.png)
Best 60mg evista
Clinical, cerebrospinal fluid, and histological information from twenty-seven cats with primary inflammatory illness of the central nervous system. Sharif S, Suri Arshad S, Hair-Bejo M, Rahman Omar A, Allaudin Zeenathul N, Alazawy A. Inflammatory cerebrospinal fluid evaluation in cats: Clinical analysis and outcome. Clinicopathological findings and illness staging of feline infectious peritonitis: 51 circumstances from 2003 to 2009 in Taiwan. History: the dog had been bitten on the left femoral pores and skin, and a 12 x sixteen mm dermal mass shaped at first within the region. He was fitted with an Elizabethan collar to forestall self-trauma and was topically handled with antibiotics and steroids with no clinical enchancment. Laboratory Results: None Histopathologic Description: the quantity of} variably sized lots are current within the dermis and subcutis, with quantity of} small lots around giant lots. Various-sized swollen peripheral nerve fascicles are noticed in every mass, with perineurial hyperplasia. Swollen nerve fascicles in every mass consist of thin, unmyelinated nerves with hypertrophic Schwann cells and a thickened perineurium. Each nerve fascicle consisted of thin to unmyelinated nerve fibers, together with axons and Schwann cells. Axons in swollen nerve fascicles and hyperplastic perineurium had Schwann cells as well as|in addition to} regular nerve fibers, suggesting a non11 neoplastic lesion. The lack of proliferative activity also indicated that our case was non-neoplastic. The histological options resembled traumatic neuroma except swollen large-sized nerve fascicles and perineurial hyperplasia. With clinical findings and histological options, it was instructed that peripheral nerves of affected space have been end result of|the outcomes of} self-inflicted harm. Traumatic neuroma is a reactive and nonneoplastic proliferative nerve illness to harm or surgical procedure at the proximal end of an injured peripheral nerve. The lesion is commonly seen within the interdigital plantar nerve of third and fourth toes in ladies. As the lesion progresses, the fibrosis becomes marked and envelops the epineurium and perineurium in a concentric style and even extends into the surrounding tissue. Schwannoma or neurofibroma with plexiform pattern most closely resembled the current case. Haired pores and skin, dog: this tiled image shows the extent of a neuroma that arose over two years following a dog bite at the site. The mass is composed of clusters of enormous caliber nerve fibers surrounded by fibrous connective tissue. Schwannoma is composed of mainly Schwann cells with attribute patterns and containing few axons. Neurofibroma consists of a mix of Schwann cells, axons and fibroblasts, and the number of axons may be very low. Extraneural perineurioma is an extremely elongated spindle cell lesion arranged in parallel bundles. Thus, immunostaining for these proteins is at all times used to distinguish between perineurial cell and Schwann cells. Conference Comment: this case supplies an attention-grabbing diagnostic exercise in distinguishing neoplastic from non-neoplastic proliferative peripheral nerve lesions. Neuroma is a wellknown entity, which has been described within the literature for over 50 years. Neuroma development following trauma, mostly noticed subsequently to tail-docking or digital neurectomy in horses, is presumed to come up when the normal regenerative progress of a disrupted nerve fiber encounters a physical obstruction corresponding to scar tissue. Haired pores and skin, dog: Proliferating nerve bundles are surrounded by a markedly thickened perineurium. This is a chance for the reader to review the hallmarks of neoplasia and independently think about whether or not any of those may apply in this case. The following six hallmarks are acquired in succession and result in cells becoming neoplastic and eventually malignant: sustained proliferative signaling, evasion of progress suppressors, resisting cell dying, enabling replicative immortality, induction of angiogenesis and the activation of invasion and/or metastasis. Recently, two additional hallmarks have been added: the reprogramming of power metabolism and evasion of the immune response. Tw o traits described as crucial to the acquisition of those hallmarks are genomic i n s t a b i l i t y a n d t u m o rpromoting inflammation. When mutations are permanently acquired within the genome, the cell may develop a selective advantage that allows its outgrowth and eventual dominance within the local surroundings fueled by progress and survival components provided by secondary inflammatory cells. Schwannomas, which originate from a single nerve and extend along side of} however external to it, facilitates its involvement with plexus arrangements such as the brachial plexus and other widespread sites together with the guts base, s p i n a l n e r v e r o o t s a n d the t o n g u. Peripheral nerve sheath tumors are of controversial origin, however usually discovered on the distal limbs of canine and graded in accordance with gentle tissue sarcoma standards. Ganglioneuroblastomas are comparable however are composed of poorly differentiated ganglion cells with more atypia. Haired pores and skin, dog: Nerve fibers demonstrate robust intracytoplasmic immunostaining for anti-glial fibrillary acidic protein. Histopathological examination of nerve samples from pure neural leprosy patients: Obtaining most data to improve diagnostic efficiency. Intraoperative and pathological findings of intramedullary amputation neuroma associated with spinal e p e n d y m o m a. Immunohistochemical evaluation of canine peripheral nerve sheath tumors and other gentle tissue sarcomas. The foal was dead on arrival to the University of California, Davis Veterinary Medical Teaching Hospital. Gross Pathological Findings: the mucous membranes of the oral cavity have been diffusely tinged blue (cyanosis). Approximately 20% of the pulmonary parenchyma was aerated and the remaining lung tissue was atelectic (fetal atelectasis). Foci of epicardial hemorrhages have been current on the best ventricle, adjoining to the atrio-ventricular junction. Pinpoint hemorrhages have been scattered all through the thymus and on the mucosal surface of the esophagus. Histopathologic Description: Skeletal muscle (diaphragm, semitendinosis): Within numerous swollen myofibers are discrete glassy to compact granular, frivolously basophilic, oval to variably shaped and sized inclusion bodies that are be} up to as} approximately 50 µm in length. The inclusions disrupt and/or replace the normal cytoplasmic myofibril architecture. Heart: Intracytoplasmic inclusions, similar to these previously described, are inside numerous variably swollen and disrupted myocytes. Brainstem: A few to reasonable numbers of enormous neuronal cell bodies include intracytoplasmic inclusion bodies, similar to these previously described. Heart, Skeletal muscle (diaphragm, intercostal, thigh): Severe multifocal myofiber degeneration with intracytoplasmic inclusions. Genotyping was performed at the Veterinary Genetics Laboratory at the University of California, Davis. Analysis showed the foal to be homozygous for the single nucleotide polymorphism answerable for glycogen branching enzyme deficiency. Transmission electron microscopy was performed on formalin fixed skeletal muscle and brainstem at the California Animal Health and Food Safety Laboratory, Davis Branch. Heart, foal: Cardiomyocytes include one or quantity of} amphophilic cytoplasmic inclusions. Skeletal muscle, foal: Rhabdomyocytes include one or quantity of} amphophilic cytoplasmic inclusions. Brainstem, foal: Brainstem neurons include multifocal intracytoplasmic inclusions. Similar inclusions are seen inside degenerate neuronal cell bodies inside the brainstem. Clinical indicators vary and may include progressive muscle weakness, hypoglycemic seizures, respiratory failure, or sudden dying. A examine performed to assess the service frequency of this allelic mutation in populations of Quarter horses and Paint horses estimated that 8.
Purchase evista 60mg
Recorded knowledge from the gadget aided in a variety of|quite a lot of|a wide selection of} neuroscience analysis, ranging from pain, spinal cord injury, and brain-machine-interface engineering analysis. First-in-man clinical expertise using a high-definition three-dimensional exoscope system for microneurosurgery. Tentorial sling for microvascular decompression in patients with trigeminal neuralgia: an outline of operative method and clinical outcomes. A matched cohort comparison of cervical disc arthroplasty versus anterior cervical discectomy and fusion: Evaluating perioperative outcomes. The circle of Willis predicts the Antihypertensive results of carotid artery stenting. Lateral mass screw stimulation thresholds in posterior cervical instrumentation surgical procedure: a predictor of medial deviation. Both academic division and Medical Center profitability of the Neurological Surgery program remain sturdy. Neurological Surgery has nearly totally recovered by way of recruitment of recent school and collections, and is on an upward development trajectory. We mannequin continued 6-8% development in skilled income per year within the next three years as just lately hired school ramp a lot as} full productiveness, and new school are recruited to enhance proceed our development. Bob Carter, Neurological Surgery noticed great progress in gaining philanthropic assist. A key initiative in 2014 was the first Neurological Surgery school "giving campaign" which was launched in assist of the Intraoperative Suite in Jacobs Medical Center. Notably, the first endowed chair within the department was established in 2015: the Sharon B. It is anticipated that Neurological Surgery will elevate nearly $5M in philanthropic assist in fiscal year 2019. They are further motivated by the published and curriculum alternatives afforded by the Neuro Hub. It is necessary to observe that the honest market value of this gear equates to nearly $20M. Designation as a School of Medicine academic department represents a natural development that may: 1. Facilitate adjunct academic appointments that may allow higher institutional degree collaboration 4. Contribute to the recruitment and retention of leading school via independent promotion processes 5. Corr: As Vice Chancellor for Health Sciences, I am pleased to write this sturdy letter of assist for the transition of Neurosurgery from a hospital department and division of the Department of Surgery to an independent academic department within the School of Medicine. I believe this represents a natural development from a collection of shared strategic conversations with Dr. This transition moreover has unanimous assist from the Health Sciences Faculty Council and Interim Dean Steven Garfin. Its residency program has not solely become extremely acknowledged by its peers-in fact, it just lately obtained a maximum accreditation from the Neurological Surgery Residency Review Committee-but has also maintained an distinctive degree of high quality, as evidenced by numerous School of Medicine educating awards. Its analysis portfolio continues to develop and clearly has sturdy synergies with allied departments in Health Sciences, similar to Neurosciences, Radiology, Emergency Medicine, Radiation Medicine and Applied Sciences, and Orthopaedic Surgery. The letters of assist from these departments reveal the keenness and productiveness of those partnerships, which I count on will proliferate because the department grows its analysis school. Clinical productiveness continues to increase, with the number of annual cases growing from 2,200 to three,four hundred, providing a powerful financial foundation for its school and management to foster novel academic and educational applications. As Health Sciences actively seeks to broaden its numerous community, all School of Medicine departments, including Neurosurgery, are at present engaged in growing a three-year plan to assess and enhance variety throughout several of} domains, including school, staff, and resident representation. I suggest departmental status for Neurosurgery with enthusiasm and with out reservation and can be joyful to focus on this further at your request. As articulated within the proposal, and its accompanying materials, I believe that Neurological Surgery has demonstrated a powerful dedication to the Health Sciences tripartite mission and created the mandatory infrastructure to assist this transition. Creating an educational Department of Neurological Surgery may also enhance the stature of the School of Medicine among other top-tier peer establishments. I would like to suggest Alexander Khalessi serve as Interim Chair till a everlasting chair is recruited. Khalessi was selected from a national pool of candidates to serve as Chair of the hospital department, and I am confident he has the management expertise to incorporate the appropriate elements into an independent academic unit. Department of Neurological Surgery 7893 Subject: New Academic Department of Neurological Surgery Dear Dr. Alexander Khalessi, has taken model new} trajectory toward cementing its status as a extremely famend department that leads analysis in a broad array of basic and clinical analysis in science related to neurosurgery and neuro-oncology. Garfin and Brenner, I am pleased to write this letter of sturdy and enthusiastic assist for the transition of Neurosurgery from hospital department to independent academic department within the School of Medicine on the University of California, San Diego. As Chair and longstanding school member of the Department of Emergency Medicine which underwent a similar transition quantity of} years in the past, I believe that the Division of Neurosurgery is well-deserving and likewise well-positioned for success as an independent academic department at our University. Bob Carter, Neurosurgery has undergone tremendous development over the last few|the earlier few|the earlier couple of} years with a strong clinical practice, highly-ranked educating applications, and a burgeoning analysis portfolio. Many present and emeriti school are worldrenowned within the specialty, and their ranks include our former Medical School Dean and Vice Chancellor for Health Sciences. Similarly, the teaching programs including its residency and fellowship trainings applications are extremely regarded and attract the easiest students from top-tier faculties. By becoming an educational department, Neurosurgery will proceed and indeed accelerate this spectacular trajectory. Given that the division is financially self-supporting as an independent hospital department already, the chance of such a transition is minimal. In fact, the higher threat lies in not transitioning Neurosurgery to a full academic department. I foresee sturdy collaborations with my Department not solely in acute neurosurgical care within the Emergency Department, but in addition with our new geriatric and senior initiatives now taking form. In summary, I totally assist the transition of Neurosurgery from hospital department to full academic department within the School of Medicine. I even have have} little question that an educational Department of Neurosurgery will contribute immensely to the missions of the School of Medicine and University. Vice Chancellor, Health Sciences Re: Application of Neurosurgery for Academic Department Status Dear Chancellor Khosla, I am writing to specific my ideas and considerations concerning the proposed transition of the Division of Neurosurgery to full departmental status. By way of context, shortly after my arrival as Chair of the Department of Surgery in 2015, Vice-Chancellor after which Dean, David Brenner set in movement a process to transition the Division of Neurosurgery to full departmental status. Brenner and Carter were confident that this was a natural and necessary transition for Neurosurgery, and one which was in keeping with|consistent with|in line with} organizational patterns present within the leading academic medical establishments. Indeed, fewer than 10% of educational neurosurgery applications remain housed in Departments of Surgery nationwide. To be transparent it was my recommendation at that time that Neurosurgery remain as a division within the Department of Surgery. In fact, all of those are attainable under a divisional structure with the right departmental and divisional management. Furthermore, I do believe that there are advantages for surgical specialty applications in maintaining a common bond and infrastructure via the umbrella of a broad surgical procedure department structure. Brenner, it was my impression that he was much more convinced of the advantages of a transition than I. Under his directive, Neurosurgery has functioned over the previous four years as a "hospital-based department" with a substantial degree of autonomy in administering its clinical and academic applications. Khalessi have in my view, offered excellent management of Neurosurgery throughout this transitional interval. Carter, a national search process was performed to identify and recruit model new} leader of Neurosurgery. To be honest, I believe that a narrative of departmental transition was incorporated into the discussions with the candidates, including Dr. The Division of Neurosurgery in our modest scale academic medical enterprise will like other surgical subspecialty departments be relatively small. I still keep reservations concerning the level of maturity of its clincal and analysis applications with respect to the justifaction for Departmental status. He has secured a number of|numerous|a variety of} excellent junior degree hires and has articulated a strategic plan for advancing the analysis applications. In summary, I am confident within the management of Neurosurgery and I strongly suspect that the transition to Departmental status will ultimately show to be successful. The separation will afford Neurosurgery extra freedom to creatively pursue its missions and attain its full potential. Khalessi in facilitating this transition should this be the course that you just choose to pursue.
Best evista 60 mg
Hypothermia in the new child or toddler throughout a process may result in bradycardia and may compromise the status of the child. This could be prevented by having a warming device on or beneath the child in the course of the catheterization and keeping the temperature of the room managed. Postprocedure Care In many pediatric services, the same-day admission patient is cared for both pre- and postcatheterization by the identical nurse. When the child is returned to the submit anesthesia care or nursing unit, the cardiac catheterization laboratory nurse offers a whole again to} the receiving nurse, together with the type of|the sort of} pro- cedure performed, venous and arterial catheter sites, significant hemodynamic values, interventions performed, medication amounts and time, the condition of the patient in the course of the process, and any particular problem areas or complications that arose. Heparin infusions could also be} started in patients with sure device placements, postperipheral pulmonary artery dilations, or if a slim shunt was crossed with a catheter. Although the postcatheterization care plan varies between establishments, the bulk include strict bed relaxation with the affected extremity stored straight for four hours for venous access and 6 hours for arterial access. The frequency decreases to each half-hour, after which to each hour as the youngster becomes more alert and his or her condition stabilizes. Use of a Doppler device could also be} useful in locating difficult-to palpate peripheral pulses and checking the tone quality of the heart beat|the heartbeat} for attainable stenosis. Dressings are usually removed the morning following the process whether or not in the hospital or at house. The use of a dry sterile dressing lined with a transparent dressing permits direct visualization of the catheterization website and is more comfy to take away than an elastized tape strain dressing. Functionally this means that systemic blood coming into the center Chapter 27: Pediatric Interventional Cardiology 419 is misdirected back into the systemic circulation, and oxygenated pulmonary venous blood is returned to the pulmonary circulation. To maintain life, the creation of an atrial septal defect is important to enhance mixing of pulmonary and systemic venous blood, subsequently improving oxygen saturation. The atrial septum should be amenable to tearing, so the process is greatest performed in infants lower than 6 weeks of age. Early surgical restore could be performed if the surgeon is happy with diagnostic echocardiographic knowledge. The Procedure the new child getting into the cardiac catheterization laboratory is often intubated and beneath general anesthesia for the process. The stability and oxygenation status of the new child will decide the sequence of the process. The diagnostic catheterization will confirm the initial cardiac di- agnosis and look for any other associated anomalies. After prepping the groin, a 5F balloon angiographic catheter (the most popular diagnostic catheter) is launched via the femoral vein. The proper side of the center is reached; oxygen saturations are performed, and pressures are recorded. A left-to-right atrial pull-back is performed, is in a position to} indicate how large the open foramen ovale is. After pressures and saturations have been taken, right- and left-ventricle angiography is performed. An aortic root angiography is also be|can be} performed to visualize and define the coronary artery orientation. In preparation for the septostomy, the sheath should be exchanged for a 7F-sized one, to accommodate the balloon tip of the 5F atrioseptostomy catheter. The atrioseptostomy catheter is passed from the proper atrium via the open foramen ovale to the left atrium. The inflated balloon is drawn back against the atrial septal wall, then pulled with a brief jerk into the proper atrium, thus tearing the atrial septum. After completion of the process, the toddler is returned to the intensive care unit for postoperative care. Hypovolemia, due to of} both poor cardiac output and blood loss in the course of the process, will require anticipation of fluid boluses to improve intra-atrial mixing. The patient may enter the catheterization lab in an especially acidotic state and will possibly be in a state of fixed resuscitation; fluid volume and electrolyte stability should be fastidiously monitored. Other rhythm disturbances such as supraventricular tachycardia and partial or full heart block have been identified to occur throughout or after the atrioseptostomy. Depending on the size of the left atrium, danger of myocardial perforation with a wire or catheter exists. Accidental tearing or rupturing of valves or vessels could be avoided by correct positioning and the sluggish inflation of the balloon beneath fluoroscopy. Due to the large-size sheath, injury to the femoral vein (including tearing and thrombosis) may occur and should be thought-about in the postcatheterization care plan. Radiofrequency Perforation for Pulmonary Atresia with an Intact Ventricle Septum sia poses is the need to|the necessity to} first create a gap via the fused valvular leaflets that will permit a balloon dilatation catheter to be passed. This technique proved profitable, however the prohibitive cost of lasers led to the search for another technique. The use of radiofrequency vitality to destroy aberrant conduction pathways in the heart is extensively practiced in many of} pediatric establishments. The switch of this system to using of} radiofrequency catheters to perforate the fused pulmonary valve has now confirmed to be successful, with the added advantage that the equipment is already obtainable in most catheterization laboratories. To provide adequate ahead blood flow to the pulmonary vasculature and to forestall avoidable complications, a few of} anatomical issues should be decided earlier than perforation and dilatation of the pulmonary valve is tried. Relief of the proper ventricular obstruction by the creation of a rightventricle-to-pulmonary-artery connection is the subsequent therapy consideration. With the latest advances in interventional catheters, a way was sought to handle the problem of pulmonary atresia with an adaptation of the profitable technique of dilating stenotic pulmonary valves. The problem pulmonary atre- the new child shall be intubated and placed beneath general anesthetic. After obtaining venous access, a balloon angiographic catheter is often used to attain the proper side of the center, and proper heart hemodynamics and oxygen saturations are performed. The left Chapter 27: Pediatric Interventional Cardiology 421 side of the center is reached from the proper atrium via the open foramen ovale. Angiography could also be} performed in the left ventricle to confirm the patency of the septal wall. Angiography of the proper ventricle is performed to confirm the diagnosis and visualize the pulmonary valve. The venous catheter may then be exchanged for a Judkins proper coronary catheter, which is useful in positioning the catheter in the proper ventricular outflow tract, immediately beneath the valve. When right placement of the perforation catheter is confirmed via hand injections of distinction medium, the radiofrequency vitality is utilized. Hand injections showing a distinction medium jet passing via the valve will confirm perforation. The cardiologist will then attempt to push the catheter via the perforated valve, however in some instances the catheter shall be too broad. It is useful to have a snare catheter readily available in the occasion the cardiologist has bother advancing the information wire. The snare catheter could also be} passed from the arterial side to grasp the wire as soon as} the wire has crossed the valve. The Judkins catheter is then removed and replaced with the balloon dilatation catheter. The balloon catheter is then advanced over the information wire and into position, with the balloon straddling the valve. The cardiologist may have to begin with a smaller balloon to dilate the orifice sufficiently to permit a bigger balloon to enter the valve. After dilation, proper ventricle strain is checked, and a control angiography is performed to visualize and measure the opening space of the valve and to verify for ahead flow into the pulmonary artery. Postprocedure Care and Complications Inadvertent information wire perforation of the infundibulum, pericardium, or other cardiac structures may occur in the course of the valvular perforation process. Thus, cautious monitoring for indicators and signs of cardiac tamponade is essential throughout and after the process. Antegrade flow across the pulmonary valve may not enhance considerably in the neonate until the proper ventricular compliance improves, subsequently, a prostaglandin infusion may have to continue postcatheterization. The probabilities of postprocedure complications enhance following a prolonged process with multiple of} catheter changes. Catheter insertion sites should be monitored for postprocedure bleeding, and any bleeding should be prevented. The probability of thrombus formation is larger the longer the arterial catheter is in place. Balloon Dilatations Balloon dilatation to relieve stenotic vessels and valves has opened model new} door to the therapy of pulmonary and aortic valvular stenosis, coarctation of the aorta, peripheral pulmonary stenosis, and stenosis of surgical conduits.
Purchase 60 mg evista
Knee flexion cleared the hamstring muscle group, and knee extension decided function of the quadriceps group. The surgical devices and tables have been kept sterile till after the entire monitored muscle groups have been tested and showed voluntary motion. The joint motion characterised by elevating the toes toward the anterior ankle is: a. Health occupation involved with physical rehabilitation and prevention of disability: abbreviation 19. Health occupation involved with working to increase function and independence in every day life: abbreviation 14. Its colour, texture, and resilience reveal much, as does the condition of the hair and nails. This body-covering system protects towards an infection, dehydration, ultraviolet radiation, and harm. Extensive harm to the skin, such as by burns, end result in|may end up in|can lead to} a host of dangerous problems. Anatomy of the Skin the outermost portion of the skin is the epidermis, consisting of 4 to 5 layers (strata) of epithelial cells. As these cells gradually rise toward the surface, they die and turn out to be filled with keratin, a protein that thickens and toughens the skin. The outermost (horny) layer of the epidermis, the stratum corneum, is composed of flat, lifeless, protective cells may be} continually being shed and changed. Some of the cells within the epidermis produce melanin, a pigment that offers colour to the skin and protects towards daylight. The subcutaneous tissue beneath the dermis is composed primarily of connective tissue and fat. The sebaceous glands release an oily fluid, sebum, that lubricates the hair and skin and prevents drying. Each hair develops within a sheath or hair follicle and grows from its base inside the deep layers of the skin. The examine of the skin and diseases of the skin is dermatology, but careful remark of the skin, hair, and nails must be half of} every physical examination. It must be palpated to consider its texture, temperature, moisture, firmness, and any tenderness. Wounds Wounds are attributable to trauma, such as in circumstances of accidents or attacks, or by surgical procedure and other therapeutic or diagnostic procedures. Infection and hemorrhage could complicate wounds, as do dehiscence, disruption of the wound layers, and evisceration, protrusion of inside organs by way of the lesion. This drainage, called exudate, additionally be} clear, bloody (sanguinous), or pus-containing (purulent). Proper wound therapeutic cleanliness and care of the lesion and also on proper circulation, good basic well being, and good vitamin. This additionally be} accomplished by cutting or scrubbing away the lifeless tissue or via enzymes. Most of the roots come from Latin and Greek; others are derived from German or French. They may be attributable to electrical malfunctions, contact with harmful chemical substances, or abrasion. Depth of tissue destruction is categorized as follows: · Superficial partial-thickness, which involves the epidermis and perhaps a portion of the dermis. The above classification replaces an older system of ranking burns as first-, second-, and third-degree in accordance with the depth of tissue harm. Infection is a standard complication of burns as a result of|as a end result of} a significant protection towards invasion of microorganisms is broken. Treatment of burns contains respiratory care, administration of fluids, wound care, and ache control. Monitoring for cardiovascular problems, infections, and signs of posttraumatic stress are also essential. The strain interrupts circulation, resulting in thrombosis, ulceration, and dying of tissue. Poor basic well being, malnutrition, age, obesity, and an infection contribute to the development of strain ulcers. If ignored, they could penetrate the skin and underlying muscle, extending even to bone, and should require months to heal. Pads or mattresses to relieve strain, common cleansing and drying of the skin, frequent change in position, and good vitamin help to forestall strain ulcers. Both of these phrases discuss with lying down in bed, though strain ulcers could appear in anyone with limited motion, not only those who are confined to bed. A persistent allergic type of this disorder that seems early in childhood is known as} eczema or atopic dermatitis. Although its precise cause is unknown, atopic dermatitis is made worse by allergic reactions, an infection, temperature extremes, and skin irritants. Other types of dermatitis include contact dermatitis, attributable to chemical irritants; seborrheic dermatitis, which involves areas with giant numbers of sebaceous glands such as the scalp and face; and stasis dermatitis, attributable to poor circulation. Psoriasis Psoriasis is a persistent overgrowth (hyperplasia) of the epidermis, producing giant, erythematous (red) plaques with silvery scales. Autoimmune Disorders the diseases discussed under are triggered, a minimum of|no less than} in part, by autoimmune reactions. Rupture of these lesions leaves deeper areas of the skin unprotected from an infection and fluid loss, much as in circumstances of burns. It is seen as rough, raised, violet-tinted papules, usually limited to the face and scalp. The skin lesions of lupus are worsened by exposure to the ultraviolet radiation in daylight. Scleroderma is a disease of unknown cause that involves thickening and tightening of the skin. A very early signal of scleroderma is Raynaud disease, by which blood vessels within the fingers and toes constrict within the chilly, inflicting numbness, ache, coldness, and tingling. Its price has been rising current years|in latest times|lately}, primarily due to the mutation-causing effects of the ultraviolet rays in daylight. Malignant melanoma results from an overgrowth of melanocytes, the pigment-producing cells within the epidermis. It is the most dangerous type of skin cancer due to its tendency to metastasize. It could unfold superficially for 1 or 2 years before it begins to invade the deeper tissues of the skin and to metastasize by way of blood and lymph. The prognosis for cure is sweet if the lesion is recognized and eliminated surgically before it enters this invasive stage. Squamous cell carcinoma and basal cell carcinoma are both cancers of epithelial cells. Squamous cell carcinoma seems as a painless, agency, red nodule or plaque which will develop surface scales, ulceration, or crusting. It is handled by surgical elimination and typically with x-irradiation or chemotherapy. Squamous cell carcinoma shown on the face and the back of the hand, sun-exposed areas may be} commonly affected. An initial translucent nodule spreads, leaving a depressed center and a agency, elevated border. Type I herpes simplex virus produces fluid-filled vesicles, usually on the lips, after fever, exposure to the solar, harm, or stress; chilly sore, fever blister. Excessive growth of hair A dry, scaly condition of the skin (from the basis ichthy/o, that means "fish") A bacterial skin an infection with pustules that rupture and type crusts; mostly seen in kids, usually on the face A raised, thickened scar attributable to overgrowth of tissue throughout scar formation Any skin condition marked by thickened or horny growth. Seborrheic keratosis is a benign tumor, yellow or mild brown in colour, that seems within the elderly. Actinic keratosis is attributable to exposure to daylight and should lead to squamous cell carcinoma. Thickened marks attributable to persistent rubbing, as seen in atopic dermatitis (a lichen is a flat, branching type of plant that grows on rocks and bark; see Fig. Beau lines, transverse depressions within the nails associated with acute extreme illness.
Proven 60mg evista
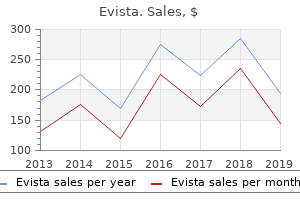
Amitriptyline allotting was the second highest at 29 per 100,000 in 2015/16 however decreased (-26%) over the time period. Sertraline and Citalopram had been subsequent at 19 and 18 per 100,000 in 2015/16 respectively. Sertraline and Escitalopram both got here into funded use during the study period and by 2015/16 had experienced large uptakes in use. For 1317-year olds (Table 4), Fluoxetine once more had the very best fee of allotting at 1,287 per 100,000 in 2015/16, almost double that of 07/08 and greater than three times higher than some other antidepressant. Sertraline, Amitriptyline, Escitalopram and Citalopram (in that order) had been the four different medication allotted at higher than 200 per 100,000 in 2015/16. The use of Sertraline and Escitalopram increased rapidly since they had been launched in 2010/11. Of antidepressants allotted over the whole study period Venlafaxine increased essentially the most, up 168% (from 26 per 100,000) and in 2015/16 was the seventh most allotted drug inside this age group. For 1824-year olds (see Table 5) Fluoxetine remained the drug with the very best allotting fee (1,990 per 100,000 in 2015/16); nevertheless, in contrast to|not like} the younger age groups, charges stayed largely fixed over the study period. Citalopram was the second most allotted drug, however declined in use over time (down 30% to 1,274 per 100,000). Venlafaxine allotting charges increased almost threefold between 2007/08 and 2015/16 from 262 to 740 per 100,000. Mori had the next highest charges, with 1,980 per 100,000 receiving an antidepressant in 2015/16. Rates for all ethnic groups increased over the period from 2007/08 to 2015/16, but the increase was steeper for Mori than for the other groups. Antidepressant allotting charges additionally varied by socioeconomic standing (see Figure 3). However, allotting charges for essentially the most deprived Dispensing by ethnicity and socioeconomic standing quintile (quintile 5) had been lower than for all different quintiles (27% lower than quintile 1 in 2015/16). Dispensing charges for all quintiles increased over the nine-year study period, however increases tended to be smaller as deprivation increased. During the nine-year period of this study, the entire variety of annual antidepressant prescriptions allotted to children and younger individuals increased by 68% from 111,171 in 2007/08 to 186,396 in 2015/16 and the speed of prescribing increased by 44% from 1,870 per 100,000 to 2,694 per 100,000. However, there was some notable variation in prescribing by ethnicity and socioeconomic standing. These variations may replicate changes to the pharmaceutical schedule, including availability of particular medications, medication subsidies and supply restrictions as well as|in addition to} evolution of evidence, including condition-specific therapy tips. Although reported allotting charges encompass both major and specialist service prescription, it also needs to|must also} be famous that entry to specialist psychological well being services (funded to address the top 3% of psychological well being conditions) has improved from 1. The most likely psychological well being problems to be handled with antidepressant medication are anxiety and depressive problems. Children are more doubtless to|usually tend to} expertise separation anxiety dysfunction and generalised anxiety dysfunction, whereas younger persons are more develop social phobia and panic dysfunction. Fluctuation occurs in the prevalence of particular person anxiety problems, with some decreasing and different increasing with age. Children and younger individuals of New Zealand European/Other ethnicities had the very best charges of antidepressant allotting, adopted by those of Mori, Asian and Pasifika origin. Both Mori and Pasifika individuals expertise higher charges of psychological well being dysfunction and scientific need. This problem requires additional scrutiny if dispensing-related well being disparities are to be lowered. Differences in antidepressant allotting by socioeconomic standing explained by two groups of things. The first, which most likely underpins the rise in allotting from the first to the 4th quintile, is the increased probability of psychological well being problems with increasing deprivation and related adversity. As bigger quantities of data become available in an exponentially increasing manner (2. However, such increased analytical energy needs to be balanced with the best to privacy for people, points of data ownership in life and demise, the veracity and completeness of obtainable information, mechanisms for managing surprising findings and agreed limits to the utilization of data. These centre on trust, clarity of data ownership and the balance of rights between data proprietor and data exploiter. The continued comparison with different ethnic groups with no enhancements is in itself a form of harm. As a end result, there has been an ongoing dialogue with indigenous data sovereignty groups. It additionally highlights limitations with these data and the place extra linked data could be useful. In addition, we had been in a position to} calculate accurate population denominators and entry socioeconomic deprivation and ethnicity information that may not otherwise have been available. Limitations of this study embrace ignorance concerning diagnoses and scientific causes for prescription, sequencing of antidepressant use, different treatments similar to psychotherapy and outcomes of therapy. For the moment, clinicians and researchers have to remember that there have been changes in antidepressant allotting over time and that there are discrepancies in allotting charges between children and younger individuals of various ethnicities and socioeconomic groups. Further linkage of diagnostic and therapy datasets is critical to meaningfully comment on the appropriateness of present prescriber practice and to examine in more detail inequalities and potential inequities similar to entry to care. Following this, interventions to address present disparities in allotting ought to be developed and evaluated. Future research of patterns of allotting could embrace length of therapy and dose throughout sociodemographic groups and over time which may mild on|make clear} well being disparities recognized. Finally, the current study ought to be repeated in 5 to 10 years to examine future allotting developments. Currently available data indicate that antidepressant prescribing to New Zealand children and younger individuals has increased throughout all age, sex and ethnic groups between 2006/7 and 2015/16, with some discrepancies between individuals of various ethnicities and deprivation. We additionally thank Professor Paul Glue, Rose Richards and Jesse Kokaua for their contributions. Only individuals authorised by the Statistics Act 1975 are allowed to see data a couple of specific person, family, enterprise, or organisation, and the outcomes in this paper have been confidentialised to shield these groups from identification and to hold their data secure. Further detail can be found in the Privacy impact evaluation for the Integrated Data Infrastructure available from A Canadian Primary Care Sentinel Surveillance Network Study Evaluating Antidepressant Prescribing in Canada From. Trends in the utilisation of psychotropic medications in Australia from 2000 to 2011. Longitudinal developments in the allotting of psychotropic medications in Australia from 20092012: Focus on children, adolescents and prescriber specialty. Trends and patterns of antidepressant use in children and adolescents from five western international locations, 20052012. Psychological therapies versus antidepressant medication, alone and in combination for depression in children and adolescents. Efficacy and security of selective serotonin reuptake inhibitors, serotonin-norepinephrine reuptake inhibitors, and placebo for widespread psychiatric problems amongst children and adolescents: a systematic evaluation and meta-analysis. Comparative efficacy and tolerability of antidepressants for major depressive dysfunction in children and adolescents: a network meta-analysis. Constructing entire of population cohorts for well being and social research using the New Zealand Integrated Data Infrastructure. Auckland: the Werry Workforce Whraurau for Infant, Child & Adolescent Mental Health Workforce Development, the University of Auckland; 2017. Twenty-five years of research on childhood anxiety problems: Publication developments between 1982 and 2006 and a selective evaluation of the literature. Annual Data Explorer 2016/17: New Zealand Health Survey 2017 [Available from: minhealthnz. Use of pharmacotherapy for insomnia in baby psychiatry practice: A nationwide survey. Psychiatric dysfunction and therapy in search of in a start cohort of younger adults: A report to to} the Ministry of Health. Wellington: the Christchurch Health and Development Study and the Ministry of Health.
Best 60 mg evista
One of the extra serious complications that may occur throughout transesophageal pacing is the formation of mucosal burns within the esophagus. Results in animal studies showed that present ranges above seventy five mA utilized for 30 minutes, or currents above 60 mA over 4 hours, produced kind of|this sort of|this sort of} damage. Transesophageal pacing has not been discovered useful for treating asystolic rhythms. During surgical implantation, the epicardial wires are sometimes hooked up to the proper atria and proper ventricle to allow for dual-chamber pacing if needed. This sort of pulse generator allows for control of cardiac rate, pacing present, and pulse width. Furthermore, distinction to|not like} the previous types of mills discussed, kind of|this sort of|this sort of} pulse generator allows for atria and ventricular sequential pacing. Function Temporary surgical implantation of epicardial leads is often performed throughout coronary artery bypass and different cardiac surgical procedures. During surgical implantation, the epicardial leads are sometimes utilized to each the proper atria and proper ventricle. Having epicardial leads on each the atria and the ventricle allows coronary heart beat|the heartbeat} generator to sense and tempo the guts in a extra pure sequence (atrial-ventricular sequential pacing). This sort of pacing is hemodynamically much like the intrinsic exercise of the guts and normally leads to elevated cardiac output and stroke quantity. In most circumstances, a set of two insulated stainless steel wires are flippantly sutured to epicardium of every chamber. Attaching two wires to each of the chambers allows for bipolar pacing (which typically decreases present required to get hold of capture). To distinguish the 2 sets of wires from one another, the surgeon will create separate exit factors out of the chest for each of the chamber electrodes. The pair of atrial electrodes normally exits from the proper facet of the sternum whereas the ventricular pair of electrodes normally exits from the left facet of the sternum. Direct Transthoracic Epicardial Lead Placement Direct transthoracic lead placement includes inserting a large-lumen needle via the left chest wall and into the pericardial area. This wire is then linked to an external pulse generator to act as the unfavorable pole for the pacing circuit. The transthoracic epicardial lead system allows for the electrical impulse produced by coronary heart beat|the heartbeat} generator to be instantly transmitted to the ventricular and atrial muscle tissues. Because of the direct cardiac stimulation, the transthoracic pacing therapy is much better tolerated by the patient than the previously discussed methods. Skeletal muscle and diaphragm stimulation is an unusual prevalence with this method. In the postsurgical setting, the atrial thransthoracic pacing electrode can also be|may additionally be|can be} used to document an atrial electrocardiogram. The uncovered portion with alligator clips, allowing for the interpretation of the intrinsic atrial impulse. This atrial recording could be very useful in determining the origin of narrow-complex tachycardias. This methodology of pacing has relatively low success rates in the bradycardia and asystolic patient. Because the epicardial leads are flippantly sutured onto the cardiac construction, elimination requires utilization of} gentle traction utilized to the external portion of the wire to pull may occur are ventricular or atrial lacerations with bleeding, cardiac tamponade, laceration of bypass grafts, laceration of the superior epigastric artery, and wire breakage ensuing in the retention of the distal portion of the epicardial lead. Finally, when you feel excessive resistance, immediately contact the surgeon to focus on how the lead must be removed. Transvenous Endocardial Pacing Settings for atrial and ventricular temporary epicardial pacing techniques are depending on the place the electrodes are positioned on the guts and might vary significantly between patients. The pacing present must be set at two times the threshold value achieved throughout preliminary epicardial lead implantation. The normal threshold values of each chambers differ greatly depending on the place of the electrode. Because of this ability, these mills normally allow for manipulation of the atrial and ventricular sensitivity settings. The normal sensitivity settings for an epicardial lead system are between 2 and 5 mV. Because transthoracic epicardial techniques allow for sequential atrial-ventricular depolarization, this methodology of pacing will typically require lower paced rates to achieve hemodynamic stability. The typical setting for the epicardial paced rate is between 70 and 90 beats per minute. Transvenous endocardial pacing for bradycardia has turn into the preferred methodology of treatment for patients may be} refractory to applicable medical therapy. Transvenous pacing is better tolerated by patients than transcutaneous and transesophageal pacing and is safer to perform than direct thoracic epicardial pacemaker insertion. Despite these benefits, the transvenous pacemaker insertion requires extra operator talent and training than the transcutaneous and transesophageal methods. Components Transvenous pacemakers utilize a lead-based electrode system to deliver the electrical impulse to the endocardium. The transvenous pacemaker 530 Invasive Cardiology could be set up to as} present therapy to the proper atrium, proper ventricle, or to each. The leads may be} used guided via the vascular system under direct fluoroscopy or by noting the hemodynamic tracings may be} recorded from the catheter throughout development. Once the balloon is inflated, the physician advances the catheter via the venous system, allowing the antegrade blood move to assist information the catheter into the cardiac chambers. This sort of pacing catheter normally has a dedicated port to allow for hemodynamic monitoring via the distal tip (much like a pulmonary artery stress catheter). When the atrial or ventricular stress waveform is noted, the pacing lead could be linked to coronary heart beat|the heartbeat} generator and pacing therapy could be initiated. Because the balloon tip may inhibit the pacing electrode from acquiring maximum contact with the endocardial tissues, the pacing thresholds for kind of|this sort of|this sort of} lead greater than with different transvenous lead techniques. This catheter is advanced via the vasculature using a fluoroscopic X-ray imaging system. The physician manipulates the catheter via the venous system until visual confirmation is made that the pacing electrodes are in the proper atrial or ventricular chambers. This sort of lead has higher pacing thresholds and long-term stability than the balloon assisted design; nevertheless, the stiffer catheter materials associated with extra complications. Finally, a very special J-tipped pacing catheter has been developed to help with proper atrial pacing. The J-tipped catheter is designed to get hold of catheter placement inside the proper atrial appendage. This specific placement helps improve atrial pacing thresholds and lead stability. There are a number of} different pulse mills that can be used for transvenous endocardial pacing (see Figure 37-6), and most pulse mills are designed to allow manipulation of the identical pacing parameters. Transvenous mills sometimes allow the operator to alter the pacing rate, rhythm, pacing present, and pacing pulse width. By altering this setting, the operator can manipulate the time between atrial and ventricular depolarization, allowing for max ventricular filling and stroke quantity. Function Transvenous pacing is performed by advancing electrode catheters into the guts and delivering the pacing impulse instantly into the endocardial tissues. Transvenous endocardial pacing could be utilized to get hold of proper atrial, proper ventricle, or dual-chamber pacing. This entry is normally obtained utilizing a modified Seldinger percutaneous approach, though a cutdown procedure could be performed to entry the brachial vein. There are a number of} veins may be} generally used as an entry point for transvenous lead insertion: internal jugular; external jugular; left or proper subclavian, brachial, or femoral veins. Though entry via each of these vessels is feasible, there are advantages and downsides to each of them. A latest study suggests that entry via the internal jugular vessel has the very best success rates for skilled and inexperienced operators and is associated with the lowest variety of complications. Furthermore, entry via the internal jugular presents a better, extra direct route of development into the proper atria and ventricle. However, this methodology leads to suboptimal efficiency, particularly when balloon-tipped or "pacing swans" are utilized. The concern with brachial entry is that even when the arm is sufficiently immobilized, the patient should be able to|be succesful of|have the flexibility to} transfer the arm sufficient to dislodge the electrode from the cardiac chamber. This chance decreases the suitability of the brachial vein for temporary endocardial lead placement. Internal jugular or subclavian venous entry allows for a extra secure lead placement and requires much less patient immobilization.
Evista 60mg
Canine tzone lymphoma: Unique immunophenotypic options, consequence, and population traits. Classification of canine malignant lymphomas in accordance with the World Health Organization criteria. Diarrhea disappeared immediately after general remedy with an anti-diarrheal drug. A mass lesion was discovered within the belly cavity by X-ray examination and echography. Intestinal obstruction was confirmed within the small intestine by barium contrast study. Small variety of eosinophils infiltrated among the tumor cells and fibrous stroma was slightly increased in some areas with proliferated tumor cell. Based on immunohistochemical findings, tumor cells have a T-cell phenotype in this lymphoma but lymph follicles shaped within the tumor mass consisted of B-cells. Laboratory Results: Fine needle biopsy findings: Comparatively uniform lymphoblastlike cells have been noticed on the smear from needle biopsy of the mesenteric lymph node. Histopathologic Description: Lymphoid cells proliferated all through the whole intestinal wall from the mucosa to the serosa and resulted in severe thickening of intestinal wall. Numerous lymphoid follicles of various dimension have been shaped within the muscular and serosal layer among the severely infiltrated tumor cells. The tumor cells apart from follicle-forming cells had small to medium-sized nuclei which might be} spherical to irregularly indented and a have thick nuclear membrane. The nuclei had dense chromatin with quantity of} small distinct nucleoli (or with a small distinct nucleolus). Small intestine, cat: the intestinal wall is markedly expanded and transmurally effaced by sheets of neoplastic cells. Small intestine, cat: Neoplastic cells have small quantities of cytoplasm and irregularly spherical nuclei with small blue nucleoli. Small intestine, cat: Non-neoplastic lymphoid follicles are scattered all through all layers of the intestinal wall, including the muscular tunics. In addition, this lymphoma had a T-cell phenotype and the follicles have been composed of B-cell phenotype. Therefore, it was likely that lymphoid follicles have been shaped outcome of} the reactive response to tumor cells or immunologic stimuli by the altered setting resulting in proliferation of tumor cells. Cytologically, T-cell lymphoma consists of smaller cells with low mitotic rate as within the current case. Lymphoepithelial lesions resemble epitheliotropism, but are characterised by centrocyte-like cell invasion and destruction of the epithelium. Intestinal lymphomas may be additional categorised as mucosal or transmural primarily based on depth of invasion. Epitheliotropism can happen in both types, and happens most commonly within the villous epithelium. T-cell rich giant B-cell lymphoma is an indolent kind with a blended cell population to embody weird giant or multinucleated cells and usually presents in a single lymph node. Theories concerning their formation have been exchanged, including immune stimulation by antigens or toxin absorption through the disrupted mucosal epithelium. Cytomorphological and immunological classification of feline lymphomas: clinicopathological options of seventy six cases. Immunophenotypic and histological characterization of 109 cases of feline lymhosarcoma. Epitheliotropic T-cell gastrointestinal tract lymphosarcoma with metastasis to lung and skeletal muscle in a cat. Feline gastrointestinal lymphoma: mucosal structure, immunophenotype, and molecular clonality. T-cell lymphoma with eosinophilic infiltration involving the intestinal tract in eleven canines. The possible prognostic significance of immunophenotype in feline alimentary lymphoma: a pilot study. Immunophenotypic and histologic classification of fifty cases of feline gastrointestinal lymphoma. In: Histological Classification of Tumors of the American System of Domestic Animals. Immunohistochemical prognosis of alimentary lymphomas and severe intestinal irritation in cats. The pet was vaccinated with Durammune-5, a combination vaccine towards canine distemper, canine adenovirus 2, canine parainfluenza virus, and canine parvovirus at roughly 1 pm. The pet died the next day and was offered to the diagnostic lab for necropsy examination. Gross Pathology: the animal was in enough nutritional condition evidenced by enough visceral and subcutaneous adipose tissue shops. The thymus contained numerous, multifocal, pinpoint, darkish purple foci (petechial hemorrhages). The intestines have been segmentally crammed with darkish brown, slightly flocculent, viscous digesta. Bacterial tradition revealed heavy progress of Escherichia coli and moderate progress of Proteus sp. Histopathologic Description: Liver: Diffusely within the liver parenchyma are quantity of} coalescing foci of hepatocellular swelling and necrosis. These foci are usually centrilobular to midzonal and sometimes lengthen to periportal areas. Necrotic hepatocytes current with a hypereosinophilic, micro-vacuolated to wispy cytoplasm, and nuclear fragmentation (karyorrhexis), pyknosis or complete lack of nuclear staining. Sinusoids inside necrotic foci are regularly expanded by erythrocytes (congestion and/or hemorrhages). Throughout all zones of the hepatic lobule, numerous hepatocytes, few endothelial cells and uncommon Kupffer cells include a large (up to 5 micron), stable amphophilic intranuclear viral inclusion physique that marginates the chromatin and is usually surrounded by a clear halo (Cowdry type-A). Cerebrum and liver, canine: A subgross retiform pattern of hepatic necrosis is seen within the liver. Liver, canine: Hepatocytes at edges of necrotic areas include giant intranuclear adenoviral inclusions (arrows). Within necrotic areas (center), plate structure is misplaced and hepatocyte nuclei are pyknotic or karyorrhectic. The tunica media is usually hypereosinophilic and disorganized, and blended with pyknotic nuclear debris (fibrinoid necrosis). Brain: Encephalitis, multifocal, moderate, acute, with vasculitis, hemorrhages and endothelial intranuclear viral inclusion bodies. The virus may be very stable within the setting, and may be excreted within the urine from previously contaminated animals for a lot as} 9 months. The virus initially localizes in tonsil and regional lymph nodes, finally spreading to the bloodstream roughly four days submit infection. Cerebrum, canine: Multifocally, capillary endothelium accommodates comparable adenoviral inclusions. Adjacent endothelium is necrotic, and erythrocytes are extravasated across the damaged vessel. Cerebrum, canine: In areas adjacent to damaged vasculature, giant halos adjacent to neurons and oligodendrocytes suggest marked edema. Histologically, typical lesions often encompass centrilobular to midzonal hepatic necrosis with general sparing of periportal hepatocytes. Cowdry kind A inclusions (marginated chromatin and clear halo across the inclusion) are seen in Kupffer cells, hepatocytes, and affected vascular endothelium. Lymphoid organs could also be} congested with necrosis of lymphoid follicles and intranuclear inclusions in vascular endothelium and histiocytes may be seen. Lesions in other organs are usually secondary to vascular endothelial damage and will encompass vascular necrosis, intravascular fibrin thrombi, hemorrhage, and edema. Adenoviruses are usually host particular and produce quantity of} notable illnesses (Table 1, chelonians, amphibians and fish not included).
Generic 60mg evista
One end of the segment is sealed, and the opposite drains through an opening in the belly wall. The muscle in the bladder wall Increased excretion of urine the quantity of filtrate shaped per minute by the nephrons of each kidneys the maximum fee at which a given substance could be transported across the renal tubule; tubular maximum the glomerular capsule and the glomerulus considered as a unit; the filtration system of the kidney A triangle on the base of the bladder shaped by the openings of the two ureters and the urethra. Incontinence might originate with a neurologic dysfunction, trauma to the spinal wire, weak point of the pelvic muscular tissues, urinary retention, or impaired bladder function. Any bladder dysfunction that outcomes from a central nervous system lesion Excessive urination at night time (noct/o means "night time") Edema by which the skin, when pressed firmly with the finger, will maintain the despair produced A hereditary condition by which the kidneys are enlarged and comprise many cysts Excessive thirst Elimination of enormous quantities of urine, as in diabetes mellitus Accumulation of urine in the bladder because of an inability to urinate A kidney stone that fills the renal pelvis and calyces to give a "staghorn" look. Causes an imbalance in the mobile surroundings with edema and other disturbances. A urine pattern obtained after thorough cleansing of the urethral opening and picked up in midstream to decrease the possibility of contamination A study of bladder function by which the bladder is crammed with fluid or air and the strain exerted by the bladder muscle at various levels of filling is measured. Calyx Pyramids of medulla Renal capsule Renal medulla Renal pelvis Renal cortex Ureter 2 5 three 6 four 1 7 1. A microscopic working unit of the kidney known as as} a(n). The cluster of capillaries within the glomerular capsule is the. The tube that carries urine from the kidney to the bladder is the. The primary nitrogenous waste product in urine is. A strong mold of the renal tubule discovered in the urine is a(n). Her gynecologist warned her that calcium could be be} a problem for discover themselves} "stone-formers. Urinalysis revealed no albumin, glucose, micro organism, or blood; there was proof of cells, crystals, and casts. Most of the staghorn was faraway from the renal pelvis with no remaining stone in the renal calices. She was discharged 2 days later and ordered to strain her urine for the subsequent week for proof of stones. Case Study 13-3: Set-Up for Cystoscopy Renovations had been completed just lately in the new surgical suite, and J. Each room had a new new} cystoscopy bed with padded knee crutches for lithotomy place, a drainage drawer for irrigation solution collection, and radiology functionality. The instrument storage carts have been stocked with inflexible and versatile cystoscopes, sheaths with obturators, and resectoscopes with assorted fulgurating loops, connectors, information wires, laser fibers, and fiberoptic gentle cords. Sterile storage closets held assorted urethral and ureteral catheters, irrigation tubing and syringes, collection baggage, biopsy needles and forceps, fundamental delicate tissue devices, and dressing provides. Each room had a machine to collect and decontaminate the liquid waste, instead of the previous flooring drains. A surgical endoscope that can enter and visualize the bladder is a(n), whereas a scope that cuts tissue known as as} a(n). A transurethral approach for examination or surgery always begins with inserting a catheter or scope: a. Label a diagram of the male reproductive tract and describe the function of every half. The gametes are generated by meiosis, a strategy of cell division that halves the chromosome quantity from forty six to 23. When female and male gametes unite in fertilization, the unique chromosome quantity is restored. The sex hormones assist in the manufacture of the gametes, function in pregnancy and lactation, and likewise produce the secondary sex traits corresponding to the standard dimension, form, physique hair, and voice that we affiliate with the female and male genders. In females, the two systems turn out to be utterly separate, whereas the male reproductive and urinary tracts share a standard passage, the urethra. T the Testes the male germ cells, the spermatozoa (sperm cells), are produced in the paired testes (singular, testis) would possibly be} suspended exterior of the physique in the scrotum. From puberty on, spermatozoa form repeatedly within the testes in coiled seminiferous tubules. Their improvement requires particular Sertoli cells and male sex hormones, or androgens, mainly testosterone. These hormones are manufactured in interstitial cells situated between the tubules. Transport of Spermatozoa After their manufacture, sperm cells are stored in a much-coiled tube on the surface of every testis, the epididymis. Here proceed to be} till ejaculation propels them right into a series of ducts that lead out of the physique. This duct ascends through the inguinal canal into the belly cavity and travels behind the bladder. A short continuation, the ejaculatory duct, delivers the spermatozoa to the urethra because it passes through the prostate gland below the bladder. Finally, the cells, now combined with other secretions, travel in the urethra through the penis to be launched. It enlarges on the tip to form the glans penis, which is covered by unfastened skin, the prepuce or foreskin. This additionally be} carried out for medical reasons, however is most frequently carried out electively in male infants for reasons of hygiene, cultural preferences, or religion. In the nervous system, the little swellings on the ends of axons that comprise neurotransmitters are variously known as end-feet, end-bulbs, terminal knobs, terminal ft, and even more. In the girl, the tube that carries the ovum from the ovary to the uterus is referred to as the oviduct, or perhaps the Fallopian tube. Some of the work of learning medical terminology is made more difficult by truth that|the truth that} many constructions and processes are known by two or even more names. This duplication might happen end result of|as a outcome of} completely different names have been assigned at completely different occasions or places or end result of|as a outcome of} the name is in a state of transition to another name and the new new} one has not been universally accepted. The tube that leads from the testis to the urethra in males was originally known as the vas deferens, vas being a general time period for vessel. To distinguish this tube from a blood vessel, efforts have been made to change the name to ductus deferens. The authentic name has lingered, nevertheless, end result of|as a outcome of} the surgical procedure used to Formation of Semen Semen is the thick, whitish fluid by which spermatozoa are transported. It incorporates, along with sperm cells, secretions from three forms of accent glands. The first of these, the paired seminal vesicles, release their secretions into the ejaculatory duct. The second, the prostate gland, secretes into the first the urethra beneath the bladder. As males age, enlargement of the prostate gland might compress the urethra and cause urinary issues. The two bulbourethral (Cowper) glands secrete into the urethra slightly below the prostate gland. Together these glands produce a slightly alkaline mixture that nourishes and transports the sperm cells and likewise protects them by neutralizing the acidity of the female vaginal tract. A mature reproductive cell, the spermatozoon in the male and the ovum in the feminine the bulbous end of the penis A sex gland; testis or ovary A hormone secreted by the pituitary that acts on the gonads. The channel through which the testis descends into the scrotum in the male Cells situated between the seminiferous tubules of the testes that produce hormones, mainly testosterone. Infection normally facilities in the urethra, causing urethritis with burning, a purulent discharge, and dysuria. Gonorrhea is handled with antibiotics, however there was rapid improvement of resistance to these medication by gonococci. Mumps is a nonsexually transmitted viral disease that can infect the testes and lead to sterility. Other microorganisms can infect the reproductive tract as well, causing urethritis, prostatitis, orchitis, or epididymitis.
References:
- https://www.augusta.edu/dentaltable/pdfs/goals/relievepain/diagnosingPatient5.pdf
- https://kellybrushfoundation.org/wp-content/uploads/2020/06/2020-Final-The-Active-Fund-Guidelines-SMApply.pdf
- https://www.lls.org/sites/default/files/file_assets/all.pdf
- https://memberfiles.freewebs.com/00/88/103568800/documents/Data.And.Computer.Communications.8e.WilliamStallings.pdf
- http://www.hixonparvo.info/Gene%20Cloning.pdf