.png)
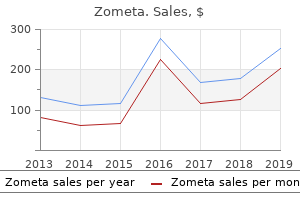
Effective zometa 4 mg
Some of the hypophysiotropic hormones are additionally found elsewhere in the body, particularly the gastrointestinal tract and placenta, the place they might have important physiologic functions. All of the hypophysiotropic hormones are additionally present in extrahypothalamic mind tissue and function as neurotransmitters. In every instance, the action of the hypophysiotropic hormone is mediated first by binding to specific receptors after which by alteration of intracellular transduction mechanisms. The feedback results of thyroid hormones, therefore, though occurring primarily at the pituitary, additionally happen at the hypothalamus. Such responses are additionally seen in patients with melancholy and schizophrenia, which can be related to disordered central bioaminergic regulation. During fetal improvement, these cells migrate across the cribriform plate, enter the forebrain with the nervus terminalis and vomeronasal nerves, journey medial to the olfactory bulbs, and eventually enter the septal-pre-optic area of the hypothalamus. In girls, positive and unfavorable steroid hormone feedback regulation of the hypothalamic-pituitary-gonadal axis happens at each the pituitary and hypothalamic ranges, the hypothalamic results being Figure 235-2 Interrelationships between hypothalamic and pituitary hormones. Plus indicators point out stimulatory results and minus indicators point out inhibitory results. In the follicular phase of the menstrual cycle, estrogen feeds back negatively on gonadotropin secretion. These ovarian peptides are additionally found in the pituitary and will therefore have additional local results on gonadotropin secretion. The hormone ranges and feedback loops talked about are primarily these of mature adults. At puberty, unfavorable feedback of steroid hormones decreases and gonadotropin and steroid ranges gradually rise. During this pubertal improvement, variation in unfavorable and positive estrogen feedback develops in females and eventually precipitates the adjustments ensuing in the ovulatory menstrual cycle. At menopause, ovarian estrogen and inhibin production stop, gonadotropin ranges rise markedly, and the signs related to estrogen deficiency develop. In men, growing older typically produces a lower in testosterone production with a modest rise in gonadotropins, however no scientific syndrome just like menopause affects men. Somatostatin can be present in the D cells of the pancreatic islets and the intestine mucosa, in addition to the myenteric neural plexus. The consequent increase in cortisol then reduces the depth of the inflammatory response and release of these monokines, thus finishing the feedback loop. Therefore this neuroendocrine-immune loop serves to modulate the inflammatory response. Such substances might have potential diagnostically and therapeutically sooner or later. The inhibitory part of hypothalamic regulation of prolactin secretion predominates over the stimulatory part. Dopamine is the predominant physiologic prolactin inhibitory issue, and the concentration of dopamine found in pituitary stalk blood is enough to lower prolactin ranges. Blockade of endogenous dopamine receptors by a wide range of medicine, such because the neuroleptics, causes a rise in prolactin. Lesions that interrupt the basal hypothalamic neuronal pathways carrying dopamine to the 1201 median eminence or that interrupt portal blood flow lead to decreased dopamine reaching the pituitary and hyperprolactinemia. Most information now recommend, however, at most a modest function for endogenous opioid peptides in neuroendocrine regulation. Three major opioid peptide receptors and three major teams of opioid peptides. The mu-receptor mediates many of the endocrine results and analgesia, morphine is its prototypic agonist, and naloxone is its prototypic antagonist. The delta-receptor mediates behavioral, analgesic, and some endocrine results and has as its primary peptide ligands met- and leu-enkephalins, that are derived from proenkephalin A. The kappa-receptor mediates sedation and ataxia and binds primarily dynorphin and the neoendorphins, that are derived from proenkephalin B (prodynorphin). The projection to the median eminence ends in important portions of beta-endorphin being found in portal blood. The pentapeptide enkephalins are derived from the 28-kd precursor proenkephalin A, which accommodates six copies of the met-enkephalin sequence and one copy of the leu-enkephalin sequence. Other extended cleavage merchandise with biologic exercise may also exist, and the ratio of met- to leu-enkephalin ranges between 5:1 and 10:1 in various places in the mind, presumably representing evidence of differences in tissue-specific cleavage and/or degradation. Neuronal perikarya containing the enkephalins are extensively distributed all through the mind, as are fiber networks. Most enkephalinergic neurons are quick and have the characteristics of interneurons. Rich enkephalinergic neural fiber networks could be found in the globus pallidus, amygdala, and midbrain, with specific areas of innervation together with the origin of the central noradrenergic system, the locus Figure 235-3 Structures of the precursors of the endogenous opioid peptides. Pre-proenkephalin A generates six copies of methionine enkephalin (met-enk) and one copy of leucine-enkephalin (leu-enk). Pre-proenkephalin B (pre-prodynorphin) generates alpha- and beta-neoendorphins; dynorphins 108, 1-7, and 1-32; and rimorphin. Enkephalinergic neurons in the magnocellular portion of the paraventricular and supraoptic nuclei project to the posterior pituitary. Within the pituitary, enkephalins have been detected primarily in the posterior pituitary. Enkephalins have additionally been found in the adrenal medulla, intestine, heart, lung, sympathetic ganglia, vagus, and retina. Dynorphin is a 17-amino acid peptide derived from a 28-kd precursor called proenkephalin B or prodynorphin. Shorter peptides termed alpha- and beta-neoendorphin, which have 10 and 9 amino acids, respectively, have additionally been isolated. Dynorphin-containing cells additionally project from the magnocellular neurons of the paraventricular nucleus to the posterior pituitary. The delta-receptors are positioned predominantly in the thalamus, hippocampus, periaqueductal grey matter, and neocortex, and the receptors are positioned primarily in the amygdala, nucleus accumbens, and hypothalamus. Dynorphin receptors have been localized to the cerebral cortex, the thalamus, and the caudate nucleus. The anterior pituitary itself is poor in opioid receptors but the hypothalamus is quite wealthy, and it has been advised that the consequences of opioid peptides on anterior pituitary hormone secretion are produced via modulation of hypothalamic bioamines and hypophysiotropic factors. The specific functions of the assorted opioid peptides and the opioid receptors are nonetheless not completely understood, though evidence links them to a variety of body functions, together with stress, psychological illness, narcotic tolerance and dependence, consuming, drinking, gastrointestinal function, learning, memory, reward, cardiovascular responses, respiration, thermoregulation, seizures, mind electrical exercise, locomotor exercise, being pregnant, and neuroimmune exercise. More specific functions relating to neuroendocrine regulation have been documented, however. Overall, the consequences of the endogenous opioids on normal physiologic regulation of the assorted pituitary hormones seem fairly minimal. The pulse amplitude of a pituitary hormone reflects the amount of releasing hormone, in addition to factors that may alter sensitivity to that releasing hormone. The frequency is generally ruled by the frequency of release of the hypophysiotropic issue, which is regulated by the hypothalamic pulse generator system. The pituitary has an intrinsic rhythm of small amplitude with a frequency of each 2 to 10 minutes. Superimposed on this intrinsic rhythm is a rhythm attributable to the pulsatile release of hypophysiotropic releasing factors, with or without the withdrawal of a corresponding inhibitory issue. These rhythms are usually synchronized with the 24-hour period by a periodic environmental cue such because the darkish-gentle cycle. Interesting adjustments happen in gonadotropin secretion as a toddler passes through puberty into adulthood. In patients with anorexia nervosa, the sample of gonadotropin secretion usually reverts to this pubertal sample, only to lose this sample once more with weight achieve. This phenomenon suggests that body composition might in some way have an effect on regulation of the pulsatile secretion of gonadotropins. Recent studies implicate leptin because the sign indicating this change in body composition. Endocrine rhythms seem to reflect a rather primitive organizing affect that helps an animal adapt to the environment.
Quality zometa 4 mg
Like rejection, the dangers improve with greater donor-recipient genetic disparity, and the danger can also be greater in male recipients of feminine (multiparous) donor stem cells. In the gut, the complication is characterized by watery diarrhea that will progressively improve in quantity and turn out to be bloody. In the liver, the illness is typically manifested by hyperbilirubinemia and an elevated alkaline phosphatase concentration. The diagnosis is confirmed by histologic examination of clinically affected tissue. The mixture of cyclosporine begun on day -1 (either a set dose of 5 mg/kg or targeted dosing to obtain plasma concentrations of 250 to 350 mug/L) with methotrexate. As an alternative choice to cyclosporine, the fungal-derived immunosuppressive tacrolimus has recently been used with obvious success. The residual host hematopoietic and immune system cells that have survived the preparative regimen are necessary targets of the incoming donor T lymphocytes. Destruction of those host cells appears important to ensure full host engraftment and may also characterize a serious component of the antitumor effect of allogenic transplantation. This activity, termed the graft-versus-leukemia effect, has been particularly properly documented in persistent myeloid leukemias. If the condition worsens or persists, further immunosuppressive agents are given, including antithymocyte globulin and monoclonal anti-T-cell antibodies. Treatment with immunosuppressive medicine, including prednisolone, cyclosporine, mycophenolic acid, azathioprine, and thalidomide, are often of solely modest benefit, and the condition has a high mortality from end-organ failure and infection. Relapse is more common after autologous transplantation due to the lack of a graft-versus-malignancy effect and perhaps also as a result of the stem cell graft could also be contaminated with malignant cells. Although illness relapse could also be treated by further doses of chemotherapy and even by further transplantation, these approaches are not often healing and have high remedy-associated mortality. An various strategy after allografting is to use the graft-versus-leukemia effect by infusing donor T cells; alloreactive T lymphocytes may then eradicate resurgent host hematopoietic malignancy. In mixture with chemotherapy, the strategy induces extended remission in 20% or more of sufferers with acute myeloid leukemia, and it could also be efficient in sufferers with relapsed myeloma. To date, solely anecdotal success has been reported in acute lymphocytic leukemia or lymphoma. It typically occurs about 6 months publish-transplant, and clinical findings embody renal insufficiency, hematuria, and anemia with evidence of microangiopathic hemolysis. In most recipients, the syndrome is self-limited and resolves with no particular remedy. The main causes of pulmonary problems during the later publish-transplant period are infection and regimen-associated toxicity. The syndrome responds poorly to remedy with steroids, tends to progress, and has a poor prognosis. The risk of endocrine dysfunction is larger in sufferers who receive whole-physique irradiation, and irregular thyroid function check outcomes will develop in about 50% of such sufferers. In most instances the abnormality is subclinical, with elevated thyroid-stimulating hormone ranges and elevated response to thyroid-releasing hormone, but about 10% will finally require substitute remedy. In ladies who receive a transplant publish-puberty with whole-physique irradiation as a part of the conditioning regimen, ovarian failure is evidenced by elevated ranges of follicle-stimulating hormone and luteinizing hormone within the presence of low estrogen. Even conditioning regimens that use chemotherapy alone produce ovarian failure, but some of these sufferers may recover, and a small number of pregnancies have been reported. Ovarian hormone substitute is usually utilized in premenopausal ladies to stop menopausal symptoms. In men who receive transplants after puberty, testosterone ranges stay regular but spermatogenesis not often recovers. Cataracts begin to develop 991 between 5 and 10 years publish-transplant and respond properly to excision. Several studies have proven a better incidence of a second malignancy in transplant recipients, notably in those who obtained radiation as a part of their conditioning. Both lymphoid and myeloid acute leukemias are elevated, and the most typical publish-transplant solid tumors are melanoma and glioblastoma. This effect can most readily be seen in sufferers receiving unrelated donor allografts for hematopoietic malignancies. Disease-free survival charges approaching or exceeding 90% can now be expected for people with aplastic anemia, persistent myeloid leukemia within the first persistent section, or thalassemia without liver harm. Conversely, survival charges for sufferers with superior malignancy stay low; the mixture of each extreme regimen-associated toxicities in these heavily pre-treated sufferers and a high relapse rate implies that solely 5 to 30% may survive 5 years. The pattern has been toward a discount within the intensity of the preparative regimen, with a correspondingly elevated reliance on the power of the donor immune system to eradicate host hematopoietic and malignant cells. A mixture of this strategy with the introduction of monoclonal antibodies (coupled to radionuclides or toxins) that particularly goal the hematopoietic system without damaging different host organs should cut back the incidence and severity of problems related to present preparative regimens. The availability of improved progress factors with activity on stem cells and on all hematopoietic lineages should allow speedy ex vivo and/or in vivo enlargement of the donor hematopoietic cells, thereby accelerating engraftment and minimizing the consequence of marrow aplasia. Summarizes the potential and the problems of hematopoietic stem cell gene remedy. A description of mesenchymal cells in marrow and their attainable functions after transplantation. Giralt S, Estey E, Ibitar M, et al: Engraftment of allogeneic hematopoietic progenitor cells with purine analog-containing chemotherapy harnessing graft versus leukemia without myeloablative chemotherapy. How the immune system might help eradicate leukemia within the absence of ablative conditioning. A good discussion of the longer-time period issues of the process and the way they have an effect on quality of life. Rubinstein P, Carrier C, Scaradavov A, et al: Outcomes among 562 recipients of placental blood transplants from unrelated donors. A large-scale multicenter account of the usage of wire blood transplantation, primarily in sufferers with malignant illness. These cells constitutively categorical anticoagulant properties that promote blood fluidity underneath regular circumstances. At a site of vascular injury, however, endothelial cells are either "activated," and are thereby transformed from an antithrombotic to a prothrombotic state, or turn out to be detached to expose circulating blood to thrombogenic constituents of the subendothelial vessel wall. These processes result within the speedy formation of a hemostatic plug that consists of platelets and fibrin. Activation of platelets and formation of fibrin happen essentially concurrently and interdependently to effect hemostasis. Subsequently, vessel wall repair is achieved by thrombolysis and recanalization of the occluded site. In the presence of intact endothelium, platelets are repelled from the vessel wall and flow into passively. Prostacyclin and nitric oxide are among the potent, domestically energetic platelet inhibitors (and vasodilators) which are elaborated by regular endothelial cells to promote blood fluidity. At a site of vascular harm, these antiplatelet substances are misplaced, and platelets adhere to the de-endothelialized intimal floor. In the method of platelet "aggregation" (platelet-platelet interactions), fibrinogen (or von Willebrand issue underneath conditions of high shear stress) mediates the formation of an occlusive platelet plug. The fibrin, which anchors the hemostatic platelet plug, is shaped from soluble plasma fibrinogen by the motion of the potent protease enzyme thrombin. Thrombin is shaped from its inactive (zymogen) plasma precursor, prothrombin, by the motion of activated Factor X (Xa) and its cofactor, Factor Va. This sequence of reactions has been classically referred to because the "common pathway" of coagulation. Factor X may be activated, in flip, by either the tissue issue ("extrinsic") pathway or the contact activation ("intrinsic") pathway of coagulation. This scheme emphasizes current understanding of (1) the significance of the tissue issue pathway in initiating clotting in vivo; (2) the interactions between pathways; and (3) the pivotal function of thrombin in sustaining the cascade by feedback activation of coagulation factors. Just as intact, regular endothelium promotes blood fluidity by inhibiting platelet activation, it likewise performs a crucial function in naturally anticoagulating blood by preventing fibrin accumulation. Antithrombin is the most important protease inhibitor of the coagulation system: it inactivates thrombin, in addition to different activated coagulation factors. Heparin functions as an anticoagulant by binding to antithrombin and thereby greatly accelerating its capacity to inhibit the coagulation proteases. Heparin and heparin sulfate proteoglycans are naturally current on endothelial cells, so antithrombin inactivation of thrombin and different coagulation proteases more than likely occurs physiologically on vascular surfaces somewhat than in fluid section plasma.
Order 4mg zometa
It is subsequently incumbent on physicians to be conversant in the rationale, indications, administration, and prevention of problems of enteral vitamin. The presence of vitamins throughout the intestinal lumen instantly increases epithelial proliferation and enhances mucosal cell renewal. In the absence of luminal stimuli or intestinal vitamins, the small and large bowels atrophy, not solely in the absorptive cells and brush border enzymes but also in the mucus-secreting cells and the gut-associated lymphoid tissue. These entities are essential protecting parts of the intestinal barrier towards micro organism, endotoxins, and other antigenic macromolecules and may provide a rationale for using small volumes. Enteral vitamins mediate many of their oblique enterotropic effects by stimulating gut hormones such as gastrin, neurotensin, bombesin, and enteroglucagon. Enteral vitamins given to animal models enhance the production of additional enterotropic hormones such as glucagon-like peptide 2. The anticipated duration of insufficient oral intake relies solely on the scientific judgment of the primary physician. Table 229-1 signifies examples of specific medical indications for enteral vitamin. Table 229-2 outlines the nutrient composition of some of these brokers, together with polymeric balanced diets, modified formulation, and modular supplements. Polymeric formulation are "complete" balanced, isotonic diets containing one hundred% of the Recommended Daily Allowance for substrates, nutritional vitamins, and minerals when prescribed in the beneficial amounts. These formulation are palatable and are the first choice for oral supplementation or tube feeding when digestion and absorption are reasonably regular. The nitrogen source consists of an intact or partially hydrolyzed pure protein. The caloric density of these formulation is usually 1 kcal/mL but could be as high as 1. Most importantly, polymeric balanced formulation are cheaper than the opposite formulation. Composed primarily of pre-digested or "elemental" vitamins, they require minimal digestion and are nearly utterly absorbed. Although the protein source could be crystalline amino acids, some pancreatic function is required to digest carbohydrates (oligosaccharides and disaccharides) and fat (up to 30% of which are provided as medium-chain triglycerides). In addition, absorption of glucose, sodium, amino acids, fat, nutritional vitamins, and trace parts requires intact mucosal transport systems. Unlike the polymeric balanced diets, modified diets are hyperosmolar, unpalatable, and comparatively expensive, costing between three and 10 times as a lot per calorie as polymeric balanced formulation. They could produce osmotic diarrhea if administered too quickly and require flavoring supplements for oral use. Examples of such limiting situations embrace persistent pancreatitis, short-bowel syndrome, and prolonged ileus. Certain modified formulation are designed for sufferers with specific dietary needs. Formulas that comprise solely essential amino acids as the protein source are designed for sufferers with renal failure. Formulas which have a protein source high in branched-chain amino acids and low in aromatic amino acids have been formulated for sufferers with hepatic encephalopathy, extreme trauma, and sepsis. Formulas which might be high in fat content (55% of calories) and low in carbohydrate content (28% of calories) have been beneficial for sufferers with respiratory insufficiency as a result of their oxidation produces much less carbon dioxide. The high fat content of these formulation could produce diarrhea in critically unwell sufferers. Recently, diets supplemented with fish oils, arginine, and nucleotides have been developed to allegedly enhance the immune response of critically unwell and postoperative sufferers. Well-controlled and correctly designed scientific trials are wanted earlier than recommending their use. Modular supplements, which encompass single or a number of vitamins, could be added to present "fastened-ratio" diets with out affecting the quality or amount of other vitamins. They are designed for sufferers for whom normal fastened-ratio formulation are suboptimal. Commercially available modules embrace carbohydrate, fat, protein, mineral, electrolyte, and vitamin formulations. Selection of the access website for supply of enteral vitamins relies on the anticipated duration of compelled feeding and the potential risk of aspiration. Ideally, enteral vitamin is given by the oral route to alert sufferers with intact gag reflexes who require dietary supplementation solely with meals. Nasogastric or nasoenteric tubes are ideal for sufferers who require short-term (less than four weeks) enteral vitamin. To use these access routes safely, sufferers must have intact gag reflexes and competent decrease esophageal sphincters. Ideal candidates are those with poor oral intake such as occurs with most cancers of the pinnacle and neck and the lung. The stomach is the popular website of supply, however the nasoenteric tube should be superior into the jejunum in sufferers with gastroparesis and a high risk of aspiration. Permanent access via tube enterostomies is the popular route of supply for long-term enteral vitamin (more than four weeks). Tube enterostomies are inserted either endoscopically, laparoscopically, or operatively into the pharynx, stomach, and jejunum. The percutaneous endoscopic strategy is the popular methodology 1164 Figure 229-1 Decision strategy for the kind and route of dietary assist. It has the benefit of decreased procedure time, native anesthesia, absence of an incision, and avoidance of ileus. The speed, simplicity, low value, and low complication price of percutaneous endoscopic gastrostomy have resulted in its alternative of surgical gastrostomy in most hospitals. Feedings of polymeric diets in a volume of 240 to 400 mL every four hours are nicely tolerated. The disadvantages of intermittent feedings encompass an preliminary requirement for nursing supervision, such as monitoring for gastric residuals, and the next risk of aspiration if delayed gastric emptying is current. Slow administration of small volumes into the stomach (25 to forty mL/hour) is nicely tolerated and avoids the stomach discomfort usually attributable to the increased price and volume of intermittent feedings. Continuous feeding, administered by infusion pump over a interval of 18 to 24 hours, requires much less nursing supervision and leads to smaller residual volumes and a decrease risk of aspiration than does intermittent feeding. When feeding into the duodenum or jejunum, steady feeding is required to keep away from distention of the bowel, fluid and electrolyte shifts, and diarrhea, all of which can occur with intermittent feeding. Feedings into the small bowel usually encompass isotonic polymeric options, initially at a price of 30 mL/hour. Infusions should be initiated at very low charges (10 mL/hour) in critically unwell sufferers. Disadvantages of steady feeding embrace the expense of the volumetric infusion pump and the limitation it locations on ambulatory sufferers. Patients receiving enteral feedings require the identical cautious monitoring as do those who obtain parenteral vitamin. Routine monitoring is best achieved by following a protocol that ensures complete and detailed surveillance to scale back the possibility of error in formulation choice and nutrient administration and to assess progress towards dietary objectives (Table 229-three). Clinical evidence of stomach distention is a contraindication to enteral feeding. In many situations, potential problems could be averted by simple maneuvers such as altering the infusion price, caloric density, or formulation. Periodic dietary evaluation is required to consider the adequacy of the dietary assist. Nitrogen steadiness, body weight change, and serum protein standing should be monitored and the nutrient prescription amended when indicated. These issues could make it essential to enhance the infusion price or to complement infusions with parenteral feeding till satisfactory enteral intake is achieved. Record the name, volume, and power of the formulation and the duration and price (mL/hr) of feeding. Every eight hr, chart the quantity of formulation administered separately from water or other oral intake. Irrigate the feeding tube with 20 mL of water on the completion of each intermittent feeding, when the tube is disconnected, after supply of crushed medications, or if feeding is stopped for any reason. When the patient is ingesting oral vitamins, request calorie counts every day upon request. As noted, a standardized monitoring protocol helps stop and detect possible issues.
| Comparative prices of Zometa | ||
| # | Retailer | Average price |
| 1 | SonyStyle | 142 |
| 2 | Williams-Sonoma | 900 |
| 3 | The Home Depot | 550 |
| 4 | Dell | 597 |
| 5 | Apple Stores / iTunes | 754 |
| 6 | BJ'S Wholesale Club | 872 |
| 7 | Toys "R" Us | 638 |
| 8 | Wal-Mart | 642 |
Best zometa 4mg
A primary defect in corticotroph cells can also be supported by a number of medical observations. Clinical suspicion is of paramount significance as a result of it establishes the first screening test before embarking on laboratory research. On the other hand, one must be discriminating and never formally evaluate everybody with weight problems, hypertension, and glucose intolerance. For instance, the centripetal distribution of fats with the characteristic "buffalo hump," "moon facies," and deposition in supraclavicular space, with minimal fats in the extremities, is rather more specific than generalized weight problems. Striae which are extensive (>1 cm) and purple reflect steroid-induced thinning of the dermis and can be distinguished from the extra common "stretch marks. Proximal muscle weak spot represents one other manifestation of glucocorticoid excess. As a outcome, cortisol can "spill over" and act on mineralocorticoid receptors in the distal tubule. B, Dramatic resolution of the manifestations of cortisol excess after successful transsphenoidal surgery. Immune suppression, opportunistic infections, and impaired wound healing can lead to considerable morbidity. The in a single day dexamethasone test is essentially the most extensively used screening test (see Table 237-eight). It ought to be famous, nevertheless, that abnormal in a single day dexamethasone suppression can be seen in as much as 30% of hospitalized patients and in lots of patients with depression or throughout alcohol withdrawal. An elevated 24-hour urine free cortisol value provides another, or further screening test for hypercortisolism. Often, two sequential specimens are collected due to day-to-day variations in hormone production. The sensitivity and specificity of urinary free cortisol measurements are higher than those of the in a single day dexamethasone suppression test, significantly in hospitalized patients. The traditional strategy is to perform a low-dose, adopted by a high-dose, dexamethasone suppression test (see Tables 237-eight and 237-10). On the second day of the test, regular individuals suppress plasma cortisol to lower than 5 mug/dL and reduce the 17-hydroxysteroids to lower than 2. Pituitary adenomas have an altered set level for glucocorticoid inhibition however retain a partial capability to respond to high-dose dexamethasone. The exact standards for dexamethasone suppression in the high-dose test are debated. Pronounced weak spot, fluid retention, glucose intolerance, hypokalemia, and poor pores and skin integrity are often seen. The metyrapone test takes benefit of the fact that inhibition of 11beta-hydroxylase blocks cortisol production. This test requires an skilled radiologist for secure and efficient catheterization of the petrosal sinuses (which drain the pituitary venous effluent). Blood samples are taken concurrently from the left and right petrosal sinuses and from the periphery. As in different pituitary tumors, complete remissions with macroadenomas are much less common. In the event of surgical remission or treatment, postoperative hypocortisolism is to be anticipated due to suppression of the hypothalamic-pituitary axis. After coverage for steroid withdrawal in the postoperative period, cortisol alternative should progressively be decreased to allow restoration of the hypothalamic-pituitary-adrenal axis. If transsphenoidal surgery is unsuccessful, reoperation could also be indicated and can lead to remission in as much as 50% of patients. It is extra efficacious in youngsters and in younger patients, however even in older adults remissions can be achieved in 50 to 60% within 2 years. To stop the continued ravages of hypercortisolism throughout this period, nevertheless, concomitant medical therapy is often given. Bilateral adrenalectomy represents one other alternative for patients with severe hypercortisolism after transsphenoidal surgery. It rapidly and effectively lowers cortisol levels however is associated with comparatively high morbidity and mortality (as high as 5%) due to the related metabolic and immune system alterations caused by hypercortisolism. This report of a large series of patients paperwork the somewhat shocking rapid good thing about irradiation after unsuccessful transsphenoidal surgery. Each of the glycoprotein hormones has a specific beta-subunit that varieties a non-covalent dimer with the common alpha-subunit. The beta-subunit genes are evolutionarily associated and share a common gene structure as well as having nucleotide and amino acid sequence homology. Similarities in the constructions of the beta-subunits account for his or her capability to type non-covalent dimers with the common alpha-subunit. The alphaand beta-subunits each undergo glycosylation, which is necessary for correct hormone folding, intracellular transport, and secretion. Glycosylation can also be required for biologic exercise, presumably due to results on the tertiary structure of the hormones. The gonadotropins are involved in sexual differentiation, intercourse steroid production, and gametogenesis. The regulation and physiologic roles of gonadotropins are quite different in males and females. Most theories maintain that the onset of puberty displays disinhibition of the heartbeat generator. The typical 28-day menstrual cycle is split into follicular and luteal phases which are separated by ovulation on day 14. In addition to suggestions regulation by steroids, ovarian peptides such as inhibin also play a task in charge of the reproductive axis. After a number of years of menstrual cycles which are typically anovulatory or irregular, menses cease, thereby defining the menopause. In males, the regulation of the hypothalamic-pituitary-gonadal axis is comparatively constant. Clinical options of hypogonadotropic hypogonadism in women are primarily due to estrogen deficiency and embody breast atrophy, vaginal dryness, and diminished libido. In premenopausal women, regular menstrual cycles provide evidence for an intact hypothalamic-pituitary-gonadal axis. In premenopausal women, preparations of estrogen and progestins ought to be used for hormonal alternative and to allow cyclical progress of the endometrium. Testosterone can be replaced in males using intramuscular injections which are given at 2- to four-week intervals. Doses and the intervals between injections ought to be adjusted on a person foundation using libido and testosterone levels before the subsequent injection as a guide. Many women have a discrete threshold for weight or exercise level that may cause lack of menstrual intervals. A variety of pathologic conditions can cause secondary hypogonadotropic hypogonadism, usually in association with deficiencies of different pituitary hormones (see Table 237-three). The majority (70-80%) of pituitary tumors categorised previously as non-functioning adenomas can be proven to produce low levels of intact glycoprotein hormones or their uncombined alpha- or beta-subunits. Biosynthetic defects in the tumor cells account for comparatively inefficient hormone secretion as well as the propensity to produce uncombined subunits. Elevated levels of free alpha-subunits are famous extra usually than increased free beta-subunits. Gonadotropin-producing tumors are considerably extra common in males than women and increase in prevalence with age. The tumors are usually large macroadenomas and present as clinically non-functioning tumors with signs and signs associated to local mass results. Visual subject loss due to suprasellar extension and compression of the optic chiasm is discovered in additional than 70% of patients. Symptoms of hypopituitarism, including 1224 hypogonadism with lack of libido, are also common. Premenopausal women with gonadotropin-producing tumors may experience menstrual irregularity or secondary hypogonadism. Because of the absence of a medical syndrome in most patients, the preoperative diagnosis of gonadotropin-producing pituitary tumors has relied on imaging research and laboratory exams. Unfortunately, the laboratory diagnosis of gonadotropin-producing tumors is lower than satisfactory.
Effective 4mg zometa
In progressive systemic sclerosis (see Chapter 290), focal myocardial necrosis and fibrosis may occur and culminate in a dilated cardiomyopathy. Edoute Y, Haim N, Rinkevich D, et al: Cardiac valvular vegetations in cancer sufferers: Prospective echocardiographic study of 200 sufferers. A study of the echocardiographic findings and clinical course of 200 sufferers with a variety of solid tumors; valvular vegetations were found in 19% of sufferers (a quarter of whom had systemic emboli), but solely in 2% of controls. Specific suggested tips for the management of suspected myocardial contusion are particularly useful. A descriptive evaluate article by the famous cardiac pathologist who has contributed many of the original observations about tumor involvement of the heart. The definitive echocardiographic study of the valvular abnormalities in systemic lupus erythematosus. Transesophageal echocardiography was performed in sixty nine sufferers with lupus (84% of whom had a repeat study), with comparability to a control inhabitants. Bourge Cardiac transplantation, once thought-about an experimental procedure, has emerged as the therapy of alternative for appropriately selected sufferers with life-threatening, irremediable coronary heart disease. The incidence of congestive coronary heart failure will increase with age and impacts more than four hundred,000 individuals in the United States yearly (see Chapter forty seven); transplantation is a therapeutic choice for a lot of of these sufferers. As survival after cardiac transplantation has markedly improved, the inhabitants of long-time period survivors has grown. Primary care physicians, as well as cardiologists not based mostly at cardiac transplant facilities, usually help in the care of these sufferers, most frequently in session with cardiac transplant physicians. In addition, a physician could also be called on to help in the management and analysis of a potential cardiac donor. The second most typical disease resulting in cardiac transplantation is idiopathic dilated cardiomyopathy (see Chapter 64). Factors that correlate with a excessive mortality, and therefore suggest potential benefit from cardiac transplantation, embody (1) a peak oxygen consumption on an train gas change stress take a look at of lower than 11 to 14 mL/kg per minute; (2) a low plasma sodium stage, especially after intensive medical management; (three) excessive proper ventricular and/or left ventricular filling pressures (a very excessive proper atrial or jugular venous strain and/or pulmonary capillary wedge strain), especially after medical management; (four) a very low ejection fraction (<15 to 20%; not predictive alone, however); (5) complicated ventricular arrhythmias; (6) a very massive left ventricular cavity (end-diastolic maximal dimension >70 to 75 mm); and (7) the need for recurrent hospitalization to deal with worsening signs despite maximum medical therapy. Other much less widespread cardiac ailments that could be treated with cardiac transplantation embody sarcoidosis (especially if limited to the heart), restrictive cardiomyopathy, hypertrophic cardiomyopathy, congenital coronary heart disease (not amenable to surgical palliation or correction), and valvular coronary heart disease (when the risk of cardiac surgical procedure is prohibitively excessive). The analysis for cardiac transplantation, which should typically be performed at an experienced cardiac transplantation heart, usually involves figuring out the underlying cardiac disease (if not already established), considering different acceptable (or preferable) treatment choices, evaluating the affected person for co-morbid situations that may restrict survival or enhance morbidity after transplantation, and educating the affected person (and household) relating to the trials of the publish-transplant medical routine. The transplantation analysis includes an assessment of the immunologic state of the potential recipient. Any main coexisting medical situation that may not be reversible with better cardiac function is a relative contraindication to transplantation, but lively severe an infection and neoplasm are the two near-absolute contraindications. Because publish-transplant compliance is so crucial, psychological instability and substance abuse are strong relative contraindications. When in doubt, a transplant physician ought to be consulted to determine potential eligibility. An analysis of social and financial sources is very important in the course of the transplantation analysis. The costs for the initial cardiac transplantation hospitalization and for follow-up procedures are formidable, even when no publish-transplant complications occur; medications alone can value $6000 to $20,000 for the primary yr after transplantation. The determination by an establishment to provide cardiac transplantation features a duty to help in the ongoing medical care of the affected person. The potential organ recipient should understand the individualized dangers involved with the decision to proceed with transplantation, together with the possible complications that may occur. Recipient Medical Care: "The Waiting List" Occasionally, a affected person is deemed too nicely to be listed for transplantation. Most sufferers ought to be re-evaluated at intervals of three to 6 months until either (1) the underlying cardiac downside improves or resolves, which occasionally occurs; or (2) worsening signs or danger elements for death develop and prompt the decision to proceed with transplantation. Organ distribution can be based mostly on the amount of time that a affected person has been listed and a standing system that varies barely inside totally different regions. About 2,500 sufferers receive transplants yearly, but of about 4000 to 4500 sufferers newly listed yearly for coronary heart transplantation, virtually eighty five% will still be awaiting cardiac transplantation on the end of the yr. As a outcome, 10 to 30% of listed sufferers die before an applicable donor is located. Physicians should consult the native or regional organ procurement organization relating to potential donors in order that applicable measures can be instituted to optimize the probability of profitable donations. Allograft electrical exercise and contraction often start spontaneously as oxygenated blood is provided, or they do so after direct present is utilized. In the trendy period, in the absence of significant pre-operative debilitation or co-morbid issues, postoperative care is often routine, with discharge to native housing possible at about 5 to 7 days after 376 surgical procedure. Prior to discharge, the recipient is instructed about publish-transplant medical care and precautions. Endomyocardial biopsies are usually performed once per week for the primary four to eight weeks, and then at progressively longer intervals. Immunosuppression begins with the preoperative administration of azathioprine and often cyclosporine. Intraoperative corticosteroids are sometimes given and continued intravenously in the immediate postoperative period. Cyclosporine and azathioprine are began soon after surgical procedure and could also be given intravenously until oral medications are tolerated. Routine chronic immunosuppression for many sufferers consists of triple-drug therapy, which often includes prednisone, azathioprine, and cyclosporine. Because larger dosages of cyclosporine may induce renal insufficiency, doses are subsequently tapered over 1 to three months to target cyclosporine levels. Tacrolimus (Prograf) is occasionally substituted for cyclosporine in sufferers with persistent or recurrent rejection and can be occasionally utilized in ladies and kids to keep away from the hirsutism associated with cyclosporine. Prednisone doses are tapered and, in some facilities, discontinued if no significant rejection occurs during tapering. In basic, the azathioprine dose is lowered if the white blood cell rely constantly falls beneath 4000 to 5000 cells/mL. Mycophenolate mofetil (CellCept) could also be superior to azathioprine and is most popular in some facilities. Routine use of influenza vaccine, although controversial, is of little danger and may provide some protection. Diltiazem can be routinely used at many transplant facilities, as it might additionally lower the risk of cardiac allograft rejection; diltiazem additionally will increase cyclosporine levels, resulting in lowered cyclosporine dosing and an overall savings in drug costs. Cardiac rejection could also be cell mediated (mobile rejection), the commonest kind, and/or antibody mediated (humoral rejection). Cellular rejection, which ends up in substantive or chronic rejection, is characterised initially by a mononuclear infiltrate. Higher grades of rejection are categorised according to the presence and extent of myocyte infiltration, myocyte necrosis, hemorrhage, and/or vasculitis. The incidence of cardiac rejection is highest early after transplantation and subsequently decreases to a low but constant fee. Symptoms and indicators associated with rejection could also be nonspecific and embody malaise, lethargy, fatigue, low-grade fever, and temper changes, or they may be cardiac-specific, corresponding to dyspnea, lower blood strain, jugular venous distention, a new S3 or S4 gallop, or a new supraventricular arrhythmia. Depressed cardiac function after cardiac transplantation, with or with out hemodynamic changes, is often attributable to acute rejection. Surveillance endomyocardial biopsies, especially inside the first 6 months after transplantation, stay the usual for detecting early indicators of rejection. About one third of sufferers develop a serious an infection publish-transplant (outlined as requiring intravenous antibiotics and/or thought-about to be life-threatening) in the course of the first yr after transplant, and an infection stays the commonest cause of death in the first yr. Lung and bloodborne infections are most typical, accounting for 50% of significant infections. The incidence of rejection episodes, calculated as the quantity per one hundred sufferers occurring each month after transplant, is highest in the first month following transplantation (34 rejections per one hundred affected person-months) and then rapidly declines over time. Cyclosporine-induced hypertension occurs in additional than ninety% of coronary heart transplant recipients inside the first yr. Antihypertensive drug dosing should permit for diurnal blood strain changes, with dosing timed to have a peak effect in the morning. To control blood strain, vasodilators (direct and calcium channel blocking drugs) and angiotensin-changing enzyme inhibitors are equally efficient. If possible, beta-adrenergic blocking drugs ought to be avoided, as a result of the denervated coronary heart relies on circulating catecholamines to enhance coronary heart fee and systolic function with train.
Zometa 4 mg
Affected individuals tend to be bright, educated, and engaged in intellectual occupations and may well give a history of psychosexual problems and socioenvironmental trauma. Rarely, however, do affected girls current with indicators and symptoms of estrogen deficiency. Psychological counseling and/or a change in lifestyle, especially for these girls engaged in strenuous exercise applications, may be efficient in inducing cyclic ovulation and menses. If steroid remedy is run, sufferers must be informed that the amenorrhea in all probability shall be current when remedy is discontinued. Other physicians consider solely periodic observation is indicated, with barrier strategies of contraception recommended for fertility control. Individuals with amenorrhea and vital weight loss should be examined for the potential for anorexia nervosa (see Chapter 227). Other midline defects such as cleft lip and palate can happen in the affected person or in members of the family. The trait is transmitted as an X-linked recessive or a male-restricted autosomal dominant trait, but genetic heterogeneity could happen. Partial or complete agenesis of the olfactory bulb is current on post-mortem, accounting for use of the term olfactogenital dysplasia. The dysfunction impacts solely gonadotropin secretion, and all different pituitary hormones are secreted usually. Sexual infantilism with a eunuchoid habitus is the scientific hallmark of this dysfunction, but moderate breast growth could happen. Estrogen substitute remedy is indicated in these girls until such time as being pregnant is desired. Hypopituitarism may be apparent on cursory inspection or sufficiently delicate to require endocrine testing (see Chapter 237). The scientific presentation is dependent upon the age of onset, the cause, and the nutritional standing of the individual. Failure of growth of secondary intercourse characteristics or for growth to progress as soon as puberty is initiated should always raise the question of hypopituitarism. Ovulation could be induced successfully with exogenous gonadotropins when being pregnant is desired and after the hypopituitarism is treated appropriately. Replacement remedy with estrogen is indicated to prevent indicators and symptoms of estrogen deficiency. Galactorrhea related to hyperprolactinemia, regardless of the cause, almost always occurs together with amenorrhea brought on by hypothalamic-pituitary dysfunction or failure. Hirsutism may be noticed often in association with amenorrhea-galactorrhea and hyperprolactinemia. The hypothalamic-pituitary unit also could fail to function usually in a variety of stressful, debilitating, systemic sicknesses that intrude with somatic development and growth. Chronic renal failure, liver illness, and diabetes mellitus are probably the most distinguished examples. Although sufferers usually current with amenorrhea, hirsutism, and weight problems, affected girls could as an alternative complain of irregular and profuse uterine bleeding, could not have hirsutism, and may be of regular weight. In the first syndrome the irregular menses, mild weight problems, and hirsutism begin during puberty and usually turn out to be extra severe with time. All such sufferers are well estrogenized no matter whether they current with primary or secondary amenorrhea or dysfunctional bleeding. Levels of most circulating androgens, especially testosterone, tend to be mildly elevated. The goal of the diagnostic evaluation is to rule out any causes (such as neoplasms) that require definitive remedy. Patients usually require remedy for hirsutism, for induction of ovulation if being pregnant is desired, and for prevention of estrogen-induced endometrial hyperplasia and 1338 most cancers. No ideal remedy exists, but quite the therapeutic method must be individualized to the needs of each patient. The method to the hirsute anovulatory lady not needing being pregnant is detailed in Chapter 255. Oral contraceptive brokers are the first line of remedy for such girls with mild hirsutism and provide safety from endometrial hyperplasia. A particularly severely affected subset of ladies current with marked weight problems, anovulation, mild glucose intolerance and excessive levels of circulating insulin with insulin resistance, acanthosis nigricans, hyperuricemia, and severe hirsutism with markedly elevated circulating androgen levels. These girls have hyperthecosis of the ovaries in which the androgen-producing cells in the stromal, hilar, and thecal parts of the ovaries are increased greatly in quantity. Both hyperthyroidism and hypothyroidism are related to a variety of menstrual disturbances, together with dysfunctional uterine bleeding and amenorrhea because of alterations in the metabolism of androgens and estrogens. These metabolic changes in flip end in inappropriate steroid suggestions and continual anovulation. A detailed dialogue of the analysis and remedy of premature ovarian failure. The abnormality could be diagnosed by ultrasonography or by the absence of proof of ovulation when the ovary is considered at laparoscopy. The dysfunction is believed to happen infrequently and sporadically and might be not a major reason for infertility. In fact, although the syndrome is believed to happen, data to substantiate its existence are solely circumstantial (although strongly suggestive) at current. Progesterone secretion in the luteal section may be reduced in length (termed luteal section insufficiency) or in amount (termed luteal section inadequacy). More hardly ever the endometrium may be unable to reply to secreted progesterone due to the absence of progesterone receptors. These problems are believed to represent causes for infertility (due to inability of fertilized ova to implant) in roughly 5% of infertile couples. Abnormalities of the follicular section, especially in the frequency of gonadotropin pulses, could account for many luteal section defects. Luteal section defects also could happen sporadically in usually ovulating girls roughly as soon as annually. Luteal section dysfunction may be related to a number of scientific entities, together with mild or intermittent hyperprolactinemia (of any cause), strenuous bodily exercise, inadequately treated 21-hydroxylase deficiency, and habitual abortion. Luteal dysfunction occurs extra commonly on the extremes of reproductive life and in the first menstrual cycles following full-term supply, abortion, or discontinuation of oral contraceptives. The analysis of luteal section dysfunction could be made either by endometrial biopsy or by serial progesterone determinations. Endometrial biopsies obtained from the uterine fundus in the late luteal phases of two totally different cycles must be at least 2 days out of section from the expected date of bleeding, as judged from the next menstrual cycle, for the analysis to be made. The absolute focus that progesterone should obtain and the size of time progesterone must be increased in the luteal section to exclude luteal dysfunction are unclear. Luteal dysfunction is extraordinarily rare in girls with menstrual cycles higher than 25 days in size in whom a single random progesterone determination is larger than 15 ng/mL. A complete consideration of the etiology, analysis, and remedy of luteal section abnormalities. In either case the state of affairs could or will not be correctable, especially for every explicit couple. Failure to reproduce thwarts a basic human instinct and causes anger, guilt, and despair. More than 10% of couples in the United States seek medical assistance for infertility. The fertilized ovum must be able to developing and implanting in appropriately ready endometrium. In fact, in roughly 40% of cases, infertility is brought on by the male (Table 250-7). In perhaps one third of couples, more than one cause contributes to the infertility. Idiopathic or unexplained (< 10%) girls of this age, the typical time during which unprotected intercourse occurs until conception is 5. The reproductive efficiency of couples is influenced by the ages of the feminine and male partners, the frequency of intercourse, and the size of time the couple has been making an attempt to conceive. There is a decline in both female and male reproductive efficiency after age 25 years. Couples who complain of infertility benefit evaluation regardless of the size of infertility.
Proven zometa 4mg
Symptoms regarding apnea are present with two to six instances greater frequency in family members of affected sufferers than in age-, sex-, and socioeconomically matched control households. Efferent exercise of the cranial nerves that supply upper airway muscle tissue is adjusted by nucleus ambigualis exercise and the neural discharge to the chest-wall muscle tissue by dorsal medullary nuclei. The exercise of those medullary teams of respiratory neurons could be altered by descending pathways from pontine and suprapontine areas and could be affected by the sleep-wake cycle, particularly the waxing and waning of the median raphe, or reticular activating system. The respiratory controller influences the exercise of upper airway as well as chest wall muscle tissue. The electrical exercise of upper airway muscle tissue usually seems to be entrained to the respiratory rhythm, and phasic increases and decreases in the exercise of many upper airway muscle tissue could be discerned. Sleep may depress the sensitivity of upper airway muscle tissue to chemical stimulation even more than the diaphragm. An essential characteristic of the obstructive sleep apnea-hypopnea syndrome is the presence of recurrent apneic episodes throughout sleep. Recurrent apnea outcomes from instability in the feedback control of respiratory, which causes ventilation to cycle quite than to preserve a relentless level. Negative pressures produced by the chest-wall muscle tissue throughout Figure 87-2 Three components decide patency of the upper airway, one or more of which might lead to a discount in airway measurement and to excessive upper airway resistance (loud night breathing) or obstruction (apnea). The mechanical features of small airstream measurement and a collapsible airway wall are essential in the pathogenesis of obstructive apnea. Inspiratory efforts against an obstruction produces instability in cardiac output and blood stress. Sleep episodes are present solely throughout instances of rest or when little consideration is required. Examples embody sleep episodes that occur whereas attending actions such as concert events, meetings, or displays. Symptoms produce impairment of social or occupational function, to the extent that folks take efforts to avoid situations the place sleep is more likely to occur. Sleep episodes are present throughout actions that require a minimum of average consideration. Examples embody uncontrollable sleepiness whereas eating or throughout conversation, walking, or driving. Families are highly aware, maybe extra aware than the individual, of opposed penalties of this level of sleepiness. Restless sleep and observed apnea are delicate and relatively specific indications of recurrent apnea. Both sleep complaints and daytime sleepiness are very roughly associated to the number and size of nocturnal arousals. Family members, quite than the affected person, are often the primary to acknowledge the sleep disturbance. Patients sometimes present with complaints of fatigue or decreased alertness, and sleepiness signs must be elicited by direct questioning and distinguished from fatigue. A variety of related features ought to suggest the prognosis of obstructive sleep apnea-hypopnea syndrome (Table 87-2). Likewise, pulmonary function checks will reveal no abnormality besides these brought on by related weight problems (considerably diminished lung capacities, with greater reduction in the expiratory reserve volume). In the affected person without upper airway or respiratory complaints, the circulate-volume loop is unhelpful. Patients with coronary heart and lung disease additionally may have the obstructive sleep apnea-hypopnea syndrome; however, no convincing epidemiologic evidence has been provided to confirm that sleep apnea happens extra regularly in sufferers with cardiopulmonary impairment. Patients with unexplained right-sided coronary heart failure or pulmonary hypertension must be questioned for the presence of sleep-disordered respiratory. Certain checks, such as arterial blood gas analyses, thyroid function testing, echocardiogram, and chest roentgenogram, are electively indicated if indicators of hypoxic exposure are present. Other variables recorded may embody noninvasive oximetry (on the lookout for falls in extra of three% from baseline values), muscle exercise from the limbs (on the lookout for non-respiratory causes for arousal), and physique position (on the lookout for expression of apneas solely in the supine position). In some cases it may be essential to measure esophageal stress to determine transient episodes of inspiratory circulate limitation leading to arousals or producing a fall in oxygen saturation of more than 3%. The most typical factor producing gentle and average levels of sleepiness is sleep restriction (a discount in nocturnal sleep size) because of lifestyle issues. Narcolepsy and restless leg syndrome are two disorders that additionally present with average and severe sleepiness. In the aged, in whom reviews of loud night breathing are excessive and a variety of episodes of apnea throughout sleep may be thought-about "normal," sleepiness could be secondary to a life-style or treatment effect. A cautious sleep historical past is the important thing to recognizing sleep apnea as well as these other diseases. Initially, a evaluation must be undertaken for the presence of anatomic or medical conditions whose reversal would ameliorate or remove respiratory disturbances throughout sleep. Treatment must be tailor-made to the person affected person and to the degree to which he or she is disabled by the respiratory disturbances throughout sleep (Table 87-3). Thyroid hormone alternative reverses the sleep apnea and scientific signs in myxedema. Patients with sleep apnea and cardiac or respiratory disease, such as coronary heart failure or asthma, must be placed on maximal remedy for the concomitant disease, as a result of decreased circulation time and/or elevated oxygenation may lower the incidence or severity of respiratory disturbances throughout sleep. The effect relies on the level of positive stress applied to the upper airway, and the optimum levels of stress differ amongst sufferers. In basic, though, at decrease levels of stress (3 to 6 cm H2 O), apneic episodes are eradicated, however episodes of partial upper airway obstruction (loud night breathing) persist. At greater levels of stress (5 to 15 cm H2 O), common respiratory tends to be restored. Factors such as alcohol use, hypothyroidism, and weight problems may worsen airway stability. Bilevel ventilation for obstructive apnea is the application of an inspiratory help over and above the expiratory stress required to hold the pharyngeal airway open. One indication for this approach is a concomitant finding of chronic hypoventilation along with obstructive apnea. Side results of remedy embody feelings of suffocation, nasal drying or rhinitis, ear pain, and conjunctivitis. Intraoral appliances are gaining wider acceptance in the remedy of both loud night breathing and obstructive apnea. Some gadgets are designed to tug the tongue forward and others to protrude the mandible or, on the very least, stop the mandible from retruding with sleep. The tracheostomy may be technically difficult owing to morphologic features such as weight problems, a short neck, or a short mandible. Problems with stomal infection and granulation tissue usually occur, and it may take a yr or extra before the tracheal website is well healed. Surgical correction directed at a selected, pathologic narrowing of the upper airway brought on by enlarged tonsils, nasal polyps, macroglossia, or micrognathia is reported to enhance indicators and signs of sleep apnea. In prospective research in which tonsillectomy has been carried out for sleep apnea, obstructive apnea may persist, however the frequency is tremendously diminished. Extensive excision of soppy tissue in the oropharynx, termed uvulopalatopharyngoplasty, may enhance pharyngeal function throughout sleep. The process includes a submucosal resection of redundant tissue from the tonsillar pillars to the arytenoepiglottic folds. In one sequence, the success fee was roughly 60%, however success has varied considerably from middle to middle. Most sufferers report symptomatic improvement; however, objective reduction in the number or magnitude of respiratory disturbances throughout sleep is often absent. Potential problems of the process embody speech and swallowing difficulties, particularly regurgitation of food. Some sufferers may have an elevated variety of respiratory disturbances throughout sleep after the process, however recognition of the disturbances is obscured as a result of loud night breathing is absent. These "silent obstructions" may be as severe as apneic episodes prior to surgical intervention. Newer procedures, such as laser-assisted uvuloplasty and radiofrequency tissue ablation, are designed and promoted as outpatient remedies for loud loud night breathing. Outcome research present some short-term (70 to eighty% at 2 to 6 months) reductions in loud night breathing loudness; however, long-term success charges at 1 yr are 50% and proceed to decline at 2 years. Sleep apnea syndrome must be excluded before either process is contemplated, as a result of apnea may improve after these procedures and since use of those procedures may delay extra definite remedies. Additional procedures embody enlargement hyoplasty, a process directed at transferring the hyoid arch forward by inserting a prosthetic device in the hyoid arch, and midline glossectomy. Success across centers in massive sequence of unselected sufferers remains to be decided.
Safe 4mg zometa
Homing to marrow seems complete within 20 hours (in all probability sooner), and engrafted stem cells rapidly enter cell cycle after intravenous infusion (within 12 hours). They subsequently move to the bone surface, giving rise to both hematopoietic and bone cells. The blood stream clears quickly of stem cells, and there seems to be just about no primary thymic engraftment, though later secondary engraftment of thymus happens. Diseases of deranged or deficient stem cells are normally manifest as cancers or as cell deficiency states (Table 158-4). Marrow transplantation (see Chapter 182) represents one of many major therapeutic advances of the past 20 years. It has been efficiently used to remedy marrow deficiency states (largely aplastic anemia), genetic marrow illnesses (hemoglobinopathies, enzymopathies), osteopetrosis, and a variety of predominately marrow or lymphoid malignancies. It was initially used to restore deficient cell production (or deficient products from cells) or to restore cell populations after otherwise lethal injury by excessive-dose radiotherapy/chemotherapy was used to remove malignant cell populations; marrow transplantation circumvented the primary barrier (killing of marrow stem cells) to dose escalation. More current research have indicated that a graft-versus-tumor effect is a serious component of the therapeutic effectivity of allogeneic brother/sister transplantation, thus indicating that transplantation may fit in part by mediating a mobile immune assault in opposition to most cancers cells. Marrow cells have been the preliminary source of stem cells for transplantation, however pheresis of peripheral blood stem cells has supplemented marrow in autologous transplantation and is rapidly replacing it in allogeneic transplantation. Fetal liver has been utilized as a source of stem cells, and umbilical cord blood is changing into a serious source of cells, particularly for unrelated transplantation. Stem cells from these sources are additionally essentially the most attractive automobiles for a variety of gene remedy approaches, though this is nonetheless an evolving area of analysis. The first successful use of a cytokine within the remedy for a cytokine deficiency state was that of erythropoietin to deal with the anemia of renal failure. Renal failure represents a true cytokine deficiency state, and thus this is a perfect target for cytokine remedy. Administration of erythropoietin to patients with renal failure corrects or partially corrects the anemia and restores a greater state of properly-being. Erythropoietin can also be used in other settings, the place its advantages are less clear (Table 158-5). Tumor development is a risk, however cytokine manipulation of tumor development, presumably in live performance with remedy to kill biking cells, is a chance. Approved for use in United States however scientific profit not clear Approved in United States for non-myeloid malignancies. The ligand for C-mpl or thrombopoietin also needs to quickly be accredited for exciting platelet production. Thus, at present, powerful biologics can increase the red cell, neutrophil, eosinophil, basophil, monocyte, and platelet counts. The red cells are normocytic (regular dimension) and normochromic (regular hemoglobin pigment), with central areas of pallor that ought to occupy less than one half of the diameter of the cells. Many red cells are microcytic (smaller than the nucleus of the traditional lymphocyte near the center of the sector) and hypochromic (with central areas of pallor that exceed one half of the diameter of the cells). Peripheral blood with oval macrocytes (giant red cells) and marked neutrophil hypersegmentation. Bone marrow aspirate exhibits red cell precursors that are giant megaloblasts, with nuclear-cytoplasmic dissociation (nuclear maturation lagging behind cytoplasmic maturation). Megaloblastic changes within the leukocyte series are demonstrated by the "giant C metamyelocyte. Peripheral smear exhibits a predominance of microspherocytes (small, densely staining red cells with lack of the central areas of pallor) alongside larger, grayish, "polychromatic" cells that in all probability represent reticulocytes. Peripheral smear exhibits fragmented red cells or "schistocytes" in a variety of sizes and shapes. Mature neutrophil with a two-lobed nucleus that has a dumbbell or "pince-nez" appearance. Bone marrow exhibits megakaryocytic clusters seen in important thrombocythemia and other conditions associated with clonal thrombocytosis. A peripheral blood smear in agnogenic myeloid metaplasia exhibiting a leukoerythroblastic picture. The characteristic findings are teardrop-shaped red cells (dacryocytes), nucleated red cells (erythroblasts), and immature granulocyte precursors. Prussian blue iron stain of the bone marrow exhibits ringed sideroblasts, which are nucleated red cell precursors with perinuclear rings of iron-laden mitochondria. Peripheral smear exhibits that the predominant leukocytes are "regular" mature-showing lymphocytes, with occasional "smudge" cells. Peripheral smear exhibits furry cells with blue-gray cytoplasm and fantastic, hairlike projections (resembling ruffles), and oval or barely indented nuclei with unfastened chromatin and vague nucleoli. Peripheral smear exhibits leukocytosis, with representation by the whole spectrum of leukocyte differentiation, starting from myeloblasts to mature neutrophils. Peripheral smear exhibits fragmented red cells alongside larger, polychromatophilic cells and a nucleated red cell that replicate hemolysis, as well as a paucity of platelets. At least a point of anemia is detectable in 20 to 40% of hospitalized patients. The hemoglobin (Hgb), measured in grams per deciliter, represents the entire quantity of hemoglobin in the entire erythrocytes in one hundred mL of blood. In addition to these standard measurements, automated absolute reticulocyte counts per microliter of blood or evaluations of new methylene blue-stained peripheral blood smears for the percent of positive-staining erythrocytes (reticulocytes) give a measure of the number of newly released (usually 1- to 2-day old) erythrocytes. It is a non-nucleated, non-dividing cell, during which greater than ninety% of the protein content is the oxygen-carrying molecule, hemoglobin. Although this classification makes it easier to perceive the pathophysiology of anemia and to decide the proper diagnostic research to perform, in lots of patients a couple of mechanism may happen concurrently. A wide variety of conditions could be liable for impaired erythropoiesis (Table 159-2). A second mechanism of anemia because of reduced production of cells by the bone marrow is deficiency of hematopoietic stem cells and/or dedicated erythroid progenitor cells. In nearly all such instances, the defect is a extra generalized bone marrow abnormality that results in reduced production of all lineages of bone marrow-derived cells, significantly erythrocytes, granulocytes, and platelets. Idiopathic bone marrow failure, commonly often known as aplastic anemia, is the prototype of such problems (see Chapter 160). Patients with severe malnutrition, together with anorexia nervosa, additionally may have bone marrow hypoplasia. A minority of patients with myelodysplasia or paroxysmal nocturnal hemoglobinuria even have vital bone marrow hypoplasia. Viral an infection, significantly with parvovirus B19, which selectively infects dedicated erythroid progenitor cells, can also cause transient or extended pure red cell aplasia because of the cytotoxic effect of this virus on the contaminated erythroid precursor cells. This category covers a broad vary of problems, together with intrinsic erythrocyte abnormalities, exogenous inhibitory effects, and nutritional deficiencies. Folate deficiency regularly may be because of insufficient dietary intake but in addition may be because of diffuse intestinal problems and to drugs that intrude with folate metabolism, similar to ethanol, sulfonamides or sulfa-related drugs, trimethoprim, methotrexate, anticonvulsants, and presumably oral contraceptives. Folate deficiency may happen in patients with an elevated requirement for folate in such conditions as persistent hemolytic anemias, being pregnant, and in childhood. In addition, severe alcoholics, patients with general malnutrition from any cause, and patients with certain unconventional dietary habits are susceptible to developing folate deficiency. A severely folate-deficient food plan will end in clinically vital folate deficiency within about 6 weeks. Cobalamin deficiency nearly never happens because of lack of dietary cobalamin intake; instead, it most frequently is due to impaired absorption of cobalamin because of lack of intrinsic issue, gastric atrophy, and abnormalities of cobalamin absorption within the terminal ileum. Because of considerable shops and very low day by day necessities for cobalamin in regular individuals, deficiency of cobalamin normally takes at least 3 to 5 years to become manifest. The heme synthetic pathway and its defects are described in additional detail in other chapters. Iron is required for the final stage of synthesis of heme, and iron deficiency impairs heme synthesis and results in anemia. Although iron-deficiency anemia is related classically with microcytosis, most patients with gentle iron-deficiency anemia actually have normocytic erythrocytes. One of the hallmarks of anemia of persistent illness or inflammation is impaired switch of iron into developing erythroid cells, leading to a functional iron deficiency in normoblasts even when iron shops within the bone marrow and the remainder of the body are enough. In most of the circumstances during which anemia of persistent illness/inflammation happens, there additionally may be concomitant iron deficiency. Impaired synthesis of alpha-globin chains in alpha-thalassemias or beta-globin chains in beta-thalassemias results in unbalanced synthesis of globin chains and a reduction within the number of hemoglobin alpha2/beta2 hemoglobin tetramers (see Chapter 167).
References:
- https://www.medschool.lsuhsc.edu/neurology/students/docs/Week%202%20Clinical%20Cases.pdf
- https://ttngmai.files.wordpress.com/2012/06/dekkerprobioticsinfoodsafetyhumanhealth.pdf
- https://www.physio-pedia.com/images/5/57/Cpt._9_Cerebral_palsy.pdf
- https://fee.org/media/14940/read-i-pencil.pdf
- https://vc2040.org/images/Final_EIR/VCGPU-FEIR_z.Atmt_1_Comment_Ltrs_Part2of4.pdf