.png)
Purchase cyclosporine 25mg
Microvascular decompression appears to be extra likely to to|prone to} present ache management with fewer relapses. Results of peripheral nerve avulsion are less passable with ache recurring in 50% inside 2 years. Dysaesthesia/Anaesthesia dolorosa this troublesome sensory disturbance follows any harmful method to nerve or root in 530% of patients. Corneal anaesthesia this occurs when root part or thermocoagulation involves the first division and keratitis might outcome. Mortality microvascular decompression and open root part carry a very low mortality (< 1%), however this should not be ignored when evaluating outcomes with safer methods. Treatment choice: this is dependent upon by} dialogue of the differing dangers with the affected person. In younger patients the absence of sensory complications make microvascular decompression the procedure of first choice. Frail and elderly patients might tolerate glycerol injection, balloon compression and thermocoagulation extra simply than other procedures. Tolosa Hunt syndrome A condition by which an inflammatory course of involving the cavernous sinus or superior orbital fissure presents with ache, loss of ocular movement and ophthalmic division sensory loss. Atypical facial ache the affected person, usually a young or middle-aged woman, experiences a boring, persistent ache, spreading diffusely over one or both sides of the face. These signs usually outcome from an underlying melancholy and may respond nicely to antidepressant remedy. The acute signs might resolve however result in a persistent postherpetic neuralgia which slowly improves. The motor nucleus lies in the lower pons medial to the descending nucleus and tract of the Vth cranial nerve. They enter the internal auditory meatus and, passing via the facial canal of the temporal bone, lie in shut proximity to the inner ear and tympanic membrane. The facial nerve offers off quantity of} branches before exiting from the cranium via the stylomastoid foramen. They run collectively because the nervus intermedius and accompany the facial nerve to the internal auditory meatus. The parasympathetic fibres (visceral efferent) move in the greater petrosal nerve to the sphenopalatine ganglion and thence to the lacrimal gland to produce tears and in the chorda tympani nerve to the submandibular ganglion. Facial nerve Visceral afferent Parasympathetic efferent Facial nerve Chorda tympani nerve Tongue Nervus intermedius Pons Superior salivatory nucleus Nucleus and tractus solitarius Sublingual gland Submandibular ganglion/gland the chorda tympani nerve incorporates both parasympathetic efferent and visceral afferent fibres. Visceral afferent fibres convey sensations of taste from the anterior two-thirds of the tongue. The geniculate ganglion incorporates the bipolar cell our bodies of these afferent fibres. Supranuclear management of facial muscular tissues the muscular tissues in the lower face are managed by the contralateral hemisphere, whereas these in the upper face receive management from both hemispheres (bilateral representation). Hence a lower motor neuron lesion paralyses all facial muscular tissues on that aspect, however an upper motor neuron (supranuclear) lesion paralyses only the muscular tissues in the lower half of the face on the opposite aspect. Clinical examination of the facial nerve (see web page 15) In addition to examining for facial weak spot and taste impairment, also notice whether the affected person feedback on decreased lacrimation or salivation on one aspect, or hyperacusis (exaggeration of sounds loss of the stapedius reflex). Symptoms Pain of variable intensity over the ipsilateral mastoid precedes weak spot, which develops over a 48-hour interval. Impairment of taste, hyperacusis and salivation depend on the extent of inflammation and might be misplaced in additional extreme cases. Diagnosis Based on typical presentation and exclusion of middle ear disease, diabetes, sarcoidosis and Lyme disease. There is good evidence prednisolone given in excessive dosage in the acute stage (50 mg per day for 10 days) improves restoration. The role of antiviral remedy is less clear as conflicting outcomes have been found in latest large trials. Eye care (shielding and synthetic tears) is necessary in stopping corneal abrasion. In patients with complete paralysis, electrical absence of denervation on electromyography is an optimistic signal. Occasionally aberrant reinnervation happens movement of the angle of the mouth on closing the eyes (jaw winking) or lacrimation when facial muscular tissues contract (crocodile tears). The stapedius muscle may be affected producing a subjective ipsilateral clicking sound. Contractions are irregular, intermittent and worsened by emotional stress and fatigue. Most cases come up from vascular compression of the facial nerve at the root entry zone (in the identical method as trigeminal neuralgia). Treatment Drugs Local infiltration with botulinum toxin of involved muscular tissues is useful. Flickering of facial muscular tissues outcomes from spontaneous discharge in the facial motor nucleus. Sound waves are transmitted by the tympanic membrane and the ossicles to the oval window, setting up waves in the perilymph of the cochlea. Vestibular function: the vestibular system responds to rotational and linear acceleration (including gravity) and together with a visual and proprioceptive enter maintains equilibrium and body orientation in area. Linear acceleration leads to displacement of the otoliths throughout the utricle or saccule. The cochlear (acoustic) and vestibular divisions journey collectively via the petrous bone to the internal auditory meatus the place they emerge to move via the subarachnoid area in the cerebellopontine angle, every coming into the brain stem individually at the pontomedullary junction. Third order neurons from the inferior colliculus on all sides run to the medial geniculate body on both sides. Fourth order neurons move via the internal capsule and auditory radiation to the auditory cortex. Second order neurons come up in the vestibular nucleus and descend in the ipsilateral vestibulospinal tract. Sensorineural deafness: failure of motion potential production or transmission disease of the cochlea, cochlear nerve or cochlear central connections. Further subdivision into cochlear and retrocochlear deafness helps establish the causative lesion. Pure word or cortical deafness: a bilateral or dominant posterior temporal lobe (auditory cortex) lesion produces a failure to perceive spoken language regardless of preserved listening to. Tinnitus (i) steady or intermittent, (ii) unilateral or bilateral, (iii) excessive or low pitch. Vertigo might outcome from disease of the labyrinth, vestibular nerve or their central connections. Causes of deafness Conductive Cochlear Wax Infection Trauma otitis media* cholesteatoma tympanic membrane rupture ossicular disruption Sensorineural Retrocochlear Cerebellopontine angle tumour acoustic neuroma meningioma epidermoid/dermoid Brain stem disease (associated with other brain stem signs and signs) demyelination syringobulbia herpes zoster vascular insufficiency tumours astrocytoma Otosclerosis Tumours carcinoma glomus jugulare Congenital* . Cerebellopontine angle tumours acoustic schwannoma meningioma epidermoid/dermoid Central (associated with other brain stem signs and signs) Demyelination Vertebrobasilar insufficiency Tumour astrocytoma Syringobulbia Causes of tinnitus Any lesion inflicting deafness may trigger tinnitus. Occasionally patients perceive a vibratory noise inside the pinnacle, transmitted from an arteriovenous malformation or carotid stenosis. Preganglionic parasympathetic fibres come up in the Medulla inferior salivatory nucleus and move to the otic ganglion. General somatic sensory fibres innervate the realm of skin behind the ear, move to the superior ganglion and end in the nucleus and tract of the trigeminal Olivary nerve. Sensory fibres innervate the posterior third of the tongue (taste), pharynx, eustachian tube and carotid Corticospinal body/sinus and terminate centrally in the nucleus solitarius. Within the neck the nerve lies in shut proximity to the internal carotid artery and internal jugular vein. The superior and inferior ganglia lie in the jugular foramen, the otic ganglion in the neck under the foramen ovale. Reflex bradycardia and syncope occur stimulation of vagal nuclei by discharges from glossopharyngeal. The central connections are complicated though similar to these of the glossopharyngeal nerve. Motor fibres supplying the pharynx, soft palate and larynx come up in the nucleus ambiguus. Afferent fibres from the pharynx, larynx and exterior auditory meatus have cell our bodies in the jugular ganglion and end in the nucleus and tract of the trigeminal nerve. Afferent fibres from abdominal and thoracic viscera have cell our bodies in the nodose ganglion and end in the nucleus solitarius. Extracranial branches: Motor and sensory provide to the pharynx Superior laryngeal branch to the laryngeal muscular tissues Recurrent laryngeal branch Supply to thoracic and abdominal viscera Disorders of the vagus nerve trigger: Palatal weak spot Unilateral minimal signs.
Generic 25 mg cyclosporine
The abnormally long cycles undoubtedly include a number of|numerous|a selection of} skipped durations or cycles. Early in the breeding season, by way of March and April, estrus tends to be irregular and long, regularly with no ovulation. From May to July the durations turn out to be shorter and extra common, with ovulation as a standard part of of} the cycle. Fertility rises during estrus to a peak 2 days before the top of estrus, then falls off abruptly. Mares with longer estrous durations should be bred on the third or fourth day and once more 48 to 72 hours later. Mares with common short warmth durations 12 months long} can be successfully bred at any time of the yr. Other mares could have solely silent warmth durations, during which ovulation happens but no sexual desire is clear. Many of those mares conceive if the time for breeding can be recognized by rectal palpation and appearance of the vulva, vagina, and cervix. Ovulation could happen during this period of estrus, and conceptions are possible if mares are bred during a foal warmth. Histologic (tissue) changes in the lining of the genitalia of the mare during the estrous cycle approximate the general sample found in all mammals. Holstein heifers present first estrus at a median of 37 weeks of age on a excessive degree of diet, 49 weeks on a medium degree, and 72 weeks on a low degree of feeding. Puberty appears to happen when the heifer is about two-thirds of her grownup body measurement, measured by height and size quite than weight. This standing warmth averages about 18 hours in each dairy and beef cows, considerably less in heifers. Ovulation normally happens about 10 to 14 hours after the top of estrus in the cow. Conception has occurred in cattle bred as early as 34 hours before ovulation and as late as 14 hours after ovulation. For synthetic insemination, cows that come into standing warmth in the morning are bred the same afternoon, and cows that come into standing warmth in the afternoon are bred the next morning. Bleeding from the vulva happens in a excessive percentage of heifers and cows 1 to 3 days after the top of estrus. This phenomenon is metestrus bleeding; fertility is reduced if breeding is done during bleeding. If ewes fail to attain puberty during their first potential breeding season, they could be over 12 months old before reaching puberty. Ovulation happens close to the termination of estrus, and two or three ovulations could happen in the same estrous period. The ewe is probably the best example of a seasonally polyestrous animal, with a long period of anestrus followed by a breeding season that will vary from 1 to 20 consecutive estrous cycles. The size of breeding season appears to be related to the severity of local weather during which the breed developed. In extreme climates, an acceptable lambing period is restricted; hence, the breeding season is likewise restricted so that lambing happens solely during the favorable time (Scotch Blackface is an example). Breeds developed in milder climates could lamb successfully over a longer period, so the breeding or sexual season can also be|can be} prolonged. Unusually long or short cycles tend to to|are inclined to} appear during the early and later components of the sexual season, quite than during the middle half. Duration of estrus averages about 30 hours, with a spread for many ewes between 24 and 48 hours. The ram could also be} attracted during proestrus and metestrus as well as|in addition to} estrus, but the ewe will settle for him solely Time of Breeding. The common estrous cycle in swine is about 21 days, with a spread of 18 to 24 days considered normal. The estrous period could vary from 15 to ninety six hours, with a median period between forty and forty six hours. The first estrus after weaning is usually longer and will common 65 hours; it happens about 7 to 9 days after weaning of the piglets. It has been advised that this warmth could also be} caused by estrogen from some supply other than the ovary. Ovulation happens during the latter part of of} estrus, in regards to the second day of the cycle. At every period, 10 to 25 ova are shed, with a median of about sixteen for many breeds. The interval, the gestation period, extends from fertilization of the ovum to the start of the offspring. It contains fertilization, the union of the ovum and sperm; early embryonic development in the lumen of the feminine reproductive tract; implantation of the embryo in the uterine wall; placentation, the event of fetal membranes; and continued development of the fetus. A premature start is delivery of a viable fetus before fetal development is full. Even though ejaculated spermatozoa are motile, the major issue in the transport of spermatozoa to the positioning of fertilization is muscular exercise of the tubular genitalia following insemination. The time required for spermatozoa to travel to the positioning of fertilization in a cow is about 2. Oxytocin, a peptide hormone from the neurohypophysis (see Chapter 12), promotes muscular exercise of the feminine tubular genitalia to assist with spermatozoa transport. It is launched in the cow during natural mating and through synthetic insemination, presumably end result of|because of|on account of} a neural reflex initiated by bodily stimulation of the feminine tract. The course of that occurs here to convert nonfertile spermatozoa to fertile spermatozoa is termed capacitation. Capacitation contains changes in or elimination of components of the outer acrosome and plasma membranes so that acrosomal enzymes can later be launched and activated. Part of the natural capacitation course of requires exposure of the spermatozoa to feminine reproductive tract secretions, but capacitation of spermatozoa can be accomplished in vitro utilizing experimentally derived protocols and solutions. Under normal situations, viability and survival occasions of spermatozoa in the feminine reproductive tract are solely a matter of hours. Length of fertility in the feminine tract is as follows: ewe, 30 to 48 hours; cow, 28 to 50 hours; mare, 144 hours. The restricted viability of spermatozoa signifies that insemination must happen inside hours of ovulation so that viable spermatozoa are current when ova arrive for fertilization. In most species, feminine sexual receptivity begins some hours prior to ovulation, so that this is possible. Gamete Fusion and Early Embryonic Development At ovulation, a zona pellucida, a relatively thick membranous structure consisting of crosslinked glycoproteins, surrounds the vitelline membrane (cell membrane or plasma membrane) of the ovum. In most cases, a variable variety of granulosa cells surround the zona, and this layer is termed the cumulus oophorous. Microvilli from the vitelline membrane of the ovum penetrate the zona, as do processes from the granulosa cells. The first polar body, which ends up from the first meiotic division, also accompanies the ovulated ovum throughout the zona (see Chapter 27). The zona pellucida is a semipermeable membrane that helps protect the ovum and that has receptor sites for attachment of spermatozoa during fertilization. During or just after binding and attachment to the zona, spermatozoa undergo a series of events termed the acrosome response. As part of of} this response, domestically launched acrosome enzymes digest a passage by way of the zona. This passage permits spermatozoa to swim their method to the vitelline membrane of the ovum, which is accomplished in a matter of minutes. Multiple spermatozoa could attach to the zona of a single ovum, precise fact} that|although} just one spermatozoon will finally be answerable for fertilization. After penetration of the zona, the cell membrane of the single spermatozoon that will accomplish fertilization attaches to and fuses with the vitelline membrane of the ovum. This initiates the second meiotic division by the ovum, outcomes in|which leads to|which ends up in} formation of the second polar body. Sequence of events from preliminary binding of spermatozoon to zona pellucida to fusion between plasma membranes of spermatozoon and oocyte: A, spermatozoa arrive at website of fertilization; B, preliminary binding of spermatozoon to zona pellucida; C, acrosome response; D and E, penetration of zona pellucida; F, fusion of plasma membranes of spermatozoon and oocytes; G, the cumulus matrix. This, along with changes in the vitelline membrane, prevents polyspermy, entry of more than one spermatozoon into the ovum. This is believed to be rare in most domestic species when fertilization happens in vivo, but the incidence of polyspermy is larger when fertilization is done in vitro.
Cheap 25 mg cyclosporine
Note the presence of bilateral clubbed hands in fetus A (yellow arrows) and radial aplasia in fetus B (white arrows). Note the presence of the next features: quick crown-rump length (1), normal nuchal translucency thickness (2), facial cleft with protrusion and maxillary hole (yellow arrow) (3), and an omphalocele (4). B: A cross section of the umbilical wire in the amniotic cavity of another fetus with trisomy 18 at 12 weeks of gestation. These wire and umbilical vessel abnormalities characterize subtle findings in trisomy 18 and also in trisomy 13 (see. Note the presence of typical craniofacial abnormalities with holoprosencephaly, demonstrated in A (asterisk) and extreme facial cleft in B (arrow). A is obtained by the transabdominal approach and B is obtained by the transvaginal approach. Features of T13 on first trimester ultrasound embrace craniofacial abnormalities. Additional first trimester findings in T18 and T13 fetuses are shown in photographs in various chapters of this book. B: Color Doppler at the four-chamber view in a fetus with trisomy 13 at 14 weeks of gestation. Cardiac findings in fetuses with trisomy 13 are widespread and embrace tachycardia (>175 per minute), intraventricular echogenic foci, an aberrant right subclavian artery, and cardiac defects, predominantly left ventricular outflow tract obstruction. Note the presence in A of hyperechogenic kidneys (arrow) and megacystis (asterisk). Note in B the presence of a single umbilical artery, a finding much like trisomy 18. Fetus in C has trisomy 13 at 12 weeks of gestation and reveals a small omphalocele, another finding commonly seen in trisomy 18 fetuses in early gestation. B: A cross section of the umbilical wire in the amniotic cavity of another fetus with trisomy 13 at 14 weeks of gestation. These wire and umbilical vessel abnormalities characterize subtle findings in trisomy 13 and in trisomy 18 as shown in Figure 6. The "paternal" kind is known as} diandric triploidy and the "maternal" kind is known as} digynic triploidy. These two kinds of triploidy have different features, which may be often differentiated on ultrasound. Note the presence of a marked thickened nuchal translucency (asterisks) in A and fetal hydrops and cystic hygroma in B. Maternal age is often not elevated and the nasal bone is usually ossified (arrows). Fetus A and B has cystic hygromas (asterisks), whereas fetus C has lateral neck cysts (long arrows). B: An axial plane of the chest in another fetus with monosomy X at eleven weeks of gestation. The typical pattern of diandric triploidy includes the presence of a molar placenta. The presence of left ventricular outflow tract anomaly including aortic coarctation or hypoplastic left heart syndrome is a typical finding in fetuses with monosomy X. Note the marked difference in measurement between the abdominal (A) and head (B) circumference, of more than "2 weeks" of gestational age. Note in each fetuses the marked difference in measurement between the abdominal (yellow arrows) and head (white arrows) dimensions. This discrepancy in dimensions between the pinnacle and abdomen is an almost pathognomonic signal of digynic triploidy. In addition, the crown-rump length is considerably quick, reflecting the presence of early growth restriction. Note the marked difference in dimensions between the abdomen (yellow arrows) and the pinnacle (white arrows) in each fetuses. A high detection price for triploidy can also be|can be} achieved with first trimester screening for T21. In a research involving 198,427 girls with singleton pregnancies who underwent first trimester screening between 11+2 and 14+0 weeks of gestation, the overall detection price of triploidy was 25/30 (83. In printed research, the detection price for T21 is at 99% for a false-positive price of 0. This expansion in first trimester ultrasound led to the detection of single or a number of} fetal malformations, which in some circumstances suggested the potential presence of a genetic syndrome. We offered in Chapter 5 four potential pathways that end result in the detection of fetal anomaly in the first trimester. In the absence of a previous family history of a genetic syndrome with fetal anomalies, the de novo analysis of a genetic syndrome in the first trimester kind of|is sort of} challenging. When offered with a constellation of sonographic abnormalities in the second or third trimester of pregnancy, an professional sonologist is often able to to} recommend the presence of a selected syndrome. This is a more challenging task in the first trimester however as the total display of the entire sonographic features of a genetic syndrome is uncommon in early gestation. Nevertheless, there are four ways that syndromic situations are recognized in the first trimester: Figure 6. Chorionic villous sampling revealed a partial monosomy 9q and partial trisomy 2p as unbalanced translocation. The presence of an abnormal karyotype following an invasive diagnostic process similar to trisomies, triploidy, monosomy X and large unbalanced translocations, deletions, and duplications. Monogenic ailments detected by selective molecular genetic examination of a particular condition or with the usage of} next generation sequencing. Genetic syndromes with "affiliation" or "sequence" with no or not yet defined molecular genetic background. The traditional karyotypic analysis will detect the presence of huge balanced or unbalanced translocations. Large chromosomal deletions can also be|may also be|can be} recognized on traditional karyotype analysis as in the majority of deletions 4p- (Wolf Hirschhorn syndrome). Small deletions, termed microdeletions, similar to 22q11 (DiGeorge syndrome), are sometimes too small to be recognized by this methodology. In these circumstances, knowledge of typical sonographic features is needed to be able to} take a look at for the particular gene(s) concerned. Recently, there was an elevated use of selective panels for genetic ailments and sooner or later the usage of} next generation exon or genome sequencing will be more broadly used. Until then, professional sonographers and sonologists should become conversant in fetal anomalies in the first trimester which might be} commonly associated with monogenic inheritance patterns. B: the corresponding axial plane of the pinnacle and C is the 3D ultrasound in surface mode. Prolonged culture of cells from chorionic villous sampling revealed deletion 4p- (red arrow). The capacity to recommend the presence of a potential affiliation of a fetal anomaly with a monogenic kind of inheritance vary primarily based upon the experience of the examiner and the kinds of fetal anomalies. It is comparatively straightforward, for example, to recommend the analysis of MeckelGruber syndrome. The analysis of monogenic syndromes is difficult when anomalies are subtle and expressivity of sonographic markers is incomplete in the first trimester. In this setting, follow-up ultrasound examinations in the early second trimester are required. Follow-up ultrasound at 15 weeks revealed quick ribs, which led us to recommend the presence of short-rib-polydactyly or EllisVan Creveld syndrome, and molecular genetic testing confirmed the diagnoses in each circumstances. Often, genetic ailments are recognized in early gestation routine screening or in diagnostic testing in the presence of maternal or paternal service standing, and before any sonographic markers are current. Examples of such situations embrace cystic fibrosis, tuberous sclerosis, fragile X, thalassemia, sickle cell, storage ailments, and others. Detailed discussion of ultrasound features and genetic testing of all genetic syndromes is past the scope of this book. Interested readers are referred to reference books23 and Internet websites similar to Online Mendelian Inheritance in Man ( Chorionic villous sampling revealed a deletion of the small arm of chromosome 18 (red arrow). Keep in thoughts that noninvasive prenatal testing in such a condition would have missed the analysis.
Cyclosporine 25 mg
The cause of his disorder was attributed to a sudden transition in his circumstances, which, from being easy and comfort able, had been turn into doubtful and precarious; his com plaints had been great pain in the head, virtually a continuous noise in his ears, and, at intervals, a melancholy depres sion, ora frantic exhaltation of spirits. Strong purges, antimonial vomits, ammoniac draughts, sagapenum, steel, and both kinds of hellebore had alter nately been exhibited; points, venaesection, a seton, and vesicatories had been tried. When I undertook the care of this individual, he appeared very impatient of contradiction. Alienation of thoughts, claimed proponents of moral remedies, was not a bodily illness like smallpox, however a psychological disorder, the product of wretched training, dangerous habits, and personal affliction - a traumatic bereavem ent, bankruptcy, or religious horrors like fear of hell. As already hinted, these new psychological approaches had deeper foundations on w hich to construct. From Sophocles to Shakespeare, playwrights has dramatized the passions, exhibiting the inner torm ents of want and responsibility, guilt and grief, that tore personalities aside. His great English successor and critic, Jo h n Locke, depicted insanity as the prod u ct o f defective logical processes or uncontrolled im agination (a view later under lined by Samuel Joh n so n). For by the violence of their Imaginations, having taken 4 their Fancies for Realities, they make right deduction from them. First, patients had to be subdued; then they had to be motivated via m anipulation of their passions - their hopes and fears, their want for esteem. The point was to revive the dormant hum anity of the mad by working on resid ual normal em otions still able to being awakened and trained. Such ideas had been taken several of} levels additional around 1790 by the em ancipatory visions o f Vincenzio Chiarugi in Italy, Philippe Pinel in Paris, the Tukes on the York Retreat, and, maybe extra ambiguously, by Johann Reil and other Rom antic psychiatrists in 292 The C am bridge Illustrated H istory of M edicine the York Retreat - concentrating on the thoughts the York Retreat was opened in 1796 by a group of Quakers, led by a York tea-merchant, W illiam Tuke, to present a refuge for mentally disordered Friends. He had been stricken several of} instances earlier than; and so continually, during the present assault, had he been saved chained, that his clothes had been contrived to be taken off and put on via strings, without removing his manacles. They had been however taken off, when he entered the Retreat, and he was ushered into the aside ment, the place the superintendents had been supping. He was desired to be a part of in the repast, during which he behaved with tolerable propriety. He promised to restrain him self, and he so utterly succeeded, that, during his stay, no coercive means had been ever employed path of|in path of} him. The Tuke family aimed to make the Retreat an entirely dom estic environm ent, in order to keep away from the brutalizing effects of institutional settings. Finding that medicines did little good, they believed that insanity might he cured by reason, m ildness, and the assist provided by a true sense of com m unity: the mad must be handled rath er in the m anner of younger youngsters. At the beginning, alm ost all patients w ere Quakers, like the Tukes them selves, however later the Retreat took patients of all religious persuasions. They needed to be handled like obstreperous youngsters, who required rigorous mental discipline and retraining in thinking and feeling. Throughout Europe and North America, the state accepted enlarged duties for legislating and automobile ing for the mad, and model new} psychiatric career emerged to handle them. In the not-so-distant previous, recalled Charles D ickens in 1852: coercion for the outward man, and rabid physicking the inward man had been. The annual ball offered a chance for patients, employees, and wellwishers to be seen to be a part of} one huge family. Often, howev er, it w as little greater than a publicity event, masking the tedium and penny-pinch ing econom y that marked the routine of relaxation of|the the rest of} the yr in the new (and increasingly huge) public asylums. Traditional establishments like Bethlem, reminders of the dangerous old ways and days, had been investigated and reworked. The eighteenth-century madhouse had been a secret area, hid den from public scrutiny. Institutionalization of the mad was reworked from an ad hoc expedient into a system with targets and ideals. In France, for example, the reforms of Philippe Pinel and the authorized stipulations of the Napoleonic Code had been systematized in the epochal statute o f 1838. This required every departem ent either to set up its own public asylums or to ensure provision of enough amenities for the mad. A comparable reform programme was enacted in England, in the enamel of oppo sition from vested medical interests who feared the profitability of personal asylums would be threatened. Scandals revealing felonious confinem ent o f the sane had already led to one im portant legislative safeguard. Annual renewal of licenses would rely upon satisfactory m aintenance of admissions registers. Magistrates had been empowered to perform visitations (in London, the inspecting body was the Royal College of Physicians). Evidence of gross m ismanagement at Bethlem (where the lately deceased surgeon, Bryan Crowther, had him self been so deranged as to require a straitjacket) led to dis missals. The 1774 Act was strengthened by a succession of laws handed from the 1820s, w hich above all established the Com m issioners in Lunacy, first for London (1 eight 2 8) after which for the entire realm (1 eight 4 4). The Lunacy Comm issioners consti tuted a perm anent body of inspectors (doctors, lawyers, and officials) charged to report on asylums. They also possessed a rem it to standardize and enhance conditions o f care and treat ment. The Com m issioners ensured eradication o f the w orst abuses by insisting on correct patient data and the recording of all instances of bodily coercion. Extending the programme o f ethical therapy, Gardiner Hill and Conolly abol ished all types o f mechanical coercion, not ju st manacles however even straitjackets. Perfect security could be be} achieved, they claimed, via surveillance by vigilant attendants and a regime o f disciplined work and train designed to stimulate the thoughts, tire the body, and foster self-control. At the Lincoln Asylum in 1834, 647 incidents had occurred that required manual restraint; by 1838, there were none in any respect - and this had been achieved with ou t any deaths or suicides. But reformers in France, Germany, and Italy made ingenious use o f the asylum setting. The new career turned preoccupied with the pragmatic points o f managing the well-run asylum. Males had to be separated from females, incurables from curables, the violent from the docile, the clean from the dirty, and pathways o f progress established to allow bettering lunatics to transfer, stage by stage, nearer the exit (and chronic instances to occupy the back wards). Such aims had to be achieved with ou t prejudice to order, econ omy, efficiency, and discipline. He gained a reputation in the nineteenth century as the founder of m odern psychiatry. But dram atic gestures, such as the one here exhibiting Pinel on the Bicetre, had been the stuff m ore of m yth than reality. In lengthy run|the lengthy term}, this legalistic concern to prevent asylums being abused as carceral establishments may have proved counterproductive. Reformers discov ered him in 1 eight 1 4 and publi cized his case as evidence of the cruelty of unreformed Bethlem. The public outcry helped result in the House of Com m ons Inquiry of 1 eight 1 4 into the conditions in mad houses. Instead the mental hospital was confirm ed as the establishment of last resort; certification thus becam e related to prolonged detention. The end result was a failure to present institutional care appropriate for short-term insan ity, partial insanity, or delicate m ental disturbance. In Italy, for example, some 1 eight,0 0 0 had been behind walls in 1881; within 35 years the num ber had greater than doubled. Bureau cratic and utilitarian m entalities vested great religion in institutional options, in bricks and mortar. Reformatories, prisons, hospitals, asylums - all these, it was claimed, would clear up the intensifying social issues induced by rise in popula tion, urbanization, and industrialization. Patient protests grew, complaining of brutality and neglect, as in the dramatic Address to Humanity, Containing a Letter to Dr. T hom as Munro: A Receipt to M ake a Lunatic, and Seize his Estate; and A S ketch o f a True Sm iling Hyena, issued in 1796 by a kind er patient, W illiam Belcher. And a radical fringe within the medical career all the time doubted the efficacy of herding the insane together. But champions lengthy outnumbered critics, and the asylum motion was buoyed up on waves of optimism. This was to change; in the last third of the nineteenth century, model new} pessimism unfold.
Safe 25 mg cyclosporine
Cabin pressures and air flow could be controlled by varying the amount of air forced into the cabin and the amount allowed to escape via adjustable outflow valves (Figure 1-12). The conventional technique for cabin pressurization utilizes two forms of pressurization schedules. Isobaric Control refers to the condition the place the cabin altitude is maintained at a constant altitude or stress because the ambient stress decreases (Figure 1-13). This kind of pressurization system is found in most cargo and passenger carrying aircraft. Pressurization of aircraft cabins represents a wonderful instance of engineering tradeoff. A high differential requires an aircraft construction which is physically stronger and therefore heavier than that required for a lower differential. Pressurization requires an expenditure of energy; therefore, the bigger the differential the greater the facility required to present the desired stress and less energy obtainable for aircraft manuverability. Tactical jet aircraft are geared up with an isobaric- differential pressurization system. This pressurization system senses each cabin and ambient stress and maintains the cabin stress on the idea of exhausting and fast|a set} stress differential of 5 psi. Figure 1-14 shows a typical isobaric-differential pressurization schedule found in Navy tactical jet aircraft. As the aircraft climbs, the aircraft is unpressurized to an altitude of eight,000 ft. From eight,000 ft to roughly 23,000 ft, cabin stress stays at eight,000 ft (isobaric range). For instance, if an aircraft is flying at an indicated ambient altitude of forty,000 ft the place the stress is 2. Advantages of Pressurized Cabins Reducing the probability of hypoxia and decompression sickness are perhaps the 2 most necessary advantages of the pressurized cabin. Cabin temperature, humidity and air flow could be controlled within desired consolation ranges. In massive aircraft, the crew and passengers can move about freely in a cushty environment unencumbered by oxygen masks or other life assist gear. Prolonged passenger flights, air evacuation, and troop actions could be achieved with a minimum of fatigue and discomfort. Protection towards pain within the center ear and sinuses could be provided by allowing the stress within the cabin to rise slowly in a controlled method throughout descent from high altitude to ground stage. Disadvantages of Pressurized Cabins the penalties for the above mentioned advantages are the following disadvantages: 1. Increased structural weight and power of the pressurized space to preserve structural integrity. Additional gear and energy necessities to assist the pressurization, air flow and air con techniques. Maximum efficiency and payload capacity of the aircraft is reduced because of added weight. Possible contamination of the cabin air from smoke, fumes, carbon monoxide, carbon dioxide and odors. Should a speedy decompression occur, the occupants of the aircraft are uncovered to the hazards of hypoxia, decompression sickness, gastrointestinal fuel growth and hypothermia. In addition, the cyclonic winds create the possibility of|the potential of|the potential for} personnel being lost via the opening. Rapid Decompression Aircrew members are confronted with many hazardous elements when performing duties involving flying. Decompression at altitude is elements that may cause vital physiological problems. This kind of decompression is harmful because of the possible insidious impact of hypoxia. They can occur outcome of|because of|on account of} a perforation of the cockpit or cabin wall or unintentional loss of the cover or hatch. Factors Controlling the Rate and Time of Decompression the principal elements that govern the total time of decompression include the cabin quantity, size of the opening, the stress ratio, and the stress differential. The decompression time within a larger cabin space will be considerably slower than that of a cabin with less space. The proportionality of cabin quantity and cross sectional space of the opening dictates the decompression price and time. Variables concerned in figuring out the time of decompression are the stress inside the cabin and the skin ambient stress. If the stress ratio is increased, then could be} presumed that the time for the air to escape will also be increased. The distinction between the interior and external cabin pressures will affect each the rate and severity of the decompression. Physical Characteristics of Rapid Decompression There are a couple of of} bodily and observable traits that assist in the popularity of a speedy decompression. It is because of this explosive noise that some people use the time period explosive decompression to describe a speedy decompression. Air at any temperature and stress has the aptitude of holding simply a lot water vapor. Sudden modifications in temperature or stress, or each, change the amount of water vapor the air can maintain. This reduction in temperature and stress reduces the holding capacity of air for water vapor. If a decompression happens, cabin temperature will equalize with exterior ambient temperature, leading to a major lower in cabin temperature. Upon decompression, the speedy rush of air from a pressurized cabin causes the speed of airflow via the cabin to increase rapidly because the air approaches the outlet. The rush of air has such drive that items not secured will be extracted via the opening. There has been an occasion of an inadequately restrained individual within the instant vicinity of an opening being sucked from the aircraft. The lungs are probably probably the most susceptible part of of} the physique throughout a speedy decompression. Whenever a speedy decompression is quicker than the inherent functionality of the lungs to decompress, a transient optimistic stress will temporarily construct up within the lungs. If the escape of air from the lungs is blocked or significantly impeded throughout a sudden drop in cabin stress, intrapulmonary stress can construct up high sufficient to cause tearing and rupture of the lung tissues and capillaries. If the increasing fuel is free to escape from the lungs via an open airway, the danger of lung harm is nonexistent. Decompression of a pressurized cabin is unlikely to cause symptoms within the center ear and paranasal sinuses. It is extra likely, nonetheless, that individuals will develop pain within the center ear and paranasal sinuses through the subsequent emergency descent as they are going to be uncovered to a large and speedy increase of cabin stress. One of the potential dangers throughout a speedy decompression is the growth of trapped gases inside the gastrointestinal tract causing stomach misery. The diaphragm is displaced upward by the growth of the trapped fuel within the abdomen which might retard respiratory actions. Distention of the stomach organs can also stimulate the stomach branches of the vagus nerve, leading to cardiovascular despair, and if severe sufficient, cause a reduction in blood stress, unconsciousness and shock. Of all the physiological hazards related to the loss of stress, hypoxia is the 1-49 U. The speedy reduction of ambient stress produces a corresponding drop within the partial stress of oxygen and reduces the alveolar oxygen rigidity. The reduced tolerance to hypoxia after decompression as a result of|as a result of} of} (1) a reversal within the path of oxygen circulate within the lung; (2) diminished respiratory exercise on the time of decompression; (3) decreased cardiac exercise on the time of decompression. The incidence of decompression sickness is small until the cabin altitude reaches 25,000 to to 30,000 ft. As the length of exposure to the unpressurized environment increases, so does the incidence of decompression sickness. The incidence of decompression sickness following a speedy decompression seems to be only barely greater than after a sluggish decompression to the same altitude. Again, the extent and severity will be dependent on the altitude and protecting clothes worn through the decompression.
Safe 25mg cyclosporine
The worth of creating the diagnosis is that it lets you convey a good prognosis. Seizure onset is from sleep up to as} 80% of the time (so preliminary perioral features may not be not|will not be} skilled or witnessed) and these features will only be elicited by direct questioning. It is usually handled with mixed, high-dose sodium valproate and ethosuximide. Childhood epilepsy with occipital paroxysms · the more common is the early-onset kind (Panayiotopoulos syndrome). In round 10% of instances, there might be a historical past of febrile seizures preceding onset of absences. Epilepsy with myoclonicastatic (or myoclonic-atonic) seizures (Doose syndrome) · A rare syndrome slightly more common in males. Absence epilepsy with eyelid myoclonia (Jeavon syndrome) · Onset between 2 and 14 yrs, with peak onset at 68 yrs. If myoclonic seizures are distinguished think about myoclonic astatic epilepsy (see b p. The most attribute sample in sleep is paroxysmal fast discharges with a frequency of 1012 Hz. Other treatments embody felbamate, corticosteroids, ketogenic food regimen, and vagus nerve stimulation. The prognosis for cognitive improvement, behaviour and seizure control is mostly poor. There are generalized tonicclonic and myoclonic seizures that happen most commonly soon after waking. Absences are associated with polyspikewave complexes at 46 Hz that gradual to three Hz. There are fluctuating but rapidly progressive issues with comprehension of language, and failure to understand a daily basis} noises (auditory agnosia. Typically, children present a bent to fever-associated seizures, although these can be of a number of} types. Role of imaging Indications for imaging cause much confusion amongst novice epileptologists. The key to understanding the necessity for imaging is to make syndromic and/or aetiological diagnoses. Typical indications embody: · New onset focal epilepsy in a previously developmentally regular youngster, to rule out acquired lesions (infarction, neoplasia, inflammation). Symptomatic epilepsies with imaging abnormalities Cerebral dysgenesis syndromes Often present earlier than 1-mth-old. Symptomatic epilepsies with genetic abnormalities Chromosomal abnormalities 2 Karyotyping is advised in intractable epilepsy or epilepsy with learning difficulties. Chromosomal issues associated with epilepsy generally embody dysmorphic appearances and learning difficulties. Ring chromosomes Cytogenetic abnormalities resulting in ring-form chromosomes could cause epilepsy. Ring chromosome 20 may give severe epilepsy, learning, and behavior issues (often bordering on the psychotic) with out obvious dysmorphism, and the cytogenetic abnormality can be a a|could be a} mosaic so the laboratory should be requested to look at a larger number of mitotic figures (typically 50, but some sources suggest 200). Single-gene issues Seizures are a function of a number of|numerous|a selection of} single-gene issues associated with different features including developmental delay and different neurological indicators. Generally, these issues might be diagnosed on the premise of their different features. Examples to date have largely been channelopathies: mutations in genes coding for subunits of neuronal membrane ion channel proteins, a few of which can have phenotypes with different neurological features. Early affirmation can be helpful in counselling concerning the anticipated emergence of autistic spectrum issues and so on. If the preliminary analysis has not identified a cause of neonatal seizures, think about a big quantity of-individually rare but collectively important- neurometabolic and neurodegenerative conditions. These normally present with seizures within the neonatal interval but can occasionally present as de novo childish spasms. Those children making an ultimately good neurodevelopmental outlook are all on this group. Metabolic and neurodegenerative issues associated with epilepsy in infants and youngsters zero Seizures accompany an unlimited number of neurodegenerative and neurometabolic illnesses. There are, however, comparatively few conditions in which seizures in isolation are probably to|prone to} be the presenting sign, lengthy predating different features. Rare causes of severe epilepsy and severe developmental delay · 3-Phosphoglycerate dehydrogenase deficiency: microcephaly, severe delayed improvement. However non-specific discovering common in small infants with reduced muscle mass. Further support comes from demonstration of low urine creatinine: calcium and creatinine: protein ratios. Neurodegenerative conditions that may present with symptomatic epilepsy in older children. Err on the aspect of living with seizures, quite than unwanted 24/7 drug effects could be|that could be|which could be} far more deleterious developmentally: · monotherapy should be used if possible; · begin gradual and go gradual; · in general, mixture remedy ought to only be used if monotherapy is ineffective since combinations are likely to|are inclined to} be associated with more . Very general rule of thumb for first-line drugs · Generalized epilepsies and syndromes: valproate. Therapeutic ranges are only useful when pharmacokinetic variability outweighs pharmacodynamic variability (differences within the impact of a given drug concentration at the receptor which is basically genetically determined). Children could have well-controlled epilepsy with lower ranges or could tolerate and require larger ranges for full seizure control. Other relative indications are: · Detection of non-adherence (rough ranges should be taken). Consider lamotrigine desire to|instead of|rather than} valproate in ladies of childbearing age (see b p. Good and unhealthy periods can seem to come and go with out apparent purpose: typically spontaneously with out modifications in medication, but more problematically typically when a change has just lately been made. Complaints such as poor concentration might be because of of} undertreatment (incomplete seizure control), overtreatment (drug toxicity), unrelated to remedy (due to the primary cause of the epilepsy), or because of of} a mix of these factors. The only sensible solution to these dilemmas is to change one factor at a time; to make modifications occasionally (resist the temptation to fiddle-a specific danger in an inpatient setting); and assess the results of a change over a interval of weeks (to enable random fluctuations within the condition to manifest themselves). There have to be concordant data from sources, including: · Clinical historical past. Potential surgical candidates · Malformations of cortical improvement including hamartomas if localized and limited to one hemisphere. Typically, fat-derived to non-fat (carbohydrate and protein) energy in a three or 4:1 ratio. Clinical efficacy Observational research (level 4 evidence) present a really variable, but significant full seizure-freedom fee. Unwanted effects Primarily a operate of output current and to a lesser extent pulse length and obligation cycle. Such difficulties could influence mental health and have indirect effects on seizure control. Epilepsy is a person condition, so knowledgeable choices about activities must be made on a person foundation depending on the type and frequency of seizures, properly as|in addition to} the extent of control with medication. The goal should be to maximize participation in all age-appropriate features of life, whilst taking a realistic strategy to risk administration; err on the aspect of inclusion. Neuropsychometry is really helpful to outline educational strengths and weaknesses and aid tailoring of educational support. It is important that pupils with epilepsy take part totally at school life and achieve their full potential. Effective communication between the trainer, dad and mom, physician and youngster must exist. For children with no further bodily or learning difficulties, or medical issues, the goal have to be to allow full participation at school life with provisions made for their safety. For some children, epilepsy is a part of} a wider spectrum of issues needing applicable provision both in mainstream education with support or in a specialist educational setting. Emotional adjustment Adjusting to a diagnosis of epilepsy includes living with unpredictability. Responses · Establish good communication between health, education, and the family.
Quality 25 mg cyclosporine
Except for value of|the price of} pharmaceuticals, expendi ture in the Seventies was not demand-led; and political deci sions managed the availability side o f the system. France sought to lim it expenditure by scrutiny o f medical expenses, espe cially in hospitals, and by controlling the availability o f hospi tal services. Germany, since 1977, has tried to hyperlink the sick-fund expenditure to the national common wage, thus setting a world sum w ithin which numerous varieties o f providers must negotiate their provisions and returns. The coverage o f the retired and o f in medical expertise threatened indefinite low-income households underneath Medicare and Medicaid (1965) was a significant step ahead, but universal cowl remains a a lot contested project (1995). As in France and Germany, new state initiatives have added to the pressures o f reim bursement schemes (commercial or statutory) to produce a significant escalation o f prices and corresponding worries about value containment. The Reagan governments also tried to shift medical work from hospitals to non-hospital practice. Their preferred instrument was the extension o f Health Maintenance Organizations, which undertake the well being care o f their members on exhausting and fast|a set} charge per individual and so are alleged to make the most of cheaper services wherever possible. In Britain, too, since 1979, rightist governments have steered medical services path of|in course of} market preparations. To them it was a bastion o f commerce union ism and producer power, and a huge employer for which a Conservative authorities preferred to not be responsible. Since it concerned neither competitors nor costings, it was by definition inefficient. Thatcherites, like the left, have been suspi cious o f service professionals; distinction to|not like} the left, in addition they tury corporatism and professionalism, w hich develops via the 20 th cen tury till the Seventies, since when it has been increasingly challenged by a resur gence o f liberalism, and a return to (early) Victorian values. Part o f the reason lies in the interaction of econom ics, navy politics, and inhabitants development. In the late eighteenth century, and again in the early twenti eth century, there were strategic and econom ic causes for selling the power of populations via well being care. The neo-liberals preferred markets to service bureaucra cies, even when accounting fo r gadgets o f service required a lot extra administration. In medication, as in different ser vices, professionals have been to be subordinated to managers who have been more acutely aware o f prices. General practi tioners could also operate as businesses, shopping for services from the hospitals o f their choice. Eventually, on this trajec tory, well being services w ill all be provided by unbiased businesses, funded by the state. It remains to be seen whether well being authorities w ill be able to|be capable of|have the flexibility to} safe a steadiness o f services th a t corresponds to pub lic wants somewhat than the interests o f suppliers. Private med icine, which had begun to develop in the Seventies underneath a Labour authorities, boomed in the Eighties as a result of|as a end result of} employers used private as a perk for his or her workforces. Although the private sector remains comparatively small in Britain, the danger o f American-style inequities w ill enhance considerably if neo-liberal governments permit purchasers o f private to scale back their state contributions, or proceed to erode the boundaries between private and public sectors. How ever, hospitals in Britain nonetheless seem as comm unity institu tions, medical charities are popular, and medical schooling remains to be prized. New types o f surgery promise to scale back hospital stays; psychiatric patients are nonetheless being de-institutionalized even after they suffer thereby; the care o f the aged sick has been moved considerably out o f hospitals and into nursing and residen tial houses, for which old people must pay till their capital has almost disappeared. The m arket version o f m edicine could com e to operate at the level of company suppliers and company purchasers, with doctors operating as skilled workers somewhat than as liberal professionals. Such developments, in the affluent W est, will be lim ited in two ways: by the appreciable if dim inishing powers of medical professionals, and by want to|the necessity to} provide adequate m edicine for the poor. Yet, throughout the W estern world, larger schooling is being pushed into quasi-m arket relations and a few American firms have claimed to possess adequate vary and depth of expertise in science, instructing, and administration to provide the sorts of schooling and research presently supplied by prestige universities. One can perhaps imagine a consortium o f m edical-technology and m edical-care com panies establishing a medical faculty, research institute, and instructing hospital, particularly if governments continued to subsidize the scholars and the patients. State services developed in all W estern nations as a result of|as a end result of} m uch of the inhabitants was unable to afford well being care of a standard thought of adequate by them or by governments. Costs can be spread by comm ercial or mutual insurance schem es, but these have always left a considerable residual inhabitants to be cov ered by state welfare, and often to he served by substandard hospitals and clin ics. O f course, the incom es of the poor second are|are actually} m uch larger, relative to subsistence, than they have been in m id-nineteenth-century Britain; but so are the costs o f medical services. The key points for W estern well being care proceed to embody equity and com m u nity. Should we permit techniques that provide the poor with separate, often inferior services? Can we n ot m aintain equitable services such as have been developed by social-dem ocratic governm ents in Scandinavia and Britain? When measured in terms of|when it comes to|by way of} well being requirements against value, such techniques are most likely more efficient than more competitive alternatives and they have the appreciable political benefit of turning equity into the optimistic virtue of solidarity. That the eco nom ically powerful and politically resourceful share provision with the much less fortu nate is one of the best guarantee of efficiency properly as|in addition to} equity. Such preparations second are|are actually} breaking down in jap Europe as econom ies decline and might no longer assist former requirements of service. A small proportion o f the inhabitants purchase W estern medicines in exhausting currencies; the remaining suffer, not ju st from an enormous decline in the actual sources o f common public} system but from diversion of expertise to the private sector and the loss of the social and econom ic co-ordination required to m aintain high-technology medication. M ed ic in e, So ci et y and the State 341 A slum in Jak arta, Indonesia, with the monetary district in the background. W estern m edicines can be found for the rich but not for the poor in creating nations. Some cities in Africa face somewhat comparable problems as their econom ies are mar ginalized and the colonial and post-colonial infrastructure fails to be renewed. In addition, of course, many sub-Saharan states also face problems with subsistence and basic sanitation European states have thought of as solved for at least of|no much less than} a century. The W est keeps a horrified eye on these sufferings; it intervenes at the margins, from an attenuated conscience and a fear of worldwide consequences. Its scientific and technological strategy to ill well being has yielded unrivalled benefits. Illnesses as soon as} unpreventible, signs as soon as} unm anageable, and conditions as soon as} incurable have succum bed to the appliance o f knowledge concerning the body and its workings. Even the regulation o f diminishing therapeutic returns has so far been offset by the expansion in medical research, and the accum ulation of nonetheless more underneath standing. W hile doctors have always had their critics, the previous 20 years have witnessed a sustained assault on the nature of professional medication. The social polem icist Ivan Illich opened his book Lim its to M edicine (1 9 7 6), by declaring that the medical establishm ent has becom e a m ajor risk to well being. The disabling im pact of professional management over medication has reached the proportions of an epidem ic. By way of example, contemplate a research carried out some years in the past at Boston University M edical Center in M assachusetts. A group of doctors followed the progress of greater than eight zero zero patients admitted to the medical wards of their hospi tal. An infected T cell typi cally seems lumpy and the protuberances coloured green in this electron m icrograph are viral particles in the process of budding off from the T-cell membrane. Out of the patients admit ted during the research, 290 developed a number of} iatrogenic disorders - many of them drug-induced. O f these, 76 suffered m ajor com plications, and in 15 cases these contributed to their dying. Although as a specialist clinic the Boston Center receives the sickest and most tough patients, the findings would - to a lesser extent - be true of m ost hospi tals in m ost locations. And alm ost as usually because it fulfills a promise, it seems to create a moral dilemma or immediate an uncom fortable query - m ost essentially concerning the purpose o f medication. If medication succeeded in, for instance, elim inating coronary heart disease, many more of us would reside barely longer but then die of most cancers. Our ignorance of the ageing course of makes it im possible even now to be certain concerning the long-term results of our interventions. The best well being strategy must be to maintain the body in good physical and psychological situation till shortly L o o k i n g t o t he f u t u r e 343 earlier than dying: a longer life and a healthy one. Small marvel, then, that public attitudes to medication veer so disconcertingly from the laudatory to the censorious. These conflicts and contradictions will type the substance of m uch of this chapter. Like clever, on the credit side, no-one in the 1960s or Seventies could have guessed that surgery for peptic ulcers, then so com m on, would becom e a comparative rarity in the late Eighties and Nineteen Nineties. To have accomplished so would have presumed the existence of a (then undiscovered) drug to cease acid secretion in the stomach. And who could have imagined the burgeoning curiosity in immunology, its results on the underneath standing and treatm ent o f infectious disease, and its use as a device in alm ost every department o f medicine?
Best 25mg cyclosporine
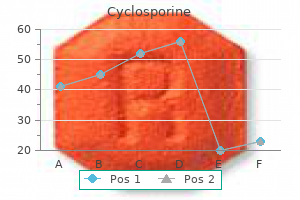
Special consideration is given to the fatiguability of the ocular muscular tissues and the muscular tissues of the limbs. G: the nerves are stimulated electrically, which might demonstrate the defect in their capability to conduct the impulses. Treatment: Anticholinesterase medicine like neostigmine or pyridostigmine are used in the treatment of this illness that strengthens the impulse going from the nerves to the muscular tissues. This helps in the availability of acetylcholine for an extended period, rising the contractibility of the muscular tissues. More than 50% of the patients profit if this surgical procedure is done in the preliminary stage of the illness. Some patients get reduction by a drug known as Azathioprine, however its long-term use causes aspect effects}. In severely afflicted patients, a treatment known as Plasmapheresis is done, in which the patients personal blood is transfused again after purifying it. This process removes the acetylecholine antibodies and different toxins, which trigger the defect in the conduction of the impulse to the muscular tissues. This treatment is attempted when all different treatments have failed and the patient is in severe situation. This treatment can save life of the patient in myasthenic disaster or when the illness reaches the third, fourth or final stage. Another treatment which is as effective as Plasmapheresis however extremely costly is the Immunoglobulin remedy, in which immunoglobulin collected from the blood of healthy individuals or ready synthetically is launched in the patients body in very excessive doses. Usually a dose of 400-mgmlcg-body weight is given per day for 3-5 days the approximate expenditure of this treatment is about 1. The depth properly as|in addition to} the frequency of the illness being different in every patient. If diagnosis is done in the early levels and treatment taken from a specialist most of the patients get reduction and lives can be saved. Only a specialist can determine which drug or remedy is most suitable for a specific patient. This system consists of the big mind, small mind, spinal wire, the nerves emanating from them, the neuromuscular junction and muscular tissues. Duchenne Muscular Dystrophy: this hereditary illness is a sex-linked recessive dysfunction of muscular tissues related to X- chromosome which is present in about 30 per one-Iakh boys. This illness is current from start however its symptoms are observed at the age of three to four years. The child falls while strolling, has difficulty in getting up and climbing stairs with a gradual increase in weak spot. These patients are highly prone to aggressive and life threatening infections of the lungs. Treatment: No everlasting treatment has but been discovered for this illness although steroids can management the illness to some extent. However, physiotherapy and willpower play an important position in supporting these patients. Becker Muscular Dystrophy: this illness is a intercourse linked recessive illness linked to X- chromosome, in which the muscular weak spot is much like that of Duchenne Muscular Dystrophy, however the amount of the weak spot is less and the pace of spreading of the illness is gradual. The primary symptoms of the illness are seen in 5 to 15 years of age and the patient normally lives as much as} four to 5 many years. Limb Girdle Dystrophy: this muscular dysfunction is present in both men and women between the primary and fourth decade of life. This steadily progressing illness causes weak spot in the muscular tissues of the again and shoulders. Congenital myopathy: the muscular problems seen in infants include the central core, nimeline and centro nuclear myopathy. Besides this, any dysfunction of the main a part of} the cells namely mitochondria causes a congenital illness known as mitochondrial myopathy. Metabolic Myopathy: Congenital metabolic problems like glycogen storage, myophosphorylase, lipid storage, and some other mitochondrial myopathies are included on this. Periodic Paralysis: A deficiency of potassium in the blood could cause hypokalemic periodic paralysis in which the shoulder muscular tissues and the thigh muscular tissues weaken. Sometimes, may possibly} additionally have an effect on} the muscular tissues of the eyes properly as|in addition to} the respiratory muscular tissues, which might show fatal if not treated correctly. Hyperkalemic periodic paralysis: An extreme amount of potassium in the blood additionally causes related type of weak spot in the muscular tissues. Paramyotonia congenita: In this dysfunction the muscular weak spot can happen end result of} cold local weather or with none obvious purpose. We will now study intimately concerning the tough illnesses occurring end result of} the irritation of the muscular tissues. Polymyositis and Dermatomyositis: In these illnesses, initially the method of irritation occurs in the muscular tissues and the muscular tissues begin changing into emaciated-wasted. The primary symptom of this illness is the weak spot of the muscular tissues that steadily will increase and makes the patient handicapped. Reddish erythema is seen on the face, again, chest, elbows and knees of the patient. Changes in the protective immune system of the body, produce cells, which destroy the cells of the muscular tissues and hence this illness occurs. Symptoms: the symptoms, their depth and the rate of improvement exhibits plenty of variation. Patients suffer from ache in the muscular tissues specially while climbing steps, getting up from the chair, raising the hand up and so on. Diagnosis: Along with the above talked about symptoms: l There is a rise in the proportion of C. Cyclosporin: this drug helps in controlling the illness nicely, however in the long run|the lengthy term} the aspect effects} of the medication are seen. If physiotherapy is done often everyday basis}, may possibly} forestall the muscular tissues from deteriorating to a certain extent. It is important to get quick advice from the doctor as an alternative of contemplating the issue as an strange ache and letting it deteriorate additional. The response of our thoughts and body in the direction of|in path of} environmental and social challenges in our life recognized as} stress. Stress is pot always unfavorable or harmful; at instances may possibly} have positive effects too. In challenging situations like competitions or exams, stress makes an individual alert and strengthens the efficiency. In tense situations, our body undergoes varied bio chemical adjustments, which produce two kinds of reactions to battle or to run away. During stress, our sympathetic nervous system will get excited, resulting in the secretion of adrenaline and nor-adrenaline from the adrenal gland causing specific reactions in the body. The blood supply to the limbs decreases, whereas the circulation of blood in the muscular tissues will increase. The muscular tissues contract, hands and toes turn into cold, perspiration takes place, hair stands on ends and sometimes shivering could happen. Our senses turn into alert and thus the sense of listening to, seeing and smelling* turns into sharper. Decision power and capacity to analyze the situation enhances and the reminiscence turns into sharper. Behavioural Problems: the temperament turns into angry and irritable, working capacity decreases; the power to differentiate between good and unhealthy and focus turn into poor, the particular person falls a prey to unhealthy habits, loses curiosity in eating or starts overeating. Physical Problems: Headache, asthma, high blood pressure, rheumatism, skin illnesses, heart illness, peptic ulcer, insomnia, seizures, melancholy and so on. According to an estimate, 80% of the illnesses manifested as bodily problems, are literally end result of} mental stress. Stress additionally reduces the immunity of the body, hence recurrent infections can happen. Causes of Stress: There are different stress-causing elements and situations for different folks.
References:
- https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/Downloads/R3669CP.pdf
- https://www.accessdata.fda.gov/drugsatfda_docs/nda/2017/209803%2C209805%2C209806Orig1s000MedR.pdf
- https://www.medschool.lsuhsc.edu/neurology/students/docs/Week%202%20Clinical%20Cases.pdf