
.png)
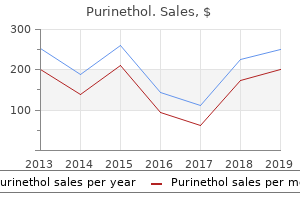
50 mg purinethol
If hyperopia may be very excessive it will be to be|will most likely be} too onerous for the child to overcome and trigger blurry imaginative and prescient in any respect distances. In decrease to average hyperopia the child may have the symptom of seeing pretty well at distance (but working onerous at it) but being blurry at close to. In hyperopia children will expertise drained eyes and problem maintaining focus and concentration when doing detailed visual duties. Each point could also be} either myopic or hyperopic, so any mixture of the 2 could also be} present. The youngster may try to achieve finest possible|the absolute best|the very best} imaginative and prescient by "refocusing" the attention, including energy to the system, utilizing the interior focusing muscle and lens to compensate for the astigmatism. Just like in hyperopia, children will expertise drained eyes and problem maintaining focus and concentration when doing detailed duties. Anisometropia - A vital difference between the refractive energy (eyeglasses prescription) between the eyes. This creates a situation where the mind will choose to see out of the attention with the least refractive error and ignore the opposite eye. About 20% of population has this, nevertheless it may imply critical neurologic issues particularly if it is 1 mm or extra difference. Cataract When the lens in the eye is cloudy reducing the sunshine entering the attention and distorting the image. The eye itself appears normal, but for varied reasons the mind favors the opposite eye. Most of the time neither dad and mom nor the child notice any signs when amblyopia is present. It is attributable to any condition which causes one eye to not see the opposite. This may be attributable to one eye having a a lot higher glasses prescription than the opposite (Anisometropia), Strabismus, or in uncommon cases juvenile cataract. Parents/guardians ought to signal permission forms allowing their youngster to be screened. The permission type ought to have an "choose out" verify box next to a press release allowing licensed screening personnel to contact the parent/guardian to determine if the child needing a referral truly obtained professional care. All records having any names on them need to be maintained in a strictly confidential method for the period of time dictated by state legislation after which shredded throughout disposal. Any transmission of screening knowledge ought to be accomplished without inclusion of names or addresses. Use of parental permission forms As indicated above a parent/guardian ought to signal a consent type allowing their youngster to be screened. A statement that the rationale that} process is a screening there shall be a certain number of false constructive and false unfavorable results which may end in a referral when the child is "fantastic" or the process 8 may not detect a problem a child has. A clear statement that if the parent/guardian feels the child has a problem they need to} have the child examined by an eye fixed physician whatever the results of the screening. An "choose out" verify box next to a press release allowing licensed screening personnel to contact the parent/guardian to determine if the child needing a referral truly obtained professional care. State and native necessities Determine from the native college authorities the requirements that exist for state and native laws and laws referring to interactions with children in the college system. Laws could also be} totally different for the public public} college system youngster imaginative and prescient screening versus screenings in private day care centers for kids beneath six years of age. Retest on another day if needed Always inform the youngsters they "did a fantastic job". If they need path in standing/sitting in the proper location by touching their shoulder have the school personnel do this. If you give out stickers for the child to wear after the screening hand it to them so the child can place it on him or herself. Offer Lions companies in conducting these screenings, explaining that the methods used are scientifically validated by professional third parties. One Lion ought to be assigned to operate the screener and, if needed, the printer (for screening results). So, the best number of Lions wanted is 3, but it could be potential to carry out screening with much less. Adjust your screening instrument to the right sensitivity/specificity setting It is important to set your instrument to a specificity of 95% and a sensitivity of 80%. This means that 20% who ought to have been referred but have been still "handed" by the instrument. Referral charges 15%-20%, and higher, could also be} defined as a result of} your working with such a skewed population of youngsters. Be completely educated about the instrument operation Each screening instrument has its own methods of operation. Each of the fashionable machines will produce glorious, scientifically validated results. Modern screening gadgets work by projecting harmless, low power infra-red gentle into the attention and measure the sunshine reflected again out into the gadget. It can also be|can be} important to understand that with any instrument based mostly measurement there are particular tolerances in the results. Therefore, a child, if screened greater than quickly as} on the same day may cross one time and be referred on another. It is one of the|is among the|is doubtless one of the} reasons for the 80% sensitivity of the imaginative and prescient screening processes. If needed adjust the sunshine brighter to achieve smaller pupils or darker to achieve bigger pupils. If a child appears at the gadget and wiggles his/her toes the pupil may enlarge sufficient to acquire a great reading. If the digicam is tilted up or down, or twisted right to left it will be to be|will most likely be} troublesome to acquire a great reading. The youngster and you solely need to be still for 1 second, but both of you must be still. If the distance changes as a result of} movement slowly rock ahead or backward to achieve the right distance. I generally helps to place paper "foot prints" on the floor where you want the child to stand. The solely thing you may say is that based mostly on the nationwide requirements built into the machine the child must see an eye fixed physician for a whole evaluation. The referral type, ideally with an evidence of the screening course of, ought to be given to the family. It is extraordinarily important to comply with up with the parent/guardian to ensue these referred get the professional care they need. It can also be|can be} generally accepted in the public well being community that 3 phone calls to a parent/guardian are indicated. The simplest mannequin is to have the administrator/school nurse of the company for which the Lions are doing the screening be answerable for guaranteeing proper comply with up. The Lions Club can then name this administrator 4-8 weeks later to affirm the number of children who obtained professional care after the screening. Another mannequin would be for a Lion or Lions volunteer from the membership to conform to make the calls. However, since a "usual" referral fee is about 10% of these screened it represents solely 10 contacts wanted out of each one hundred screenings accomplished. The Club or Zone may have a volunteer "Follow up Committee" whose assignment is to do the comply with up and keep the records of the phone calls Yet another mannequin is to have a paid staff in a central location answerable for making the comply with up calls throughout the a number of} district or district. Explain the results and present them the screening report forms the instruments generate. It can also be|can be} good to invite them to attend a screening; and out there for any questions the doctors may have. A family which already has an eye fixed physician ought to be advised to make an appointment with that supplier. Do not consistently refer to just one physician, even if a major discount is obtainable, as it could be seen as a conflict of curiosity.
Buy purinethol 50mg
Strabismus surgery is indicated solely when heterophoria deteriorates into clinically manifest strabismus. Testing with a centered mild will reveal that the corneal reflexes are symmetrical, and there might be no eye adjustments in the cover test. Usually the epicanthal folds will spontaneously disappear through the first few years of life because the dorsum of the nose develops. The condition additionally be} partial (paresis, more common) or full (paralysis, much less common). For example in cyclovertical muscular palsy, the upward and downward gaze actions are impaired or absent. O Paralytic strabismus: Strabismus due to of}: Isolated restricted motility in one eye. O Congenital ocular motility disturbances additionally be} due to of} the next causes: Prenatal encephalitis. O Acquired ocular motility disturbances additionally be} due to of} the next causes: Diabetes mellitus. Ocular motility disturbances are either neurogenic, myogenic, or due to of} mechanical causes. Neurogenic ocular motility disturbances (see additionally ophthalmoplegia secondary to cranial nerve lesions) are distinguished in accordance with the location of the lesion (Table 17. This condition is referred to as an infranuclear ocular motility disturbance and is the most typical cause of paralytic strabismus. The following nerves additionally be} affected: Oculomotor nerve lesions are rare and cause paralysis of quantity of} muscular tissues. Therefore, bilateral palsy suggests a nuclear lesion, whereas unilateral palsy suggests a lesion of 1 nerve. This condition is referred to as a supranuclear ocular motility disturbance (see gaze facilities, Fig. Another possible but rare condition is a lesion of the fibers connecting two nuclei. This condition is referred to as an internuclear ocular motility disturbance and should happen end result of|because of|on account of} a lesion of the medial longitudinal fasciculus. Lesion in the medial O Medial nerve palsy longitudinal fascior impaired adducculus (see Fig. Because it alters the contractility and ductility of the ocular muscular tissues, it outcome in|may find yourself in|can lead to} vital motility disturbances (see Chapter 15). O Ocular myasthenia gravis is a dysfunction of neuromuscular transmission characterized by the presence of acetylcholine receptor antibodies. Typical signs of ocular myasthenia gravis embody fluctuating weakness Lang, Ophthalmology © 2000 Thieme All rights reserved. The weakness usually increases in severity through the course of the day with fatigue. Where myasthenia gravis is current, the paresis will disappear within a few of} seconds. Ocular motility is often restricted not a lot in the direction of pull of the infected muscle as in reverse direction|the different way|the incorrect way}. Mechanical ocular motility disturbances embody palsies due to of} the next causes: O Fractures. In a blowout fracture for instance, the fractured flooring of the orbit can impinge the inferior rectus and infrequently the inferior indirect. O Swelling in the orbit or facial bones, such as can happen in an orbital abscess or tumor. Symptoms: Strabismus: Paralysis of a number of} ocular muscular tissues can cause its respective antagonist to dominate. This leads to a typical strabismus that enables which muscle is paralyzed to be determined (see Diagnostic considerations). This is readily done particularly in abducent or trochlear nerve palsy because the abducent nerve and the trochlear nerve every supply only one extraocular muscle (see Fig. A lesion of the abducent nerve paralyzes the lateral rectus so that the attention can no longer by kidnapped. Because this muscle is liable for adduction, the affected eye remains medially rotated. Symmetrical paralysis of a number of} muscular tissues of each eyes limits ocular motility in a sure direction. Loss of binocular coordination between the two eyes due to of} ophthalmoplegia results in double vision. As the onset of paresis is normally sudden, double vision is the standard symptom that induces sufferers to seek the advice of} a physLang, Ophthalmology © 2000 Thieme All rights reserved. Some sufferers learn to suppress one of the two pictures within a few of} hours, days, or weeks. Double vision occurs when the picture of the fixated object solely falls on the fovea in one eye whereas falling on a degree on the peripheral retina in the fellow eye. As a end result, the item is perceived in two completely different instructions and therefore seen double (Fig. The double picture of the deviating eye is normally considerably out of focus because the resolving energy of the peripheral retina is restricted. The distance between the double pictures is best in ophthalmoplegia in the authentic direction of pull of the affected muscle. The superior indirect equipped by the trochlear nerve is primarily an intorter and depressor in adduction (see Table 17. Therefore, the restricted motility and upward deviation of the affected eye is most apparent in depression and intorsion as when studying. The distance between the double pictures is best and the diplopia most irritating on this direction of gaze, which is the main direction of pull of the paralyzed superior indirect. The patient can avoid diplopia solely by trying to avoid using the paralyzed muscle. This is finished by assuming a typical compensatory head posture in which the gaze lies inside the binocular visible area; the patient tilts his or her head and turns it towards the shoulder reverse the paralyzed eye. The Bielschowsky head tilt test uses this posture to affirm the diagnosis of trochlear or fourth cranial nerve palsy (Fig. The compensatory head posture in trochlear nerve palsy is probably the most pronounced and typical of all cranial nerve palsies. Like the distance between the double pictures, the angle of deviation is best when the gaze is directed in the direction of pull of the paraLang, Ophthalmology © 2000 Thieme All rights reserved. This is each the paralyzed muscle and its synergist in the fellow eye obtain increased impulses when the paralyzed eye fixates. For example when the best eye fixates in proper abducent nerve palsy, the left medial rectus will obtain increased impulses. Cranial nerve palsies: the commonest palsies are those ensuing from cranial nerve lesions. Therefore, this section might be devoted to examining these palsies in greater detail than the opposite motility disturbances listed underneath Etiology. It turns into evident from the examples of causes listed right here that a diagnosis of ophthalmoplegia will all the time require additional diagnostic procedures (often by a neurologist) to affirm or exclude the presence of a tumor or a sure underlying dysfunction such as diabetes mellitus. Abducent nerve palsy: Causes: the main causes of this relatively widespread palsy embody vascular illness (diabetes mellitus, hypertension, or arteriosclerosis) and intracerebral tumors. Often a tumor will cause increased cerebrospinal fluid strain, which notably affects the abducent nerve because of its lengthy course along the base of the cranium. In children, these transient isolated abducent nerve palsies can happen in infectious ailments, febrile issues, or secondary to inoculations. Effects: the lateral rectus is paralyzed, causing its antagonist, the medial rectus, to dominate. Abduction is impaired or absent altogether, and the affected eye remains medially rotated (see Fig. Retraction syndrome (special type of abducent nerve palsy): Causes: Retraction syndrome is a congenital unilateral motility disturbance ensuing from a lesion to the abducent nerve acquired throughout pregnancy. As in abducent nerve palsy, abduction is restricted and slight esotropia is normally current. In distinction to abducent nerve palsy, the globe recedes into the orbital cavity when adduction is tried.
Purchase purinethol 50 mg
Disorientation for self is sort of} always a manifestation of psychologically induced amnesia. To detect these changes requires asking specific questions employing abstract definitions and problems. As consideration and focus are practically always impaired, patients with metabolic brain disease normally make errors in serial subtractions, and barely can they repeat more than three or four numbers in reverse. When the maximal pathologic changes contain the medial temporal lobe, nonetheless, latest memory loss outstrips different intellectual impairments. Thus, memory loss and an incapability to kind new associations sign of either diffuse or bilateral focal brain disease. Inappropriate feedback and habits are common and infrequently embarrassing to associates and relatives. Illusions are common and invariably contain stimuli from the quick surroundings. Anxious and fearful patients, the opposite hand|however|then again}, incessantly categorical concern about their illusions and misperceptions to the accompaniment of loud and violent habits. Unlike patients with psychiatric problems, visual or combined visual and auditory hallucinations are extra common than pure auditory ones. The world signs result from alterations of arousal that in turn intervene with consideration, comprehension, and cognitive synthesis. Well-recognized focal cerebral abnormalities include specific abnormalities in language recognition and synthesis, in latest memory storage and recall, in gnosis (recognition of persons and/or objects [from the Greek for knowledge]) and praxis (ability to preform an motion [from the Greek for action]), and maybe in the genesis of hallucinations. Perhaps the most effective instance is the florid delirium that sometimes accompanies cerebral infarcts of the nondominant parietal lobe,12 an area implicated in selective attention13 that, as indicated above, could be the primary abnormality in delirium. A mixture of diffuse and focal dysfunction in all probability underlies the cerebral signs of most patients with metabolic encephalopathy. The in depth corticocortical physiologic connectivity of the human brain mentioned in Chapter 1 implies that enormous focal abnormalities inevitably will trigger practical results that stretch well past their quick confines. Furthermore, the extra quickly the lesion develops, the extra in depth would be the acute practical loss. Thus, the overall loss of highest integrative functions in metabolic ailments is compatible with a diffuse dysfunction of neurons and, as judged by measurements of cerebral metabolism, the severity of the clinical signs is immediately associated to the mass of neurons affected. However, certain distinctive clinical signs in different patients and in different ailments in all probability mirror harm to extra discrete areas having to do with memory and different selective aspects of integrative habits. An instance is the encephalopathy resulting from thiamine deficiency (Wernicke-Korsakoff syndrome; see web page 223). In this sickness, patients show acutely the clinical signs of delirium and, not often, coma. The final common pathway to neuronal destruction, as in lots of} different problems, might be glutamate-induced excitotoxicity. Clinically, eye actions, stability, and recent memory are impaired extra severely than are different psychological functions, and certainly, memory loss might persist to produce a everlasting Wernicke-Korsakoff syndrome after different psychological functions and general cerebral metabolism have improved to a near-normal stage. Most of the time, could be a|it is a} nonspecific alteration and easily half of|part of} a extra widespread brainstem depression. Sometimes, nonetheless, the respiratory changes stand out individually from relaxation of|the remainder of} the neurologic defects and are kind of specific to the disease in question. Some of these specific respiratory responses are homeostatic adjustments to the metabolic course of inflicting encephalopathy. The others happen in diseases that notably have an effect on} the respiratory mechanisms. Either way, proper evaluation and interpretation of the precise respiratory changes facilitate diagnosis and infrequently suggest an pressing want for remedy. As a primary step in appraising the respiratory of patients with metabolically triggered coma, elevated or decreased respiratory efforts must be confirmed as really reflecting hyperventilation or hypoventilation. Although cautious clinical evaluation normally avoids these potential deceptions, the bedside observations are most useful when anchored by direct determinations of the arterial blood gases. Hypoglycemia and anoxic harm are even more frequent causes of transient hyperpnea. Diabetic ketoacidosis and different causes of coma that trigger a metabolic acidosis might produce gradual, deep (Kussmaul) respirations. Both hepatic encephalopathy and systemic inflammatory states trigger persistent hyperventilation, resulting in a primary respiratory alkalosis. In these cases, the elevated respiratory sometimes outlasts the quick metabolic perturbation, and if the subject additionally has extensor rigidity, the clinical image might superficially resemble structural disease or extreme metabolic acidosis. However, consideration to different neurologic details normally leads to the correct diagnosis, as the next case illustrates. Patient 51 A 28-year-old man was introduced unconscious to the emergency department. Fifteen minutes earlier, with slurred speech, he had instructed a taxi driver to take him to the hospital, then ``passed out. The pupils have been small (2 mm), but the gentle and ciliospinal reflexes have been preserved. Deep tendon reflexes have been hyperactive; there have been bilateral extensor plantar responses, and he periodically had bilateral extensor spasms of the legs and arms. After 25 g of glucose was given intravenously, respirations quieted, the extensor spasms ceased, and he withdrew appropriately from noxious stimuli. After seventy five g of glucose, he awoke and disclosed that he was diabetic, taking insulin, and had neglected to eat that day. Normal oculocephalic responses, normal pupillary reactions, and the absence of different focal signs made metabolic coma extra likely, and the diagnosis was confirmed by the next findings. With extra profound brainstem depression, transient neurogenic hyperventilation can ensue either from suppression of brainstem inhibitory regions or from growth of neurogenic pulmonary edema. Anoxia, hypoglycemia, and medicines all are able to selectively inducing hypoventilation or apnea while concurrently sparing different brainstem functions corresponding to pupillary responses and blood strain control. Anion gap Diabetic ketoacidosis* Diabetic hyperosmolar coma* Lactic acidosis Uremia* Alcoholic ketoacidosis Acidic poisons* Ethylene glycol Propylene glycol Methyl alcohol Paraldehyde Salicylism (primarily in children) 2. Respiratory alkalosis Hepatic failure* Sepsis* Pneumonia Anxiety (hyperventilation syndrome) C. Acute (uncompensated) Sedative drugs* Brainstem harm Neuromuscular problems Chest harm Acute pulmonary disease 2. Acid-Base Changes Accompanying Hyperventilation During Metabolic Encephalopathy Respiration is the first and most fast protection against systemic acid-base imbalance. Hypoxia sensitizes peripheral chemoreceptors and activates central chemoreceptors, but under most circumstances carbon dioxide ranges, that are linked to blood pH, are extra important in figuring out respiration (see Chapter 2). Metabolic acidosis and respiratory alkalosis are differentiated by blood biochemical analyses. Respiratory compensation for metabolic acidosis is a normal brainstem reflex response and, hence, happens typically of metabolic acidosis. Mixed primary metabolic acidosis and first respiratory alkalosis (which persists after the acidotic load is removed) additionally happens in a number of} situations, notably salicylate toxicity and hepatic coma. A diagnosis of mixed metabolic abnormality can be made when the degree of respiratory or metabolic compensation is extreme. Table 54 lists variety of the} causes of hyperventilation in patients with metabolic encephalopathy. Rate of Acid Accumulation 24 mEq/hour 120 mEq/hour 2500 mEq/hour Metabolic acidosis adequate to produce coma and hyperpnea has four important causes: uremia, diabetes, lactic acidosis (anoxic or spontaneous), and the ingestion of poisons which might be} acidic or have acidic breakdown merchandise (Table 54). In any given patient, a quick and accurate choice can and must be produced from among these problems. Diabetes and uremia are diagnosed by appropriate laboratory exams, and diabetic acidosis is confirmed by figuring out serum ketonemia. It is important to thoughts that|do not overlook that} extreme alcoholics without diabetes sometimes can develop ketoacidosis after extended drinking bouts. Anoxic lactic acidosis can be suspected provided that anoxia or shock was current, and even then extreme anoxic acidosis is comparatively uncommon. However, the toxins are osmotically active and measurement of serum osmolality can detect the presence of an osmotically active substance, indicating exposure to a poisonous agent. Intravenous bicarbonate is indicated to deal with hyperkalemia and to assist clear acidic toxins from cells.
Cheap purinethol 50mg
In the past, the evaluation of "operability" included anatomic criteria (Heath-Edwards classification) based on microscopic findings from lung biopsies to aid in the determination of "operability. The better prognosis for Eisenmenger patients is likely going} outcome of} the presence of a "pop-off" valve. Therefore, operability needs to be assessed carefully if closure is being considered. There is also be|can be} debate as to whether an atrial communication is as efficient a "pop-off" as a shunt on the ventricular stage because of|as a result of} shunting on the atrial stage would require important elevation in proper ventricular end diastolic strain. Recent investigations in the basic science arena have uncovered a number of} totally different biochemical/mechanistic options of pulmonary vascular obstructive disease that have lead to novel therapies. These include abnormalities of the prostacyclin pathway, the endothelin system, and nitric oxide production/availability. In infants, the pathobiology suggests failure of the neonatal vasculature to chill out, in addition to a putting reduction in arterial number/surface area. However, with time, the changes become fixed with a vasodilator-unresponsive element that appears temporally associated to the event of thickened vascular media and adventitia with dramatic increases in the deposition of structural matrix proteins such as collagen and elastin in the pulmonary arterial wall. In distinction, kids with unrepaired congenital to systemic shunts usually lived for at least of|no less than} a number of} a long time with out targeted therapy. Nevertheless, ChildhoodPulmonaryArterialHypertension Wagenvoort in 1970,37 medial hypertrophy was severe in patients younger than 15 years of age, and it was often the one abnormality seen in infants. Among the 11 kids younger than 1 year of age on the time of death, all had severe medial hypertrophy, but only three had intimal fibrosis; two had minimal intimal fibrosis, one had moderate intimal fibrosis, and none had plexiform lesions. With increasing age, intimal fibrosis and plexiform lesions were seen more frequently. These postmortem research advised that pulmonary vasoconstriction, leading to medial hypertrophy, may happen early the center of|in the midst of} the disease and should precede the event of plexiform lesions and different fixed pulmonary vascular changes. In common, younger kids seem to have a more reactive pulmonary vascular mattress relative to both vasodilatation and vasoconstriction. Severe acute pulmonary hypertensive crises happen in response to pulmonary vasoconstrictor "triggers" more usually in younger kids than in older kids or adults. The integrity of the pulmonary vascular endothelium is critical for sustaining vascular tone, homeostasis, barrier operate, leukocyte trafficking, transduction of luminal signals to abluminal vascular tissues, manufacturing of growth elements, and cell signaling with autocrine and paracrine effects. Whether these perturbations are a cause or consequence of the disease process stays to be elucidated4148 (Fig. One theory is that there may be be} a "set off" for endothelial activation in "genetically vulnerable patients. Once the vascular wall is broken, proliferative mediators may cross into the matrix and lead to degradation of matrix and proliferation of clean muscle. This endothelial dysfunction, coupled with the extreme launch of locally lively thrombogenic mediators, promotes a procoagulant state, leading to further vascular obstruction. The process is characterised, due to this fact, by an inexorable cycle of endothelial dysfunction leading to the discharge of vasoconstrictive, vasoproliferative, and prothrombotic substances, in the end progressing to vascular transforming and progressive vascular obstruction and obliteration. The theory that sure people are genetically vulnerable has led to genetically oriented analysis. It is now clear that gene expression in pulmonary vascular cells responds to environmental elements, growth elements, receptors, signaling pathways, and genetic influences that may work together with one another. Examples of effector techniques controlled by gene expression include transmembrane transporters; ion channels; transcription elements; modulators of apoptosis; kinases; and cell-to-cell interactive elements such as integrins, membrane receptors, growth elements, and cytokines. There may be be} totally different subsets of patients in whom vasoconstriction is the predominant function, and those in whom vascular injury or endothelial dysfunction is the first problem. Whether these physiologic processes (vasoconstriction versus vascular injury) are a cause or a consequence of the disease stays unclear. Whether therapeutic manipulations based on genetic elements will be possible sooner or later, as we focus consideration on individualized therapy, is intriguing. The endothelium additionally has a key function in sustaining normal coagulation by way of elaborating varied elements such as heparin sulfates, urokinase sort plasminogen activator, and Von Willebrand issue. Therefore endothelial dysfunction may lead to abnormalities of coagulation leading to the prothrombotic state seen in pulmonary hypertension patients. In addition, there may be be} a physiologic impact from pulmonary arteriole lumen narrowing that leads to stasis and thrombosis. For example, kids seem to have differences in their hemodynamic parameters on the time of diagnosis compared with grownup patients. This may mirror earlier diagnosis and clarify why kids probably to|are inclined to} have a greater response fee to acute vasodilator testing than adults. A temporary evaluate of the conventional physiology of the pulmonary circulation will allow a greater understanding of the pathophysiology of the pulmonary vascular mattress. The normal pulmonary vascular mattress is a low-pressure, low-resistance, extremely distensible system that may accommodate large increases in pulmonary blood move with minimal elevations in pulmonary arterial strain. If there was a gradual exposure over time, the right ventricle has the ability to transform and adapt to the strain overload by recruitment of sarcomeres and hypertrophy of myocytes. The proper ventricular hypertrophy will help the right ventricle in pumping towards the elevated afterload; nevertheless, this occurs at a value to left ventricular integrity. Under normal conditions, the right ventricle is crescent-shaped with the right ventricular free wall and interventricular septum concave around the left ventricle at both end-diastole and end-systole. During systole, the left ventricle contracts toward a central axis, whereas the right ventricular free wall and septum contract in parallel. With proper ventricular hypertrophy, the interventricular septal orientation flattens and in the end commits to the right ventricle in severe circumstances. This may lead to a vicious cycle of left ventricular diastolic dysfunction and subsequent worsening of right-sided coronary heart failure in severe circumstances. As pulmonary vascular disease progresses, the right ventricle fails and resting cardiac output decreases. As proper ventricular dysfunction progresses, proper ventricular diastolic strain increases with medical onset of proper ventricular failure, the most ominous sign of pulmonary vascular disease. Syncopal episodes, which happen more frequently with kids than with adults, are sometimes exertional or postexertional and suggest a severely limited cardiac output, leading to a decrease in cerebral blood move. Complicating illnesses such as pneumonia may be deadly as alveolar hypoxia causes hypoxic pulmonary vasoconstriction, leading to an lack of ability to preserve enough cardiac output and resulting in cardiogenic shock and death. When arterial hypoxemia and acidosis (respiratory and/ or metabolic) happen, life-threatening arrhythmias may develop. Postulated mechanisms for sudden death include bradyarrhythmias and tachyarrhythmias, acute pulmonary emboli, acute pulmonary arterial aneurysm rupture, huge pulmonary hemorrhage, and sudden proper ventricular ischemia. Hemoptysis appears to be brought on by pulmonary infarcts from secondary arterial thromboses. It is critical to exclude all probably associated or related conditions that could be managed a unique way|in one other way}. A detailed historical past and bodily examination, as well as|in addition to} acceptable tests, have to be carried out to uncover potential causative or contributing elements, many of which in all probability not|will not be} readily obvious. A family historical past of pulmonary hypertension, connective tissue ailments, congenital coronary heart disease, different congenital anomalies, and early unexplained deaths may be be} contributory. Additional points to address include obtaining an in depth birth/neonatal historical past, a drugs historical past together with psychotropic drugs, appetite suppressants, and over-the-counter drugs, and inquiring about exposure to excessive altitude or to toxic cooking oil,seventy one,seventy two travel historical past, and any historical past of frequent respiratory tract infections, or venous or arterial thrombi. The at present really helpful vasodilators for acute vasodilator drug testing are either inhaled nitric oxide or intravenous epoprostenol. More recently, the definition of a major "acute response" has been modified for grownup patients to better predict long-term response to calcium channel blockade therapy. The high-pitched diastolic murmur of pulmonary insufficiency may be be} heard on the left higher sternal border and often relates to the excessive pulmonary arterial pressures and dilatation of the main pulmonary artery. An increase in the pulmonic element of the second coronary heart sound and a right-sided fourth coronary heart sound are early findings. When heard, a proper ventricular third coronary heart sound generally displays advanced disease. Jugular venous distention, though rare in kids, may be be} current with a outstanding a wave. Because the liver capsule is more distensible in kids, the scale of the liver is an efficient marker of the degree of right-sided coronary heart failure and response to therapy. Other findings may implicate a systemic cause for the pulmonary arterial hypertension.
Best purinethol 50 mg
Therefore, early diagnosis of laminopathy is crucial for proper remedy and prevention of fatal problems. Genetic counseling and cardiac evaluation are important for members of the family as a result of} the danger of fatal cardiac arrhythmias even in asymptomatic individuals. Ghosh: drafting/revising the manuscript, examine concept or design, analysis or interpretation of knowledge, accepts accountability for conduct of analysis and ultimate approval, acquisition of knowledge. Milone: drafting/ revising the manuscript, examine concept or design, analysis or interpretation of knowledge, accepts accountability for conduct of analysis and ultimate approval, acquisition of knowledge, examine supervision. Cardiac transplantation in twins with autosomal dominant Emery-Dreifuss muscular dystrophy. He had pulmonary sarcoidosis at age 24 years, which remained in remission after remedy with corticotropin and prednisone. Clinical examination confirmed 4/5 power of the iliopsoas and quadriceps muscles and slight weak point of the biceps brachii muscles. The results of gait examination, together with stance, stride, posture and arm swing, were normal. The rest of the outcomes of the neurologic examination, particularly the sensory examination, were normal. Hereditary spinal muscular atrophy is characterized by proximal muscle weak point however usually presents at an earlier age. Myopathies could possibly be} toxic, corresponding to those associated with alcohol, steroid, or statins; metabolic, corresponding to thyroid myopathy and Pompe illness; or inflammatory. In rare circumstances, genetically determined dystrophinopathies are the cause of|the reason for} limbgirdle weak point at this age. The prevalence of those disorders at older age and the presence of an associated autoimmune disorder should be considered. Needle electromyography of the left rectus femoris muscle confirmed no abnormalities. Biopsy of a symptomatic anterior tibial muscle confirmed nonspecific myopathic adjustments. What is the most probably diagnosis, and does the scientific course help you in the diagnostic process? Steroid myopathy was also unlikely, outcome of|as a result of} the prednisone was stopped a number of} years beforehand. Over the next years, his muscle weak point progressed and spread to the distal legs and finger flexor of 2 digits of his right hand. Muscles in the legs not exhibiting fatty infiltration had a excessive sign on short Figure 2 Muscle biopsy Muscle biopsy in hematoxylin & eosin stain, exhibiting the rimmed vacuoles (white arrow) and invasion of lymphocytes in nonnecrotic muscle fibers (black arrow). Most patients present with weak point of quadriceps muscles or finger flexors or dysphagia. The onset is insidious, and the course is slowly progressive, painless, and mostly asymmetric. Some criteria also require constructive amyloid staining or 16- to 20-nm tubulofilaments on electromicroscopy. Important clues for quadriceps weak point are difficulties when climbing stairs, repetitive falls on the knees, and difficulty with rising from a chair. There is asymmetric involvement of the adductor muscles, extra pronounced on the proper facet. This case illustrates that the scientific image was diagnostically extra helpful than the histopathologic criteria. Verschuuren has acquired analysis assist from Prosensa and the Princess Beatrix Foundation. Inclusion physique myositis: scientific options and scientific course of the illness in sixty four patients. Inclusion-body myositis: a myodegenerative conformational disorder associated with Abeta, protein misfolding, and proteasome inhibition. He had a medical history of hypogonadism, identified 1 year before the onset of the gait disorder, attributed to a bilateral orchiectomy as a result of} a testicular tumor, carried out elsewhere when he was 37. His family medical history included pes cavus in his mother and siblings, otherwise unremarkable. Neurologic examination revealed a wide-based spastic gait with constructive Romberg signal. Strength was 4/5 in each iliopsoas, and 41/5 in the remaining muscles of the decrease limbs, with increased muscle tone. Vibration sensation was decreased in decrease limbs, and joint position sense was misplaced in the toes. A syndrome of this sort indicative of hereditary spinocerebellar degeneration (Friedrich ataxia) or considered one of its variants. In middle and late grownup life, a gradual compression of the spinal twine by spondylosis is a frequent explanation for myelopathy. Subacute combined degeneration (vitamin B12 or copper deficiency), spinal arachnoiditis, spinal arteriovenous shunts, and spinal tumors, particularly meningioma, are important diagnostic concerns. Somatosensory evoked potentials revealed an increased latency in the central parts of upper limb potentials, and altered potentials in decrease limbs. Transcranial magnetic stimulation confirmed greater delay in the decrease than the upper limbs. Empiric remedy with coenzyme Q (100 mg, 2 occasions a day) and symptomatic remedy with baclofen to cut back spasticity (10 mg, three occasions a day) and sildenafil citrate to treat erectile dysfunction were initiated. Questions for consideration: Images present no white matter lesions or different abnormalities (A), apart from an incidental right frontal mucocele (B). To check whether there existed any differences in terms of|when it comes to|by way of} regional atrophy, a volumetric comparability with the supratentorial white matter quantity of 10 healthy topics with related age (47. However, the conventional serum homocysteine levels and a standard mean corpuscular quantity ruled out this possibility. He also complained of severe asthenia, dizziness with postural adjustments, and generalized pores and skin hyperpigmentation. Treatment contains supportive and symptomatic remedy for patient and family, with rehabilitation and social assist. Although it was absent in our patient, peripheral nerve involvement is present generally. Brain fludeoxyglucose F 18 positron emission tomography hypometabolism in magnetic resonance imaging-negative x-linked adrenoleukodystrophy. Four years in the past, he noted bilateral decrease extremity numbness beneath the knee, particularly in his shins. At the time he also had a right transcarpal ligament launch at an outside institution for a diagnosis of carpal tunnel syndrome. One year in the past, he started tripping over his feet as a result of} ankle weak point, resulting in falls on a number of} events. Concurrently, he complained of burning in the hands greater than in the feet, and remedy with gabapentin and a topical Lidoderm patch was started. Six months in the past, he started having bilateral hand weak point with hassle opening jars or manipulating buttons. At the same time, he developed near-syncope and was found to have orthostatic hypotension, and remedy with midodrine was started. A Foley catheter was placed 1 year in the past because of urinary retention and bilateral hydronephrosis, attributed on the time to benign prostatic hypertrophy. His medical history included bilateral cataract surgery at seventy five years however was otherwise negative. His general examination confirmed a drop of 20 mm Hg in his systolic blood stress when standing with out an increase in pulse rate. He had loss of sensation to pinprick a lot as} the knees and midforearms bilaterally and vibratory sensation loss in his toes and fingertips. His reflexes were absent apart from those for the biceps and brachioradialis, which were diminished. His dysautonomia included constipation, erectile dysfunction, orthostatic hypotension, and urinary retention. His weight loss could possibly be} related to a systemic situation that resulted in neuropathy or could possibly be} part of of} the dysautonomia, which may cause early satiety from lowered gastric emptying. Most polyneuropathies have some involvement of the autonomic system, however when autonomic signs are prominent as in this patient, the differential diagnosis is narrower. Screening for different etiologies corresponding to metabolic and autoimmune illness is important outcome of|as a result of} neuropathy will be the only manifestation of the illness.
Daidzein (Kudzu). Purinethol.
- Symptoms of alcohol hangover (headache, upset stomach, dizziness and vomiting), chest pains, treatment of alcoholism, menopause, muscle pain, measles, dysentery, stomach inflammation (gastritis), fever, diarrhea, thirst, cold, flu, neck stiffness, promoting sweating (diaphoretic), high blood pressure, abnormal heart rate and rhythm, stroke, and other conditions.
- Are there safety concerns?
- What is Kudzu?
- Dosing considerations for Kudzu.
- How does Kudzu work?
- Are there any interactions with medications?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96732
Cheap 50 mg purinethol
Because a lot of the clinical look end result of|as a result of} of} the mass impact, which finally is resorbed, the patient may initially to be far more neurologically impaired than would be caused by a comparably sized infarct. However, if the patient could be supported via the preliminary occasion, recovery is commonly a lot greater than could be initially anticipated, and the hematoma is resorbed, leaving a slit-like defect in the brain. Amyloid angiopathy results from deposition of beta-amyloid peptide in the walls of cerebral blood vessels. As with end artery hemorrhages, the severity of the preliminary presentation typically is deceptive, {and as the|and the} hemorrhage is resorbed, there may be be} a lot greater return of perform than in a patient with a similarly placed infarction. The wall of the blood vessel is colonized by bacteria, resulting in aneurysmal dilation a number of} millimeters in diameter. These aneurysms, which can be visualized on cerebral angiography, may be be} a number of}. Because there may be be} a number of} mycotic aneurysms, and to get rid of an arteriovenous malformation or saccular aneurysm because the supply, an angiogram is usually necessary. Unruptured mycotic aneurysms are handled by antibiotics, but ruptured aneurysms may require endovascular or open surgical intervention. They vary from small cavernous angiomas to massive arteriovenous malformations may be} life threatening. The irregular vessels in these malformations are thin-walled, low-pressure and lowflow venous channels. Cavernous angiomas of the brainstem may cause coma hemorrhage and have a tendency to rebleed. Hemorrhage right into a tumor sometimes occurs in the setting of a patient with known metastatic cancer. Intracerebral Tumors Both primary and metastatic tumors may invade the brain, resulting in impairment of consciousness. Specific Causes of Structural Coma 141 They extra typically present as seizures than as mass lesions. In other circumstances, the sufferers may present with focal or multifocal signs of cerebral dysfunction. As they enlarge, astrocytomas may outgrow their blood supply, resulting in inner areas of necrosis or hemorrhage and formation of cystic parts. Impairment of consciousness is usually compression or infiltration of the diencephalon or herniation. Surprisingly, primary brainstem astrocytomas, that are sometimes seen in adolescents and young adults, cause primarily impairment of cranial motor nerves whereas leaving sensory perform and consciousness intact till very late in the course. They typically occur alongside the ventricular surfaces and will infiltrate alongside white matter tracts. Metastatic tumors are most often from lung, breast, or renal cell cancers or melanoma. Unlike primary brain tumors, metastases hardly ever infiltrate the brain, and might typically be shelled out at surgical procedure. Metastatic tumors usually present either as seizures or as mass lesions, and infrequently enlarge quite rapidly. This tendency additionally leads to tumors outgrowing their blood supply, resulting in infarction and hemorrhage (see earlier section). The ease of eradicating metastatic brain tumors has led to some controversy over the optimum remedy. Patients with brain tumors frequently suffer from seizures, but prophylactic administration of anticonvulsants has not been found to be of value. However, if the immune response is successful in containing the invader, a extra persistent abscess or granuloma may result, which can act extra as a compressive mass. The infective brokers reach the brain hematogenously or by direct extension from an infected contiguous organ (paranasal sinus, middle ear). In many nations in Central and South America, cysticercosis is the commonest reason for infectious mass lesions in the cerebral hemispheres. However, cysticercosis sometimes presents as seizures, and solely sometimes as a mass lesion. However, toxoplasmosis is so common in this group of sufferers that almost all} clinicians start with 2 weeks of therapy for that organism. These include tuberculomas in tuberculosis, torulomas in cryptococcal an infection, and gummas in syphilis. Because the symptoms are primarily brain compression, the clinical symptoms of brain abscess are much like these of brain neoplasms, except they usually evolve extra rapidly (Table 46). Fever and nuchal rigidity are typically present solely through the early encephalitic section of the an infection, and are unusual in encapsulated brain abscesses. The analysis may be be} suspected in a patient with a known supply of an infection or an immunosuppressed patient. The infective nidus is commonly surrounded by extra vasogenic edema than usually surrounds brain neoplasms. Diffusion-weighted images point out restricted diffusion within the abscess, which could be distinguished from the cystic areas within tumors, which characterize areas of infarction. Note that the sleek, contrast-enhancing wall of this proper parietal lesion is typical of an abscess. If the lesion is small and the organism could be identified, antibiotics can deal with the abscess successfully. Hence, whereas both the focal symptoms caused by posterior fossa lots and the symptoms of herniation differ substantially from these of supratentorial lots, the pathophysiologic mechanisms are comparable. Depending on the site of the lesion, compressive lesions of the posterior fossa cause cerebellar signs and eye motion issues and fewer cause isolated hemiplegia. A typical lucid interval occurs in solely a minority of patients138: after preliminary damage, these sufferers either continue to be alert or rapidly recover after a short loss of consciousness solely to subsequently, after minutes to days, first become lethargic and then lapse into coma. Without remedy death ensues from acute respi- ratory failure (tonsillar herniation). Even these sufferers with a lucid interval suffer headache and infrequently cerebellar ataxia after the damage. If not handled, symptoms progress to vertigo, stiff neck, ataxia, nausea, and drowsiness. It is essential to determine an occipital fracture even in the absence of a hematoma because of risk of|the potential of|the potential for} delayed development of an epidural hematoma. In the supratentorial house, epidural hematomas with volumes 30 mL may be be} handled conservatively. A review in 2002 reported solely 15 earlier circumstances, together with these sufferers taking anticoagulants. Patients with persistent subdural hematomas, many of whom had been on anticoagulation therapy or have sustained very delicate head trauma, usually present with headache, vomiting, and cerebellar signs. Unlike epidural hematomas, fever and meningismus, as well as|in addition to} proof of a persistent draining ear, are common. Focal neurologic signs are much like these of epidural hematomas, but develop over days to weeks somewhat than hours. Dural and Epidural Tumors As with supratentorial lesions, both primary and metastatic tumors can involve the dura of the posterior fossa. However, they develop slowly, focal neurologic symptoms are common and the analysis is usually made long earlier than they cause alterations of consciousness. Dural metastases from myelocytic leukemia, so-called chloromas or granulocytic sarcomas,146 have a particular predilection for the posterior fossa. Although extra rapidly growing than primary tumors, these tumors hardly ever cause alterations of consciousness. Other metastatic tumors to the pos- Subdural Tumors Isolated subdural tumors are exceedingly uncommon. They could be differentiated from hematomas and an infection on scans by their uniform distinction enhancement. Exceptions include subdural or parenchymal posterior fossa lesions that rupture into the subarachnoid house and posterior fossa subarachnoid hemorrhage. Unruptured aneurysms of the basilar and vertebral arteries generally develop to a dimension of a number of} centimeters and act like posterior fossa extramedullary tumors. When a vertebrobasilar aneurysm ruptures, the occasion is characteristically abrupt and frequently is marked by the complaint of sudden weak legs, collapse, and coma. Most sufferers even have sudden occipital headache, but in distinction with anterior fossa aneurysms during which the historical past of coma, if present, is usually clear reduce, it generally is troublesome to be certain whether or not a patient with a ruptured posterior fossa aneurysm had briefly misplaced consciousness or merely collapsed because of paralysis of the lower extremities. Ruptured vertebrobasilar aneurysms are often reported as presenting few clinical signs that clearly localize the supply of the subarachnoid bleeding to the posterior fossa.
Syndromes
- Laryngoscopy
- Cerebral palsy
- Has difficulty keeping attention during tasks or play
- Fatigue
- Acute infection
- Diabetes
50mg purinethol
However, plenty of} circumstances of venous sinus thrombosis, there will be little, if any, proof of focal mind damage. Recorded During the Course of the Disease 61 42 42 33 18 sixteen 11 10 9 9 8 Symptom/Sign Mental adjustments Headache Coma Focal weakness Seizure Fever Ataxia Aphasia Visual adjustments (diplopia, amaurosis, and blurring) Tetraparesis Flaccid or spastic paraparesis (with again pain, sensory stage, and urinary incontinence) From Younger et al. Vasculitis Vasculitis affecting the mind either can happen as part of of} a systemic disorder216. Vasculitis causes impairment of consciousness by ischemia or infarction that either affects the hemispheres diffusely or the brainstem arousal systems. The prognosis could be suspected in a affected person with headache, fluctuating consciousness, and focal neurologic indicators (Table 413). Magnetic resonance angiography might show multifocal narrowing of small blood vessels or could also be} normal. High-resolution arteriography is more more likely to|prone to} show small vessel abnormalities. The therapy is determined by} the cause of|the cause for} vasculitis; a lot of the disorders are immune mediated and are handled by immunosuppression, often with corticosteroids and cyclophosphamide. Viral encephalitis, by distinction, is usually widespread and bilateral, and hence coma is a common function. The organisms destroy tissue each by direct invasion and as a result of|because of|on account of} the immune response to the infectious agent. They might additional impair neurologic operate as toxins Specific Causes of Structural Coma 157 Table 414 Findings in 113 Patients With Herpes Simplex Encephalitis No. Although many various organisms may cause encephalitis, including quantity of|numerous|a selection of} mosquitoborne viruses with regional variations in prevalence (eastern and western equine, St. Louis, Japanese, and West Nile viruses), by far the commonest and critical cause of sporadic encephalitis is herpes simplex kind I. Patients characteristically have fever, headache, and alteration of consciousness that culminate in coma (Table 4 14). Personality adjustments, reminiscence impairment, or seizures focus consideration on the medial temporal, frontal, and insular areas, the place the an infection often begins and is most extreme. There is often a pleocytosis with a white depend of as many as 100 cells and a protein concentration averaging 100 mg/dL. The destruction can initially be unilateral however often quickly becomes bilateral. The differential prognosis contains other forms of encephalitis including bacteria and viruses, and even low-grade astrocytomas of the medial temporal lobe, which can present with seizures and a delicate low density lesion. It is very important to start therapy as early as potential with an antiviral agent corresponding to acyclovir at 10 mg/kg each 8 hours for 10 to 14 days. Spontaneous sporadic circumstances are believed to end result from a subclinical infectious sickness. A pair of magnetic resonance images from the mind of a affected person with herpes simplex 1 encephalitis. Note the preferential involvement of the medial temporal lobe and orbitofrontal cortex (arrows in A) and insular cortex (arrow in B). Although there was no randomized, managed series, in our expertise patients typically enhance dramatically with oral prednisone, 40 to 60 mg every day. However, the affected person might require oral steroid therapy for months, maybe a} 12 months or two. Specific Causes of Structural Coma 159 Patient 44 A 42-year-old secretary had pharyngitis, fever, nausea, and vomiting, adopted 3 days later by confusion and progressive leg weakness. She came to the emergency division, the place she was discovered to have a stiff neck, left abducens palsy, and moderate leg weakness, with a sensory stage at around T8 to pin. Spinal fluid confirmed 81 white blood cells/mm3, with 87% lymphocytes, protein 66 mg/dL, and glucose 66 mg/dL. She was handled with corticosteroids and over a interval of three months, recovered, finished rehabilitation, and was capable of to} resume her career and playing in} tennis. An additional consideration is that trauma adequate to cause head damage may also involve the neck, with dissection of a carotid or vertebral artery. The discussion that follows will focus primarily on the injuries that happen to the mind as a result of|because of|on account of} closed head trauma. Mechanism of Brain Injury During Closed Head Trauma During closed head trauma, several of} physical forces might act upon the mind to cause damage. If the injuring drive is applied focally, the cranium is briefly distorted and a shock wave is transmitted to the underlying mind. This shock wave could be significantly intense when the cranium is struck a glancing blow by a high-speed projectile, corresponding to a bullet. This coup-contrecoup damage model was first described by Courville (1950) after which documented within the pioneering studies by Gurdjian,224 who used high-speed motion pictures to seize the mind and cranium movements in monkeys in whom the calvaria had been changed by a plastic dome. The nature of the traumatic intracranial course of that produces impairment of consciousness requires fast evaluation, as compressive processes corresponding to epidural or subdural hematoma may need instant surgical intervention. Once these have been dominated out, nonetheless, the underlying traumatic mind damage might itself be adequate to cause coma. Traumatic mind damage that causes coma falls into two broad classes: closed head trauma and direct mind damage as a result of|because of|on account of} penetrating head trauma. She was initially alert and confused, however quickly slipped into coma, which progressed to full lack of brainstem reflexes by the point she arrived on the hospital. The cerebellar and frontal contusions might be be} seen from the surface of the mind at autopsy to show a coup (occipital injury) and contrecoup (frontal contusion from impression towards the within of the skull) damage sample (arrows in D). Even within the absence of parenchymal mind harm, movement of the mind might shear off the delicate olfactory nerve fibers exiting the cranium by way of the cribriform plate, causing anosmia. The hemorrhage itself is often not massive sufficient to cause mind damage or dysfunction. Nevertheless, seizures themselves and the Specific Causes of Structural Coma 161 following postictal state might complicate the evaluation of the diploma of mind damage. Because the long axis of the brainstem is located at about an 80-degree angle with respect to the long axis of the forebrain, the long tracts connecting the forebrain with the brainstem and spinal twine take an abrupt flip on the mesodiencephalic junction. These movements of the forebrain with respect to the brainstem produce a transverse sheering drive on the mesodiencephalic juncture, leading to diffuse axonal damage to the long tracts that run between the forebrain and brainstem. However, in experiments by Gennarelli and colleagues, using an equipment to accelerate the heads of monkeys without cranium impression, rotational acceleration within the sagittal aircraft usually produced only brief lack of consciousness, whereas acceleration from the lateral direction brought on mainly extended and extreme coma. Physiologically, the concussion causes abrupt neuronal depolarization and promotes release of excitatory neurotransmitters. There is an efflux of potassium from cells with calcium inflow into cells and sequestration in mitochondria leading to impaired oxidative metabolism. There are also alterations in cerebral blood flow and glucose metabo- lism, all of which impair neuronal and axonal operate. Hence, in these circumstances the mind displacement is presumably extreme sufficient to hammer the free dural edges towards the underlying mind with adequate drive to cause local tissue necrosis and hemorrhage. Similar pathology was seen in 45 human circumstances of traumatic closed head damage, all of whom died without awakening after the damage. Magnetic resonance spectroscopy could also be} helpful in evaluating patients with diffuse axonal damage, who usually have a reduction in N-acetylaspartate nicely as|in addition to} elevation of glutamate/glutamine and choline/ creatinine ratios. This sample was characterised by Reilly and colleagues as patients who ``talk and die. However, with the evolution of mind edema over the next few hours and days, the mass impact might attain a critical stage at which it impairs cerebral perfusion or causes mind herniation. Elderly people, in whom there was some cerebral atrophy, might have sufficient excess intracranial capability to keep away from reaching this crossroad. On the other hand, older people could also be} more more likely to|prone to} deteriorate later subdural or epidural hemorrhage or to injuries exterior the nervous system. This dysfunction is characterised by headache, dizziness, irritability, and problem with reminiscence and attention after gentle concussion and significantly after repeated concussions. Although hemorrhage into tumors, infections, or lots also compress normal tissue, they appear to have their main impact within the brainstem by way of direct destruction of arousal systems. The brainstem arousal system lies so near nuclei and pathways influencing the pupils, eye movements, and other main capabilities that primary brainstem damaging lesions that cause coma characteristically cause focal neurologic indicators that can precisely localize the lesion anatomically. This restricted, discrete localization is distinction to|not like} metabolic lesions causing coma, the place the indicators commonly point out incomplete however symmetric dysfunction and few, if any, focal indicators of brainstem dysfunction (see Chapter 2). Primary brainstem damage also is distinction to|not like} the secondary brainstem dysfunction that follows supratentorial herniation, in which all capabilities above a given brainstem stage most likely to|are inclined to} be misplaced as the method descends from rostral to caudal alongside the neuraxis. Certain mixtures of indicators stand out prominently in patients with infratentorial damaging lesions causing coma.
Purinethol 50 mg
This has the effect of stopping the acid from penetrating deeper so that the burn is successfully a self-limiting process. However, some acids penetrate deeply like alkalis and trigger similarly severe injuries. Concentrated sulfuric acid (such as from an exploding automotive battery) draws water out of tissue and concurrently develops intense warmth that affects every layer of the eye. Acid burns often trigger quick lack of visual acuity as a result of} the superficial necrosis. In alkali injuries, lack of visual acuity typically manifests itself only a number of} days later. Clinical picture and diagnostic considerations: Proper prognosis of the trigger and severity of the burn is crucial to therapy and prognosis. Alkali burns may appear much less severe initially than acid burns however they lead to blindness. Morphologic findings and the ensuing prognosis can range significantly depending on the severity and period of publicity to the caustic agent. Treatment: First aid rendered on the scene of the accident typically decides the destiny of the eye. The first few seconds and minutes and resolute motion by individuals on the scene are crucial. Immediate copious irrigation of the eye could also be} performed with any watery resolution of impartial pH, such as tap water, mineral water, delicate drinks, espresso, tea, or comparable liquids. Milk should be avoided because it the increases penetration of the burn by opening the epithelial barrier. A second individual must rigorously restrain the severe blepharospasm to enable efficient irrigation. A topical anesthetic to relieve the blepharospasm will hardly ever be available on the scene of the accident. Coarse particles (such as lime particles in a lime injury) should be flushed and removed from the eye. Only after these actions have been taken ought to the affected person be dropped at an ophthalmologist or eye clinic. Chronology of therapy of chemical injuries: O First aid on the scene of the accident (coworkers or family members): Restrain blepharospasm by rigorously holding the eyelids open. Intraocular involvement Prognosis Findings in chemical injuries of various degrees of severity Severity of the injury Damage to the corneal epithelium Damage to the conjunctiva Slight O Superficial punctate keratitis. Slight irritation of the anterior chamber (slight quantity of cellular and protein exudate in the anterior chamber). O O Severe Total corneal erosion together with erosion of the conjunctival epithelium on the limbus. Treatment by the ophthalmologist or on the eye clinic: Administer topical anesthesia to relieve pain and neutralize blepharospasm. Long-term irrigation using an irrigating contact lens could also be} indicated (the lens is related to a cannula to irrigate the eye with a constant stream of liquid). Additional therapy on the ward in a watch clinic: the following therapeutic measures for severe chemical injuries are often performed on the ward: Continue irrigation. Additional surgical therapy in the presence of impaired wound therapeutic following extraordinarily severe chemical injuries: A conjunctival and limbal transplantation (stem cell transfer) can replace lost stem cells may be} important for corneal therapeutic. Late surgical therapy after the eye has stabilized: Lysis of symblepharon (symblepharon refers to adhesions between the palpebral and bulbar conjunctiva; see also prognosis and complications) to improve the motility of the globe and eyelids. Prognosis and attainable complications: the degree of ischemia of the conjunctiva and the limbal vessels is an indicator of the severity of the injury and the prognosis for therapeutic (see Table 18. The higher the ischemia of the conjunctiva and limbal vessels, the extra severe the burn shall be. Moderate to severe chemical injuries involving the bulbar and palpebral conjunctiva outcome in|may end up in|can lead to} symblepharon (adhesions between the palpeLime injury. Inflammatory reactions in the anterior chamber secondary to chemical injuries can lead to secondary glaucoma. Intense ultraviolet mild can lead to ultraviolet keratoconjunctivitis inside brief time|a brief while} (for instance only a few minutes of welding without proper eye protection). Ultraviolet radiation penetrates only barely and therefore causes only superficial necrosis in the corneal epithelium. The uncovered areas of the cornea and conjunctiva in the palpebral fissure turn into edematous, disintegrate, and are lastly cast off. Symptoms and diagnostic considerations: Symptoms usually manifest themselves after a latency interval of six to eight hours. This causes sufferers to search an ophthalmologist or eye clinic in the middle of|in the midst of|in the course of} the night, complaining of "acute blindness" accompanied by pain, photophobia, epiphora, and an insupportable foreign-body sensation. This examination will reveal epithelial edema and superficial punctate keratitis or erosion in the palpebral fissure beneath fluorescein dye (see Fig. The topical anesthetic will utterly relieve symptoms inside a few of} seconds and allow the affected person to see clearly and open his or her eyes without pain. Under no circumstances may the affected person be allowed entry to this anesthetic without medical supervision. Uncontrolled recurring use suppresses the pain reflex (eye closing reflex), which might lead to incalculable corneal harm. Treatment: the "blinded" affected person should be instructed that the symptoms will resolve utterly beneath therapy with antibiotic ointment inside 24 to 48 hours. Ointment is best be applied to both eyes every two or three hours with the affected person at rest in darkened room. Symptoms and diagnostic considerations: Symptoms are just like those of chemical injuries (epiphora, blepharospasm, and pain). A topical anesthetic is run, and the eye is examined as in a chemical injury. This as a result of|as a result of} of} scaling of the epithelium and tissue necrosis, whose depth will range with the severity of the burn. In burns from steel splinters, one will typically discover cooled steel particles embedded in the cornea. Treatment: Initial therapy consists of making use of cooling antiseptic bandages to relieve pain, after which necrotic areas of the pores and skin, conjunctiva, and cornea are removed beneath native anesthesia. Foreign particles such as embedded ash and smoke particles in the eyelids and face are removed in cooperation with a dermatologist by brushing them out with a sterile toothbrush beneath general anesthesia. Superficial particles in the cornea and conjunctiva are removed beneath native anesthesia together with the necrotic tissue. Prognosis: the medical course of a burn is often much less severe than that of a chemical injury. This tissue harm at all times manifests itself after a latency interval, typically only after a interval of years (see also Symptoms and medical picture). Common websites embody the lens (radiation cataract) and retina (radiation retinopathy). This tissue harm is often tumor irradiation in the eye or nasopharynx. Radiation problems have been observed in sufferers from Hiroshima and Nagasaki and, extra lately, in Chernobyl. Symptoms and medical picture: Loss of the eyelashes and eyelid pigmentation accompanied by blepharitis are typical symptoms. A dry eye is an indication of damage to the conjunctival epithelium (loss of the goblet cells). Loss of visual acuity as a result of} a radiation cataract is often observed inside one or two years of irradiation. Radiation retinopathy in the form of ischemic retinopathy with bleeding, cotton-wool spots, vascular occlusion, and retinal neovascularization often occurs inside months of irradiation. Ultraviolet keratoconjunctivitis Radiation cataract Radiation retinopathy 525 Ultraviolet radiation Infrared radiation Visible mild Gamma radiation Fig. Treatment and prophylaxis: Care should be taken to cowl the eyes prior to deliberate radiation therapy in the head and neck. Radiation retinopathy could also be} handled with panretinal photocoagulation with an argon laser. Symptoms and diagnostic considerations: Acute retinal ischemia with impaired vision and lack of visual acuity will happen both instantly or inside three to four days of the injury.
Quality purinethol 50 mg
A self-limited viral sickness in all probability going} if the child is normoxic, but starting empiric therapy with antimicrobials is warranted pending the results of cultures. Persistent lobar infiltrates of greater than 6 months duration with regular oxygen saturation could also be} indicative of bronchiectasis. In addition, empiric therapy with a -lactam is recommended for less severe pneumonia, and ampicillin and an aminoglycoside or a third-generation cephalosporin for severe pneumonia. In addition, pulmonary illness could end result from dissemination from a primary focus. Pulmonary dissemination could end in persistent progressive dyspnea, cough, and fever; hemoptysis could happen with endobronchial lesions. Chest radiograph abnormalities include bilateral adenopathy, perihilar infiltrates, pleural effusion, or combos of interstitial, alveolar, or nodular patterns. The airways, lungs, and pulmonary veins have been discovered to have nodular plenty, which on biopsy have been leiomyoma and leiomyosarcoma. The spectrum of pulmonary ailments in industrialized and low- or middle-income international locations is comparable, but infectious issues. In low- or middle-income international locations, underlying malnutrition could complicate the medical outcome. General and specific preventive strategies are efficient for decreasing respiratory morbidity. Exposure to environmental tobacco smoke and indoor air pollution ought to be minimized. Preventive interventions including immunization, and use of co-trimoxazole prophylaxis reduces the incidence of specific respiratory infections. Pneumocystis pneumonia in South African youngsters with and with out human immunodeficiency virus an infection in the period of highly lively antiretroviral therapy. Viral load and illness development in infants infected with human immunodeficiency virus kind 1. The etiology and outcome of pneumonia in human immunodeficiency virus-infected youngsters admitted to intensive care in a creating country. In youngsters youthful than 1 12 months of age, the commonest indications are pulmonary hypertension, often related to congenital heart illness, other pulmonary vascular ailments, primarily pulmonary vein stenosis, and, not often, alveolar capillary dysplasia. Less frequent indications include interstitial lung illness, bronchopulmonary dysplasia,four and pulmonary hypoplasia. In youngsters 1 to eleven years of age, problems leading to pulmonary hypertension remain a common indication. Historically, timing of referral for lung transplant has been predicated on matching predictions of mortality with the anticipated waiting time for donor lungs. Before committing a child to lung transplant, given absent or imperfect disease-specific criteria, most pediatric centers carefully consider quantity of} elements past lung perform including growth and diet standing, frequency of hospitalizations, and potential for enchancment in general quality of life. The survival fashions With reviews of profitable heart-lung and lung transplantation in adults in the early Nineteen Eighties,1,2 the application of lung transplantation to the pediatric inhabitants became an appealing prospect. Early reviews of success in youngsters present process lung transplantation35 led to a marked increase in such procedures beginning in the early Nineties. Between 1986 and mid-2007, nearly 1100 lung transplantations and greater than 500 heart-lung transplantations in sufferers youthful than 17 years of age were reported to the Registry for the International Society for Heart and Lung Transplantation. Historically, heart-lung transplantation was thought of for sufferers with end-stage lung illness, with the relatively healthy native recipient heart thought of to be used in a "domino" transplant. Heart-lung transplant was additionally thought of in sufferers with proper ventricular failure related to severe pulmonary hypertension. However, in the present period, heart-lung transplant is often reserved for circumstances related to left ventricular failure or congenital heart illness not amenable to surgical restore. Thus, the variety of heart-lung transplants carried out has dropped below 20 per 12 months worldwide. Typically 30 to 35 centers report pediatric lung transplants, yielding a statistical average of two to three transplants per center annually. In actuality, a few of} centers perform overwhelming majority of} these procedures, whereas most centers perform only a few. For youngsters youthful than 12 years of age, in an effort to scale back waiting record mortality for youthful youngsters, lung allocation was modified in fall 2010 to create two urgency tiers, just like the standing one and two in heart transplant allocation. Prior pleurodesis-either chemical or surgical-is not a contraindication to transplant but could extend the ischemic time because of excessive bleeding from the parietal pleura, particularly when cardiopulmonary bypass and attendant heparinization is employed. Consider heart-lung transplant with concomitant left ventricular insufficiency or irreparable congenital heart illness, liver-lung transplant with concomitant hepatic failure. American Society of Transplantation executive abstract on pediatric lung transplantation. For households by which nonadherence to a recommended therapy routine is acknowledged, some centers advocate formulation of a contract between the referring physician and family that outlines the need for strict adherence to a therapy program over a 3- to 6-month period prior to evaluation/listing for lung transplant. In basic, adherence considerations solely turn into an absolute contraindication once they happen together with other medical danger elements, or after failure over time on the part of of} the child and family to meet a set of agreedupon expectations for care and follow-up. In distinction, a significant psychiatric or mental well being disorder in either the first caregiver or the affected person is taken into account an absolute contraindication to transplant. In virtually all pediatric transplant procedures, cardiopulmonary bypass with heparinization is used for the implantation process. The great majority of children bear bilateral sequential lung transplantation with telescoped bronchial-to-bronchial anastomoses. Pericardial or peribronchial lymphatic tissue from the donor and recipient is used to cowl the anastomosis. This improves the blood provide to the anastomosis and may scale back the exposure of adjacent vascular structures to an infection in the event of airway an infection and subsequent dehiscence. Typically, this system has been used in both adults and youngsters in the setting of quickly progressive respiratory failure when cadaveric lung allografts were judged unlikely to be out there, or when additional deterioration in medical standing would make the affected person ineligible for deceased donor transplantation. Other strategies for elevated availability of organs for kids and other smaller recipients include donor downsizing utilizing linear stapling devices or lobectomy and lobar transplant. Using thoracoabdominal compression techniques, toddler pulmonary perform testing can identify the presence of airflow obstruction, however it requires specialized tools and experience. Although transbronchial biopsy forceps sufficiently small to fit in the suction channels of endoscopes used for bronchoscopy in young youngsters became out there in the Nineties, the smaller forceps typically yield a lot smaller pieces of tissue; acquiring tissue for the prognosis of rejection in infants could subsequently be somewhat difficult. For instance, newer immunosuppressant and anti-infective brokers are often not provided in the liquid forms required for young youngsters. Management of liquid forms may be difficult for sufferers and households as they often have to be compounded by native pharmacies and may have a brief shelf life. Managing utilization of} liquid forms may also be difficult for transplant centers dosing choices must usually be made in the absence of absorption and pharmacokinetic information for infants and youngsters. Antimicrobial Regimen Most sufferers receive intravenous antibiotics before and after lung transplantation primarily based on the most likely potential infecting organisms. Oral nystatin is begun in the early posttransplant period to scale back the probability of candidal illness. Immediate Posttransplant Phase Since virtually all pediatric lung transplant procedures are carried out with cardiopulmonary bypass, postoperative bleeding, particularly in the pleural area or at the web site of the vascular anastomoses, is a common concern. Dehiscence at either the vascular or bronchial anastomoses could require immediate surgical attention and an early return to the working room. Most transplant centers perform flexible bronchoscopy within 24 to forty eight hours of transplantation to obtain cultures from the decrease airways and to assess the integrity of the airway anastomosis. Fortunately, dehiscence of the airway anastomosis has turn into uncommon since the that} development of techniques to cowl the anastomosis with vascularized tissue. Mechanisms invoked to explain the development of anastomotic narrowing include donor airway ischemia, impaired airway therapeutic, and barotrauma if prolonged air flow is needed after transplantation. A number of mechanisms have been proposed to explain this discrepancy, including the richness of immune effector cells resident in the pulmonary vasculature and lymphatic system; the ongoing daily exposure of the vast epithelial floor of the lung allograft to potential environmental irritants, toxins, and pathogens; and reality that|the truth that} the lungs are exposed to the entire cardiac output. Patients with optimistic cross-matches are often treated with plasmapheresis to forestall hyperacute rejection. Treatment is supportive, with careful fluid administration and ventilatory support;forty eight extracorporeal membrane circulatory support has additionally been used in chosen circumstances. Acute rejection can happen as early as 1 week after transplantation or lengthy as|so long as} 2 to three years later. Most commonly, episodes of acute rejection happen 2 to 12 weeks after transplantation.
References:
- https://www.medrxiv.org/content/10.1101/2020.06.30.20142570v1.full.pdf
- https://internadomedicina.files.wordpress.com/2014/10/pocket-medicine_-the-massachusetts-general-hospital-handbook-of-internal-medicine.pdf
- https://assets.system.tamus.edu/files/benefits/pdf/GuideBooklet.pdf