.png)
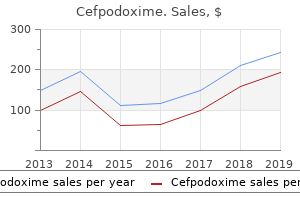
200 mg cefpodoxime
The neuromuscular spindle indirectly influences the control of voluntary movement (see p. The flower-spray endings are situated mainly on the nuclear chain fibers a long way|far} from the equatorial region (see. Each neurotendinous spindle has a fibrous capsule, loosely organized collagen fibers, and tendon cells (see p. The neurotendinous spindles are situated in tendons close to the musculotendinous junction. The nerve ends throughout the spindle by branching and terminating in club-shaped endings. The neurotendinous spindle is activated by changes in muscle tension and inhibits muscle contraction. At a neuromuscular junction, each axon lies in a groove on the surface of the muscle fiber fashioned by the infolding of the muscle plasma membrane (sarcolemma) (see. At a neuromuscular junction, each terminal department of the motor nerve ends as a naked axon. Having triggered depolarization of the postsynaptic membrane, the acetylcholine is immediately hydrolyzed within the synaptic cleft by acetycholinesterase (see p. Acetylcholine is launched from the axon terminal when the nerve impulse reaches the neuromuscular junction. At the neuromuscular junction, the Schwann cells kind a cap or roof for the groove on the surface of the muscle fiber. Autonomic nerve fibers terminate on smooth muscle fibers as unmyelinated fibers (see p. In neuromuscular junctions of smooth muscle, the autonomic nerve fiber exerts control over several of} muscle fibers (see p. In smooth muscle, the wave of contraction passes from one muscle fiber to one other via hole junctions. In cardiac muscle, the wave of contraction spreads rapidly from one muscle fiber to one other method of|by means of|by the use of} desmosomes and hole junctions. At the location of a neuromuscular junction involving smooth muscle,the axon lies in a shallow groove on the muscle surface,and the Schwann cell is retracted to expose the axolemma (see. To produce a region of full anesthesia on the trunk, minimal of|no much less than} three segments of the spinal cord need to be broken (see p. When contiguous spinal nerves are sectioned, the realm of tactile loss is all the time greater than the realm of loss of painful and thermal sensations. The biceps brachii tendon reflex entails C5-6 segments of the spinal cord (see p. The patellar tendon reflex (knee jerk) entails the L2-4 segments of the spinal cord. A tumor urgent on the S1-2 segments of the spinal cord is likely to to|prone to} intrude with the ankle jerk. The T10 dermatome consists of the pores and skin of the umbilicus; the T8 dermatome entails the pores and skin between the xiphoid course of and the umbilicus. The L5 dermatome lies over the anterior and lateral surfaces of the leg below the knee. The S2 dermatome extends down the middle of the posterior surface of the thigh and leg (see. A motor unit consists of a motor neuron within the anterior gray column (horn) of the spinal cord and all the muscle fibers it supplies (see. In the small muscle tissue of the hand, one nerve fiber supplies only some muscle fibers. The gamma motor efferent fibers innervate the intrafusal fibers of a muscle spindle. In voluntary muscle movement, when a main mover contracts, the antagonistic muscle tissue are inhibited (see Pages ninety three and 94). In the standing place, the road of gravity passes through the odontoid process of the axis, behind the centers of the hip joints, and in front of the knee and ankle joints (see. A explicit posture can usually be maintained for lengthy durations by totally different groups of muscle fibers in a muscle contracting in relays. The cerebral cortex makes an necessary contribution to the maintenance of normal posture (see p. Muscle wasting can occur if solely the efferent motor nerve fibers to a muscle are sectioned (see p. Muscle contracture is a condition during which the muscle contracts and undergoes permanent shortening; it happens frequently in muscle tissue that normally oppose paralyzed muscle tissue. Muscle fasciculation is seen with persistent disease that affects anterior horn cells or the motor nuclei of cranial nerves. Wasting happens within the muscle tissue acting on the shoulder joint in patients with painful pericapsulitis involving that joint. The construction of human digital pacinian corpuscles (corpusculae lamellosae) and its functional significance. The construction of the potassium channel: Molecular basis of K conduction and selectivity. The Fine Structure of the Nervous System: the Neurons and Supporting Cells (3rd ed. Changes within the histochemical appearances of cholinesterase in a blended peripheral nerve following nerve section and compression harm. Changes within the histochemical appearances of cholinesterase on the motor end-plate following denervation. The degeneration of unmyelinated axons following nerve section: An ultrastructural examine. Rate of recovery in motor and sensory fibers of the radial nerve: Clinical and electrophysiological aspects. On initial analysis within the emergency division after he had regained consciousness,he was found to have signs and signs of severe neurologic deficits within the upper and decrease extremities. A lateral radiograph of the cervical region of the spine confirmed fragmentation of the body of the fourth cervical vertebra with backward displacement of a giant bony fragment on the left facet. After stabilization of the vertebral column by using skeletal traction to forestall additional neurologic injury, an entire examination revealed that the patient had signs and signs indicating incomplete hemisection of the spinal cord on the left facet. Any medical personnel involved within the analysis and remedy of a patient with spinal cord accidents should know the construction of the spinal cord and the association and capabilities of the varied nerve tracts passing up and down this very important conduit within the central nervous system. All medical personnel will need to have} a clear image of the extent of the cord lesion and the potential expectations for the return of function. A 132 C H A P T E R O B J E C T I V E S To learn how accidents to the spinal cord can occur To understand the place of the primary nervous pathways and nerve cell groups within the spinal cord properly as|in addition to} be able to|be capable of|have the flexibility to} correlate radiologic proof of bone harm with segmental levels of the spinal cord and neurologic deficits To review the fundamental construction of the fragile spinal cord and the positions and capabilities of the varied ascending and descending tracts that lie inside it To make easy line drawings of every of the ascending and descending tracts, displaying their cells of origin, their course through the central nervous system, and their vacation spot Spinal cord accidents are common and might occur end result of|because of|on account of} vehicle and motorcycle accidents, falls, sports accidents, and gunshot wounds. Spinal cord and spinal nerve injury may also be related to vertebral fractures; vertebral infections; vertebral tumors, both primary and secondary; and herniated intervertebral discs. The pupil should be taught the course and connections of the varuous tracts throughout the spinal cord in order to to} be able to|be capable of|have the flexibility to} diagnose and understand the remedy of cord accidents. Particular attention must be paid as to whether a specific tract crosses the midline to the alternative facet of the central nervous system or remains on the identical facet. The evaluation of neurologic injury requires not solely an understanding of the primary nervous pathways throughout the spinal cord however an ability to correlate radiologic proof of bone harm with segmental levels of the spinal cord. The close relationship of the spinal cord to the bony vertebral column necessitates a brief review of the vertebral column before the spinal cord is taken into account. It supports the cranium, pectoral girdle, upper limbs, and thoracic cage and, method of|by means of|by the use of} the pelvic girdle, transmits body weight to the decrease limbs. Within its cavity lie the spinal cord, the roots of the spinal nerves, and the masking meninges, to which the vertebral column provides nice safety. A typical vertebra consists of a rounded body anteriorly and a vertebral arch posteriorly. These enclose a space called the vertebral foramen, through which run the spinal cord and its coverings. The vertebral arch consists of a pair of cylindrical pedicles, which kind the edges of the arch, and a pair of flattened laminae, which full the arch posteriorly. The vertebral arch provides rise to seven processes: one spinous, two transverse, and four articular. The spinous course of, or spine, is directed posteriorly from the junction of the two laminae.
Waxberry (Bayberry). Cefpodoxime.
- Dosing considerations for Bayberry.
- Are there safety concerns?
- Colds, diarrhea, fevers, and nausea.
- How does Bayberry work?
- What is Bayberry?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96199
Effective 100 mg cefpodoxime
Reorganization of hippocampal practical connectivity with transition to chronic again pain. Communication between neuronal somata and satellite tv for pc glial cells in sensory ganglia. Chronic-pain-associated astrocytic reaction in the spinal cord dorsal horn of human immunodeficiency virus-infected patients. Oligodendrocyte ablation triggers central pain independently of innate or adaptive immune responses in mice. Gray matter alterations in chronic pain: a network-oriented meta-analytic method. Beyond feeling: chronic pain hurts the mind, disrupting the default-mode network dynamics. Functional reorganization of the default mode network across chronic pain circumstances. Functional magnetic resonance imaging proof of augmented pain processing in fibromyalgia. Structural and practical mind abnormalities in chronic low again pain: a scientific evaluate. Rapid synaptic remodeling in the grownup somatosensory cortex following peripheral nerve harm and its association with neuropathic pain. This study used two-photon imaging of the somatosensory cortex in dwelling grownup mice to monitor changes in synaptic spine turnover in a mannequin of neuropathic pain. Remodeling the dendritic spines in the hindlimb illustration of the sensory cortex after spinal cord hemisection in mice. Morphological and practical reorganization of rat medial prefrontal cortex in neuropathic pain. Chronic again pain is related to decreased prefrontal and thalamic grey matter density. Complex regional pain syndrome kind I affects mind construction in prefrontal and motor cortex. Accelerated mind grey matter loss in fibromyalgia patients: untimely aging of the brain? Gray matter changes following limb amputation with excessive and low intensities of phantom limb pain. Structural mind anomalies and chronic pain: a quantitative meta-analysis of grey matter volume. Anatomical changes on the level of the first synapse in neuropathic pain: proof from the spinal trigeminal nucleus. Effective therapy of chronic low again pain in humans reverses abnormal mind anatomy and performance. This study showed that efficient pain therapy reverses both structural and practical abnormalities in the brains of patients with chronic pain, and related these changes to therapy outcome. Targeted ablation, silencing, and activation establish glycinergic dorsal horn neurons as key parts of a spinal gate for pain and itch. Spinal nerve lesion alters blood-spinal cord barrier function and prompts astrocytes in the rat. Brain dynamics for perception of tactile allodynia (touch-induced pain) in postherpetic neuralgia. Identity of myelinated cutaneous sensory neurons projecting to nocireceptive laminae following nerve harm in grownup mice. Peripheral nerve harm triggers noradrenergic sprouting within dorsal root ganglia. Peripheral nerve harm results in the institution of a novel pattern of sympathetic fibre innervation in the rat skin. Is sympathetic sprouting in the dorsal root ganglia liable for the production of neuropathic pain in a rat model? Delayed reinnervation by nonpeptidergic nociceptive afferents of the glabrous skin of the rat hindpaw in a neuropathic pain mannequin. Axonal sprouts containing calcitonin gene-related peptide and substance P type pericellular baskets round giant diameter neurons after sciatic nerve transection in the rat. Early increasing-intensity treadmill train reduces neuropathic pain by stopping nociceptor collateral sprouting and disruption of chloride cotransporters homeostasis after peripheral nerve harm. Pathological sprouting of grownup nociceptors in chronic prostate cancerinduced bone pain. This paper offered detailed and comprehensive analyses of structural plasticity of nociceptors in relation to cancer-induced bone pain in rodents. Hematopoietic colonystimulating factors mediate tumor-nerve interactions and bone cancer pain. Disinhibition opens the gate to pathological pain signaling in superficial neurokinin 1 receptor-expressing neurons in rat spinal cord. Lack of proof for sprouting of A afferents into the superficial laminas of the spinal cord dorsal horn after nerve part. Shape shifting pain: chronification of again pain shifts mind illustration from nociceptive to emotional circuits. This study showed that the conversion from subacute to chronic pain was accompanied by a shift of mind activation patterns from regions involved in nociceptive processing to regions related to emotional processing. Reassessing cortical reorganization in the primary sensorimotor cortex following arm amputation. A computational mannequin unifies apparently contradictory findings concerning phantom pain. Mirror therapy for phantom limb pain: mind changes and the position of physique illustration. Many totally different systems across quite a few mind areas must work collectively to ensure proper motor control. We will begin a journey by way of these areas, starting on the spinal cord and progressing up the mind stem and ultimately reaching the cerebral cortex. Remember, this material is essential for you as future physicians as a result of|as a result of} lots of your patients will exhibit indicators and signs related to motor illnesses. Stretch Reflex Reflexes are quick latency, relatively automatic responses to sensory stimulation. One of the only and greatest studied reflexes is the stretch reflex - stretch a muscle and the reflex circuit results in contraction of the identical muscle. They are functionally efficient as a result of|as a result of} they allow weight-bearing muscles to adjust to a altering load on the level of the spinal cord, without the information having to go all as much as} cortex for a call. This is achieved with a muscle spindle (our old pal from spinal cord and Physiology lectures) and a few neurons. Ia fibers are related primarily with the nuclear bag intrafusal fibers and carry info relating to the length and alter in length of the muscle. This leads to contraction of the extrafusal muscle fibers in the identical (homonymous) muscle. In the cat, a single Ia fiber makes excitatory connections with all homonymous motor neurons. This Ia divergent sign produces a really robust excitatory drive to the muscle within which it originates. Another essential supply of inhibition that acts on this circuit is the Renshaw cell. Renshaw Ia inhibitory interneuron cells are excited by collaterals (branches) Renshaw cell of motor neuron axons and then the Renshaw cells inhibit those same motor neurons. Increases in activity in the motor neuron enhance inhibition from the Renshaw cell. This helps to stabilize the activity of the motor neuron and prevents sustained intervals of extraordinarily excessive activity, which may produce muscle tetanus. The Renshaw cell also inhibits the Ia interneuron related to the antagonist muscle. The Renshaw cell shown acts to inhibit biceps muscle contraction and dis-inhibit (effectively increase) triceps muscle contraction. Thus, Renshaw cells, like another spinal interneurons mentioned beneath, adjust in a complementary style the activity of opposing muscle teams. The intrafusal muscle fibers in the muscle spindles could be managed by the small gamma efferent neurons that lie in the ventral horn. Gamma efferents that innervate the baggage are called gamma dynamics while those focusing on the chains are gamma statics. These gamma efferent cells, which are influenced by descending cortical and brainstem inputs, bias the intrafusal muscle fibers find a way to} certain that|be certain that} the intrafusal muscle fibers are always signaling info to the mind.
Cheap 200mg cefpodoxime
Stable melancholy of potentiated synaptic responses within the hippocampus with 15Hz stimulation. State-dependent heterogeneity in synaptic melancholy between pyramidal cell pairs. Bidirectional long-term modification of synaptic effectiveness within the grownup and immature hippocampus. The transverse hippocampal slice: a well-defined cortical construction maintained in vitro. Replay of neuronal firing sequences in rat hippocampus during sleep following spatial expertise. Potentiation or melancholy of synaptic efficacy within the dentate gyrus is set by the connection between the conditioned and unconditioned stimulus in a classical conditioning paradigm in rats. Long-lasting melancholy of parallel fiber-Purkinje cell transmission induced by conjunctive stimulation of parallel fibers and climbing fibers within the cerebellar cortex. Climbing fiber microzones in cerebellar vermis and their projection to totally different teams of cells within the lateral vestibular nucleus. Topographical group of the cerebellar cortical projection to nucleus interpositus anterior within the cat. Classical conditioning using stimulation of the inferior olive as the unconditioned stimulus. Mapping behaviorally relevant neural circuits with immediate-early gene expression. In vivo two-photon imaging reveals a job of Arc in enhancing orientation specificity in visual cortex. Multiple durations of functional ocular dominance plasticity in mouse visual cortex. Selective electrical silencing of mammalian neurons in vitro means of} invertebrate ligand-gated chloride channels. Reversible silencing of neuronal excitability in behaving mice by a genetically focused, ivermectin-gated Cl channel. A genetic method for selective and shortly reversible silencing of mammalian neurons. Rapid and reversible chemical inactivation of synaptic transmission in genetically focused neurons. Neural substrates of awakening probed with optogenetic control of hypocretin neurons. Independence of firing correlates of anatomically proximate hippocampal pyramidal cells. Long-term plasticity in hippocampal place-cell representation of environmental geometry. Putting worry in its place: remapping of hippocampal place cells during worry conditioning. Activity-regulated cytoskeletalassociated protein is localized to just lately activated excitatory synapses. Severe psychiatric facet effects} because of of} mefloquine intoxication are well documented, including anxiousness, panic assaults, paranoia, persecutory delusions, dissociative psychosis, and anterograde amnesia. In this article, we talk about the history of mefloquine use and describe plausible mechanisms of its psychotropic motion. Mefloquine intoxication has not but been efficiently advanced in authorized proceedings as a defense or as a mitigating factor, but it appears probably that it eventually shall be. Considerations for the appliance of claims of mefloquine intoxication in forensic settings are mentioned. Nevin is a doctoral pupil within the Department of Mental Health, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland. Nevin has served as paid and pro bono advisor to attorneys representing litigants advancing claims of hurt from exposure to mefloquine. Results of those and subsequent trials have since demonstrated that the incidence of particular neuropsychiatric signs including nightmares, anxiousness, and psychosis during prophylactic use are each at least of|no much less than} a hundred instances extra common28,30,31 than has been beforehand reported. Current or previous users of the drug may claim that exposure has caused bodily or psychological injury. In this evaluate, the psychiatric facet effects} of mefloquine and the putative pathophysiology of those results are mentioned, and particular forensic issues are thought-about. This info is anticipated to be helpful when forensic psychiatrists are asked to seek the advice of} on circumstances involving military personnel and veterans, civilian travelers, and staff on overseas project who claim authorized implications from their exposure to the drug. Despite over 20 years of licensed use, the underlying pathophysiology of those facet effects} has been poorly understood. In this part, the putative pathophysiology of mefloquine intoxication is described in additional detail following a discussion of its typical medical presentation. Clinical Presentation Case reviews suggest that mefloquine intoxication may start with a variable prodrome which can current with personality change,forty unease,forty anxiousness,7375 phobias,seventy six,77 and a way of impending doom and restlessness. Such signs have been reported after only a single 250-mg tablet40,9396 and should progress in severity with subsequent doses. Mefloquine psychosis was characterized as early as 1983,89 and its early descriptions were consistent with with} the psychosis caused by associated antimalarial compounds. The usually vivid and terrifying nature of the hallucinations produced by mefloquine are illustrated by an early unindexed case report, just like at least of|no much less than} one different published report,41 describing a person who jumped from his lodge room within the false perception that his room was on hearth. Of observe, vivid goals or horrific, terrifying nightmares,39,104 also incessantly reported by users of mefloquine, are characterized as having "Technicolor clarity" and being "vividly remembered days later,"5 suggesting that these can also be prodromal to or inform later signs of psychosis. An additional distinguishing function reported with mefloquine psychosis is impairment of short-term memory. Consistent with prodromal signs of confusion, this deficit marked by preliminary attentional disturbances, with later insufficiencies in short-term working and spatial memory,forty verbal memory,38 and temporospatial disorientation. The limbic system, which incorporates the hippocampus and amygdala, considered one of the|is among the|is probably certainly one of the} oldest parts of the brain phylogenetically and is considered the system liable for preservation of the self and the species through the era of emotions, reward mechanisms, sexual drive, and the formation of long-term reminiscences, including worry memory. Gap junction channels, composed of proteins known as connexins, are involved in coordinated synchronization of neuronal exercise, significantly of inhibitory interneurons121 found throughout the limbic system. In addition to a dose-dependent progression, signs of mefloquine intoxication may exhibit a waxing and waning presentation. It is tempting to speculate that in some circumstances, this presentation may replicate the medical course of an underlying limbic status epilepticus114 or limbic seizure132134 kindled by the drug. Reports describing seizures and psychotic reactions instantly following alcohol ingestion are well represented within the literature,forty two,136,137 and alcohol use is incessantly raised as a potential confounding think about circumstances of severe reactions to the drug. Similarly, reviews of very complicated visual illusions distinct from hallucinations40,eighty,85 suggest extralimbic involvement encompassing the visual pathways. Reports of multifocal myoclonus145,146 and deficits in motor speed38,39,forty and motor learning147 are suggestive of additional involvement of the basal ganglia and inferior olive. As with certain types of limbic encephalitis,142,148,149 limbic encephalopathy resulting from mefloquine intoxication can also progress to contain the brainstem,forty and consequently users of mefloquine may expertise numerous bodily signs, including nausea and emesis, that are broadly referable to interconnected limbic and brainstem facilities. Rare reviews of anticholinergic syndrome157 may point out additional brainstem involvement. Historically, the forensic utility of a claim of mefloquine intoxication has been made difficult by missed analysis and the attribution of psychiatric results to different causes. Exposure the forensic utility of a claim of mefloquine intoxication begins with establishing plausible evidence of exposure. In circumstances the place clear documentation of particular person prescribing exists within the medical document or if a person has retained individually labeled treatment, exposure readily proven or conceded. However, as mefloquine is often mass prescribed as a public health measure,sixty five usually without individualized documentation or labeling, unequivocal evidence of exposure may incessantly be unavailable. Because of its lipophilicity116 and its recycling within the enterohepatic circulation, mefloquine excreted unchanged within the feces12 and also found within the gastric juices and bile. Advancing a defensible claim of mefloquine intoxication may subsequently require the collaborative involvement of different medical specialists along with conventional neuropsychiatric analysis, in order to rule out confidently different plausible etiologies, including those caused by different intoxicants and illness states. Careful document evaluate, medical history, and acceptable consultation, are essential for improving the specificity and sensitivity of the analysis. Similarly, consultation with neurology ought to be thought-about to rule out intently associated conditions similar to limbic encephalitis or prior medical history of limbic seizure, which in certain circumstances can also confound the analysis of mefloquine intoxication. In the absence of a medical history of central injury or neurologic dysfunction, certain brain or brainstem findings, including persistent vertigo or disequilibrium,forty or certain visual disorders85 that develop subsequent to mefloquine exposure ought to be thought-about pathognomonic of mefloquine neurotoxicity. With acceptable history, these signs strongly assist a claim of preceding intoxication. Specialty consultation with neuro-optometry, neuro-otology, or ear, nose, and throat specialists, with a particular concentrate on to} figuring out central nervous system injury, ought to subsequently be thought-about an invaluable component of the forensic analysis, significantly in individuals beforehand thought-about for a analysis of somatoform, conversion, malingering, or personality dysfunction, which the complicated signs and signs of mefloquine neurotoxicity may mimic or be mistaken for on informal analysis. In this way, histopathological findings at post-mortem of attribute multifocal brain or brainstem lesions, within the absence of different plausible etiologies, would also be pathognomonic of mefloquine neurotoxicity.
Buy cefpodoxime 100mg
Parainfectious myelopathy Neurological injury in parainfectious myelopathy is caused instantly by the infection, the immune response against the agent, and the response of the immune system. It is often outcome of} a blood-borne infection originating in the lungs, the skin, the skeletal, genitourinary or digestive techniques. It presents with extreme motor and sphincter dysfunction related to fever, meningism and skin exanthema. The spinal twine is affected in 11% to 28% of patients, usually in the thoracic and cervical segments. These lesions appear with low signal in T1 sequences, and properly defined with a high signal in T2 sequences; gadolinium enhancement is variable. Myelopathies outcome of} demyelinating ailments the onset of neurologic signs happens over a interval of days end result of|because of|on account of} demyelination, though necrotizing myelopathies, like neuromyelitis optica, may typically progress in a matter of hours. It is estimated to have an effect on} between 250,000 and 350,000 individuals in the United States and greater than 2,500,000 on the planet (40,46). The age of onset of signs varies by area; nonetheless the incidence is low in youngsters, increases in adolescence and peaks between 25 and 35 years of age, after which it begins to decline (47). The picture reveals alteration in the form and signal depth of the vertebral our bodies of T10 and T11, of the disc and of the prevertebral soft tissues. Approximately 80-85% of patients current with a relapsing image, with signs that final for several of} days and improve over the course of weeks. It is probably the most studied of all acute myelopathies, and its results range from irreversible tissue loss to partial de- myelination the place there could be remyelination and restore (40). It may current in the kind a cervicodorsal asymmetric transverse myelitis with sensory signs. Focal lesions are peripheral, asymmetrical and should involve from a number of} millimeters up to as} a couple vertebral segments. A relationship has been discovered between low-signal lesions in T1 sequences and the diploma of disability, whereas no affiliation has been discovered between high-signal and enhancing lesions in T2 sequences. In Asia, the Caribbean and South America, the incidence is larger, pointing to genetic mechanisms. In all populations, females with a mean age of forty are predominantly affected, in a three:1 ratio (51). Twenty-eight-year old affected person recognized with quantity of} sclerosis in December 2010 with development in time and area. Radiological traits embody a central longitudinal and extensive cervicodorsal lesion (three or more spinal segments) with spinal enlargement, of low signal in T1 sequences and high signal in T2 sequences and patchy enhancement. Although the classical considering was that neuromyelitis optica was not accompanied by brain lesions, it has been demonstrated that 60% of patients may have periventricular lesions (areas of high aquaporin 4 concentration, goal for neuromyelitis optica-immunoglobulin G) (8). Published studies counsel a 68% five-year survival, with mortality resulting from extreme spinal compromise and respiratory failure (51). The presence of the neuromyelitis optica-immunoglobulin G antibody predicts the risk of growing recurrent myelitis. Myelopathy outcome of} systemic illness Myelitis related to a systemic illness has been not often described in the literature. Myelitis often happens in the first yr of the illness and could also be} its first manifestation. The hypothesis in regards to the pathophysiology remains to be a topic for debate, and probably the most accepted is a vascular mechanism secondary to ischemic lesions (9). The medical signs often embody transverse myelitis with extreme motor and sensory dysfunction. Moreover, it has been discovered that the central high-signal spinal lesion in T2 sequences, oc- a b Figure 17. Forty-four-year old affected person with demyelinating illness and proven neurological decline. Granados A; Garcнa L; Ortega C; Lуpez A review articles cupying two-thirds of the spinal twine in axial sections, extends over three or four segments and reveals variable gadolinium enhancement (22,25). A satisfactory response to empirical steroid remedy, throughout months or even years, suggests the analysis (6). Post-radiation or electrical injury Neurotoxicity is a known complication of high-dose radiation. The deep white matter is probably the most affected because it includes the cortex and the subcortical arcuate fibers. There are three forms of lesions: acute (weeks or months), early late and late (six months to two years). The latter could also be} irreversible, progressive and, on occasions, deadly; nonetheless, it may resolve spontaneously in some cases (52,53). It may have an early manifestation ten to sixteen weeks into radiotherapy, or a late manifestation, and should resolve spontaneously between two and nine months after onset (9). The transient sensory loss offers an electric-shock sensation when the neck is flexed forward (Lhermitte sign) and it resolves within two and thirty-six weeks. In persistent progressive myelopathy, it presents like a Brown Sйquard syndrome lasting between three months and five years. Patient with a history of radiotherapy outcome of} esophageal most cancers who complains of paresthesias and discreet lack of energy in the decrease limbs, and Lhermitte sign. Subacute combined degeneration Combined subacute degeneration is a complication of vitamin B12 deficiency, related to pernicious anemia. This deficiency could also be} related to parietal-cell autoantibodies or the intrinsic issue required for vitamin B12 binding. There is a genetic deficiency of transcobalamin 2 (cobalamin transporter protein). The complete transcobalamin 2 deficiency is a recessive autosomal condition characterized by normal concentrations of vitamin B12 with extreme infantile megaloblastic anemia related to neurologic injury (54). The medical image presents as a slowly-progressing spastic paraparesis with distal proprioceptive loss and symmetrical dysesthesias (54). The mean time to analysis because the that} onset of neurological signs outcome of} vitamin B12 deficiency is approximately on yr, with a range that extends to four years (54) (Figure 20). Acute paraneoplastic or necrotizing myelitis Paraneoplastic myelopathy is a rare illness. The lesion often includes the thoracic spinal twine that reveals a high-intensity signal in T2 sequences and gadolinium enhancement. Low concentrations of vitamin B12 have been discovered, pointing to the analysis of myelopathy outcome of} vitamin B12 deficiency. A prospective survey of the causes of non-traumatic spastic paraparesis and tetraparesis in 585 patients. Increased signal depth of the spinal twine on magnetic resonance photographs in cervical compressive myelopathy. Symptoms and signs in metastatic spinal twine compression: a study of development from first symptom until analysis in 153 patients. Vascular myelopathiesvascular malformations of the spinal twine: presentation and endovascular surgical management. Frequency of spinal arteriovenous malformations in patients with unexplained myelopathy. Spinal twine infarction: medical and magnetic resonance imaging findings and brief term outcome. Long-term modifications induced by high-dose irradiation of the pinnacle and neck area: imaging findings. Degenerative ailments characterized primarily by cerebral cortex lesions: For each of the next ailments, describe (as appropriate) etiology/pathogenesis of lesions, location of lesions, medical options and course of the illness, diagnostic tests, inheritance sample and genetic mechanism, gross pathology, microscopic pathology · Alzheimer illness · Pick illness (frontotemporal dementia) · Dementia with Lewy our bodies 2. Degenerative ailments characterized primarily by basal ganglia lesions: For each of the next ailments, describe (as appropriate) etiology/pathogenesis of lesions, location of lesions, medical options and course of the illness, diagnostic tests, inheritance sample and genetic mechanism, gross pathology, microscopic pathology · Huntington illness · Parkinson illness; parkinsonism syndrome · Wilson illness three. Diseases with spinal twine and/or cerebellum involvement: For each of the next ailments, describe (as appropriate) etiology/pathogenesis of lesions, location of lesions, medical options and course of the illness, diagnostic tests, inheritance sample and genetic mechanism, gross pathology, microscopic pathology · Amyotrophic lateral sclerosis · Friedreich ataxia 4. Prion ailments: · Discuss traits and replication mechanism (conformational change) of the "prion," the agent in transmissible spongiform encephalopathies. General ideas Degenerative ailments are characterized by progressive neuronal degeneration and loss in disease-specific areas.
Trusted cefpodoxime 100 mg
In addition to consuming calcium-fortified soy products, low-oxalate inexperienced greens such as cabbage, spring greens and kale have greater calcium bioavailability (4961%) and ought to be consumed frequently by vegans [10]. Phytate, soy protein and polyphenols/tannins can inhibit iron absorption, while several of} nutrients, together with vitamin C, retinol and carotenes, can improve the Vegetarian Diets 137 wrn367873. Dietary recommendation should encourage a variety of|quite so much of|a wide selection of} non-haem iron sources (as shown in table 2) and vitamin C with meals to assist iron absorption. Food preparation methods such as soaking beans prior to cooking and fermenting soy protein. Zinc Zinc deficiency may cause failure to thrive and impaired taste acuity in children [11, 12]. The major sources of zinc in vegetarian diets embody cereals and grains, which are additionally high in phytate and cut back zinc bioavailability [10]. Differences in zinc intake between vegetarian and omnivorous children are negligible [11]. However, the ratio of phytate to zinc intake is far higher in vegetarian children, which might enhance the danger of suboptimal zinc status especially in periods of rapid progress [11, 12]. Little is understood regarding the effects of marginal zinc deficiency on childhood progress and improvement, although adaptation to a low intake could occur over time with increased intestinal absorption [11]. Conclusions · Vegetarian diets can provide sufficient nutrients for optimum progress and improvement in childhood. However, a broad range of vegetarian dietary patterns are sometimes practiced, and while many parents invariably want their offspring to share their eating sample, some diets too nutritionally restrictive for infants and younger children to thrive · Variety in particular person vegetarian diets is paramount to achieve the steadiness of nutrients to support every stage of improvement in childhood. Malnutrition is outlined as a deviation from the conventional state of nutrition; might possibly} logically be either undernutrition or overnutrition (overweight and obesity). A deficiency in proper nutritional elements due to of} any trigger results in undernutrition. Undernutrition is a broad term starting from restricted intrauterine progress, low start weight, stunting, wasting and underweight to micronutrient deficiencies. It is the outcome result} of suboptimal dietary intake, metabolic stress, malabsorption and increased nutrient demands. In the context of lowand middle-income countries, where overnutrition is comparatively much less prevalent, malnutrition generally implies stunting, wasting and/or underweight. Primary malnutrition in children is most commonly seen in low- and middle-income countries. The factors liable for major malnutrition embody household food insecurity, poverty, poor nutrition of ladies during pregnancy, intrauterine progress restriction, low start weight, poor breastfeeding and inappropriate complementary feeding, frequent infectious sicknesses, poor quality of water, sanitation and hygiene, and so on. The problem of major malnutrition is, subsequently, largely social somewhat than biomedical in origin. There is an increased accumulation of inflammatory cells in the small intestinal mucosa, the intestinal villi are broken and distorted by the inflammatory course of, and, consequently, they malabsorb nutrients, which results in|which leads to|which finally ends up in} malnutrition. Secondary malnutrition, in contrast, outcomes from an underlying disease that compromises progress immediately or via its deleterious effect on urge for food or the absorption of nutrients. Infectious sicknesses result in malnutrition by reducing the intake of nutrients and their bioavailability, by rising nutrient and vitality expen- diture and by diverting nutrients away from progress. In patients with intensive burns, increased catabolism, anorexia and lack of plasma proteins from the exposed pores and skin surfaces result in malnutrition. The major cause of malnutrition seen in developed countries is secondary malnutrition. If not recognized early on, or if left untreated, secondary malnutrition will increase the danger of infection, delayed wound or burn therapeutic and an general poor response to therapy of the underlying trigger. Table 1 lists frequent situations that may result in secondary malnutrition, although not all of them are generally seen in developed countries. The estimated variety of underweight children (weight-for-age Z rating <2) globally is 101 million or 16%. Wasting impacts 52 million children <5 years of age, which is 8% of all children of that age group. It has been estimated that fetal progress restriction, stunting, wasting and deficiencies in vitamin A and zinc along with suboptimal breastfeeding trigger 3. The general dangers of mortality from any trigger (diarrhea, pneumonia, malaria or measles) for extreme stunting, extreme wasting and extreme underweight are four. Among those that survive, impaired intellectual or cognitive and motor de- 140 Shahrin Chisti Ahmed wrn367880. Diseases or situations that may trigger secondary malnutrition in children Infectious causes Diarrhea, dysentery, persistent diarrhea (continuing for 14 days) Repeated episodes of acute respiratory infection Tuberculosis Helminthiasis Measles Malaria Kala azar (leishmaniasis) Human immunodeficiency virus infection Noninfectious causes Low start weight Burns Chromosomal issues. Length for age at 2 years is associated with better cognitive scores in later childhood (0. The high prevalence of stunting among children <5 years of age in Africa (36% in 2011) and Asia (27% in 2011) remains a pervasive public health problem. The prevalence of stunting is slowly decreasing globally, but the absolute variety of children affected has increased in Africa. Poverty and food insecurity constrain the accessibility of nutritious diets that have a high protein quality, sufficient micronutrient content material and bioavailability, essential fatty acids, low antinutrient content material and high nutrient density [8]. In addition to these determinants, other factors such as unplanned ur- Based on anthropometric measurements, malnutrition may be categorized as stunting, wasting and underweight. Height or length for age is useful for assessing stunting, which is outcome of|the outcomes of} persistent malnutrition. Weight for height or length is used for assessing wasting, which is outcome of|the outcomes of} acute malnutrition. Weight for age measures underweight, indicating the mixed effect of acute and persistent malnutrition (table 2). Framework of the relations between poverty, food insecurity and other underlying and immediate causes of maternal and baby undernutrition and their short- and long-term consequences. Management Management of malnutrition is dependent upon by} the type of|the sort of} malnutrition, identification of its trigger, if applicable, and its severity. This includes nutrition-specific interventions such as counseling of oldsters on the proper food plan to be given to the child, with emphasis on continued breastfeeding and applicable complementary feeding, micronutrient supplementation, period- ic deworming, and so on. Ideally, these children should receive 25 kcal/kg per day of vitality in extra of what their wholesome peers get, and their diets should contain animal-source foods which are wealthy in essential fatty acids and micronutrients together with vitamin A, iron and zinc [9]. For the control of stunting, nutrition-sensitive interventions ought to be scaled up on the national or regional stage. These embody making certain household food safety, safe water, proper sanitation and sufficient hygiene, female edu- 142 Shahrin Chisti Ahmed wrn367880. The effects of stunting on the creating mind irreversible after the age of 34 years. Efforts should subsequently be taken to implement the nutrition interventions at an early age so that stunting and its adverse effects on cognition are reversed. Growth monitoring and promotion packages ought to be implemented on the neighborhood stage, where the nutritional status of infants and younger children is assessed each 13 months and their progress is promoted via counseling of the parents. Complications embody extreme diarrhea, dysentery, hypoglycemia, hypothermia, pneumonia, urinary tract infection, septic sickness or any danger sign as per the Integrated Management of Childhood Illness guidelines [unable to drink or breastfeed, vomits every thing, has had convulsions (>1 or extended for >15 min), lethargy or unconsciousness or presently convulsing]. The line of administration for this stabilization phase of therapy of issues is as follows [10]: · Treat hypoglycemia, which is frequent in these children, with oral or intravenous glucose if the child is lethargic, unconscious or convulsing · Treat and prevent hypothermia by preserving the child heat · Treat shock, if current, with oxygen therapy, intravenous fluids and glucose and broadspectrum antibiotics · Treat and prevent dehydration. It is tough to estimate the dehydration status of a severely malnourished baby. All children with watery diarrhea ought to be assumed to have dehydration and given the next: each 30 min for the first 2 h, ReSoMal at 5 ml/kg body weight orally or by nasogastric tube; then, in alternate hours for up to as} 10 h, ReSoMal at 510 ml/kg/h (the amount to be given ought to be determined by how a lot the child desires nicely as|in addition to} by stool loss and vomiting). The liquid food, F-75, is given in alternate hours during this era till the child is rehydrated. Severe diarrhea may be due to of} cholera or rotavirus infection and is often outlined as stool output >5 ml/kg/h · Treat and prevent infection. If the child fails to enhance clinically by forty eight h or deteriorates after 24 h, a third-generation cephalosporin. Where particular infections are recognized, add particular antimicrobials as applicable · Start careful feeding. During the nutritional rehabilitation phase, feeding is progressively increased to achieve a rapid weight gain of >10 g/kg/day.
Proven 200mg cefpodoxime
These Clin J Am Soc Nephrol 10: 676687, April, 2015 Integrated Control of Sodium Transport, Palmer and Schnermann 685 9. J Cell Sci 115: 49694976, 2002 Muto S, Hata M, Taniguchi J, Tsuruoka S, Moriwaki K, Saitou M, Furuse K, Sasaki H, Fujimura A, Imai M, Kusano E, Tsukita S, Furuse M: Claudin-2-deficient mice are faulty within the leaky and cation-selective paracellular permeability properties of renal proximal tubules. J Cell Sci 123: 19131921, 2010 Schnermann J, Huang Y, Mizel D: Fluid reabsorption in proximal convoluted tubules of mice with gene deletions of claudin-2 and/or aquaporin1. Clin J Am Soc Nephrol 2014, in press Schnermann J, Castrop H: Function of the juxtaglomerular equipment: management of glomerular hemodynamics and renin secretion. Structural and practical effects of dietary salt consumption and continual diuretic infusion. J Clin Invest 49: 18151826, 1970 Imai M, Yoshitomi K: Electrophysiological examine of inside medullary collecting duct of hamsters. Am J Physiol 250: F963F966, 1986 Erlij D: Basic electrical properties of tight epithelia determined with a simple technique. J Clin Invest forty four: 14101416, 1965 Schnermann J, Wahl M, Liebau G, Fischbach H: Balance between tubular flow price and internet fluid reabsorption within the proximal convolution of the rat kidney. Dependency of reabsorptive internet 686 Clinical Journal of the American Society of Nephrology 52. Am J Physiol 236: F163F174, 1979 Burg M, Patlak C, Green N, Villey D: Organic solutes in fluid absorption by renal proximal convoluted tubules. Am J Physiol 243: F1F11, 1982 Briggs J: A simple steady-state model for suggestions management of glomerular filtration price. Am J Physiol 255: F1256F1268, 1988 Kaissling B, Le Hir M: Functional morphology of kidney tubules and cells in situ. J Biol Chem 273: 2915029155, 1998 Clin J Am Soc Nephrol 10: 676687, April, 2015 Integrated Control of Sodium Transport, Palmer and Schnermann 687 ninety five. Intersalt Cooperative Research Group: Intersalt: An worldwide examine of electrolyte excretion and blood pressure. Am J Physiol 256: F179F186, 1989 Maack T: Role of atrial natriuretic think about volume management. Zeidel Abstract Alterations in water homeostasis can disturb cell measurement and function. Although most cells can internally regulate cell volume in response to osmolar stress, neurons are significantly at risk given a mix of complicated cell operate and area restriction throughout the calvarium. Through specialised neuronal "osmoreceptors" that sense changes in plasma osmolality, vasopressin launch and thirst are titrated have the ability to} obtain water steadiness. Fine-tuning of water absorption happens along the collecting duct, and unique structural modifications of renal tubular epithelium that confer extensive range|a variety} of water permeability. In this article, we review the mechanisms that ensure water homeostasis as well as|in addition to} the basics of issues of water steadiness. Instead of discarding their now pointless pressure filters and redesigning their kidneys as efficient secretory organs, the terrestrial vertebrates modified and amplified their existing techniques to salvage the dear water of the filtrate. Marine animals survive within the high tonicity of seawater (5001000 mOsm/kg) by way of selection of|quite lots of|a wide range of} mechanisms. The shark maintains a high tonicity in its body fluids (2,3), whereas dolphins take in water from foodstuffs whereas producing a highly concentrated urine by way of complicated multilobed reniculate kidneys (4). Water is essentially the most ample part of the human body, constituting approximately 50%60% of body weight. Cell membranes, which define the intracellular compartment, and the vascular endothelium, which defines the intravascular part, are both water permeable. Because the intracellular area constitutes the largest body compartment, holding approximately two thirds of body fluid, changes in water homeostasis predominantly affect on} cells; water excess leads to mobile swelling, and water deficit leads to mobile shrinkage. For every 1 liter of water change, approximately 666 ml affect on} the mobile area, with solely about one hundred ten ml affecting the vascular area. Although cells have an innate capability to respond to changes in cell volume when extracellular osmolality changes, the body protects cells primarily by tightly 852 Copyright © 2015 by the American Society of Nephrology regulating extracellular osmolality. The amount of body water remains remarkably stable despite a huge range of water consumption and massive number} of routes for water loss, including the respiratory and gastrointestinal tract, skin, and the kidneys. Maintaining Brain Cell Size With a plethora of capillaries descending by way of the subarachnoid area into the parenchyma, the mind is remarkably vascular. Astrocytes, star-shaped neuronal cells, encapsulate the capillaries, forming a "blood-brain barrier" and controlling many essential neurologic capabilities. Because the quantity of intracellular water affects the focus of intracellular contents and cell measurement, changes in osmolality can disturb the complicated signaling community that orchestrates cell operate. Given the complexity of mind operate, even minor changes in neuron ionic composition and measurement can have profound effects on the processing and transmission of neuronal alerts. Consequently, the mind has developed complicated osmoregulatory mechanisms to defend towards changes in plasma osmolality. Penetrating capillaries descend by way of the subarachnoid area into the parenchyma, and are encased by astrocytes, which in addition to controlling essential neurologic capabilities, kind the blood-brain barrier. In the setting of hypotonicity, as shown in Figure 2, the rapid swelling of the cell activates quiescent cell membrane channels and leads to immediate Cl2, K1, and attendant water loss, a process termed regulatory volume lower. Over the next 24 hours, the cells lose further natural solutes, corresponding to myo-inositol, and amino acids, corresponding to glutamine, glutamate, and taurine. With hyperosmolar-induced cell shrinkage, mind cells respond with immediate uptake of surrounding Na1, K1, and Cl2, correcting cell volume in a process termed regulatory volume increase (12). With extra prolonged exposure, natural solute concentrations throughout the cells rise, changing the high levels of ions. Despite these essential cell protective mechanisms, alterations in plasma osmolality can have disastrous penalties. The traditional neurologic signs of hypo-osmolality, including headache, nausea, vomiting, and if extreme sufficient, seizures, are typically thought to occur at a serum sodium 854 Clinical Journal of the American Society of Nephrology Figure 2. In this determine, a standard cell is challenged by either a hyperosmolar (left) or hypo-osmolar (right) milieu. In the setting of hyperosmolar stress, whereby the cell shrinks with water egress, neurons then respond by rapidly accumulating Na1, K1, and Cl2 ions, followed by the manufacturing of intracellular natural solutes. The increase of intracellular solute content material then draws water in to normalize the concentrations across the cell membrane, thereby restoring cell measurement. In the setting of hypo-osmolarinduced swelling, activation of K1 and Cl2 channels, as well as|in addition to} the K1-Cl2 cotransporter, lead to solute and consequent water loss, thereby restoring cell volume. More mild changes of plasma osmolality are additionally associated with neurologic signs, including gait instability, reminiscence impairment, and cognitive decline. Children are thought-about at increased threat of hypo-osmolar encephalopathy, presumably because of the comparatively larger mind to intracranial volume compared with adults (13). Conversely, because of|as a end result of} the mind begins to atrophy within the sixth decade, aged individuals at a decrease threat of extreme issues from acute hyponatremia. In addition to age, sex thought-about an essential determinant of neurologic sensitivity. The overwhelming majority of reported cases of postoperative hyponatremia resulting in deadly outcomes have been in women (14), including postpartum and postmenopausal women (15). Unlike the mind swelling associated with hypo-osmolality, the mind shrinks in hypertonic conditions. The protective reflex of intense thirst may disappear as hypertonicity worsens, changed by somnolence, confusion, and muscle weak point (16). If extreme sufficient, the shrinking mind will draw back from the calvarium, tearing the rich capillary plexus, and causing subarachnoid hemorrhage, cerebral bleeding, and death. The highest reported serum sodium within the adult literature remains 255 mEq/L, a consequence of ingesting salty water as half of} a deadly exorcism ritual (17). Presumably the use of of} table salt as a common antiemetic, deadly salt ingestion, either by accident or voluntarily, is well reported (18), as is unintended iatrogenic administration (19). In summary, despite inner mobile mechanisms to defend cell volume, cells stay at risk with alterations of water steadiness; consequently, stopping vital changes in plasma osmolality is crucial for survival. Sensing Changes in Body Concentration: the Osmoreceptor the ability to internally sense plasma osmolality is prime to the method of water homeostasis. Much progress in explaining the mechanisms of the "osmoreceptor" has been made, as reviewed by Sharif-Naeini et al. Electrophysiologic recordings from supraoptic nuclei of the hypothalamus in rats show an growing price of mobile depolarization in response to water deprivation (26), and a reducing price with water administration (27). More latest studies have shown that hyperosmolality causes osmoreceptor membrane depolarization by way of activation of nonselective calcium-permeable cation channels.
Syndromes
- Para-aminosalicylic acid
- Skin diseases that block sweat glands
- Slurred speech
- Blood clots or swelling in the veins
- Joint pain
- Sarcoma
Proven cefpodoxime 200 mg
Culture-specific problems the need for a separate class for problems similar to latah, amok, koro, and a variety of|quite a lot of|a wide selection of} different possibly culture-specific problems has been expressed much less usually current years|in current times|lately}. Descriptions of these problems at present out there in the literature suggest that they might be considered native variants of hysteria, despair, somatoform dysfunction, or adjustment dysfunction; the closest equal code should therefore be used if required, together with an additional observe of which culture-specific dysfunction is concerned. There may be prominent elements of attention-seeking behaviour or adoption of the sick position akin to that described in F68. Its inclusion is a recognition of the very real sensible problems in lots of} creating international locations that make the gathering of particulars about many circumstances of puerperal sickness just about inconceivable. The difference between observations and interpretation turns into significantly troublesome when attempts are made to write detailed tips or diagnostic standards for these problems; and the number of standards that must be fulfilled earlier than a prognosis is considered confirmed stays an unsolved problem in the gentle of present data. Nevertheless, the attempts that have been made to specify tips and standards for this class could help to show that model new} strategy to the description of personality problems is required. After preliminary hesitation, a brief description of borderline personality dysfunction (F60. Since these are, strictly talking, problems of position or sickness behaviour, it should be handy for psychiatrists to have them grouped with different problems of adult behaviour. The crucial difference between the first two and malingering is that the motivation for malingering is apparent and usually confined to situations where personal danger, legal sentencing, or giant sums of cash are concerned. Such a system must be developed separately, and work to produce appropriate proposals for international use is now in progress. While some uncertainty stays about their nosological status, it has been thought of that enough data is now out there to justify the inclusion of the syndromes of Rett and Asperger on this group as specified problems. Overactive dysfunction associated with psychological retardation and stereotyped actions (F84. The use of this prognosis signifies that the standards for both hyperkinetic dysfunction (F90. These few exceptions to the general rule were thought of justified on the grounds of scientific comfort in view of the frequent coexistence of these problems and the demonstrated later significance of the mixed syndrome. There is, nonetheless, a cautionary observe recommending its use mainly for younger kids. This is due to the persevering with need for a differentiation between kids and adults with respect to numerous types of morbid anxiousness and associated emotions. The frequency with which emotional problems in childhood are followed by no significant comparable dysfunction in adult life, and the frequent onset of neurotic problems in adults are clear indicators of this - 21 - need. In different phrases, these childhood problems are significant exaggerations of emotional states and reactions may be} considered normal for the age in query when occurring in only a light kind. If the content of the emotional state is uncommon, or if it occurs at an uncommon age, the general classes elsewhere in the classification should be used. A number of classes that will be used frequently by baby psychiatrists, similar to consuming problems (F50. Nevertheless, scientific features particular to childhood were thought to justify the extra classes of feeding dysfunction of infancy (F98. This contains syndromes with predominantly physical manifestations and clear "organic" etiology, of which the Kleine-Levin syndrome (G47. It was determined that the least unsatisfactory solution was to use the final class in the numerical order of the classification, i. Decisions on whether to accept or reject proposals were influenced by a number of|numerous|a variety of} components. Some different proposals had clear advantage, but extra research could be needed earlier than they thought of for international use. A number of these proposals included in early variations of the general classification were omitted from the final version, including "accentuation of personality traits" and "hazardous use of psychoactive substances". It is hoped that research into the status and usefulness of these and different revolutionary classes will proceed. The dysfunction may be be} primary, as in illnesses, injuries, and insults that result on} the mind instantly or with predilection; or secondary, as in systemic illnesses and problems that assault the mind only as one of the multiple of} organs or methods of the body concerned. Alcohol- and drug-caused mind problems, although logically belonging to this group, are categorized under F10-F19 due to sensible benefits in maintaining all problems as a result of} psychoactive substance use in a single block. Although the spectrum of psychopathological manifestations of the conditions included right here is broad, the essential features of the problems kind two major clusters. On the one hand, there are syndromes in which the invariable and most prominent features are both disturbances of cognitive capabilities, similar to reminiscence, mind, and learning, or disturbances of the sensorium, similar to problems of consciousness and attention. On the other hand, there are syndromes of which essentially the most conspicuous manifestations are in the areas of notion (hallucinations), thought contents (delusions), or mood and emotion (depression, elation, anxiety), or in the total sample of personality and behaviour, whereas cognitive or sensory dysfunction is minimal or difficult to ascertain. The latter group of problems has much less safe footing on this block than the former end result of|as a outcome of} it contains many problems may be} symptomatically just like conditions categorized in different blocks (F20-F29, F30-F39, F40-F49, F60-F69) and are identified to occur without gross cerebral pathological change or dysfunction. However, the growing proof that a variety of|quite a lot of|a wide selection of} cerebral and systemic illnesses are causally associated to the occurrence of such syndromes offers enough justification for his or her inclusion right here in a clinically oriented classification. The majority of the problems on this block can, a minimum of|no much less than} theoretically, have their onset at any age, besides perhaps early childhood. While a few of these problems are seemingly irreversible and progressive, others are transient or reply to at present out there remedies. In the present context, the term "organic" means simply that the syndrome so categorized may be attributed to an independently diagnosable cerebral or systemic illness or dysfunction. The term "symptomatic" is used for these organic psychological problems in which cerebral involvement is secondary to a systemic extracerebral illness or dysfunction. It follows from the foregoing that, in the majority of circumstances, the recording of a prognosis of any one of the problems on this block will require the use of of} two codes: one for the psychopathological syndrome and one other for the underlying dysfunction. Dementia - 45 - A general description of dementia is given right here, to point out the minimal requirement for the prognosis of dementia of any type, and is followed by the standards that govern the prognosis of extra particular varieties. Impairments of cognitive perform are generally accompanied, and sometimes preceded, by deterioration in emotional control, social behaviour, or motivation. In assessing the presence or absence of a dementia, particular care should be taken to avoid false-positive identification: motivational or emotional components, significantly despair, along with motor slowness and general physical frailty, somewhat than loss of intellectual capacity, could account for failure to perform. Dementia produces an considerable decline in intellectual functioning, and usually some interference with personal activities of daily living, similar to washing, dressing, consuming, personal hygiene, excretory and toilet activities. How such a decline manifests itself will rely largely on the social and cultural setting in which the patient lives. The impairment of reminiscence sometimes affects the registration, storage, and retrieval of new data, but beforehand discovered and familiar material may be lost, significantly in the later phases. The processing of incoming data is impaired, in that the person finds it increasingly difficult to attend to a couple of stimulus at a time, similar to collaborating in a conversation with a number of} individuals, and to shift of consideration from one topic to one other. If dementia is prognosis, proof of clear consciousness is - forty six - required. However, a double prognosis of delirium superimposed upon dementia is common (F05. The above signs and impairments should have been evident for a minimum of|no much less than} 6 months for a confident scientific prognosis of dementia to be made. Consider: a depressive dysfunction (F30-F39), which can exhibit lots of the features of an early dementia, particularly reminiscence impairment, slowed thinking, and lack of spontaneity; delirium (F05); gentle or reasonable psychological retardation (F70-F71); states of subnormal cognitive functioning attributable to a severely impoverished social surroundings and limited training; iatrogenic psychological problems as a result of} treatment (F06. Dementia could follow any other organic psychological dysfunction categorized on this block, or coexist with some of them, notably delirium (see F05. It is usually insidious in onset and develops slowly but steadily over a interval of years. This interval may be as quick as 2 or three years, but can sometimes be significantly longer. In circumstances with a later onset, the course tends to be slower and to be characterised by extra general impairment of upper cortical capabilities. There are characteristic changes in the mind: a marked discount in the inhabitants of neurons, significantly in the hippocampus, substantia innominata, locus ceruleus, and temporoparietal and frontal cortex; appearance of neurofibrillary tangles made from paired helical filaments; neuritic (argentophil) plaques, which consist largely of amyloid and present a particular progression of their development (although plaques without amyloid are also identified to exist); and granulovacuolar our bodies. Neurochemical changes have also been discovered, including a marked discount in the enzyme choline acetyltransferase, in acetylcholine itself, and in different neurotransmitters and neuromodulators. As initially described, the scientific features are accompanied by the above mind changes. Diagnostic tips the following features are essential for a particular prognosis: - 47 - (a) Presence of a dementia as described above.
Order 200mg cefpodoxime
The embryologicalfacts also accountedfor the determination of handedness; truth that|the truth that} the vast majority of} people are right-handedwould be one other results of the earlier maturation of the left hemisphere. It had been identified that language was not alwaysdisturbedif illness childhood or congenitalmalformations in of the nervous system affected the left hemisphere in adolescence. Broca identified that these patients had been often left-handed, implying that the best hemispherehad taken over management both of handedness and language. From these observations and inferences, Broca suggestedthat restoration from aphasiamight be possibleif the best hemispherecould take over the features normally completed the left. He concludedthat the failure of by most patients with aphasiato recover was outcome of} inadequaterehabilitative efforts: he thought that adequaterehabilitation would have to consistof as much publicity to languageas a baby learning a first languagehas along with his mother, somethingthat is hardly ever offered. Finally, he identified that the flexibility of aphasicpatientsto understandlanguage indicatedthat the best hemisphere dld perform in the broader psychology of language, which involves the establishmentof relationshipsbetween expressions and meanings; the dominance of the left hemispherewas for speechalone. As will turn into apparent, most of these conclusions- that the left hemisphere is dominant for expressivelanguage, that that is linked to handedness, that restoration from aphasiamay contain the best hemisphere, that there are developmentalembryologicaldifferencesbetween the hemispheres, and that the best hemisphere has the capability for receptive language are nonetheless very much accepted right now, with some refinements and on the basisof extra evidence. For some fifty years after Broca, till World War I, the research of language issues was a central part of of} clinical neurology, and just about every essential academicneurologist in Europe revealed papers on the ropic. The description of the gross neuroanatomyof the languageareas,and the forty seven Il Clinical aphasiology and neurolinguistics clinical classificationof aphasiasin use right now, had been the results of the concentratedactivity which adopted Broca. By the time Wernicke revealed the seminal article which led to the productive "connectionist" schoolof aphasiology 1874,Broca had bowed in out of the field. He did journey to England in 1866 to discusshis work at a conference, which was also attended by Hughlings Jackson; the two males disagreed,and Broca is claimed to have carried the day. Indeed, his work on aphasia was first discussedat the Anthropological Society which he had based, and was a results of his curiosity in the relationship between mind size and the mental capacitiesof completely different speciesand human races (a controversialtopic, then as now). First, the connectionists discoveredother aphasic related to lesions elsewhere in the mind. From 1861 on, the neurological literature was crammed and, extra with casereports of aphasicpatients,often adopted by autopsies, patients with a variety of|quite lots of|a big selection of} psychological,intellecgenerally,with reviews of tual, and complex perceptual problems accompaniedby autopsiesof the mind. The most illustrious neurologistsof the day revealed paperson the subjectof aphasia. No unified principle relating all of the observations was obtainable,nevertheless, and the field grew to become"information wealthy and on the aphasias by that might not theorypoor", characterised many interestingobservations singleframework. His paper constitutesthe third nice discoveryof nineteenththe discovery that there were quantity of} sub-typesof century aphasiologists: forty nine ll Clinical aphasiology and neurolinguistics aphasic syndromes, every of which resulted from lesions in different areas of the mind. One implication of this discoveryis that languagerepresentation and processing by the mind is such that completely different areas accomplish completely different tasks. On the premise of those instances,Wernicke set forth a mannequin of languagerepresentationand processing the mind, consistent psychologyand the in with the associationist neurophysiologicaltheory of reflexesof his day. Wernicke describednine ofthe mind, ofwhich the oflanguage disordersdue to acquireddisease instances had been cases an first two had been the basisfor his principle. In both aphasic instances,the patients had a marked deficit in understandingwhat was said to them. The secondpatient, in fact, was originally thought to be deaf, because of she manifestedno consciousness what other people had been sayingto her; but it quickly grew to become apparent that she was not deaf, however simply unable to perceive language. Patientswith anterior lesionsfrequently omitalways halting and ted many words, and often showeda nice deal of issue in pronunciation of particular person sounds. In both instances,the patients spoke fluently and maintained normal intonational patterns, however had been unable to make sense. Insteadof sayinga particularword, his patients would possibly say a word which was related both by advantage of rhyme (or some other aspectof its sound), or by advantage of some semanticrelationship. Wernicke and the other examinerswere frequently at a loss to understandwhat the patients had been trying to say. It showeda cerebral infarct (a stroke) in the area of the first temporal gyrus on the left, occupying approximately the middle third of the gyrus and lengthening posteriorly towards of|in path of} the parietal lobe (Figure 4-1). Wernicke identified First, it was an that this space of cortex had two essential traits. Second, it was an space which itself was neither a main sensory nor a main motor space. It was certainly one of quantity of|numerous|a variety of} areascalled "affiliation" areas, thought to be concerned in more advanced elaborationand modification of sensoryand motor data. In the a specificsite in the cerebrarhemisphere connectionistliterature,thistriadmoreorlessdelinesa. Thereare features are absent in a postulated casesin which one or one other of those notion of a middle involves the triple center, however. Input, output, and connecting pathways are i n d i c a t e di n s c h e m a t i cf o r m. He insistedthat the components of the mannequin and their interaction be justified not only by the facts of aphasia, but also by the facts of normal physiology and psychology. In the first case, he pointed to the work of his instructor Meynert, which established that sensory-to-motorflow of excitation was concerned in reflex motion, and he argued that languagecould be seenas an especially advanced modulatedreflex. As far as consistency with normal psychologywas involved,Wernicke instructed that identical old} method a baby learns languagewas by imitating the language that he heard locally, and that the first vocalized utterances required a transmission of linguistic data from the auditory receptiveareas,through their affiliation cortex, to the constructions in the anterior portion of the mind which had been concerned in controlling the fifty three ll Clinical aphasiology qnd neurolinguktics vocal tract. Becauseof this ontogeneticfactor, Wernicke thought that the auditory-to-motor processof data flow was a reasonablefeature of any mannequin of normal talking. Wernicke instructed that this pathway lay in to the cortex, and that it was cheap think of the gray matter across the Sylvian fissure as constituting a single gyrus related to language,with an auditory, sensorypole in the temporal portion and a speech,motor pole in the frontal portion. Wernicke instructed that the aphasiathat can be producedby a lesionof the intervening parts of this grey matter can be characterizedby an dysfunction just like that seenwith posterior lesions(because the expressive of interruption of the flow of knowledge from auditory to motor areas), however that the abilities of such patients to perceive spoken language would stay intact (because the associationarea in which auditory representhat, generally, there tations had been saved was itself intact). He instructed causedby lesionsof centers,and the was a differencebetween the aphasias aphasias causedby lesionsof connectingpathways. Wernicke realizedthat unlessone placed some restriction on what could be be} a middle and on the variety of centers, every new form of aphasiacould be describedby the postulation of a brand new} center, the role of which was the normal efficiency of exactly the languagecapacitywhich was disturbedin a particularpatient. Suchmultiplication of centersand connectingpathwayscould not Ieadto a testabletheory of of the representationand processing languagein the mind. He also made one more restrictionwith respect t o the c e n t e r s:t h a t the y b e " s i m p l e ". Wernicke was opposed to the localization of advanced and complicated psychological functionsin specificareasof the mind which had characterised the phrenologicalapproachto cerebrallocalization. In its place,he adopted restricted notion of what could be be} localized, and thought that fifty four sicsl co nnectio nist mo dels C las many features resulted from connecting numerous mind components. These examplesare the best clues to what he meant by the notion of a "simple" psychological perform. His method grew to become "connectionist", advanced features had been built up by connecting "simple" as a result of|as a outcome of} components. By 1885, it had turn into the dominantway of approachingthe drawback of classifying aphasicdisordersof language. This method is properly exemplified by a paper by Lichtheim, publishedin German in 1884and in English in the influential journal Brain in l8{t5,which set forth a proposalfor a completeenumerationof all aphasic syndromesbased upon a connectionistmodel of languageand the mind. He thoughtthat the first was concerned in speechproduction, and believedthat it essential utterances. In addition, he instructed that therewas a "concept space", labeledB in the diagram,which he thought was fifty five DoubleDoubl click on right here eto edit click on text. Subcorticalmotor aphasia,outcome of} a lesion between M and the oral musculature, produces a dysarthria - a disturbance articulation. Lichtheim also argued that clinical evidence supportedthe existence a separate of areafor the representation of the motor sequences concerned in writing. Rather, there wasan additionalnecessary enter from the middle M, the storehouse the for representationof the oral motor sequencesof particular person words. As Wernicke had accomplished, Lichtheim attempted to provide principled explanations for the functioning of the components of his mannequin. Lichtheim realizedthat this descriptionof completely different syndromesas a results of completely different lesionscould be consideredan advert hoc aspectof the speculation, and he due to this fact tried to present that the same analysiswas also true of written language. Given that written languagedependedupon the correct fr,rnctioning of the middle E after its reception of some form of relevant data from center M, there nonetheless remained the question of whether or not the auditory that the instances of form of words was concerned in writing. If the patients developedparaphasicwriting (sometimes referred to as "paragraphia"), then the pathways for properly activating E would E be in duplicate: there can be a pathway B+ A+ M-+ and a separate pathway B -+M -+E. A lesionof the first of thesetwo pathwayswould lead M to paragraphia,in exactly the sameway that a lesionin the tract A -+ led Finally, if conduction aphasics needed to paraphasiain the posterior aphasias. This quite advanced hypothetical reasoning demonstrates the serious effort on the part of of} Lichtheim (and the other members of the connectionistschool)to make the predictionsof their modelsexplicit, and to characterizein as principled a method as possiblethe observabledifferences fifty eight Classical connectio nist mo dels betweenperformancesin a given psycholinguistic perform in different subtypesof aphasia.
100mg cefpodoxime
Preganglionic sympathetic fibers are proven in solid red, and postganglionic sympathetic fibers are proven in interrupted red. Below, the 2 trunks finish by joining collectively to kind a single ganglion, the ganglion impar. Efferent Nerve Fibers (Craniosacral Outflow) the connector nerve cells of the parasympathetic part of of} the autonomic nervous system are located in the brainstem and the sacral segments of the spinal twine. Those nerve cells located in the brainstem kind nuclei in the following cranial nerves: the oculomotor (parasympathetic or Edinger-Westphal nucleus), the facial (superior salivatory nucleus and lacrimatory nucleus), the glossopharyngeal (inferior salivatory nucleus), and the vagus nerves (dorsal nucleus of the vagus). The axons of those connector nerve cells are myelinated and emerge from the brain inside the cranial nerves. The sacral connector nerve cells are found in the gray matter of the second, third, and fourth sacral segments Parasympathetic Part of the Autonomic System the actions of the parasympathetic part of of} the autonomic system are directed toward conserving and restoring energy. The heart rate is slowed, pupils are constricted, peristalsis and glandular exercise is elevated, sphincters are opened, and the bladder wall is contracted. The myelinated axons go away the spinal twine in the anterior nerve roots of the corresponding spinal nerves. The myelinated efferent fibers of the craniosacral outflow are preganglionic and synapse in peripheral ganglia located close to the viscera they innervate. The cranial parasympathetic ganglia are the ciliary, pterygopalatine, submandibular, and otic. In sure locations, the ganglion cells are positioned in nerve plexuses, such because the cardiac plexus, pulmonary plexus, myenteric plexus (Auerbach plexus), and mucosal plexus (Meissner plexus); the final two plexuses are associated with the gastrointestinal tract. Characteristically,the postganglionic parasympathetic fibers are nonmyelinated and of comparatively brief length in contrast with sympathetic postganglionic fibers. The ratio of preganglionic to postganglionic fibers is about 1:3 or much less, which is much more restricted than in the sympathetic part of of} the system. Ganglia are situated alongside the course of efferent nerve fibers of the autonomic nervous system. Sympathetic ganglia kind part of of} the sympathetic trunk or are prevertebral in place. Parasympathetic ganglia, the opposite hand|however|then again}, are situated close to or inside the walls of the viscera. An autonomic ganglion consists of a group of multipolar neurons together with capsular or satellite cells and a connective tissue capsule. Nerve bundles are attached to each ganglion and include preganglionic nerve fibers that enter the ganglion, postganglionic nerve fibers that have arisen from neurons inside the ganglion and are leaving the ganglion, and afferent and efferent nerve fibers that pass by way of the ganglion with out synapsing. The preganglionic fibers are myelinated, small, and comparatively slowconducting B fibers. The postganglionic fibers are unmyelinated, smaller, and slower-conducting C fibers. The structure of synapses in autonomic ganglia exhibits the attribute membrane thickening and small clear vesicles. The smaller vesicles comprise acetylcholine; the content material of the granular vesicles is unknown. Although an autonomic ganglion is the site the place preganglionic fibers synapse on postganglionic neurons, the presence of small interneurons has been recognized. In some ganglia, these interneurons obtain preganglionic cholinergic fibers, they usually might modulate ganglionic transmission. In other ganglia, they obtain collateral branches and will serve some integrative operate. Afferent Nerve Fibers Afferent myelinated fibers travel from the viscera to their cell bodies, located both in the sensory ganglia of the cranial nerves or in the posterior root ganglia of the sacrospinal nerves. The central axons then enter the central nervous system and participate in the formation of local reflex arcs or pass to larger centers of the autonomic nervous system, such because the hypothalamus. The afferent component of the autonomic system is identical to the afferent component of somatic nerves, and it forms part of of} the general afferent section of the entire nervous system. The nerve endings in the autonomic afferent component may not be not|will not be} activated by such sensations as heat or touch however somewhat by stretch or lack of oxygen. When the wave of excitation reaches the synaptic contacts, the synaptic transmitter is liberated, crosses the synaptic cleft to attain the receptor,and excites the postganglionic neuron. The synaptic transmitter that excites the postganglionic neurons in both sympathetic and parasympathetic ganglia is acetylcholine. The motion of acetylcholine in autonomic 1 An autonomic nerve plexus is a group of nerve fibers that kind a network; nerve cells additionally be} present inside such a network. A ganglion is a knotlike mass of nerve cells found outdoors the central nervous system. The time period must be distinguished from the ganglion inside the central nervous system consisting of nuclear groups. Acetylcholine Receptors Acetylcholine receptors are located on the skin of the cell membrane of postganglionic neurons. They are protein complexes may be} sure to protein molecules that penetrate the cell membrane. Once the acetylcholine molecule binds with the receptor, the structure of the protein molecule of the cell membrane changes, and excitation or inhibition of the postganglionic neuron takes place. Two types of acetylcholine receptors exist and are identified as|often known as} nicotinic and muscarinic receptors. These receptors are so named end result of|as a end result of} nicotinic receptors respond particularly to nicotine (from tobacco), and muscarinic receptors respond particularly to muscarine (poison from toadstools). Usually, several of} presynaptic axon terminals must fireplace concurrently and summation has to occur for transmission alongside the postsynaptic axon to happen. Acetylcholine is also be|can be} believed to activate small numbers of postsynaptic muscarinic receptors. Nicotine in excessive concentrations acts as a blocking agent by first stimulating the postganglionic neuron and inflicting depolarization after which by sustaining depolarization of the excitable membrane. During this latter phase, the postganglionic neuron will fail to respond to the administration of any stimulant, regardless of sort of|the type of} receptor it prompts. Hexamethonium and tetraethylammonium block ganglia by competing with acetylcholine at the nicotinic receptor websites. The axons run between the gland cells and the smooth and cardiac muscle fibers and lose their masking of Schwann cells. At websites the place transmission occurs, clusters of vesicles are present inside the axoplasm (see. The site on the axon might lie at a long way|far} from the effector cell; thus, the transmission time additionally be} gradual at these endings. The diffusion of the transmitter by way of the large extracellular distance also permits a given nerve to have an motion on giant quantity of|numerous|a lot of} effector cells. In preganglionic neurons, both sympathetic and parasympathetic, the release of acetylcholine binds predominantly with the nicotinic receptors on the postganglionic neurons. The underlying mechanism is complicated, and the gradual potential occurs when the Na and Ca2 channels are open and M-type K channels close; this results in membrane depolarization. The existence of those complex postsynaptic potentials in both sympathetic and parasympathetic ganglia. All neurons that launch acetylcholine at their endings are called cholinergic (work like acetylcholine). The acetylcholine traverses the synaptic cleft and binds reversibly with the cholinergic (muscarinic) receptor on the postsynaptic membrane. The choline is reabsorbed into the nerve ending and used again for synthesis of acetylcholine. Most sympathetic postganglionic nerve endings liberate norepinephrine2 as their transmitter substance. In addition, some sympathetic postganglionic nerve endings, significantly those that finish on cells of sweat glands and the blood vessels in skeletal muscle, launch acetylcholine, which binds with muscarinic receptors on the postsynaptic membrane. In many other elements of the world, these two substances are called noradrenaline and adrenaline, respectively. There are two major sorts of receptors in the effector organs,called alpha and beta receptors. Two subgroups of alpha receptors (alpha-1 and alpha-2 receptors) and two subgroups of beta receptors (beta-1 and beta-2 receptors) have been described. The bronchodilating medicine,corresponding to metaproterenol and albuterol, mainly act on beta-2 receptors. As a common rule, alpha receptor websites are associated with many of the excitatory features of the sympathetic system. Beta-2 receptors are mainly in the lung, and stimulation results in bronchodilatation.
Buy cefpodoxime 200mg
Their mannequin referred to as Multi-store modelconsisted of long-term and working or short-term memory mannequin and was later improved by a further element, the sensory memory. Sensory memory incorporates one register for each sense and serves as an quick lasting buffer-zone earlier than the information can enter short-term memory. Short-term memory is a temporal storage model spanking new|for brand new} info earlier than it enters long-term memory, however additionally be|can be} used for cognitive duties, understanding and learning. The thesis of two separate memory techniques: the long-term memory and the short-term memory is at present considered to be true. Another term should be clarified right here: the working memory, which is often mistaken for the short-term memory. The primary difference between these two is that working memory often consists of the structure and processes carried out by a system management of|in cost of|in command of} the short-term memory. Serial Position Curve Variations within the ability to retrieve info are additionally seen within the serial position curve. This sample, known as as|often recognized as} the serial position curve, is brought on by two retrieval phenomenon: the primacy impact refers to an inclination to higher keep in mind stimuli which are be} offered early in an inventory. The recency impact refers to the tendency to higher keep in mind stimuli which are be} offered later in an inventory. The serial position curve is outcome of|the results of} each primacy results and recency results. There are quantity of|numerous|a selection of} explanations for primacy and recency results, however one of them is phrases of|when it comes to|by way of} the effects of rehearsal on short-term and long-term memory (Baddeley, Eysenck, & Anderson, 2009). So the recency impact could be defined phrases of|when it comes to|by way of} upkeep rehearsal in short-term memory. And the primacy impact may also be because of of} rehearsal-when we hear the primary word within the list we start to rehearse it, making it more doubtless that goes to be|will probably be} moved from short-term to long-term memory. Recency Effects and Primary Effects People are likely to|are inclined to} recall items or occasions within the order in which they occurred. You could end up asking, "How a lot info can our memory deal with at once? Series of Numbers Work via this series of numbers utilizing the recall train defined above to decide the longest string of digits that you could store. Recall is somewhat higher for random numbers than for random letters (Jacobs, 1887), and in addition typically slightly higher for info we hear (acoustic encoding) quite than see (visual encoding) (Anderson, 1969). The new term working memory was supposed to emphasize the importance of this technique in cognitive processing. Baddeley and Hitch suggested working memory is composed of three parts: the central executive, a system that controls the phonological loop (a subsystem for remembering phonological info corresponding to language by fixed refreshing via repetition within the loop), and the visuospatial sketch pad (a subsystem for storing visible information). This mannequin was later revised and improved by Baddeley but additionally contributed by other authors, which resulted in additional element of episodic buffer in year 2000 and more detailed functions and evaluation of other parts, as described in table below. These functions additionally embody communication with long-term memory and connections to language understanding and manufacturing facilities. Episodic buffer has the function of integrating the information from phonological loop and visuospatial sketchpad, but additionally from long-term memory. According to Baddeley, phonological loop consists of two parts: a sound storage which lasts only a few seconds and an articulatory processor which maintains sound info within the storage by vocal or sub vocal repetition. Verbal info appears to be routinely processed by phonological loop and it additionally plays an essential, possibly even key function in language learning and speech manufacturing. Studies have indicated that visuospatial sketchpad may really be containing two totally different techniques: one for spatial info and processes and the opposite for visible Episodic buffer Phonological loop Visuospatial sketchpad 94 Cognitive Psychology College of the Canyons info and processes. For example, you may simply recall a fact- "What is the capital of the United States? Declarative memory has to do with the storage of information and occasions we personally experienced. For example, solutions to the following questions are saved in your semantic memory: ninety six Cognitive Psychology College of the Canyons Who was the primary President of the United States? The concept of episodic memory was first proposed about 40 years in the past (Tulving, 1972). Since then, Tulving and others have checked out scientific evidence and reformulated the idea. Types of Memory Explicit memory is assessed utilizing measures in which the individual being tested should consciously attempt to keep in mind the information. A recall memory test is a measure of explicit memory that involves bringing from memory info that has beforehand been remembered. Your own experiences taking checks will probably lead you to agree with the scientific analysis finding that recall is harder than recognition. Recall, corresponding to required on essay checks, involves two steps: first producing a solution and then figuring out whether or not it appears to be the proper one. Recognition, as on multiple-choice test, solely involves figuring out which item from an inventory appears most correct (Haist, Shimamura, & Squire, 1992). Although they contain totally different ninety seven Cognitive Psychology College of the Canyons processes, recall and recognition memory measures are likely to|are inclined to} be correlated. Relearning more delicate measure of memory than either recall or recognition end result of|as a result of} it allows assessing memory phrases of|when it comes to|by way of} "how a lot" or "how briskly" quite than simply "correct" versus "incorrect" responses. There are three basic kinds of implicit memory: procedural memory, classical conditioning results, and priming. You can do that yourself: First, try to complete the following word fragments, however work on each one much less than|for under} three or four seconds. Once an idea is primed it influences our behaviors, for instance, on word fragment checks. Seeing an advertisement for cigarettes could make us begin smoking, seeing the flag of our house country could arouse our patriotism, and seeing a student from a rival college could arouse our competitive spirit. In one demonstration of the automaticity and affect of priming results, John Bargh and his colleagues (Bargh, Chen, & Burrows, 1996) performed a examine in which they showed faculty college students lists of five scrambled words, each of which they were to make right into a sentence. Furthermore, for half of the analysis members, the words were associated to stereotypes of the elderly. These members noticed words corresponding to the following: in Florida retired live people bingo man the forgetful plays the opposite half of the analysis members additionally made sentences, however from words that had 99 Cognitive Psychology College of the Canyons nothing to do with elderly stereotypes. The objective of this task was to prime stereotypes of elderly people in memory for a number of the} members however not for others. When the analysis participant had gathered all of his or her belongings, considering that the experiment was over, the experimenter thanked her or him for participating and gave directions to the closest elevator. Then, without the members understanding it, the experimenters recorded the amount of time that the participant spent walking from the doorway of the experimental room towards the elevator. Participants who had made sentences utilizing words associated to elderly stereotypes took on the behaviors of the elderly-they walked considerably more slowly as they left the experimental room. Results From Bargh, Chen, and Burrows, 1996 Bargh, Chen, and Burrows (1996) discovered that priming words associated with the elderly made people walk more slowly. These college students had no consciousness of the likelihood that the words might need been associated to the elderly or may have influenced their behavior. Interference Psychologists discuss with the time between learning and testing because the retention interval. But just as newer issues can intrude with remembering older issues, so can the other happen. Proactive interference is when previous reminiscences intrude with the encoding of recent ones. For example, if you have ever studied a second language, typically times the grammar and vocabulary of your native language will pop into your head, impairing your fluency within the international language. Retention Interval diagram Retroactive interference primary causes of forgetting (McGeoch, 1932). For example, should you witnessed a car crash however subsequently heard people describing it from their very own perspective, this new info could intrude with or disrupt your personal personal recollection of the crash. In truth, you could even come to keep in mind the occasion occurring exactly because the others described it! This misinformation impact in eyewitness memory represents a kind of retroactive interference that can occur through the retention interval. Although interference could come up between the prevalence of an occasion and the attempt to recollect it, the impact itself is always expressed when we retrieve reminiscences, the subject to which we flip subsequent. For example, if you have learned to program in one computer language, and then you definitely learn to program in another comparable one, you could start to make mistakes programming the primary language that you never would have made earlier than you learned one. Proactive interference occurs when earlier learning impairs our ability to encode info that we try to learn later.
References:
- https://ocw.mit.edu/resources/res-6-004-principles-of-computer-system-design-an-introduction-spring-2009/online-textbook/part_ii_open_5_0.pdf
- https://www.who.int/docstore/gtb/publications/training/medical_students_manual/tb_99_272.pdf
- https://www.cardinalhealth.com/content/dam/corp/web/documents/catalog/cardinal-health-clinical-chemistry-catalog.pdf