitor-induced sexual dysfunction might persist after the agent is discontinued. The time to onset of sexual dysfunction after initiation of antipsy chotic medicine or medicine of abuse is unknown. It is probable that the antagonistic results of nico tine and alcohol might not seem till after years of use. There is some proof that disturbances in sexual operate associated to substance/medication use increase with age. Culture-Related Diagnostic Issues There an interaction amongst cultural components, the influence of medications on sexual functioning, and the response of the person to these modifications. Gender-Related Diagnostic Issues Some gender differences in sexual facet effects} might exist. Functional Consequences of Substance/Medication-Induced Sexual Dysfunction Medication-induced sexual dysfunction might end in medicine noncompliance. Many psychological circumstances, such as depressive, bipolar, anxiety, and psychotic problems, are related to disturbances of sexual operate. Thus, differentiating a substance/medication-induced sexual dys operate from a manifestation of the underlying psychological dysfunction may be quite tough. The analysis is often established if an in depth relationship between substance/medication ini tiation or discontinuation is observed. A clear analysis may be established if the issue occurs after substance/medication initiation, dissipates with substance/medication dis continuation, and recurs with introduction of the same agent. Most substance/medication-in duced facet effects} happen shortly after initiation or discontinuation. Sexual facet effects} that only happen after chronic use of a substance/medication extremely tough to di agnose with certainty. This is finished by recording "different specified sexual dysfunction" followed by the particular purpose (e. The area of intercourse and gender is highly controversial and has led to a proliferation of phrases whose meanings vary over time and within and between disciplines. An additional supply of confusion is that in English "intercourse" connotes both male/female and sexuality. In this chapter, intercourse and sexual refer to the biological indicators of female and male (understood within the context of reproductive capacity), such as in intercourse chromosomes, gonads, intercourse hormones, and nonambiguous internal and exterior genitalia. Disorders of intercourse improvement denote circumstances of inborn somatic deviations of the reproductive tract from the norm and/or discrepancies among the biological indica tors of female and male. Cross-sex hormone remedy denotes the use of of} feminizing hor mones in a person assigned male at start based on traditional biological indicators or the use of of} masculinizing hormones in a person assigned feminine at start. The need to introduce the term gender arose with the realization that for people with conflicting or ambiguous biological indicators of intercourse. Thus, gender is used to denote the general public} (and often legally recognized) lived position as boy or lady, man or lady, however, in distinction to certain social constructionist theories, biolog ical components are seen as contributing, in interaction with social and psychological components, to gender improvement. Transgender refers to the broad spectrum of people who tran siently or persistently establish with a gender completely different from their natal gender. Transsexual denotes a person who seeks, or has undergone, a social transition from male to feminine or feminine to male, which plenty of}, however not all, instances also involves a somatic transition by cross-sex hormone remedy and genital surgery (sex reassignment surgery). In boys (assigned gender), a powerful choice for cross-dressing or simulating fe male attire: or in girls (assigned gender), a powerful choice for sporting only typ ical masculine clothes and a powerful resistance to the sporting of typical female clothes. A sturdy choice for the toys, video games, or actions stereotypically used or en gaged in by the other gender. In boys (assigned gender), a powerful rejection of sometimes masculine toys, video games, and actions and a powerful avoidance of rough-and-tumble play; or in girls (as signed gender), a powerful rejection of sometimes female toys, video games, and actions. The condition is related to clinically important distress or impairment in social, college, or different necessary areas of functioning. A sturdy need for the first and/or secondary intercourse traits of the other gender. The condition is related to clinically important distress or impairment in social, occupationali^or different necessary areas of functioning. Specify if: Posttransttion: the person has transitioned to full-time dwelling within the desired gender (with or without legalization of gender change) and has undergone (or is getting ready to have) a minimum of|no much less than} one cross-sex medical process or remedy regimen-namely, regu lar cross-sex hormone remedy or gender reassignment surgery confirming the specified gender (e. Specifiers the posttransition specifier used within the context of continuing remedy procedures that serve to support model new} gender assignment. Experienced gender might embrace al ternative gender identities beyond binary stereotypes. Usually, they dis play intense negative reactions to parental makes an attempt to have them put on attire or different female attire. Some might refuse to attend college or social events where such garments are required. These girls might reveal marked cross-gender identification in role-playing, dreams, and fantasies. Contact sports activities, rough-and-tumble play, traditional boyhood video games, and boys as playmates are most often most popular. They avoid rough-and-tumble play and aggressive sports activities and have little interest in stereotypically masculine toys (e. In younger adolescents with gender dysphoria, medical options might resemble these of kids or adults with the condition, relying on developmental level. In adults with gender dysphoria, the discrepancy between experienced gender and bodily intercourse traits is often, however not all the time, accompanied by a need to be rid of major and/or secondary intercourse traits and/or a powerful need to purchase some pri mary and/or secondary intercourse traits of the other gender. To varying levels, adults with gender dysphoria might adopt the habits, clothes, and mannerisms of the experi enced gender. They really feel uncomfortable being regarded by others, or functioning in soci ety, as members of their assigned gender. Some adults might have a powerful need to be of a different gender and treated as such, they usually might have an internal certainty to really feel and re spond as the experienced gender without seeking medical remedy to alter physique char acteristics. They might discover different methods to resolve the incongruence between experienced/ expressed and assigned gender by partially dwelling within the desired position or by adopting a gen der position neither conventionally male nor conventionally feminine. Associated Features Supporting Diagnosis When visible signs of puberty develop, natal boys might shave their legs on the first signs of hair development.
References:
- https://www.scotusblog.com/wp-content/uploads/2016/01/ACOG-WilmerHale.pdf
- http://iimlcmee.org/emcbconference2017/wp-content/uploads/2016/11/Listening-to-Consumers-of-Emerging-Markets.pdf
- https://edwardsprod.blob.core.windows.net/media/De/sapien3/doc-0045533b%20-%20commander.pdf