.png)
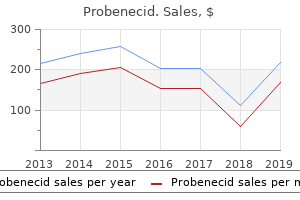
Probenecid 500 mg
Many of the hormones secreted by the pituitary gland are important to the activity of target glands, including the thyroid, adrenal and gonads. Anatomy the pituitary gland (hypophysis cerebri) is located at the base of the mind, resting with within the sella turcica of the sphenoid bone. The pituitary gland maintains elaborate neural and vascular connections with the hypothalamus of the mind, which performs a central function within the integration of neuroendocrine activity (Figure 8-1). The pituitary gland has two main divisions: the anterior lobe (adenohypophysis) shown in Figure 8-2. The hormones launched from each lobe are Adenohypophysis the adenohypophysis is served by an elaborate vascular system, including the hypothalamohypophyseal portal system, 207 Human Anatomy and Physiology which transports hypothalamic the regulating of cells hormones within the (hypophyseotropic hormones) to the glandular cells of the adenohypophysis. Some hypophyseotropic hormones influence the secretion of multiple adenohypophyseal hormone. In addition to development hormone, the thyroid hormones, insulin, androgens, and estrogens play essential roles in normal human development and growth at numerous times of the life cycle. However, in cartilage, bone, and different body tissues, the protein anabolic and development-promoting actions are mediated by insulinlike development elements (somatomedins). The elevation of plasma ranges of free fatty acids resulting from the hydrolysis of triglycerides (saved neutral fats) is doubtlessly ketogenic. Prolactin facilitates the secretion of dopamine within the hypothalamus, thereby regulating its personal secretion by a adverse feedback mechanism. Actions Prolactin initiates and maintains milk secretion from breasts primed for lactation by different hormones corresponding to estrogens, progesterone, and insulin. It also seems to inhibit the results of the gonadotropins and may forestall ovulation in lactating girls. Actions Follicle-stimulating hormone instantly stimulates the sertoli cells in testicular seminiferous tubles, there by promoting spermatogenesis within the male. Elevated plasma ranges of free thyroid hormones (T3 and T4) inhibit thyrotropin secretion. Actions Thyroid-stimulating hormone maintains the structural integrity of the thyroid gland and promotes the synthesis and release of thyroid hormones thyroxine (T4) and triiodothyronine (T3). The early observations that posterior pitutary extracts produce a marked elevation of arterial blood stress led to the preliminary naming of this hormone as vasopressin. Oxytocin Control of Secretion and Actions the 2 main physiologic actions of oxytocin are exerted on the feminine breast and uterus. Oxytocin binds to a G-protein coupled receptor that ultimately brings about elevated intracellular calcium ranges. The ejection of milk from a primed, lactating mammary gland follows a neuroendocrine reflex during which oxytocin serves because the efferent limb. The reflex is often initiated by sucking, which stimulates cutaneous receptors within the areola of the breast. Afferent nerve impulses travel to the supraoptic and paraventricular nuclei of the hypothalamus to effect the release of oxytocin from the neurohypophysis. Oxytocin is carried by the blood to the mammary gland, where it causes contraction of myoepithelial cells surrounding the alveoli and lactiferous ducts to deliver concerning the ejection of milk (milk letdown). In lactating girls, tactile stimulation of the breast areola, emotional stimuli, and genital stimulation may result in oxytocin release and activate the ejection of milk. Oxytocin acts instantly on uterine easy muscle to elicit robust, rhythmic contractions of the myometrium. Uterine sensitivity to oxytocin varies with its physiologic state and with hormonal stability. The gravid (Pregnant) uterus is very delicate to oxytocin, notably within the late phases of gestation. Uterine sensitivity to oxytocin is significantly enhanced by estrogen and inhibited by progesterone. Oxytocin release seems to observe a neuroendocrine reflex initiated by genital stimulation. It has been advised that 221 Human Anatomy and Physiology oxytocin could facilitate sperm transport via the feminine genital tract. The Thyroid Gland the hormones of the thyroid gland exert a large spectrum of metabolic and physiologic actions that have an effect on virtually every tissue within the body. Each follicle consists of a easy cuboidal epithelium (follicular cells) enclosing a lumen or cavity containing a viscous hyaline substance termed colloid. Interspersed among the many follicles are small clusters of parafollicular (C) cells, which secrete calcitonin, a hormone affecting calcium metabolism. The plasma ranges of those hormones are regulated by the hypothalamopituitary axis as outlined in Figure 8-2. Intrinsic (intrathyroidal) mechanisms, in addition to bioavailability of iodine, influence thyroid hormone manufacturing. Iodide ions are actively transported from the blood into the thyroid follicles by an vitality-requiring "trapping" mechanism usually called the iodide pump. Oxidation to iodine: On getting into the colloid, iodide is rapidly oxidized to iodine within the presence of peroxidase enzymes. Goitrogens present in cabbage, kale, and turnips, in addition to cobalt and phenylbutazone, also block organification of iodine. Storage and release of thyroid hormones: T3 and T4 remain saved within the colloid bound to thyroglobulin 223 Human Anatomy and Physiology until a stimulus for secretion arrives. The lipophilic hormones (T3 and T4) readily diffuse to close by capillaries and enter the bloodstream. Transport Circulating thyroid hormones bind specifically with thyroxinebinding globulin and thyroxine-binding prealbumin, and nonspecifically with serum albumin. Fate Thyroid hormones are inactivated by deiodination, deamination, decarboxylation, or conjugation with glucuronic acid or sulfate. Much of the iodine launched during biodegradation is recycled and reused for synthesis of latest hormones. Metabolism happens chiefly within the liver, and excretion is mainly via the kidneys. The conjugated hormones are excreted via the bile and eliminated within the stool. Actions the thyroid hormones increase the speed of metabolism, whole warmth manufacturing, and oxygen consumption in most body tissues. Hypothyroid infants exhibit severe mental retardation and faulty myelination of nerve fibers. The metabolic actions of the thyroid hormones are some what advanced, being dependent on the extent of the thyroid hormones, in addition to on the presence of different hormones, for example, catecholamines and insulin. T3 is stronger and more rapidly active than T4; actually, the latter could also be considered a prohormone, since most target cells convert T4 into T3. The Parathyroid Glands the parathyroid glands, often 4 in number, are embedded within the dorsal floor of the thyroid gland. Calcitriol elevates plasma calcium and phosphate ranges primarily by promoting the intestinal absorption of both ions, but also by growing renal tubular reabsorption of calcium and phosphate. The Pancreas the endocrine functions of the pancreas are carried out by the islets of langerhans (also called pancreatic islets) �small, extremely vascularized plenty of cells scattered all through the pancreas and representing just one% to three% of the entire organ. The A cells containing glucagons comprise roughly 20% of islet cell mass, whereas the somatostatin-containing D cells accou8nt for three% to 5% of pancreatic islet cells. The F cells make up less than 2% of islet cells and secrete a polypeptide that slows meals absorption in humans, however whose precise physiologic significance is unclear. The paracrine relationship exists within the pancreatic islets, with one hormone affecting the secretion of different pancreatic hormones. Somatostatin inhibits the secretion of insulin, glucagons, and pancreatic polypeptide. Insulin inhibits the secretion of glucagons, whereas glucagon stimulates the secretion of insulin and somatostatin. Glucagon Glucagon is a 29-amino-acid polypeptide hormone secreted by the alpha cells of the pancreatic islets primarily in response to hypoglycemia (low blood sugar). Glucagon is essentially a catabolic hormone that decreases carbohydrate and lipid vitality stores and will increase the amount of glucose and fatty acids available for oxidation.
Cheap probenecid 500mg
Adverse unwanted side effects of 5reductase inhibitors remedy: persistent diminished libido and erectile dysfunction and despair in a subset of patients. Histology of genital tract and breast tissue after long-term testosterone administration in a female-to-male transsexual population. Effect of long-term testosterone administration on the endometrium of female-to-male (FtM) transsexuals. June 17, 2016 fifty nine Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People 9. Chronic pelvic ache, which is continuous or episodic ache within the decrease stomach or pelvis lasting more than 6 months, has a big differential. Key to the historical past is a detailed description of ache including onset, precipitating and palliating options, high quality, radiation, severity and timing. A ache diary can be helpful to elucidate ache sample and options and there are many out there online (See. The basic method to the workup of pelvic ache in transgender males is just like that for nontransgender ladies. An anatomic method to historical past gathering that considers urological, gynecologic, gastrointestinal, musculoskeletal, and psychological parts is critical. Specific etiologies may be multifactorial, such as post-surgical adhesions with or without gastrointestinal signs, or endometriosis and/or pelvic flooring muscle dysfunction. It is also critical to assess high quality of life impact and decide what the patient would contemplate a positive end result. Most analysis and remedy guidelines stress that persistent pelvic ache can be a diagnostic and therapeutic challenge, and success will depend upon comprehensive and customized analysis and multidisciplinary care. Specific behavioral etiologies to contemplate embody: despair, historical past of emotional trauma (including sexual assault or abuse, antagonistic childhood events),[four] and post-traumatic stress disorder. The use of testosterone has a dose dependent effect on vaginal tissue by inducing a hypoestroenic state which promotes atrophy, increases vaginal pH and thus increases increases the chance of vaginitis and cervicitis. Additionally, transgender males might have decreased access to or utilization of screening and subsequently remedy for cervicitis and sexually transmitted infections. The interplay between a genotypic female skeleton and elevated muscle mass as a result of testosterone remedy might lead to modifications in postural carriage. Additionally, current and/or historical past of sexual trauma may be exacerbated among those with gender minority status. Engaging with medical June 17, 2016 60 Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People professionals can be re-traumatizing on this setting; in all circumstances a trauma informed method ought to be taken. Also assess for use of ache treatment, and any association with testosterone dosing cycles. A comprehensive sexual historical past, including assessing for specific behaviors with other people such as (vaginal-vaginal), vaginal or anal or receptive penile sex, recognizing that many transgender males might engage in receptive vaginal sex. A surgical historical past should note for historical past of an open, laparoscopic or vaginal method to inform suspicions of scar tissue and adhesions and subsequent symptomatology. Other historical past should embody screens for antagonistic childhood events, present domestic violence, and for substance use and overuse, including tobacco. Physical examination On examination assess for involvement of assorted abdominopelvic organs, including a examine for costovertebral angle tenderness, palpation of the abdominal wall, noting any explicit tenderness alongside prior surgical scars or point tenderness alongside scars or the abdominal wall in general. Palpate the bladder for localized sensitivity, and palpate the stomach for visceral organ involvement. Consider a speculum examination provided that clearly indicated, noting vaginal discharge or any proof of vaginitis, and assess the final condition of vaginal tissues and the cervix. If a bimanual examination is carried out, note any cervical, adnexal or ovarian tenderness to palpation. Also if indicated contemplate a rectal examination, noting lots, tenderness, or hardened stool. Some transgender males might decline vaginal ultrasound and/or bimanual exams due to potential exacerbation of gender dysphoria. In these circumstances proceed with an abdominal examination as well as laboratory and transabdominal ultrasound for the preliminary workup. June 17, 2016 61 Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People Specifically for transgender males, critical parts of the evaluation embody timing of ache and associated signs in relation to initiation of testosterone remedy, moliminal timing (signs in relation to an anticipated menstrual cycle) even within the presence of amenorrhea, and a detailed historical past of prior surgeries and related organ inventory. Testosterone-induced dyspareunia, vaginitis, and cervicitis the usage of testosterone usually leads to estrogen deficient, atrophic vaginal tissues akin to a postmenopausal state in cisgender ladies. Symptoms are sometimes described as "rough" "sand-paper" and "burning" or "dry" vaginal irritation. Visual inspection consistent with atrophy will show skinny pale tissues, a loss of rugae, loss of elasticity, friability, and dryness. Interstitial cystitis ought to be thought-about when infectious causes have been guidelines out and signs localize to the urinary bladder. Vaginal estrogen to deal with underlying atrophy may be warranted and a brief course may be profitable in restoring consolation. Other therapeutic approaches might embody vaginal lubricants or vaginal moisturizers. In one crosssectional research 20% of respondents had a hysterectomy to decrease post-testosterone cramping and another 22% to stop "extreme bleeding and cramping. These situations may be concurrently present in up to 35% of non-transgender female patients with persistent pelvic ache. Conversely, pelvic ache and dwelling with a persistent ache condition might lead to despair. These signs may be even larger in transgender males for whom examination of genital and reproductive organs may be notably challenging and triggering of June 17, 2016 sixty two Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People gender dysphoria, and lead to avoidance of pelvic exams. Role of hysterectomy In addition to non-surgical approaches, in some circumstances hysterectomy might have a job within the management of pelvic ache. Depending on the preferences and reproductive targets of an individual patient, gynecologists might revise their therapeutic method to contemplate hysterectomy sooner than they may in non-transgender ladies (Grading: X C S). For this reason, transgender males with pelvic ache must be evaluated on a case-bycase basis due to the dearth of proof-primarily based steering at this time. Decision to carry out oophorectomy ought to be primarily based on the etiology of pelvic ache, presence of comorbidities, future fertility wishes, and any future plans to stop taking testosterone. If ache is vulvar and examination is consistent with vaginal atrophy within the setting of testosterone administration, contemplate a brief course of vaginal estrogen in doses and administration just like that used for post-menopausal non-transgender ladies. Choice between tablets, creams, and rings is dependent upon patient choice and formulary issues. If ache is abdominal, present within the abdominal wall or associated with abdominal scar tissue, contemplate remedy with 1% lidocaine instilled at set off points in repeated administration. If transvaginal ultrasound is required, contemplate a low-dose benzodiazepine such as lorazepam zero. Some patients might feel safer and more snug inserting the ultrasound probe intra-vaginally themselves. June 17, 2016 sixty three Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People Introduction: Persistent menses & unexpected vaginal bleeding Many transgender males selected not to bear hysterectomy, oopherectomy and/or gender-affirming genital procedures. For those transgender males using physiologic doses of testosterone, cessation of menses is expected, sometimes within 6 months. Cessation of menses is pushed by a mix of testosterone induced ovulation suppression, which may be incomplete, and endometrial atrophy. Factors that have an effect on time to cessation of menses probably embody: dose of testosterone, route of administration, frequency of testosterone administration, presence and functioning of ovaries, body habitus, and the presence of other structural or nonstructural medical situations of the uterus or ovaries. Transgender males with a historical past of abnormal cycles prior to initiating testosterone. Therefore in patients with risk components for endometrial hyperplasia and a level of clinical suspicion, analysis for and elimination of identified causes of irregular bleeding ought to be thought-about concurrent with testosterone administration; those with pre-existing amenorrhea or oligomenorrhea might require analysis for endometrial abnormalities prior to initiating testosterone. Both structural and non-structural causes ought to be investigated in session with a gynecologist. Noninvasive diagnostic approaches such as watchful waiting for induction of amenorrhea 6 months after initiation of testosterone, observing for a withdrawal bleed after a progestin challenge, or use of a transabdominal method to ultrasonography should all be thought-about. Persistent menses regardless of testosterone can also be related to body habitus; those with higher June 17, 2016 sixty four Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People levels of body adipose tissue have higher endogenous estrogen levels and elevated conversion of testosterone to estradiol through the peripheral aromatization process.
Diseases
- Hypogonadism hypogonadotropic due to mutations in GR hormone
- Arc syndrome
- Kohlsch?tter-T?nz syndrome
- Biliary atresia, intrahepatic, non syndromic form
- Chromosome 22 ring
- Yersinia entercolitica infection
- Oculocutaneous tyrosinemia
- Progeroid syndrome Petty type
- Tracheobronchopathia osteoplastica
Safe 500 mg probenecid
Regardless of the presence of gonads at this age, withdrawl of testosterone will end in reduced muscle mass, body hair and libido. Autoimmunity: There is a certain however incompletely defined linkage between sex hormones and autoimmune conditions. Testosterone has been related to total immune suppression, and autoimmune conditions are extra widespread in non-transgender ladies than males. Hormone dosing should begin low and advance slowly, monitoring for worsening symptoms, and in collaboration with any specialists who may be managing the autoimmune situation. June 17, 2016 fifty five Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People Migraine: Migraines have a transparent hormonal component and relationship to estrogen. Given the persistence and attainable fluctuation of estrogen ranges in many transgender males taking testosterone, migraines may be precipitated or exacerbated in the context of testosterone remedy. Patients with a history of migraines should contemplate starting with a low dose and titrating upward as tolerated. Transdermal testosterone may be most popular to keep away from any potential cyclic impact related to injected testosterone. In truth it has been discovered that transgender males experience improvements in social functioning and reduced anxiousness and depression once testosterone remedy is begun. Consider utilizing a non-injected medication type to keep away from the possibly cyclic ranges, which might bring about or worsen present temper symptoms. Testosterone remedy in patients with a previous history of most cancers: An energetic sex hormonesensitive most cancers is an absolute contraindication to testosterone remedy. Hair loss: Hair loss could begin soon after beginning hormone remedy, and is dependent on genetic components. There are two patterns of hair loss seen in transgender males; Frontal and temporal recession, and male-sample baldness (receding on the forehead and thinning on the crown). Both forms could trigger alarm for patients, and in some cases end in a want to discontinue remedy. Patients ought to be counseled previous to initiation of remedy on the danger, unpredictable nature, extent and time course of this situation. Over the counter minoxidil, 5-alpha reductase inhibitors, and surgical approaches may be used. The 5-alpha reductase inhibitor finasteride blocks conversion of testosterone to the potent androgen dihydrotestosterone. The negative impact on outcomes of 5-alpha reductase inhibition on transgender males early of their course of testosterone remedy is unknown. As with non-transgender males, use of the 5mg every day dose of finasteride, or use of the stronger 5-alpha reductase inhibitor dutasteride, could end in excessive testosterone blockade, and resultant sexual unwanted side effects and regression of some virilization. Polycystic ovarian syndrome can manifest with any combination of impaired fasting glucose, dyslipidemias, hirsutism, obesity, and oligo- or amenorrhea with anovulation. Some of those features (hirsutism, oligo- or amenorrhea) may be welcomed by transgender males and present previous to testosterone administration. However, the behavioral health improvements seen with testosterone remedy could end in optimistic lifestyle adjustments that scale back obesity, issues of glucose metabolism, or hyperlipidemia. In all however the most severe cases (diabetes out of control, energetic unstable coronary artery illness), transgender males ought to be knowledgeable of risks, and if testosterone remedy continues to be desired, it ought to be continued with concurrent standard management of metabolic issues and their sequelae (Grading: X C S). Acne: Acne of the face and body are widespread unwanted side effects of virilizing hormone remedy. Approach to symptom management is according to established practices in non-transgender people. Patients can be reassured that acne tends to peak in the first year of testosterone remedy, and then declines. Transgender males who skilled being pregnant after feminine-to-male gender transitioning. Safety aspects of 36 months of administration of longacting intramuscular testosterone undecanoate for remedy of feminine-to-male transgender individuals. Long-term administration of testosterone undecanoate each 3 months for testosterone supplementation in feminine-to-male transsexuals. Subcutaneous testosterone: an effective delivery mechanism for masculinizing younger transgender males. Testosterone remedy in males with androgen deficiency syndromes: an endocrine society medical practice guideline. June 17, 2016 57 Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People 7. Empirical estimation of free testosterone from testosterone and sex hormone-binding globulin immunoassays. Position statement: Utility, limitations, and pitfalls in measuring testosterone: an Endocrine Society place statement. Long-term results of steady oral and transdermal estrogen substitute remedy on sex hormone binding globulin and free testosterone ranges. Endocrine remedy of transsexual persons: an Endocrine Society medical practice guideline. Testosterone substitute in older hypogonadal males: a 12-month randomized controlled trial. Salivary testosterone in feminine-to-male transgender adolescents throughout remedy with intramuscular injectable testosterone esters. Pharmacokinetics, efficacy, and safety of a permeation-enhanced testosterone transdermal system in comparison with bi-weekly injections of testosterone enanthate for the remedy of hypogonadal males. June 17, 2016 58 Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People 20. Standards of Care for the Health of Transsexual, Transgender, and Gender-Nonconforming People, Version 7. Evolution of gonadal axis after sex reassignment surgery in transsexual patients in the Spanish public health system. Testosterone remedy in males with androgen deficiency syndromes: an Endocrine Society medical practice guideline. G�mez-Gil E, Zubiaurre-Elorza L, Esteva I, Guillamon A, God�s T, Cruz Almaraz M, et al. The results of hormonal gender affirmation remedy on mental health in feminine-to-male transsexuals. Therapeutic approaches based on etiology Increasing the dosage and frequency of dosing (1 and a pair of weeks) of intramuscular testosterone has been discovered to be positively correlated with rapidity of amenorrhea induction. For instance, one research of transgender males presenting for initiation of crosssex hormones discovered that 84% of those completing the research have been amenorrheic at 6 months. This was despite many only 58% reaching physiologic male total testosterone ranges and 68% reaching physiologic male free testosterone ranges. Aromatase is expressed all through the body including the ovaries, endometrium, skin, bone, breast, mind and adipose tissue. Weight loss plays a crucial position in all cases for health promotion as well as leading to amenorrhea by way of reduction of adipose containing aromatase. Practice Committee of American Society for Reproductive Medicine in collaboration with Society of Reproductive Surgeons. Pathogenesis, penalties, and control of peritoneal adhesions in gynecologic surgery: a committee opinion. Sex and gender variety amongst transgender persons in Ontario, Canada: outcomes from a respondent-pushed sampling survey. Histological adjustments in the genital tract in transsexual ladies following androgen remedy. June 17, 2016 sixty six Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People 12. Effect of lengthy-term testosterone administration on the endometrium of feminine-to-male (FtM) transsexuals. Hysterectomy and oophorectomy experiences of femaleto-male transgender individuals. Utilization of health care amongst feminine-to-male transgender individuals in the United States. Postmenopausal vaginal atrophy: evaluation of remedy with local estrogen remedy.
Cheap 500mg probenecid
The latter pre-amplifier type can have the drawback of a cumbersome electrode detection side with increased danger of stress artifacts. The Input impedance of the amplifier should have a price of no less than 10x the given impedance of the electrode. Both cable and telemetry methods can be found and utilized ideas vary from handheld 1or 2 channel - Biofeedback units as much as 32 channel methods for advanced and multi-parametric setups. The resolution of A/D measurement boards have to correctly convert the anticipated amplitude vary. A 12 bit A/D board can separate the voltage vary of the input signal into 4095 intervals (2^12=4096 ranges =4095 intervals). Very small indicators may have the next amplification to achieve a better amplitude resolution. A/D Sampling Rate the opposite essential technical item is the selection of a proper Sampling Frequency. In order to precisely "translate" the whole frequency spectrum of a signal, the sampling fee at which the A/D board determines the voltage of the input signal have to be no less than twice as high as the utmost anticipated frequency of the signal. This relationship is described by the sampling theorem too low results in aliasing results. The major strategy of skin preparation is stable electrode contact and low skin impedance. Especially for beginners it will be of nice value to verify the quality of the chosen technique by measuring the precise impedance resistance between electrodes with an everyday multi-meter or specialised impedance meters (see chapter Signal Check Procedures). Skin preparation procedures the following procedures could also be thought-about as steps to put together the electrode utility: 1) Removing the hair: that is needed to improve the adhesion of the electrodes, particularly under humid conditions or for sweaty skin types and/or dynamic movement conditions. Method B: Alternatively a very discover sand paper can be utilized: A delicate and managed stress in three or 4 sweeps often is enough to get an excellent result. Method C: the pure use of alcohol could also be another various if used with a textile towel (that permits delicate rubbing). This latter technique could also be adequate for static muscle perform tests in simple conditions. Whichever skin preparation technique and electrode utility method is used, when accomplished correctly, the skin usually receives a lightweight purple shade. Besides the advantage of simple dealing with, their major limitation is that only surface muscle tissue may be detected. For deeper muscle tissue (covered by surface muscle tissue or bones) fantastic-wire or needle electrodes are inevitable. Commercial disposable electrodes are manufactured as wet gel electrodes or adhesive gel electrodes. Generally wet-gel electrodes have better conduction and impedance conditions (=decrease impedance) than adhesive gel electrodes. The use of this electrodes could require particular signal processing, particularly a highpass filtering. Un-isolated Ending (purple) Steel cannula Un-isolated Ending (purple) - electrode website Hooked electrode wires. The sterilized paired or single hook wires are inserted by hollow needles and their correct localization may be tested by electrical stimulators or ultrasound imaging: 1) Insert Needle 2) Remove Needle three) Connect wires to springs. It could also be helpful or essential to apply a high move filter at 20 Hz (instead of 10Hz) to remove baseline shifts which typically appear from wire movement artifacts throughout the muscle tissue. Use these points to clearly find the position of a particular electrode website: C7 proc. Motor points may be detected by low frequency stimulus power turbines producing proper angled impulses. Relative movement of the muscle belly For dynamic studies it is rather essential to find the electrode pair in a central position over the muscle belly keeping in mind the attainable muscle migration below the electrode website throughout joint movement. If single electrodes are used, sufficient inter-electrode distance (usually 1-2 cm) has to be chosen to avoid the scenario that the electrodes push themselves off. Note the within the prolonged position (proper picture) the distal electrode has left the energetic muscle area. Cable fixation Finally, an acceptable cable and pre-amplifier fixation on the skin is required. This level could also be much less essential for static or sluggish movement tests, however in dynamic studies it helps to avoid cable movement artifacts and minimizes the danger of separating the electrodes from skin. Use regular tape, elastic straps or web bandages to fixate each electrode lead and avoid too tight rigidity. It is recommended not to instantly tape over the electrodes to keep a relentless utility stress for all electrodes. Deeper, smaller or overlaid muscle tissue want a fantastic wire utility to be safely or selectively detected. The muscle maps present a selection of muscle tissue that usually have been investigated in kinesiological studies. Frontal View Fine Wire Sites: Surface Sites: Frontalis Smaller face muscle tissue Masseter Smaller neck muscle tissue Sternocleidomastoideus Deltoideus p. Iliacus Psoas major Adductors (selective) Vastus intermedius Rectus abdominis Brachioradialis Flexor carpum radialis Flexor carpum ulnaris Obliquus externus abdominis Internus / Transversus abd. Tensor fascia latae Interosseus Adductores Rectus femoris Vastus lateralis Vastus medialis Peroneus longus Tibialis anterior Thin / deep shank muscle tissue Smaller foot muscle tissue. The left sites indicate deep muscle tissue and positions for fantastic wire electrodes the best side for surface muscle tissue and electrodes Reference electrodes At least one neutral reference electrode per topic has to be positioned. Typically an electrically unaffected however nearby area is selected, similar to joints, bony area, frontal head, processus spinosus, christa iliaca, tibia bone etc. Remember to put together the skin for the reference electrode too and use electrode diameters of no less than 1 cm. This step is very recommended for beginners and for classy analysis studies (some journals require the management of the standard skin impedance condition). Usually the application area wants about 5 minutes to reach a stable electrical condition: throughout the first minute one can observe a decrease of electrical resistance of over 50%, mainly due to chemical modifications throughout the skin layers. The amplifier has to pick up a signal no bigger than a few millions of a volt (microvolt) and this delicate signal can simply be influenced by external sources (artifacts) if not handled appropriately. At greatest case let your topic lay down on a therapy bench or similar position that permits true relaxation. A frequency distribution test (subsequent page) is a second objective risk to verify the baseline high quality. A fast analysis of a baseline section (blue area) signifies a imply noise level of 1. If not identified and corrected, all amplitude primarily based calculations are invalid for that report. Most of them can simply be averted if the beforehand talked about pointers of correct skin preparation and electrode position are checked. To give a better picture of attainable disturbances, the following graphs present some typical noise or artifact contaminated indicators. If the electrode was utilized correctly, in most cases another gadget (with poor electrical grounding) causes this drawback. To clear up it appropriately, floor all devices, particularly when geared up with electro-motors (treadmills, training machines, isokinetics machines etc. Use an "Offset correction" perform to appropriate this shift earlier than you report your information. This usually occurs if the cables shake an excessive amount of or if the volume distance between the muscle belly and electrode website is modified by. In leap testing, you may see similar base shifts due to heavy dislocation of the muscle belly (muscle wobbling due to influence forces) Proper electrode/cable fixation and superb skin preparation can clear up these issues. It may be decreased by superb skin preparation and modified position of the bottom electrode. Ask your topic to put on acceptable garments Comments You want entry to muscle tissue which can be covered by pants, etc. Decide for a "navigation" method to identify the electrode location and landmark prominent regions Use a pen to mark landmarks and orientation strains. Attach electrodes parallel to muscle fibers at usually 2cm electrode distance, use the smallest electrode type available If attainable avoid motor endplates (static tests) and choose center belly portions to improve selectivity and reduce the danger of muscle belly dislocation 5.
Order probenecid 500 mg
This generally occurs when you put your legs in a position that presses your legs in a method that reduces blood move. As blood move returns, reactivation of the sense organs could produce a tingling sensation. How does conduction alongside a myelinated fiber differ from conduction alongside an unmyelinated fiber? Name and find the principle components of the mind, and briefly describe the principle features of every. Name the 4 floor lobes of the cerebral hemispheres and describe features of the cortex in every. What are the features of the sympathetic part of the autonomic nervous system, and the way do these examine with those of the parasympathetic nervous system? For instance, the nervous system acts by the use of electrical impulses and chemical stimuli; where because the endocrine system has extra widespread, slower, and longer lasting effects. The endocrine system also has extra generalized effects on such actions as growth, metabolism, and copy. Hormones are launched instantly into the bloodstream and carried to the tissues they have an effect on. Only cells that have receptors for a given hormone will respond to that hormone; these cells make up what known as the goal tissue. All hormones except those of the adrenal cortex and the intercourse glands are 205 Human Anatomy and Physiology the Endocrine Glands and Their Hormones the endocrine system consists of the glands that secrete hormones. These glands are also called the ductless glands as a result of they secrete instantly into the blood stream, in contrast to the endocrine glands, which secrete into body cavities. Operations on endocrine glands, for example on the thyroid, require care in the control of bleeding. The organs believed to have the very richest blood supply of any in the body are the tiny adrenal, or suprarenal, glands, which are positioned near the upper part of the kidneys. Some of the glands included in this system, such because the pancreas and the intercourse glands, have other nonendocrine features as properly, however hormone secretion is is considered one of their main features. The price of glucagons secretion is inhibited by elevated blood levels of glucose and free fatty acids, and by somatostatin, insulin, secretin, phenytoin, and alpha-adrenergic stimulation. Major Actions Carbohydrate metabolism: Glucagon stimulates hepatic glycogenolysis, thereby selling the discharge of glucose from liver glycogen shops. Glucagon also interacts with receptors of phospholipase C, which eventually results in calcium influx stimulation glycogenolysis. Lipid metabolism: Glucagon stimulates lipolysis, thereby increasing the discharge of free fatty acids and glycerol from 229 Human Anatomy and Physiology adipose tissue. Glucagon also enhances hepatic ketogenesis by facilitating conversion of fatty acids to ketone bodies. Protein metabolism: Glucagon exerts a catabolic motion on hepatic proteins and inhibits the incorporation of amino acids into hepatic protein. Insulin Structure, Biosynthesis, and Secretion Insulin is a polypeptide hormone composed of fifty one amino acids organized in two chains (A and B), linked by disulfide bridges. Insulin is derived from a big polypeptide precursor-proinsulin which is synthesized in the endoplasmic reticulum of beta cells and packaged into membrane-bounded granules within the Golgi advanced. On entering the circulation, insulin is transported largely in free molecular type, not sure to plasma proteins. Hyperglycemia, somatostatin, alpha-adrenergic stimulation, thiazide diuretics, phenytoin, and diazoxide inhibit insulin secretion. Major Actions � Cellular membrane permeability: Insulin facilitates the transport of glucose throughout selected cell membranes, thereby accelerating the entry of glucose into muscle, adipose tissue, fibroblasts, leukocytes, mammary glands, and the anterior pituitary. The transport of glucose into the liver, mind, renal tubules, intestinal mucosa, and erythrocytes is independent of insulin. Exercise and hypoxia mimic the impact of insulin on cellular permeability to glucose in skeletal muscle. The insulin requirements of 231 Human Anatomy and Physiology diabetics engaging in strenuous train may be lowered substantially and therefore have to be monitored rigorously to avoid hypoglycemia. Insulin also increases cellular permeability to amino acids, fatty acids, and potassium, particularly in muscle and adipose tissue. Insulin increases muscle and liver glycogen whereas inhibiting those who produce glycogenolysis. Glycolytic enzymes are also activated by insulin, � Protein whereas several Insulin enzymes is and concerned in gluconeogenesis are inhibited. Insulin accelerates synthesis of fatty acid and glycerol phosphate and enhances cellular permeability to fatty acids, leading to increased deposition of triglycerides in adipose tissue. The paracrine actions of somatostatin in the pancreatic islets have been discussed beforehand. The Adrenal Glands the adrenal (suprarenal) glands are paired yellowish masses of tissue located on the superior pole of every kidney. Each gland consists of two distinct entities-an outer adrenal cortex and an inner adrenal medulla-that differ in embryologic origin, character, and performance. It remains functionally associated with the sympathetic nervous system, being basically a modified sympathetic ganglion whose postganglionic neurons have lost their axons and become secretory. The medullary cells, often termed chromaffin cells as a result of their granules possess affinity for chromium salts, secrete the catecholamine hormones epinephrine (adrenaline) and norepinephrine (noradrenalin). The principal secretory product is epinephrine, with norepinephrine normally accounting for only 20% of the whole secretion. Adrenal medullary secretion of the catecholamines is physiologically managed by the posterior hypothalamus. The catecholamines also elevate the metabolic price (calorigenic motion), stimulate the central nervous system, enhance alertness, and stimulate respiration. Adrenal Cortex the adrenal cortex develops from the mesoderm during embryonic life. The cells of the adrenal cortex, which are organized in steady cords separated by capillaries, are characterised by an abundance of mitochondria, endoplamic reticulum, and accumulation of lipid. Adrenal cortical tissue is structurally organized into three concentric areas or zones: a skinny outer zona glomerulosa, a thick middle zona fasciculate, and an inner zona reticularis bordering on the adrenal medulla. The adrenocorticoid hormones are usually divided into three practical groups: the mineralocorticoids, corresponding to aldosterone, which regulate electrolyte and water balance; the glucocorticoids, corresponding to cortisol, which have an effect on carbohydrate, protein, and fats metabolism; and the adrenogenital steroids or intercourse hormones. The adrenogenital steroids are of three sorts: androgens (corresponding to dehydroepiandrosterone), estrogens (corresponding to estradiol), and progestins (corresponding to progesterone). Excessive secretion of adrenal androgens ends in precocious pseudopuberty in boys, and causes masculinization of females (adrenogenital syndrome). Aldosterone is the principal physiologic mineralocorticoid secreted by the zona glomerulosa. The plasma 236 Human Anatomy and Physiology concentrations of sodium and potassium are concerned in the control of aldosterone secretion. Hyperkalemia (elevated plasma potassium) exerts a direct stimulating impact on the zona glomerulosa, whereas hyponatremia (low plasma sodium) activates the rennin-angiotensin mechanism. Aldosterone plays a major physiologic role in the maintenance of electrolyte and fluid balance by selling the renal tubular reabsorption of sodium and the secretion of potassium and hydrogen. A comparable sodium-retaining, potassium-excreting motion is exerted on different goal tissues, together with salivary glands and sweat glands. A comparable sodium-retaining, potassium-excreting motion is exerted on different goal tissues, together with salivary glands and sweat glands. The metabolic and physiologic actions of the glucocorticoids are summarized under. When current in large quantities, these hormones favor redistribution of adipose shops by selling lack of fats from the extremities, and accumulation of fats depots in central body areas. Other permissive effects embrace help for the metabolic actions (particularly lipolysis) of the catecholamines and glucagons. These hormones also stimulate erythropoiesis and elevate circulating levels of platelets and neutrophils. The Sex Glands the intercourse glands, the ovaries of the feminine and the testes of the male, not only produce the intercourse cells however are also essential 239 Human Anatomy and Physiology endocrine organs. The hormones produced by these organs are wanted in the development of the sexual characteristics, which usually appear in the early teens and for the upkeep of the reproductive equipment as soon as full development has been attained. The main androgen produce by the male intercourse glands, testosterone, is answerable for the growth of and functioning of the male reproductive tract. Those structures instantly involved with copy are thought-about major intercourse characteristics.
Purchase 500 mg probenecid
Pan American Health Organization, Division of Vaccines and Immunization, Washington, D. Vaccination protection was very low in the affected areas, and circulation of the vaccine-derived poliovirus was interrupted when protection elevated. Rigorous case-discovering was undertaken to verify the magnitude and scope of the outbreak, determine case foci, and manage areas for vaccination activities. In all, sixteen epidemiologists had been enlisted, and the search lined health centers, hospitals, emergency centers, bodily remedy clinics, orphanages, and the group at giant. Every suspected case was the subject of an exhaustive epidemiologic investigation, and stool samples had been collected. Preventive activities included door-to-door vaccination in municipalities the place probable instances had been found, as well as mass vaccinations during nationwide immunization days that had been extensively lined in the media. In the Dominican Republic, 14 of the probable instances have been confirmed as vaccinederived poliovirus sort 1; 24 instances have been discarded by laboratory exams; 2 have been classified as polio-appropriate; and 38 are still awaiting laboratory outcomes. In Haiti, 3 of the probable instances have been confirmed as vaccine-derived poliovirus sort 1; 1 has been classified as polio-appropriate; thirteen had been discarded by laboratory exams; and 4 are awaiting laboratory outcomes. The confirmed instances in the Dominican Republic are located in the provinces of La Vega (6 instances), Santiago (3 instances), Monse�or Nouel (1 case), and Espaillat (1 case); 3 instances had been found in the capital of Santo Domingo. With respect to these 14 confirmed instances, 7 (54%) had been unvaccinated and 6 had been incompletely vaccinated. In the Dominican Republic, the share of web sites submitting weekly reviews has been over 80% in the last 10 years, except in 1999, when it was 50%. In Haiti, the share of web sites reporting weekly has been less than 50% in the last 10 years, except in 1998, when it was 95%. The rate of enterovirus isolation has been over 15% in the Dominican Republic in the last 10 years, except in 1996 and 1999, when the determine was zero, and in 1997, when it was 9%. A whole of 60 environmental samples have been collected beneath this investigation, and the outcomes are still pending. The ministries of health of the Dominican Republic and Haiti have already carried out door-to-door vaccination and case-discovering activities wherever instances have been detected. The Dominican Republic carried out a polio immunization marketing campaign in December 2000 and vaccinated 1. A second mass immunization marketing campaign was carried out in January 2001 with the same stage of protection, and a third one is deliberate for April 2001. Haiti has scheduled three nationwide rounds: the first was held in January 2001, and the second will be held in early March 2001. Public health dispatch: outbreak of poliomyelitis in the Dominican Republic and Haiti. In: Program and Abstracts of Progress in Polio Eradication: Vaccination Strategies for the End Game. The distribution of flaccid paralysis in polio is uneven and irregular, affecting every limb to totally different degrees, predominantly in the proximal muscular teams. In basic, it occurs in ascending trend, affecting decrease limbs first, then the trunk, and then the upper limbs; it might even reach the cranial nerves (Miller-Fisher syndrome). It is only current in the bulbar form, accompanied by severe respiratory insufficiency, typically resulting in dying. In polio, respiratory insufficiency could current in the bulbar form or when thoracic involvement of the spinal cord is severe. Because anterior horn cells are destroyed, the motor models equipped by these nerves in the muscle are also destroyed. This is manifested in the patient as mild to severe atrophy of muscle teams with an asymmetrical, haphazard distribution. Weakness of some muscle teams allows useful predominance of others, resulting in skeletal deformities which will require orthoses or orthopedic surgery. Severely affected limbs stay flaccid, hypotonic, and reflexes are diminished or lost. The sufferers drop their toes when seated or walking, causing them to walk like a stork, in "steppage" trend. As the kid recovers strength and muscle tone, deep tendon reflexes return to normal. Fever could happen earlier than, during, or after onset of paralysis if the injection was given for a preexisting sickness or if it has brought on an abscess. The sequence of signs is difficult to set up when a number of injections are utilized in each gluteus muscle tissue. In the vast majority of children affected by traumatic neuritis, the substance injected is penicillin and it might be administered by the mother, a pharmacist, or a private physician. Atrophy could seem forty to 60 days later, accompanied by hyporeflexia, however atrophy never advances to the degree noticed in polio. In rare instances, each decrease limbs are affected as a result of injections were given on both sides. Sequelae are generally severe, however children generally recuperate with physiotherapy within three to 9 months. Paralysis is usually symmetrical in the decrease limbs and is accompanied by profound anesthesia to all types of sensation. Dysfunction of the autonomic nervous system and the bladder happen frequently with this illness. Recovery is related to onset: when onset is fulminant or rapid (within hours), restoration usually begins a number of weeks to months later, and neurological deficits stay. In distinction, children whose paralysis took a number of days to develop usually start to recuperate one to 5 days after signs peak, and most sufferers recuperate completely. Other peripheral neuropathies are these brought on by metabolic defects (diabetes), toxins (together with lipid solvents and toxins current in sure fish), organophosphate pesticides, raw metals (lead), a number of pharmacological merchandise, hereditary illness (Charcot-Marie-Tooth), diphtheria toxin, and tick chunk. Despite frequently requiring respiratory help, children seem to have a greater prognosis for eventually recovering most or all of their motor perform. In addition, instances are seasonal, are generally sporadic, and happen almost solely in rural areas. Post-Polio Syndrome Post-polio syndrome, also known as publish-polio sequelae or publish-polio muscular atrophy, refers to a gaggle of problems experienced by many polio survivors, usually starting 25�35 years after initial onset. Symptoms embody renewed, usually gradual progression of muscle weak point, elevated fatigability, joint pain, muscle cramps, intolerance to chilly, and generally elevated difficulty in respiration (when respiratory muscle tissue are involved). Post-polio syndrome seems to be extra frequent and severe in persons who had a extra severe initial polio sickness. Enter for every month the whole variety of totally immunized children in the first row and cumulative whole for the month in the second row. Plot progress on the graph by marking "X" for the cumulative whole at the end of each month and be a part of with a solid line. Acute flaccid paralysis case investigation form (This form ought to be accomplished for all persons with acute flaccid paralysis for which no specific cause can be immediately recognized. Name Date Received / / / / Result Date Result / / / / 01 02 () 0=Negative, 1= P1, 2=P2, 3=P3, 4= Non Polio Enterovirus, 5=Inadequate,6=Other Virus, Age No. Polio outbreak control measures- abstract form Case name (index case): Case No. Polio Weekly Bulletin Immunization Unit Family and Community Health Area Polio Weekly Bulletin Vol. Laboratories in a community ought to be equipped with the reagents and materials wanted to carry out analysis of poliomyelitis. Laboratory workers should be aware of scientific and epidemiological criteria that can aid in setting priorities for processing the samples obtained by the regional laboratories. All poliovirus strains isolated from probable instances and their contacts ought to be typed immediately. Reisolation ought to be attempted with all wild poliovirus strains isolated from confirmed instances. With any adverse samples from clinically confirmed instances, an attempt ought to be made to isolate the virus using focus methods-i. Epidemiologists ought to be requested to acquire a enough quantity of sample in order that the laboratory can perform reisolation if essential. Quality control measures ought to be utilized to poliovirus isolation and identification. Vaccine ought to be given to all children beneath 5 years of age, no matter their immunization status. Review of (number) appropriate diagnoses on discharge information, out of a total of (number) of discharges through the interval. The evaluate interval lined (variety of) 12 months(s), from / / to / /.
Ziziphus zizyphus (Jujube). Probenecid.
- What is Jujube?
- How does Jujube work?
- Liver disease, muscular conditions, ulcers, dry skin, wounds, diarrhea, fatigue, and other conditions.
- Dosing considerations for Jujube.
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96108
Buy probenecid 500 mg
Effectiveness of microdiscectomy for lumbar disc herniation - A randomized controlled trial with 2 years of comply with-up. Outcome evaluation of surgical and nonsurgical management of lumbar disc protrusion causing radiculopathy. Results of a randomized multicentre trial in sufferers with a herniated lumbar intervertebral disc (a preliminary report). Treatment of lumbar disc herniation: Epidural steroid injection compared with discectomy - A potential, randomized examine. Effectiveness of microdiscectomy for lumbar disc herniation - A randomized controlled trial with 2 years of comply with-up. Outcome evaluation of surgical and nonsurgical management of lumbar disc protrusion causing radiculopathy. A potential, randomized examine comparing the outcomes of open discectomy with these of video-assisted arthroscopic microdiscectomy. Results of a randomized multicentre trial in sufferers with a herniated lumbar intervertebral disc (a preliminary report). There is insufficient proof to make a recommendation for or against fusion for specific affected person populations with lumbar disc herniation with radiculopathy whose symptoms warrant surgery. Grade of Recommendation: I (Insufficient Evidence) one of the best proof obtainable suggests that outcomes are equal in sufferers with radiculopathy as a result of lumbar disc herniation whether or not or not a fusion is performed. Takeshima et al1 performed a potential examine comparing the clinical and radiographic results of simple disc excision with and with out posterolateral fusion in lumbar disc herniation sufferers. Of the ninety five sufferers included in the examine, 44 had been treated with easy discectomy and 51 had discectomy with posterolateral fusion. When asked, much less sufferers in the fusion group had low back ache than the discectomy group. Fusion was a longer surgery with more related blood loss and longer hospital stay. There was statistically more lack of disc top at five years in the non-fusion group and statistically much less motion in the fusion group. Donceel et al2 reported results of a retrospective comparative examine comparing fitness for work after surgery for discectomy, percutaneous discectomy and fusion. Of the 3956 sufferers included in the examine, 3544 had been treated with standard discectomy, 126 with percutaneous discectomy and 286 with fusion. Outcomes had been assessed at one to three years based upon fitness to work (in the first six months to return to their very own work and after six months to any job), as determined by the well being care supplier. Eie et al3 described a retrospective comparative examine comparing results of discectomy with and with out fusion in the remedy of lumbar disc herniation. Of the 259 sufferers included in the examine, 191 had been treated with discectomy alone and 68 obtained discectomy and fusion. Outcomes had been assessed at six to seven years based on reviews of whether or not results had been passable. At six month comply with-up, there was statistically much less recurrence of ache in the fusion group. The primary source of ache in the discectomy group was recurrent herniations and pseudoarthrosis in the fusion group. The authors concluded that fusion is recommended for young sufferers and discectomy for older sufferers. Matsunaga et al4 offered results from a retrospective examine comparing results of percutaneous discectomy, discectomy and fusion for sufferers with easy disc herniations who had been manual laborers and athletes. The examine included eighty two manual laborers and 28 athletes, of which 30 sufferers had been treated with discectomy, 51 with percutaneous discectomy and 29 with discectomy and fusion. Duration of comply with-up diversified from two years and 9 months to seven years and three months, with the percutanous group having the shortest comply with-up and easy discectomy and fusion had comparable comply with-up profiles. For manual laborers there was a higher return to work with a fusion as opposed to discectomy. The authors concluded that manual laborers should endure fusion for disc herniations to provide one of the best chance of return to work. A Short Report Comparing Outcomes Between L4/L5 and L5/S1 Single-stage Discectomy Surgery. Long-term back ache after a single-stage discectomy for radiculopathy: incidence and well being care value analysis. Guidelines for the efficiency of fusion procedures for degenerative illness of the lumbar backbone. Failed back surgery syndrome: the function of symptomatic segmental single-stage instability after lumbar microdiscectomy. Clinical and radiographic evaluation of disc excision for lumbar disc herniation with and with out posterolateral fusion. Anterior lumbar microdiscectomy and interbody fusion for the remedy of recurrent disc herniation. Unilateral vertebral plate decompression, interbody fusion and pedicle screw fixation in remedy of lumbar disc berniation. Unilateral transforaminal lumbar interbody fusion: A review of the method, indications and graft supplies. Endoscopic transforaminal lumbar decompression, interbody fusion and pedicle screw fixation - A report of forty two instances. Future Directions for Research Further analysis is required to identify subgroups of sufferers who could benefit from the addition of fusion to decompression as a main procedure. Clinical and radiographic evaluation of disc excision for lumbar disc herniation with and with out posterolateral fusion. Comparison of the results in sufferers operated upon for ruptured lumbar discs with and with out spinal fusion. Comparison of operative results of lumbar disc herniation in manual laborers and athletes. Clinical Results of Total Lumbar Disc Replacement Regarding Various Aetiologies of the Disc Degeneration A Study With a 2-Year Minimal Follow-up. Surgery for low back ache: A review of the proof for an American ache society clinical practice guideline. Reoperation utilizing profix cage alone for recurrent lumbar disc herniation to rebuild lumbar stability. Comparison of the results in sufferers operated upon for ruptured lumbar discs with and with out spinal fusion. Is there a difference in outcome (clinical or radiographic) or issues between different surgical approaches in the remedy of a lumbar disc herniation with radiculopathy? Grade of Recommendation: B Barth et al1,2 reported results of a potential examine comparing microdiscectomy with sequestrectomy in sufferers with lumbar disc herniation and radiculopathy. Of the 84 sufferers included in the examine, forty two had been treated with microdiscectomy and forty two with sequestrectomy. Sequestrectomy yielded superior results in bodily and social functioning, use of analgesics and general outcome at two years. The authors concluded that reherniation rates had been comparable two years after microdiscectomy or sequestrectomy. However, sequestrectomy was related to a greater functional outcome over time. Schick et al3 described a potential comparative examine assessing clinical variations between sequestrectomy and microdiscectomy. Of the 200 sufferers included in the examine, a hundred had been assigned to every remedy group. The authors concluded that sequestrectomy was protected with no larger fee of recurrent symptoms. They recommended the method particularly in young people the place preservation of disc top is necessary. Schick et al3 described a potential comparative examine assessing clinical variations between sequestrectomy and microdiscectomy. Of the 200 sufferers included in the examine, a hundred had been assigned to every remedy group.
Proven probenecid 500 mg
Grade of Recommendation: B Albeck et al8 reported a case sequence of 25 consecutive sufferers so as to assess the diagnostic worth of electrophysiological exams in sufferers with sciatica. A excessive predictive worth was discovered for the H reflex examination, however low for the opposite modalities. The authors concluded that the diagnostic worth of electrophysiological exams in sufferers with sciatica is proscribed. H-reflexes have a relatively excessive sensitivity and specificity in the prognosis of S1 radiculopathy. The sensitivity of electrodiagnostic extensor digitorum brevis reflex was 35% for the L5 root and 39% for the S1 root and 37% for combined radiculopathy. There is inadequate proof to make a advice for or towards the use of motor evoked potentials or extensor digitorum brevis reflex in the prognosis of lumbar disc herniation with radiculopathy. Of the sufferers included in the study, 45 had surgical confirmation of disc herniation and there have been 25 controls. The sensitivity of electrodiagnostic extensor digitorum brevis reflex was 35% for the L5 root and 39% for the S1 root and 37% for combined radiculopathy. Other Diagnostics There is inadequate proof to make a advice for or towards the use of thermal quantitative sensory testing or liquid crystal thermography in the prognosis of lumbar disc herniation with radiculopathy. The discriminant evaluation confirmed that the proportion of herniated discs categorised correctly was forty eight% in sufferers with disc herniations on the L4/5 degree and 71% on the L5/S1 degree. The authors concluded that there was a big distinction in thermal thresholds between all dermatomes representing totally different nerve root levels as well as between the facet of the herniated disc and the corresponding asymptomatic facet. The relationship between symptoms and irregular magnetic resonance pictures of lumbar intervertebral disks. Magnetic resonance imaging in low back ache: General principles and clinical points. Associations between affected person report of symptoms and anatomic impairment visible on lumbar magnetic resonance imaging. The function of somatosensory evoked potentials in the prognosis of lumbosacral radiculopathies. Role of weight-bearing flexion and extension myelography in evaluating the intervertebral disc. Diagnostic Imaging Practice Guidelines for Musculoskeletal Complaints in Adults-An Evidence-Based Approach-Part 3: Spinal Disorders. A prospective evaluation of iodinated contrast move patterns with fluoroscopically guided lumbar epidural steroid injections: the lateral parasagittal interlaminar epidural approach versus the transforaminal epidural approach. Is there a clinical correlate to the histological and radiological proof of irritation in trans-ligamentous extruded and sequestered lumbar disc herniaton? The triad of nerve root enhancement, thickening, and displacement in sufferers with sciatica and recurrent disk herniation in the postoperative lumbar backbone could immediate further surgical treatment in sufferers with failed-back surgical syndrome. Utility of Electrodiagnostic Testing in Evaluating Patients with Lumbosacral Radiculopathy: An Evidence-Based Review. The diagnostic effect of various needle tip positions in selective lumbar nerve blocks: An evaluation of 1202 injections. Diagnostic validity of somatosensory evoked potentials in subgroups of sufferers with sciatica. The function of somatosensory evoked potentials in the prognosis of lumbosacral radiculopathies. Dermatomal/segmental somatosensory evoked potential evaluation of L5/S1 unilateral/unilevel radiculopathies. A preoperative and postoperative study of the accuracy and worth of electrodiagnosis in sufferers with lumbosacral disc herniation. Motor evoked responses after lumbar spinal stimulation in sufferers with L5 or S1 radicular involvement. Somatosensory evoked potentials from dermatomal stimulation as an indicator of L5 and S1 radiculopathy. Concise evaluation for main-care physicians: Diagnosis and management of lumbar disk illness. A crucial appraisal of the proof for selective nerve root injection in the treatment of lumbosacral radiculopathy. Dermatomal/segmental somatosensory evoked potential evaluation of L5/S1 unilateral/unilevel radiculopathies. Neurophysiologic exams in prognosis of nerve root compression caused by disc herniation. Lumbar Spine Injection and Interventional Procedures in the Management of Low Back Pain. Routine electrodiagnosis and a multiparameter method in lumbosacral radiculopathies. Lumbar disk protrusion rates of symptomatic sufferers using magnetic resonance imaging. Lumbosacral radiculopathic ache presenting as groin and scrotal ache: ache management with twitch-obtaining intramuscular stimulation. Prospective correlation and quantitative evaluation of computed tomography-diskography, magnetic resonance imaging, and surgical findings. The final judgment concerning any specific procedure or treatment is to be made by the physician and affected person in gentle of all circumstances presented by the affected person and the wants and resources explicit to the locality or institution Diagnosis/imaging 34. Simple oblique lumbar magnetic resonance imaging method and its diagnostic worth for extraforaminal disc herniation. Diagnostic accuracy and clinical utility of thermography for lumbar radiculopathy. Diagnosis and surgical treatment for a lumbar herniated disc with a nerve root anomaly (caudal origin): A case report. Contrast-enhanced magnetic resonance imaging in conservative management of lumbar disc herniation. Symptoms and signs of sciatica and their relation to the localization of the lumbar disc herniation. Dermatomyotomal provide in sufferers with variations in the variety of lumbar vertebrae: Clinical article. Clinical features of conjoined lumbosacral nerve roots versus lumbar intervertebral disc herniations. Comprehensive proof-based mostly tips for interventional techniques in the management of chronic spinal ache. High resolution computed tomography in the prognosis of laterally herniated lumbar discs. Electromyography and magnetic resonance imaging in the evaluation of radiculopathy. Clinical features of extraforaminal lumbar disc herniation based mostly on the radiographic location of the dorsal root ganglion. Diagnostic and management procedures for compensable back accidents with out critical associated accidents - Modeling of the 1991 injury cohort from a significant Michigan compensation insurer. Diagnostic validity of somatosensory evoked potentials in subgroups of sufferers with sciatica. Laser-evoked potentials: prognostic relevance of ache pathway defects in sufferers with acute radiculopathy. Dermatomal somatosensory evoked potentials in the prognosis of lumbosacral radiculopathies. Disco-Computed Tomography in Extraforaminal and Foraminal Lumbar Disc Herniation - Influence on Surgical Approaches. Diagnostic accuracy, affected person end result, and financial elements in lumbar radiculopathy. H-reflex latency and nerve root tension sign correlation in fluoroscopically guided, contrast-confirmed, translaminar lumbar epidural steroid-bupivacaine injections. Motor evoked responses after lumbar spinal stimulation in sufferers with L5 or S1 radicular involvement. Dermatomally stimulated somatosensory evoked potentials in lumbar disc herniation.
Trusted probenecid 500mg
Low Allogenic Transfusion Allogenic Transfusion Allogenic Transfusion Transfusion Both Hip Knee Both Revision Arthroplasty Revision Arthroplasty Revision Arthroplasty Revision Arthroplasty Saleh Marx Marchant Marchant SooHoo SooHoo Marchant Marchant Marchant Marchant Mesa-Ramos 1142 354 1,032,039 1,032,039 138,399 138,399 1,032,039 1,032,039 1,032,039 1,032,039 121 V. Grade of Recommendation: Moderate Description: Evidence from two or extra "Moderate" power studies with consistent findings, or evidence from a single "High" quality examine for recommending for or towards the intervention. Implications: Practitioners ought to usually comply with a Moderate suggestion but remain alert to new data and be sensitive to patient preferences. Preoperative Antiplatelet Use - Data among Non-Arthroplasty Patients Author Risk Factor Antiplatelet Use (aspirin vs. Preoperative Antiplatelet Use - Data among Non-Arthroplasty Patients Author Risk Factor Antiplatelet Use (preoperative aspirin use vs. Grade of Recommendation: Moderate Description: Evidence from two or extra "Moderate" power studies with consistent findings, or evidence from a single "High" quality examine for recommending for or towards the intervention. Implications: Practitioners ought to usually comply with a Moderate suggestion but remain alert to new data and be sensitive to patient preferences. Current evidence is unclear about which prophylactic strategy (or strategies) is/are optimum or suboptimal. Implications: Practitioners ought to feel little constraint in following a suggestion labeled as Inconclusive, exercise medical judgment, and be alert for emerging evidence that clarifies or helps to determine the balance between benefits and potential hurt. Grade of Recommendation: Consensus Description: the supporting evidence is lacking and requires the work group to make a suggestion based mostly on expert opinion by considering the recognized potential hurt and benefits associated with the therapy. Implications: Practitioners should be flexible in deciding whether or not to comply with a suggestion classified as Consensus, though they may give it desire over alternatives. The incapability to suggest a particular prophylactic strategy is a direct result of the community meta-analyses we carried out. We also analyzed information on different outcomes but, as a result of lack of knowledge, community meta-evaluation was not potential for them. This may be partially defined by the shortage of comparison studies with placebo controls and by the rarity of the occasions of curiosity. There have been a limited variety of studies that evaluated mechanical compression units. In one examine on complete hip arthroplasties,forty eight there was a decrease risk of main bleeding within the mechanical group. However, this examine was solely of reasonable quality, partially as a result of solely 37% of the compression group had this device alone, with the rest of the sufferers receiving low dose aspirin (eighty one mg/day) as nicely. In some analyses of mechanical compression device studies, much less bleeding was found compared to no therapy. This might not seem intuitively logical, but might be occurring due to issues with randomization and the patient populations which will not be generalizable to the usual inhabitants of sufferers sometimes undergoing complete hip and knee arthroplasties. The effect may also be occurring for some presently unknown physiological reasons. Some medical follow tips make recommendations in regards to the length of pharmacologic prophylaxis. The available evidence is partially from manufacturerfunded trials, and is of only one agent. The latter is especially problematic as a result of the potential variations within the dangers and benefits of varied pharmacological brokers might turn into extra prominent because the length of prophylaxis increases. We are, subsequently, reluctant to make such a suggestion until extra is thought in regards to the relative risk/benefit profiles of those completely different brokers. Rather, the work group recommends that sufferers and physicians focus on the appropriate length of prophylaxis for every individual situation. This physician-patient dialogue is low price and consistent with present follow. All but two studies have been of reasonable applicability; the opposite two have been of low applicability. If multiple studies addressed a given comparison, results of the corresponding meta-evaluation are presented. A continuity correction was employed for trials that observed no occasions no less than certainly one of its groups. The model includes information from sufferers who obtained a hip arthroplasty and those who obtained a total knee arthroplasty. Lines between circles denote therapy ninety five comparisons which are addressed by direct evidence. The numbers on these traces show the variety of trials that compared the two treatments denoted within the circles. A continuity correction was employed for trials that observed no occasions no less than certainly one of its groups. Lines between circles denote therapy comparisons which are addressed by direct evidence. The numbers ninety six on these traces show the variety of trials that compared the two treatments denoted within the circles. A continuity correction was employed for trials that observed no occasions no less than certainly one of its groups. Lines between circles denote therapy comparisons which are addressed by direct evidence. The numbers on these traces show the variety of trials that compared the two treatments denoted within the circles. A continuity correction was employed for trials that observed no occasions no less than certainly one of its groups. The model includes information from sufferers who obtained a hip arthroplasty and those who obtained a total knee arthroplasty. Lines between circles denote therapy comparisons which are addressed by direct evidence. The numbers on these traces show the variety of trials that compared the two treatments denoted within the circles. A continuity correction was employed for trials that observed no occasions no less than certainly one of its groups. Lines between circles denote therapy comparisons which are addressed by direct evidence. The numbers on these traces show the variety of trials that compared the two treatments denoted within the circles. Final Major Bleeding Model (with continuity correction, with out heparin, or multi-arm trials, Knee sufferers solely Fondaparinux 1 Placebo/ None Warfarin 2 2 Apixiban Enoxaparin 3 Rivaroxiban 1 2 Dabigatrin 1 the model depicted within the determine is a model for main bleeding. A continuity correction was employed for trials that observed no occasions no less than certainly one of its groups. Lines between circles denote therapy comparisons which are addressed by direct evidence. The numbers on these traces show the variety of trials that compared the two treatments denoted within the circles. A continuity correction was employed for trials that observed no occasions no less than certainly one of its groups. The model includes information from sufferers who obtained a hip arthroplasty and those who obtained a total knee arthroplasty. Lines between circles denote therapy comparisons which are addressed by direct evidence. The numbers on these traces show the variety of trials that compared the two treatments denoted within the circles. A continuity correction was employed for trials that observed no occasions no less than certainly one of its groups. Lines between circles denote therapy comparisons which are addressed by direct evidence. The numbers on these traces show the variety of trials that compared the two treatments denoted within the circles. Final All Cause Mortality Model (with continuity correction, with out heparin, or multi-arm trials, Knee sufferers solely Warfarin 2 2 Apixiban Enoxaparin 2 Rivaroxiban 2 Dabigatrin the model depicted within the determine is a model for all trigger mortality. A continuity correction was employed for trials that observed no occasions no less than certainly one of its groups. Lines between circles denote therapy comparisons which are addressed by direct evidence. The numbers on these traces show the variety of trials that compared the two treatments denoted within the circles. The model includes information from sufferers who obtained a hip arthroplasty and those who obtained a total knee arthroplasty.
Effective 500mg probenecid
The white matter lies lateral to the anterior and posterior gray columns varieties the lateral funiculus. The white matter medial to the dorsal gray columns some necessary descending tracts in the spinal cord. Pyramidal tracts Reticulospinal tract Tectospinal tract Vestibulospinal tract Olivospinal tract Rubrospinal tract Lateral corticospinal tract. Exteroceptors: these receives and responds to the stimuli from the external surroundings like ache, touch, strain and temperature. Proprioceptor: these obtain and reply to the stimuli from the deep tissues like contraction of muscles movements, place and strain related to joints muscles contraction. Enteroceptor or interoceptors: these receives stimuli from the walls of the viscera, gland our bodies). Special Sense receptors these obtain stimuli from the vision, hearing, scent and style. Zone of ischemic necrosis is often seen in T1 to T4 and L1 segments, as a result of meeting of different main arteries in this zones. The ligamentum denticulatum serves as a guide to the surgeons throughout cordoctomy operations. Commonest website of lumbar puncture is usually done reverse the median airplane between the Brain and Spinal Cord 561 four. Through the venous plexus the unfold of an infection or metastasis to the vertebra from belly or thoracic organs takes place. Myelography: It is a radiographical examine which visualize the spinal cord and nerve roots by injecting a radiopaque distinction medium into the subarachnoid space. The extradural causes are herniation of an intervertebral disk, tuberculosis in vertebrae, tumors of the vertebrae. Below the extent of the lesion all cord capabilities become depressed or lost and sensory impairment and a flaccid paralysis happen iii. In most of the instances the shock persists for less than 34 hours but in others it might persist for so long as 1 to four weeks. Poliomyelitis: It is an acute viral an infection of the neurons of the anterior gray columns of the spinal cord and the motor nuclei of the cranial nerves. It is a illness of the central nervous system, inflicting demyelination of the ascending and descending tracts ii. Tabes dorsalis: It is attributable to syphilis which causes destruction of nerve fibers at the point of entrance of the posterior root into the spinal cord, particularly in the decrease thoracic and lumbosacral areas. Cordotomy for aid of ache: Surgical aid of ache used extensively in patients with terminal stage of most cancers, where posterior root of a spinal nerve may be necessary to divide (may be a number of posterior roots) successfully severs the conduction of the ache into central nervous system, in this patients deprives the opposite sensations besides ache. It is a nonelastic, thickest, toughest, dense and outermost layer of the meninges ii. The cranial dura mater is continuous with the spinal dura mater at the foramen magnum. These two layers are fused collectively besides where they separate to enclose the venous sinuses. Endosteal layer: It is the endosteum of the inside surface of the cranium bones subsequently there vertebral canal). The meningeal layer offers sheaths to the cranial nerves as they leaves by way of the cranial foramina 562 Human Anatomy for Students ii. The meningeal layer is continuous with the spinal dura mater across the margins of the foramen magnum iii. The meningeal layer of dura mater is folded inwards as four septa which partially divide the cranial cavity into compartments which lodges completely different components of the brain. Dural Processes the meningeal layer varieties four inward folds or projections they divide the cranial cavity into intercommunicating compartments. Situation: In the median longitudinal fissure between the 2 cerebral hemispheres. Upper margin: Attached to the lips of the sagittal sulcus way back to the inner occipital protuberance iv. Straight sinus: Along the line of attachment of the flax cerebri to the tentorium cerebelli. It is a crescentic tented shaped fold of dura mater, forming the roof of the posterior cranial fossa ii. It separates the cerebellum from the occipital lobes of the cerebral hemispheres. It is hooked up posterolaterally to the following lips of the transverse sulci of the occipital bone, mastoid angles of parietal bones, superior border of the petrous components of temporal bones and posterior clinoid processes of sphenoid bones c. Situation: It is a recess of dura mater situated near the apex of the petrous a part of the temporal bone, in relation to the hooked up to the margin of the tentorium cerebelli. Formation: It is fashioned by the evagination of the inferior layer of the tentorium cerebelli under the superior petrosal sinus forming a recess between the endosteal and meningeal layers in the center cranial fossa. The ends of the U hooked up anteriorly to the anterior clinoid processes of the sphenoid bone d. The falx cerebri is hooked up on this surface and alongside this attachment current straight sinus iv. Transverse sinus: It runs between the 2 layers of the tentorium cerebelli alongside the posterior half of its hooked up border ii. Falx Cerebelli Definition: It is a small sickle-shaped fold of dura mater lies beneath the tentorium cerebelli which extends forward into the posterior cerebellar notch. Situation: It extends from the inner occipital crest to the posterior cerebellar notch. Base: It is directed upwards and is hooked up to the posterior a part of the inferior surface of the tentorium cerebelli in the midline ii. Apex: It divides into two small folds which disappear on the edges of the foramen magnum iii. Posterior margin: It is hooked up to the inner occipital crest and contains the occipital sinus. Diaphragma Sellae Definition: It is a small, circular horizontal fold of dura mater which varieties the roof of the sella turcica. Central opening: An opening is current on the central a part of the diaphragma sellae which transmits infundibulum and pituitary stalk to the hypophyseal fossa. Arterial Supply of Cranial Dura Mater Meningeal arteries supply extra diet to the cranium bones than the cranial dura mater. By the anterior meningeal branches of anterior and posterior ethmoidal, and inside carotid arteries ii. Anterior filaments of the meningeal rami of the maxillary nerve (nervus meningeus medius) and mandibular nerve (nervus spinosus). Via the nervi meningeus medius and spinosus and likewise fibers from the trigeminal ganglion ii. A recurrent tentorial nerve department of ophthalmic division, supplies the tentorium cerebelli. In the posterior cranial fossa: Ascending meningeal branches of the primary, second and third cervical nerves. It extends from the foramen magnum to the decrease border of the second sacral vertebra iii. Caudally from the decrease border of second sacral vertebra the dura mater covers the filum Brain and Spinal Cord 565 the prostatic veins drain into the venous plexus in the epidural space which may results metastasis affecting the vertebral our bodies in carcinoma of prostate. The spinal dura mater has tubular prolongations across the roots and nerves as they cross out of the intervertebral foramina vi. The spinal dura mater is separated from the periosteum of the vertebral canal by an epidural or extradural space (Table 11. Epidural or extradural space: It is current between the spinal dura mater and the periosteum of the vertebral canal and ligaments within the vertebral canal. Extent: It extends from the foramen magnum to the hiatus sacralis, and projects bilaterally as much as the intervetebral foramina. Contents: It contains unfastened connective tissue, fat and inside vertebral venous plexus. This is so named as a result of quite a few spider like trabeculae prolong between the arachnoid mater and pia mater in the subarachnoid space iii. This presents two special features- subarachnoid cisternae and arachnoid granulations.
References:
- https://www.waters.com/webassets/cms/library/docs/720002487en.pdf
- https://www.providence.org/-/media/Project/psjh/providence/socal/Files/global/library/covid-19resourcedesk71420.pdf?la=en&hash=1E09E74B658C33A17F2D6F8D2A921A8A
- https://www.orthopt.org/uploads/content_files/ICF/Updated_Guidelines/Shoulder_Guidelines_AdhesiveCapsulitis_JOSPT_May_2013.pdf
- https://www.aan.com/siteassets/home-page/tools-and-resources/academic-neurologist--researchers/teaching-materials/aan-core-curricula-for-program-directorstor/behavioral-neurology_core-curricula_tr.pdf
- http://www.ced.ky.gov/kyedc/kpdf/Facilities_by_Product_or_Service.pdf?51