.png)
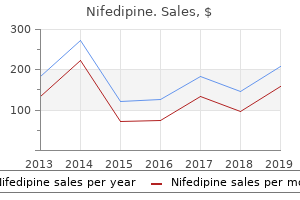
Proven nifedipine 30 mg
Metabolic disturbances, cerebral infection, encephalitis, meningitis, sepsis, or thyrotoxicosis wants to|must also} be thought-about. End-organ complications similar to ulcers, hepatitis, cirrhosis, pancreatitis, cardiomyopathy, or peripheral neuropathy should prompt consideration of alcoholism as an underlying trigger. Recurrent trauma, particularly skeletal fractures, sleep issues, fatigue, depression, sexual dysfunction, and labile hypertension, wants to|must also} arouse suspicion of alcoholism. Hospitalization may precipitate the surprising appearance of an alcohol withdrawal syndrome within several of} days of admission. Because advice and dialogue by a involved physician are simple, cost-effective ways to cut back heavy ingesting, routine screening for alcohol issues is beneficial, particularly in main care. Complex ethanol-drug interactions should also be thought-about when prescribing drugs to sufferers who use alcohol. Ethanol potentiates the central nervous system depressant results of narcotic, sedative, and psychoactive drugs (see Chapter 26), and sufferers for whom these brokers are prescribed must be counseled explicitly about this interaction. In distinction, the induction of microsomal enzymes within the liver by ethanol accelerates the elimination of drugs metabolized by these enzymes (see Chapter 26). As a outcome, ethanol can lower drug efficacy by lowering the amount of active drug available or improve toxicity and promote unusual unwanted side effects} caused by drug metabolites. Severe acute alcohol intoxication, outlined by a depressed stage of consciousness, may be deadly and is a medical emergency. The instant historical past should embrace information about the quantity of alcohol consumed, the speed of ingesting, use of different drugs including methanol and ethylene glycol, complicating medical and psychiatric issues, and prior alcohol abuse or alcoholism. If the patient is stuporous and unable to walk, the airway should be evaluated instantly. Indications for endotracheal intubation and assisted air flow embrace marked hypoventilation, accumulating secretions, or coma. Complications similar to hypoglycemia, meningitis, subdural hematoma, and hepatic encephalopathy should be thought-about. Evidence of head trauma or focal cerebral signs suggests urgent intracranial pathology, and a computed tomography scan must be performed instantly. Gastric lavage may be be} performed if the obtundation {is due to|is of} current and big alcohol consumption, but it should be preceded by endotracheal intubation. Hemodialysis must be thought-about if the blood alcohol focus exceeds 500 mg/dL or when methanol or ethylene glycol has been ingested concurrently. After a historical past and physical examination, sufferers with sufficient vital signs and acceptable psychological status however without evidence of different issues may be kept calm beneath statement till sobriety returns. Routine blood counts and laboratory studies may uncover anemia (see Chapter 159), hypokalemia, hypophosphatemia, and hypomagnesemia. Alcoholic hypoglycemia (see Chapter 243) may be evaluated quickly by a bedside blood glucose willpower. Alcoholic ketoacidosis (see Chapter 102) will be improved by infusion of 5% dextrose in half-normal saline, additionally with thiamine. Alcoholics cease ingesting so much of} reasons, including serious alcohol-related medical, surgical, or psychiatric situations. Hence signs or signs of trauma, infection, liver illness, gastritis, pancreatitis, arrhythmia, or electrolyte disturbance must be sought. The alarming signs of ethanol withdrawal are best managed by substituting one other central nervous system depressant. However, alcoholics undergoing withdrawal are very immune to sedatives (cross-tolerance), so massive doses are often required to calm their agitation. Benzodiazepines are broadly used to manage tremulousness and disordered perceptions during ethanol withdrawal. The goal is to suppress signs and produce gentle sedation, and the drug dosage is adjusted to the severity of the withdrawal response. Treatment includes managing delirium and autonomic stability and preventing seizures. A sedative-hypnotic agent, usually a benzodiazepine, is prescribed as various to|an different alternative to} alcohol, and the dose is tapered over several of} days. Patients with gentle tremulousness and few associated signs usually respond to oral diazepam, 5 to 10 mg each four to 6 hours. The dosage is then reduced by 20 to 25% on successive days or increased if signs of ethanol withdrawal return. Detoxification may be carried out with shut monitoring in an outpatient setting in socially stable sufferers with gentle withdrawal. If withdrawal is more severe or accompanied by significant medical, surgical, or psychiatric sickness or the patient is in an unstable social setting, inpatient detoxing may be be} wanted. In such instances, benzodiazepines similar to diazepam (Valium), chlordiazepoxide (Librium), oxazepam (Serax), or lorazepam (Ativan) are administered orally or parenterally in doses enough to keep the patient calm. Patients may require hourly treatment at doses that might be deadly in non-tolerant individuals. The first several of} days of severe alcohol withdrawal may require intravenous administration of complete day by day diazepam doses exceeding four hundred mg (or the equal of different benzodiazepines) to obtain gentle sedation. Multivitamin and thiamine supplementation must be continued, as should meticulous attention to electrolyte status. The benzodiazepine dosage can then be tapered by approximately 20 to 25% on successive days, with an increase in dosage if withdrawal signs recur. Alcohol withdrawal seizures can typically be managed with intravenous benzodiazepines similar to diazepam or lorazepam. Management of status epilepticus is the same as in different conditions (see Chapter 484). Alcoholics are at increased danger for head trauma and central nervous system infection; studies to exclude these more serious diagnostic possibilities must be performed when seizures occurring within the setting of withdrawal show focal options or are accompanied by a chronic post-ictal state or when status epilepticus intervenes. Delirium tremens requires hospitalization and vigorous management in an intensive care setting. Mortality has reached 15% in the past, primarily due to injuries or associated medical issues sophisticated by hyperthermia and dehydration. Volume depletion accompanying delirium tremens may trigger circulatory collapse, and fluid losses can require substitute of four to 10 L within the first day. The goal of remedy is to control behavior and suppress signs without hazard to the patient. Five to 10 mg or more of diazepam is given intravenously each 5 to 15 minutes till the patient is calm, and maintenance remedy is sustained each 1 to four hours, as wanted. Initially, as much as 200 mg of diazepam may be be} required before the agitation subsides. Seizures are unusual in sufferers with delirium tremens and must be evaluated promptly due to the possibility of|the potential of|the potential for} meningitis or different issues. Coexisting hepatic and cardiac illness may complicate fluid management, and the chance that sedative brokers may precipitate hepatic encephalopathy must be kept in thoughts. Alcoholics and alcohol abusers come to medical attention due to alcohol-related medical or psychiatric situations, by referral from social service or criminal justice agencies, or by way of screening in medical follow. Physicians should confront alcoholics in a firm however non-judgmental style, educate them about health dangers, and assess their motivation to cease ingesting (see Fig. It is efficacious to establish a contract with the patient to lower ingesting and return for follow-up assessments. Alcoholics must be referred to a rehabilitation program however may first require inpatient detoxing. Intervention is more effective earlier in the course of of|in the midst of} the sickness, before the onset of associated medical issues. Many alcohol-related medical complications similar to ulcer illness, acute pancreatitis, hepatitis, myopathy, and neuropathy stabilize or regress with continued abstinence. Others similar to cirrhosis with portal hypertension, Wernicke-Korsakoff syndrome, or dilated cardiomyopathy regularly trigger permanent disability or demise. About half of socially stable, middle-class alcoholics remain sober for at least of|no much less than} a year after rehabilitation. Alcoholics Anonymous and Al-Anon provide low-cost support for alcoholics and their households in nearly all communities within the United States. A helpful evaluate of the pathophysiology, remedy objectives, and drugs options for alcohol withdrawal and dependence. A comprehensive dialogue of the most important biomedical and socioeconomic issues of alcoholism and alcohol abuse. Medical complications of drug abuse are predominantly infectious however span organ techniques and vary from cocaine-related cardiac arrhythmia to the neuropsychiatric results of hallucinogens. The terms drug (or substance) "dependence" and drug "abuse" have particular medical meanings (Table 17-1).
Order nifedipine 30 mg
Breakthroughs in infectious ailments, the regulation of blood stress, fundamental immunology, fundamental genetics, and metabolic regulation by hormones symbolize milestones in the middle of|in the midst of} medical history that now present the instruments to help unravel the intricacies of human disease. Nonetheless, the clues now being ferreted out at the molecular stage anticipate options of even these issues, realistically filling future expectations with pleasure and anticipation. The scientific infrastructure that we recognize today is the springboard for the longer term run} in which many of the readers of Cecil Textbook of Medicine, 21st edition, will follow. However, this case has entirely modified: By one hundred fifty years in the past things have been beginning to change, and by the 20 years spanning the turn of the century, the first fundamental lights began to illuminate the "golden age of microbiology. To define microorganisms, to understand how they cause infection and transmit ailments, and to understand the host response represented a turning point and forever established the scientific methodology as the basis for understanding and treating disease. It is a tremendous experience to read the scientific papers from Paris and Berlin at the moment as a result of|as a result of} in a comparatively short period these two schools of thought set us on a pathway from which medication can by no means depart-that of demanding precision, of requiring experimental proof, and of building confidence by accumulating irrefutable information. It is precision based mostly on a century or extra of refining definitions of disease in highly specific phrases. We now experience these "golden ages" in more rapid order: the discovery of antibiotics lower than 60 years in the past; an understanding of immunology in molecular phrases 2 inside the last 30 years; and now in genetics, not simply data at the molecular stage, however understanding the way to|tips on how to} manipulate genes for the quick benefit of about} mankind. We are indeed within the age of molecular-biophysical medication, an influence that permeates and unifies all the traditional disciplines of medicine. Whether one is talking about inborn errors of metabolism, neurotransmitters, cytokines, oncogenes, or hormone regulation, all are being defined with exquisite detail at the molecular stage. The capacity to define each gene, its product, and its role and explicit perform has turn out to be a shared international aim. Concurrent with these advances in fundamental human biology has been a dramatic shift within the methods for evaluating the appliance of scientific advances to the patient and to populations. As studies progress from people who demonstrate biologic impact, to people who elucidate dosing schedules and toxicity, and finally to people who assess true clinical benefit, the metrics of measuring outcome have additionally improved from subjective impressions of physicians or sufferers to reliable and valid measures of morbidity, quality of life, functional status, and other patient-oriented outcomes. These marked improvements within the scientific methodology of clinical investigation have expedited extraordinary modifications in clinical follow, similar to reperfusion therapy for acute myocardial infarction, and have demonstrated that reliance on intermediate outcomes, similar to a discount in asymptomatic ventricular arrhythmias with sure drugs, might unexpectedly increase somewhat than decrease mortality. Just because the physician for the twenty-first century must understand advances in fundamental biology, a similar understanding is required of the basics of clinical research design because it applies to diagnostic and therapeutic interventions. Advances in molecular and structural biology and the wonders of immunology and genetics must not permit us to neglect the numerous features of human psychology, anthropology, and sociology that influence the world in which we reside and that play such a major role in morbidity and eventual mortality. According to the National Center for Health Statistics, behavioral causes-including alcohol, drugs, violence, suicide, smoking, and extreme aggression-generate more than half the fee to the nation for health care. We are only simply beginning to grasp the impact of those components on our nation and the world. In our joy-and sometimes boastful pride-over achievements in molecular medication and randomized managed trials, we must additionally humbly realize that the sciences that analyze human or population behavior and try and improve it, properly as|in addition to} the best way|the method in which} that society is structured, are indispensable to medication and have to be incorporated into the self-discipline of our profession. Biomedical science becomes the working instrument for the physician who, by definition, practices an analytic profession. Most of those learned expertise prolong to the administration of particular person circumstances at the bedside, i. A central tenet of all sciences is to continually ask, "Could my conclusion be wrong? The explosion in medical data has led to increasing specialization and subspecialization, defined initially by organ system and extra recently by locus of principal exercise (inpatient as in contrast with outpatient), reliance on guide expertise (proceduralist as in contrast with nonproceduralist), or participation in research. Every physician must enjoyment of learning the brand new}, correcting the old, and perfecting the longer term run}. Much of what medication now accomplishes is determined by} large-scale testing of procedures, interventions, vaccines, and new drugs. The truth that|proven reality that} many such studies have to be conducted in large populations via a multicenter approach provides an opportunity for all physicians to participate in clinical investigation ultimately at some time of their professional careers. Indeed, this step is important for medication and for physicians to move ahead together as a profession. The patient-physician interaction proceeds via quantity of|numerous|a selection of} phases of clinical reasoning and determination making. The interaction begins with an elucidation of complaints or considerations, adopted by inquiries or analysis to address these considerations in increasingly exact ways. The course of generally requires a careful history or physical examination, ordering of diagnostic tests, integration of clinical findings with the check outcomes, understanding of the dangers and advantages of the possible courses of action, and careful consultation with the patient and family to develop future plans. Physicians can increasingly name on a growing literature of evidence-based medication to guide the method so that benefit is maximized while respecting particular person variations amongst totally different sufferers. New information, new methods, and new expertise could be brought into the method and their contribution evaluated in a conceptualization of the scientific methodology often termed steady quality enchancment. Through such fixed commitment to advancing the frontiers of medicine, physicians improve health, uncover true cures, devise new ways of delivering care, and cut back ultimate health costs. A physician can diagnose and prescribe in a technically right and scientific, however insensitive method. The patient made better, even cured, however still really feel unsatisfied with the interaction. In these circumstances, sufferers are probably to|prone to} ask the questions: Does my physician actually care? They need their physicians to be excited about them as people who search advice, properly as|in addition to} reduction from ache, disease, and suffering. Easy, supportive interaction with sufferers and others less lucky is a talent that comes readily for some and with great difficulty for others. In learning the way to|tips on how to} demonstrate compassion, Kahlil Gibran taught us: "You give however little whenever you give of your possessions-it is whenever you give of yourself that you just truly give" (The Prophet). The giving of oneself with ease, with grace, and with that means is, for many persons, an acquired talent. Nevertheless, these traits stay imperatives if the aim is to turn out to be a "full physician. Patients must consider that their physicians care about them as folks, not simply as sufferers. Physicians, in turn, must understand that they do much better as professionals if they that they} err on the aspect of being human with their sufferers. Dag Hammarskjold advised us of "the humility that comes from others having religion in you. This commitment continues beyond a single insightful diagnosis or the completion of a procedure. The patient still needs care when the info come back from the clinical laboratory, the radiology division, the cardiac catheterization laboratory, or the surgical pathology laboratory. Patients continue to need help in understanding their disease, in coping with family interactions, and find a caring ear once they suffer most. They often need help in acquiring essential extra medical help from specialists or consultants and personal help in coping with processes involving households and personal situations. A notably troublesome time comes as physicians cope with sufferers who turn out to be old, frail, dependent, crippled, or cognitively impaired. These are the circumstances from which essentially the most delicate amongst us truly learn what it means to give of ourselves. A commitment to the highest requirements of excellence within the follow of medicine and within the technology and dissemination of knowledge. A commitment to the attitudes and behaviors that maintain the pursuits and welfare of sufferers. Professionalism aspires to altruism, accountability, excellence, duty, service, honor, integrity, and respect for others. The interest of the patient lies above self-interest-an indispensable attribute not only of medicine however of all professions. It has to do with our private behavior transcending our technical skills, our scientific data, and even our attitudes of compassion and caring. What it means is that we offer to others a special sensitivity-whether they be physician colleagues, students, residents, nonphysician caregivers, sufferers, or their households. To stay professionals, dignity and understanding must permeate all our interactions-all our pondering, teaching, learning, and listening. As they cross into residency, the avenues of participation turn out to be an increasingly unbiased course of coaching. In this intellectual experience of growing independence, younger physicians analyze information, manage it, render compassionate and considered care, and cope with their professional colleagues, properly as|in addition to} with sufferers and their households. This historical independence of thought and action can make it troublesome for a lot of} physicians who shall be coming into follow in the future to understand that the evolving modifications within the health care delivery system will unavoidably result on} that perceived stage of independence. Patient care within the mass is changing into an enormous enterprise, minimal of|no less than} because it relates to insurers, managed care organizations, and groups of employers.
Best 30mg nifedipine
The requirement for selective ventilation excludes many sufferers with severe pulmonary hypertension or acute respiratory failure. In contrast, many sufferers with chronic respiratory insufficiency and preserved ventilation-perfusion matching will tolerate intervals of selective lung ventilation. The ability of many sufferers with severe emphysema to tolerate selective ventilation has led to the appliance of thoracoscopy for lung volume discount surgery. Obliteration of the pleural house, either from an infection or previous surgery, is a relative contraindication for thoracoscopic surgery. A number of benign lung ailments current as focal parenchymal lesions that require a tissue biopsy for prognosis. The traditional strategy to lung biopsy has been a restricted thoracotomy and wedge resection. As different to|an various choice to|a substitute for} restricted thoracotomies, thoracoscopy has proven to be an efficient strategy to the prognosis of localized problems of the lung. Thoracoscopy can provide a more complete view of the ipsilateral hemithorax, including the visceral, parietal, and mediastinal pleura. Diffuse lung ailments can usually be diagnosed clinically on the basis of history, attribute chest radiographs, bodily findings, and pulmonary function testing. In instances that require histopathologic affirmation, lung tissue can be obtained by transbronchial biopsy. Thoracoscopy plays a restricted function in diffuse lung disease but additionally be} useful when a large pathologic sample is required. In some instances, the speedy growth of these bullae can be associated with a substantial increase in respiratory symptoms and a decrease in expiratory air circulate. Chest radiographs of sufferers with acute respiratory symptoms incessantly reveal compression of surrounding lung tissue. Alternatively, 479 sufferers with bullous lung disease sometimes current with an contaminated bulla and require drainage previous to definitive surgery. The indications for thorascopic bullectomy are much like lung volume discount surgery for emphysema. Patients who benefit most from surgery are those who have rapidly progressive symptoms associated with the growth of a single bullous lesion and radiographic demonstration of compression of the encompassing lung parenchyma. Primary spontaneous pneumothorax (see Chapter 86) is brought on by rupture of subpleural blebs of the lung. In approximately 5% of instances, related subpleural blebs are discovered at the margin of the lower lobe, often within the superior phase. In an otherwise wholesome affected person with lower than a 20% pneumothorax, the uncomplicated pneumothorax can be observed with out intervention. In sufferers with bigger pneumothoraces, a tube additionally be} essential to evacuate the pleural air and re-expand the lung. Most instances of primary spontaneous pneumothorax heal from the irritation associated with pleural rupture and are free of ongoing air leak after re-expansion of the lung. Although most spontaneous pneumothoraces are uncomplicated, three to 20% of sufferers with pneumothoraces develop problems similar to tension pneumothorax, persistent air leaks, or recurrent pneumothoraces. Patients who develop a second pneumothorax have a 70 to 80% chance of a third recurrence inside 2 years. The surgical strategy to the therapy of recurrent pneumothoraces has been the removing of subpleural blebs. These blebs can be successfully removed using a thoracoscopic strategy or through a more traditional axillary incision. Solitary pulmonary nodules or "coin lesions" are defined as spherical lesions, lower than three cm in diameter, current within the outer one-third of the lung (see Chapter 72). Transthoracic needle biopsy has a low morbidity: fewer than 10% of normal sufferers and a slightly higher proportion of sufferers with emphysema will develop a postprocedure pneumothorax. However, a small but tangible false-negative fee happens with transthoracic needle biopsies. Furthermore, within the absence of a malignant prognosis, transthoracic needle biopsies hardly ever are place to} establish a benign prognosis. Thoracoscopic resection of the solitary pulmonary nodule is different to|an various choice to|a substitute for} transthoracic needle biopsy. The drawback of thoracoscopic resection is that it requires common anesthesia; nonetheless, the hospital keep will usually be lower than 24 hours. In most instances of primary lung cancer, a standard anatomic resection is indicated to decrease the incidence of local recurrence. Patients who can tolerate common anesthesia and single lung ventilation for the thoracoscopic resection are usually place to} tolerate the segmentectomy or lobectomy. In sufferers with isolated regional metastases, this staging info may provide important info to guide possible adjuvant remedy. Anatomic resections can be carried out with a variety of|quite so much of|a wide selection of} methods, including video-assisted surgical methods. The distinction between normal lobectomy and a thoracoscopic lobectomy has turn into much less distinct current years|in recent times|lately}. Thoracoscopic instruments have turn into commonplace within the resection of a lobe of the lung, even when carried out through a standard thoracotomy. The improved visualization and smaller instruments have resulted in smaller incisions and less morbidity. This article is a comprehensive examine of the morbidity and mortality of thoracoscopy applied to a spread of lung ailments. A broadly cited randomized examine reporting the higher local recurrence fee of lung cancer with restricted (wedge) resection when compared with anatomic lobectomy. Joint Statement of American Society of Transplant Physicians/American Thoracic Society/European Respiratory Society/International Society of Heart and Lung Transplantation: International Guidelines for the Selection of Lung Transplant Candidates. Recently released consensus assertion concerning guidelines for evaluation and listing of sufferers thought-about for transplantation. Although the respiratory rhythm emerges primarily from neurons within the medulla and pons, these neurons receive afferent enter from quantity of|numerous|a selection of} sources that provide constant details about blood gases. During wakefulness, ventilation is also be|can be} considerably influenced by behavioral activities similar to speech, swallowing, and anxiety. Similarly, decreases in Pa O2 from 500 mm Hg to approximately 65 mm Hg have a negligible effect on respiration; below 65 mm Hg, a hyperbolic relationship happens between decreasing Pa O2 and rising ventilation. Within the normal physiologic range, the pretty weak chemical management system permits comparatively unfettered behavioral management of respiration. Because of the shapes of the ventilatory response curves relative to those of normal blood gases, hypercapnia somewhat than hypoxia stimulates the response to hypoventilation and thereby normalizes blood gases. In clinical conditions in which 480 Figure 90-1 A simplified diagram of the principal efferent (left) and afferent (right) respiratory management pathways. A part through the mind, mind stem, and spinal cord is proven (with pertinent respiratory areas indicated by shading), as are the central nervous system hyperlinks with the respiratory apparatus. Figure 90-2 Typical ventilatory responses to hypercapnia (left) and hypoxia (right). As a outcome, ventilation usually falls in response to this elevated upper airway resistance. First, the event of hypercapnic respiratory failure usually displays an interplay between ventilatory management (often quantified by the slope of the hypoxic and hypercapnic ventilatory responses) and the work of respiration (increments in work of respiration are often a product of parenchymal lung disease or chest wall disease, including obesity). When chemoresponsiveness is markedly diminished or absent, hypercapnia could develop in an individual with a normal respiratory apparatus and normal work of respiration. Therefore, although low or diminished chemoresponsiveness could predispose an individual to hypercapnia, the work required to keep ventilation will usually determine when hypercapnia truly happens. Second, particular person variability in chemoresponsiveness is substantial, with slopes various sixfold or sevenfold from one particular person to another due to genetic variations, previous neurologic disease. Regardless of the trigger, low chemoresponsiveness together with elevated work of respiration contribute to the event of hypercapnic respiratory failure. Acute adjustments in blood gasoline values (over hours), similar to happen with a respiratory an infection, can usually be detected rapidly by a affected person. Conversely, with diminished ventilatory management, hypercapnia and hypoxia could develop slowly, with little sensation of dyspnea, making the early detection of respiratory failure troublesome. Hypoventilation Associated with "Pure" Control of Breathing Abnormalities (without Cardiopulmonary Disease) Hypoventilation can develop in an individual with quite normal lungs and respiratory muscle function but with a markedly diminished ability to respond to hypoxia or hypercapnia. The commonest such dysfunction in adults is acquired central alveolar hypoventilation, which is defined by markedly diminished ventilatory chemoresponsiveness, normal respiratory apparatus (normal pulmonary function), and an absence of obesity or chest wall disease.
Proven nifedipine 30mg
Protist parasites embrace the causative brokers of malaria, African sleeping illness, and waterborne gastroenteritis in humans. Other protist pathogens prey on vegetation, effecting large destruction of food crops. Plasmodium Species Members of the genus Plasmodium must colonize both a mosquito and a vertebrate to complete their life cycle. In vertebrates, the parasite develops in liver cells and goes on to infect red blood cells, bursting from and destroying the blood cells with each asexual replication cycle (Figure 23. In 2010, it was estimated that malaria brought on between one-half and a million deaths, largely in African kids. In response to waste merchandise launched as the parasites burst from infected blood cells, the host immune system mounts a massive inflammatory response with episodes of delirium-inducing fever as parasites lyse red blood cells, spilling parasite waste into the bloodstream. Techniques to kill, sterilize, or avoid publicity to this extremely aggressive mosquito species are crucial to malaria control. In this light microscopic image taken using a 100Ч oil immersion lens, the ring-shaped P. The glycoproteins are identified by the immune system as overseas antigens, and a specific antibody defense is mounted against the parasite. Greater surveillance and control measures result in a reduction in reported circumstances; a few of the the} lowest numbers reported in 50 years (fewer than 10,000 circumstances in all of sub-Saharan Africa) have occurred since 2009. The parasite inhabits heart and digestive system tissues within the chronic part of infection, resulting in malnutrition and heart failure due to of} abnormal heart rhythms. An estimated 10 million persons are infected with Chagas disease, and it brought on 10,000 deaths in 2008. Shultz; scale-bar information from Matt Russell) Plant Parasites Protist parasites of terrestrial vegetation embrace brokers that destroy food crops. The oomycete Plasmopara viticola parasitizes grape vegetation, inflicting a disease called downy mildew (Figure 23. The unfold of downy mildew almost collapsed the French wine business within the nineteenth century. Late blight continues to plague potato crops in sure parts of the United States and Russia, wiping out as a lot as 70 percent of crops when no pesticides are applied. Saprobic protists have the important function of returning inorganic vitamins to the soil and water. This process allows for brand spanking new|for model new} plant progress, which in flip generates sustenance for other organisms along the food chain. Indeed, without saprobe species, corresponding to protists, fungi, and micro organism, life would stop to exist as all natural carbon turned "tied up" in useless organisms. It was cardio outcome of|as a result of} it had mitochondria that have been an cardio alpha-proteobacterium that lived inside a bunch cell. Whether this host had a nucleus on the time of the preliminary symbiosis remains unknown. The last common ancestor could have had a cell wall for at least of|no less than} part of of} its life cycle, however more information are wanted to verify this speculation. Protists display extremely varied cell structures, quantity of} forms of reproductive strategies, nearly every attainable type of diet, and varied habitats. Most single-celled protists are motile, however these organisms use numerous structures for transportation. The majority view at present is to order all eukaryotes into six supergroups: Excavata, Chromalveolata, Rhizaria, Archaeplastida, Amoebozoa, and Opisthokonta. The goal of this classification scheme is to create clusters of species are derived from a common ancestor. At present, the monophyly of a few of the the} supergroups are better supported by genetic information than others. Although large variation exists inside the supergroups, commonalities on the morphological, physiological, and ecological levels may be identified. In addition, many protists are parasites of vegetation and animals that can trigger deadly human ailments or destroy useful crops. Protists with the capabilities to carry out photosynthesis and to absorb vitamins from useless organisms are called. Which of those protists is believed to have evolved following a secondary endosymbiosis? What genus of protists appears to contradict the statement that unicellularity restricts cell size? Which parasitic protist evades the host immune system by altering its surface proteins with each generation? Giardia lamblia is a cyst-forming protist parasite that causes diarrhea if ingested. The chlorophyte (green algae) genera Ulva and Caulerpa both have macroscopic leaf-like and stem-like structures, however solely Ulva species are considered actually multicellular. This electron micrograph shows (c) the spore-bearing structures of Aspergillus, a type of toxic fungi found largely in soil and vegetation. Indeed, the acquainted mushroom is a reproductive construction utilized by many forms of fungi. Being eukaryotes, a typical fungal cell contains a real nucleus heaps of|and plenty of} membrane-bound organelles. The kingdom Fungi consists of an unlimited variety of living organisms collectively referred to as Eucomycota, or true Fungi. While scientists have identified about a hundred,000 species of fungi, that is solely a fraction of the 1. Edible mushrooms, yeasts, black mold, and the producer of the antibiotic penicillin, Penicillium notatum, are all members of the dominion Fungi, which belongs to the domain Eukarya. Fungi, once as} considered plant-like organisms, are more carefully related to animals than vegetation. Some fungal organisms multiply solely asexually, whereas others bear both asexual reproduction and sexual reproduction with alternation of generations. Most fungi produce massive number of|numerous|a lot of} spores, that are haploid cells that can bear mitosis to kind multicellular, haploid people. Fungi typically interact with other organisms, forming beneficial or mutualistic associations. The roots of the plant join with the underground parts of the fungus forming mycorrhizae. Through mycorrhizae, the fungus and plant exchange vitamins and water, greatly aiding the survival of both species Alternatively, lichens are an affiliation between a fungus and its photosynthetic associate (usually an alga). For instance, Dutch elm disease, which is caused by the fungus Ophiostoma ulmi, is a very devastating type of fungal infestation that destroys many native species of elm (Ulmus sp. Many European and Asiatic elms are less susceptible to Dutch elm disease than American elms. Fungal infections could show deadly for individuals with compromised immune techniques. They possess a stem-like construction just like vegetation, properly as|in addition to} having a root-like fungal mycelium within the soil. Progress within the field of fungal biology was mycology: the scientific examine of fungi. Based on fossil proof, fungi appeared within the pre-Cambrian period, about 450 million years ago. Molecular biology analysis of the fungal genome demonstrates that fungi are more carefully related to animals than vegetation. They are a polyphyletic group of organisms that share characteristics, somewhat than sharing a single common ancestor. Mycology is a branch of microbiology, heaps of|and plenty of} mycologists begin their careers with a level in microbiology. Mycologists can focus on taxonomy and fungal genomics, molecular and cellular biology, plant pathology, biotechnology, or biochemistry. Some medical microbiologists think about the examine of infectious ailments caused by fungi (mycoses). Mycologists collaborate with zoologists and plant pathologists to determine and control difficult fungal infections, such as the devastating chestnut blight, the mysterious decline in frog populations in lots of} areas of the world, or the deadly epidemic called white nostril syndrome, which is decimating bats within the Eastern United States.
Nifedipine 20mg
Cancer Categories Cancers are classified in three major classes: (1) hematologic malignancies, (2) lymphomas, and (3) strong tumors. Although tremendous advances have been made within the study of strong tumors, much more information is understood in analysis, prognosis, and therapy of the leukemias (see Chapters 176 and 177). This is so despite the far larger numbers of strong tumors, because of difficulties in obtaining the suitable strong tumor tissue, and culturing and obtaining good-quality chromosomes. Nevertheless, end result of|as a end result of} there have been many improvements, many laboratories can carry out strong tumor cytogenetics. The number of recognized recurrent chromosome abnormalities in all classes is now massive. For many cancers, malignancy conduct, prognosis, and therapy modalities additionally be} decided by the specific chromosomal change(s). This volume presents internationally accepted guidelines for naming and numbering human chromosomes, regular and abnormal. An wonderful practical textual content of medical genetics containing excellent chapters on primary and scientific cytogenetics. Structural abnormalities that end result from errors in embryogenesis or the fetal period are called congenital anomalies. These anomalies, which are additionally typically referred to as major and minor malformations and delivery defects, can occur in all organ techniques and elements of the physique, either in isolation or in affiliation with different anomalies. Severe anomalies are outlined as structural anomalies that require medical and/or surgical therapy and are cosmetically important. Mild anomalies are structural alterations posing no important health or social burdens. When multiple of} congenital anomalies occur together and are etiologically related they might end result from syndromes, including monogenic (see Chapter 31) and chromosome disorders (see Chapter 34). An affiliation refers to the non-random statistical affiliation of two or extra anomalies not recognized to be etiologically related. A sequence refers to a pattern of congenital anomalies that outcomes from a single primary abnormal occasion in embryogenesis (malformation), from a single mechanical issue (deformation), or from a disruptive occasion (disruption). Severe congenital anomalies are recognized in 2 to 3% of all newborns born in North America. Higher rates of congenital anomalies are reported in underdeveloped countries and dur-ing durations of famine and warfare. This fee doubles within the first yr of life as congenital anomalies not recognized within the neonate turn out to be clinically apparent. By 5 years of age, 7 to 10% of all youngsters have been recognized with minimal of|no much less than} one extreme congenital anomaly. Those with two gentle anomalies have a 10% danger of a extreme anomaly, and those with three or extra gentle anomalies have a 20% danger for a extreme anomaly. Congenital anomalies and genetic disorders pose a big burden on health care services and are important contributors to pediatric morbidity and mortality. In North America, over half of all North American youngsters evaluated in subspecialty medical clinics or admitted to hospitals are seen for therapy of disorders resulting from congenital abnormalities. Two thirds of the deaths of infants and youngsters in pediatric hospitals in developed countries are caused by an underlying congenital anomaly. Genetic disorders and genetic predisposition to certain diseases are major contributors to health care costs in any respect ages. The fee of congenital anomalies and chromosomal abnormalities is higher in miscarried fetuses and stillborn infants, compared with liveborn infants (Table 35-1). Prenatal screening of pregnancies with maternal serum triple display screen markers and ultrasound research carried out at 16 to 19 weeks of pregnancy can determine roughly half of all congenital anomalies. Positive screening exams warrant pressing referral to a medical center with experience in fetal analysis and therapy. By the end of eight weeks publish fertilization, the embryo has taken human kind and most organs are absolutely formed and positioned of their final position within the physique. Exceptions include external genitalia (12 weeks), abdominal wall closure (10 weeks), heart (postnatal closure of patent ductus arteriosus and defect of the atrial septum secundum), brain, and dental buildings (Table 35-2). The pathogenesis of congenital anomalies is split into malformations, deformations, disruptions, and dysplasias (Table 35-3). There are many alternative causes of congenital anomalies (etiologic heterogeneity), and there may be variation within the scientific presentation of individuals with the identical disorder (phenotypic heterogeneity). Specific information on potential teratogenic effects of an exposure may be obtained by way of teratogen information services, computerized databases, and reference books. The most common teratogen used throughout pregnancy is alcohol, adopted by cocaine, and related drugs. Commonly used medicines incessantly encountered in apply may be} teratogenic include anticonvulsants, angiotensin-converting enzyme inhibitors, antineoplastic agents, isotretinoin, warfarin (Coumadin), tetracycline, and thalidomide. Common in utero infections that affect on} the embryo and fetus include rubella, syphilis, toxoplasmosis, human immunodeficiency virus, herpes virus, cytomegalovirus, parvovirus, coxsackie virus, hepatitis, Venezuelan equine encephalitis, and varicella-zoster. Maternal situations resulting in metabolic teratogens and different effects on the fetus include poor nutrition and starvation, diabetes mellitus, untreated hypothyroidism (including iodine deficiency), hyperthyroidism, hyperparathyroidism, systemic lupus erythematosus, myasthenia gravis, alcoholism, phenylketonuria, Rh isoimmunization, homocystinuria, adrenal hyperactivity, and myotonic dystrophy. Congenital anomalies mostly current in infants youthful than 2 months of age or are detected prenatally with fetal sonograms. Evaluation of the congenital anomaly consists of an correct anatomic description with respect to look, dimension, shape, location, consistency and density, continuity with surrounding buildings, patency, shade, and whether or not contiguous buildings are distorted, misplaced, or malformed. Associated structural anomalies must be documented and described, including gentle anomalies and delivery marks. Accurate anthropometric measures of physique length, weight, occipital-frontal head circumference, and facial and different physique buildings must be recorded and in comparison with} standardized tables. A complete physical examination of all organ techniques including the central nervous system may determine occult anomalies not apparent on examination of external options. Pertinent historic information consists of age at presentation, look on the time of presentation and alter with time, previous therapy and investigations, functional expectations, and present and future plans for therapy. A evaluation of techniques must be carried out, with emphasis on identification of symptoms related to associated structural anomalies that generally occur in affiliation with the presenting anomaly. The affected person is assessed for sensory deficits, notably those affecting listening to and vision. The presence of associated structural anomalies, elevated minor anomalies, abnormal progress parameters, and dysmorphic facial options signifies an underlying syndrome, genetic disorder, or chromosomal abnormality. Gestalt analysis is incessantly attainable for frequent syndromes, such as Down syndrome. The majority of associations require additional diagnostic investigations and assistance with computerized databases earlier than a final analysis is possible. In fetuses and newborns, emphasis is positioned on pregnancy historical past (length of gestation; problems such as bleeding, infections, fevers, high blood pressure, and those regarding delivery; gestational diabetes; maternal age and medical issues; medicines and different exposures; onset of fetal movement); placenta and umbilical wire pathology; diagnostic investigations during the pregnancy; previous pregnancy historical past; and particular concerns that the pregnant mom had that she believes may have caused the issue. Aborted embryos and fetuses want a whole autopsy, histologic examination, radiography, photographic documentation, cultures for infections, and different investigations as indicated. Pathologic examination of the placenta, membranes, and umbilical wire is indicated in every delivery with a structural anomaly or pregnancy complication. In infants and youngsters, properly as|in addition to} in individuals with intellectual disabilities, a historical past of developmental milestones must be decided. Informal developmental screening and/or formal developmental or intelligence testing is important for overall management, and at times analysis. In basic, individuals with congenital anomalies be underestimated somewhat than overestimated of their talents. Many individuals with congenital anomalies of one organ system have associated structural anomalies that may current after childhood with scientific signs and symptoms specific for the concerned organ system. Other signs of undiagnosed congenital anomalies include the presence of elevated minor structural anomalies, certain pores and skin lesions, abnormal progress, developmental delay, and psychological retardation. Family historical past is as important in helping within the analysis of a disorder as different investigations. A three-generation pedigree must be obtained, with specific reference to different members of the family having an identical, associated, or different congenital anomaly; medical sicknesses; early dying; stillbirths and miscarriages; prolonged hospitalizations; institutionalization; psychological retardation; studying disabilities; progress disorders; relatedness. Diagnosis of the cause of|the cause for} a congenital anomaly is important end result of|as a end result of} it facilitates the prediction of an overall prognosis and natural historical past of the disorder. A differential analysis is useful in directing investigations for potential problems and the presence of anomalies properly as|in addition to} the exclusion of disorders that may have a extra extreme end result. Preventative health care by early detection and therapy of potential problems of a particular disorder improves the quality of life of the affected person.
Lipolight (Phosphatidylcholine). Nifedipine.
- A movement disorder called tardive dyskinesia.
- Are there any interactions with medications?
- What other names is Phosphatidylcholine known by?
- Hepatitis C when used together with regular treatments.
- Hepatitis A.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96507
Purchase nifedipine 30mg
This evaluate describes the pure history and various clinical features of cutaneous T-cell lymphomas and summarizes present approaches to the therapy of those diseases. Particularly necessary is the collaboration between the medical and radiation oncologist as a result of|as a result of} therapies usually involve mixed chemotherapy/radiation methods, and single-modality alternate options could result on} future therapy options if relapse occurs. These complexities make the disease finest handled by experienced multidisciplinary groups working in main medical centers. In developed Western nations, the age-specific incidence of the disease is bimodal, with its best peak in the third decade of life and a second, smaller peak after age 50. Parent-child combinations have been extra common than partner pairing incidences, which presumably might replicate the influence of an infectious or environmental agent during childhood or early adolescence. The incidence of clinical infectious mononucleosis additionally be|can be} related to these elements; certainly, infectious mononucleosis becomes clinically detectable only after early childhood. Some believe that a viral infection at a certain age and host circumstances could induce a malignant transformation. The Reed-Sternberg (R-S) cell is the diagnostic tumor cell that should be identified within the appropriate cellular milieu of lymphocytes, eosinophils, and histiocytes. The R-S cell is characterized by its massive measurement and basic binucleated construction with massive eosinophilic nucleoli. However, current info helps the notion that R-S cells are of B-cell origin. It has characteristics of each a macrophage and a lymphocyte, including the flexibility to phagocytose. These markers reside on the R-S cells or their variants and never on the background inflammatory cells. Each is predicated on the quantity and look of R-S cells properly as|in addition to} the background milieu. The distinguishing characteristic is the presence of broad birefringent bands of collagen that divide the cellular process into macroscopic nodules. The tumors comprise massive numbers of T lymphocytes, eosinophils, neutrophils, and histiocytes. Both entities could include sclerosis, massive binucleated large cells, and a T-cell lymphocytic infiltrate. Accurate pathologic diagnosis is important as a result of|as a result of} the 2 diseases usually result on} the same young female population and current as massive mediastinal masses, but therapy and prognosis may be be} decidedly totally different. It is identified extra usually in males, usually presents as generalized lymphadenopathy or as disease in extranodal sites, and produces related systemic symptoms. R-S cells are regularly identified and bands of collagen are absent, although a fantastic reticular fibrosis could exist. The cellular background includes lymphocytes, eosinophils, neutrophils, and histiocytes. R-S cells are numerous and may be be} pleomorphic, the cellular background is sparse, and diffuse fibrosis and necrosis may be be} current. By the time of diagnosis, affected sufferers usually have advanced-stage disease, extranodal involvement, an aggressive clinical course, and poor prognosis. More than 80% of sufferers current with lymphadenopathy above the diaphragm, usually involving the anterior mediastinum; lower than 10 to 20% current with lymphadenopathy limited to regions under the diaphragm. Therefore, the differential diagnosis is usually not that of generalized lymphadenopathy but, extra generally, that of regional lymphadenopathy in chosen sites. Masses could reach a large measurement before sufferers complain of symptoms such as cough, wheeze, chest discomfort, or tightness. Cervical, supraclavicular, axillary, or, uncommonly, inguinal lymphadenopathy could be the initial grievance. Many circumstances can cause regional lymphadenopathy, including infections with reactive lymphadenopathy (particularly frequent in the cervical and inguinal distributions); neoplasms (such as primary head and neck, lung or thyroid, breast, rectum), and autoimmune disorders. It is necessary to keep in mind that|remember that|understand that} sufferers with lymphoma could develop superimposed regional reactive lymphadenopathy that will enhance partially with a course of antibiotics. When residual lymphadenopathy persists, nevertheless, it deserves further investigation. Occasionally, sufferers come to attention due to systemic complaints or findings. These findings include continual pruritus, which may be intense and produce destructive excoriation; systemic "B" symptoms of fever, night time sweats, or weight loss; lymph node ache with alcohol consumption; an abnormal blood profile, such as leukocytosis with neutrophilia, eosinophilia, or thrombocytosis; or hardly ever hypercalcemia, nephrotic syndrome, or pancytopenia with a fibrotic bone marrow and splenomegaly. Detailed documentation of the extent of disease additionally offers the baseline for evaluating the response to therapy and for monitoring potential relapse. Accurate delineation of disease sites is mandatory for the design of radiation therapy fields. The use of a normal staging system additionally permits comparability of the results of therapeutic interventions in several clinical trials. It was initially designed to distinguish sufferers who would profit from extended-field radiation therapy from those who would require systemic chemotherapy. The staging system is an anatomic one and describes the sites of tumor in relation to the diaphragm (Fig. The Ann Arbor staging classification was revised at a gathering in Cotswolds, England, to recognize the significance of tumor bulk (Table 180-1). The history ought to give special attention to the presence or absence of disease-associated symptoms, which may occur in as much as} one third of sufferers and include fever, night time sweats, weight loss (B symptoms), pruritus, and, less generally, ache in concerned regions after ingestion of alcohol. In each anatomic stage, the presence of B symptoms is an adverse prognostic indicator that will result on} the therapy choice. History and physical examination with specific attention to the pres ence and length of B symptoms (see Table 180-1) and pruritus 3. Hematologic studies Complete blood cell depend Erythrocyte sedimentation rate Bone marrow biopsy 5. Biochemical studies Liver operate tests Renal operate tests Lactate dehydrogenase, albumin, calcium 6. Although pruritus is now not thought of a B symptom, the presence of generalized itching is considered by many to be an adverse prognostic symptom. Certain combinations of B symptoms have been found to be extra prognostically vital than others. For instance, the mixture of fever and weight loss has a extra adverse prognosis than night time sweats alone. B symptoms in all probability replicate the end-product manifestation of cytokines produced by the tumor cells. The physical examination ought to rigorously determine the situation and measurement of all palpable lymph nodes. A moderate to marked leukemoid reaction and thrombocytosis are common, particularly in symptomatic sufferers, and usually disappear with therapy. Abnormalities of liver operate studies ought to immediate further analysis of that organ, with imaging and potential biopsy. An elevated alkaline phosphatase worth may be be} a non-specific marker, nevertheless it additionally could point out bone involvement that ought to be appropriately evaluated by a radionuclide bone scan and directed skeletal radiographs. In most sufferers, a bipedal lymphogram and a gallium radionuclide scan provide necessary info and are highly recommended. The normal chest radiograph offers primary info concerning the extent of disease in the chest and provides a easy take a look at for monitoring sufferers after therapy (Fig. This extra info could alter the therapy recommendation in a minimum of|no less than} 10% of sufferers. The lymphogram detects not only abnormal lymph node measurement but also abnormalities of inner lymph node architecture. The lymphogram is especially correct in analysis of retroperitoneal and pelvic lymph nodes. In one massive collection, the overall accuracy of lymphography in figuring out concerned nodes was 92%. Lymphography additionally helps in designing radiation fields and assessing the response to therapy. Radionuclide bone scans are appropriate for investigating the nature of bone ache or an elevated serum alkaline phosphatase. Bone marrow involvement is comparatively uncommon, but due to the impression of a constructive biopsy on further staging and therapy, unilateral iliac crest bone marrow biopsy ought to be half of} the staging process. Staging laparotomy includes splenectomy and sampling of the splenic hilar, porta hepatis, para-aortic, and iliac nodes (with special attention given to areas that look suspicious on imaging studies).
Best nifedipine 20 mg
Mosses are very sensitive to air air pollution 676 Chapter 25 Seedless Plants and are used to monitor air high quality. They are also sensitive to copper salts, so these salts are a common ingredient of compounds marketed to eliminate mosses from lawns. Mosses kind diminutive gametophytes, that are the dominant part of the lifecycle. Green, flat structures-resembling true leaves, but lacking vascular tissue-are connected in a spiral to a central stalk. The plants take in water and nutrients instantly via these leaf-like constructions. Some primitive traits of inexperienced algae, similar to flagellated sperm, are still present in mosses may be} depending on water for reproduction. The moss lifecycle follows the sample of alternation of generations as shown in Figure 25. The most acquainted construction is the haploid gametophyte, which germinates from a haploid spore and types first a protonema-usually, a tangle of single-celled filaments that hug the bottom. Cells akin to an apical meristem actively divide and give rise to a gametophore, consisting of a photosynthetic stem and foliage-like constructions. The male organ (the antheridium) produces many sperm, whereas the archegonium (the female organ) types a single egg. At fertilization, the sperm swims down the neck to the venter and unites with the egg inside the archegonium. The zygote, protected by the archegonium, divides and grows into a sporophyte, still connected by its foot to the gametophyte. The concentric tissue across the mouth of the capsule is manufactured from triangular, close-fitting items, a little like "tooth"; these open and close depending on moisture levels, and periodically release spores. Several evolutionary improvements explain their success and their capability to unfold to all habitats. The lack of roots for absorbing water and minerals from the soil, nicely as|in addition to} a lack of bolstered conducting cells, limits bryophytes to small sizes. Vascular plants, the opposite hand|however|then again}, can obtain enormous heights, thus competing successfully for gentle. Photosynthetic organs turn out to be leaves, and pipe-like cells or vascular tissues transport water, minerals, and fixed carbon throughout the organism. In seedless vascular plants, the diploid sporophyte is the dominant part of the lifecycle. Seedless vascular plants still rely upon water during fertilization, because the sperm should swim on a layer of moisture to reach the egg. This step in replica explains why ferns and their family members are extra plentiful in damp environments. Vascular Tissue: Xylem and Phloem the primary fossils that present the presence of vascular tissue date to the Silurian interval, about 430 million years in the past. The easiest association of conductive cells shows a sample of xylem at the center surrounded by phloem. Xylem is the tissue answerable for the storage and long-distance transport of water and nutrients, nicely as|in addition to} the switch of water-soluble growth 678 Chapter 25 Seedless Plants elements from the organs of synthesis to the goal organs. The tissue consists of conducting cells, known as as|often known as} tracheids, and supportive filler tissue, referred to as parenchyma. Xylem conductive cells incorporate the compound lignin into their partitions, and are thus described as lignified. With their rigid cell partitions, the xylem cells present help to the plant and permit it to obtain impressive heights. Tall plants have a selective advantage by being able to|with the flexibility to|having the flexibility to} reach unfiltered sunlight and disperse their spores or seeds further away, thus expanding their vary. By growing higher than other plants, tall timber solid their shadow on shorter plants and limit competition for water and precious nutrients within the soil. Phloem is the second kind of vascular tissue; it transports sugars, proteins, and other solutes throughout the plant. Phloem cells are divided into sieve elements (conducting cells) and cells that help the sieve elements. Nevertheless, appears that|it appears that evidently|plainly} roots appeared later in evolution than vascular tissue. The development of an intensive network of roots represented a major new function of vascular plants. In contrast, roots, with their outstanding vascular tissue system, switch water and minerals from the soil to relaxation of|the the rest of} the plant. The extensive network of roots that penetrates deep into the soil to reach sources of water also stabilizes timber by appearing as a ballast or anchor. The majority of roots set up a symbiotic relationship with fungi, forming mycorrhizae, which profit the plant by greatly increasing the floor space for absorption of water and soil minerals and nutrients. Leaves, Sporophylls, and Strobili A third innovation marks the seedless vascular plants. Accompanying the prominence of the sporophyte and the event of vascular tissue, the appearance of true leaves improved their photosynthetic efficiency. Leaves seize extra sunlight with their elevated floor space by using extra chloroplasts to entice gentle vitality and convert it to chemical vitality, which is then used to repair atmospheric carbon dioxide into carbohydrates. The carbohydrates are exported to relaxation of|the the rest of} the plant by the conductive cells of phloem tissue. The existence of two forms of morphology suggests that leaves advanced independently in a number of} groups of plants. The first kind of leaf is the microphyll, or "little leaf," which could be dated to 350 million years in the past within the late Silurian. A single unbranched vein-a bundle of vascular tissue manufactured from xylem and phloem-runs via the center of the leaf. Microphylls might have originated from the flattening of lateral branches, or from sporangia that misplaced their reproductive capabilities. Microphylls are present within the club mosses and possibly preceded the event of megaphylls, or "massive leaves", that are larger leaves with a sample of branching veins. Megaphylls most probably appeared independently a number of} times during the course of evolution. Their advanced networks of veins suggest that a number of} branches might have combined into a flattened organ, with the gaps between the branches being full of photosynthetic tissue. In addition to photosynthesis, leaves play one other position within the lifetime of the plants. Pine cones, mature fronds of ferns, and flowers are all sporophylls-leaves that had been modified structurally to bear sporangia. Ferns and Other Seedless Vascular Plants By the late Devonian interval, plants had advanced vascular tissue, well-defined leaves, and root methods. During the Carboniferous interval, swamp forests of club mosses and horsetails-some specimens reaching heights of greater than 30 m (100 ft)-covered a lot of the land. These forests gave rise to the extensive coal deposits that gave the Carboniferous its name. In seedless vascular plants, the sporophyte became the dominant part of the lifecycle. Water remains to be required for fertilization of seedless vascular plants, and most favor a moist setting. Modern-day seedless tracheophytes embrace club mosses, horsetails, ferns, and whisk ferns. Phylum Lycopodiophyta: Club Mosses the club mosses, or phylum Lycopodiophyta, are the earliest group of seedless vascular plants. They dominated the landscape of the Carboniferous, growing into tall timber and forming large swamp forests. The phylum Lycopodiophyta consists of close to 1,200 species, together with the quillworts (Isoetales), the club mosses (Lycopodiales), and spike mosses (Selaginellales), none of that are true mosses or bryophytes. Some gametophytes develop underground and kind mycorrhizal associations with fungi. In club mosses, the sporophyte offers rise to sporophylls arranged in strobili, cone-like constructions that give the class its name. The single genus Equisetum is the survivor of a giant group of plants, known as as|often known as} Arthrophyta, which produced large timber and whole swamp forests within the Carboniferous. Horsetails had been as soon as} used as scrubbing brushes and had been nicknamed scouring brushes. Phylum Monilophyta: Class Psilotopsida (Whisk Ferns) While most ferns kind large leaves and branching roots, the whisk ferns, Class Psilotopsida, lack both roots and leaves, most likely misplaced by discount.
Cheap nifedipine 20mg
The technical success price of this technique is more than 90%, and its morbidity and mortality are lower than those of emergency surgical portacaval shunts. Angiographic reintervention may be be} required to preserve portal decompression (Fig. Similar strategies can be used for nerve blocks, corresponding to celiac ganglion blocks in sufferers with intractable pain secondary to superior pancreatic carcinoma (see Chapter 140) or continual pancreatitis (see Chapter 141). Investigational strategies that show promise for tissue ablation include percutaneous alcohol injection and tissue ablation with radiofrequency, laser, or cryotherapy probes. More than 90% of simple stomach abscesses can be drained by percutaneous catheter drainage. The success rates with more difficult abscesses, corresponding to those in the pancreas or those related to underlying bowel issues, are in the vary of 70 to 90%. Percutaneous biliary interventions (see Chapter 157) beneath fluoroscopic management are complementary to endoscopic and surgical procedures. Transhepatic strategies are of specific worth when endoscopic strategies fail or are contraindicated, corresponding to in sufferers with prior surgical interventions in the biliary system that make endoscopic entry inconceivable. Transhepatic insertion of an indwelling expandable metallic prosthesis is well established as palliation for malignant biliary obstructions and will keep away from endoscopic treatment or palliative surgery. Emergency percutaneous biliary drainage may be be} needed in sufferers with acute cholangitis. Transhepatic balloon dilatation has a higher than 70% long-term success price in sufferers with benign biliary strictures. Percutaneous cholecystostomy is beneficial for preliminary decompression of the gallbladder in sufferers with acute calculous or acalculous cholecystitis, significantly if sufferers are thought of to be at excessive threat for emergency surgery, and permits subsequent elective cholecystectomy. Alternatively, percutaneous methods can be used for fragmentation and removal of stones from the gallbladder in sufferers who stay at excessive threat for surgery. Gastrointestinal interventions corresponding to balloon dilatation of benign strictures of the esophagus or placement of an endoprosthesis for palliative treatment of malignant obstructions of the esophagus (see Chapter 124) or colon (see Chapter 139) can be carried out by interventional endoscopists or interventional radiologists. Review of the role of imaging in the management of sufferers with acute stomach pain. This article summarizes outcomes and limitations of percutaneous management of sufferers with pancreatic abscesses. With its outstanding accessibility, the gastrointestinal tract, maybe more than another organ system, has significantly benefited from the endoscopic approach. The main advantages of endoscopy over contrast radiography in evaluation of illnesses of the alimentary tract include direct visualization, leading to a more accurate and delicate evaluation of mucosal lesions; the flexibility to acquire biopsy specimens from superficial lesions; and the flexibility to carry out therapeutic interventions. These advantages make endoscopy the procedure of selection in most cases in which mucosal lesions or growths are suspected. Conversely, contrast radiography is more useful when anatomic data may be be} required, corresponding to in sufferers with suspected volvulus, intussusception, or delicate strictures; sufferers with difficult postsurgical modifications; or elements of the small bowel that are be} comparatively inaccessible to endoscopy. For most higher gastrointestinal lesions, nevertheless, the sensitivity (about 90%) and specificity (nearly 100%) of endoscopy are far higher than for barium radiography (about 50% and 90%, respectively). Diagnostic endoscopy (Table 122-1) is normally a remarkably secure and well-tolerated procedure. However, complications do happen and need to be carefully explained to the patient as half of} the knowledgeable consent process; sufferers also should be appropriately prepared to cut back complication rates (Table 122-2). Although not listed in the desk, a few of the the} new diagnostic modalities that are be} already in clinical trials include endoscopic magnetic resonance imaging, endoscopic spectroscopy, and optical coherence tomography. Potential new therapeutic modalities include endoscopic antireflux surgery (using endoscopic "stitching machines") and photodynamic remedy. In other cases, endoscopy is required to evaluate specific lesions discovered by other diagnostic imaging, corresponding to a gastric ulcer or colon polyp discovered by barium radiography. Finally, screening endoscopy is often carried out in asymptomatic people based mostly on their threat for generally occurring and preventable conditions corresponding to colon most cancers (see later). In dealing with the evaluation of gastrointestinal symptoms, several of} questions therefore need to be addressed by the referring doctor and the endoscopist: Which sufferers want endoscopy? However, the presence of sure symptoms or indicators in a patient with reflux-like symptoms ought to result in an early endoscopy: dysphagia or odynophagia, weight loss, gastrointestinal bleeding, or frequent vomiting. Patients with extreme, persistent, or incessantly recurrent symptoms might have significant esophagitis and are therefore appropriate candidates for endoscopy (see Fig. If needed, additional evaluation with ambulatory pH monitoring may be be} indicated to set up the diagnosis. The commonest causes in sufferers with human immunodeficiency virus an infection are Candida, cytomegalovirus, herpesvirus, and idiopathic esophageal ulcers. Because most sufferers with the acquired immunodeficiency syndrome and esophagitis will have candidiasis, an empirical 1- to 2-week course of antifungal remedy may be be} justified. Those who fail this approach, nevertheless, ought to almost all the time have an endoscopy and biopsy as a result of|as a outcome of} every of the frequent causes requires specific remedy. Dysphagia can usually be categorized as oropharyngeal based mostly on the clinical features of nasal regurgitation, laryngeal aspiration, or problem in moving the bolus out of the mouth. Endoscopic treatment choices can be found for a lot of} causes of esophageal dysphagia. Tumors may be be} dilated mechanically, ablated by thermal means (cautery or laser), or stented with prosthetic devices; metallic expandable stents have become the palliative procedure of selection for most sufferers with symptomatic esophageal most cancers. Benign lesions of the esophagus, such a strictures or rings, dilated endoscopically, normally with excellent outcomes (Color Plate 1 D). Finally, some motility disturbances corresponding to achalasia are best approached endoscopically with the use of of} massive balloon dilators for the lower esophageal sphincter or sometimes with the local injection of botulinum toxin. Dyspepsia, which is continual or recurring pain or discomfort centered in the higher abdomen, is seen in roughly 25% of the population and accounts for 2 to 5% of all family apply consultations. Up to 40% of sufferers with dyspepsia will have a structural lesion corresponding to peptic ulcer (15-25%), reflux esophagitis (5-15%), and, rarely, gastric or esophageal most cancers (<2%). Other structural lesions corresponding to gallstones, pancreatic illnesses, infiltrative illnesses of the abdomen or intestines. The optimal diagnostic approach to dyspepsia is considerably controversial and remains to be evolving (see Fig. In recent years there has been a transfer towards empirical approaches to dyspepsia as a result of|as a outcome of} solely a minority of sufferers with dyspepsia have peptic ulcers and gastric most cancers is extraordinarily rare in Western countries. However, dyspepsia is a recurrent situation, and sufferers who fail to reply to empirical remedy will generally bear endoscopy. If a diagnostic check is to be carried out, endoscopy, sometimes with biopsies to detect H. Finally, higher gastrointestinal cancers are occasionally related to significant bleeding. Endoscopy ready to|is ready to} detect and localize the site of the bleeding in 95% of instances and is clearly superior to contrast radiography (with an accuracy of solely 75 to 80%). The endoscopic look of bleeding lesions can even help predict the chance of rebleeding, thus facilitating the triage and treatment process. Finally, and maybe most significantly, bleeding can be effectively managed in the course of the preliminary endoscopy itself in the majority of instances. In common, endoscopy should be carried out solely after sufficient stabilization of hemodynamic and respiratory parameters. The timing of subsequent endoscopy depends on two factors: the severity of the hemorrhage and the chance status of the patient (see Fig. Patients with active, persistent, or extreme bleeding (>3 models of blood) will require urgent endoscopy. Patients with slower or inactive bleeding may be be} evaluated by endoscopy in a "semi-elective" method (usually within 12-20 hours), however a case can be made to carry out endoscopy very early even in these stable sufferers (perhaps in the emergency department itself) to allow triage choices to be made more confidently. Most bleeding from higher gastrointestinal lesions can be effectively managed endoscopically. The endoscopist considers factors corresponding to age (older sufferers have a higher threat of rebleeding) and the severity of the preliminary hemorrhage (which has a direct correlation with the chance of rebleeding) in addition to the appearance of the lesion when figuring out the need for endoscopic remedy. Non-variceal bleeding vessels can be treated with a variety of|quite a lot of|a wide selection of} means together with injections of varied substances (epinephrine, saline, sclerosants) or thermal coagulation (laser or electrocautery). In the United States, the most popular approach to a bleeding peptic ulcer lesion is a mixture of injection with dilute epinephrine and electrocoagulation.
References:
- https://www.swinehealth.org/wp-content/uploads/2016/03/Influenza-virus-C-IVC-and-influenza-virus-D-IVD.pdf
- https://www.dshs.state.tx.us/IDCU/investigation/electronic/VHF.pdf
- https://law.yale.edu/sites/default/files/area/center/ghjp/documents/final_covid-19_letter_from_public_health_and_legal_experts.pdf
- https://www.govinfo.gov/content/pkg/CHRG-106shrg78656/pdf/CHRG-106shrg78656.pdf