.png)
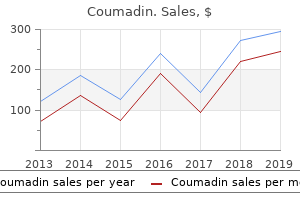
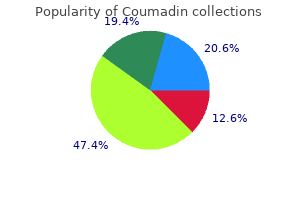
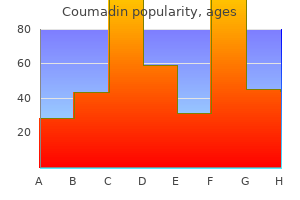
Buy 1mg coumadin
Phase I examine of stereotactic radiosurgery in patients with domestically superior pancreatic most cancers. Induction gemcitabine and stereotactic body radiotherapy for domestically superior nonmetastatic pancreas most cancers. Long-term outcomes of induction chemotherapy and neoadjuvant stereotactic body radiotherapy for patients with domestically superior unresectable pancreatic adenocarcinoma. Therapy of domestically unresectable pancreatic carcinoma: a randomized comparison of high dose (6000 rads) radiation alone, average dose radiation (4000 rads + 5-fluorouracil), and high dose radiation + 5-fluorouracil: the Gastrointestinal Tumor Study Group. The position of stereotactic body radiation therapy for pancreatic most cancers: a single-institution expertise. Cost-effectiveness of recent radiotherapy strategies in domestically superior pancreatic most cancers. Adjuvant chemoradiotherapy and chemotherapy in resectable pancreatic most cancers: a randomised controlled trial. Single- versus multifraction stereotactic body radiation therapy for pancreatic adenocarcinoma: outcomes and toxicity. A comparison of helical intensity-modulated radiotherapy, intensity-modulated radiotherapy, and 3D-conformal radiation therapy for pancreatic most cancers. Adjuvant stereotactic body radiotherapy for resected pancreatic adenocarcinoma with close or positive margins. Gemcitabine chemotherapy and single-fraction stereotactic body radiotherapy for domestically superior pancreatic most cancers. Intensity-modulated radiation therapy considerably improves acute gastrointestinal toxicity in pancreatic and ampullary cancers. The treatment of major malignant gliomas of the mind in any of the next instances: 1. In a poorly performing or aged particular person, a hypofractionatedaccelerated course additionally be} effective. Proton beam therapy � please refer to the Proton Beam Radiation Therapy clinical guideline D. Familial tremor classifications with major systemic illness � 2019 eviCore healthcare. Authorization for this group of ailments will only be granted quickly as} all commonplace therapies have proven to be ineffective. While this combination has improved survival, the prognosis stays poor in the majority of people. The most essential prognostic components for survival are histologic subtype, tumor dimension, and age. The relative value of each method other choices is unknown nicely as|in addition to} it stays open which sequence of modalities must be chosen. Some people with recurrent illness might profit from retreatment with radiotherapy, depending on prognostic components including grade of tumor, age, and performance status. Results have been also considerably poorer for patients with more than two prior surgical procedures or chemotherapy regimens. Recommendations for people with good performance status embrace a high dose methotrexate routine. For youthful people, this is normally adopted by radiation (24 to forty five Gy in commonplace fractionation). The timing of radiation is controversial; regardless of high response charges with a mixture of the 2 modalities, elevated neurotoxicity has been observed. Therefore, the recommendation for older (non-immune-suppressed) � 2019 eviCore healthcare. For people with poor performance status single modality treatment is used, either radiation therapy or chemotherapy. Radiation indicated when there has been an incomplete or limited response to chemotherapy and in the setting of ocular or recurrent illness. There insufficient proof relating to the benefits/harms in the usage of} stereotactic fractionated radiation therapy for people with newly diagnosed or progressive/recurrent malignant glioma. The condition to be treated have to be inflicting severe symptoms or pose a serious risk to function or life expectancy and have an expected benefit of about} stabilizing or improving the clinical state. Accurate simulation and reproducibility of all treatment angles or arcs References Malignant tumors 1. Safety and efficacy of stereotactic radiosurgery and adjuvant bevacizumab in patients with recurrent malignant gliomas. Survival and high quality of life after hypofractionated stereotactic radiotherapy for recurrent malignant glioma. Phase I dose escalation trial of vandetanib with fractionated radiosurgery in patients with recurrent malignant gliomas. Validation and simplification of the Radiation Therapy Oncology Group recursive partitioning analysis classification for glioblastoma. A part I trial of surgery, Gliadel wafer implantation, and immediate postoperative carboplatin together with radiation therapy for major anaplastic astrocytoma or glioblastoma multiforme. Dedicated treatment planning and precise calculation with verification of setup and accuracy of all treatment parameters including but not limited to quantity of} isocenters, arcs, angles, number of beams (size and weight), isodose plans and calculations Radiation Therapy Criteria 10. Hypofractionated stereotactic radiotherapy for low grade glioma at McGill University: long-term follow-up. Exercise habits, functional capability, and survival in adults with malignant recurrent glioma. Prospective randomized trial of low- versus high-dose radiation therapy in adults with supratentorial low-grade glioma: initial report of a North Central Cancer Treatment Group/Radiation Therapy Oncology Group/Eastern Cooperative Oncology Group examine. Stereotactic radiosurgery and fractionated stereotactic radiotherapy for the treatment of acoustic schwannomas: comparative observations of a hundred twenty five patients treated at one institution. Gamma knife radiosurgery for motion disorders: a concise evaluate of the literature. Gamma knife radiosurgery for important tremor: a case report and evaluate of the literature. Philadelphia:Lippincott Williams & Wilkins, a Wolters Kluwer business, 2013:351-361. Long-term results after stereotactic radiosurgery for patients with cavernous malformations. Glycerol rhizotomy versus gamma knife radiosurgery for the treatment of trigeminal neuralgia: An analysis of patients treated at one institution Int J Radiat Oncol Biol Phys. Temozolomide versus 6-week radiotherapy versus hypofractionated radiotherapy in patients older than 60 years with glioblastoma:the Nordic randomised, part 3 trial. Long-term outcomes of fractionated stereotactic radiotherapy for intracranial skull base benign meningiomas in single institution. Abbreviated course of radiation therapy in older patients with glioblastoma multiforme: a potential randomized clinical trial. Extracranial radiosurgery-applications in the management of benign intradural spinal neoplasms. Stereotactic neurosurgery for disabling tremor in quantity of} sclerosis: thalamotomy or deep mind stimulation? Symptomatic Radiation therapy for prostate most cancers is medically needed in the following situations: I. Negative bone scan within the final 6 months, the place applicable � 2019 eviCore healthcare. Proton beam therapy Please refer to the separate Proton Beam Therapy Clinical Guideline. Hypofractionated regimens corresponding to 60 Gy in 20 fractions wants to|must also} be thought of. For people with intermediate- or high-risk illness, mixture external beam mixed with brachytherapy is taken into account medically needed. Combination therapy is taken into account not medically needed for people with low-risk illness. Moderate hypofractionation was outlined as a radiation fraction dimension between 240 cGy and 340 cGy. Ultrahypofractionation was outlined as a radiation fraction dimension higher or equal to 500 cGy. The suggestion was made no matter whether or not the seminal vesicles are included in the treatment field, affected person age, comorbidities, anatomy, and/or urinary function.
Buy 5 mg coumadin
Observational studies of this method are very heterogeneous; nevertheless, they report success charges starting from 57% (551) to 85% (549, 550). This is probably more important than the selection of antibiotic regimen in determining treatment charges and ranges from a single operation involving solely arthroscopic lavage to a number of} operations involving the removing of all infected periprosthetic tissue and loose cement, the change of the prosthesis liners, and high-volume lavage with antiseptic-containing options. Cure charges on this setting appear to be lower than in early postoperative an infection, starting from 50 to 70% (554, 558, 559). This includes an initial operation with removing of the prosthesis and all infected bone and cement, adopted by a period of i. There are few knowledge to guide the period of remedy between the 2 phases or the selection of antibiotics. Based on a stringent definition of success, the speed of successful remedy was higher in the daptomycin group (60% versus 38%). This examine is troublesome to extrapolate, as the take a look at of treatment was at a really early time level (1 to 2 weeks following the second stage). While 2-stage replacement is the commonest mode of change arthroplasty, one-stage joint replacement (where the infected prosthesis is eliminated and changed with a new new} one at a single operation) appears to have related success charges in skilled facilities. Infections of prosthetic cardiac valves and prosthetic joints are described above, but this part offers further background on the formation of biofilms, the pathognomonic characteristic of system infections. Device infections of implantable cardiac gadgets, intravascular catheters, and different prostheses are discussed in higher depth. The biofilm offers a protective matrix across the encased bacteria and is highly resistant to host immune defenses and antimicrobials (567, 569, 570). Within the endovascular system, the host deposits fibrin (571�573), fibronectin (573), fibrinogen (574), and collagen (575) in a sheath along the surface of an inserted system (571, 572, 576). The formation of a biofilm occurs in the following 4 steps: (i) initiation, (ii) colonization, (iii) replication, and (iv) dispersal (576). The bacteria initially adhere to a protein-coated system through hydrogen bonds, van der Waals forces, and electrostatic interactions (567, 576). In the third step, the bacteria divide to kind microcolonies, spreading nonuniformly along the surface of the system (576). In the fourth step, some bacteria will change again to the planktonic state and disperse end result of} hemodynamic stress, a decrease in nutrient availability, or different unknown physiological causes, leading to bacteremia (576). However, an infection poses menace of|the specter of} serious and vital complications (590). While the incidence of cardiac system implantation has continued to enhance, with 42% more cardiac gadgets implanted in 1999 than in 1990 in U. Medicare beneficiaries, the speed of system an infection has elevated at a substantially higher price, with a 124% enhance in the an infection price over the same period (600). This finding is more likely to|prone to} mirror the larger variety of sufferers with long-standing cardiac gadgets quite than higher charges of seeding. Studies that externally validate this clinical phenomenon and establish its biological basis are needed. In such settings, clinical presentation may be be} limited to localized inflammatory signs on the website of the pocket, without any systemic symptoms (604, 614). The explanted system and leads should be cultured and Gram stained (615), and postoperative blood cultures should be drawn (604). Generator pocket website tissue should be obtained, as culture of tissue has a better yield than that of swabs of the pocket website (616). It wants to|must also} be borne in mind that leads are usually extracted through an open generator pocket and thus susceptible to lead contamination. A course of at least of|no less than} 2 weeks of antibiotic remedy is recommended after system extraction if the affected person had bacteremia, and a course of at least of|no less than} 4 weeks is recommended for sufferers with 24 h of ongoing constructive blood cultures regardless of system extraction (615). After system removing, the affected person should be reevaluated as to whether or not reimplantation of the system is indicated (615). If replacement is warranted, the new new} website should be contralateral to the extraction website (615). Additionally, blood cultures should be adverse for at least of|no less than} seventy two h previous to replacement (615). Fever, erythema, tenderness, induration, and/or purulence on the catheter insertion website might suggest catheter an infection (628, 630, 632, 640). Other studies have found that immunosuppression and preexisting valvular disease are also host elements that enhance the chance for complications associated with S. Methicillin resistance a threat issue for complications stemming from an S. In explicit, chance of|the potential of|the potential for} septic thrombophlebitis should be thought of in every affected person with S. Importantly, an ultrasonogram was provided to all enrolled examine topics and was not dependent upon clinical suspicion of underlying septic thrombophlebitis by the treating physicians. First, septic thrombophlebitis was frequent; 71% of the forty eight sufferers had particular or possible hemodynamically vital thrombosis visualized by Doppler ultrasonography. Second, physical examination was insufficient to exclude the presence of underlying septic thrombophlebitis. The sensitivity of physical examination comparability with} Doppler ultrasonography was solely 24%. Based upon these findings, ultrasonography should be performed on every affected person with S. This discount has been attributed to improved procedures for catheter insertion and care (67, 648�650). The main areas of emphasis are "1) educating and training well being care personnel who insert and keep catheters; 2) utilizing maximal sterile barrier precautions during central venous catheter insertion; 3) utilizing a 0. The tips emphasize the implementation of bundled strategies and documenting and reported charges of compliance with all components of the bundle. Rarely, catheter removing is sufficiently problematic in an individual affected person with limited i. In such determined conditions, adjunctive antibiotic lock remedy, in which antibiotics are instilled into the catheter lumen for prolonged intervals, should be thought of along with parenteral remedy (628, 647, 653). For instance, in a multicenter retrospective cohort of 106 sufferers with confirmed or suspected breast prosthesis an infection, Feldman et al. In contrast, not one of the} sixty five culture-confirmed silicone breast infections reported by Ahn et al. Breast implantation for reconstructive functions is a big threat issue for an infection (658, 660, 661), as these sufferers sometimes have a better diploma of tissue scarring, ischemia, and delayed July 2015 Volume 28 Number 3 Clinical Microbiology Reviews cmr. Other threat elements for an infection are (i) hematoma formation secondary to insufficient hemostasis, (ii) seroma formation, (iii) adjuvant chemotherapy or radiation, and (iv) pores and skin irritation (658, 660). The bacteria acquire access to the deep breast tissue through the nipple ducts, which give a passage for bacteria to enter the deep breast tissue from the pores and skin surface (655, 660). This pores and skin flora may be the source of an infection during periareola or transareola breast surgical procedures (660). Fever, localized pain, fluctuance, erythema, and accumulation of pus in the breast are all symptoms indicative of an infected breast implant (658, 660). A single dose of antistaphylococcal antibiotic prophylaxis previous to surgery is recommended to forestall implant an infection (660). Additionally, there may be be} a role for antimicrobialimpregnated implants, as Darouiche et al. The recommended administration for an infected breast implant is surgical removing of the implant with postsurgical drainage, accompanied by 10 to 14 days of appropriate antibiotics (520, 660). Other frequent symptoms are malaise, nausea, vomiting, and signs of elevated intracranial pressure and meningeal irritation (663, 665). Management of an infected ventricular shunt typically requires surgical removing and appropriate parenteral antibiotics (665, 668). Fever, leukocytosis, and constructive blood cultures are less frequent and sometimes happen later in the middle of|in the midst of} an infection (669). Spinal injury and steroid use are two vital threat elements for an infection of penile prosthesis (669). Improved surgical approaches, together with using of} antibiotic-coated hydrophilic implants and a "no-touch" surgical technique (with change of surgical devices and gloves immediately previous to insertion of the prosthesis), have lowered the charges of penile implant an infection (670). Management of an infected penile prosthesis with out complications or bacteremia consists of two to 4 weeks of systemic antibiotics, and most consultants now advocate a single-stage removal-and-replacement process with vigorous irrigation (671).
Diseases
- Factor VII deficiency
- Syringomas
- Pulmonary hypertension, secondary
- 4-Alpha-hydroxyphenylpyruvate hydroxylase deficiency, rare (NIH)
- Pulmonary veno-occlusive disease
- X-linked mental retardation craniofacial abnormal microcephaly club
- Adrenal gland hypofunction
- Senior L?ken syndrome
- Lassueur Graham Little syndrome
- Chorioretinitis
2 mg coumadin
A similar picture additionally be} seen throughout upward transtentorial herniation, which kinks the midbrain (Figure 3�8). Respiratory sample Eupneic, though often extra shallow and rapid than regular or Slow and irregular in rate and amplitude (ataxic) b. Motor responses at relaxation and to stimulation or No response to noxious orbital stimulus; bilateral Babinski indicators or occasional flexor response in lower extremities when feet stroked Motionless and flaccid Figure 3�14. Pressure on the olivary pretectal nucleus and the posterior commissure produces slightly enlarged (typically four to 6 mm in diameter) pupils that are be} fixed to mild. If the affected person is awake, there may also be a deficit of convergent eye movements and associated pupilloconstriction. The presence of retractory nystagmus, during which the entire eye muscle tissue contract simultaneously to pull the globe back into the orbit, is attribute. Deficits of arousal are current in solely about 15% of patients with pineal region tumors, however these are as a result of} early central herniation. Motor responses at relaxation and to stimulation Appropriate motor response to noxious orbital roof strain Paratonic resistance Figure 3�15. Safety of Lumbar Puncture in Comatose Patients A frequent query encountered clinically is, ``Under what circumstances is lumbar puncture protected in a affected person with an intracranial mass lesion? The precise frequency of circumstances during which this hypothetical risk causes transtentorial herniation is tough to ascertain. On the opposite hand, if it is impossible to acquire an imaging examine in a well timed fashion and the neurologic examination exhibits no papilledema or focal indicators, the danger of lumbar puncture is sort of|is kind of} low (probably less than 1%). Under such circumstances, risk-benefit analysis may properly favor continuing with lumbar puncture if the examine is required to make potentially lifesaving choices about scientific care. False Localizing Signs in the Diagnosis of Structural Coma It is often comparatively easy for a talented examiner to differentiate supratentorial from infratentorial indicators, and the cranial nerve findings as a result of} herniation syndromes are attribute. The sagging of the brain in an upright posture is thought to trigger traction on the abducens nerve. More not often other cra- nial nerves, together with the trochlear, oculomotor, or trigeminal nerves, additionally be} similarly affected. Differentiation of supratentorial from infratentorial causes of ataxia has introduced a diagnostic dilemma the rationale that} earliest days of neurology. Similarly, unilateral ataxia of finger-nose-finger testing, which seems to be cerebellar in origin, may sometimes be seen with parietal lobe lesions. Although rare, acute supratentorial lesions can on occasion trigger lower cranial nerve palsies (asymmetric palate, tongue weakness on one side). Bilateral supratentorial lesions can produce dysarthria, dysphagia, and bilateral facial weakness (pseudobulbar palsy, additionally referred to as the opercular or Foix-Chavany-Marie syndrome70). Conversely, the well-known higher motor neuron facial palsy (weakness of the lower a part of} the face) may be seen with some posterior fossa lesions. The distinction between higher versus lower motor neuron cranial nerve weakness can often be made on the basis of reflex versus voluntary movement. For example, a affected person with supranuclear bulbar weakness will often show intact, and even hyperactive, corneal or gag reflexes. A affected person with an higher motor neuron facial palsy will usually show a much more|a way more} symmetric smile on responding to a joke than when requested to smile voluntarily. Fortunately, these basic problems with localization not often intrude on interpretation of the examination of a affected person with an impaired level of consciousness, because the indicators related to herniation usually develop comparatively quickly because the affected person loses consciousness. If the affected person displays false localizing indicators whereas awake, the progression of latest indicators that happen during the herniation process typically clarifies the matter. Although essential to|it may be very important|you will want to} acknowledge the hallmarks of a destructive, as opposed to a compressive, lesion, the true value out there in} distinguishing patients who may benefit from immediate therapeutic intervention from those who want primarily supportive care. The remaining neurons are essentially minimize off from each other and from their outputs, and thus are unable to provide significant behavioral response. However, over the following week or so there additionally be} a progressive degeneration of the subcortical white matter, essentially isolating the cortex from its main inputs and outputs. Adrenoleukodystrophy may trigger primarily posterior hemispheric white matter disease, however not often affects the extent of consciousness until very late in the disease. Infectious causes of dysfunction of the cerebral cortex or subjacent white matter include prion infections (Creutzfeldt-Jakob disease, �ussler syndrome, etc. These disorders progress over a period of weeks to months, and so not often current a diagnostic dilemma by the time international consciousness is impaired. The posterior thalamic penetrating arteries take their origin from these posterior parts of the circle of Willis, and as a consequence there additionally be} bilateral posterior thalamic infarction with a single site of vascular occlusion. Occasional inflammatory and infectious disorders may have a predilection for the diencephalon. Fatal familial insomnia, a prion dysfunction, is reported to have an effect on} the thalamus selectively, and this has been proposed as a reason for the sleep disorder (although this pro� duces hyperwakefulness, not coma). In patients with anti-Ma antitumor antibodies, there are sometimes diencephalic lesions extreme sleepiness and generally other symptoms of narcolepsy, such as cataplexy. These additionally be} both astrocytomas or main central nervous system lymphomas, and they can cause impairment of consciousness as an early sign. Unlike rostrocaudal deterioration, nevertheless, during which all capabilities of the brainstem above the extent are lost, tegmental lesions of the brainstem often are accompanied by extra limited findings that pinpoint the extent of the lesion. Destructive lesions on the level of the midbrain tegmentum usually destroy the oculomotor nuclei bilaterally, resulting in fixed midposition pupils and paresis of adduction, elevation, and despair of the eyes. At the same time, the kidnapping of the eyes with oculocephalic maneuvers is preserved. A destructive lesion of the rostral pontine tegmentum spares the oculomotor nuclei, so that the pupils remain reactive to mild. If the lateral pontine tegmentum is concerned, the descending sympathetic and ascending pupillodilator pathways are both damaged, resulting in tiny pupils whose response to mild additionally be} discernible solely through the use of a magnifying glass. Damage to the medial longitudinal fasciculus causes loss of adduction, elevation, and despair in response to vestibular stimulation, however abduction is preserved, as are behaviorally directed vertical and vergence eye movements. If the lesion extends somewhat caudally into the midpons, there additionally be} gaze paresis toward the facet of the lesion or sluggish vertical eye movements, referred to as ocular bobbing, or its variants (Table 2�3). When the lesion involves the bottom of the pons, there additionally be} bilateral flaccid paralysis. Facial or trigeminal lower motor neuron paralysis seen if the lesion extends into the extra caudal pons. Behavior of the systemic blood strain, pulse rate and spinal fluid strain related to acute modifications in intracranial strain artificially produced. Clinical characterization of idiopathic intracranial hypertension on the Detroit Medical Center. Paroxysmal techniques in intracranial hypertension, studied with ventricular fluid strain recording and electroencephalography. Continuous recording and control of ventricular fluid strain in neurosurgical practice. Obscurations and additional time-related paroxysmal disorders in intracranial tumors: syndrome of preliminary herniation of parts of the brain through the tentorial incisure. Some experimental and scientific observations regarding states of increased intracranial tension. Lateral displacement of the brain and level of consciousness in patients with an acute hemispheral mass. Destructive lesions of the brainstem may happen as a result of|because of|on account of} vascular disease, tumor, an infection, or trauma. The most typical reason for brainstem destructive lesions is the occlusion of the vertebral or basilar arteries. Such occlusions usually produce indicators that pinpoint the extent of the infarction. Hemorrhagic lesions of the brainstem are most commonly intraparenchymal hemorrhages into the bottom of the pons, though arteriovenous malformations may happen at any level. Infections that have a predilection for the brainstem include Listeria monocytogenes, which tends to trigger rhombencephalic abscesses86 (see Figure 4�13). The tentorial notch: anatomical variation, morphometric analysis, and classification in 100 human autopsy circumstances. Localization of the pupillomotor and lodging fibers in the oculomotor nerve: experimental observations on paralytic mydriasis. Traumatic trochlear nerve palsy diagnosed by magnetic resonance imaging: case report and evaluate of the literature. Symptoms and disease associations in idiopathic intracranial hypertension (pseudotumor cerebri): a case-control examine.
Proven coumadin 2mg
Accidental poisoning could happen in farmers while spraying in the fields or opening the lid of the containers. Absorption, Metabolism and Excretion Organochloride compounds are absorbed through skin, inhalation and thru gastrointestinal tract. Most of the compounds are metabolized slowly in the physique and stays in tissues, especially in fatty tissues for prolonged length. These compounds are metabolized in liver and are excreted in urine, feces and milk. Fatal dose � � Extremely poisonous or extremely poisonous - carbaryl, carbfuran, methomyl, propoxur Moderately poisonous or slightly poisonous - aldicarb, triallate. Hyperthermia must be managed in ordinary method Arrhythmias could be managed with lidocaine. Avoid Giving � � � Epinephrine - could exacerbate ventricular arrhythmias Atropine Oil based mostly fluid/food/cathartics management Decontamination � � � Skin - the affected half must be washed thoroughly with copious water Ocular - copious eye irrigation with normal saline or faucet water Ingestion - gastric lavage and administration of activated charcoal. Antidote Administration � Atropine is competitive antagonist of acetylcholine and blocks muscarinic manifestations. The atropine must be given 2 mg intravenous promptly with dose repeated every 10 minutes until indicators of atropinization are evident. Principles of Forensic Medicine and Toxicology Fatal dose Pyrethrum 1 gm/kg clinical Features � � � � Dermal publicity causes erythema, dermatitis, blister formation Ocular publicity causes irritation, lacrimation Inhalation causes rhinorrhea, sore throat, wheezing, cough, dyspnea Ingestion causes nausea, vomiting, paresthesia, vertigo, fasciculation, hyperthermia, altered mental standing, convulsions, pulmonary edema and coma. However, in many of the cases, toxicity with these agents happens because of the allergic reactions to these compounds. The tablets can be found in market with various commerce names similar to - celphos, alphos, sulphas and so on. Fatal dose 4 mg/kg Fatal Dose 3 gm clinical Features Paraquat causes corrosion to mucosa of mouth, esophagus and gastrointestinal tract. Fatal Period 12 to 36 hours mechanism of action Aluminium phosphide liberates phosphine when it comes in in} contact with air and moisture. Phosphine is a protoplasmic poison interfering with enzymes and protein synthesis. In animal studies, phosphine has been shown to cause non-competitive inhibition of cytochrome oxidase of myocardial mitochondria. Suicidal poisoning is common with this agent, especially in the northern India. Rarely unintentional poisoning could happen to employees working in grain elevators, wear homes and grain freighter and so on. Silver nitrate check � the affected person is asked to breathe through a piece of filter paper impregnated with zero. It is alleged that administration of magnesium sulfate is helpful for management of cardiac arrhythmias Gastric lavage is contraindicated since administration of water will release phosphine from the obtainable aluminium phosphide in the stomach. High efficiency liquid chromatographic method for the evaluation of organophosphorus and carbamate pesticides. A retrospective study of acute poisoning in adults � in rural region of Beed district of Maharashtra. Aluminium phosphide poisoning � a clinical, biochemical and histopathological study. Hydrocyanic acid Tobacco Tobacco (tambakhu) is ready from cured leaves of Nicotina tabacum. Uses � � � � Smoking tobacco Chewing Snuff Insecticide Fatal Dose forty to 60 mg of nicotine 15 to 30 gm of crude tobacco Fatal period: 5 to 15 minutes Mechanism of action Nicotine acts on nicotine receptors current in autonomic ganglia, adrenal medulla, central nervous system, spinal wire, neuromuscular junction and chemoreceptors of carotid and aortic our bodies. Accidental poisoning could happen outcome of} overdose Occupational hazard Malingering to induce sickness Suicide or murder is uncommon Chronic Poisoning � Also known as as|often identified as} nicotine habit � Common among smokers, tobacco chewers � Develops physical dependence, manifested by recurrent longing for tobacco, tolerance, cough, impaired reminiscence and amblyopia. Fatal period: 20 to 36 hours clinical Features � � � � Nausea and vomiting Diarrhea Tachycardia Breathlessness Management � Gastric lavage with activated charcoal � Benzodiazepines for convulsions � Symptomatic therapy. The fruits are initially greenish in color but turns yellow after which black when becomes ripe. The fruit accommodates a single nut, which is elongated triangular with deep groove along the sting. Accidental death happens outcome of} consumption of folks medicine containing oleander 3. Common oleander resist decomposition and burning, thus could be detected from decomposed our bodies or ash. Fatal Dose � eight to 10 seeds � 15 to 20 gm of root � 5 to 10 leaves Fatal period: 2 to 3 hours if powdered root taken. B Section Features � this shrub resembles common oleander but have large bell-shaped yellow color flowers. Autopsy Findings � Congestion of organs � Subendocardial and perivascular hemorrhage with focal myocardial edema5 Medicolegal significance: Same as for common oleander. Features � Perennial plant with deeply minimize leaves and lengthy spikes ofdeepbluecolorflowers,withonuprightdownystalks. Theuppersepalofflowerresemblesahood or helmet or cowl, therefore the common name monkshood. It additionally inhibits full repolarization of the membraneofmyocardialtissuecausingrepetitivefiring. Metabolism Metabolism of aconitum alkaloids is especially carried out by the enzyme esterase. Aconitine is converted into benzoyaconine through hydrolysis in C-8 position and into aconine. Fatal Dose � 1 to 2 gm of root � 3 to 5 mg of aconitine Fatal period: 2 to 6 hours. Toxic Principles � Aconitine � Mesoaconitine � Hypoaconitine clinical Features � � � � � � � � Nausea and vomiting Salivation Tingling and numbness in mouth and lips Diarrhea Palpitation Weakness Hypotension Ventricular ectopics B Section. Aconite will get easily destroyed by decomposition and is probably not|will not be} detected in chemical evaluation. Plants: cyanide is current in type of cyanogenic glycoside in broad number of vegetation similar to: � Bitter almond (Figs forty one. Combustion: similar to � Burning of plastic furnishings � Burning of silk or wool � Cigarette smoking. Enzyme rhodanase (present in mitochondria of liver and kidney) converts them to thiocyanate. Some cyanide is converted into cyanocobalamin (vitamin B12) in presence of hydroxocobalamin (vitamin B12a). Mechanism of action of nitrites: nitrates induce methemoglobinemia, which causes detachment of cyanide from the heme group of cytochrome oxidase since methemoglobinhasahigherbindingaffinityforcyanide. Cyanide attaches to the iron of the prosthetic group of cytochrome oxidase resulting in disturbance of the transport and utilization of oxygen in cells and causing a cytotoxic anoxia. Chronic poisoning: Chronic low level of publicity leads to: � Headache � Amblyopia � Optic atrophy � Peripheral neuropathy � Ataxia � Deafness � Glossitis � Stomatitis. Embalming interferes with cyanide detection, due to this fact interpretation in postmortem period becomes difficult. In: Forensic Toxicology � Proceedings of a symposium held at the chemical protection institution Porton Down 29-30 June 1972. Section Toxicology B Chapter forty two - Thomas Sydenham(1680) Somniferous Poisons Among the treatments which it has pleased Almighty God to give man to relieve his sufferings; none is so universal and so efficacious as opium. Codeine Opium Common name: Afim Opium (afim) is the dried extract of the poppy plant (Papaver somniferum). The unripe opium capsules are incised to get hold of the extract, which is milky fluid (Figs forty two. Crude opium is irregular mass of brownish in color with a characteristic scent and bitter style. Poppy seed (khaskhas) are white seeds used as condiment in India for cooking. Benzoisoquinoline group: have delicate analgesic but no narcotic properties � Papaverine � Noscapine (narcotine). Phenanthrene group: have narcotic properties � Morphine � Codeine � Thebaine (non-analgesic).
Coumadin 1 mg
Asterixis can also be|may also be|can be} elicited in stuporous patients by passively flexing and abducting the hips. Unilateral, or less generally bilateral, asterixis has been described in patients with focal mind lesions. However, it could be seen in some waking patients with neurodegenerative problems. Ventilatory patterns, with the exception of psychogenic hyperventilation, are regular. In some patients with psychogenic coma, the eyes deviate towards the bottom when the patient is positioned on his or her aspect. Most patients with metabolic mind disease have diffusely abnormal motor signs together with tremor, myoclonus, and, particularly, bilateral asterixis. Finally, metabolic and structural mind ailments are distinguished from one another by a combination of signs and their evolution. Most aware patients with metabolic mind disease are confused and many of|and a lot of} are disoriented, particularly for time. Early through the sickness, the outstretched dorsiflexed hands present irregular tremulousness and, regularly, asterixis. Posthyperventilation apnea elicited and there hypoventilation or hyperventilation, depending on the precise metabolic sickness. Neurons and glial cells undergo many chemical processes in fulfilling their specialised features. The nerve cells should repeatedly preserve their membrane potentials, synthesize and store transmitters, manufacture axoplasm, and replace their at all times decaying structural elements (Figure 5�2). In addition, they might aid neuronal operate by supplying substrate (lactate)51 (although the diploma, if any, to which neurons metabolize lactate in vivo is controversial53). Astrocytes also take part in controlling blood flow52 and in maintaining the blood-brain barrier. Awake or asleep, the mind metabolizes at one of the highest rates of any organ within the body. However, though the overall metabolism of the mind is relatively fixed, totally different areas of the mind metabolize at totally different rates, depending on how lively an area is. These considerations are central to an understanding of many of the metabolic encephalopathies, and the following paragraphs focus on them in some detail. Overall flow in gray matter, for instance, is generally three to four times greater than in white matter. At glutamatergic synapses, presynaptically released glutamate depolarizes postsynaptic neurons by acting at specific receptor subtypes. The action of glutamate is terminated by an environment friendly glutamate uptake system located primarily in astrocytes. Lactate, once as} released by astrocytes, could be taken up by neurons and serves them as an sufficient energy substrate. A useful magnetic resonance imaging scan of the normal particular person flexing and increasing his fingers. Blood flow will increase to a larger diploma than oxygen consumption within the motor areas, resulting in an increase in oxyhemoglobin. The paramagnetic oxyhemoglobin causes an elevated blood oxygen level-dependent signal within the motor cortex bilaterally. The increase in glucose metabolism over oxygen metabolism ends in elevated lactate manufacturing, presumably the substrate for the elevated demand of neurons58 (Figure 5�4). Important amongst these are adenosine, nitric oxide, dopamine, acetylcholine, vasoactive intestinal polypeptide, and arachidonic acid metabolites. Examples of such reactive hyperemia or ``uncoupling' of flow and metabolism happen in areas of traumatic or postischemic tissue damage, properly as|in addition to} in regions of irritation or within the regions surrounding certain mind tumors. So far, the nature of the native stimulus to such pathologic vasodilation also has eluded investigators. The results of the method, nevertheless, can act to increase the bulk of the concerned tissue and thereby intensify the pathologic results of compartmental swelling within the mind, as mentioned in Chapter 2. Intrinsic arterial spasm in cerebral vessels, which reduces tissue flow below metabolic wants, is an unusual phenomenon restricted largely to arteries at the base of the mind. Multifocal cerebral arteriolar spasm had been invoked to clarify the regional cerebral vascular damage of malignant hypertension; recent work, nevertheless, offers a different interpretation of the pathogenesis of that dysfunction (see page 168). Ions (H� and K�) contribute to the extracellular currents that are be} related to synaptic transmission. In astrocytes, the [Ca2�] increase is produced by activation of metabotropic glutamate receptors (mGluRs) and by propagation of Ca2� waves from neighboring astrocytes through activation of purinergic receptors (P2Y) or entry of 1P3 (inositol (1,4,5)-triphosphate) through gap junctions. Spatial buffering currents in astrocytes release K� from perivascular end-feet, where K� conductance is biggest (K� siphoning). If the flow falls to 10 mL/100 g/minute, membrane integrity is misplaced and calcium inflow into the cells leads to irreversible damage. Flows of 18 mL could be tolerated for several of} hours without resulting in infarction, whereas flows of 5 mL lasting for more than 30 minutes will trigger infarction. Cerebral acidosis is a potent vasodilator, as is potassium, which leaks into the mind extracellular house throughout hypoxia. The reply seems to lie within the specialised properties of the blood-brain barrier, which, by rigorously limiting or facilitating the entry or egress of gear to and from the mind, guards the slim homeostasis of that organ. Glucose is transported across the blood-brain barrier by a carrier-mediated glucose transporter (Glut-1). The uptake of glucose into neurons facilitated by a glucose transporter (Glut-3), and glucose uptake into astrocytes by Glut-1. Under regular circumstances, mind glucose concentration is roughly 30% of that of plasma. Nevertheless, the mind is wealthy in insulin receptors with substantial regional variation, the richest area being the olfactory bulb. In internet metabolic phrases, each 100 g of mind in a traditional human being makes use of about zero. This internet determine, nevertheless, hides truth that|the truth that} glucose consumption in native regions of the mind varies widely according to native useful modifications. However, neurons in all probability make the most of lactate produced from glucose by astrocytes when stimulated with glutamate. These substances provide elevated fuel to the mind when beta-hydroxybutyrate, acetoacetate, and different ketones increase within the blood throughout states such as hunger, the ingestion of high-fat diets, or ketoacidosis. Under regular circumstances, all but about 15% of glucose uptake within the mind is accounted for by combustion with O2 to produce H2O and energy, the remainder going to lactate manufacturing. The mind accommodates about 1 mmol/kg of free glucose in reserve and a considerable amount of glycogen, perhaps as high as 10 mg/L, which is present in astrocytes. Despite this, deprivation of glucose and oxygen to the mind quickly ends in lack of consciousness, regular cerebral operate being maintained a matter of seconds. The energy balance of the mind is influenced both by its supply of energy precursors. Just as intrinsic mechanisms Multifocal, Diffuse, and Metabolic Brain Diseases Causing Delirium, Stupor, or Coma 203 appropriately increase or lower the rate of metabolism in several regions of the mind during periods of regionally elevated or decreased useful exercise, intrinsic mechanisms seem in a position to} ``turn down' general cerebral metabolic exercise and produce stupor or coma when circumstances threaten to deplete blood-borne substrate. The response seems to be important in defending the mind against irreversible damage, nevertheless, and is properly illustrated by describing the neurochemical modifications that accompany hypoglycemia. Some consider that the elevated manufacturing of lactate and reducing of the pH leads to the cellular damage. However, lactate might be a good substrate for neurons, and the elevated blood glucose must be protecting. In truth, in experimental animals, a glucose load given 2 to three hours before an ischemic insult is protecting, but the identical glucose load administered 15 to 60 minutes before ischemia aggravates the ischemic outcome,seventy four though these findings have been challenged. Although adaptive within the short term, in lengthy term|the long run} sustained hyperglycemia damages vasopressin-secreting neurons within the hypothalamus and supraoptic nucleus. In addition, some proof suggests that sustained hyperglycemia damages hippocampal neurons as properly,70 resulting in cognitive defects in both humans71 and experimental animals. These results seem to be unbiased of diabetes-induced damage to mind vasculature resulting in stroke, a standard complication of continual poorly managed diabetes.
Oligomeric Procyanidins (Grape). Coumadin.
- Preventing heart disease, treating varicose veins, hemorrhoids, constipation, cough, attention deficit-hyperactivity disorder (ADHD), chronic fatigue syndrome (CFS), diarrhea, heavy menstrual bleeding (periods), age-related macular degeneration (ARMD), canker sores, poor night vision, liver damage, high cholesterol levels, and other conditions.
- Circulation problems, such as chronic venous insufficiency that can cause the legs to swell.
- Decreasing certain types of eye stress.
- How does Grape work?
- Hayfever and seasonal nasal allergies.
- What is Grape?
- Are there safety concerns?
- Are there any interactions with medications?
- Dosing considerations for Grape.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96481
Proven coumadin 1mg
Total joint substitute of the shoulder should be evaluated as other joint replacements considering anatomical bone loss, mobility defects and muscle atrophy. Excision of the humeral head as with excision of the head of the femur the identical as} 50% for anatomical bone loss. Percent Loss of Use of the Leg: Anterior Flexion Defects of the Hip Anterior Flexion of the Hip to 90 degrees forty five degrees 25 degrees % Loss of Use of the Leg 10% 33 1/3% sixty six 2/3% Posterior extension equals 7 1/2% to 10% loss of use of the leg. Normal abduction is forty five degrees and regular adduction is 35 degrees and loss of each equals 33 1/3% loss of use of the leg. Amputee with 100 percent loss of use of the leg can receive an extra schedule award for a second accident or consequential harm. Synovitis of the hip, bursitis (Iliopsoas bursa, trochanteric bursa, ischiogluteal bursa): defer last evaluation for two years and ordinary schedule award is zero to 7 1/2% loss of use of the leg. Mild defect of flexion and extension equals 10-15% schedule loss of use of the leg; reasonable defects of flexion and extension equals 40-45%; marked defects of flexion and extension equals sixty six 2/3%. Recurrent dislocation of the patella with or without surgery equals 10-15% loss of use of the leg if residual impairment is current. Osteochondritis desiccans with or without surgery equals 7 half - 10% loss of use of the leg. If surgery fails and instability persists which will require utilization of} a brace, consider classification. Revision surgery tends to be much less successful and have more problems than initial replacements. If loss of top of the heel leads to shortening of the leg, a leg schedule should be given. Ankle fusion equals 75% loss of use of the foot which exceeds 60% for ankylosis if additional toe defects are current. Amputations of the distal phalanx/distal interphalangeal joint equals 50% loss of use of the great toe. Amputation of a serious portion of the great toe distal phalanx equals 50% loss of use of the great toe. Special Considerations (Loading) Amputations of two or more toes are loaded 50% and transformed to a foot schedule. Use of assistive gadget similar to a cane, walker, crutches, wheelchair, leg brace, orthopedic particular sneakers, i. Pelvic obliquity, gluteal folds, discrepancy of leg length, deformities of the spine, and flabby abdominal muscles. Persistent radicular pains to the decrease extremities and constructive correlative bodily findings of radiculopathy. Needs assistance to carry out the actions of every day dwelling similar to self care, private hygiene and transportation. The examining doctor is confronted with components in disability, and to fulfill the letter of the Law, an examining doctor has to try to convert variables into constants. No Disability Claimants with persevering with temporary partial or complete disability with circumstances approaching or having exceeded two years in length may have a finding of permanency. It is necessary that the examining doctor feels that full restoration is unlikely and all avenues of reasonable medical and surgical therapy have been explored. Extremes of flexion and extension (whiplash) can even injure the cord or cervical roots. Pathophysiology is both a transient posterior dislocation or a momentary retropulsion of the intervertebral disc into the spinal cord. Consider much less severe injuries to the cervical spine, brachial plexus injuries (thoracic outlet syndrome) or diseases of the shoulder itself (capsular tears). Defer last evaluation for two years for such circumstances may lead to a classification and/or a facial disfigurement (with esotropia and the like). Symptoms additionally be} just like those following a prefrontal lobotomy if there was selective frontal lobe harm with apathy, inappropriate frivolity (Witzelsucht), indifference, lack of spontaneity with a blunting of emotional management (bursts), delicacy of feeling, consideration of others and forethought. There is an incapability to elevate the eyebrow, frown, shut the eye, present teeth, whistle, or purse the lips. Cortex Motor defects additionally be} central as with traumatic harm to the motor neurons (frontal cortex) with a resultant hemiparesis or hemiplegia which might be be} permanent and will end in a permanent complete disability. Fracture dislocations occur most incessantly on the decrease cervical area (C5, C6), often following falls on the head, auto accidents and diving injuries. Syringomyelia is congenital in origin; nevertheless cavities of the cord with comparable signs additionally be} secondary to trauma to the cord. Psychological testing is required to verify the sort and degree of dementia, as well as|in addition to} behavioral modifications current. Spinal cord lesions contain the appreciation of ache and temperature at two levels beneath the precise lesion. Conclusion on the time of evaluation depends on by} subjective and objective findings. In abstract the next criteria are most necessary within the evaluation of partial and complete disability of the central nervous system: 1. The examining doctor is left to make a last determination on partial and complete disability relying on the severity of the above impairments and the degree of loss of function. Vehicular trauma may at instances end in a complete brachial plexopathy with a paralyzed arm and complete absence of reflexes. Reevaluate after two years for return of function, at which time it might be amenable for a schedule loss of use of the arm. Persistent severe weak spot and intractable ache might necessitate considering a partial disability which might lead to a classification. Sensory, greater than motor function, is impaired and signs fluctuate with activity and rest. The strategy of performance of the take a look at for obstruction of the subclavian artery by the scalenus anticus muscle is as follows: claimant is seated with elbows at sides and neck prolonged. It could be confused with cervical discs, carpal tunnel syndrome or ulnar nerve compression on the elbow. The etiology is mostly a compression of the median nerve end result of} thickening of the synovium around the flexor tendons on the wrist, i. Carpal Tunnel Syndrome with or without decompression are often given a schedule loss of the hand which often averages 10-20% loss of use. Elbow the ulnar nerve is topic to direct trauma within the elbow due to its superficial place being covered by fascia and skin solely. Pressure may occur during anesthesia however more commonly the nerve is injured by being drawn tightly in opposition to the ulnar groove. Entrapment of the ulnar nerve on the elbow is often given a schedule loss of use of the arm if accompanied with defects on the elbow. Sensory loss is over the radial aspect of the palm and palmar aspect of the thumb, index, center and radial half of the ring finger. Such circumstances are often given a schedule loss of use of the hand relying upon motor and sensory deficits. The ensuing neuropathy causes the burning kind ache over the anterolateral thigh with some hypaesthesia. In severe circumstances, the claimant additionally be} crippled and demoralized (temporary complete disability). Neurolysis on the web site of the harm may help or a proximal sympathetic block additionally be} effective. Reflex sympathetic dystrophy at instances is taken into account a separate entity having more psychogenic components than causalgia. The etiology could be very unsure and the disorder impacts skin, muscles, tendons, blood vessels and bones. Cases of causalgia and reflex sympathetic dystrophy may require referral to a ache clinic. When modalities of therapy fail and signs persist, especially ache, then consider classification. Symptomatic disabling circumstances additionally be} given permanent partial or complete disability relying on severity of signs, medical findings and useful impairment. Scars and disfigurement involving the neck are restricted to the region above the clavicle. Review the case folder, medical data, emergency room reviews, and reviews of hospitalization, and cardiac care. The claimant in a position to|is ready to} carry out ordinary duties and actions of every day dwelling without dyspnea. The claimant has a causally associated respiratory disorder and/or impairment with pulmonologist documentation and an appropriate diagnostic take a look at.
Effective 2mg coumadin
Those patients with a rating of zero had a prevalence of resistant organisms of 15%, whereas nearly 75% of these with a rating of 6 to 10 had a resistant pathogen (711). Thus, it was potential to develop one other prediction rating for this setting (714), an undertaking that has since been repeated in other geographic settings (715). Of the quite a few virulence elements necessary in staphylococcal infections, quantity of} seem to be particularly implicated in the development of pleuropulmonary infec- July 2015 Volume 28 Number three Clinical Microbiology Reviews cmr. Massive polymorphonuclear leukocyte influx into the lung parenchyma and the formation of microabscesses are typical findings of S. Notably, immunization towards alphahemolysin is protecting towards lethal pneumonia in mice (722, 723). Clinical Features and Outcomes tor of mortality (731), maintaining with|consistent with|in line with} comparable findings from a previous meta-analysis of 107 circumstances (732). The median age of these with bacterial coinfection was forty three years, and the mortality rate was 21%. Pleural effusions have been current in 9/15 patients, and the mortality rate was 13% (730). Interpretation of those outcomes was complicated by the use of of} a vancomycin dosing routine that was much less aggressive than would be recommended underneath present dosing guidelines (747). Additionally, vancomycin trough ranges have been suboptimal in 50% of patients (750�752). The suggested duration of remedy is 7 to 21 days, depending on the medical response. The desire for linezolid and clindamycin over vancomycin in this setting is based upon the speculation that linezolid and clindamycin, which suppress toxin production, might enhance survival with this specific infection, for which toxin production is a key virulence factor. Two retrospective studies suggest that there may be be} a medical profit for suppression of poisons in such circumstances (756, 757). However, in the case of hematogenous septic pulmonary emboli, as from right-sided endocarditis, daptomycin may be be} an possibility (119). Intracranial epidural abscesses are a lot much less widespread than spinal epidural abscesses and usually comply with surgical procedure or trauma. Although a uncommon infection (1 in 20,000 hospitalized patients [763]), spinal epidural abscess is the second most common infectious explanation for medical malpractice in the United States (764). The incidence of epidural abscess appears to have increased over the previous 30 years (765). Thus, posterior epidural area involvement is more widespread than anterior epidural area involvement, and lumbar and lower thoracic epidural abscesses are more widespread than cervical epidural abscesses (769). Because the epidural area is a steady vertical region, epidural abscesses typically unfold over quantity of} vertebral ranges and infrequently might contain the whole spine. The most necessary potential consequence of spinal epidural abscesses is harm to the spinal twine and nerve roots, which might happen end result of} direct compression of the twine by an expanding assortment of pus (770) or not directly via arterial or venous ischemia. The basic medical triad for epidural abscess is back ache, fever, and neurological signs; nonetheless, the whole triad is current in only a minority of patients at presentation (773). For this reason, the diagnosis of spinal epidural abscess is often not initially thought of. For example, only 40% of admitting diagnoses included spinal epidural abscess as the suspected diagnosis for one sequence of forty three patients finally found to have epidural abscess (763). In basic, surgical decompression (laminectomy, debridement of infected or necrotic tissue, and drainage of pus) is required to obtain a profitable outcome in circumstances of S. Because of risk of|the potential of|the potential for} everlasting paralysis, spinal epidural abscess is a medical and surgical emergency. Once paralysis is established for 24 to 48 h, the harm is doubtless to|prone to} be everlasting. Thus, the important thing} step is the early recognition of risk of|the potential of|the potential for} spinal epidural abscess and speedy investigation to confirm the diagnosis. Most authors suggest that surgical decompression be carried out urgently (within 24 h of diagnosis) in patients with S. Fever and alter in consciousness are the two most common medical symptoms (782, 789). After the removing of highly absorbent tampons from the market, the annual incidences of S. Nonmenstrual circumstances have been associated with the next mortality rate than menstrual circumstances (807). This results in an awesome systemic inflammatory response syndrome and is manifested by septic shock with organ failure. However, this benign appearance on no account reduces the need for surgical debridement in patients with wound-associated S. Because it could possibly} block the production of exotoxins by the bacterial ribosome, clindamycin or linezolid is often added to normal antibiotic remedy (381). Septic pelvic thrombophlebitis manifests as excessive fever regardless of antibiotics and acute belly ache (825). Treatment with anticoagulation remedy and acceptable antibiotics is recommended for circumstances of pelvic septic thrombophlebitis (825). For patients with central venous catheter-associated septic thrombophlebitis, Crowley et al. Other symptoms are hematuria, altered psychological status, dysuria, suprapubic ache, and, much less commonly, flank ache (818). Not only have there been waves of increasing antimicrobial resistance (827), however the spectrum of medical disease additionally continues to change. Detection and medical relevance of Staphylococcus aureus nasal carriage: an replace. Reduced vancomycin susceptibility in Staphylococcus aureus, including vancomycin-intermediate and heterogeneous vancomycin-intermediate strains: resistance mechanisms, laboratory detection, and medical implications. The changing epidemiology of Staphylococcus aureus bloodstream infection: a multinational population-based surveillance study. Stable incidence and continued enchancment in short term mortality of Staphylococcus aureus bacteraemia between 1995 and 2008. Allard C, Carignan A, Bergevin M, Boulais I, Tremblay V, Robichaud P, Duperval R, Pepin J. Secular changes in incidence and mortality associated with Staphylococcus aureus bacteraemia in Quebec, Canada, 1991-2005. Temporal tendencies in the incidence of Staphylococcus aureus bacteremia in Olmsted County, Minnesota, 1998 to 2005: a populationbased study. Staphylococcus aureus bloodstream infections: threat elements, outcomes, and the affect of methicillin resistance in Calgary, Canada, 2000-2006. Invasive methicillin-resistant Staphylococcus aureus infections in the United States. Evaluation of the national Cleanyourhands campaign to cut back Staphylococcus aureus bacteraemia and Clostridium difficile infection in hospitals in England and Wales by improved hand hygiene: four year, potential, ecological, interrupted time sequence study. Significant reductions in methicillin-resistant Staphylococcus aureus bacteraemia and medical isolates associated with a multisite, hand hygiene culture-change program and subsequent profitable statewide roll-out. Curbing methicillin-resistant Staphylococcus aureus in 38 French hospitals via a 15-year institutional management program. Epidemiology, microbiology and mortality associated with community-acquired bacteremia in northeast Thailand: a multicenter surveillance study. Community-acquired bacteremia among kids admitted to a rural hospital in Mozambique. Staphylococcus aureus bacteraemia in Iceland, 1995-2008: changing incidence and mortality. Population-based epidemiology of Staphylococcus aureus bloodstream infection in Canterbury, New Zealand. Trends and outcome of nosocomial and community-acquired bloodstream infections end result of} Staphylococcus aureus in Finland, 19952001. Community-associated strains of methicillin-resistant Staphylococcus aureus and methicillin-susceptible S. Impact of ethnicity and socio-economic status on Staphylococcus aureus bacteremia incidence and mortality: a heavy burden in indigenous Australians. Staphylococcus aureus bacteraemia at Alice Springs Hospital, Central Australia, 2003-2006. Prospective study of 424 circumstances of Staphylococcus aureus bacteraemia: determination of things affecting incidence and mortality. Prospective study of 125 circumstances of Staphylococcus aureus bacteremia in kids in New Zealand. Human immunodeficiency virus infection and other threat elements for pores and skin abscesses and endocarditis among injection drug customers.
Coumadin 2 mg
Other related past medical historical past included diabetic foot an infection, hypertension, dyslipidemia, and ex-smoker (22. Relevant prior medicine at the time of randomization included bezafibrate 200 mg day by day, enalapril 10 mg day by day, and furosemide 20 mg day by day. On Day 81, the topic had an infected ulcer on his left foot with discoloration of toes, and was hospitalized for remedy. The subject was treated for peripheral arterial occlusive illness with aspirin 300 mg day by day, ongoing from Day 127. On that day, the topic had ache in his left leg with discoloration of the first and second toes, was hospitalized with a working prognosis of sentimental tissue an infection, and was treated with ceftriaxone, metronidazole, and dipyrone. On Day 174, the topic skilled a critical antagonistic occasion of peripheral artery occlusion (peripheral arterial occlusion). This occasion was thought-about critical end result of|as a outcome of} hospitalization was required or extended, and since persistent or vital incapacity or incapacity was involved. On Day 184, the topic underwent supracondylar amputation of the left leg, and on Day 188 he was discharged. At discharge, the stump of the left leg was clear and bandaged, the sutures had been nicely apposed with no blood or exudate, and the skin was pink. At the time of discharge, he was prescribed diclofenac and acetaminophen (doses and dates not provided). The occasion of peripheral arterial occlusive illness resolved, with a sequela of strolling incapacity, on Day 184. The subject accomplished Phase A of the study and entered Phase B, and the topic accomplished Phase B on Day 364. Other related past medical historical past included diabetic neuropathy, coronary artery illness, cardiac catheterization, hypertension and dyslipidemia. Relevant prior medicine at the time of randomization included pregabalin a hundred and fifty mg day by day, aspirin 81 mg day by day, lisinopril 10 mg day by day and amlodipine 2. On Day 352, the topic skilled a critical antagonistic occasion of cellulitis of right great toe. On Day 352, the topic injured his right great toe causing redness and some bleeding. The subject had absent protecting and epicritic sensation within the decrease extremities, with dorsalis pedis and posterior pulses faintly palpable bilaterally. An X-ray showed no acute fracture or dislocation, however vascular calcifications had been noted. The subject was admitted to the hospital with cellulitis and treated with intravenous piperacillin/tazobactam and clindamycin. On Day 353, a nuclear magnetic resonance imaging advised early osteomyelitis within the distal phalanx of the first digit. There was no drainable fluid assortment, and delicate tissue swelling was noted around the forefoot. An evaluation of the decrease extremity arterial system was performed bilaterally using Doppler ultrasonography revealing scattered atherosclerotic illness with peripheral vascular illness of the decrease extremities. The anterior tibial, posterior tibial, and peroneal arteries had been monophasic to the ankle. During the procedure, pus was found to be draining from the distal tuft of the best first distal phalanx. A phalangectomy was performed and the complete bone was revealed to be utterly eroded and osteomyelitic with pus emanating from the medullary canal of the bone. The subject was treated submit operatively with antibiotic, anti-inflammatory, and analgesic medicines during hospitalization (medications, study days, and doses unknown). The occasion of cellulitis resolved on Day 358, and the topic was discharged from hospital on Day 359. Other related past medical historical past includes cardiac failure chronic, dyslipidemia, hypertension, myocardial ischemia, peripheral venous illness, and diabetic neuropathy. Relevant prior medicine included rosuvastatin 10 mg day by day, carvedilol thirteen mg day by day, amlodipine (+) valsartan 5/160 mg day by day, rilmenidine 1 mg day by day, and indapamide 1. She was really helpful to bear right decrease extremity amputation which she declined. The subject was treated with ciprofloxacin 400 mg day by day from Day one hundred twenty ongoing for prophylaxis of an infection. Physical examination at the time revealed blood stress of 200/120 mmHg, heart rate of 100 bpm, arrhythmic cardiac sounds, bilateral subcrepitant rales, absent peripheral pulse of tibial and periosa arteries, and right foot gangrene. Echocardiography revealed stage 3 mitral regurgitation, stage 2 tricuspid regurgitation, and reasonable secondary pulmonary hypertension. Based on chest X-ray, and thoracic surgery consultation, left pleurisy was present, and left thoracentesis was performed. The worsening of cardiac failure was thought-about to be attributable to the toe amputation on Day 101. The subject was treated with spironolactone 50 mg day by day from Day one hundred twenty ongoing and furosemide forty mg day by day from Day one hundred twenty ongoing. No medicine remedy for the occasion of glomerular filtration rate decreased was indicated. The end result of the occasion of glomerular filtration rate decreased was unknown on Day 161. His related medical historical past included anemia, angina pectoris/stent placement, peripheral arterial occlusive illness, diabetic neuropathy, foot deformity, hyperlipidemia, hypertension/hypertensive heart illness, and diabetic retinopathy. Relevant medicines included rosuvastatin, nebivolol, isosorbide mononitrate, calcium dobesilate, ticlopidine, pentoxifylline, furosemide, and indapamide. The condition was treated with clindamycin and amoxicillin/clavulanic acid from Day 30 by way of 58 (dose, unit and frequency not available), betahistine, and bandaged with betadine. Other related past medical historical past included aortic dysfunction, polyneuropathy, spinal ache, dyslipidemia, myocardial infarction, peripheral artery bypass, peripheral ischemia, toe operation, peripheral venous illness, and current smoking behavior of 18 cigarettes per day (11. Relevant prior medicine at the time of randomization included metoprolol, sulodexide, nafronyl oxalate, diosmin (+) hesperidin, and aspirin. On Day 250, the topic presented with ache of the decrease extremities and was hospitalized. The second digit on the left decrease extremity was perfused with skin trophic dysfunction and a reddening within the instep, no fluctuation. The subject was treated with clopidogrel bisulfate seventy five mg day by day and pentoxifylline 800 mg day by day from Day 250 till ongoing and clindamycin 900 mg day by day from Day 250 by way of 266. On Day 252, a distal left femoral-popliteal bypass of the left decrease extremity was performed, and the second toe of the left decrease extremity was amputated. The subject had a chronic obstruction of bilateral superficial femoral artery, and there was vital stenosis of the popliteal artery over 70% and gangrene on the second toe of the left decrease extremity. The gangrene was associated to progression of ischemic illness of the decrease extremity resulting within the amputation. On Day 260, the occasion of peripheral ischaemia resolved, and the topic was discharged from the hospital. Other related past medical historical past included diabetic polyneuropathy, diabetic angiopathy of decrease extremities, peripheral artery illness, and ex-smoker (36 pack-years). Relevant medicine at the time of randomization included atorvastatin, nebivolol, and aspirin. On presentation at the hospital, physical examination showed swelling and redness of the left foot and blackening of the second toe on the left foot with localized hyperthermia. Relevant medical historical past included dyslipidemia, hypertension and exsmoker (21 pack-years). Relevant medicine at the time of randomization included atorvastatin, enalapril, and amlodipine. Prior to the occasion (Day 194), the topic skilled cellulitis of the left foot that regardless of antibiotic remedy worsened to crucial ischemia. The subject was hospitalized on Day 227 and on Day 228 underwent amputation of the left second toe. The subject received ciprofloxacin, metronidazole, moxifloxacin hydrochloride, acetaminophen (+) tramadol hydrochloride for the events. The subject was hospitalized on Day 405 and on Day 406, an X-ray of the limb revealed thickening of the third proximal phalanx, delicate tissue swelling, and suspected chronic osteomyelitis. The subject received sulfamethoxazole (+) trimethoprim and moxifloxacin hydrochloride for the occasion.

Buy 2mg coumadin
Blinding and Treatment Assignments: Study medications have been usually offered by the Applicant utilizing a double-blind/masking technique. Subjects, investigators, personnel or designees (Covance and Parexel) of the Applicant, remained blinded all through the Phase A double-blind treatment period, while personnel. Generally, the blinding and randomization methods utilized by the Applicant in the respective Phase three trials have been acceptable. Additionally, open-label metformin doses remained unchanged in the course of the double-blind treatment period. Administrative Structure of the Ertugliflozin Development Program Merck and Pfizer co-developed the ertugliflozin Phase three medical development program, with Merck-managed trials conducted with their designee, Covance, and people managed by Pfizer conducted with Parexel. Protocol Procedures and Schedule All Phase three trials included a 2-week placebo run-in period, with scheduled study visits at baseline and Weeks 6, 12, 18, and 26 (Phase A). Depending on the trial, further visits (Phase B) have been scheduled at 4- to 13-week intervals till study completion (see Appendix thirteen. Dietary Restrictions/Instructions: Subjects often acquired counseling on dietary and life-style modifications (in accordance with native medical standards of take care of subjects with T2D) by a dietician or qualified healthcare skilled at screening, and have been requested to follow the recommendations all through the trial. Additional follow-up at subsequent visits might have been carried out by other study personnel responsible for the analysis of the subject. Medications generally utilized by diabetic sufferers or recommended as standard of medical care have been usually allowed. However, secure dosing regimens of antihypertensives, antihyperlipidemics, hormonal contraceptives, and thyroid hormone replacement remedy have been required previous to randomization. Use of medicines that could have an effect on} body weight was not allowed for any of the trials (Table 4), and using of} herbal dietary supplements and pure products was discouraged. Adherence to Study Treatment: the investigator was required to preserve an accountability document of study medications, and subjects have been requested to bring in any used or unused bottles at every visit. Subjects who have been <80% compliant with the treatment routine in the course of the 2-week placebo run-in section have been ineligible to participate in the trial. During the rest of the trial, the significance of adherence to study medications was strengthened for all subjects who have been <80% compliant following randomization. Rescue Medication: Subjects with inadequate glycemic management during Phase A, the double-blind treatment period, have been eligible to obtain open-label rescue medication based on the factors presented in Table 5. Subjects have been requested to continue with the planned study visits and continued to obtain blinded study medication. These subjects also have been required to complete a rescue visit, and continue with their scheduled follow-up visits. In correspondence with the Applicant (dated December 28, 2015, July 29, 2016, and September 30, 2016), the Agency reiterated that the primary efficacy evaluation should use all HbA1c data from all subjects randomized, regardless of treatment adherence and rescue status. Subjects prematurely discontinuing the trial for causes apart from withdrawn consent have been requested to attend a discontinuation visit and a posttreatment follow-up visit/phone call. Study Endpoints Primary Efficacy Endpoint: Mean change from baseline in HbA1c (%) at Week 26 (or Week fifty two for Trial P002/1013) the primary efficacy endpoint for all seven Phase three trials was the change from baseline (randomization) in HbA1c (%). HbA1c is considered an acceptable efficacy endpoint, and a optimistic end result would point out a clinically meaningful profit for the next causes: HbA1c is a widely-accepted, goal, surrogate measure of glycemic management that correlates well with mean blood glucose over the previous 1-3 months. Use of standardized methodology has decreased interlaboratory coefficients of variation to <5%. Secondary Efficacy Endpoints: In addition to the primary efficacy endpoint, the Applicant also evaluated other glycemic endpoints, non-glycemic and pharmacodynamic endpoints. To management for Type I error multiple of} testing, the above secondary efficacy endpoints. Treatment, time, treatment-time interactions, and extra protocol-specified covariates have been used in the model. The regression model included phrases for treatment, baseline HbA1c, and other protocol-specified covariates. The prespecified study-wise type I error rate related to the primary and secondary efficacy endpoints was controlled on the two-sided zero. Cambon for an in depth itemizing of the hierarchical testing order of the primary and secondary endpoints of every trial. The Tipping point evaluation was used to assess how giant the distinction between the non-missing and the lacking data would wish to be to alter the conclusion of the evaluation. He expressed concern with the exclusion of these data by the Applicant for his or her efficacy analyses, as these results might not reflect the actual efficacy findings should the entire subjects who participated in the trial and the entire data following rescue remedy have been included in the analyses. Therefore, he reanalyzed the primary and key secondary efficacy endpoints utilizing all available data, including HbA1c data measurements collected after rescue or discontinuation. They observe that the next medical investigators/subinvestigators had reportable financial interests/arrangements to (b) (6) disclose:, who participated in Trials P005/ (b) (6) and P006/ (b) (6). Across the Phase three medical program, major protocol deviations have been reported in roughly 24% to 48% of subjects. In their submit hoc analyses of Study P001/1016 (the devoted reasonable renal impairment trial), the Applicant famous that metformin might have been utilized in violation of the protocol. Approximately 17% of subjects included in the Week 26 HbA1c evaluation might have been uncovered to metformin, based on the discovering of at least of|no less than} one optimistic assay end result. The Applicant felt that this will have confounded the primary (b) (4) efficacy findings, leading to a failed trial. Demographics and Clinical Characteristics A complete of 4859 have been randomized and treated into the seven Phase three trial, of 1450 subjects acquired placebo or energetic comparator, 1716 subjects acquired ertugliflozin 5 mg, and 1693 subjects acquired ertugliflozin 15 mg. Relevant demographics and baseline medical characteristics of the all treated topic populations for these trials are presented in Table 7. Rates for the individual research have been reported as follows: Trial P003/1022: No subjects (0/461) Trial P005/1019: 1% (12/1232) of subjects Trial P007/1017: 1% (6/621) of subjects Trial P001/1016: 1. Concomitant Medications: Concomitant medications usually used as standard of care with T2D are presented in Table 7 above. Across the Phase three trials, antihypertensive (48-94% of subjects) and antihyperlipidemic medications (32-78% of subjects) have been generally utilized by subjects. Use of these medications was allowed in the respective protocols, much like other antihyperglycemic development applications. However, subjects have been to have been on secure doses of these medications earlier than and in the course of the trials. Rescue Medication Use: Glycemic rescue criteria have been prespecified as described above (Section 6. This may end result in the analysis of only those subjects who achieved a therapeutic response or tolerated remedy. Cambon famous that rescue medication was used earlier than the ultimate HbA1c efficacy assessment by 0% up to as} 31. N consists of all randomized, treated sufferers who had at least of|no less than} one measurement of the end result} variable. Cambon concluded the next for the primary endpoints: Superiority of ertugliflozin 15 mg and ertugliflozin 5 mg comparability with} placebo was demonstrated for the primary endpoint (HbA1c change from baseline to Week 26) for the four placebo-controlled trials: P003/1022, P007/1017, P006/1015, and P017/1047. Superiority was demonstrated at Week 26 for the primary endpoint in the full factorial trial (P005/1019) for the ertugliflozin 15 mg plus sitagliptin one hundred mg arm vs. For the factorial trial (P005/1019), both ertugliflozin/sitagliptin treatment arms. For the sixth trial (P003/1013), noninferiority with glimepiride was only achieved for the ertugliflozin 15 mg treatment arm. Durability of Response For six of the seven trials, the primary endpoint was assessed at 26 weeks. These trials allowed subjects to take part in a 26- to 78-week site- and subject-blind long-term treatment period (Phase B). Cambon requested further analyses from the Applicant and conducted several of} sensitivity analyses of the primary efficacy endpoint (data not shown). Please discuss with his Statistical Review for detailed dialogue of the sensitivity analyses carried out to support the findings of the primary efficacy evaluation. Cambon also carried out subgroup analyses (based on the next intrinsic elements: intercourse, race, age, and geographic region) of a pool of 4 Phase three trials. The pooled subgroup analyses (dated September sixteen, 2017) yielded comparable results to those conducted by Dr. The medical relevance of these nominal adjustments is unsure, nevertheless it does suggest that the 15 mg dose of ertugliflozin presents a profit for some sufferers above what could be seen with the 5 mg dose. All seven Phase three medical trials included a 26- to 52-week double-blind treatment period. This trial also consists of three 18-week sub-studies that evaluate the efficacy of ertugliflozin in subjects receiving background insulin with or without metformin, background sulfonylurea monotherapy, and background metformin plus a sulfonylurea. Since these antihyperglycemic agents are generally used as mixture remedy for sufferers with T2D, the findings from these sub-studies might assist to decide the potential profit and dangers associated with ertugliflozin utilized in mixture with these medications.
Proven 2mg coumadin
This condition has been acknowledged at least of|no much less than} as far back as|way again to} the nineteenth century, however its distinctive name was utilized within the first edition of this monograph (1966), reflecting the implications of this condition for the prognosis of coma and for the specialized care such patients require. Although not unconscious, locked-in patients are unable to reply to most stimuli. The most common trigger is a lesion of the base and tegmentum of the midpons that interrupts descending cortical management of motor features. Such patients normally retain management of vertical eye movements and eyelid opening, which can be utilized to verify their responsiveness. It is necessary to establish locked-in patients in order that they might be handled appropriately by the medical and nursing staff. At the bedside, discussion must be with the affected person, not, as with an unconscious individual, about the affected person. Patients with giant midpontine lesions typically are awake , with greatly diminished sleep on physiologic recordings. As the above definitions suggest, each of these conditions includes a fairly big selection of behavioral responsiveness, and there may be be} some overlap among them. Subacute or Chronic Alterations of Consciousness Dementia defines an everlasting and sometimes progressive decline in mental processes owing to an organic course of not normally accompanied by a discount in arousal. Conventionally, the term implies a diffuse or disseminated discount in cognitive features rather than the impairment of a single psychologic activity corresponding to language. The development of quantity of} cognitive defects manifested by both: (1) Memory impairment (impaired capacity to be taught new info or to recall previously discovered information); (2) One (or more) of the next cognitive disturbances: aphasia (language disturbance), apraxia (impaired capacity to carry out motor activities regardless of intact motor function), agnosia (failure to recognize or establish objects regardless of intact sensory function), disturbance in executive operate. Usually, the term dementia is utilized to the results of primary disorders of the cerebral hemispheres, corresponding to degenerative conditions, traumatic accidents, and neoplasms. Patients with dementia are normally awake and alert, however as the dementia worsens, might become much less responsive and finally evolve right into a vegetative state (see below). Patients with dementia are at significantly increased threat of developing delirium once they become medically sick or develop comorbid mind disease. Hypersomnia refers to a state characterised by extreme however normal-appearing sleep from which the subject readily, even when briefly, awakens when stimulated. Many patients with both acute or persistent alterations of consciousness sleep excessively. In the truly hypersomniac affected person, sleep seems normal and cognitive features are normal when patients are awakened. Hypersomnia results from hypothalamic dysfunction, as indicated later in this chapter. Abulia is normally related to bilateral frontal lobe disease and, when extreme, might evolve into akinetic mutism. Akinetic mutism describes a condition of silent, alert-appearing immobility that characterizes certain subacute or persistent states of altered consciousness in which sleep-wake cycles have returned, however externally obtainable evidence for mental activity stays virtually completely absent and spontaneous motor activity is missing. Such patients usually have lesions together with the hypothalamus and adjoining basal forebrain. For an in depth discussion of the clinical standards for the prognosis of the minimally acutely aware state, see Chapter 9. Very few surviving patients with extreme forebrain injury stay in eyes-closed coma for greater than 10 to 30 days. Patients within the vegetative state, like comatose patients, present no evidence of awareness of self or their surroundings. Unlike mind demise, in which the cerebral hemispheres and the brainstem both endure overwhelming useful impairment, patients in vegetative states retain brainstem regulation of cardiopulmonary operate and visceral autonomic regulation. Other phrases within the literature designating the vegetative state include coma vigil and the apallic state. Brain demise is outlined as the irreversible lack of all features of the whole mind,14 such that the body is unable to maintain respiratory and cardiovascular homeostasis. Although vigorous supportive care might hold the body processes going for a while, notably in an Table 1�2 Terms Used to Describe Disorders of Consciousness Acute Clouding Delirium Obtundation Stupor Coma Locked in (not coma; see text) Subacute or Chronic Dementia Hypersomnia Abulic Akinetic mutism Minimal consciousness Vegetative Brain demise Pathophysiology of Signs and Symptoms of Coma 9 in any other case wholesome young person, the lack of mind operate finally leads to failure of the systemic circulation inside a few of} days or, hardly ever, after quantity of} weeks. That the mind has been lifeless for a while prior to the cessation of the heartbeat is attested to by the fact that|the truth that} the organ in such cases is normally autolyzed (respirator brain) when examined postmortem. The clinician should determine rapidly whether the impairment is structural or metabolic, and what treatments should be instituted to save the lifetime of the affected person. Since the final edition of this monograph in 1980, there was a revolution in mind imaging. In applicable clinical circumstances, if the preliminary examination suggests structural mind injury, a scan might establish the alteration of consciousness and dictate the therapy. If coma is structural, it usually as a result of|as a outcome of} of} a focal injury along the course of the neural pathways that generate and maintain a normal waking mind. Therefore, the clinical prognosis of structural coma decided by} the popularity of the indicators of injury to buildings that accompany the arousal pathways by way of the mind. Structural processes that impair the operate of the arousal system fall into two classes: (1) supratentorial mass lesions, which may compress deep diencephalic buildings and hence impair the operate of both hemispheres, and (2) infratentorial mass or destructive lesions, which immediately injury the arousal system at its source within the upper brainstem. The the rest of Chapter 1 will systematically look at the main arousal systems within the mind and the physiology and pathophysiology of consciousness. Chapter 2 addresses examination of the affected person with a disturbance of consciousness, notably those elements of the examination that assay the operate of the arousal systems and the main sensory, motor, and autonomic systems that accompany them. Once the examination is accomplished, the examiner ought to ready to|be capable of|have the ability to} determine whether the source of the impairment of consciousness is brought on by a structural lesion (Chapters 3 and 4) or a diffuse and due to this fact presumably metabolic course of (Chapter 5). Although query members of the family or attendants who might have particulars of the historical past, together with emergency medical personnel who bring the affected person into the emergency division, the historical past for comatose patients is usually scant or absent. The key elements of the examination, which could be accomplished by a skillful doctor in only a few minutes, include (1) the level of consciousness of the affected person, (2) the pattern of breathing, (3) the size and reactivity of the pupils, (4) the attention movements and oculovestibular responses, and (5) the skeletal motor responses. From this info, the examiner should ready to|be capable of|have the ability to} reconstruct the type of|the kind of} the lesion and transfer swiftly to lifesaving measures. Only from this angle is it potential to understand how the elements of the coma examination check pathways that are be} intertwined with those that maintain consciousness. Box 1�1 Constantin von Economo and the Discovery of Intrinsic Wake and Sleep Systems within the Brain Baron Constantin von Economo von San Serff was born in 1876, the son of Greek parentage. He was introduced up in Austrian Trieste, studied drugs in Vienna, and in 1906 took a post within the Psychiatric Clinic under Professor Julius von Wagner-Jauregg. In 1916 throughout World War I, he began seeing cases of a brand new} and previously unrecorded sort of encephalitis and printed his first report of this sickness in 1917. Although subsequent accounts have typically confused this sickness with the epidemic of influenza that swept by way of Europe after which the rest of|the the rest of} the world throughout World War I, von Economo was fairly clear that encephalitis lethargica was not related to respiratory symptoms, and that its appearance preceded the onset of the latter epidemic. Von Economo continued to write and lecture about this experience for the remainder of his life, until his untimely demise in 1931 from heart disease. Based on his clinical observations, von Economo proposed a dual center concept for regulation of sleep and wakefulness: a waking influence arising from the upper brainstem and passing by way of the gray matter surrounding the cerebral aqueduct and the posterior third ventricle; and a rostral hypothalamic sleeppromoting space. These observations turned the idea for lesion studies done by Ranson in 1939,20 by Nauta in 1946,21 and by Swett and Hobson in 1968,22 in which they showed that the posterior lateral hypothalamic lesions in monkeys, rats, and cats may reproduce the prolonged sleepiness that von Economo had observed. The rostral hypothalamic sleep-promoting space was confirmed experimentally in rats by Nauta in 194621 and in cats by Sterman and Clemente within the 1960s. A photograph of Baron Constantin von Economo, and excerpts from the title page of his lecture on the localization of sleep and wake selling systems within the mind. He noted that additionally they had attacks of cataplexy in which they misplaced all muscle tone, typically when excited emotionally. Von Economo noted precisely that these symptoms were just like the uncommon condition previously identified by Gelinaux as narcolepsy. Wilson even described inspecting a affected person in his workplace, with the young home officer McDonald Critchley, and that the affected person certainly had atonic paralysis, with lack of tendon reflexes and an extensor plantar response in the course of the assault. A corollary was that consciousness may solely be eradicated by lesions that simultaneously damaged both cerebral hemispheres. The nascent field of neurosurgery also began to contribute cases in which lack of consciousness was related to lesions confined to the upper brainstem or caudal diencephalon. However, essentially the most convincing body of evidence was assembled by Baron Constantin von Economo,19 a Viennese neurologist who recorded his observations throughout an epidemic of a unique dysfunction, encephalitis lethargica, that occurred within the years surrounding World War I. Most victims of encephalitis lethargica were very sleepy, spending 20 or extra hours per day asleep, and awakening solely briefly to eat. When awakened, they might work together in a relatively unimpaired trend with the examiner, however quickly fell asleep if not constantly stimulated.
References:
- https://cpb-us-w2.wpmucdn.com/u.osu.edu/dist/5/1926/files/2016/02/Dictionary-Biology-1s0uug7.pdf
- https://www.lls.org/sites/default/files/file_assets/lymphomaguide.pdf
- https://www.ecdc.europa.eu/sites/default/files/documents/novel-coronavirus-risk-assessment-china-31-january-2020_0.pdf