.png)
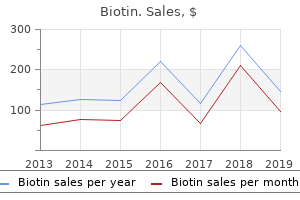
Effective biotin 5000 mcg
Low-grade fever, malaise, anorexia, and nausea every happen in a minority of sufferers. In a typical case of cat-scratch illness, lymph nodes stay enlarged for at least of|no less than} 2 to 4 months. Infrequently, inoculation of the attention leads to a granulomatous lesion of the conjunctiva and in preauricular adenopathy, a situation generally known as|often known as} the oculoglandular syndrome of Parinaud (affecting 4 to 6% of cat-scratch illness patients). Severe or systemic, non-neurologic manifestations are reported in 2% of cat-scratch illness sufferers. These embody persistent fever, weight loss, splenomegaly, diffuse papular rash, erythema nodosum, pleuritis, splenic abscess, central lymphadenopathy, osteolytic lesions, hepatitis, and thrombocytopenic purpura. An additional 2% of cat-scratch illness sufferers develop neurologic complications. Encephalopathy or encephalitis are most common and are manifest by seizures and confusion; different presentations embody radiculitis, meningitis, cranial neuritis, neuroretinitis, and cerebral arteritis. The prognosis of both bacillary angiomatosis and cat-scratch illness rests on tissue examination and serologic exams in a suitable medical setting. Histology typical of bacillary angiomatosis in hematoxylin and eosin-stained tissue is suggestive of the prognosis. Commercial laboratories, nicely as|in addition to} the Centers for Disease Control and Prevention, offer an immunofluorescent or enzyme-linked immunosorbent assay for serum IgG antibodies directed against B. Treat sufferers with bacillary angiomatosis-peliosis for at least of|no less than} 3 to 4 months, sufferers with bacteremia for two to 4 weeks, and sufferers with Bartonella endocarditis for at least of|no less than} 6 weeks. Bartonella species are slow-growing and fastidious, however they can be cultivated on blood-enriched media or within the presence of endothelial cells (see earlier). Formation of colonies on an agar floor instantly from an infected medical specimen could require greater than 21 days of incubation and subculturing on freshly prepared media. Acridine orange staining procedures and lysis centrifugation tradition methods improve the detection and restoration, respectively, of Bartonella species from blood specimens. The serologic cross-reactivity of Chlamydia and Bartonella species could present a diagnostic drawback because of|as a result of} both groups of microorganisms must be thought-about in instances of culture-negative endocarditis. The differential prognosis of trench fever includes epidemic (louse-borne) typhus, which happens beneath related demographic circumstances and shares the identical vector (P. Local illness endemicity or historical past of physique louse infestation ought to increase the medical suspicion of trench fever. Bacilli may be be} seen within pink blood cells as single organisms or in pairs or clusters. Cat-scratch illness is identified most often by examination of Warthin-Starry silver-stained tissue or by utilizing serologic methods. The differential prognosis for localized cat-scratch illness could embody pyogenic lymphadenitis, mycobacterial an infection, tularemia, brucellosis, lymphogranuloma venereum, syphilis, fungal illness, toxoplasmosis, and Epstein-Barr virus or cytomegalovirus an infection. There are few knowledge from prospective randomized studies from which to select an antimicrobial regimen for Bartonella-associated illness. Retrospective or empirical medical observations offer the primary foundation for the suggested approaches in Table 357-2. All forms of Bartonella-associated vasculoproliferative illness warrant antimicrobial treatment. In specific, there are well-documented instances of medical failure with beta-lactam brokers. Based on empirical observations, the treatment of alternative for bacillary angiomatosis-peliosis is either erythromycin, 500 mg every 6 hours, or doxycycline, a hundred mg every 12 hours. Because illness relapse is otherwise so widespread in these immunocompromised hosts, sufferers should be handled for at least of|no less than} 3 months. Bartonella bacteremia also warrants antimicrobial treatment, despite the fact fact} that|even though|although} some immunocompetent hosts with B. The same medicine and doses listed earlier for treatment of bacillary angiomatosis-peliosis are beneficial for main bacteremias. Treatment should be administered for at least of|no less than} 6 weeks and for two to 4 weeks in sufferers with and with out endocarditis, respectively. Close monitoring of hemodynamics is important because of|as a result of} traditionally the vast majority of} endocarditis sufferers have in the end required valve restore or substitute, maybe related to delay in prognosis in lots of} instances. Patients with trench fever often reply quickly to antibiotic remedy with resolution of fever and different symptoms within 1 to 2 days. In sufferers with Oroya fever, medical observations suggest that penicillin, chloramphenicol, tetracycline, and streptomycin are efficient. Chloramphenicol at a dose of 2 to 4 g/day for 7 or more days is the remedy of alternative due to the frequent affiliation of Salmonella an infection in endemic regions. After the establishment of remedy, fever typically disappears within 2 to 3 days, although blood smears could stay constructive for a while. Antibiotic remedy should be reserved for immunocompromised people or these with evidence of extreme or systemic illness. One published randomized placebo-controlled research suggests that a 5-day course of azithromycin speeds resolution of cat-scratch lymphadenopathy. First published prospective randomized research of treatment for cat-scratch illness. Describes the primary medical software of a molecular method for figuring out previously uncharacterized fastidious or uncultivated microbial pathogens instantly from infected host tissue. The results of this research suggested an in depth relationship between the agent(s) of bacillary angiomatosis and the Rochalimaea/Bartonella genus. These sudden findings occurred after the establishment of a more sensitive blood tradition protocol at a significant public hospital in Seattle. Characteristic features embody a typically prolonged latency period between preliminary an infection and overt illness, distinguished pulmonary illness (although different organs may be involved), and a granulomatous response associated with intense tissue irritation and injury. However, given the singular epidemiologic, medical, public well being, and therapeutic concerns associated with M. Disease caused by different organisms of this genus should be referred to as "mycobacteriosis M. Mycobacterial cell walls contain excessive concentrations of lipids or waxes, making them proof against commonplace staining methods. The ability to invade and unfold all through the human physique has largely to do with the capability of tubercle bacilli to survive and proliferate within mononuclear phagocytes. Infection is unfold virtually completely by aerosolization of contaminated respiratory secretions. Patients with cavitary lung illness are significantly infectious because of|as a result of} their sputum often incorporates 1 to a hundred million bacilli/mL, they usually cough incessantly. However, the intact pores and skin and respiratory mucous membranes of regular exposed people are fairly proof against invasion. Once deposited in alveoli, bacilli are adapted to promote uptake by alveolar macrophages, which-depending on innate, genetically determined properties-may be kind of permissive to bacillary proliferation (see later). To attain the alveoli, which lie on the finish of a ramifying system of progressively smaller airways, the bacilli must be suspended in very fine units that behave as the air itself and not as particles with important mass. These units are the dehydrated residuals of the tinier particles generated by high-velocity exhalational maneuvers; cough-inducing procedures such as bronchoscopy or endotracheal intubation are significantly probably to|prone to} generate infectious aerosols. These droplet nuclei are calculated to be 1 to 5 mum in diameter, could stay suspended in room air lots of} hours, and when inhaled can traverse the airways to attain the alveoli. Although sufferers with cavitary tuberculosis expectorate huge numbers of bacilli, the chance of generating infectious particles is comparatively low. Hence case of pulmonary tuberculosis is of a low order of infectiousness compared with an airborne illness such as measles. The preponderance of transmission happens as described earlier however different mechanisms of transmission have been recognized. Aerosols generated by debridement or by dressing adjustments of pores and skin or delicate tissue abscesses M. Also, tissue agitation associated with autopsies and direct inoculation into delicate tissues from contaminated instruments or bone fragments also have been reported. When an immunologically naive alveolar macrophage engulfs a tubercle bacillus, it initially supplies a nurturing environment within its phagosome by which the bacilli survive and replicate. However, the infected macrophage releases substances that entice T lymphocytes; the macrophages then present antigens from the phagocytized bacilli to these lymphocytes, initiating a series of committed immune effector cells.
Buy biotin 5000mcg
It is thus prudent to repeat the genetic check on a separate peripheral blood sample, preferably in a couple of laboratory. It is cheap to exclude an individual with two or more adverse genetic check results from additional screening efforts. Screening additionally be|can be} beneficial for apparently sporadic tumors outcome of|as a result of} household history may be unreliable. Interpretation must be made based on the specific parameters of the process used. Molecular genetic methods enable gene provider status to be assigned in a affected person at risk and with a well-documented pedigree. However, confounding components such as mistaken diagnoses and non-paternity can complicate genetic evaluation. Accepted surgical procedures embody unilateral or bilateral adrenalectomy for diseased glands by anterior, posterior, or laparoscopic approaches or unilateral cortical sparing adrenalectomy in an try to protect adrenal cortical operate. Bilateral adrenalectomy at an early age is mandatory in the rare kindred with malignant pheochromocytoma. Hyperparathyroidism may be be} managed by both subtotal parathyroidectomy or total parathyroidectomy with transplantation of parathyroid tissue to the non-dominant forearm. Thyroidectomy should be based mostly on genetic testing and performed early in childhood. An various strategy is to initiate calcium or pentagastrin testing on gene carriers at age 5 years with removing of the thyroid gland on the time of a positive check, an strategy which has been the mainstay of diagnosis and administration for the past 25 years. A vexing drawback for clinicians is the persistence of calcitonin elevations following main surgical administration. The main question is whether or not} reoperation to take away all identifiable lymph nodes in the neck (compartment-oriented dissection) has value. A latest body of expertise has accrued concerning reoperative strategy in patients with persistent disease. In the number of these patients it is important to|it could be very important|you will need to} carry out a careful seek for distant metastatic disease and to exclude hepatic, bone, and pulmonary metastasis by applicable imaging studies. In patients with no evidence of distant metastatic disease, reoperative compartment-oriented lymphadenectomy may be be} applicable. A detailed exposition of multiple of} endocrine neoplasia and the regulation of calcitonin-gene products. Genotype/phenotype correlation of medical syndromes with particular mutations of the c-ret proto-oncogene. Renal osteodystrophy encompasses extensive variety|all kinds} of derangements in mineral and bone metabolism. With progressive lack of excretory kidney operate, abnormalities in divalent ions and secondary hyperparathyroidism usually develop early. However, the early stages of renal failure are marked by some indicators of end-organ resistance to vitamin D, such as a mild lower in intestinal calcium absorption and an altered calciuric response to oral supplementation of calcitriol. In experimental studies on rats, alterations in the vitamin D receptor heterodimer partner (retinoid X receptor) have been noticed; however, this mechanism has not been proved in people. With more advanced nephron loss, the phosphate load of the remaining functioning nephrons progressively will increase. This elevated load results in inhibition of C1-alpha-hydroxylase, the enzyme liable for the conversion of 25-hydroxyvitamin D to its lively metabolite 1,25-dihydroxyvitamin D (calcitriol). Calcitriol deficiency in flip additional decreases intestinal calcium absorption and thus results in hypocalcemia. Calcitriol deficiency in advanced renal failure is associated with a decreased variety of vitamin D receptors, in particular, receptors in parathyroid glands. Calcium exerts its results on parathyroid gland cells through a lately isolated G protein-coupled calcium-sensing receptor situated on the cell membrane. The decreased variety of calcium-sensing receptors with low circulating calcitriol could, a minimum of|no less than} partly, explain the relative insensitivity of parathyroid gland cells to calcium in patients present process dialysis (higher set point). When the glomerular filtration fee reaches ranges of less than 25% of normal, the serum phosphorus content material rises. At this level of decreased renal operate, the flexibility of the remaining nephrons to improve phosphate excretion is exhausted. Increased serum phosphorus ranges additional lower serum calcium through physicochemical binding and suppress C1-alpha-hydroxylase activity, additional lowering of the circulating ranges of calcitriol. Monoclonal cell growth may also develop and result in the formation of tumor-like nodules that have less or no vitamin D and calcium-sensing receptors and that promote parathyroid gland resistance to calcitriol and calcium. Accumulation of aluminum in bone and different organs such as the parathyroid glands could happen in patients present process dialysis or earlier than the initiation of dialysis. In addition, aluminum inhibits renal and intestinal C1-alpha-hydroxylase activity and should thus additional contribute to decreased ranges of calcitriol. Possible sources of aluminum embody excessive concentrations in the water used for dialysis, prescription of aluminum-containing phosphate binders, and aluminum in ingesting water, infant formulation, and different liquids or solid food. Metabolic acidosis has been proven to stimulate bone resorption and suppress bone formation, thereby leading to adverse bone steadiness. Disturbed osteoblastic activity results in a disorderly manufacturing of collagen, which is deposited not only toward the trabecular surface but additionally in the marrow cavity, thereby inflicting peritrabecular and marrow fibrosis. Osteoid seams not exhibit their traditional birefringence underneath polarized light; instead, a disorderly arrangement of woven osteoid and woven bone with a typical crisscross sample underneath polarized light is seen. The mineral apposition fee and variety of actively mineralizing websites are elevated, as documented underneath fluorescent light after the administration of time-spaced tetracycline markers. Low-turnover uremic osteodystrophy is the other finish of the spectrum of renal osteodystrophy. The majority of trabecular bone is covered by lining cells, with few osteoclasts and osteoblasts. Two histologic subgroups may be identified in sort of|this type of|this kind of} renal osteodystrophy, depending on the sequence of events leading to a decline in the number and/or Figure 266-1 Predominant hyperparathyroid bone disease with a excessive fraction of the trabecular surface coated by osteoid seams, many osteoblasts and osteoclasts, and marrow fibrosis; undecalcified 3-mum-thick section of iliac bone (brightfield light microscopy; modified Masson-Goldner stain; authentic magnification, Ч125). Low-turnover osteomalacia is characterised by an accumulation of unmineralized matrix by which a diminution in mineralization precedes or is more pronounced than the inhibition of collagen deposition. The elevated lamellar osteoid quantity of} the presence of wide osteoid seams that cover a large portion of the trabecular surface (Fig. The occasional presence of woven bone buried within the trabeculae signifies past excessive bone turnover. With adynamic uremic bone disease, the reduction in mineralization is coupled with a concomitant and parallel lower in bone formation. Adynamic uremic bone disease is characterised by few osteoid seams and few bone cells (Fig. Mixed uremic osteodystrophy is brought on primarily by hyperparathyroidism and faulty mineralization with or with out elevated bone formation. Because Figure 266-3 Adynamic bone disease with no accumulation of osteoid, and absence of osteoblasts and osteoclasts; undecalcified 3-mum-thick section of iliac bone (brightfield light microscopy; modified Masson-Goldner stain; authentic magnification, Ч125). Few osteoblasts, osteoclasts, and gentle peritrabecular fibrosis; and an undecalcified, 3-mum-thick section of human iliac bone (brightfield light microscopy; modified Masson-Goldner stain; authentic magnification, Ч125). Whereas lively mineralizing surfaces improve in woven bone with a better mineralization fee and diffuse labeling, mineralization surfaces may be be} decreased in lamellar bone with a decreased mineral apposition fee. Aluminum accumulates in bone on the mineralization entrance, on the cement strains, or diffusely. The extent of stainable aluminum on the mineralization entrance correlates finest with histologic abnormalities in mineralization. In patients in whom an elevated aluminum burden develops, bone mineralization and bone turnover progressively lower. With progressive lack of renal operate, cancellous bone quantity is elevated together with a lack of cortical bone. Patients present process continual dialysis might have a loss or acquire in bone quantity depending on bone steadiness. In the case of adverse bone steadiness, bone loss occurs in cortical and cancellous bone and is more rapid when bone turnover is excessive. When the bone steadiness is positive, osteosclerosis may be be} noticed when osteoblasts are lively in depositing new bone, thus superseding bone resorption. When bone turnover is low, however, positive bone steadiness results in hypercalcemia and possibly extraosseous calcification. Clinical manifestations are preceded, however, by an abnormal biochemical profile that should alert the doctor and immediate steps to stop more extreme problems.
Cheap 5000 mcg biotin
Reconstitution with human albumin enhances the steadiness of hematin and prevents these facet effects}. Carbohydrate loading could suffice for mild assaults and could be given orally as sucrose, glucose polymers, or carbohydrate-rich foods. If oral intake is poorly tolerated or is contraindicated by distention and ileus, intravenous administration of glucose (at least 300 g daily) is normally indicated. A central venous line facilitates extra full parenteral nutrition help and avoids extra fluid volumes. Parenteral nutrition help may be be} indicated in some sufferers who require heme remedy. Occasionally, persistent pain and other signs develop, but they may improve in lengthy term|the long run}. Chronic signs and depression enhance the chance of suicide and thus require careful administration. Diet regimens for weight problems should present for gradual weight loss in periods of medical remission of porphyria. Most sufferers have unrelated parents and have inherited a unique mutation from every father or mother. The severity of the illness is variable and relates to the degree of enzyme deficiency attributable to the particular mutations. There is appreciable accumulation of hydroxymethylbilane (the substrate of the deficient enzyme), which is transformed non-enzymatically to uroporphyrinogen I. Uroporphyrin I and other porphyrins accumulate in bone marrow erythroid cells may be} actively synthesizing hemoglobin and lead to intramedullary and intravascular hemolysis. Even in the most severe cases some residual cosynthase activity is noted, and heme manufacturing is definitely elevated in response to hemolysis. Sunlight, other sources of ultraviolet mild, and minor trauma to friable pores and skin are other determinants of medical expression. In most cases, reddish urine and severe cutaneous photosensitivity are noted in early infancy. Lesions on sun-exposed pores and skin embody bullae and vesicles, that are vulnerable to rupture and become infected, hypopigmented or hyperpigmented areas, and hypertrichosis. Porphyrins are deposited within the teeth (producing a reddish brown shade termed "erythrodontia") and in bone. No neurologic manifestations are known, but hemolysis and splenomegaly are nearly all the time present. Porphyrins in urine are primarily uroporphyrin and coproporphyrin, and in feces porphyrins mostly consist of coproporphyrin. Protection of the pores and skin from sunlight and minor trauma and immediate remedy of secondary bacterial infections help forestall scarring and mutilation. Blood transfusions adequate to suppress erythropoiesis and bone marrow transplantation may be be} the best present therapies but entail important risks. It is commonest in men but has become extra frequent in women in affiliation with alcohol and estrogen use. The amount of hepatic uroporphyrinogen decarboxylase protein, as measured immunochemically, is regular, thus suggesting that an acquired process has inactivated the enzyme. With remedy and remission of the illness, enzyme activity progressively increases to regular. This deficiency is an autosomal dominant trait and may end up} from quantity of|numerous|a selection of} completely different mutations of the uroporphyrinogen decarboxylase gene. Most notably, an extensive outbreak of porphyria occurred in jap Turkey in 1955-1958 after seed wheat containing the fungicide hexachlorobenzene was used for meals. This accumulation precedes the appearance of extra porphyrins in plasma and urine. The enzyme-catalyzed decarboxylation of uroporphyrinogen happens in 4 sequential steps. In addition, pentacarboxyl porphyrinogen could be metabolized by coproporphyrinogen oxidase to a series of tetracarboxyl porphyrins termed isocoproporphyrins. These substances are excreted primarily in bile and feces and are diagnostic of uroporphyrinogen decarboxylase deficiency. Multiple components could contribute to the inactivation of hepatic uroporphyrinogen decarboxylase. Iron could catalyze the formation of free radicals that harm the enzyme protein or oxidize its porphyrinogen substrates to porphyrins. The illness could develop in men handled with estrogens for prostate most cancers and in women taking oral contraceptives or alternative estrogens. Vesicles and bullae develop on the face, dorsum of the arms and ft, forearms, and legs. Sun-exposed pores and skin becomes friable, and minor trauma could precede the formation of bullae or cause denudation of the pores and skin. Hypertrichosis and hyperpigmentation sometimes occur even within the absence of vesicles. Thickening, scarring, and calcification of affected pores and skin ("pseudoscleroderma") may be be} hanging. Cirrhosis and hepatocellular carcinomas are commonest in older sufferers and at autopsy. The illness can also be|can be} associated with systemic lupus erythematosus and acquired immune deficiency syndrome. Very hardly ever, hepatic tumors themselves contain and presumably produce extra porphyrins. It is important to differentiate these situations by laboratory testing earlier than starting remedy. A course of phlebotomies is the popular remedy and nearly all the time produces a remission. Patients are also advised to discontinue the usage of} alcohol, estrogens, iron supplements, or other contributing components. A course of low-dose chloroquine, a hundred twenty five mg twice weekly, or hydroxychloroquine, 100 mg twice weekly for quantity of} months, is normally efficient when repeated phlebotomies are contraindicated. One hypothesis is that chloroquine types complexes with porphyrins and promotes their removal from the liver. The affected person was a 37-year-old woman with a history of extra alcohol intake and persistent hepatitis C. Further iron depletion is of no additional profit and will cause anemia and associated signs. Plasma porphyrins become regular and the appearance of recent pores and skin lesions ceases inside quantity of} months. Mutations within the uroporphyrinogen decarboxylase gene are discovered on this illness and are associated with some residual enzyme activity. Increased erythrocyte protoporphyrin most likely displays an earlier accumulation of uroporphyrinogen in erythroblasts, which after completion of hemoglobin synthesis is metabolized to protoporphyrin. A related rationalization can account for elevated erythrocyte protoporphyrin in other homozygous forms of porphyria. A particular mutation of the protoporphyrinogen oxidase gene is frequent in South Africa. Furthermore, coproporphyrinogen is extra readily lost from the liver than are other porphyrinogens, and its loss increases additional when heme synthesis is stimulated. Impaired biliary excretion by concurrent liver ailments or medication similar to contraceptive steroids may cause porphyrin retention and worsen photosensitivity. Cholestyramine could decrease the photosensitivity occurring with liver dysfunction. The pattern of inheritance often appears to be autosomal dominant, but some obligate carriers have little or no enhance in purple cell protoporphyrin. Co-inheritance of a standard ferrochelatase allele that expresses low levels of enzyme could clarify an incompletely dominant trait, a minimum of|no much less than} in some households. Zinc protoporphyrin dissociates much less readily from hemoglobin binding websites and persists within the purple cell it circulates.
| Comparative prices of Biotin | ||
| # | Retailer | Average price |
| 1 | Meijer | 682 |
| 2 | Ruddick Corp. | 830 |
| 3 | Tractor Supply Co. | 968 |
| 4 | A&P | 974 |
| 5 | QVC | 171 |
| 6 | Wendy's / Arby's Restaurants | 126 |
Order biotin 5000mcg
Insulin acts on responsive tissues by first passing by way of the vascular compartment and, on reaching its goal, binding to its particular receptor. The insulin receptor is a heterodimer with two alpha- and beta-chains fashioned by disulfide bridges. The alpha-subunit resides on the extracellular surface and is the positioning of insulin binding. The beta-subunit spans the membrane and can be phosphorylated on serine, threonine, and tyrosine residues on the cytoplasmic face. The intrinsic protein tyrosine kinase exercise of the beta-subunit is crucial for insulin receptor operate. Rapid receptor autophosphorylation and tyrosine phosphorylation of cellular substrates. A number of different hormones termed counterregulatory hormones (glucagon, growth hormone, catecholamines, and cortisol) oppose the metabolic actions of insulin. Among these, glucagon and to a lesser extent growth hormone have important roles in improvement of the diabetic syndrome. Glucagon is secreted by pancreatic alpha cells in response to hypoglycemia, amino acids, and activation of the autonomic nervous system. Its major effect is on the liver, the place it stimulates glycogenolysis, gluconeogenesis, and ketogenesis through cyclic adenosine monophosphate-dependent mechanisms. It is generally inhibited by hyperglycemia but is totally or comparatively elevated in both type 1 and kind 2 diabetes regardless of the presence of hyperglycemia. Growth hormone secretion by the anterior 1266 pituitary can also be|can be} inappropriately elevated in type 1 diabetes consequently, minimal of|no less than} in part, of an attempt to overcome a defect in insulin-like growth factor type 1 era caused by insulin deficiency. The major metabolic actions of growth hormone are on peripheral tissues, the place it acts to promote lipolysis and inhibit glucose consumption. In type 1 diabetic patients with decreased portal vein insulin levels, growth hormone can also be|can be} capable of stimulating hepatic glucose production. After an overnight quick, low basal levels of insulin diminish glucose uptake in peripheral insulin-sensitive tissues (muscle and fat). Most glucose uptake occurs in non-insulin-sensitive tissues, primarily the brain, which because of its inability to use free fatty acids is critically dependent on glucose for oxidative metabolism. Maintenance of stable blood glucose levels is achieved by release of glucose by the liver and to a small extent by the kidney at charges (7 to 10 g/hour) matching these of consuming tissues. The hepatic processes concerned include glycogenolysis and gluconeogenesis, with gluconeogenesis contributing about half and glycogenolysis contributing the remainder. Both play a big position, and both depend upon the stability of insulin and glucagon in the portal circulation. Glucagon additionally stimulates gluconeogenesis, whereas the lowered insulin promotes peripheral mobilization of glucose precursors (amino acids, lactate, pyruvate, glycerol) and fuels (free fatty acids) for gluconeogenesis. Ingestion of a giant glucose load triggers a number of} homeostatic mechanisms that reduce glucose excursions and restore normoglycemia. These mechanisms embody (1) suppression of endogenous glucose production, (2) stimulation of hepatic glucose uptake, and (3) acceleration of glucose uptake by peripheral tissues, predominantly muscle. In addition, about 30% of the ingested glucose is deposited in the liver outcome of|because of|on account of} the mixed effects of hyperglycemia and hyperinsulinemia in the portal circulation. Consequently, a considerable amount of glucose is retained in the liver as glycogen. Insulin-stimulated glucose transport across the plasmalemma of both adipose and muscle tissue is attributable to the recruitment of glucose-transporting proteins. In muscle, glucose used for glycogen synthesis or undergo oxidative or non-oxidative metabolism. In adipose tissue, glucose is used for the formation of alpha-glycerophosphate, which is critical for the esterification of free fatty acids to form triglycerides. Insulin promotes glycogen formation by stimulating glycogen synthase and glucose oxidation by activating pyruvate dehydrogenase and reducing lipolysis (free fatty acids compete with glucose for oxidative metabolism). If the quantity of carbohydrate consumed and the resultant insulin response are small, glucose homeostasis is maintained largely by a discount in hepatic glucose production quite than by a rise in glucose uptake end result of|as a result of} glucose production is rather more delicate than glucose uptake to the effects of small changes in insulin secretion. The rise in insulin that accompanies the consumption of mixed meals additionally facilitates protein and fats storage. Because muscle is in unfavorable nitrogen stability in the fasting state, repletion of muscle nitrogen depends on by} a net uptake of amino acids in response to protein feeding. In muscle, insulin acts to promote positive nitrogen stability by inhibiting the breakdown of protein and to a lesser extent by stimulating the synthesis of new protein. Similarly, in adipose tissue the motion of insulin accelerates triglyceride incorporation by stimulating lipoprotein lipase while simultaneously decreasing the hormone-sensitive lipase that catalyzes the hydrolysis of stored triglycerides. In type 1 diabetes, portal insulin deficiency is invariably present and thus hepatic glucose production is constantly elevated. In addition, insulin deficiency leads to hypersecretion of glucagon and growth hormone, which additional intensify glucose overproduction. Because basal glucose uptake occurs largely in non-insulin-sensitive tissues, total-body glucose uptake tends to be elevated because of the mass motion of hyperglycemia. This tendency underscores the essential position that the liver performs in determining the fasting glucose stage in diabetes. The increase in glucose production in both forms of diabetes of} an acceleration of gluconeogenesis. Loss of the restraining effect of insulin on the alpha cell leads to a relative increase in portal glucagon and, in turn, a rise in the uptake and conversion of glycogenic substrates to glucose within the liver. In the intense situation of whole insulin lack, extreme release of a variety of|quite a lot of|a wide selection of} counterregulatory hormones causes gluconeogenesis to increase additional and blocks compensatory increases in glucose disposal. Fasting levels of free fatty acids are additionally incessantly elevated because of accelerated mobilization of fats shops. Endogenous insulin secretion in type 2 diabetes supplies sufficient levels of insulin in portal blood to suppress the conversion of free fatty acids to ketones in the liver. In type 1 diabetes, nevertheless, mobilized free fatty acids are extra readily converted to ketone bodies. The mixed effects of insulin deficiency and the presence of glucagon suppress fats synthesis in the liver. In addition, hypoinsulinemia, by reducing ketone turnover, enhances the magnitude of the ketosis for any given stage of ketone production. During diabetic ketoacidosis, ketone levels are additional elevated because of the concomitant release of counterregulatory hormones. The rise in glucagon accelerates Figure 242-2 the effects of severe insulin deficiency on physique fuel metabolism. Lack of insulin leads to mobilization of substrates for gluconeogenesis and ketogenesis from muscle and adipose tissue, accelerated production of glucose and ketones by the liver, and impaired elimination of endogenously produced and exogenous fuels by insulin-responsive tissues. The increase in substrate delivery might turn into so pronounced that it saturates the oxidative pathway and leads to a fatty liver and severe hypertriglyceridemia. Diabetes is characterised by marked postprandial hyperglycemia after carbohydrate ingestion. In type 2 diabetes, the mixed effects of delayed insulin secretion and hepatic insulin resistance impair the suppression of hepatic glucose production and the flexibility of the liver to retailer glucose as glycogen. Hyperglycemia ensues, even though fact} that|although} insulin levels might ultimately rise to levels above these seen in non-diabetic individuals (insulin secretion stays deficient relative to the prevailing glucose level), end result of|as a result of} insulin resistance reduces the capability of muscle to take away the excess glucose released from the liver and retailer it in the myocyte as glycogen. The regular increase in glucose-6-phosphate in muscle after insulin is markedly attenuated in diabetes, which implies that the block in glycogen synthesis precedes glucose-6-phosphate formation and is mediated at the stage of either glucose transport or its conversion to glucose-6-phosphate (by hexokinase). These defects are extra pronounced in patients with severe hyperglycemia, in whom insulin secretion is additional decreased. Type 1 patients show essentially the most marked and extended elevations in blood glucose after ingestion of carbohydrate. Consequently, the liver fails to cut back its glucose production or to appropriately take up glucose and retailer it as glycogen. In addition, glucose uptake by peripheral tissues is impaired by the shortage of insulin and the development of insulin resistance secondary to persistent insulin deprivation and the poisonous effects of persistent hyperglycemia. An insulin-deficient affected person might exhibit defects in the disposal of ingested protein and fats as properly. In the absence of an increase in insulin, meal ingestion might trigger hyperaminoacidemia because of failure to stimulate the web uptake of amino acids in muscle and may trigger hypertriglyceridemia because of decreased exercise of lipoprotein lipase.
5000 mcg biotin
Not a lot is thought about its bodily findings early within the disease; findings after 3 to 5 days of sickness are generally normal except for fever and possibly tachypnea. The sickness lasts about 3 to 5 days, though some patients could have persistent fatigue or non-focal neurologic complaints for weeks to months afterward. Interstitial infiltrates are uncommon, though they might occur early the center of|in the midst of} disease and then progress to consolidating infiltrates. The infiltrates could also be} unilateral or bilateral and might unfold brief time} to involve the whole lung. Pleural effusion, often small in volume, happens generally and could be the sole abnormal radiographic finding in early disease. These abnormal findings embody proteinuria, pyuria, hematuria, leukocytosis, leukopenia, and thrombocytopenia. Hyponatremia, hypophosphatemia, hyperbilirubinemia, and elevated serum alanine transminase, serum aspartate transaminase, and alkaline phosphatase concentrations can also be discovered. Cerebrospinal fluid is often normal, though uncommon patients could have 25 to one hundred white blood cells per microliter of cerebrospinal fluid. The most sensitive and particular test is tradition of respiratory tract secretions, similar to sputum. Sputum tradition for Legionella should be performed on each patient suspected of having this disease. Serologic testing is extra helpful to epidemiologists than to clinicians because of cross-reactions with antibodies to unrelated organisms. The diagnosis of Pontiac fever is based on demonstration of legionellae in water to which the patient was exposed, vital increases in antibody to the isolated Legionella species, and a medical course suitable with this diagnosis. Mycoplasmal pneumonia is mostly a lot much less extreme and causes vital respiratory system complaints. Erythromycin (Table 323-4) is considered the drug of selection for this disease on the basis of retrospective research, which present that the case fatality rate is lowered about two-fold by immediate administration of erythromycin. Intravenous drug therapy should be given till medical improvement is seen, which often happens in 2 to 4 days. Culture is the most sensitive diagnostic technique, but its absolute sensitivity is unknown; reasonable estimates are 80 to 90%. Quinolone antimicrobials (especially levofloxacin, trovafloxacin, and sparfloxacin) and the newer macrolide antimicrobials (clarithromycin and especially azithromycin) are more practical than erythromycin or doxycycline in experimental laboratory research. The availability of newer and extra energetic medicine makes such combination therapy much less fascinating. The signs clearing most rapidly are rigors, psychological confusion, myalgia, anorexia, fatigue, and abdominal complaints. Fever could persist for per week after the initiation of therapy but starts a downward pattern inside a couple of of} days. Despite this medical proof of improvement, different findings could falsely suggest disease development, similar to proof of increased pulmonary consolidation on bodily examination and on radiography. Patients with respiratory failure have a relatively poor prognosis and have a tendency to have a a lot slower response to therapy. Streptococci colonize the pores and skin and mucous membranes of animals, produce catalase, and could also be} aerobic, anaerobic, or facultative. On blood agar plates, streptococci could cause full (beta), incomplete (alpha) or no hemolysis (gamma). The exhaustive work of Rebecca Lancefield has allowed hemolytic streptococci to be categorised into types A via O primarily based on acid-extractable carbohydrate antigens of cell wall materials. The availability of fast latex agglutination kits offers even small medical laboratories with the means to establish streptococci in accordance with Lancefield group. Modern schemes of classification of hemolytic and non-hemolytic streptococci use advanced biochemical and genetic techniques. All group A streptococcal infections have the best incidence in youngsters younger than 10 years. The asymptomatic prevalence is also be|can be} higher (15 to 20%) in youngsters than in adults (<5%). Impetigo is commonest in youngsters aged 2 to 5 and will occur year-round in tropical areas but largely in the summer in temperate climates. Briefly, scarlet fever had disappeared from that isolated island group for quantity of} a long time till it was reintroduced by a customer with unsuspected scarlet fever. An epidemic of scarlet fever ensued, with vital assault charges in all age teams, thus suggesting that different components, similar to the shortage of protective antibody in opposition to scarlatina toxin or the introduction of a new new} pressure, somewhat than age predisposed those people to medical sickness. In contrast to pharyngitis, impetigo, and scarlet fever, bacteremia has had the best age-specific assault rate within the elderly and in neonates. However, between 1986 and 1988, the prevalence of bacteremia increased 800 to 1000% in adolescents and adults in western international locations. Pharyngeal and cutaneous acquisition is by person-to-person unfold through aerosolized microdroplets or by direct contact, respectively. Epidemics of pharyngitis and scarlet fever have also occurred after the consumption of contaminated, non-pasteurized milk or meals. Epidemics of impetigo have been reported, particularly in tropical areas, in day care centers, and among underprivileged youngsters. Group A streptococcal infections in hospitalized patients occur throughout childbirth (puerperal sepsis), times of warfare (epidemic gangrene), and surgical convalescence (surgical wound infection, surgical scarlet fever) or as a result of|because of|on account of} burns (burn wound sepsis). Thus in most medical streptococcal infections, the mode of transmission and portal of entry are simply ascertained. In contrast, among patients with streptococcal poisonous shock syndrome, the portal of entry is apparent in only 50% of cases. Adherence of cocci to the mucosal epithelium is necessary but not adequate to cause disease in all cases inasmuch as extended asymptomatic carriage is nicely documented. Complex interactions between host epithelium and streptococcal components similar to M protein, lipoteichoic acid, and fimbriae are essential for adherence. Fibronectin binding protein (protein F) also contributes to adherence end result of|as a end result of} protein F-deficient mutants are incapable of binding to epithelial cells. Within the tissues, streptococci could evade opsonophagocytosis by virtue of a hyaluronic acid capsule, a C5a peptidase that destroys or inactivates complement-derived chemoattractants and opsonins, or by immunoglobulin binding protein. In tissues, streptolysin O secreted in excessive focus destroys approaching phagocytes. A unique function of the pyrogenic exotoxins and a few M protein fragments is their ability to work together with sure Vbeta areas of the T-cell receptor within the absence of basic antigen processing by antigen-presenting cells (Fig. Luxuriant manufacturing of M protein can also impart a mucoid colony morphology, and this trait has been associated with M-18 strains. An operon promoter sequence is necessary thing} component in both the constitutive and dynamic regulation of hyaluronic acid synthesis in group A streptococci, and its exercise is increased throughout best progress situations and log-phase progress. The cell wall consists of a peptidoglycan backbone with integral lipoteichoic acid parts. Over 80 completely different M protein kinds of group A streptococci are presently described. Region A close to the N terminus is extremely variable, and antibodies to this region confer type-specific protection. Within the extra conserved B to D areas lies an space that binds one of the complement regulatory proteins (factor H), stearically inhibiting antibody binding and complement-derived opsonin deposition and effectively camouflaging the organism in opposition to humoral immune surveillance. Observations by Lancefield recommend that the amount of M protein produced decreases with passage on artificial media and conversely increases rapidly with passage via mice. The quantity of M protein produced by an infecting pressure progressively decreases throughout convalescence and through extended carriage. Cholesterol inhibits toxicity 1621 in isolated myocytes and hemolysis of red blood cells in vitro. Purification and characterization of this protein have been tough, and its only function in pathogenesis could also be} in direct or contact cytotoxicity. Dnases can also contribute to cytokine manufacturing, though their significance in pathogenesis has not been established. This extracellular enzyme hydrolyzes hyaluronic acid in deeper tissues, thereby facilitating the unfold of infection along fascial planes. The gene for pyrogenic exotoxin A (speA) is transmitted by bacteriophages, and stable manufacturing depends on by} lysogenic conversion in a fashion analogous to diphtheria toxin manufacturing by Corynebacterium diphtheriae. Patients with streptococcal pharyngitis have an abrupt onset of sore throat, submandibular adenopathy, fever, and chilliness but not often frank rigors. The uvula is edematous, tonsils are hypertrophied, and the pharynx is erythematous with exudate punctate or confluent. Depending on the infecting pressure, pharyngitis could progress to scarlet fever, bacteremia, suppurative head and neck infections, rheumatic fever, post-streptococcal glomerulonephritis, or streptococcal poisonous shock syndrome.
Trusted biotin 5000mcg
The differentiation of disseminated herpes zoster from chickenpox additionally be} difficult. Fluorescence microscopy is a rapid and accurate method of confirming the analysis from vesicular scrapings. Virus can often be isolated during the first 3 or four days after the onset of lesions. My preference is to acquire vesicular fluid in unheparinized capillary tubes and put the specimen instantly into human embryonic lung fibroblasts on the bedside. Specimens from throat, urine, or stool are of little value for isolation of virus. Polymerase chain response can be utilized to show the presence of virus in vesicular fluid and throat swabs. The laboratory director ought to be consulted regarding acceptable time of collection of specimens as well as|in addition to} interpretation of data. Fluorescence antibody testing utilizing fixed cells typically yields false-positive results. It was hoped that these would possibly differentiate varicella from herpes zoster in cases in which this was unclear. Major therapeutic aims are the prevention of superinfection and aid of pruritus. Bacterial superinfection can best be prevented by encouraging daily bathing with an antibacterial soap. Following this with a colloidal starch tub additionally additionally be} useful for relieving pruritus. Relief of systemic signs could require further medicine similar to acetaminophen, although this may enhance pruritus. Special care ought to be taken to be sure that over-the-counter drugs containing salicylates are avoided. Necrotizing fasciitis end result of} group A Streptococcus has been associated with the usage of} ibuprofen. Some patients, significantly those who are immunocompromised, could require antiviral remedy. Intravenous acyclovir has been proven to be efficient in immunocompromised kids with varicella. Studies on the usage of} oral acyclovir in the remedy of varicella have demonstrated some efficacy. Corticosteroids appear to be most deleterious when given during the incubation period. They have been used in the remedy of pneumonia after the eruption has occurred with none obvious deleterious effects. Live attenuated varicella vaccine is recommended for all kids aged 1 by way of 12 years and for sure adults. A single dose is recommended for kids and two doses a minimum of|no less than} 2 months aside are given to adults. Immunization of kid care or establishment employees, these traveling overseas, the military, and postpartum girls is extremely desirable. Immunization during being pregnant ought to be avoided but when it happens it ought to be reported by calling 1-800-986-8999. Some vaccinees have developed a rash after immunization and may unfold vaccine virus to contacts. Caution is suggested when immunizing those who could are available in} contact with pregnant girls or immunocompromised individuals. Increased immunization of health care employees and increased use of the vaccine in the general inhabitants can be anticipated to decrease the chance of nosocomial an infection. Some immunized workers could develop varicella and have the potential to infect others. Patients who develop varicella ought to have strict isolation precautions in a adverse stress room if potential. Screening for susceptibility with the latex agglutination test additionally be} useful in cohorting patients. Consideration ought to be given to administration of acyclovir orally from the seventh day after publicity for 7 days. Candidates are those who (1) are susceptible, (2) are at excessive threat of developing difficult varicella, and (3) have had a significant publicity to the disease. Reference to tips printed by the Academy of Pediatrics or Centers for Disease Control and Prevention additionally be} useful. A symposium on the epidemiology, price burden, and problems of varicella and on varicella vaccine. A useful guide to administration of patients uncovered to varicella, including control of nosocomial an infection. Mumps is an acute systemic viral an infection that occurs most commonly in kids, is often self-limited, and is clinically characterized by non-suppurative parotitis. Mumps virions are pleomorphic, roughly spherical, enveloped particles with an average diameter of 200 nm. Humans are the only pure hosts for mumps virus, although an infection may be induced experimentally in selection of|quite lots of|a big selection of} mammalian species. In unvaccinated urban populations, mumps is a disease of school-aged kids (5 to 9 years), and more than 90% may have mumps antibodies by age 15 years. Before the mumps vaccine was released in the United States in 1967, mumps was an endemic disease with a seasonal peak of exercise occurring between January and May. The largest number of cases reported in the United 1809 States was in 1941, when the incidence of mumps was 250 cases per 100,000 inhabitants. In 1968, when the mumps vaccine was first entering scientific use, the incidence of mumps was seventy six cases per 100,000 inhabitants. Between 1985 and 1987, the incidence of mumps in the United States increased fivefold to 5. More than one third of the cases reported between 1985 and 1989 occurred in adolescents and younger adults, reflecting the sluggish acceptance of common mumps vaccination during the Nineteen Seventies. Epidemiologic studies of mumps epidemics in excessive schools, colleges, and military models during the Eighties demonstrated that outbreaks had been due principally to failure to vaccinate. Renewed emphasis on vaccination resulted in a further decline in the annual incidence of mumps. More recent studies have attributed smaller mumps outbreaks in the Nineties to major vaccine failure and probably to waning vaccine-induced immunity. In 1996, the Centers for Disease Control and Prevention reported only 751 cases of mumps in the United States, the bottom annual complete ever recorded. Mumps is extremely contagious and may be transmitted experimentally by inoculation of virus onto the nasal or buccal mucosa, suggesting that the majority all} pure infections end result from droplet unfold of higher respiratory secretions. Primary viral replication takes place in epithelial cells of the higher respiratory tract, adopted by unfold of virus to regional lymph nodes and subsequent viremia and systemic dissemination. Virus may be isolated from saliva for five to 7 days earlier than and as much as} 9 days after the onset of scientific signs, that means that an contaminated individual is probably capable of to} transmit mumps for a period of about 2 weeks. An estimated 30% of mumps infections in kids are subclinical or associated only with non-specific higher respiratory an infection signs. Mumps often begins with a short prodromal part of low-grade fever, malaise, headache, and anorexia. Patients then develop the attribute parotid tenderness and enlargement, which lifts the earlobe forward and obscures the angle of the mandible. The parotid glands are concerned most commonly, although different salivary glands sometimes additionally be} enlarged. Parotitis initially additionally be} unilateral, with swelling of the contralateral parotid gland occurring 2 to 3 days later; bilateral parotitis finally develops in 70% of patients with symptomatic salivary gland involvement. Painful parotid gland enlargement progresses over about 3 days, adopted by defervescence and resolution of parotid pain and swelling within about 7 days. Symptomatic meningitis happens in 15% of cases and is the second most common manifestation of mumps. Signs and signs of meningeal irritation (headache, neck stiffness, vomiting, and lethargy) plus excessive fever often develop four to 5 days after the onset of parotitis, although the meningitis could sometimes precede the parotitis.
Best biotin 5000 mcg
There is a decline in both feminine and male reproductive efficiency after age 25 years. Couples who complain of infertility advantage evaluation regardless of the length of infertility. The evaluation begins with a detailed historical past obtained from both companions and physical examinations of both people. Each couple must be questioned collectively and separately because of|as a result of} separate interviews could uncover info that would not be imparted within the presence of the partner. Initial evaluation for infertility generally contains (1) assessment of semen, (2) documentation of ovulation by basal physique temperature, serum progesterone determination approximately 6 to 8 days earlier than menses, or endometrial biopsy less than 3 days earlier than onset of menses, and (3) evaluation of the feminine genital tract by hysterosalpingography. Diagnostic laparoscopy with tubal dye instillation must be performed if results of all earlier exams are normal because of|as a result of} 30 to 50% of ladies are found to have endometriosis or tubal disease on surgical evaluation. Induction of ovulation should by no means be tried till serious problems precluding being pregnant are ruled out or handled. Furthermore, ovulation induction must be utilized solely in ladies with persistent anovulation, because of|as a result of} ladies with ovarian failure are unresponsive to any type of ovulation induction. A typical course of clomiphene remedy is begun on the fifth day following both spontaneous or induced uterine bleeding. Clomiphene appears to act as an anti-estrogen and stimulates gonadotropin secretion by the pituitary gland to initiate follicular development. If ovulation is still not achieved, dosage is elevated in a stepwise fashion by 50-mg increments to a maximum of 200 to 250 mg every day for five days. The highest dose must be continued for 3 to 6 months earlier than the affected person is considered a clomiphene failure. The amount of drug and the length of time that used, as advised here, are higher than those recommended by the producers, but conform with printed sequence. Ovulation can be documented by monitoring adjustments in basal physique temperature or preferably by measuring serum progesterone approximately 14 days after the last clomiphene tablet is taken. Of appropriately chosen sufferers, 75 to 80% will ovulate and forty to 50% can be expected to turn out to be pregnant. The most serious ones embody vasomotor flushes (10%), belly discomfort (5%), breast tenderness (2%), nausea and vomiting (2%), visible symptoms (1. Concern has lately been raised about the potential for clomiphene to enhance the danger of epithelial ovarian cancer. The proof is insufficient to change current practices but suggests that clomiphene be administered prudently and much less than|for under} a restricted variety of cycles. Both bromocriptine and cabergoline, two dopamine agonists, are efficient in inducing ovulation in hyperprolactinemic ladies. Ovulatory menses and being pregnant are achieved in about 80% of sufferers with 1340 galactorrhea and hyperprolactinemia. The majority of ladies with prolactin-secreting pituitary tumors remain asymptomatic during being pregnant. It is rare for a affected person with both a microadenoma or a macroadenoma to develop an issue related to the tumor that impacts both the mother or the fetus during being pregnant. Monitoring during being pregnant need consist solely of questioning the affected person about the development of visible symptoms and headaches. No antagonistic results of dopamine agonists on fetuses or pregnancies have been reported. Several preparations of purified and synthetic biochemically engineered gonadotropins to be used for induction of ovulation now exist. Use of the analogues necessitates administration of larger portions of exogenous gonadotropins. Ovulation can be induced in almost 100 percent of sufferers, but being pregnant occurs in solely 50 to 70%. Concerns have been raised that exogenous gonadotropins could enhance the danger of ovarian epithelial cancer, but the data are too tenuous to require any change in current apply. The ovaries enlarge remarkably on this treatment-induced syndrome, and a number of} follicle cysts, stromal edema, and a number of} corpora lutea are current. There is a shift of fluid from the intravascular space into the belly cavity with resultant hypovolemia and hemoconcentration. Sexual responses generally are divided into 4 phases: excitement, plateau, orgasm, and determination. With sexual arousal and excitement, vasocongestion and muscular rigidity enhance progressively, primarily within the genitals, manifested by vaginal lubrication within the feminine. Sexual excitement is initiated by any of selection of|quite a lot of|a wide range of} psychogenic or somatogenic sexual stimuli and must be bolstered to lead to orgasm. With continued stimulation, the excitement section increases in intensity right into a plateau section during which a excessive state of sexual curiosity is maintained. The orgasmic section tends to be brief and is characterized by fast launch from the developed vasocongestion and muscular rigidity. Although ladies could resolve toward sleep following orgasm, many remain responsive to sexual stimulation and may return to plateau and subsequent orgasm. Estrogens amplify the sexual responses, but responses could occur in estrogen-deficient ladies. For ladies these adjustments occur within the breasts and within the pudendal region and are variable from one response cycle to one other. For some ladies, excitement proceeds rapidly through plateau to orgasm, and orgasm is explosive and accompanied by vocalization and involuntary contractions of the pelvic skeletal muscles. For other ladies, the responses are sluggish in constructing, managed in amplitude, and long-lasting. The somatic sensate focus enabling orgasmic launch is variable and may embody stimulation of the breasts, vagina, or clitoris. The psychological side of coitus could involve concentration on the present partner or act or fantasies about other times and persons. Women could search session because of disturbances in normal sexual arousal or orgasm. A variety of ailments affecting neurologic perform, including diabetes mellitus and a number of} sclerosis, could stop sexual arousal. So, too, could local pelvic problems, similar to endometriosis and vaginitis, which trigger dyspareunia and result in sexual avoidance. Estrogen deficiency inflicting vaginal atrophy and dyspareunia is a relatively frequent explanation for sexual dysfunction. Debilitating systemic ailments similar to malignant disease may affect on} sexual perform not directly. For instance, vaginismus entails involuntary contractions of the muscles surrounding the introitus and results in dyspareunia. It is a conditioned response engendered by a earlier imagined or real traumatic sexual expertise. Feelings of guilt, attributable to incest or rape as examples; of inadequacy, attributable to hysterectomy or mastectomy; or of melancholy or anxiousness could result in failure to be aroused. Failure to achieve orgasm additionally be} seen as a dysfunction if the lady is annoyed or dissatisfied. Treatment of sexual dysfunction is best achieved by eliminating useful causes and providing the affected person, often collectively along with her partner, with acceptable psychological counseling. Behavioral modification is efficient in treating many women with psychological sexual dysfunction. A easy textual content graphically detailing the therapeutic strategies first introduced by Masters and Johnson. Sterilization must be thought-about to be everlasting, despite the possibility of|the potential of|the potential for} surgical reversal. During contraceptive counseling these benefits and downsides must be thoroughly defined so the person will select probably the most acceptable methodology and never discontinue use prematurely and have an undesirable being pregnant. In the United States in 1995 there were about 60 million ladies within the reproductive age group (15 to 44) and 39 million (65%) were utilizing a method of contraception. Of the remainder, about 5% were sterile (prior hysterectomy), 9% were pregnant or making an attempt to conceive, 11% were by no means sexually lively, and 6% had no latest sexual exercise. Next in frequency of use was the male condom followed by male sterilization (Table 251-1). Of the ladies with an undesirable being pregnant, 50% said they were utilizing a method of contraception within the month they conceived. The terms methodology effectiveness and use effectiveness (or methodology failure and affected person failure) were beforehand used to describe the frequency of conceptions that occurred while the tactic was getting used accurately or incorrectly. They also present a mechanical barrier and need to be placed into the vagina earlier than each coital act.
Cheap biotin 5000 mcg
A exact source for gram-negative bacteremia is recognized in only a minority of cases, however the gastrointestinal tract, respiratory tract, delicate tissue, and urinary tract are probably the most possible sources for an infection. As a basic rule, nonetheless, nearly any organism can be pathogenic if host defenses are severely impaired. Enterobacter species, Citrobacter species, and Serratia marcescens are much less frequently encountered however are notable outcome of|as a result of} they quickly turn into proof against beta-lactam antibiotics through the induction of chromosomally mediated beta-lactamases. Of concern, a rise in Enterobacter sepsis has been noticed at a number of|numerous|a selection of} remedy centers. Other much less common gram-negative isolates embrace Acinetobacter species, Haemophilus species (usually non-typable H. The gram-positive organisms most frequently encountered are the coagulase-negative staphylococci (most commonly S. Both coagulase-positive and coagulase-negative staphylococci are most commonly isolated from the blood, typically from sufferers with indwelling intravenous catheters or from these with foreign bodies such as prosthetic heart valves or orthopedic implants. During the last decade, coagulase-negative staphylococci have turn into increasingly proof against beta-lactam antibiotics, and the bulk (50 to 80%) are methicillin resistant and customarily require remedy with vancomycin. Enterococcus has emerged as a trigger of serious an infection in some centers and is especially necessary due to the increased resistance to vancomycin. Infections caused solely by anaerobic micro organism are much less common and often related to a concomitant abnormality in gastrointestinal mucosal integrity. Although Bacteroides fragilis and Clostridium perfringens are the most typical organisms, other Bacteroides species, nicely as|in addition to} other Clostridium species. Anaerobes are frequent components of intra-abdominal infections, including peritonitis, intra-abdominal abscesses, and perirectal cellulitis or abscesses. Clostridium difficile is a common cause of colitis in neutropenic sufferers treated with antibiotics or cytotoxic brokers. More commonly, fungal infections happen as a secondary course of in sufferers receiving antibacterial brokers. Although fungal infections may be be} encountered in a neutropenic host, Candida and Aspergillus species predominate. In neutropenic sufferers, Candida infections might embrace candidemia, catheter-related infections, invasive mucosal infections. Other fungal pathogens that will happen in neutropenic sufferers embrace Mucoraceae organisms (Mucor, Rhizopus, Absidia, and Cunninghamella-often clinically resembling Aspergillus infections), Trichosporon beigelii (which might trigger disseminated visceral and cutaneous disease), Fusarium, Drechslera, Pseudallescheria boydii, and Malassezia furfur. Qualitative Abnormalities of Phagocytes the microbicidal activity of granulocytes and monocytes involves advanced interactions between the cell and the organism or inflammatory site. Some of the main capabilities necessary for microbicidal activity embrace migration of the cell to the inflammatory site (or chemotaxis), cell activation, phagocytosis, and intracellular and extracellular killing via each oxygen-dependent and oxygen-independent pathways. Nevertheless, through the secure continual part of the disease, infectious problems are hardly ever seen in these sufferers. In addition to immunoglobulin deficiencies that impair opsonization, sufferers with continual lymphocytic leukemia and a number of} myeloma may have such abnormalities as faulty granulocyte adherence, decreased granulocyte migration, a lower in the number of granulocyte receptors for C3b and IgG, and decreased chemotaxis of monocytes. Although the predominant defect in host defense in most sufferers with aplastic anemia is neutropenia, followed by immune suppression remedy. Patients with paroxysmal nocturnal hemoglobinuria appear to have an increased susceptibility to bacterial an infection. In addition to splenic dysfunction, irregular complement activation, and faulty serum opsonizing capability, faulty phagocytic function has been described in sufferers with sickle cell anemia, though the importance of this relationship is unclear. Neutrophils from infection-prone children with sickle cell disease have been proven to have faulty bactericidal activity, perhaps second to zinc deficiency. Some sufferers with extreme glucose-6-phosphate dehydrogenase deficiency appear to have an increased susceptibility to infections attributable to catalase-positive micro organism. The medical picture resembles that of continual granulomatous disease of childhood, though only hardly ever are infections reported in the 1st decade of life. The granulocytes present normal phagocytosis and chemotaxis however faulty bactericidal activity. Most cytotoxic medication used for the remedy of malignant and autoimmune illnesses or transplantation have antiproliferative effects resulting in neutropenia and monocytopenia. Among the antineoplastics, probably the most commonly implicated brokers embrace methotrexate, 6-mercaptopurine, vincristine, vinblastine, anthracyclines, cyclophosphamide, carmustine, and platinum compounds. As a basic rule, the indicators and signs of even extreme infections may be be} masked or significantly decreased in sufferers receiving steroids. In addition, steroids might trigger monocytopenia nicely as|in addition to} defects in monocyte chemotaxis, phagocytosis, and killing of micro organism and fungi. In addition to their motion on granulocytes and monocytes, steroids might enhance susceptibility to an infection by impairing wound therapeutic, rising pores and skin fragility, and miserable lymphocyte function, the production of cytokines, and humoral immune responses. The appropriate use of these hematopoietic cytokines in neutropenic cancer sufferers has been the topic of debate and is finest guided by the recommendation from the American Society of Clinical Oncologists that restricts use to high-risk sufferers with a higher than 40% likelihood of fever related to a neutropenic episode. It must be underscored that utilization of} new biologic brokers in medical follow ought to be guided by carefully carried out medical trials. Chronic granulomatous disease has served as a prototype for illnesses characterized by faulty oxidative metabolism of phagocytes. Although continual granulomatous disease represents a heterogeneous group of problems from a molecular and genetic perspective, the common denominator is that phagocytes lack important components of oxidative metabolism and fail to generate the respiratory burst in response to numerous stimuli, including certain pathogenic organisms. The organisms that trigger critical infections in sufferers with continual 1573 granulomatous disease are most frequently people who include the enzyme catalase. In the absence of cellular production of H2 O2, the peroxide generated by non-catalase-containing organisms sufficient to|is sufficient to} ameliorate the neutrophil deficiency and allow microbicidal activity. The majority of infections in sufferers with continual granulomatous disease are attributable to S. Serious recurrent infections often begin in the 1st 12 months of life in children with continual granulomatous disease. The lung is the most typical site of an infection (pneumonias and abscesses), with other common infections including pores and skin and delicate tissue abscesses, visceral abscesses (particularly hepatic), osteomyelitis (especially of the small bones in the palms and feet), and suppurative lymphadenopathy. Uncommonly, continual granulomatous disease can happen in adolescence or adulthood, though with a careful historical past, infectious problems typically date back to childhood. Antibiotic prophylaxis with trimethoprim-sulfamethoxazole has been advocated by many investigators. Interferon-gamma has additionally been proven to reduce the incidence of serious an infection and the number of hospital days for sufferers with continual granulomatous disease. Myeloperoxidase deficiency is probably the most typical of all granulocyte problems, with an estimated frequency ranging from 1 in 2000 to 1 in 4000. Myeloperoxidase is a lysosomal enzyme that catalyzes the formation of hypochlorous acid from H2 O2 produced in the respiratory burst. Interestingly, most people recognized with myeloperoxidase deficiency are wholesome, and infectious problems are exceedingly rare. Systemic Candida infections have occurred in a small number of myeloperoxidase-deficient sufferers who additionally had diabetes mellitus. Chediak-Higashi syndrome is a rare dysfunction characterized by autosomal recessive inheritance, recurrent infections, partial oculocutaneous albinism, central and peripheral neuropathy, and increased bleeding time. Infections result from the mixed effects of neutropenia and practical defects in phagocytes, which embrace impaired degranulation and faulty chemotaxis. Infections frequently involve the pores and skin, respiratory tract, and mucous membranes and are most commonly attributable to S. Accordingly, neutrophils show defects in aggregation, margination, chemotaxis, and phagocytosis. The most typical infections are pores and skin and subcutaneous tissue infections, otitis, mucositis, gingivitis, and periodontitis. A number of problems have been described which are be} characterized by defects in the chemotaxis of granulocytes and/or monocytes. Infections in these sufferers tend to to|are inclined to} be cutaneous, and the most typical pathogens are S. The "lazy leukocyte" syndrome may be related to neutropenia and is characterized by gingivitis, recurrent otitis media, rhinitis, and stomatitis. Chemotaxis defects have been reported in sufferers with congenital ichthyosis and recurrent T. Defective cell-mediated immunity might lead to infections attributable to micro organism, fungi, viruses, and protozoa. The predominant pathogens are intracellular organisms (those microbes that survive inside macrophages) and embrace mycobacteria (both M. Cell-mediated immunity defects have been postulated to assist clarify the incidence of atypical mycobacterial infections in sufferers with furry cell leukemia and also happen in comparatively rare T-cell malignancies such as mycosis fungoides and T-cell continual lymphocytic leukemia.
References:
- https://novascotia.ca/dhw/populationhealth/surveillanceguidelines/viral_hemorrhagic_fevers.pdf
- https://resources.sei.cmu.edu/asset_files/TechnicalReport/2008_005_001_14993.pdf
- https://www.naspghan.org/files/documents/pdfs/position-papers/Health_Supervision_in_the_Management_of_Children.19%5B1%5D.pdf