.png)
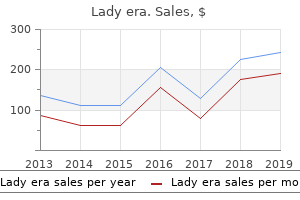
Buy 100 mg lady era
The tendon reflexes are present, and the plantar reflexes are both flexor or extensor. In some cases, the ataxia is later related to spasticity quite than hypotonia (spastic-ataxic diplegia). In the older youngster, a cerebellar gait, ataxia of limb movements, nystagmus, and uneven articulation of phrases are readily distinguished from myoclonus, chorea, athetosis, dystonia, and tremor. Aplasia or hypoplasia of the cerebellum has been observed, but sclerotic lesions of the cerebellum are more widespread. A cerebral and cerebellar lesion may coexist in patients with congenital ataxia, which is the rationale for the time period cerebrocerebellar diplegia. Most importantly, cerebellar ataxia may be the most prominent or sole impact of neonatal ischemia-hypoxia. Radiation of the maternal abdomen through the first trimester of being pregnant is claimed to have resulted in cerebellar hypoplasia. Pontocerebellar Hypoplasias Aside from the congenital ataxia described above, there are a number of uncommon familial types by which a failure of cerebellar development is related to psychological retardation. Joubert reported a household by which there was dysgenesis of the vermis of the cerebellum; psychological retardation; episodic hyperpnea; irregular, jerky eye movements; and unsteady gait. In different reports, choroidalretinal colobomas, polydactyly, cryptorchidism, and prognathism have been mentioned. In the Gillespie syndrome, a mixture of aniridia, cerebellar ataxia, and psychological retardation are the denominating features. These dysgeneses and the disequilibrium syndrome reported from Sweden are unified by the cerebellar ataxia; up to now, they fell into the group of ataxic cerebral palsies. Genetic factors are operative in some, but matters pertaining to etiology remain obscure (see Harding for details). One type of a pure congenital cerebellar hypoplasia has been mapped to a gene locus on chromosome Xq. The ataxia was inherited as an X-linked recessive trait and was nonprogressive past early childhood. Differential Diagnosis of the Congenital Ataxias the congenital ataxias must be distinguished from the progressive hereditary ataxias. Some hereditary ataxias are intermittent or episodic, considered one of which is responsive to acetazolamide, as pointed out on page 827. Also to be distinguished from the ataxias of congenital and neonatal origin is an acute cerebellar ataxia of childhood, which can often be traced to a viral infection or a postinfectious encephalitis, significantly after chickenpox. The opsoclonus-myoclonus ("dancing eyes") syndrome of Kinsbourne is another postinfectious illness peculiar to childhood (see pages 239 and 641). The cerebellar ataxia on this illness may be overshadowed by polymyoclonus, which mars each tried motion. With enchancment, under the affect of corticosteroids, a cerebellar dysfunction of speech and motion turns into evident. A majority of the patients by which the illness grew to become chronic (16 of the 26 cases adopted by Marshall et al) were discovered later to be mentally backward. In the differential prognosis of these acute types of cerebellar ataxia, one should not overlook intoxication with phenytoin, barbiturates, or similar drugs. The Flaccid Paralyses and the "Floppy Infant" (Table 38-5; See additionally pages 946 and 1198) the uncommon cerebral type of generalized flaccidity, first described by Foerster and known as cerebral atonic diplegia, has already been mentioned. It can often be distinguished from the paralysis of spinal and peripheral nerve origin and congenTable 38-5 Causes of congenital hypotonia- the floppy toddler syndrome (see additionally Chap. Polymyopathies-central core, nemaline, rod-physique, myotubular, fiber-kind disproportion B. The Prader-Willi syndrome, discussed earlier in the chapter, additionally presents at first as a generalized hypotonia. The syndrome of infantile spinal muscular atrophy (WerdnigHoffmann illness) is the leading example of flaccid paralysis of lower motor neuron kind. Perceptive moms may concentrate on a paucity of fetal movements in utero; typically the motor defect turns into evident quickly after start or the toddler is born with arthrogrypotic deformities. Several different forms of familial progressive muscular atrophy have been described by which the onset is in early or late childhood, adolescence, or early grownup life. Weakness, atrophy, and reflex loss with out sensory change are the principle features and are discussed in detail in Chap. A few patients suspected of having infantile or childhood muscular atrophy show, with the passage of time, to be merely inactive "slack" children, whose motor development has proceeded at a slower price than regular. These and several other different congenital myopathies- central core, rod-physique, nemaline, mitochondrial, myotubular, and fiber-kind disproportion and predominance- are described in Chap. Unlike WerdnigHoffmann illness, the results of many of them tend to diminish as the natural progress of muscle proceeds. Rarely, polymyositis and acute idiopathic polyneuritis manifest themselves as a syndrome of congenital hypotonia. Infantile muscular dystrophy and lipid and glycogen storage ailments can also produce a scientific picture of progressive atrophy and weakness of muscles. The prognosis of glycogen storage illness (often the Pompe form) must be suspected when progressive muscular atrophy is related to enlargement of the tongue, heart, liver, or spleen. Certain types of muscular dystrophy (myotonic dystrophy and several other forms of congenital dystrophy) can also be evident at start or quickly thereafter. All of these problems are described in detail in the chapters on muscle ailments. Brachial plexus palsies, properly-known problems of dystocia, often end result from forcible extraction of the fetus by traction on the shoulder in a breech presentation or from traction and tipping of the top in a shoulder presentation. Their neonatal onset is betrayed later by the small size and insufficient osseous development of the affected limb. Either the higher brachial plexus (fifth and sixth cervical roots) or the lower brachial plexus (seventh and eighth cervical and first thoracic roots) suffer the brunt of the harm. Upper plexus accidents (Erb) are about 20 occasions more frequent than lower ones (Klumpke). Facial paralysis, because of forceps harm to the facial nerve immediately distal to its exit from the stylomastoid foramen is another widespread (often unilateral) peripheral nerve affection in the newborn. Failure of 1 eye to shut and difficulty in sucking make this condition straightforward to acknowledge. � In most cases of facial paralysis because of physical harm, perform is recovered after a couple of weeks; in some, the paralysis is everlasting and should account for lifelong facial asymmetry. Treatment Assistive gadgets, stretching therapy, and conventional orthopedic measures for joint stabilization and aid of spasticity are all useful. Most printed trials have been too small, nonetheless, to enable firm conclusions to be drawn in regards to the durability of this treatment. Finally, hyperbaric oxygen treatment of youngsters with cerebral palsy was not efficient in a randomized trial conducted by Collet and colleagues, regardless of periodic claims to the opposite. In abstract, it can be said that each one these types of disabling motor abnormalities rank high as essential points in neuropediatrics. In makes an attempt at prevention, steps have been taken in most hospitals to identify and eliminate threat factors. Indeed, better prenatal care, reduction in untimely births, and control of respiratory problems in critical care wards have reduced their incidence and prevalence. Physical and psychological therapeutic measures seem to be useful, but many of the strategies have been troublesome to evaluate in a nervous system undergoing maturation and development. The neurologist can contribute most by segregating groups of cases of equivalent pattern and etiology and in differentiating the congenital groups of delayed expressivity from the treatable acquired ailments of this age interval. We include a dialogue of these intrauterine infections here as a result of some of them may result in malformations or damaging lesions of the mind and, later in life, must be distinguished from developmental abnormalities. The rubella virus enters embryonal tissues through the first trimester, Treponema pallidum in the fourth to fifth postconceptional months, and Toxoplasma after that interval. Bacterial meningitis (apart from that because of Listeria monocytogenes, described below) is basically a paranatal infection contracted during or immediately after parturition. Neonatal herpes simplex encephalitis, because of the kind 2 (genital) virus, can be often acquired by passage by way of an contaminated start canal. Nevertheless, on scientific grounds alone, sure infections may be identified and others excluded.
Syndromes
- AIDS (acquired immunodeficiency syndrome)
- Diaper rash medications
- Fast heart beat
- Zinc oxide ointment
- Breathing difficulty (respiratory failure)
- Chills, sore muscles, and headache
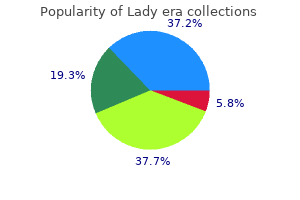
Trusted 100mg lady era
Arteriovenous malformations have been designated by a variety of other terms, such as angioma and arteriovenous aneurysm, however these are less appropriate; angioma suggests a tumor, and the time period aneurysm is mostly reserved for the lesions described within the previous section. Hypertrophic dilated arterial feeders may be seen approaching the primary lesion and to break up into a network of thin-walled blood vessels that join instantly with draining veins. The latter usually type tremendously dilated, pulsating channels, carrying away arterial blood. Arteriovenous malformations occur in all elements of the cerebrum, brainstem, and cerebellum (and spinal wire), but the larger ones are more incessantly discovered within the central part of a cerebral hemisphere, generally forming a wedge-shaped lesion extending from the cortex to the ventricle. Some lie on the dural surface of the mind or spinal wire, however these most often turn out to be direct arteriovenous fistulas, as discussed further on. Arteriovenous malformations are about one-tenth as widespread as saccular aneurysms and about equally frequent in men and women. The first hemorrhage may be deadly, however in more than 90 p.c of cases the bleeding stops and the affected person survives. The fee of hemorrhage in untreated sufferers is established to be 2 to four p.c per 12 months, far lower than for aneurysms. The mortality fee in two main series (Crawford et al, Ondra et al) has been 1 to 2 p.c per 12 months however as excessive as 6 to 9 p.c within the quick 12 months following a primary hemorrhage. Before rupture, chronic, recurrent headache may be a criticism; usually the headache is of a nondescript sort, however a basic migraine with or with out neurologic accompaniment occurs in about 10 p.c of sufferers- most likely with higher frequency than it does within the general inhabitants. Most of the lesions related to migraine-like headaches lie within the parieto-occipital area of 1 cerebral hemisphere, and about two-thirds of such sufferers have a household historical past of migraine. Not sometimes one or each carotid arteries pulsate unusually forcefully within the neck. Exercise that increases the pulse pressure may bring out a bruit if none is current at relaxation. Rarely, skull movies present crescentic linear calcifications within the larger malformations. In the latter examine, comprising 343 sufferers, 217 have been managed with out surgery and observed for a few years (mean, 10. By 20 years after analysis, 29 p.c had died and 27 p.c of the survivors had a neurologic handicap. In almost half of sufferers, the first clinical manifestation is a cerebral subarachnoid hemorrhage; in 30 p.c, a seizure is the first and solely manifestation; and in 20 p.c, the only symptom is headache. Progressive hemiparesis or other focal neurologic deficit is current in about 10 p.c of sufferers. Adams, 464 had a hemorrhage as the first manifestation and 218 had a seizure (primarily with frontal and frontoparietal lesions). In 139, the lesion got here to attention on account of a progressive neurologic deficit; most of those have been situated within the posterior fossa or axially within the cerebrum. Headaches have been an early symptom in 212, however solely 59 of those sufferers had a subsequent hemorrhage. The combination of a prolonged historical past of headaches, seizures, and a progressive deficit almost at all times indicated a large malformation. Small ones may be obscured by hemorrhage; even at autopsy, a careful search under the dissecting microscope may be necessary to find them. In the others, that are inaccessible, makes an attempt have been made to obliterate the malformed vessels by ligation of feeding arteries or by the use of endovascular embolization with liquid adhesives or particular ma- Figure 34-25. Arteriogram displaying large feeding and draining vessels and the characteristic vascular blush of the malformation. The strategy of radiosurgery has been adopted by others using photon radiation sources, such as a linear accelerator, gamma knife, and other modes of centered x-ray radiation, as an accepted alternative to operative therapy of lesions situated in deep regions, including the brainstem, or in "eloquent" areas of the cortex. The relaxation have proven no change at this low dose level, however even on this group, the morbidity and mortality are lower than within the untreated group. In one examine, the chance of hemorrhage was lowered by 54 p.c between the time of radiation and obliteration of the malformation and by 88 p.c thereafter (Maruyama et al). Two kinds of issues of radiation occur at a combined fee of roughly 2 to four p.c. The first is delayed radiation necrosis, which is predictable based mostly on the radiation dose, and the second is a venous congestion that occurs a number of weeks or months after therapy. Most just lately, combined remedy that begins with endovascular discount of the lesion and is adopted by both surgery or radiation has been seen most favorably. In series of sufferers using this strategy, over 90 p.c of lesions could possibly be obliterated with a really low rebleeding fee over a number of years. Even then, there might be differences of opinion based mostly on native assets and experience. Finally, if the first problem is recurrent seizure, successful therapy with discount or cessation of seizures is achieved in a really excessive proportion of cases. There is speedy filing of the cerebral venous system after injection of dye into one inner carotid artery. Dural Arteriovenous Fistulas these curious vascular abnormalities, occurring in each the cranial and spinal dura, have different displays at each web site; the latter type is discussed with other ailments of the spinal wire in Chap. The defining features are radiologic- a nidus of abnormal arteries and veins with arteriovenous shunting contained totally throughout the leaflets of the dura. The lesion is fed by dural arterial vessels derived from the interior cranial circulation and sometimes, more prolifically, from the exterior cranial circulation (exterior carotid artery and muscular branches of the vertebral artery). The speedy transit of injected angiographic dye via these fistulas accounts for the early opacification of the draining venous structures; within the case of excessive-move connections, this may not be seen except images are taken almost immediately after the injection. A number of potential feeding vessels should be injected to show all the conduits into the lesion. In other cases, the dilated draining vessels may be seen solely with the injection of dye or gadolinium. The origin of those vascular lesions has not been settled- a number of mechanisms may be involved. The finest-defined examples are people who come up adjoining to a venous sinus thrombosis or in affiliation with a vascular atresia, most often within the transverse sigmoid sinus or adjoining to the cavernous sinus. In a variety of cases, a dural fistula has appeared after a forceful head damage, usually in a area remote from the positioning of influence. Usually, all of those causes may be excluded and the largest group stays idiopathic. It seems that the dural lesions most vulnerable to bleeding are those situated within the anterior cranial fossa and at the tentorial incisura. In young children, the excessive-move lesions may shunt a lot blood as to cause congestive heart failure, much like malformations of the vein of Galen. Surgery appears preferable for the smaller lesions and embolization for larger and inaccessible ones. Dural fistulas of the spine, that are as widespread because the cerebral ones, symbolize a special problem, discussed on page 1070. The exact incidence of bleeding is unsure however is estimated to be lower than 1 p.c per 12 months per lesion. A small however unsure quantity are related to adjoining venous malformations, visualized by imaging studies. The lack of formation of a mass over a protracted period of time separates this lesion from a malignant tumor that has bled. The inheritance adopted an autosomal dominant sample; Marchuk and coworkers have localized the abnormal gene in other kindreds to the lengthy arm of chromosome 7. One fascinating characteristic of this group, as identified by Labauge and colleagues, is the looks over time of latest lesions in a single-third of sufferers. Treatment Cavernous angiomas on the surface of the mind, within reach of the neurosurgeon, even those within the brainstem, may be plucked out, like clusters of grapes, with low morbidity and mortality. Kjellberg and colleagues have treated 89 deeply situated cavernous angiomas with low-dose proton radiation. Lesions that cause recurrent bleeding and are surgically accessible with little risk are sometimes eliminated, however by the way discovered angiomas and people that are inaccessible may be left alone. Most cavernous angiomas are much smaller and sometimes mulitple however have the identical sign characteristics. Other Causes of Intracranial Bleeding Next to hypertension, anticoagulant remedy is presently the most typical cause of cerebral hemorrhage. The hemorrhages that develop, though sometimes situated within the websites of predilection of hypertensive hemorrhage, are more likely to occur elsewhere, primarily within the lobes of the mind. When the bleeding is precipitated by warfarin remedy, therapy with recent-frozen plasma and vitamin K is recommended; when bleeding is related to aspirin remedy or other brokers that have an effect on platelet perform, recent platelet infusion, usually in large amounts, is required to control the hemorrhage. The use of thrombolytics within the therapy of stroke is sophisticated by intracranial hemorrhage in 6 to 20 p.c of cases, relying on the dose and timing of drug administration after the onset of symptoms, as discussed on page 694.
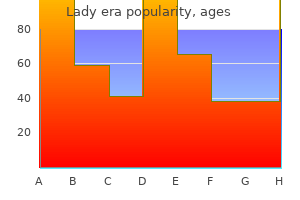
Trusted lady era 100mg
Other Patterns of Evolution In addition to the particular configurations mentioned further on, there are lots of patterns of neuromuscular involvement aside from the one just described. In our expertise this crural amyotrophy is considerably less frequent than the brachial-guide type. Another variant is the early involvement of thoracic, stomach, or posterior neck muscles, the final being one of the causes of head lolling in older individuals. Yet another sample is of early diaphragmatic weakness; such cases come to consideration due to respiratory failure. The sample of extra symmetrical proximal limb or shoulder-girdle amyotrophy with onset at an early age can also be well known and simulates muscular dystrophy (Wohlfart-Kugelberg-Welander illness- page 946). However, this condition extra incessantly turns out to be as a result of a number of sclerosis. The first manifestations could also be a spastic weakness of the legs, during which case a prognosis of major lateral sclerosis could also be made (mentioned further on); only after a yr or two do the hand and arm muscles weaken, waste, and fasciculate. Early on, a spastic bulbar palsy with dysarthria and dysphagia, hyperactive jaw jerk and facial reflexes, but without muscle atrophy, could be the preliminary phase of illness. From time to time, as the illness advances, very mild distal sensory loss is noticed in the toes without clarification, but all the time, if the sensory loss is a definite and early characteristic, the prognosis must remain in doubt. In about half the sufferers, the illness takes the form of a symmetrical (typically asymmetrical) losing of intrinsic hand muscles, slowly advancing to the extra proximal elements of the arms; less typically, the legs and thighs are the websites of the preliminary atrophic weakness; less typically still, the proximal elements of the limbs are affected before the distal elements. Progressive Bulbar Palsy Here reference is made to a condition during which the primary and dominant signs relate to weakness and laxity of muscles innervated by the motor nuclei of the lower brainstem, i. Usually the voice is modified by a combination of atrophic and spastic weakness, as indicated under. Defective modulation of the voice with variable degrees of rasping and nasality is another attribute. The pharyngeal reflex is misplaced, and the palate and vocal cords transfer imperfectly or not at all during tried phonation. Fasciculations and focal loss of tissue of the tongue are normally early manifestations; finally the tongue becomes shriveled and lies ineffective on the ground of the mouth. The jaw jerk could also be present or exaggerated at a time when the muscles of mastication are markedly weak. In reality, spasticity of the jaw muscles could also be so pronounced that the slightest tap on the chin will evoke clonus and blinking; rarely, attempts to open the mouth elicit a "bulldog" reflex (jaws snap shut involuntarily). Commonly, when a jaw jerk is present, a optimistic snout reflex may also be detected, each of those reflect degeneration of the posterior frontal lobe. Spastic weakness of the oropharyngeal muscles could be the preliminary manifestation of bulbar palsy and may at occasions surpass signs of atrophic weakness; pseudobulbar signs (pathologic laughter and crying) could reach extreme degrees. This is the one widespread medical situation during which spastic and atrophic bulbar palsy coexist. As with other types of motor system illness, the course of bulbar palsy is inexorably progressive. Eventually the weakness spreads to the respiratory muscles and deglutition fails entirely; the patient dies of inanition and aspiration pneumonia, normally inside 2 to three years of onset. About 25 percent of cases of motor system illness start with bulbar signs, but rarely if ever does the sporadic form of progressive bulbar palsy run its course as an impartial syndrome (pure heredofamilial types of progressive bulbar palsy in the adult are known but rare). In general, the sooner the onset of the bulbar involvement, the shorter the course of the illness. These cases have distinctive neuropathologic features and are designated as major lateral sclerosis, a term originally suggested by Erb in 1875. A historical evaluate of the topic seems in the article by Pringle and colleagues. Walking continues to be attainable with the assistance of a cane for many years after the onset, but finally this condition acquires the attribute features of a extreme spastic paraparesis. Over the years, finger movements become slower, the arms become spastic, and, if the illness persists for many years, speech takes on a pseudobulbar tone. The legs are sometimes found to be surprisingly sturdy, the problem in locomotion being attributable primarily to rigid spasticity. Pringle and associates recommend that an important diagnostic criterion of the illness is development for three years without evidence of lower motor neuron dysfunction. A rare type begins in the oropharyngeal muscles, as mentioned above, but virtually all the time, atrophy and fasciculations on this same region are evident inside months. Pathologic studies in a restricted number of cases have disclosed a comparatively stereotyped sample of reduced numbers of Betz cells in the frontal and prefrontal motor cortex, degeneration of the corticospinal tracts, and preservation of motor neurons in the spinal cord and brainstem (Beal and Richardson, Fisher, Pringle et al). Whether some of these cases are examples of late-onset familial spastic paraplegia (see further on) has not been explored with molecular techniques. Almost unique amongst cases of this type have been a couple of linked to an adult onset of phenylketonuria or other aminoacidopathies, or to vitamin B12 deficiency. Laboratory Features of Motor Neuron Disease Laboratory investigation supplies useful confirmatory evidence even in the typical medical syndrome. Sensory nerve motion potentials ought to be normal; exams of motor nerve conduction have a standard velocity, but the amplitudes become progressively lower as the illness progresses- in the earliest stages, they too could also be normal. Sensory evoked potentials are mildly abnormal in a proportion of sufferers, but the clarification for this finding is obscure. Motor evoked potentials elicited from the cortex are additionally prolonged in sufferers with outstanding corticospinal signs. Many of the surviving nerve cells are small, shrunken, and full of lipofuscin. According to some reviews, swelling of the proximal axon is an early finding, presumably antedating seen modifications in the cell physique itself. Whitehouse and coworkers found a depletion of muscarinic, cholinergic, glycinergic, and benzodiazepine receptors in areas of the spinal cord where motor neurons had disappeared. The corticospinal tract degeneration is most evident in the lower elements of the spinal cord, but it may be traced up through the brainstem to the posterior limb of the internal capsule and corona radiata by means of fat stains, which show the macrophages that accumulate in response to myelin degeneration. Other fibers in the ventral and lateral funiculi are depleted, imparting a attribute pallor in myelin stains. Motor system illness beginning in the proximal limb muscles could also be misdiagnosed as a limb-girdle type of muscular dystrophy. The primary issues in relation to progressive bulbar palsy are myasthenia gravis and, less typically, polymyositis, muscular dystrophy, and particularly the inherited (Kennedy) type of bulbospinal atrophy, which is mentioned further on. The spastic form of bulbar palsy could recommend the pseudobulbar palsy of lacunar illness. There can also be a rare form of subacute poliomyelitis (presumably viral) in sufferers with lymphoma or carcinoma; it leads to an amyotrophy that progresses to death over a interval of several months. For further discussion of the paraneoplastic number of motor system illness, see page 585. However, we regard this condition of extra diffuse pallor as as a result of a loss of collaterals of motor neurons that contribute to the lamina propria. Several reviews of such a partial spinal amyotrophy have appeared lately (Hirayama et al; Moreno Martinez et al). In the kind described by Hirayama, young men are affected with progressive and asymmetrical amyotrophy of the forearm and hand that has been traced to ligamentous hypertrophy in the ventral spinal canal. This causes a compression of the cervical spinal cord, presumably a continual ischemic effect (page 1077). In a familial number of pure restricted amyotrophy, only the vocal cords grew to become paralyzed over a interval of years in adult life; only later have been the palms affected. We favor the explanation that atrophy of anterior horn cells with aging brings to light a critically depleted motor neuron inhabitants (see further on). A number of cases of this type have been discovered in Ashkenazi Jews by the use of lysosomal enzyme evaluation. An even rarer and recessively inherited childhood form of motor neuron illness (affecting corticospinal more than spinal motor neurons) has been attributed to mutations in a gene whose protein (alsin) is a part of the neuronal cell-signaling pathways. It is obvious that the mobile mechanisms that sustain motor neurons may be disrupted at several websites. Younger and coworkers have found a higher incidence of paraproteinemia in sufferers with motor system illness than may be accounted for by likelihood. It has never been proved that intoxication with heavy metals (lead, mercury, aluminum) may cause motor system illness, although there are reviews of concurrent myelopathic and radicular motor signs in sufferers with lead intoxication. There is little evidence that such cases symbolize a reactivation of the virus or the presence of another infectious agent.
Buy 100mg lady era
If shock was present on admission to the emergency ward, the mortality was sixty five percent. Although the hypotension that follows some accidents is a vasodepressor response and usually comes beneath management with out pressor medication, a big, unimpeded intravenous line should be inserted. Persistent hypotension because of head damage alone is an uncommon prevalence and will always raise the suspicion of a ruptured viscus or thoracic or stomach internal bleeding, intensive fractures, or trauma to the cervical twine. Initially, the infused fluid should be normal saline, avoiding the administration of extreme free water due to its opposed impact on mind edema. Oxygen ought to continue to be administered till it may be shown that the arterial oxygen saturation is normal with out it. A rapid survey can now be made, with consideration to the depth of coma, measurement of the pupils and their response to mild, ocular actions, corneal reflexes, facial actions during grimace, swallowing, vocalization, gag reflexes, muscle tone and actions of the limbs, predominant postures, reactions to pinch, and reflexes. Bogginess of the temporal or postauricular area (Battle signal), bleeding from the nostril or ear, and intensive conjunctival edema and hemorrhage are helpful indicators of an underlying basal skull fracture. However, it should be remembered that rupture of an eardrum or a blow to the nostril may also cause bleeding from these components. Fracture of the orbital bones may displace the attention, with resulting strabismus; fracture of the jaw ends in malocclusion and discomfort on attempting to open the mouth. If urine is retained and the bladder is distended, a catheter should be inserted and kept there. Temperature, pulse, respiration, blood stress, arterial oxygen saturation, and state of consciousness should be checked and charted each hour. A sizable epidural, subdural, or intracerebral blood clot is a sign for quick surgical procedure. The presence of contusions, mind edema, and displacement of central buildings calls for measures to monitor development of these lesions and to management intracranial stress. Nor do the neurologic indicators that represent the Glasgow Coma Scale replicate the stress within the cranium. While the risk of infection is low, prolonged use may be difficult by bacterial meningitis. For this reason, the measurement of serum sodium is in some ways a more accurate reflection of free water depletion. Intravenous fluids with free water should be averted in order not to intensify cerebral edema. This poses a selected hazard in kids who, due to inappropriate secretion of antidiuretic hormone, easily develop water intoxication. With this exception, nevertheless, restriction of the general volume of fluid is less of a priority than effecting a discount in free water. The effects of mannitol have been of great interest to neurosurgeons who treat head trauma, however the most effective plan for its use has never been established. Among the randomized research that present medical information, only the one by Cruz and colleagues has demonstrated a clear profit and significantly in relation to acute subdural hematoma. Attempts to prolong the impact of hypocarbia and the alkalosis by the intravenous administration of ammonium buffers have met with combined success. It has even been instructed that hyperventilation may be harmful to some head-injured sufferers due to a discount in cerebral blood move, but the risk, if any, appears to be minimal. The methodology of deep cooling has had its proponents over the years, however most attempts to reveal improved outcome have been unsuccessful (see Clifton et al). A randomized managed trial of cooling sufferers with severe closed head damage (Glasgow Coma Scale scores of three to 7) to 33 C for 24 h appeared to hasten neurologic recovery and should have modestly improved outcome (Marion et al). It has been instructed by Shann, who has summarized the many trials of hypothermic treatment, that the majority have been unlikely to present profit as a result of the diploma and duration of cooling have been insufficient. The more definitive randomized examine by Eisenberg and associates confirmed no profit from barbiturate-induced anesthesia in headinjured sufferers. Consequently, their use has been deserted except for cases of marked edema surrounding a contusion or hematoma; even then, the profit is unsure (Gudeman et al; Dearden et al; Braakman et al; Saul et al). The use of extensive decompression craniectomy in cases of intractable mind swelling is commented on beneath. Immediately after head damage, the sympathoadrenal response and elevation of blood stress will recede spontaneously in a matter of some hours or days. Unless the blood stress elevation is extreme (greater than a hundred and eighty/95 mmHg), it may be disregarded within the early phases. In animal experiments, it has been discovered that severe hypertension leads to elevated perfusion of the mind and an augmentation of the edema surrounding contusions and hemorrhages. This displays a failure of autoregulatory vascular mechanisms, with resulting transudative edema in damaged areas of the mind. Observations similar to these emphasize the need for quick and vigorous administration of hypotension in severely head-injured sufferers. In decreasing high levels of blood stress, diuretics, beta-adrenergic blocking agents, or angiotensin converting enzyme inhibitors should be used, quite than agents which will dilate the cerebral vasculature (nitroglycerin and nitroprusside, hydralazine, and a few of the calcium channel blockers). General Medical Measures If coma persists for greater than forty eight h, a nasogastric tube should be handed and fluids and nutrition given by this route. Agents that cut back gastric acid production- or the equal, antacids by abdomen tube to hold gastric acidity at a pH above three. Restlessness is managed by diazepam or a similar sedative, however provided that careful nursing fails to quiet the affected person and supply sleep for a couple of hours at a time. Fever is counteracted by antipyretics similar to acetaminophen, and, if needed, by a cooling blanket. The use of morphine or bromocriptine to quiet episodes of vigorous extensor posturing and accompanying adrenergic exercise has already been talked about. The use of decompressive craniectomy in sufferers with progressive and intractable traumatic mind swelling has been a subject of renewed interest in recent years, after having been practically deserted several a long time in the past. Guerra and colleagues have reported on fifty seven such sufferers, principally young adults, who underwent extensive frontotemporal craniectomy, unilateral in 31 and bilateral in 26. Of these, 11 sufferers died, 5 remained in a persistent vegetative state, and 6 survived in a severely damaged condition; nevertheless, 33 sufferers (58 percent) attained surprisingly good states of rehabilitation. These authors have been of the opinion that these results represented a significant enchancment over the anticipated outcome on this explicit group of sufferers. The treatment of different problems attendant on protracted coma has been outlined in Chap. Some features of prognosis have been talked about earlier however the following common comments serve to body the issue. In the survey of the big European Brain Injury Consortium, comprising 10,005 grownup sufferers, the damage proved deadly in 31 percent; three percent have been left in a persistent vegetative state, and sixteen percent remained severely disabled neurologically (Murray et al). Data from the extensively analyzed Traumatic Coma Data Bank are comparable (Marshall et al). The indicators of focal mind disease, whether because of closed head accidents or to open and penetrating ones, have a tendency always to ameliorate as the months cross. Many of the indicators of brainstem disease (cranial nerve dysfunction and ataxia) enhance additionally, usually within the first 6 months after damage (Jennett and Bond) and often to a shocking extent. According to Jennett and Bond, these mental and personality changes are a greater handicap than focal neurologic ones as far as social adjustment is concerned. In open head wounds and penetrating mind accidents, Grafman and coworkers discovered that the magnitude of tissue loss and placement of the lesion have been the primary factors affecting the end result. Russell has identified that the severity of the damage as measured by the duration of traumatic amnesia is a helpful prognostic index. Of sufferers with a period of amnesia lasting lower than 1 h, 95 percent have been again at work within 2 months; if the amnesia lasted longer than 24 h, only eighty percent had returned to work within 6 months. However, about 60 percent of the sufferers in his giant collection nonetheless had signs on the end of two months, and forty percent on the end of 18 months. Of essentially the most severely injured (these comatose for several days), many remained permanently disabled. However, the diploma of recovery was usually higher than one had anticipated; the motor impairment, aphasia, and dementia tended to lessen and generally cleared. Report of the Quality Standards Subcommittee of the American Academy of Neurology. The thought of a demyelinative disease is, roughly, an abstraction that serves primarily to focus consideration on one of many more putting and distinctive features of one group of pathologic processes. The commonly accepted pathologic criteria of a demyelinative disease are (1) destruction of the myelin sheaths of nerve fibers with relative sparing of the other parts of nervous tissue, i.
Order lady era 100 mg
New York, Dover, 1964 (originally published in 1885; reprinted as quantity 1 in the American Academy of Neurology reprint sequence). Clinical manifestations and outcome in eighty two patients treated surgically between 1929 and 1988. When referred to as upon, the doctor must due to this fact be ready to implement a speedy, systematic investigation of the comatose affected person; the necessity for immediate therapeutic and diagnostic motion allows no time for deliberate, leisurely investigation. Some thought of the scale of this class of neurologic disease could be obtained from published statistics. Many years ago, in two large municipal hospitals, it was estimated that 3 p.c of all admissions to the emergency wards were for ailments that had brought on coma. Alcoholism, cerebral trauma, and cerebrovascular ailments were the most common causes, accounting for eighty two p.c of the comatose patients admitted to the Boston City Hospital in previous years (Solomon and Aring). Epilepsy, drug intoxication, diabetes, and extreme infections were the opposite major causes for admission. It is surprising to learn that latest figures from municipal hospitals are a lot the same; they emphasize that the common situations underlying coma are relatively invariant generally medical apply. In university hospitals, which are likely to appeal to more obscure circumstances, the statistics are considerably different. For instance, in the sequence collected by Plum and Posner (Table 17-1), solely onequarter proved to have cerebrovascular disease, and in solely 6 p.c was coma the consequence of trauma. Indeed, all "mass lesions"- such as tumors, abscesses, hemorrhages, and infarcts- made up less than one-third of the coma-producing ailments. A majority were the result of exogenous (drug overdose) and endogenous (metabolic) intoxications and hypoxia. Subarachnoid hemorrhage, meningitis, and encephalitis accounted for one more 5 p.c of the whole. Thus the order is, relatively talking, reversed, but still intoxication, stroke, and cranial trauma stand because the "massive three" of coma-producing situations. Equally common in some sequence, albeit obvious and often transient, is the coma that follows seizures or resuscitation from cardiac arrest. William James once remarked that everybody is aware of what consciousness is until he makes an attempt to outline it. This slender definition has an advantage in that unconsciousness has the other that means- a state of unawareness of self and surroundings Table 17-1 Final prognosis in 500 patients admitted to hospital with "coma of unknown etiology" Metabolic and other diffuse disorders Drug poisoning Anoxia or ischemia Hepatic encephalopathy Encephalomyelitis and encephalitis Subarachnoid hemorrhage Endocrine disorders (including diabetes) Acid-base disorders Temperature regulation Uremic encephalopathy Pulmonary disease Nutritional Nonspecific metabolic coma Supratentorial mass lesions Intracerebral hematoma Subdural hematoma Cerebral infarct Brain tumor Brain abscess Epidural hematoma Thalamic infarct Pituitary apoplexy Closed head injury Subtentorial lesions Brainstem infarct Pontine hemorrhage Cerebellar hemorrhage Cerebellar tumor Cerebellar infarct Brainstem demyelination Cerebellar abscess Posterior fossa subdural hemorrhage Basilar migraine Psychiatric disorders 326 (65%) 149 87 17 14 thirteen 12 12 9 8 3 1 1 101 (20%) forty four 26 9 7 6 4 2 2 1 65 (thirteen%) 40 11 5 3 2 1 1 1 1 8 (2%) Note: Listed here are solely those patients in whom the initial prognosis was uncertain and a last prognosis was established. Some authors make a distinction between the extent of consciousness- that means the state of arousal or the diploma of variation from regular alertness as judged by the appearance of facial muscles, fixity of gaze, and body posture- and the content of consciousness, i. For medical functions, the lack of regular arousal is by far the more necessary and dramatic facet of disordered consciousness and the one recognized by laypersons and physicians as being the central problem in coma. Much more could possibly be said concerning the history of our ideas regarding consciousness and the theoretical problems with regard to its definition. While it serves little practical purpose to evaluate these topics intimately, we note that up to date investigations point out that a constructive strategy is to outline the neurobiological correlates of nicely-defined elements of consciousness. Importantly, these controversies are being informed to some extent by analyses of unusual neurologic disorders, such as those that disturb perception and consciousness of perception (phantom limb, "blindsight," etc. The interested reader is referred to the discussions of consciousness by Crick and Koch, Plum and Posner, Young, and Zeman listed in the references. States of Normal and Impaired Consciousness the following definitions, although most likely not acceptable to all psychologists, are of service to clinicians and can provide the coed and practitioner with a convenient terminology for describing the states of awareness and responsiveness of their patients. In this state the individual is absolutely conscious of a thought or perception and indicates by his conduct and speech the same awareness of self and surroundings as that of the examiner. This regular state might fluctuate during the day from one of keen alertness or deep concentration with a marked constriction of the field of attention to one of mild common inattentiveness, but even in the latter circumstances, the traditional particular person could be introduced instantly to a state of full alertness and performance. Confusion the time period confusion lacks precision, but generally it denotes an incapability to think with customary pace, readability, and coherence. All states of confusion are marked by some extent of inattentiveness and disorientation. This state also implies a level of imperceptiveness and distractibility, referred to traditionally as "clouding of the sensorium. Confusion outcomes most often from a course of that influences the mind globally, such as a poisonous or metabolic disturbance or a dementia. Any condition that causes drowsiness or stupor, includ- ing the natural state that comes from sleep deprivation, leads to some degradation of psychological performance and inattentiveness. A confusional state can even accompany focal cerebral disease in various places, notably in the right hemisphere, or outcome from disorders that disturb primarily language, reminiscence, or visuospatial orientation, but these are readily distinguished from the global confusional state. The affected person might even be roughly oriented as to time and place, with solely occasional irrelevant remarks betraying an incoherence of thinking. Periods of irritability and excitability might alternate with drowsiness and diminished vigilance. Severely confused and inattentive persons are often unable to do more than carry out the best commands, and these solely inconsistently and briefly sequence. Their speech is often limited to a few words or phrases; occasionally the other pertains- particularly, some people are voluble. Occasionally, hallucinatory or delusional experiences impart a psychotic cast to the clinical picture, obscuring the deficit in attention. It tends to be least pronounced in the morning but will increase because the day wears on and peaks in the early evening hours ("sundowning") when the affected person is fatigued and environmental cues are much less clear-minimize. Many occasions that involve the confused affected person depart no hint in reminiscence; actually, the capability to recall occasions of the previous hours or days is one of the most delicate checks of psychological readability. So is using so-referred to as working reminiscence, which requires the short-term storage of the solution of one task to be used in the subsequent. This deficit in working reminiscence, which is such a typical function of the confusional states, could be demonstrated by checks of serial subtraction and the spelling of words (or repeating a telephone number) ahead and then backward. Careful analysis will show these defects to be tied to inattention and impaired perception or registration of information quite than a fault in retentive reminiscence. In some medical writings, notably in the psychiatric literature, the phrases delirium and confusion are used interchangeably, the previous connoting nothing more than a nondescript confusional state by which hyperactivity could also be distinguished. Drowsiness and Stupor In these states, psychological, speech, and bodily exercise are decreased. Drowsiness denotes an incapability to maintain a wakeful state without the applying of external stimuli. The lids droop without closing completely; there could also be snoring, the jaw and limb muscles are slack, and the limbs are relaxed. This state is indistinguishable from mild sleep, with gradual arousal elicited by talking to the affected person or making use of a tactile stimulus. When left unstimulated, these patients shortly drift again into a sleep-like state. Tendon and plantar reflexes and respiration pattern might or will not be altered, relying on how the underlying disease has affected the nervous system. In psychiatry, the time period stupor has been utilized in a second sense- to denote an uncommon condition by which the perception of sensory stimuli is presumably regular but exercise is suspended and motor exercise is profoundly diminished (catatonic stupor). Coma the affected person who appears to be asleep and is on the identical time incapable of being aroused by external stimuli or inner need is in a state of coma. There are variations in the diploma of coma; in its deepest levels, no response of any sort is obtainable: corneal, pupillary, pharyngeal, tendon, and plantar reflexes are in abeyance, and tone in the limb muscles is diminished. With lesser levels of coma, pupillary reactions, reflex ocular movements, and corneal and other brainstem reflexes are preserved in varying diploma, and muscle tone in the limbs could also be elevated. Respiration could also be gradual or speedy, periodic, or deranged in other methods (see further on). In still lighter levels, generally referred to by the ambiguous time period semicoma, many of the above reflexes could be elicited, and the plantar reflexes could also be both flexor or extensor (Babinski signal). Moreover, vigorous stimulation of the affected person or distention of the bladder might trigger a stirring or moaning and a quickening of respiration. The depth of coma and stupor, in comparison in serial examinations, is most useful in assessing the course by which the disease is evolving. Sleep shares numerous other options with the pathologic states of drowsiness, stupor, and coma. These embody yawning, closure of the eyelids, cessation of blinking and swallowing, upward deviation or divergence or roving move- ments of the eyes, lack of muscular tone, lower or lack of tendon reflexes, and even the presence of Babinski indicators and irregular respirations, generally Cheyne-Stokes in kind. Upon being awakened from deep sleep, a normal person could also be confused for a few moments, as each doctor is aware of.
Arctium (Burdock). Lady era.
- How does Burdock work?
- Are there safety concerns?
- What is Burdock?
- Dosing considerations for Burdock.
- Fluid retention, fever, anorexia, stomach conditions, gout, acne, severely dry skin, and psoriasis.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96153
Quality 100mg lady era
Several but not all the different beta-blocking drugs are considerably effective; metoprolol and nadolol, which may be better tolerated than propranolol (in terms of bronchospasm, sleepiness, impotence, and so forth. The relative deserves of different drugs in this class are mentioned in evaluation articles by Louis and by Koller et al (2000), that are recommended for additional steering on remedy. Young and associates have proven that neither propranolol nor ethanol, when injected intra-arterially into a limb, decreases the amplitude of essential tremor. These findings counsel that the therapeutic results of these agents are due much less to blockade of the peripheral betaadrenergic tremorogenic receptors than to the action of these agents on structures inside the central nervous system. It is recommended that remedy be initiated at a low dosage and elevated slowly to 75 mg per day. In each, the bottom hint is an accelerometric recording from the outstretched hand; the higher two traces are surface electromyographs from the wrist extensor (higher) and flexor (middle) muscle groups. The alternate-beat, kinetic-predominant type of essential tremor is harder to suppress but could reply nicely to clonazepam (Biary and Koller); in our experience, nevertheless, this method has not been as profitable. Indeed, the tremor has often been proof against most makes an attempt at suppression by medication. Injections of botulinum toxin can reduce the severity of essential tremor, however the accompanying weakness of arm and hand muscles often proves unacceptable to the affected person. The similar medication injected into the vocal cords can suppress severe voice tremor but caution have to be exercised to keep away from paralyzing the cords. In determined circumstances, a thalamic stimulator of the sort used to treat Parkinson disease (page 924) has been quite profitable and apparently has produced a durable response over a few years; particulars can be discovered in the small research reported by Sydow and colleagues. Parkinsonian (Rest) Tremor this can be a coarse, rhythmic tremor with a frequency of 3 to 5 Hz. The tremor is most frequently localized in one or both hands and forearms and less regularly in the ft, jaw, lips, or tongue. It happens when the limb is in an attitude of repose and is suppressed or diminished by willed motion, no less than momentarily, only to reassert itself as soon as the limb assumes a brand new position. For this cause the parkinsonian tremor is often referred to as a resting tremor, to distinguish it from postural-action tremor, but these terms have to be qualified. Maintaining the arm in an attitude of repose or maintaining it nonetheless in different positions requires a sure diploma of muscular contraction, albeit slight. Usually he maintains a state of slight tonic contraction of the trunk and proximal muscles of the limbs. Parkinsonian tremor takes the type of flexion-extension or abduction-adduction of the fingers or the hand; pronation-supination of the hand and forearm is also a typical presentation. Flexion-extension of the fingers in combination with adduction-abduction of the thumb yields the traditional "capsule-rolling" tremor. It continues whereas the affected person walks, not like essential tremor; indeed, it could first turn into obvious or be exaggerated during walking. The tremor frequency is surprisingly constant over lengthy intervals, however the amplitude is variable. Emotional stress augments the amplitude and should add the results of an enhanced physiologic or essential tremor; with advance of the disease, rising rigidity of the limbs obscures or reduces it. Resting tremor is most frequently a manifestation of the Parkinson syndrome, whether the idiopathic variety described by James Parkinson (paralysis agitans) or the drug-induced type. The tremor of postencephalitic parkinsonism (which is now extinct) often had larger amplitude and involved proximal muscles. In neither disease is there a close correspondence between the diploma of tremor and the diploma of rigidity or akinesia. A parkinsonian type of tremor may be seen in elderly persons without akinesia, rigidity, or masks-like facies. This most likely equates with the sooner talked about alternate-beat type of essential tremor. Patients with the familial (wilsonian) or acquired type of hepatocerebral degeneration may present a tremor of parkinsonian type, normally blended with ataxic tremor and different extrapyramidal motor abnormalities. Stereotactic lesions in the basal ventrolateral nucleus of the thalamus diminish or abolish tremor contralaterally. The state of affairs is made harder because a parkinsonian tremor is often related to an additional tremor of sooner frequency (see above and page 916); the latter is of essential type and responds better to beta-blocking drugs than to antiParkinson drugs. The term ataxic is an appropriate substitute for intention, because this tremor is always mixed with cerebellar ataxia and provides to it, as described in Chap. Its salient feature is that it requires for its full expression the performance of an exacting, precise, projected motion. The tremor is absent when the limbs are inactive and in the course of the first a part of a voluntary motion, but because the action continues and fantastic adjustments of the motion are demanded. Unlike familial and parkinsonian tremors, the oscillations occur in multiple aircraft. As already indicated, this kind of tremor factors to disease of the cerebellum or its connections, notably by way of the superior cerebellar peduncle, but sure peripheral nerve ailments could occasionally simulate it. In such circumstances, the lesion is normally in the midbrain, involving the upward projections of the dentatorubrothalamic fibers and the medial a part of the ventral tegmental reticular nucleus. Because of the location of the lesion in the area of the purple nucleus, Holmes originally referred to as this a rubral tremor. However, experimental proof in monkeys signifies that the tremor is produced not by a lesion of the purple nucleus per se but by interruption of dentatothalamic fibers that traverse this nucleus- i. This type of tremor is seen most frequently in sufferers with multiple sclerosis and Wilson disease, occasionally with vascular and different lesions of the tegmentum of the midbrain and subthalamus, and infrequently as an impact of antipsychotic drugs. It is abolished by a lesion in the reverse ventrolateral nucleus of the thalamus. Betaadrenergic blocking agents, anticholinergic drugs, and L-dopa have little therapeutic impact. Thalamic stimulation could also be helpful in severe circumstances which might be the result of multiple sclerosis lesions in the cerebellar peduncles. The mechanisms involved in the production of intention or ataxic tremor have been mentioned in Chap. Geniospasm this can be a strongly familial episodic tremor disorder of the chin and lower lip that begins in childhood and should worsen with age. Psychic stress and focus are recognized to precipitate the actions, that are described by Danek as "trembling. The disorder have to be distinguished from essential tremor, facial myokymia, and palatal tremor. The trait is inherited in an autosomal dominant trend from a locus on chromosome 9. The frequency of this tremor has been recorded as approximately 14 to sixteen Hz, making it tough to observe and more easily palpable. Nonetheless, it could produce considerable disability because the affected person makes an attempt to stabilize himself in response to the tremulousness. An important accompanying feature is the sensation of severe imbalance, which causes the affected person to assume a widened stance whereas standing; these sufferers are unable to stroll a straight line (tandem gait). We have noticed prominent tonic contraction of the legs during standing, seemingly in an try and overcome imbalance (see Heilman, Thompson et al). Falls are surprisingly rare; due to this fact the situation is often attributed to hysteria. Often step one or two when the affected person begins to stroll are halting, but thereafter, the gait is completely regular. Although some authors such as Wee and colleagues have categorized the disorder as a sort of essential tremor, most of its traits counsel in any other case. The suggestion has been made by Sharott and colleagues that it represents an exaggerated physiologic tremor in response to imbalance; others have discovered an intrinsic rhythm at approximately sixteen Hz generated by the damaged spinal twine in sufferers with myelopathy, suggesting a spinal origin for the tremor. Many of these circumstances have responded to the administration of clonazepam, gabapentin, mysoline, or sodium valproate. Dystonic Tremor Also tough to classify but not to be overlooked are tremors which might be intermixed with dystonia. They tend to be focal in the neck, which is usually rotated slightly to one facet, or they might be evident in one dystonic hand. Hysterical Tremor Tremor is a comparatively rare but quite dramatic manifestation of hysteria, nevertheless it simulates some kinds of organic tremor, thereby inflicting difficulty in analysis. If the affected hand and arm are restrained by the examiner, the tremor could transfer to a more proximal a part of the limb or to one other a part of the body ("chasing the tremor"). Other useful options in identifying hysterical tremor are exaggeration of the tremor by loading the limb- for instance, by having the affected person maintain a e-book or different heavy object, which reduces nearly all different tremors- and the remark of mirror actions in the contralateral hand.
Lady era 100mg
Methylprednisolone remedy in acute spinal cord harm: the myth challenged by way of a structured evaluation of printed literature. Chikuda H, Yasunaga H, Takeshita K, Horiguchi H, Kawaguchi H, Ohe K, Fushimi K, Tanaka S. Mortality and morbidity after high-dose methylprednisolone remedy in patients with acute cervical spinal cord harm: a propensity-matched evaluation utilizing a nationwide administrative database. Range-of-movement restriction and craniofacial tissue-interface stress from four cervical collars. Pre-hospital care administration of a possible spinal cord injured affected person: a systematic review of the literature and proof-based mostly guidelines. In easy phrases, pelvic trauma could be thought of as: � Pelvic ring fractures � High threat life-threatening haemorrhage � Acetabular fractures � May bleed, best problem in surgical reconstruction/long term end result. Beware related hip dislocation � Pubic rami fractures 370 � Generally secure, occur in the elderly but can be a explanation for mobility restricted by pain. The stability of the pelvic ring relies upon upon the rigidity of the bony elements and the integrity of the strong ligaments that bind the three segments collectively. The strongest of these ligaments are the sacroiliac and iliolumbar, supplemented by the sacrotuberous, sacrospinous and the ligaments of the symphysis pubis. The major branches of the frequent iliac vessels come up within the pelvis and are significantly weak to posterior pelvic accidents. The nerves of the lumbar and sacral plexuses are also in danger with these accidents. The bladder lies behind the symphysis pubis and is held in place by the lateral ligaments, and in the male, by the prostate. The prostate is held laterally by the medial fibres of levator ani, and anteriorly is firmly hooked up to the pubic bones by the puboprostatic ligament. In extreme pelvic accidents the membranous urethra is damaged when the prostate is compelled backwards whilst the urethra this chapter will concentrate on pelvic ring fractures because of their important mortality. Pelvic fractures are life-threatening accidents 371 Pelvic Arterial Anatomy stays static. When the puboprostatic ligament is torn, the prostate and base of the bladder can turn into grossly displaced from the membranous urethra. However, the rectum and anal canal are more firmly tethered and weak in pelvic fractures. A force which continues after the pubic symphysis has separated, will sequentially disrupt the anterior then posterior sacroiliac ligaments. If, nevertheless, the posterior ligaments are also in372 jured there shall be each rotational and vertical instability with posterior translation of the injured hemipelvis. Vertical instability is therefore an ominous signal suggesting complete lack of ligamentous support. Pelvic Ring Fractures the major concern with pelvic ring fractures, is that the pelvic quantity could be tremendously increased allowing important hidden haemorrhage from the broken vessels. Venous bleeding can generally be managed by the tamponade impact of decreasing the pelvic quantity. Arterial bleeding is probably not managed by this straightforward measure and these patients might continue to be haemodynamically unstable. Mechanism of Pelvic Injury Certain mechanisms of harm are classically associated with particular kinds of pelvic fracture. Lateral compression (D, E & F beneath) � Side on impression 373 Young-Burgess Classification of Pelvic Fractures � Lateral compression accidents are generally secure as one aspect of the pelvis is crushed in towards the other and actually lower the pelvic quantity. Vertical shear � Fall from top onto one leg (G beneath) � Vertical shear accidents are unstable. In particular relation to pelvic accidents, the abdomen and perineum should be examined for indicators of bruising or swelling. This can be a doubtlessly devastating manoeuvre by dislodging clots and creating additional bleeding. Think - if you suspected a femoral fracture, would you try to disrupt it to assess stability or immobilise it on index of suspicion and x-ray it? Diagnosis of a pelvic ring fracture can often be made by on suspicion from mechanism, inspection or viewing radiographs, leaving this examination unnecessary and anything more then gentle palpation ought to be averted. A rectal examination should be carried out, feeling for location of the prostate and any fractures or tenderness. Neurological examination is essential as there could also be damage to the lumbar/sacral plexus, but as we noticed in the spinal chapter this may be unreliable. Other x-rays, such as inlet/outlet and proper/ left obliques (Judet views) could be helpful and could also be requested following session with the orthopaedic surgeons. In evaluation of the urological tract, the affected person could be encouraged to void urine. If a urethral harm is suspected because of clinical findings, early urological referral is crucial. Further investigations might embrace an intravenous urethrogram or retrograde urethrogram. If a pelvic ring fracture is suspected, early intervention to address a possible increase in pelvic quantity can reduce blood loss. A circumferential strap could be utilized in the pre-hospital setting and ought to be at the stage of the larger trochanters. It is usually essential to control exterior rotation of the ft by strapping collectively. Pelvic ring fractures could be definitively managed with exterior fixators or open reduction and inside fixation, depending on affected person and fracture factors. They can be used to briefly stabilise an unstable ring fracture and are most likely finest utilized in an working theatre by skilled palms. There are only a few, if any, indications for placing an exterior fixator on a haemodynamically unstable affected person in the emergency department. Always beware of the overly-optimistic orthopaedic surgeon who claims that they can be utilized in quarter-hour or less! A pelvic binder takes less than a minute and is simply pretty much as good no less than in the initial levels of care. That said, the C-clamp could be utilized rapidly by a suitably trained and skilled surgeon. Management of patients with indicators of persistent bleeding with a stabilised pelvic fracture is troublesome. This inevitably stops all blood circulate to the decrease half of the body, beneath this point and the clock is ticking as soon as the balloon is inflated. Caution when considering a laparotomy in a affected person with a pelvic fracture, as this process can release any stomach tamponade impact leading to catastrophic pelvic haemorrhage. Experienced surgeons should be available with the ability to pack the pelvis or cross clamp the aorta if required. Apply pelvic strap Presented at London Trauma Conference 2012 A simpler alternative will be the Abdominal tourniquet, which has proven some promise in easy trials. If issues are nonetheless not bettering then different bleeding sources should be excluded, assume 378 Extremity Trauma Extremity trauma is frequent, often dramatic, but hardly ever life threatening. It is essential to be sure that even apparently minor accidents are identified, as later when the affected person has recovered from the initially more important accidents, the potential limb dysfunction can have the best impression on returning to normal activities. Extremity trauma is a huge topic and this chapter aims to give steering on the protected evaluation and initial administration of such accidents. One should not simply contemplate fractures, but also dislocations, traumatic amputations, crush harm, degloving and burns. The pores and skin, musculo-tendinous items, neuro-vascular buildings, bone and joints could be affected and should be appropriately examined. Limb Examination Further limb evaluation often happens in the course of the secondary survey following adequate exposure. Simple fracture patterns Superficial abrasion or contusion attributable to stress from within. Mild to moderately extreme fracture configuration Deep, contaminated abrasion associated with localised pores and skin or muscle contusion. More essential is an consciousness of the mechanism of harm and potential for important gentle tissue involvement. Laceration greater than 1cm long, with extensive gentle tissue damage, flaps, or avulsion. Extensive gentle tissue damage together with muscular tissues, pores and skin and neuro-vascular buildings.
Purchase 100mg lady era
Congenital extrapyramidal disorders (double athetosis; erythroblastosis fetalis and kernicterus) E. For such details, the interested reader should check with several excellent monographs. These are supplemented by special atlases of congenital malformations talked about further on. In this chapter we sketch only the most important teams and discuss in detail a number of of the more frequent illness entities. The classification in Table 38-1 adheres to a grouping in accordance with the principle presenting abnormality or abnormalities. Represented listed below are the frequent issues that lead households to seek session with the pediatric neurologist: (1) structural defects of the cranium, backbone, and limbs, and of eyes, nose, ears, jaws, and pores and skin; (2) disturbed motor operate- taking the form of retarded improvement or irregular movements; (3) epilepsy; and (four) psychological retardation. One has only to walk via an institution for the mentally retarded to respect the remarkable quantity and diversity of bodily disfigurements that attend abnormalities of the nervous system. Smith, in the third edition of his monograph on the patterns of human malformations, listed 345 distinctive syndromes; in the fourth edition (edited by K. Indeed, a traditional-appearing and severely retarded particular person stands out in such a crowd and will incessantly be discovered to have an inherited metabolic defect or birth damage. The intimate relationship between the growth and improvement of the cranium and that of the mind deserves remark. In embryonic life essentially the most quickly rising parts of the neural tube induce special modifications in and at the same time are influenced by the overlying mesoderm (a process generally known as induction); hence abnormalities in the formation of skull, orbits, nose, and backbone are regularly related to anomalies of the mind and spinal cord. During early fetal life the cranial bones and vertebral arches enclose and defend the developing mind and spinal cord; all through the interval of fast mind progress, as pressure is exerted on the internal table of the skull, the latter accommodates to the rising dimension of the mind. This adaptation is facilitated by the membranous fontanels, which remain open until maximal mind progress has been attained; only then do they ossify (close). In addition, stature is managed by the nervous system, as shown by the fact that a majority of mentally retarded people are additionally stunted bodily to a varying degree. Cranial Malformations at Birth and in Early Infancy Certain alterations in dimension and form of the top in the toddler, youngster, or even adult always signify a pathologic process that affected the mind earlier than birth or in early infancy. The dimension of the cranium displays the size of the mind; subsequently the tape measure is one of the most useful tools in pediatric neurology- no examination in a neurologically affected youngster is full without a measurement of the circumference of the top. Graphs of the top circumference in women and men from birth to 18 years of age have been compiled by Nellhaus. A newborn whose head circumference is under the third percentile for age and intercourse and whose fontanels are closed may be judged to have a developmental abnormality of the mind. Enlargement of the Head (Macrocephaly) this may be as a result of factors extrinsic to the mind, such as hydrocephalus and hydranencephalus (as defined under), or excessive mind progress (megaloor macroencephaly) (Table 38-2). The hydrocephalic head is distinguished by several features- frontal protuberance, or bossing; a tendency for the eyes to flip down so that the sclerae are visible between the upper eyelids and iris (sunset signal); thinning of the scalp and prominence of scalp veins; separation of the cranial sutures; and a "cracked pot" sound on percussion of the skull. Infantile hydrocephalus often comes to medical consideration due to an expanding cranium that exceeds regular dimensions for age. The hydranencephalic head (hydrocephalus and destruction or failure of improvement of parts of the cerebrum) is often related to enlargement of the skull. The lack of mind tissue reduces resistance to intraventricular pressure, permitting great enlargement Table 38-2 Causes of macrocephaly 1. This type of destruction of the cerebral mantle in the embryonal interval might lead to the formation of huge defects, with apposition of ventricular and pial surfaces (porencephaly) and subsequent failure of improvement (evagination) of the mind. Yakovlev and Wadsworth referred to the localized failure of evagination as schizencephaly and postulated that it was the results of a focal developmental defect in the wall of the cerebral mantle. They primarily based their interpretation on the discovering of malformed cortex in the margins of the defect, however this would possibly point out only that the lesion preceded neuronal migration. Levine and coworkers have attributed it to a destructive, presumably ischemic lesion occurring in the first few weeks of gestation, at a time when neuronal migration was incomplete. We favor the latter explanation and describe it further in relation to the cerebral palsies. In both occasion, the dearth of resistance of the faulty cerebral mantle to ventricular pressure expands the mind and cranium. Agenesis of the corpus callosum, a standard congenital defect, may be related to macrocephaly and ranging levels of psychological impairment, optic defects, and seizures. In a series of 56 patients with agenesis of the corpus callosum, Taylor and David reported the presence of epilepsy in 32 and ranging levels of psychological retardation in 28; only 9 had no recognizable neurologic defects. In a number of of those patients, an autosomal dominant inheritance has been discovered (Lynn et al). Agenesis of the corpus callosum can also be part of the Aicardi syndrome (see further on) and the Andermann syndrome, and it has been noted in some circumstances of nonketotic hyperglycinemia. Subdural hematomas can also enlarge the top and trigger bulging of the fontanels and separation of the sutures. In the latter condition, the toddler is often irritable and listless, taking nourishment poorly. Infants and children with neurofibromatosis, osteogenesis imperfecta, and achondroplasia even have enlarged heads; in the final condition some extent of hydrocephalus seems to be responsible. Ultrasonography, which can be performed in the prenatal and neonatal intervals, is often diagnostic in all these cranial enlargements. Many of those people come from households with massive heads; Schreier and colleagues, who traced this condition via three generations of some households, declared it to be an autosomal dominant trait. This group represented 20 p.c of 557 kids referred to a clinic due to cranial enlargement (Lorber and Priestley). Hemimegaloncephaly this term refers to a marked enlargement of one cerebral hemisphere as a result of a developmental abnormality. The cortical grey matter and generally the basal ganglia are greatly elevated in volume and weight. Neurons are in disarray and a few are enlarged; in some locations the pure lamination of the cortex is effaced. Nothing is known about causation, however apparently embryogenesis has been deranged at the stage of neuroblast formation. Clinically, most affected people have been mentally retarded and a few are epileptic. A degree of hemiparesis may be current, however extreme hemispheral neurologic deficits are usually not reported. The hemimegalencephaly has been found at post-mortem in a number of people who had no psychological or neurologic deficits. Craniostenoses Some of essentially the most startling cranial deformities are attributable to untimely closure of the cranial sutures (membranous junctions between bones of the skull). Such situations are estimated to happen in 1 of every a thousand births, with a predominance in males (Lyon and Evrard). The progress of the cranium is inhibited in a path perpendicular to the involved suture(s), with a compensatory enlargement in different dimensions, as allowed by the patent sutures. For instance, when the lambdoid and coronal sutures are each affected, the thrust of the rising mind enlarges the top in a vertical path (tower skull, or oxycephaly, additionally referred to as turricephaly and acrocephaly). The orbits are shallow, the eyes bulge, and skull movies show islands of bone thinning (Luckenschadel). When only the sagittal suture is involved, the � head is lengthy and slim (scaphocephalic), and the closed suture projects, keel-like, in the midline. With untimely closure of the coronal suture, the top is excessively extensive and short (brachycephalic). If this condition is acknowledged earlier than 3 months of age, the surgeon could make artificial sutures that will allow the form of the top to turn out to be more regular (Shillito and Matson). Once mind progress has been completed, little can be accomplished aside from advanced reconstructive surgery. When several sutures (often coronal and sagittal) are closed, in order to diminish the cranial capacity, intracranial pressure might enhance, impairing cerebral operate and inflicting headache, vomiting, and papilledema. In acrocephalosyndactyly or Apert syndrome, craniostenoses which are combined with syndactyly (fused, or webbed, fingers or toes), there are often added complications- psychological retardation, deafness, convulsions, and loss of sight secondary to papilledema. The so-known as clover-shaped skull is essentially the most extreme and deadly of the craniostenoses due to the related developmental anomalies of the mind (see further on).
Safe 100mg lady era
The arteritic modifications can also be revealed by arteriography of the exterior carotid arteries. The administration of prednisone, 50 to 75 mg/day, provides putting relief of the headache and polymyalgic symptoms within days and generally within hours and also prevents blindness. The medication have to be given in very steadily diminishing doses for a minimum of several months or longer, guided by the symptoms and the sedimentation fee. Intracranial Granulomatous Arteritis Scattered examples of a small-vessel large-cell arteritis of undetermined etiology by which only brain vessels are affected have come to medical attention over the years. In different instances it has masqueraded as a cerebral tumor, evolving over a period of weeks, or as a viral encephalitis or an uncommon dementia. In contrast to temporal arteritis, the sedimentation fee is generally regular or only slightly elevated. In only about half the sufferers can the analysis be made by angiography, which demonstrates an irregular narrowing and in some instances blunt ending of small cerebral arteries. Occasionally the white matter abnormalities turn into confluent and the radiologic look simulates Binswanger disease or hypertensive encephalopathy. The analysis is made most often by a brain biopsy, which includes a sample of the meninges, but even with tissue sampling, only about half of suspected instances show the standard histopathologic modifications; typically, nonetheless, sufferers with regular angi- Figure 34-31. Carotid angiogram, lateral projection, demonstrating numerous areas of irregular narrowing (arrows) and, in some areas, contiguous slight dilation ("beading"), significantly in the anterior cerebral artery. As identified by Alrawi and colleagues, many sufferers show to have an alternative condition, mainly an infectious encephalitis and brain or intravascular lymphoma, abscess, or Creutzfeldt-Jakob disease. Tissue excised during an operation (or brain biopsy) for a suspected brain tumor, lymphoma, or white matter disease has revealed the attribute vasculitis in some instances; in others the analysis has been made only at post-mortem, the findings coming as a definite shock. The affected vessels are in the 100- to 500-mm vary and are surrounded and infiltrated by lymphocytes, plasma cells, and different mononuclear cells; large cells are distributed in small numbers in the media, adventitia, or perivascular connective tissue. Sometimes only part of the brain has been affected- in certainly one of our instances the cerebellum, in another, one frontal lobe and the opposite parietal lobe. Among an important concerns is the cerebral arteritis attributable to varicella zoster virus, which might simulate in radiographic look granulomatous arteritis and large cell arteritis (page 643). The viral form of arteritis follows or evolves in affiliation with herpes zoster ophthalmicus. As talked about, brain lymphoma of the intravascular type and a number of sclerosis are diagnostic concerns from each a scientific and a radiologic perspective. Some sufferers with isolated central nervous system angiitis (those presenting as an aseptic meningitis with a number of infarcts) have responded to corticosteroid and cyclophosphamide therapy (Moore). Takayasu Disease (Aortic Branch Disease, Occlusive Thromboaortopathy) this can be a nonspecific arteritis involving mainly the aorta and the large arteries arising from its arch. It is similar in many ways to large-cell arteritis apart from its propensity to involve the proximal quite than the distal branches of the aorta. Most of the sufferers have been young Asian girls, but there are scattered reviews of similar instances from the United States, Latin America, and eastern Europe. The actual etiology has never been ascertained, but an autoimmune mechanism is suspected. Constitutional symptoms such as malaise, fever, anorexia, weight loss, and night time sweats often introduce the disease. The affected arteries no longer pulsate, therefore the descriptive time period pulseless disease. However, it should be famous that in non-Asian individuals, the disease is often as a result of atherosclerosis. When renal arteries are involved, hypertension may result, and there may be coronary occlusion, which is usually fatal. Coolness of the palms and weak radial pulses are frequent indicators of the disease and complications are frequent. Blurring of imaginative and prescient, especially upon bodily exercise, dizziness, and hemiparetic and hemisensory syndromes are the usual neurologic manifestations (Lupi-Herrera et al). The inflamed vessels in the thorax are well demonstrated in radionuclide scans using gallium. Pathologic research disclose a periarteritis, typically with large cells and reparative fibrosis. According to Ishikawa and colleagues, the administration of corticosteroids in the acute inflammatory stage of the disease improves the prognosis. Reconstructive vascular surgical procedure has helped a few of the sufferers in the later stages of the disease. The lungs are often spared, nonetheless, which is the idea of distinguishing this form of vasculitis from the allergic granulomatous angiitis of Churg and Strauss, talked about above. The vasa nervorum are incessantly involved by the lesions of polyarteritis, giving rise to a mononeuropathy multiplex or to a symmetrical axonal type of polyneuropathy (see page 1137). The scientific manifestations differ: included are headache, confusion and fluctuating cognitive issues, convulsions, hemiplegia, and brainstem signs. Wegener Granulomatosis this can be a rare disease of unknown trigger, affecting adults as a rule and favoring males slightly. A subacutely evolving vasculitis with necrotizing granulomas of the upper and decrease respiratory tracts adopted by necrotizing glomerulonephritis are its primary options. Neurologic complications come later in a single-third to one-half of instances and take two varieties: (1) a peripheral neuropathy both in a pattern of polyneuropathy or, way more incessantly, in a pattern of mononeuropathy multiplex (page 1138) and (2) a number of cranial neuropathies as a result of direct extension of the nasal and sinus granulomas into adjacent upper cranial nerves and from adjacent to pharyngeal lesions to the decrease cranial nerves (see also page 1188). The basilar elements of the cranium may be eroded, with unfold of granuloma to the cranial cavity and more distant elements. Cerebrovascular events, seizures, and cerebritis are much less frequent neurologic complications. Spastic paraparesis, temporal arteritis, Horner syndrome, and papilledema have been noticed but are rare (see Nishino et al). The orbits are involved in 20 percent of sufferers, and lesions right here simulate the scientific and radiologic look of orbital pseudotumor, cellulitis, or lymphoma. Pulmonary granulomas, often asymptomatic but evident on a chest film, are also frequent. There is a fibrinoid necrosis of their walls and an infiltration by neutrophils and histiocytes. The sedimentation fee is elevated, as are the rheumatoid and antiglobulin elements. A degree of therapeutic success on this previously fatal disease has been achieved by the use of cyclophosphamide, chlorambucil, or azathioprine. Cyclophosphamide in oral doses of 1 to 2 mg/kg per day has cured ninety to 95 percent of the instances. In acute instances, quickly acting steroids- prednisone, 50 to 75 mg/day -should be given in conjunction with the immunosuppressant drug(s). Disturbances of mental operate- together with alteration of consciousness, seizures, and signs referable to cranial nerves- are the usual neurologic manifestations; most often they develop in the late stages of the disease, but they could happen early and may be mild and transient. Hemiparesis, paraparesis, aphasia, homonymous hemianopia, movement issues (chorea), and derangements of hypothalamic operate happen but have been infrequent in our experience. Larger infarcts are often traceable to emboli from Libman-Sacks (nonbacterial thrombotic, marantic) endocarditis. Most of the neurologic manifestations may be accounted for by widespread microinfarcts in the cerebral cortex and brainstem; these, in turn, are related to destructive and proliferative modifications in arterioles and capillaries. Attachment of immune complexes to the endothelium is the postulated mechanism of vascular harm. Other neurologic manifestations are related to hypertension, which incessantly accompanies the disease and may precipitate cerebral hemorrhage; to endocarditis, which may give rise to cerebral embolism; to thrombotic thrombocytopenic purpura, which generally complicates the terminal section of the disease (Devinsky et al); and to remedy with corticosteroids, which may precipitate or accentuate muscle weak point, seizures, and psychosis. A related set of neurologic problems arises in relation to the anti� phospholipid antibody syndrome, which may be a feature of lupus or come up independently (see page 735). With respect to the former, if deep infarctions have occurred, a basal meningitis as a result of tuberculosis, cryptococcosis, or syphilis with occlusion of penetrating vessels must always be entertained. Drug-induced vasculitis is tough to distinguish from a more frequent state of focal vasospasm that may even be induced by these similar agents, as discussed earlier (page 730). Finally, a real cerebral or spinal wire vasculitis can not often be present in affiliation with systemic lymphoma, significantly with Hodgkin disease.
Proven 100 mg lady era
Loss of imaginative and prescient, coarse nystagmus and strabismus, macular cherry-pink spots (in half the instances), flexion pseudocontractures of elbows and knees, kyphoscoliosis, and enlarged liver and sometimes enlarged spleen are the opposite essential clinical findings. Radiographic abnormalities include subperiosteal bone formation, midshaft widening and demineralization of lengthy bones, and hypoplasia and beaking of the thoracolumbar vertebrae. Vacuoles are seen in 10 to eighty percent of blood lymphocytes and foam cells in the urinary sediment. In addition, the epithelial cells of renal glomeruli, histiocytes of the spleen, and liver cells include a modified keratan sulfate and a galactose-containing oligosaccharide. The changes in the bone are additionally like those in the Hurler form of mucopolysac- Infantile Niemann-Pick Disease (Sphingomyelinase Deficiency) that is additionally an autosomal recessive disease. The disease ought to be suspected in an toddler having the facial features of mucopolysaccharidosis and extreme early-onset neurologic abnormalities. A remarkably benign variant, additionally inherited as an autosomal recessive trait, begins later in childhood but could advance so slowly as to allow attainment of adult life. Dystonia, myoclonus, seizures, visual impairment, and macular pink spots had been features of the 2 instances described by Goldman and coworkers. Globoid Cell Leukodystrophy (Krabbe Disease, Galactocerebrosidase Deficiency) that is an autosomal recessive disease with out ethnic predilection, first described by Krabbe, a Danish neurologist, in 1916. The onset is often before the sixth month and infrequently before the third month (10 percent after 1 12 months). Early manifestations are generalized rigidity, lack of head control, diminished alertness, frequent vomiting, irritability and bouts of inexplicable crying, and spasms induced by stimulation. With growing muscular tone, opisthotonic recurvation of the neck and trunk develops. Later signs are adduction and extension of the legs, flexion of the arms, clenching of the fists, hyperactive tendon reflexes, and Babinski signs. Later still, the tendon reflexes are depressed or lost but Babinski signs remain, a sign that neuropathy is added to corticospinal harm. This finding, shared with a number of the other leukodystrophies, is of diagnostic value. In the final stage of the disease, which can happen from one to several months after the onset, the child is blind and often deaf, opisthotonic, irritable, and cachectic. Most sufferers die by the top of the primary 12 months and survival past 2 years is uncommon, although a considerable variety of instances of later onset have been reported (see below). As the disease advances, extra of the cerebral white matter and brainstem turn into concerned. The deficiency ends in the buildup of galactocerebroside; a poisonous metabolite, psychosine, results in the early destruction of oligodendrocytes and depletion of lipids in the cerebral white matter. The globoid cell reaction, however, indicates that impaired catabolism of galactosylceramide can also be essential. Gross examination of the mind discloses a marked reduction in the cerebral white matter, which feels firm and rubbery. The characteristic globoid cells are giant histiocytes containing the accrued metabolite. Visual failure with optic atrophy and a standard electroretinogram is an early finding. Adams, a progressive quadriparesis with gentle pseudobulbar signs, slowly progressive impairment of reminiscence and other psychological functions, dystonic posturing of the arms, and preserved sphincteric control constituted the clinical image. We have noticed another uncommon variant, starting in adult years, with spastic quadriparesis (asymmetrical) and optic atrophy. The nerve conduction velocities in the late-onset form could also be either regular or abnormal. Kolodny and colleagues have reported 15 instances of even later onset (ages 4 to 73 years); pes cavus, optic pallor, progressive spastic quadriparesis, a demyelinating sensorimotor neuropathy, and symmetrical parieto-occipital white matter changes (on imaging studies) had been the principle features. The onset is in the first weeks of life, with a hoarse cry as a result of fixation of laryngeal cartilage, respiratory distress, and sensitivity of the joints, adopted by characteristic periarticular and subcutaneous swellings and progressive arthropathy, main lastly to ankylosis. The diagnostic abnormality is a deficiency of ceramidase, leading to accumulation of ceramide. Seitelberger has obtained pathologic verification of this lesion in instances starting as late as adult years. This disease and Cockayne syndrome are the only leukodystrophies by which nystagmus has been an invariable finding. Koeppen and Robitaille, in a current and thorough review of the topic, summarize the current-day understanding of the pathogenesis, based on misfolding of myelin proteins. Unclassifiable Sporadic and Familial Sudanophilic Leukodystrophies There are two types of such dysfunction, one with early and the opposite with late onset. In the former, onset is before three months, with survival of lower than 2 years; in the latter sort, onset is from three to 7 years and the course is persistent. Psychomotor regression; spastic paralysis; incoordination; blindness and optic atrophy; seizures (uncommon); extreme microcephaly; and absence of skeletal, visceral, and hematologic evidence of the metabolic abnormality are the principle features. Rabinowicz, a brother and sister residing to adolescence, the destroyed white matter was extensively cavitated. Sudanophilic Leukodystrophies and Pelizaeus-Merzbacher Disease these are a heterogeneous group of problems that have in frequent a defective myelination of the cerebrum, brainstem, cerebellum, spinal wire, and peripheral nerves. Morphologic peculiarities and genetic features separate a sure group known as Pelizaeus-Merzbacher disease; other varieties have been artificially delineated; as a result, a comparatively meaningless terminology has been launched. Pelizaeus-Merzbacher Disease that is predominantly an Xlinked disease of infancy, childhood, and adolescence and consists of other carefully related pathologic entities with completely different modes of inheritance. Koeppen and associates have provided evidence of a defective synthesis of this protein. The onset of symptoms is most often in the first months of life; other instances start later in childhood. The first signs are abnormal actions of the eyes (rapid, irregular, usually asymmetrical pendular nystagmus), jerk nystagmus on extremes of lateral actions, upbeat nystagmus on upward gaze, and hypometric saccades (Trobe et al). There is spastic weak point of the limbs, optic atrophy (usually with unexplained retention of pupillary gentle reflex), ataxia of limb motion and intention tremor, choreiform or athetotic actions of the arms, and sluggish psychomotor growth with delay in sitting, standing, and strolling. In later-growing instances, pendular nystagmus, choreoathetosis, corticospinal signs, dysarthria, cerebellar ataxia, and psychological deterioration are the main manifestations. There are milder instances of later onset with behavioral peculiarities and lack of tendon reflexes and, hardly ever, pure spastic paraparesis. In the most extreme instances, Seitelberger has noticed an absence of oligodendrocytes and myelinated fibers. It is hypothesized that proteolipids accumulate in the endoplasmic reticulum of the oligodendrocytes, resulting in apoptosis. One group of instances resembles the Cockayne syndrome (page 824), with photosensitivity of skin, dwarfism, cerebellar ataxia, corticospinal signs, cataracts, retinitis pigmentosa, and deafness. Pathologically, islands of preserved myelin impart a tigroid sample of degenerated and Spongy Degeneration of Infancy (Canavan-van Bogaert-Bertrand or Canavan Disease) that is an autosomal recessive disease described in 1931 by Canavan as a form of Schilder disease (see Chap. Onset is early, often recognizable in the first three months of life and sometimes in the first neonatal weeks. There is either a scarcity of growth or rapid regression of psychomotor perform, lack of sight and optic atrophy, lethargy, difficulty in sucking, irritability, lowered motor exercise, hypotonia adopted by spasticity of the limbs with corticospinal signs, and an enlarged head (macrocephaly). An fascinating but unexplored facet of the disease is the prevalence of blond hair and light-weight complexion in affected members, in contrast to the darker hair and complexion of their regular siblings (Banker and Victor). Instead, after a protracted interval of constipation, sleep disorder, and orthostatic hypotension throughout adolescence, bulbar symptoms (dysarthria, dysphonia, and dysphagia), seizures, and in some instances ataxia gradually emerged throughout adult years. Alpers Disease this can be a progressive disease of the cerebral gray matter, recognized additionally as progressive cerebral poliodystrophy or diffuse cerebral degeneration in infancy. A familial form (in all probability autosomal recessive) as properly many sporadic instances has been reported. In some situations, the late onset of jaundice and fatty degeneration or cirrhosis of the liver have been described (Alpers-Huttenlocher syndrome); the hepatic changes are distinctive and possibly not related to using anticonvulsant medication, as had been hypothesized (Harding et al). The nature of this combined hepatic-cerebral degeneration remains unexplained, but some situations have been related to the mitochondrial problems, as famous below. Neuropathologic examination exhibits marked atrophy of the cerebral convolutions and cerebellar cortex, with lack of nerve cells and fibrous gliosis ("walnut mind"). In some instances, the spongiform vacuolization of the gray matter of the mind resembles that seen in Creutzfeldt-Jakob disease. Hypoglycemic, hypoxic, and hypotensive encephalopathies must at all times be thought-about in the prognosis but can often be eradicated by knowledge of the clinical circumstances at the onset of the sickness. A variety of biochemical abnormalities have been identified in sufferers with Alpers disease, together with pyruvate dehydrogenase deficiency, decreased pyruvate utilization, dysfunction of the citric acid cycle, and decreased cytochromes a and aa3.
References:
- https://thrive.kaiserpermanente.org/care-near-you/northern-california/santarosa/wp-content/uploads/sites/15/2015/10/Conjunctivits-Styes_tcm28-489813.pdf
- https://www.accessdata.fda.gov/drugsatfda_docs/nda/2019/209379Orig1s000MultiDisciplineR.pdf
- https://www.healthinfotranslations.org/pdfDocs/ViralHepatitis_Viet.pdf
- https://cdn.ymaws.com/www.alaskachiropracticsociety.com/resource/resmgr/Events/2014_Ankylosing_Spondylitis.pdf
- http://www.ajnr.org/content/ajnr/15/4/689.full.pdf