.png)
Generic chitosan 500mg
Interdischarge Interval: Time between consecutive discharges of the same potential. Interference: Unwanted electric exercise recorded from the encircling environment. Interference Pattern: Electric exercise recorded from a muscle with a needle electrode during maximal voluntary effort. A full interference pattern implies that no particular person motor unit action potentials can be clearly identified. The term discrete exercise is used to describe the electrical exercise recorded when each of several totally different motor unit action potentials can be identified in an ongoing recording as a result of limited superimposition of waveforms. The term single unit pattern is used to describe a single motor unit action potential, firing at a speedy fee (must be specified) during maximum voluntary effort. The drive of contraction related to the interference pattern must be specified. The following are measured within the time area: (1) the number of turns 852 Glossary of Electrophysiologic Terms per second and (2) the amplitude, outlined because the imply amplitude between peaks. International 10�20 System: A system of electrode placement on the scalp by which electrodes are positioned both 10% or 20% of the total distance on a line on the cranium between the nasion and inion within the sagittal airplane and between the best and left preauricular points within the coronal airplane. Interpeak Interval: Difference between the height latencies of two components of a waveform. Intraoperative Monitoring: using electrophysiological stimulating and recording methods in an working room setting. The term is often utilized to methods which are used to detect injury to nervous tissue during surgical procedure or to information the surgical process. The condition underneath which they occur must be described, for example, spontaneous or reflex potentials. Isoelectric Line: In electrophysiologic recording, the show of zero potential difference between the two input terminals of the recording apparatus. In conditions of disturbed neuromuscular transmission, together with early reinnervation and myasthenic issues, the variability can be sufficiently massive to be simply detectable by eye. Jitter: the variability of consecutive discharges of the interpotential interval between two muscle fiber action potentials belonging to the same motor unit. Jolly Test: A approach named after Friedrich Jolly, who utilized an electric current to excite a motor nerve repetitively whereas recording the drive of muscle contraction. Kinematics: Technique for description of physique movement without regard to the underlying forces. Late Component (of a Motor Unit Action Potential): See most well-liked term, satellite tv for pc potential. Late Response: A basic term used to describe an evoked potential in motor nerve conduction research having an extended latency than the M wave. The onset latency is the interval between the onset of a stimulus and the onset of the evoked potential. The peak latency is the interval between the onset of a stimulus and a specified peak of the evoked potential. Latency of Activation: the time required for an electric stimulus to depolarize a nerve fiber (or bundle of fibers as in a nerve trunk) past threshold and to initiate an action potential within the fiber(s). An equivalent Glossary of Electrophysiologic Terms 853 term, now rarely used, is the "utilization time. Lipoatrophy: Pathologic lack of subcutaneous fat and connective tissues overlying muscle which mimics the medical look of atrophy of the underlying muscle. Long-Latency Reflex: A reflex with many synapses (polysynaptic) or a protracted pathway (lengthy-loop) in order that the time to its occurrence is bigger than the time of occurrence of brief-latency reflexes. Long-Loop Reflex: A reflex thought to have a circuit that extends above the spinal section of the sensory input and motor output. Should be differentiated from reflexes arising from stimulation and recording within a single section or adjoining spinal segments. M Wave: A compound muscle action potential evoked from a muscle by an electric stimulus to its motor nerve. By convention, the M wave elicited by a supramaximal stimulus is used for motor nerve conduction research. Ideally, the recording electrodes must be positioned in order that the preliminary deflection of the evoked potential from the baseline is unfavorable. Normally, the configuration is biphasic and steady with repeated stimuli at gradual rates (1�5 Hz). The following traits can be specified quantitatively: (1) maximal peakto-peak amplitude, (2) space contained underneath the waveform, and (3) number of phases. Malignant Fasciculation: Used to describe massive, polyphasic fasciculation potentials firing at a gradual fee. Membrane Instability: Tendency of a cell membrane to depolarize spontaneously in response to mechanical irritation or following voluntary activation. May be used to describe the occurrence of spontaneous single muscle fiber action potentials similar to fibrillation potentials during needle electrode examination. Microneurography: the strategy of recording peripheral nerve action potentials in humans via intraneural electrodes. Special methods are needed to produce this measurement in motor or sensory nerves. Mononeuritis Multiplex: A dysfunction characterised by axonal injury and/or demyelination affecting nerve fibers in a number of nerves (a number of mononeuropathies). Mononeuropathy Multiplex: A dysfunction characterised by axonal injury and/or demyelination affecting nerve fibers completely along the course of one named nerve. Monophasic Action Potential: An action potential with the waveform totally on one facet of the baseline. Despite the term monopolar, a separate floor or subcutaneous reference electrode is required for recording electric indicators. May even be used as a cathode in nerve conduction research with one other electrode serving as an anode. Motor Latency: Interval between the onset of a stimulus and the onset of the resultant compound muscle action potential (M wave). The term could also be certified, as proximal motor latency or distal motor latency, depending on the relative position of the stimulus. Motor Nerve: A nerve containing axons which innervate extrafusal and intrafusal muscle fibers. These nerves additionally include sensory afferent fibers from muscle and different deep constructions. Motor Neuron Disease: A medical condition characterised by degeneration of motor nerve cells within the mind, mind stem, and spinal cord. Primary lateral sclerosis happens when degeneration affects mainly corticospinal tract motor fibers. Amyotrophic lateral sclerosis happens when degeneration affects each corticospinal tracts and decrease motor neurons. Motor Point: the location over a muscle the place its contraction could also be elicited by a minimal intensity brief-period electric stimulus. Motor Response: (1) the compound muscle action potential (M wave) recorded over a muscle in response to stimulation of the nerve to the muscle. Motor Unit: the anatomic component consisting of an anterior horn cell, its axon, the neuromuscular junctions, and all of the muscle fibers innervated by the axon. The following measures could also be specified, quantitatively if potential, after the recording electrode is positioned randomly inside the muscle: 1. Recruitment traits (a) Threshold of activation (first recruited, low threshold, excessive threshold). A variety of methods, together with spike-triggered averaging, incremental motor nerve stimulation, F-wave measurement, or a Poisson statistical approach can be used. Synonyms can embody motor unit number estimation and motor unit number estimating. Motor Unit Territory: the realm of a muscle cross part within which the muscle fibers belonging to an individual motor unit are distributed. Movement-Related Cortical Potential: Electroencephalogram exercise related to (earlier than and after) a voluntary movement. There are several components together with the Bereitschaftspotential earlier than the movement and the motor potential at in regards to the time of the movement. Multifocal Motor Neuropathy: A disease characterised by selective focal block of motor nerve conduction in a number of nerves.
Cheap chitosan 500mg
Oral antibiotics are indicated when regional lymphadenitis or erythema/cellulitis is current. Medial spread entails the center ear and the mastoid, whereas anterior spread entails the temporomandibular joint. Surgical intervention is indicated to identify organisms when nerve involvement or overseas body obstruction is suspected. In the previous, counseling may be needed on correct ear hygiene; in the latter, over-the-counter ear drops containing an alcohol/glycerine mixture could be really helpful for use after bathing or swimming. These signs relate to irritation and irritation of the mucosa and elevated nasal secretions. Antigen challenge in prone hosts, histamine challenge, or activating nonmyelinated nerves with substance P can reproduce signs found in acute allergic reactions and acute rhinitis. Subacute and continual signs and nasal obstruction result from the activation of mucosal prostanoids and cytokine networks to promote the nasal inflammatory response, recruit inflammatory cells, and promote therapeutic. Acute insults take 3 to 5 days to resolve unless bacterial superinfection, concomitant eustachian tube or sinus obstruction, or repeated publicity to a causative noninfectious agent or allergen occurs. A persistent inflammatory state can develop in prone individuals and lead to continual signs, nasal polyps, and altered or decreased sense of scent (anosmia). The severity of viral infections could be attenuated by amantadine or related brokers if taken near the time of publicity. Topical decongestants like oxymetrazoline, used as directed, relieve nasal obstruction; however, rebound congestion and the potential problems of continual vascular constriction observe if remedy is extended past 1 week. Bacterial superinfection presenting as sinusitis or otitis must be suspected if recurrent fever, regional lymphadenopathy, persistent mucopurulent discharge, or persistent signs last more than 5 days. Most circumstances occur as a complication of the widespread cold or different higher respiratory tract infections, with occasional presentations as a result of extension of a periodontal infection under the maxillary sinus. Less than 1% of higher respiratory tract infections result in the scientific syndrome of acute sinusitis, and fewer meet the factors for continual sinusitis. Normal mild transmission to the frontal sinus from the supraorbital ridge or to the maxillary sinus via the onerous palate excludes sinusitis; lowered or absent transmission is less useful as a result of appreciable intraindividual anatomic variation exists. A coronal computed tomography image with bone window settings is the popular test. Magnetic resonance imaging and ultrasonography have limited but specialized applications. Sinus aspiration and endoscopic sinuscopy may be essential to recuperate organisms or to impact drainage. Surgical interventions are indicated for therapy failure, suppurative problems, diagnosis of nosocomial infection, and fever of unknown origin with sinus opacification. Most causes of sinusitis are bacterial infections similar to people who produce otitis. The course of acute sinusitis is 3 to four weeks due to the anatomic difficulties in drainage. The routine use of antihistamines is controversial due to issues that mucociliary clearance may be impaired. Occasionally, surgical interventions are used when disease is continual and immune to empiric remedy. Aspergillus is commonest, but Candida, Mucor, and Penicillium organisms may be recovered from infected sinus aspirates. Invasive disease with eye, mouth, and mind extension occurs in patients with acquired immunodeficiency disease or on chemotherapy. Finally, maxillary antrum tumors produce a unilateral bloody nasal discharge that can be confused with sinusitis. Clues to a malignant process are the chronicity of signs, refractoriness to conventional remedy, and the presence of bony destruction of the antrum on radiographic examination. Duration of signs, presence of a fever, history of local trauma, orthodontic difficulties, shortness of breath, or dysphagia could assist localize lesions and identify potential problems. The web site of swelling of the jaw is set on bodily examination by palpation, running the finger intraorally alongside the inside and outer borders of the mandible, and comparing the right and left sides. Fracture of the lower jaw normally presents with a history of trauma, although sometimes minor in nature. Jaw fractures are treated like compound fractures as a result of the teeth communicate with the oral cavity. Aseptic necrosis caused by a 2248 Figure 515-1 Appropriate position of the lymph nodes (left) and the salivary glands (proper). Periodontal abscess outcomes from poor dental hygiene or tooth trauma, significantly in the aged, the diabetic, or the immunocompromised host. Complications result from periodontal abscess as a result of infection can observe quickly alongside tissue planes to the basal structures of the cranium and to the neck and mediastinum. Left unrecognized or untreated, it could possibly progress quickly to respiratory obstruction. Intravenous antibiotics and corticosteroids should regularly be accompanied by surgical exploration and drainage. The commonest nonmalignant tumor is an epulis (which means "on the gum"), a granulomatous and fibrous tissue progress. Other growths embody osteoma, cyst, ameloblastoma (a tumor of the cells that make enamel), and malignant epithelioma. The last is a uncommon situation with jaw modifications resembling acromegaly but with out enlargement of the palms or ft. Pain in the lower jaw with out swelling is usually as a result of dental caries, periodontal disease, or temporomandibular dysfunction (otomandibular syndrome). Pain from cardiac angina also may be referred to the jaw and has been mistaken for periodontal disease. The commonest explanation for an acute onset of hoarseness is a bacterial or viral infection. Stridor suggests greater than edema and irritation of the vocal folds and warrants evaluation for extrinsic or intrinsic airway encroachment. Intermittent or recurrent hoarseness is normally associated with smoking and/or allergy. Hoarseness persisting 2 weeks or more must be investigated by immediately inspecting the laryngeal structures. Chronic hoarseness may result from benign and malignant processes, including gastroesophageal reflux, laryngeal carcinoma or polyps, arthritis, hypothyroidism, goiter, and infections (tuberculosis, syphilis, and histoplasmosis). Chronic hoarseness as a result of malignancy in the chest, with entrapment of the left recurrent laryngeal nerve, and to pharyngeal or esophageal carcinomas, with entrapment of nerves or extrinsic compression, normally occurs after the primary tumor has declared itself by different signs. Hoarseness as a result of recurrent laryngeal nerve paralysis could current years after thyroid or parathyroid surgery, trauma to the neck, or goiter and is attributed to fibrosis and/or growing older. Hoarseness following endotracheal intubation is widespread but ought to resolve inside 3 to 5 days after eradicating the tube. Nerve-grafting procedures can restore operate in a paralyzed wire and laser remedy can be used for vocal folds entrapped after extended intubation, tracheostomy, or granuloma formation. There may be signs of elevated airway resistance with inspiratory chest retractions and lively expiratory efforts. Assessment of the patient with signs at relaxation ought to focus first on restoring or assuring a patent airway earlier than an examination. Most widespread misdiagnoses are bronchial asthma and coronary heart failure, so that a failure to respond to empiric therapy ought to raise suspicion for an higher airway trigger for dyspnea, wheezing, and hypercapnic respiratory failure. Direct examination could precipitate complete airway closure and must be carried out in a controlled setting like an emergency department. If the patient is steady, a move-volume loop is one non-invasive test that can reveal the presence of move limitation on inspiration or on both inspiration or expiration. A soft tissue lateral radiograph with the neck extended could localize the site of the obstruction. Causes of acute obstruction embody bacterial epiglottis, trauma, angioneurotic edema, allergic reactions, and overseas body aspiration. Chronic obstruction can be a presenting characteristic of neoplastic disease (sqamous cell carcinoma being the most common), cricoarytenoid arthritis, vocal wire polyps, bilateral vocal wire paralysis, goiter, and neurofibromatosis. Glottic dysfunction, also known as factitious bronchial asthma, is an uncommon dysfunction characterized by intermittent episodes of dyspnea and wheezing. The patient could current with hypercapnia but with a 2249 regular arterial-alveolar gradient, indicating that gasoline trade in the distal airways and lung units is regular.
Safe 500mg chitosan
Some sources will refer to the connection between a postganglionic fiber and a goal effector as neuroeffector junctions; neurotransmitters, as defined above, can be known as neuromodulators. Instead of a synaptic end bulb, a neurotransmitter is released from swellings alongside the length of a fiber that makes an prolonged community of connections in the goal effector. The authentic utilization of the epithet "battle or flight" comes from a scientist named Walter Cannon who worked at Harvard in 1915. The concept of homeostasis and the functioning of the sympathetic system had been launched in France in the previous century. Cannon expanded the concept, and launched the idea that an animal responds to a risk by preparing to stand and battle or run away. The nature of this response was totally defined in a guide on the physiology of ache, hunger, worry, and rage. When students learn in regards to the sympathetic system and the battle-or-flight response, they typically stop and marvel about different responses. If you were faced with a lioness operating towards you as pictured at the beginning of this chapter, would you run or would you stand your floor? The common epithet of "battle or flight" is being enlarged to be "battle, flight, or fright" or even "battle, flight, fright, or freeze. The sympathetic system is liable for the physiological responses to emotional states. The name "sympathetic" could be said to imply that (sym- = "collectively"; -pathos = "ache," "suffering," or "emotion"). The system comes from a time when threats were about survival, but in the trendy age, these responses turn into a part of stress and anxiety. This video describes how the autonomic system is simply a part of the response to threats, or stressors. What different organ system will get concerned, and what a part of the brain coordinates the two methods for the whole response, together with epinephrine (adrenaline) and cortisol? The primary distinction between the somatic and autonomic methods is in what goal tissues are effectors. The autonomic system, however, targets cardiac and clean muscle, in addition to glandular tissue. Whereas the essential circuit is a reflex arc, there are differences in the structure of these reflexes for the somatic and autonomic methods. The Structure of Reflexes One distinction between a somatic reflex, such because the withdrawal reflex, and a visceral reflex, which is an autonomic reflex, is in the efferent department. The output of a somatic reflex is the lower motor neuron in the ventral horn of the spinal cord that projects on to a skeletal muscle to trigger its contraction. The output of a visceral reflex is a two-step pathway beginning with the preganglionic fiber emerging from a lateral horn neuron in the spinal cord, or a cranial nucleus neuron in the brain stem, to a ganglion-followed by the postganglionic fiber projecting to a goal effector. The different a part of a reflex, the afferent department, is commonly the identical between the two methods. Somatic reflexes, for instance, contain a direct connection from the ventral horn of the spinal cord to the skeletal muscle. Visceral reflexes contain a projection from the central neuron to a ganglion, followed by a second projection from the ganglion to the goal effector. Afferent Branch the afferent department of a reflex arc does differ between somatic and visceral reflexes in some instances. The baroreceptor apparatus is a part of the ending of a unipolar neuron that has a cell body in a sensory ganglion. The baroreceptors from the carotid arteries have axons in the glossopharyngeal nerve, and people from the aorta have axons in the vagus nerve. The sensory homunculus-the illustration of the body in the major somatosensory cortex-only has a small area allotted for the notion of inside stimuli. When particularly sturdy visceral sensations rise to the level of acutely aware notion, the sensations are often felt in unexpected locations. For example, sturdy visceral sensations of the center will be felt as ache in the left shoulder and left arm. This irregular sample of projection of acutely aware notion of visceral sensations is known as referred ache. Depending on the organ system affected, the referred ache will project to totally different areas of the body (Figure 15. The most broadly accepted principle for this phenomenon is that the visceral sensory fibers enter into the identical level of the spinal cord because the somatosensory fibers of the referred ache location. By this explanation, the visceral sensory fibers from the mediastinal area, where the center is positioned, would enter the spinal cord on the similar level because the spinal nerves from the shoulder and arm, so the brain misinterprets the sensations from the mediastinal area as being from the axillary and brachial regions. Projections from the medial and inferior divisions of the cervical ganglia do enter the spinal cord on the center to lower cervical ranges, which is where the somatosensory fibers enter. Some sensations are felt locally, whereas others are perceived as affecting areas which might be quite distant from the concerned organ. The spleen is in the higher-left abdominopelvic quadrant, but the ache is more in the shoulder and neck. The sympathetic fibers linked to the spleen are from the celiac ganglion, which might be from the mid-thoracic to lower thoracic area whereas parasympathetic fibers are found in the vagus nerve, which connects in the medulla of the brain stem. However, the neck and shoulder would connect with the spinal cord on the mid-cervical level of the spinal cord. The incorrect assumption can be that the visceral sensations are coming from the spleen instantly. The motor fibers that make up this nerve are liable for the muscle contractions that drive ventilation. Therefore, the visceral fibers from the diaphragm enter the spinal cord on the similar level because the somatosensory fibers from the neck and shoulder. The visceral sensation is definitely in the diaphragm, so the referred ache is in a area of the body that corresponds to the diaphragm, not the spleen. Efferent Branch the efferent department of the visceral reflex arc begins with the projection from the central neuron alongside the preganglionic fiber. This fiber then makes a synapse on the ganglionic neuron that projects to the goal effector. The effector organs which might be the targets of the autonomic system vary from the iris and ciliary body of the attention to the urinary bladder and reproductive organs. The thoracolumbar output, through the various sympathetic ganglia, reaches all of those organs. The cranial part of the parasympathetic system projects from the attention to a part of the intestines. The sacral part picks up with nearly all of the big gut and the pelvic organs of the urinary and reproductive methods. Visceral reflexes that contain the thoracolumbar or craniosacral methods share similar connections. A lengthy reflex has afferent branches that enter the spinal cord or brain and contain the efferent branches, as beforehand defined. A brief reflex is completely peripheral and only entails the native integration of sensory input with motor output (Figure 15. The brief reflex entails the direct stimulation of a postganglionic fiber by the sensory neuron, whereas the lengthy reflex entails integration in the spinal cord or brain. Because the efferent department of a visceral reflex entails two neurons-the central neuron and the ganglionic neuron-a "brief circuit" could be attainable. There are a few myenteric plexuses in which the nervous tissue in the wall of the digestive tract organs can instantly influence digestive operate. If stretch receptors in the abdomen are activated by the filling and distension of the abdomen, a short reflex will instantly activate the smooth muscle fibers of the abdomen wall to improve motility to digest the excessive meals in the abdomen. That neuron, linked to the smooth muscle, is a postganglionic parasympathetic neuron that can be managed by a fiber found in the vagus nerve. In the top, one skilled, one query, and a simple blood strain cuff solutions the query. Why would the center need to beat quicker when the teenager changes his body position from lying all the way down to sitting, after which to standing? Balance in Competing Autonomic Reflex Arcs the autonomic nervous system is important for homeostasis because its two divisions compete on the goal effector. The stability of homeostasis is attributable to the competing inputs from the sympathetic and parasympathetic divisions (dual innervation). At the level of the goal effector, the sign of which system is sending the message is strictly chemical.
Order 500mg chitosan
The lumen of the small duct and ductule incorporates homogenous pinkstaining protein-rich pancreatic juice. There is a small islet (small cells, pale cytoplasm) on the upper border, picture left (asterisk). Acinar tissue with an intralobular ductule in cross section, human pancreas (H & E). Note the only layer of cuboidal duct cells and the almost complete absence of collagen in the wall of this ductule. The lumen of the ductule incorporates a pink granular proteinaceous precipitate from pancreatic juice. The clear spaces between the duct cells and the skinny connective tissue wall of the ductule reflects artifactual separation of the cells from the basement membrane. Islets differ tremendously in measurement; ~70% are in the measurement vary of 50250 m in diameter in humans with a median in the vary of 100-150 m (four). Smaller islets are dispersed all through the acinar lobules and most bigger islets lie along the main and interlobular ducts of the pancreas. Most islets are spherical or ellipsoid, however they can be irregular in shape-generally reflecting the pressure of an adjacent structure, often a duct, or limitation by a tissue aircraft. Several stories present support for the presence of a higher population density of islets in the tail of the pancreas than in the head and physique though others find no difference (5, thirteen, 16, 17). In adult humans the variety of islets is calculated to be 500,000-1 million whereas there are far fewer in smaller animals (9, eleven). In addition to the islets, isolated islet cells could also be found dispersed in the acinar lobules or in association with ducts. Several of these have been immunostained utilizing antibodies to specific islet peptide hormones to show various islet cell varieties together with -cells (insulin), -cells (glucagon), and -cells (somatostatin). This low energy histologic section illustrates three islets in the background of the more abundant acinar tissue with a small duct in the upper picture right corner. The massive islet, picture left, could also be two adjacent islets with a small islet conforming to the lower border of a big round islet. The islet cells are smaller and have paler cytoplasm than the surrounding acinar cells. Although most islets are oval or round in cross section, islets differ tremendously in shape as illustrated here. Serial sections of an islet have been immunostained utilizing antibodies to insulin (picture left), glucagon (heart) and somatostatin (picture right). In the middle and picture right pictures, the situation of -cells and cells is primarily on the border of groups of cells. Triple-immunolabeling of islet hormones shows the predominance of insulin-secreting cells and their distinct distributions. This islet was stained utilizing antibodies to insulin, glucagon and somatostatin to show beta cells (pink), alpha cells (brown), and delta cells (blue). These images present a minor species difference in the location of -cells in mouse and human islets. In humans, -cells appear within the islet though they appear to be on the periphery of clusters of -cells. Note that unstained cells are situated in the periphery of the islet corresponding to the situation of glucagon staining in. At the ultrastructural level, the cell varieties are distinguished primarily by differences in their granules. Online Resources the next websites present extra images of the pancreas. Some of the drawings are labeled intimately whereas others will challenge you to identify unlabeled buildings. We suggest that you go to several of these after you evaluation the text and pictures offered above. Due to the scale of the files, it may take a minute or longer for some sites to open. References Because this is an online publication, some references might be offered as web site hyperlinks when this is applicable. Several of the references are chapters in the Pancreas: Biology, Pathobiology, and Disease. Actual distribution of the quantity and volume of the islets of Langerhans in different measurement lessons in non-diabetic humans of varying ages. The frequency distribution of the quantity and volume of the islets of Langerhans in man. The pancreatic polypeptide cells in the human pancreas: the results of age and diabetes. Quantitation of endocrine cell content material in the pancreas of nondiabetic and diabetic humans. Role of actin in regulated exocytosis and compensatory membrane retrieval: insights from an old acquaintance. Selective beta-cell loss and alpha-cell enlargement in patients with kind 2 diabetes mellitus in Korea. Wall layer Subdivisions of the layer (if relevant) mucosa 1) epithelium 2) lamina propria 3) muscularis mucosa submucosa (not relevant) muscularis externa 1) circular layer 2) longitudinal layer serosa or adventitia (not relevant) safety Organs of the Alimentary Canal 2. The tubelike digestive system canal that extends from the mouth to the anus is the alimentary 3. Changes from stratified squamous (esophagus) to easy columnar (abdomen) How do the epithelia of these two organs relate to their specific capabilities? The esophagus is subjected to constant abrasion (stratified squamous is nicely adapted for this). The massive gut includes the colon, but also includes the cecum, vermiform appendix, rectum, and anal canal. You have studied the histological structure of numerous organs on this laboratory. Correctly label all buildings provided with leader strains in the diagram of a molar below. There are 2 incisors, 1 canine, 2 premolars, and three molars in every jaw (upper and lower) from the median line posteriorly. Various forms of glands form part of the alimentary tube wall or duct their secretions into it. Match the glands listed in column B with the function/areas described in column A. The pancreas has two main populations of secretory cells-those in the islets and the acinar cells. First printed 1963 Second edition 1969 Third edition 1977 Reprinted 1979 Fourth edition 1983 Fifth edition 1988 Reprinted 1990 Sixth edition 1993 Reprinted 1995 Seventh edition 1997 Reprinted 1998 Italian first edition 1972 Japanese fourth edition 1989 German fifth edition 1992 Library of Congress Cataloging-in-Publication Data Ellis, Harold, 1926� Anatomy for anaesthetists / Harold Ellis, Stanley Feldman, William Harrop-Griffiths; with a chapter on the Anatomy of pain contributed by Andrew Lawson. Further illustrations for the seventh and this edition have been prepared by Jane Fallows with nice ability. Some regions of the physique, for instance the respiratory passages, the most important veins and the peripheral nerves, the anaesthetist should know with an intimacy of detail that rivals and even exceeds that of the surgeon; different areas may be all however ignored. The role of anatomy in anaesthetic instructing is usually thought of merely as a prerequisite for the secure practice of native anaesthetic blocks. It is an anatomy e-book written for anaesthetists, keeping in thoughts the special necessities of their daily practice. He brings with him special experience in fashionable anaesthetic expertise and has tremendously assisted us in updating the text and illustrations. Dr Andrew Lawson has fully up to date his essential section on the Anatomy of Pain and has given priceless advice on procedures relevant to the practice of pain medicine. The vestibule is fashioned by the lips and cheeks with out and by the gums and teeth within. An essential characteristic is the opening of the parotid duct on a small papilla reverse the 2nd upper molar tooth. The mucosa of the floor of the mouth between the tongue and mandible bears the median frenulum linguae, on both facet of which are the orifices of the Uvula Palatopharyngeal arch Palatine tonsil Palatoglossal arch. Backwards and outwards from these ducts prolong the sublingual folds that cowl the sublingual glands on both sides. The palate the hard palate is made up of the palatine processes of the maxillae and the horizontal plates of the palatine bones. The mucous membrane covering the hard palate is peculiar in that the stratified squamous mucosa is intently connected to the underlying periosteum, in order that the two dissect away at operation as a single sheet termed the mucoperiosteum. This is skinny in the midline, however thicker more laterally as a result of the presence of numerous small palatine salivary glands, an unusual however nicely-recognized site for the event of blended salivary tumours.
Best 500mg chitosan
Although not proven to happen, kindling phenomenon might play a role in worsening a seizure disorder. Kindling occurs within the experimental setting the place frequent repeated stimulation of cerebral neurons arrange circuitry that initiates spontaneous seizures. With the exception of standing epilepticus, seizures are generally not life threatening. Generics are available so these drugs are extra reasonably priced than they used to be however can still be expensive in giant sufferers. Approximately 80% of canines respond to a traditional monotherapy protocol (phenobarbital or potassium bromide). Euthanasia may be pursued for quality of life purposes however some animals succumb to the seizures themselves or complications of seizure remedy. It is extraordinarily necessary to have present serum concentrations of medicine previous to adjusting the dose. I may consider weaning drug #1 if the affected person is seizure free for an prolonged period (1 yr) or if unwanted side effects are an issue. Hypoallergenic diets and acupuncture have been touted as having anti-convulsant properties however these remain unproven. Vagal stimulation could be offered by an implantable stimulator, ocular strain, or carotid strain. Implantable units have been utilized in refractory idiopathic epileptics with some success. Epilepsy surgical procedure Surgical remedy for epilepsy is pursued in children however is sometimes performed within the veterinary inhabitants. A corpus callosotomy, division of the white matter of the corpus callosum between the two cerebral hemispheres, might stop seizure generalization. Lastly, in a sure inhabitants of kids, unilateral hemispherectomies have been described. Because of neuroplasticity within the younger, they tolerate the process relatively nicely. Ben Carson was the innovator of this process and his story is capitulated in Gifted Hands. A medicine is taken into account effective if the seizure frequency is reduced by 50%. Even although a medicine is taken into account effective, it will not be sufficient to achieve what is taken into account good seizure control (no seizures or rare seizures, for instance <three seizures/6 weeks). Secondary objectives embrace reduction within the period of the seizure or decrease in severity of the seizure phenotype. Ideally we would like to reduce price for the owner and unwanted side effects within the affected person. It is extraordinarily useful for the owner to keep a seizure log, recording when a seizure occurs, triggers, period, and appearance. A reduction in seizure frequency by 50% or extra is taken into account wonderful anti-convulsant remedy. Monitoring Monitoring depends on the medicine used since pharmacokinetics differ. Phenobarbital is unique in that it causes hepatic induction of the cytochrome P450 enzymes. Since phenobarbital is primarily metabolized by this enzyme system, further enzymatic induction results in elevated metabolism of the drug and a subsequent drop within the steady state focus. Thus with phenobarbital, serum concentrations should be evaluated at steady state, three months, six months, after which each six months. Because of this enzymatic induction, phenobarbital administration may alter metabolism of different medicines and endogenous hormones. For this purpose, animals on phenobarbital might have low thyroid values and require larger dosages of hepatically metabolized medicines. It could be extraordinarily troublesome to show if an animal on phenobarbital has concurrent hypothyroidism. Failing to appropriately monitor sufferers is the commonest explanation for seizure remedy failure. At a minimum renal values, liver values and urine specific gravity should be performed. Unlike different drugs, long run phenobarbital remedy may very well cause hepatopathy and a few advocate a fasting bile acid test along with minimum database each 6-12 months. Chronic use of sulfa drugs like zonisamide may alter thyroid function and this should be evaluated yearly or in animals exhibiting scientific signs consistent with hypothyroidism. I sometimes try to wean phenobarbital before bromide in a affected person receiving each these medicines. My philosophy is that phenobarbital is related to potentially extra life-threatening opposed effects (hepatotoxicity, hepatocutaneous syndrome, bone marrow suppression) than bromide, especially when maintained at chronically excessive normal serum concentrations. If seizures recur during the weaning, I return to the final effective dose, recheck the serum focus and wait twice as lengthy (2 years) before attempting weaning once more. A single research analyzing the impact of a particular rehabilitation program on survival of canines with degenerative myelopathy showed vital profit (Kathmann et al 2006). Additional research looking at the impact of bodily rehabilitation on neurologic and orthopedic situations is missing in veterinary medicine. Physical rehabilitation might promote sooner restoration following surgical procedure or in non-surgical sufferers by enhancing blood circulate, limiting irritation, sustaining and rising muscle mass, selling joint well being, rising range of movement, enhancing quality of movement, assisting weight reduction, and preventing complications. A broad variety of techniques and modalities are used to achieve these helpful effects. Physical rehabilitation has identified therapeutic effects however is also a psychologically rewarding engagement for a lot of shoppers and sufferers. It permits and encourages client-affected person interaction and prevents boredom during periods of rest and healing. That being mentioned, not each neurologic disease will profit from all rehabilitation techniques and in some circumstances there are identified contra-indications for explicit therapies. A thorough history, bodily examination, neurologic examination, and radiographic analysis may be adequate in some circumstances. Radiographs are incessantly not diagnostic for many situations for which bodily rehabilitation is indicated. However, they might help rule out ailments that may require a radically different therapeutic approach. For non-surgical situations similar to degenerative myelopathy and fibrocartilaginous embolism, extra is healthier. For canines with suspected kind I intervertebral disc herniations, strict rest should be adhered to for 2 weeks. If the affected person is enhancing, light and passive workout routines could be initiated after 2 weeks. Once a prognosis has been made, discuss with the shoppers about their monetary and time funding as well as their expectations. It can be unrealistic for shoppers with a 7 yr old, grade 5 paraplegic greyhound to anticipate their dog to return to racing and never want long run medical care. Assessing sufferers for rehabilitation involves not only the neuroanatomic localization of an issue, however an evaluation of their neuromuscular function. Simple measures similar to circumferential muscle mass could be evaluated using a rigidity loading measuring tape. Joint range of movement could be quantified using goniometry as well as characterizing the end feel (soft, onerous, empty); this is sometimes less necessary than evaluation of muscle mass for neurologic sufferers until comorbid situations are at play. More expensive tools similar to stance analyzers, kinematic movement sensors, and drive plates are additionally obtainable at some institutions/practices. Pharmaceutical control should always be initiated first and to no matter extent potential. Once a affected person is snug sufficient to willingly have interaction in your plan, the remedy itself and institution of normal movement patterns may also be ache relieving. Motivational instruments are different for every affected person and could embrace meals, toys, reward, or even the chance to escape!
Ice Vine (Pareira). Chitosan.
- Dosing considerations for Pareira.
- Fluid retention, promoting the menstrual cycle, and other uses.
- What is Pareira?
- How does Pareira work?
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96493
Trusted chitosan 500 mg
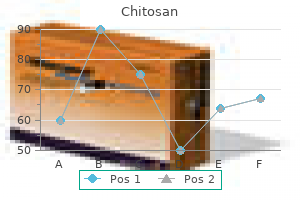
In most situations, gradual charges of stimulation of 2 Hz, with an interstimulus interval of 500 ms, will maximize any potential decrement. The biggest lower in acetylcholine launch at gradual charges of stimulation occurs through the first 4 stimuli. The slower the rate and the fewer the variety of stimuli given, the higher the patient is able to tolerate the procedure. The practice of four stimuli ought to be repeated, with no less than 15�30 seconds of rest between trains. The trains are repeated to verify for reproducible amplitudes, areas, and configurations in addition to the stability of the baseline, the presence of stimulus artifact, patient leisure or movement, and the stability of the recording and stimulating electrodes. If any abnormalities are found, you will need to exclude any potential supply of artifact that could lead to such an abnormality earlier than proceeding with additional testing. After excluding any such artifact, three reproducible and technically satisfactory sets of four stimuli at 2 Hz with 15�30 seconds between sets ought to be obtained as a baseline. A Depending on the clinical problem and the results of the baseline 2-Hz repetitive stimulation, a decision have to be made about the usefulness of additional testing of neuromuscular transmission with repetitive stimulation after train or tetanic stimulation. In general, train is completed for a short period (10 seconds) or an intermediate period (1 minute). After 10 seconds of train, the discharge of acetylcholine with each action potential is potentiated for 30�60 seconds. In myasthenia gravis, the decrement at baseline may be decreased or repaired during this era. A practice of four stimuli got at 2/second (s) with the muscle rested on three events, separated by 30 seconds of rest for the three baseline studies (B1, B2, B3). This histogram is an effective instance of the sample of abnormality that may be expected in issues of neuromuscular transmission. In each practice of four, the best decrement is between the primary and second response, with much less decrement between the second and third and the third and fourth responses. Middle, the 4 responses to 2-Hz stimulation four minutes after train are displayed within the x-shifted trend. Bottom, Numerical display of the amplitudes and areas of every of the responses (Potential [pot] 1�four) and the share decrements (decr) in amplitude (amp) and area four minutes after train. Examples of supramaximal repetitive stimulation at three Hz of the ulnar nerve at the wrist whereas recording over the hypothenar muscle at rest and at three seconds, 2 minutes, and 10 minutes after train. In the patient who has myasthenia gravis, the lower in amplitude from the primary to third response repairs after 10 seconds of train and then becomes more pronounced 2 minutes after train. Myasthenic syndrome sometimes associated with bronchial neoplasm: Neurophysiologic studies. The 1-minute period of train ought to be performed in three sets of 20 seconds of train interspersed with 2�5 seconds of rest between each set, to simulate extended stimulation. For 2�5 minutes after train, the amount of acetylcholine released with each stimulus ought to be minimal, providing the best chance for detecting any defect of neuromuscular transmission. Usually, after the patient completes 1 minute of train, 4 stimuli are given at 2 Hz immediately after train, and at 30, 60, 120, one hundred eighty, and 240 seconds after train. As emphasised above, any change in amplitude, configuration, or area ought to initially be thought-about a technical problem, and technical components, including strength of stimulation, ought to be checked. The display of the results varies with the machine, hardware, software program, and display units. In general, the sensitivity ought to be adjusted to display the potentials as massive as possible with out overflowing or blocking. The sweep speed ought to be gradual sufficient to unfold the potential out so that it may be analyzed visually and quick sufficient such that the whole potential is displayed, including any late elements. This implies that the onset of the sweep for each successive stimulus is shifted to the right on the horizontal, or x-axis, or delayed so that each potential could be analyzed individually. Results ought to be both printed immediately or saved for later evaluate and printing. An enhance in size occurs with facilitation and is measured because the percent increment (enhance) within the response; a lower in size occurs with post activation exhaustion and is measured as percent decrement (lower). Increments and decrements in responses are measured by dividing the change in size by the baseline size. For instance, a baseline amplitude of 10 mV with: with a postexercise amplitude of eight or 12 mV equates to 20% decrement and 20% increment, respectively, with postexercise amplitudes of 1 and 19 mV equates to ninety% decrement and ninety% increment, respectively, with postexercise amplitudes of 20, 25, and 30 mV equates to a hundred%, 150%, and 250% increments, respectively. Small apparent decrements (<10%) could occur for technical reasons in normal individuals. Such an increment is normally accompanied by a lower in duration with little or no change in area and is called pseudofacilitation. This is because of an elevated synchronization of the firing of motor units somewhat than a rise within the variety of units or the amplitude of the response of individual fibers. There are a number of possible causes for abnormal leads to the absence of illness (false positives) which ought to all the time be thought-about earlier than making the analysis of a disorder of neuromuscular transmission. Submaximal stimulation is recommended by a lack of amplitude of the preliminary response within the practice compared to the amplitude obtained through the baseline testing. A shift within the baseline or seen muscle activity between the stimuli is suggestive of such movement. The potentials evoked by repetitive stimulation could be displayed in a staggered, or x-shifted, trend to allow inspection of every potential and willpower of the sequence of any modifications. Superimposition of the potentials allows simpler visible identification of small decrements. Repetitive Stimulation Studies 377 Key Points � Educate patients as to what to anticipate, and the way greatest to relax. Technical issues such as poor leisure or movement during repetitive stimulation can produce apparent decrements in normal topics, as seen in these examples. This is preferable to making a severe analysis on the idea of questionable information. False-unfavorable outcomes or normal leads to a patient with a disorder of neuromuscular transmission could be attributable to low temperature, which is able to masks a mild defect of neuromuscular transmission, or continuation of pyridostigmine or neostigmine through the testing. Temperatures ought to be monitored with the hand skin temperature greater than 32 C and the foot skin temperature greater than 30. If the temperatures are cool, the patient ought to be warmed earlier than additional studies are performed. When possible, therapy with acetylcholinesterase inhibitors such as pyridostigmine or neostigmine ought to be discontinued for no less than four�6 hours earlier than the take a look at and preferably overnight. The threat to the patient from discontinuing therapy have to be weighed towards the importance of the take a look at. False-unfavorable outcomes may occur if therapy with immunosuppressants, intravenous immunoglobulin, or plasma exchange is successful. Ideally, the take a look at ought to be carried out when the patient is most symptomatic- normally late within the day when fatigued. Patients for whom the analysis is in question ought to preferably be examined when the effects of remedies such as plasma exchange, intravenous gamma globulin, and corticosteroids are minimal. Therefore, a conservative criterion of abnormality is to require a decrement in each area and amplitude of no less than 10% in two different muscle/nerve mixtures. An abnormal take a look at ought to meet the next standards: 378 Clinical Neurophysiology � Reproducible outcomes ought to be obtained on repeated testing (three baseline trains of four stimuli are beneficial). Brief train with voluntary, robust contraction produces the identical effect with out ache; nonetheless, some patients are unable to produce a powerful contraction because of excessive weakness, lack of know-how, or incapability to cooperate. If a disorder is suspected such as Lambert� Eaton myasthenic syndrome, fast charges of stimulation may be essential. Stress the importance of remaining as still and relaxed as possible so that the results of the take a look at shall be dependable. Before beginning, verify the machine and electrode setup to stop any technical errors. If a large facilitation is anticipated, the acquire or sensitivity ought to be set so that a much bigger response could be recorded with out blocking. It additionally allows the patient to get used to the technique earlier than transferring on to proximal muscular tissues of more interest.
Chitosan 500mg
In contrast, the amplitude of a compound sensory nerve action potential, motor unit potential, fibrillation potential, optimistic sharp wave, fasciculation potential, and most different action potentials is measured from probably the most optimistic peak to probably the most unfavorable peak. Amplitude Decay: the percent change in the amplitude of the M wave or the compound sensory nerve action potential between two different stimulation points alongside the nerve. Abnormal decay without elevated temporal dispersion might indicate a conduction block. Anodal Block: A native block of nerve conduction brought on by membrane hyperpolarization underneath a stimulating anode. Antidromic: Propagation of a nerve impulse in the path reverse to physiologic conduction; for example, conduction alongside motor nerve fibers away from the muscle and conduction alongside sensory fibers away from the spinal twine. Artifact (also Artefact): A voltage change generated by a biologic or nonbiologic supply aside from the ones of interest. The stimulus artifact (or shock artifact) represents cutaneous spread of stimulating current to the recording electrode and the delay in return to baseline which relies on the ability of filters to respond to excessive voltage. Movement artifact refers to a change in the recorded activity brought on by movement of the recording electrodes. Asterixis: A fast involuntary movement brought on by a quick lapse in tonic muscle activation. Specific options embrace dysmetria (incorrect distance moved) and dysdiadochokinesis (irregularity of tried rhythmic actions). Most commonly due to a disorder of the cerebellum or proprioceptive sensory system. Averaging: A methodology for extracting timelocked potentials from random background noise by sequentially including traces and dividing by the entire number of traces. Glossary of Electrophysiologic Terms 841 Axonal Degeneration: Degeneration of the phase of a nerve distal to the cell body with preferential distal pathology. Axonotmesis: Nerve injury characterised by axon and myelin sheath disruption with supporting connective tissue preservation, leading to axonal degeneration distal to the injury web site. Backaveraging: Averaging a signal which occurs in a time epoch previous a triggering event. Baseline: (1) the potential recorded from a biologic system while the system is at rest. Benign Fasciculation Potential: A firing sample of fasciculation potentials occurring in affiliation with a clinical syndrome of fasciculations in a person with a nonprogressive neuromuscular disorder. Biphasic Action Potential: An action potential with one baseline crossing, producing two phases. Bipolar Needle Electrode: Recording electrode that measures voltage between two insulated wires cemented side-by-side in a steel cannula. The naked tips of the electrodes are flush with the extent of the cannula which may serve as a floor. Bizarre High-Frequency Discharge: See most popular term, complicated repetitive discharge. Blink Responses: Compound muscle action potentials evoked from orbicularis oculi muscles because of transient electrical or mechanical stimuli applied to the cutaneous area innervated by the supraorbital (or less commonly, the infraorbital) department of the trigeminal nerve. Generally, only the R2 wave is associated with a visible contraction of the muscle. The configuration, amplitude, period, and latency of the 2 components, along with the websites of recording and stimulation, must be specified. The R1 and R2 waves are oligosynaptic and polysnaptic brain stem reflexes, respectively. The afferent arc is offered by the sensory branches of the trigeminal nerve and the efferent arc is offered by facial nerve motor fibers. Blocking: Term utilized in single fiber electromyography to describe dropout of one or more components of the potential during sequential firings. A signal of irregular neuromuscular transmission, which may be due to major neuromuscular transmission issues, corresponding to myasthenia gravis and different myasthenic syndromes. Also seen because of degeneration and reinnervation in neuropathies or myopathies. Concomitant blocking may be generated by a split muscle fiber or failure of conduction at an axon department serving a number of muscle fibers. Used to describe a recruitment sample of transient period, small amplitude, overly ample, polyphasic motor unit action potentials, with respect to the amount of pressure generated; normally a minimal contraction. Quantitative measurements of motor unit action potential period, amplitude, numbers of phases, and recruitment frequency are most popular. C Reflex: An irregular reflex response representing the electrophysiologic correlate of sensory evoked myoclonus. The term "C" was chosen to indicate that the reflex may be mediated in the cerebral cortex. Center Frequency: the imply or median frequency of a waveform decomposed by frequency analysis. Central Electromyography: Use of electrodiagnostic recording techniques to research reflexes and the management of movement by the spinal twine and brain. Central Motor Conduction: the time taken for conduction of action potentials in the central nervous system from motor cortex to alpha motoneurons in the spinal twine or brain stem. Calculated from the latencies of the motor evoked potentials produced by transcranial magnetic stimulation or transcranial electrical stimulation, subtracting the time for peripheral conduction. Chorea: Clinical term used to describe irregular, random, transient, abrupt, involuntary actions of the top or limbs due to a disorder of the basal ganglia. Clinical Electromyography: Term used commonly to describe the scientific methods of recording and analysis of biologic electrical potentials from human peripheral nerve and muscle. Collision: When used close to nerve conduction research, the interaction of two action potentials propagated towards each other from reverse instructions on the same nerve fiber so that the refractory durations of the 2 potentials stop propagation previous each other. Consists of a frequently repeating sequence of complicated polyphasic or serrated potentials that start abruptly after needle electrode movement or spontaneously. The potentials have a uniform form, amplitude, and discharge frequency ranging from 5 to a hundred Hz. Thought to be due to ephaptic excitation of adjacent muscle fibers in a cyclic style. This term is most popular to bizarre excessive-frequency discharge, bizarre repetitive discharge, bizarre repetitive potential, pseudomyotonic discharge, and synchronized fibrillation. Compound Action Potential: A potential or waveform resulting from the summation of multiple particular person axon or muscle fiber action potentials. See compound mixed nerve action potential, compound motor nerve action potential, compound nerve action potential, compound sensory nerve action potential, and compound muscle action potential. Compound Mixed Nerve Action Potential: A compound nerve action potential recorded from a mixed nerve when an electrical stimulus is applied to a phase of the nerve that contains each afferent and efferent fibers. Elicited by stimulation of a motor nerve, a motor department of a mixed nerve, or a ventral nerve root. Baseline-to-peak amplitude, period, and latency of the unfavorable phase must be famous, along with particulars of the tactic of stimulation and recording. Use of specific named potentials is beneficial, for example, M wave, F wave, H wave, T wave, A wave, and R1 or R2 wave (blink responses). Details of the tactic of stimulation and recording must be specified, along with the fiber sort (sensory, motor, or mixed nerve). May also be elicited when an sufficient stimulus is applied synchronously to sensory receptors. The latency is measured as both the time to the preliminary deflection or the unfavorable peak, and the period because the interval from the first deflection of the waveform from the baseline to its final return to the baseline. Concentric Needle Electrode: Recording electrode that measures an electrical potential distinction between a centrally insulated wire and the cannula of the needle by way of which it runs. Conduction Block: Failure of an action potential to propagate previous a selected level in the nervous system whereas conduction is possible beneath the point of the block. Documented by demonstration of a reduction in the area of a compound muscle action potential higher than that usually seen with stimulation at two different points on a nerve trunk; anatomic variations of nerve pathways and technical components related to nerve 844 Glossary of Electrophysiologic Terms stimulation must be excluded as the reason for the discount in area. Conduction Distance: the length of nerve or muscle over which conduction is decided, usually measured in centimeters or millimeters. The nerve fibers studied (motor, sensory, autonomic, or mixed nerve) must be specified. For a nerve trunk, the utmost conduction velocity is calculated from the latency of the evoked potential (muscle or nerve) at maximal or supramaximal intensity of stimulation at two different points.
500mg chitosan
These capabilities embrace:1 � � � � � Convenient storage and retrieval of records Montage reformatting Filter, sensitivity, and time base changes Reliability of interpretation Rapid location of events and features of interest � Annotating recordings � Quantitative evaluation of background exercise and transients the disadvantages of digital devices embrace the next: � Cost-Digital devices could also be more expensive, particularly in the long term, as a result of with the fast evolution of computer technology, digital devices become out of date extra rapidly than their analog counterparts did. Maintenance personnel have to be knowledgeable about computers and computer software program in addition to hardware. Digital devices could also be much less fault-tolerant, and gear failures could also be extra catastrophic with digital methods, with potential loss of a complete study because of system failure. To surmount this difficulty, some firms now supply reader programs for private computers which are capable of reading the info codecs used by many alternative producers, but these programs are an additional expense. However, the advantages of digital recording outweigh the disadvantages, and all fields of clinical neurophysiology are shifting steadily towards digital technology. Also, digital recording of video significantly facilitates the enhancing and copying of video segments. This significantly reduces storage space requirements compared with analog recordings on paper and eliminates the necessity for microfilming paper recordings. With commonplace computer networks, recordings (including digital video, when relevant) could also be considered on appropriately configured private computers positioned at sites remote from the devices used for recording with no have to physically transport the report. Digital devices report all data using a referential montage with a single common reference electrode (such as Cz or a mean ear reference). All different montages then can be reconstructed by easy arithmetic operations on the recorded � � � � referential data. In addition to the routine bipolar and referential montages, special montages such as a common common reference or a laplacian (supply) montage could also be used. Reliability of interpretation-A current study comparing the accuracy of interpretation of digital vs. The research had been read both in conventional analog paper format, using a digital show but with out use of digital instruments such as montage reformatting, digital filtering, time base or sensitivity adjustment at evaluate time, or using all of the features of a digital system. As proven in Table four�1, the inter-reader settlement in classification of records as regular vs. The potential generally is directly proportional to the physiologic amount represented by the signal; subsequently, that potential is an analog of the physiologic amount. Analog indicators are generally steady within the sense that the potential varies constantly as a perform of time. In contrast, a single digital signal could tackle solely one of two potential potentials. Analog representations are extra suited to human interpretation; for Construction Of Digital Systems A digital (computerized) system for acquisition, storage, and show of physiologic waveforms has the next key components: � � � � � � � Electrodes Amplifiers and filters Analog-to-digital converters Solid-state digital reminiscence Digital processor (central processing unit) Magnetic or optical disk (or tape) storage Screen or printer for waveform show the electrodes, amplifiers, and filters in a digital system are essentially identical to these in an all-analog system. A digital processor is capable of shifting digital data around in reminiscence and processing or manipulating it; it may additionally ship data to a magnetic or optical disk or tape storage media for permanent storage, or it may generate shows of waveforms and associated textual annotations on a screen or printer. Digital Signal Processing 57 instance, a waveform show generally uses vertical displacement as an analog to the physiologic amount, such as the potential being displayed, and horizontal displacement as an analog to elapsed time. Key Points � An analog signal takes on any potential (voltage); the potential is directly proportional to the amount measured. A typical value might be 9�16 bits (corresponding to �1 half in 256 to 1 half in 32,768). Input potentials above or under the utmost or minimum are known as overflow or underflow, respectively. Analog-to-Digital Conversion Digitization, or analog-to-digital conversion, is the method by which analog indicators are converted to digital indicators. It is the transformation of steady potential changes in an analog signal representing a physiologic amount to a sequence of discrete digital numbers (binary integers). Outputs consist of four digital indicators (+3 or 0 V representing "1" and "0") that together can encode a four-bit integer (range 0�15). Key Points � Quantization is the assignment of a digital quantity to the instantaneous potential of the signal. The following two terms characterize sampling: � Sampling interval-This determines the temporal resolution of the digitizer. In addition to determining the temporal resolution of the digitizer, the sampling frequency determines the utmost frequency within the signal to be digitized that may be adequately represented. The sampling theorem (Nyquist theorem) states that if a signal accommodates component frequencies starting from 0 to fN, then the minimum sampling frequency that can be used for the digitized data to adequately represent the frequency content material of the original signal is 2fN, where fN is the Nyquist frequency. The Nyquist frequency can be calculated from the sampling interval as fN = 1/(2 � sampling interval). For instance, if fN = 50 Hz, then the sampling frequency have to be at least a hundred Hz (sampling interval of 0. This sampling frequency is the minimum essential to avoid gross distortion of the input signal; a larger sampling frequency (by an element of 3�5) could also be essential in lots of purposes to Figure four�2. In A, the signal exceeds the input range, in order that its digital representation (D) is clipped. In B, the signal uses more than 50% of the input range and is relatively nicely represented (E). Evoked potential primer: Visual, auditory, and somatosensory evoked potentials in clinical prognosis, 35�52. Aliasing is distortion of a signal caused by folding of frequency components within the signal greater than fN onto decrease frequencies. For instance, a sine wave of 75 Hz, if sampled at a hundred Hz, will seem within the digitized data as a sine wave of frequency 25 Hz, not 75 Hz. Aliasing should at all times be averted or else the digitized data will be a gross misrepresention of the true signal. In apply, aliasing is averted by filtering the input signal before digitization to remove all frequencies above the Nyquist frequency. For instance, if the sampling interval in use is 5 ms, the Nyquist frequency is a hundred Hz. A 70-Hz low-move filter with 6 dB per octave slope would attenuate frequencies of a hundred Hz to 0. A 50-Hz low-move filter with 12 dB per octave slope would attenuate frequencies of a hundred Hz to 0. Key Points � Sampling at a frequency decrease than twice the Nyquist frequency produces aliasing (distortion of the signal). Averaging may be applied to repetitive transient waveforms and event-associated potentials (such as movement-associated potentials). Effect of sampling interval and aliasing on the constancy with which an analog signal can be represented digitally. In A, the sampling frequency is 14 times that of the signal frequency and the signal is nicely represented (D). In B, the sampling frequency is just six times the signal frequency, and the representation is much less correct but nonetheless acceptable (E). Evoked potential primer: Visual, auditory, and somatosensory evoked potentials in clinical prognosis, 44. Less common but nonetheless essential uses are in time�frequency evaluation, including interval and Fourier (spectral) evaluation, autocorrelation evaluation, statistical evaluation, and automated sample recognition. Other uses are likely to be extra specialized to specific types of clinical neurophysiologic research; some of these are discussed elsewhere on this book. Key Points � Signal averaging is carried out in evoked potential research and averaging of repetitive transient waveforms. Their perform is similar no matter the kind of Analog Stimulus signal averaged, though for various kinds of research the epoch size for averaging differs significantly. Epoch lengths of 200�500 ms are typical for visual and long-latency auditory evoked potentials. Epoch lengths of 30�a hundred ms are typical for center-latency auditory evoked potentials and for nerve conduction research. Epoch lengths of 10�20 ms are typical for mind stem auditory evoked potentials and electrocochleograms. After every stimulus, the input signal is digitized at several discrete sampling times within a set-size epoch that begins on the time of the stimulus. Digitized values of potential at every discrete sample time, every characterised by its latency (time after the stimulus), are averaged for many stimuli; the ensuing averaged signal could also be displayed on a screen or printed on paper.
References:
- https://www.acponline.org/acp_policy/policies/racial_ethnic_disparities_2010.pdf
- https://www.rheumatology.org/Portals/0/Files/2015%20PMR%20guidelines.pdf
- https://www.cincinnatichildrens.org/-/media/cincinnati%20childrens/home/service/s/speech/hcp/doctor-info/information-general-pdf-comm-disorders-3.pdf?la=en
- https://www.clevelandclinicmeded.com/specialties/documents/RJF_Booklet_38singlepages.pdf
- https://publications.iarc.fr/_publications/media/download/1408/9062c1e8dff7c28b45dccfe1fd9783f1bb5b5fbe.pdf