.png)
2.5mg lisinopril
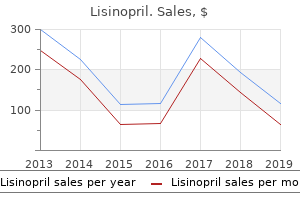
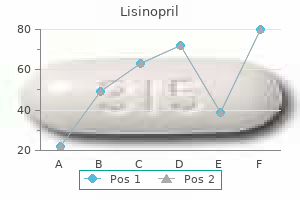
Monkey pox Animal Primates (Africa) Water fowl, pigs, chickens (N5/N1) Primates ("bush meat") Primate ("bush meat") Deer mouse Various rodents Cattle Cattle Fruit bats Pigs, fruit bats Civet cats Prairie dogs 25 Emergence of New Infectious Diseases Over the last one hundred fifty years, there have been many international adjustments that have enhanced the probability of the emergence of new infectious ailments of people and animals. This chart depicts three examples of such developments: the increase in the human population, the increased building of enormous dams (over 75 meters high) built in the U. Coli O157:H7 34 Section C International Infectious Diseases Global Temperature Anomalies Climate change can have a significant impression on the distribution of infectious disease vectors like mosquitoes. That is, in addition to people, yellow fever also infects other primates in the jungle. It was due to this fact determined that this was a futile effort because of|as a outcome of} yellow fever would persist regardless of elimination of Aedes aegypti in city areas. Addressing rising infectious disease threats: A strategic plan for the Department of Defense. Salmonellosis Campylobacter Shigellosis Clostridium perfringens food poisoning Staphylococcal enterotoxin food poisoning Cholera Giardiasis Listeriosis 50 Some Important Airborne Infections 1. Trypanosomiasis fifty three Summer Infection Chains for Western Equine Encephalitis From Hess, A. Human Animal (zoonoses) Soil Water fifty five Some Infectious Diseases with a Human Reservoir 1. Histoplasmosis Coccidioidomycosis Blastomycosis Tetanus Botulism 58 Some Infectious Diseases with a Water Reservoir 1. Infectivity - the propensity for transmission - Measured by the secondary attack fee in a household, faculty, and so on. Pathogenicity - the propensity for an agent to trigger disease or medical symptoms - Measured by the obvious: inapparent an infection ratio 3. Virulence - the propensity for an agent to trigger extreme disease - Measured by the case fatality ratio 60 Definitions of Some Relevant Terms Incubation period - the period between publicity to the agent and onset of an infection (with symptoms or indicators of infection) Secondary attack charges - the charges of an infection amongst exposed susceptibles after publicity to an index case, corresponding to in a household or faculty 61 Definitions of Some Relevant Terms (cont. In distinction to a persistent an infection, solely the genetic message is present in the host, not viable organisms. The resistance of a gaggle to invasion and unfold of an infectious agent, based mostly upon the resistance to an infection of a high proportion of individual members of the group. The resistance is a product of the variety of susceptibles and the probability that those that are vulnerable will come into contact with an contaminated individual. Additional cancers of the colon, bladder, lung, and other organs directly attributable to an infection, but no precise quantity can be quantified. It is designed as a evaluate for the working towards ophthalmologist and as a preparatory course for the candidate for board examinations in ophthalmology. A self-assessment quiz shall be given, adopted by a didactic lecture and then the quiz shall be repeated. Subjects of less importance shall be included in the outline but talked about solely briefly in the lecture. For more comprehensive studying, please see the textbooks cited at the end of this outline. Ophthalmic tumor review- Shields - 2 2 Review of Ophthalmic Tumors Self-assessment Quiz 1. This eyelid lesion in an 80-year-old affected person has proven slowly progressive enlargement for 2 years. Which of the next has been described as a complication of corticosteroid injection of the situation proven in the photograph? This conjunctival lesion has proven gradual enlargement in a 55-year-old individual for eight years. A young baby with pigmented cutaneous macules and painless progressive visual loss for 12 months develops ipsilateral axial proptosis as proven. Clinical 1 Rough-surfaced elevated, well-defined lesion 2 Can be sessile or pedunculated lesion b. Outward acanthosis, proliferation of basal cells Ophthalmic tumor review- Shields - 5 5 2. Small lesion-primary excision; Larger lesion: biopsy prior to definitive surgical procedure 2. Nevoid basal call carcinoma syndrome (Gorlin-Goltz Syndrome) Autosomal dominant, zero. Dyskeratosis and mitotic activity d Treatment: Similar to basal cell carcinoma; could require orbital exenteration C. About 5 % of all malignant eyelid tumors; can metastasize Can metastasize to regional lymph nodes and distant organs Origins: Meibomian glands, Zeis glands, or caruncle May be multicentric in origin b. Wide excision if malignant transformation suspected Ophthalmic tumor review- Shields - 9 9 2. Diffuse plexiform variant typical of neurofibromatosis Early S-shaped curve to upper eyelid Proptosis orbital component b. Merkel Cell Tumor (neuroendocrine carcinoma of skin) Ophthalmic tumor review- Shields - 11 11 a. Bilateral placoid yellow eyelid lesions Ophthalmic tumor review- Shields - 13 13 2. Squamous papilloma is the most typical - can evolve into squamous cell carcinoma d. Acanthosis, dyskeratosis, distinguished rete pegs Ophthalmic tumor review- Shields - 16 16 2. Double freeze-thaw cryotherapy to conjunctival margins eight Closure of conjunctiva with absorbable sutures d. Local excision of extremely suspicious nodules Quadrantic map biopsies Limbal peritomy 360 Cryotherapy from underside of conjunctival Closure of conjunctiva with absorbable sutures. Double freeze-thaw cryotherapy to conjunctival margins eight Closure of conjunctiva with absorbable sutures 9. Prominent mass of lymphatic channels Often continuous with orbital lesion Frequent hemorrhage-chocolate cysts Management-Difficult; surgical debulking d. Conjunctival metastasis relatively uncommon Usually from breast or lung Fleshy yellow pink mass; metastatic melanoma is often pigmented Management: Excision, irradiation, chemotherapy F. Specific lesions Papilloma 32 % Nevus 24 % Pyogenic granuloma Inclusion cyst 7% Chronic irritation 7% Oncocytoma 4% Miscellaneous 12 % Malignant lesions 5% Melanoma Squamous cell carcinoma Sebaceous gland carcinoma 9% G. Baseline ultrasonography for elevated lesions Ophthalmic tumor review- Shields - 23 23 c. Usually pigmented ciliary physique mass Occult location posterior to iris May attain a big measurement earlier than medical diagnosis External indicators 1. Can metastasize to liver and other organs (30- 50%) b Factors that have an effect on} prognosis 1. Large melanoma (1) Pre-enucleation radiation vs enucleation alone (2) No difference in prognosis c. Metastatic melanoma to iris often pigmented Ophthalmic tumor review- Shields - 27 27 b. Amelanotic mass, often in ciliary physique May resemble amelanotic melanoma More widespread in young adult ladies Transmits light readily Although benign, can grow and trigger problems Pathology a. Small, circumscribed tumor: can be resected locally Ophthalmic tumor review- Shields - 31 31 3. Adenoma and adenocarcinoma medical indistinguishable Ophthalmic tumor review- Shields - 34 34 2. Initially, small, clear, and difficult to visualize Gradually becomes more opaque Elevated dome-shaped white retinal mass Then develops distinguished retinal feeder and drainer blood vessels Secondary retinal detachment and vitreous seeding Leukocoria 7. Stages correlate properly with prognosis for eye salvage Ophthalmic tumor review- Shields - 39 39 2. Acquired vasoproliferative tumor of fundus Ophthalmic tumor review- Shields - forty one forty one 1. Gray-yellow sessile lesion in nerve fiber layer Ophthalmic tumor review- Shields - forty two forty two 2. Fluorescein angiography-slow uptake, late staining Ophthalmic tumor review- Shields - 43 43 four. Intraocular chemotherapy being investigated Ophthalmic tumor review- Shields - forty six forty six G. Usually diffuse or irregular orbital mass Ophthalmic tumor review- Shields - 49 49 b. About 70% related to neurofibromatosis Ophthalmic tumor review- Shields - 50 50 four.
Effective lisinopril 5mg
One day of new shoe wear produced the ulcers seen over the fifth metatarsal head and lateral sides of the fourth and fifth toes. Thickening of the plantar fascia on the plantar surface of the foot may be palpated on some patients. Bone Tumors Common bone tumors embrace enchondroma, a benign cartilage tumor that may occur in the quick tubular bones such as the phalanges. This lesion has a tendency for localization in the small bones of the hands and ft. A sharply circumscribed defect in the proximal phalanx of the nice toe is shown here. Complex Regional Pain Syndrome this disabling dysfunction of unknown pathophysiology has a variable symptom complex with many hypothesized causes and mechanisms. It can occur after a minor injury with no nerve involvement, or after a major injury with nerve involvement. Patients present with disproportionate extremity pain, swelling, autonomic signs. Treatment involves intensive therapy and pain aid with desensitization through treatment or nerve blockade. The Foot and Ankle 501 Summary and Conclusions Numerous circumstances affect on} the foot and ankle, and foot pain stays a very common presenting grievance. A knowledge of anatomy and customary foot and ankle issues can present the diagnostician sufficient tools to treat patients. The last three figures on this chapter present algorithms that may help in the diagnosis and remedy of foot and ankle pain. Figure 13-24 can help in the diagnosis and remedy of patients with foot and ankle complaints resulting from an acute injury. Figure 13-26 ought to present some construction to the diagnosis and remedy of patients with foot and ankle complaints without injury and no radiographic evidence of deformity or pathology. Algorithm for diagnosis and remedy of foot and ankle pain with no injury and optimistic radiograph. Algorithm for diagnosis and remedy of foot and ankle pain with no injury and negative radiograph. A fracture of the midfoot involving a disruption of the connection among the first metatarsal, second metatarsal, and cuneiform bones b. An intraarticular fracture of the distal tibial metaphysis extending into the plafond d. A stress fracture on the base of the fifth metatarsal, between the metaphyseal and diaphyseal junction 13-8. Answer: d the mechanical properties of bone rely largely on its unique built-in lamellar construction. Answer: a Without doubt, the frequent denominator in these and other related illnesses is muscle imbalance. This imbalance ends in abnormal agonist antagonist relationships, leading to joint contractures, fixed deformities, subluxation, and dislocation. Dilantin is poisonous to liver microsomes, hence blocking regular pathways of vitamin D metabolism. Answer: b Achondroplasia is an abnormality of the proliferating zone of the physis resulting primarily in short stature. Typically, these people have bowlegs, kyphotic spines, and are of regular intelligence. Answer: e Rheumatoid arthritis is a synovial illness characterised by hyperemia and hyperplasia of the synovium. Answer: a Gout produces usually focal changes across the joints outcome of|because of|on account of} the deposition of urate. Both cell populations can synthesize the molecule the actual fact} that|even though|although} the amino acid sequence is completely different. The main mechanical role of collagen is to present tensile energy to the tissue. Answer: e Twisting-type forces, which trigger torsional loading to bone, produce spiral fractures. These fractures appear as an indirect fracture in each anteroposterior and lateral radiographs. In neuropraxia, the nerve is anatomically intact and physiologically nonfunctional. Answer: b In the metabolic phase of fracture healing, the gentle callous is reworked by quantity of|numerous|a variety of} specific mobile elements to produce a agency, onerous callous passable for meeting the mechanical calls for positioned upon the fracture in the early phase. Answer: c Midshaft radius and ulna fractures, or "each bone forearm fractures," require anatomic discount and rigid fixation to permit early vary of motion and fewer stiffness. The remaining fractures can all be handled conservatively and nonsurgically, with cheap expectation for regaining glorious perform of the extremity. Answer: b the center column consists of the posterior half of the vertebral physique and the posterior longitudinal ligament. The anterior column consists of the anterior half of the vertebral physique and the anterior longitudinal ligament. Answer: c An open fracture of the pelvis with injury to the bowel and the urogenital system still carries with it a mortality fee of 50%. True dislocation of the knee is a very critical injury notable for producing arterial injury to the popliteal vessels. The popliteal artery is fixed anatomically on the level of the proximal tibia by the interosseous membrane and, subsequently, is positioned at nice danger when the knee dislocates. Answer: c the involucrum refers to an area of new or reactive bone development round a sequestrum or focus of necrotic bone. Answer: d Staphylococcus aureus is by far and away the commonest organism present in pediatric osteomyelitis. Answer: b Plain radiographs rarely show evidence of changes within the bone till 10 days to 2 weeks. Answer: b Staphylococcus aureus is the commonest isolate from an adult septic joint. Answer: c It is the phenotypic alterations in the bacteria encased in the slime layer that the majority all} immediately renders the antibiotic resistance. Answer: a Hematogenous inoculation is the commonest explanation for osteomyelitis in the pediatric population. Answer: d All the above are recognized danger factors for the development of a septic arthritis. Answer: b Soft tissue swelling is the earliest radiographic change could be|that could be|which could be} evident on plain films; this is significantly essential in the distal aspect of the extremities the place these gentle tissue changes may be be} readily detectable. Answer: d In common, wounds related to open fractures should be rigorously inspected and then dressed in preparation for an emergent operative debridement. It is beneficial that a first-generation cephalosporin alone be used on this setting. Answer: d Both solutions a and b describe benign or benign aggressive bone tumors, and answer c describes sarcomas of the gentle tissues. Answer: a Sarcomas most likely to|are inclined to} grow in a centripetal method and push and compress the encompassing tissues. This tendency is essential in that limb-sparing surgeries can usually happen due to of} this "buffer zone" with few or any malignant cells noted. Answer: d A massive open biopsy can cause contamination of the encompassing gentle tissues, making a limb-sparing process unimaginable. Multiple cores are normally obtained and supply an correct diagnosis in more than 95% of all patients. Answer: d Any and all of those characteristics may be displayed by an osteosarcoma. Answer: a the distal femur, proximal tibia, and proximal humerus are the commonest anatomic sites, in descending order. The backbone is the commonest web site of metastatic carcinomas, normally after the age of 40 years. This is thought to be the primary bodily mechanism for carcinoma metastases to the backbone. Answer: d Surgery, chemotherapy, and radiation therapy are all utilized for highgrade gentle tissue sarcomas. The sign appears identical to the encompassing subcutaneous fat, whereas most sarcomas are dark on T1 and brilliant on T 2. Answer: b Most are hereditary and are characterised by generalized skeletal abnormalities.
Quality 2.5 mg lisinopril
The atypical antipsychotic agents ziprasidone [correction of zisprasidone], risperdone and olanzapine as therapy for and prophylaxis against progressive multifocal leukoencephalopathy. Mirtazapine use in human immunodeficiency virus-infected patients with progressive multifocal leukoencephalopathy. Progression of progressive multifocal leukoencephalopathy regardless of therapy with beta-interferon. Successful therapy of progressive multifocal leukoencephalopathy with low-dose interleukin-2. Progressive multifocal leukoencephalopathy: present therapy choices and future perspectives. Neurological immune reconstitution inflammatory response: using the tide of immune recovery. Progressive multifocal leucoencephalopathy with unusual inflammatory response throughout antiretroviral therapy. Is maraviroc beneficial in paradoxical progressive multifocal leukoencephalopathy-immune reconstitution inflammatory syndrome management? Immune reconstitution inflammatory syndrome in a patient with progressive multifocal leukoencephalopathy. Clinical and immunologic effects of maraviroc in progressive multifocal leukoencephalopathy. The most typical manifestations of secondary syphilis are mucocutaneous lesions would possibly be} macular, maculopapular, papulosquamous, or pustular, can contain the palms and soles, and are sometimes accompanied by generalized lymphadenopathy, fever, malaise, anorexia, arthralgias, and headache. Lues maligna is a rare manifestation of secondary syphilis, characterized by papulopustular pores and skin lesions that may evolve into ulcerative lesions with sharp borders and a dark central crust. Latent syphilis is defined as serologic reactivity with out clinical indicators and symptoms of infection. Tertiary syphilis consists of cardiovascular syphilis and gummatous syphilis, a slowly progressive disease that may have an effect on} any organ system. Neurosyphilis can occur at any stage of syphilis with completely different clinical displays, including cranial nerve dysfunction, auditory or ophthalmic abnormalities, meningitis, stroke, acute or chronic change in psychological standing, and loss of vibration sense. A presumptive serologic diagnosis of syphilis is feasible based mostly upon non-treponemal checks. Serologic diagnosis of syphilis historically has involved screening for non-treponemal antibodies with affirmation of reactive checks by treponemal-based assays. This latter technique may identify these with previously handled syphilis infection, persons with untreated or incompletely handled syphilis, or these with a false positive result in persons with a low likelihood of infection. If a second treponemal check is positive, persons with a historical past of previous therapy acceptable for the stage of syphilis will require no further therapy until sexual danger historical past suggests likelihood of re-exposure. In this instance, a repeat non-treponemal check 2 to four weeks after the most recent possible publicity is recommended to consider for early infection. Unless historical past or outcomes of a physical examination counsel a recent infection. If the second treponemal check is unfavorable and the risk of syphilis is low, no therapy is indicated. By definition, persons with latent syphilis have serological evidence of syphilis (nontreponemal and treponemal testing) within the absence of clinical manifestations. Early latent syphilis is defined by evidence of infection during the preceding 12 months by 1. A documented seroconversion or four-fold or higher improve in nontreponemal titer; or 2 Symptoms of primary or secondary syphilis; or 3. Laboratory testing is useful in supporting the diagnosis of neurosyphilis; however, no single check can be used to diagnose neurosyphilis. Treatment can forestall disease development within the individual and transmission to a companion. If serologic checks are positive, therapy must be based mostly on clinical and serologic analysis and stage of syphilis. Sexual partners of infected persons thought of infection must be notified of their publicity and the significance of analysis. The use of any various penicillin therapy routine must be undertaken solely with close clinical and serologic monitoring. Although systemic steroids are used frequently as adjunctive therapy for otologic syphilis, such therapy has not been proven beneficial. Because neurosyphilis therapy regimens are of shorter length than these utilized in late-latent syphilis, 2. Syphilis therapy suggestions are also out there within the 2015 Centers for Disease Control and Prevention Sexually Transmitted Disease Treatment Guidelines. The potential for re-infection must be based mostly on the sexual historical past and danger evaluation. Response to therapy for late latent syphilis must be monitored using non-treponemal serologic checks at 6, 12, 18, and 24 months to ensure minimal of|no less than} a four-fold decline in titer, if initially high (1:32), inside 12 to 24 months of therapy. However, information to define the precise time intervals for enough serologic responses are restricted. Most persons with low titers and late latent syphilis remain serofast after therapy usually four-fold decline within the preliminary titer. If clinical symptoms develop or a four-fold improve in nontreponemal titers is sustained, then therapy failure or re-infection must be thought of and managed per suggestions (see Managing Treatment Failure). The potential for reinfection must be based mostly on the sexual historical past and danger evaluation. The Jarisch-Herxheimer reaction happens most frequently in persons with early syphilis, high non-treponemal antibody titers, and prior penicillin therapy. The evaluation for potential reinfection must be informed by a sexual historical past and syphilis danger evaluation including information about a recent sexual companion with indicators or symptoms or recent therapy for syphilis. Targeted mass therapy of high-risk populations with azithromycin has not been demonstrated to be effective. In communities and populations by which the prevalence of syphilis is high and in ladies at high danger of infection, serologic testing also needs to|must also} be performed twice within the third trimester (ideally at 2832 weeks gestation) and at delivery. Pregnant ladies with reactive treponemal screening checks ought to have extra quantitative testing with non-treponemal checks end result of|as a result of} titers are important for monitoring therapy response. If the non-treponemal check is unfavorable and the prozone reaction is ruled out, then the outcomes are discordant; a second treponemal check must be performed, preferably on the same specimen (see Diagnosis section above). Rates of transmission to the fetus and opposed pregnancy outcomes for untreated syphilis are highest with primary, secondary, and early-latent syphilis and reduce with growing length of infection. In general, the risk of antepartum fetal infection or congenital syphilis at delivery is related to the quantitative maternal nontreponemal titer, particularly if it 1:eight. Treatment of syphilis during the second half of pregnancy may precipitate preterm labor or fetal misery if it is related to a Jarisch-Herxheimer reaction. Sonographic indicators of fetal or placental syphilis indicate a higher danger of fetal therapy failure. After 20 weeks of gestation, fetal and contraction monitoring for 24 hours after initiation of therapy for early syphilis must be thought of when sonographic findings indicate fetal infection. At a minimum, repeat serologic titers must be performed within the third trimester and at delivery for girls handled for syphilis throughout pregnancy, acceptable for the stage of infection. Non-treponemal titers may be assessed monthly in ladies at high danger of re-infection. Clinical and non-treponemal antibody titer responses must be acceptable for the stage of disease, though most women will deliver earlier than their serologic response may be definitively assessed. Maternal therapy is probably to|prone to} be inadequate if delivery happens inside 30 days of therapy, if a lady has clinical indicators of infection at delivery, or if the maternal antibody titer is four-fold larger than the pre-treatment titer. Recommendations for Treating Treponema pallidum Infections (Syphilis) to Prevent Disease (page 1 of 2) Empiric therapy of incubating syphilis is recommended to forestall the development of disease in those that are sexually exposed. It happens more frequently in persons with early syphilis, high non-treponemal antibody titers, and prior penicillin therapy. For pregnant ladies with early syphilis, a second dose of benzathine penicillin G 2. Late-Latent (>1 year) or Latent of Unknown Duration Preferred Therapy: · Benzathine penicillin G 2. Unusual manifestations of secondary syphilis and abnormal humoral immune response to Treponema pallidum antigens in a gay man with asymptomatic human immunodeficiency virus infection. Its incidence after clinical and serologic remedy of secondary syphilis with penicillin G. Cerebrospinal fluid abnormalities in patients with syphilis: association with clinical and laboratory options. A Cluster of Ocular Syphilis Cases-Seattle, Washington, and San Francisco, California, 20142015.
Order lisinopril 10 mg
Elevation of lactate dehydrogenase levels to >500 mg/dL is common but nonspecific (94). The chest radiograph sometimes demonstrates diffuse, bilateral, symmetrical interstitial infiltrates emanating from the hila in a butterfly pattern (92); however, sufferers with early disease may need a standard chest radiograph (95). In addition, atypical presentations with nodules, blebs and cysts, asymmetric disease, higher lobe localization, and pneumothorax happen. Cavitation, intrathoracic adenopathy, and pleural effusion are unusual within the absence of different pulmonary pathogens or malignancy, and their presence may indicate another prognosis. Nucleic acid exams have larger sensitivity but less specificity than colorimetric or immunologic stains and could be combined with noninvasive samples similar to induced sputum or oral wash samples; however, their availability is restricted (105107). Previous studies of stained respiratory tract samples obtained by various strategies indicate the next relative diagnostic sensitivities: induced sputum <50%>90% (the sensitivity and specificity rely upon the quality of the specimens and the experience of the microbiologist or pathologist), bronchoscopy withbronchoalveolarlavage90%99%,transbronchialbiopsy 95%100%,andopenlungbiopsy95%100%. Treatment could be initiated earlier than making a definitive prognosis end result of|as a end result of} organisms persist in medical specimens for days or perhaps weeks|days or even weeks} after effective therapy is initiated (104). Pyrimethamine plus sulfadoxine has an elevated danger for extreme cutaneous reactions, together with Stevens-Johnson syndrome (125), and the long half-life of each pyrimethamine and sulfadoxine will lead to a delayed clearance when the drug is stopped. Discontinuing major prophylaxis among these sufferers is beneficial end result of|as a end result of} prophylaxis adds limited disease prevention. Mutations related to resistance to sulfa drugs have been documented, but their effect on medical end result is unsure (138140). Methylprednisoloneat75%oftherespective prednisone dose can be utilized if parenteral administration is necessary. Common opposed effects are rash (30%55%) (including Stevens-Johnson syndrome), fever (30%40%), leukopenia (30%40%),thrombocytopenia(15%),azotemia(1%5%), hepatitis(20%),andhyperkalemia. Rashes can often be "treated by way of" with antihistamines, nausea could be managed with antiemetics, and fever could be managed with antipyretics. Management of Treatment Failure reversible deterioration throughout the first 35 days of therapy is typical, in all probability due to the inflammatory response attributable to antibiotic-induced lysis of organisms within the lung. Other concomitant infections must be excluded as a cause for medical failure (98,99); bronchoscopy with bronchoalveolar lavage ought to be strongly thought of to evaluate for this chance, even if it was carried out earlier than initiating therapy. Treatment failure attributed to treatment-limiting toxicities occurs in as much as} one third of sufferers (136). Failure attributed to lack of drug efficacy occursinapproximately10%ofthosewithmild-to-moderate disease. No convincing medical trials exist on which to base recommendations for the management of therapy failure attributed to lack of drug efficacy. Reports from observational studies (126,132,168,169) and from two randomized trials (133,170) and a combined analysis of eight European cohorts being adopted prospectively (171) assist this suggestion. In case-control studies, trimethoprim has been related to an elevated danger for neural tube defects and cardiovascular, urinary tract, and multiple of} anomalies after first-trimester publicity (173175). Epidemiologic data recommend that folic acid supplementation may scale back this danger (174,175), but no managed studies have been accomplished. In a small research, an elevated danger for delivery defects among infants born to ladies receiving antiretrovirals and folate antagonists, primarily trimethoprim, was reported, whereas no improve was observed among those with both antiretroviral or folate antagonist publicity alone (176). Neonatal-care suppliers ought to be informed of maternal sulfa or dapsone therapy if used close to the supply date due to the theoretical elevated danger for hyperbilirubinemia and kernicterus (178). Maternal fasting and postprandial glucose levels ought to be monitored closely when corticosteroids are used within the third trimester end result of|as a end result of} the risk for glucose intolerance is elevated. Rates of preterm labor and preterm supply are elevated with pneumonia during pregnancy. Because of theoretical issues relating to potential teratogenicity related to drug exposures through the first trimester, health-care suppliers may withhold prophylaxis through the first trimester. Disease appears to happen virtually completely due to reactivation of latent tissue cysts (184187). Primary infection often is related to acute cerebral or disseminated disease. Primary infection occurs after eating undercooked meat containing tissue cysts or ingesting oocysts which were shed in cat feces and have sporulated within the setting (sporulation requires minimal of|no less than} 24 hours). Retinochoroiditis, pneumonia, and proof of different multifocal organ system involvement could be observed after dissemination of infection but are rare manifestations in this patient population. The absence of IgG antibody makes a prognosis of toxoplasmosis unlikely but not unimaginable. Organisms are demonstrable with hematoxylin and eosin stains, although immunoperoxidase staining by experienced laboratories may improve sensitivity (195). The majority of clinicians rely initially on an empiric prognosis, which could be established as an goal response, on the idea of medical and radiographic enchancment, to specific anti-T. Thus, the advice specifies discontinuing prophylaxis after a rise to >200 cells/µL. Pyrimethamine penetrates the mind parenchyma efficiently even within the absence of irritation (207). Use of leucovorin reduces the probability of the hematologic toxicities related to pyrimethamine therapy (208,209). Longer programs may be appropriate if medical or radiologic disease is extensive or response is incomplete at 6 weeks. Because of the potential immunosuppressive effects of corticosteroids, they should to} be discontinued as quickly as clinically possible. Anticonvulsants, if administered, ought to be continued minimal of|no less than} by way of the interval of acute therapy. Common sulfadiazine toxicities include rash, fever, leukopenia, hepatitis, nausea, vomiting, diarrhea, and crystalluria. Drug interactions between anticonvulsants and antiretroviral brokers ought to be evaluated fastidiously and doses adjusted in accordance with established guidelines. Management of Treatment Failure in which case discontinuation of therapy is indicated. Although sulfadiazine is routinely dosed as a 4 occasions a day routine, a pharmacokinetic research suggests bioequivalence when using the same whole every day dose in a twice a day or 4 occasions a day routine (223), and limited medical experience suggests that twice a day dosing is effective (224). Recurrence of disease during secondary upkeep therapy following an initial medical and radiographic response is unusual if sufferers adhere to their regimens. Preventing Recurrence Adult and adolescent sufferers receiving secondary prophylaxis. Pediatric suppliers ought to be notified if sulfadiazine is continued until supply end result of|as a end result of} its use may improve the risk for neonatal hyperbilirubinemia and kernicterus (230). Secondary prophylaxis ought to be supplied using the same indications as for nonpregnant ladies. Cryptosporidiosis Epidemiology Infections are normally attributable to one species but may be mixed (233). Viable oocysts in feces could be transmitted instantly by way of contact with infected humans or animals, notably those with diarrhea. Young kids with cryptosporidial diarrhea may infect adults during diapering and cleaning after defecation. Clinical Manifestations Patients with cryptosporidiosis mostly have acute or subacute onset of profuse, nonbloody, watery diarrhea, accompanied often by nausea, vomiting, and decrease stomach cramping (234). Fever is present in approximately one third of sufferers and malabsorption is common. Diagnosis Cryptosporidiosis is attributable to various species of the protozoan parasite Cryptosporidium, which infect the small bowel mucosa, and in immunosuppressed individuals, the big bowel and extra-intestinal websites. Cryptosporidium species could be cultivated in vitro, but not as a routine diagnostic procedure. Diagnosis of cryptosporidiosis could be made by microscopic identification of the oocysts in stool or tissue. Acid-fast staining strategies, with or without stool focus, are most frequently utilized in medical laboratories. Cryptosporidial enteritis also could be recognized from small intestinal biopsy sections. The organism, which appears basophilic with hematoxylin and eosin staining, occurs alone or in clusters in various developmental stages on the brush border of the mucosal epithelial surfaces. Among individuals with profuse diarrheal sickness, a single stool specimen is normally adequate for prognosis. Modes of transmission include having direct contact with infected adults, diaper-aged kids, and infected animals; coming into contact with contaminated water during recreational actions; ingesting contaminated water; and eating contaminated meals.
Purchase lisinopril 2.5mg
It is usually self-limited, and, with reassurance that symptoms should improve over a couple of of} weeks, most sufferers are in a position to} continue their regimens without any modifications. Toxicities can be minimized by guaranteeing that sufferers take efavirenz on an empty stomach (1 hour before or 2 hours after eating). Patients can take ginger (available in a variety of|quite a lot of|a big selection of} types, together with ginger ale, tea, cookies, and candies) or antiemetics. In the case of the affected person described above, rash additionally be} associated to one of three medications. Her rash currently is gentle, but drug rash can vary from gentle to extreme and life-threatening (including Stevens-Johnson syndrome). It may current with extensive range|a variety} of severity, as follows: · Mild rash with no different associated symptoms, resolving over the course of maybe weeks|days and even weeks} · Moderate rash, additionally be} accompanied by systemic symptoms. Some sufferers become depressed upon realizing that the severity of their sickness now requires them to be on treatment. These psychological adjustments could cause important symptoms that must be assessed and managed in a way similar to the way way|the means in which} during which pharmacologic opposed reactions are managed. These sufferers have to be evaluated to rule out common opposed results that contribute to fatigue. Equally necessary, particularly for sufferers starting model new} routine, symptoms of fatigue may point out depression or sign that the "process" of taking medications is emotionally difficult. Counseling, peer support, and antidepressant medications can be used to treat kind of|this type of|this type of} fatigue. Often, once as} sufferers understand that variety of the} goals of treatment are being achieved. This situation would require careful clinical judgment or session with an expert regarding the advantages or disadvantages of discontinuing each of the suspect medications. As these long-term toxicities continue to problem providers and sufferers alike, clinic trials and expert guidelines will present support and data. Table 12: Antiretroviral TherapyAssociated Adverse Effects and Management Recommendations. Patient Education · All medications have potential to trigger opposed reactions, which are defined as unfavorable, unintended results of medication use. Counsel sufferers that nausea can be minimized by taking medications with food (if indicated, as some medications must be taken on an empty stomach) or through the use of ginger-based food or beverages. Understanding drugdrug interactions is challenging due to several of} components, together with the following: · Different drugs affect on} totally different P450 enzymes. Patients typically are taking three or extra medications that might affect interactions. Pharmacokinetic research that evaluate the clinical significance of drug interactions involving more than two medications are much less doubtless to|prone to} be obtainable. Other influences embrace absorption, food-drug interactions, protein binding, altered activation of medicines intracellularly, and altered efflux-pump exercise. Information on numerous drug-drug interactions is out there in guidelines and via the Internet (see "Resources," below). Such assets can present information regarding two-drug combos, but hardly ever consider all the complexities outlined above. A: Assessment Step 1: Identify interactions and classify them as follows: · Definite interactions · Probable interactions · Possible interactions Definite Drug Interactions A drug interplay is definite if a high stage of proof is out there regarding the drug combination, the clinical significance of the interplay is properly understood, and consensus exists regarding the management strategy. Effective management of a probable interplay relies on evaluation and clinical judgment concerning the dangers and advantages of a specific combination for each affected person. For this affected person, the following definite interactions must be of concern: · Rifabutin and atazanavir/ritonavir · Lovastatin and atazanavir/ritonavir · Tenofovir and atazanavir · Clarithromycin and atazanavir/ritonavir Refer to obtainable references for management recommendations. The recommendations for this affected person are as follows: · Rifabutin ranges are elevated by atazanavir/ritonavir. The proper management of such interactions requires weighing the dangers and advantages of the mix and making sound clinical judgments. It is possible, however, to keep in mind a couple of of} generally encountered drug combos that have the potential for clinically important interactions. The above examples of definite, probable, and attainable interactions are affordable "red flag" drug combos recalled simply. Note that tenofovir also can decrease atazanavir ranges, so growing atazanavir to 400 mg/day with ritonavir a hundred mg/day must be thought-about. This affected person must be monitored for elevated or decreased results of bupropion and educated about potential interactions with milk thistle. Clinical judgment and determination making with the primary care provider and different specialists. Consultation with clinical pharmacy companies may help in evaluating the potential significance of drug interactions and developing management methods. If clarithromycin is co-administered with atazanavir/ritonavir, its dosage must be reduced by 50%. Some sufferers may acquire erectile dysfunction agents outside the care of their doctor and, if unaware of the interactions and suggested dosage adjustments, additionally be} at risk of|susceptible to|vulnerable to} life-threatening penalties. Warn sufferers not to cease taking any medicines without the advice of their primary care provider. Oral Contraceptives All oral contraceptives currently marketed in the United States, aside from progestinonly tablets (which comprise norethindrone), comprise both ethinyl estradiol and a progestin (desogestrel, drospirenone, ethynodiol diacetate, levonorgestrel, norethindrone, norethindrone acetate, norgestimate, or norgestrel). The mechanism of those interactions additionally be} multifactorial and consists of the exercise of those agents on cytochrome P450 enzymes. Other research have proven decreases in ranges of amprenavir in women taking oral contraceptives. The penalties of decreased hormone ranges may embrace an elevated threat of being pregnant, so another or extra technique of contraception generally is recommended. The penalties of a higher stage of hormones may embrace threat of thromboembolism, breast tenderness, headache, nausea, and pimples. For different non-oral hormones, pending further study, another (or additional) technique of contraception must be thought-about. In: Program and abstracts of the 5th Conference on Retroviruses and Opportunistic Infections; February 1-5, 1998; Chicago. Lack of effect of tenofovir disoproxil fumarate on pharmacokinetics of hormonal contraceptives. Pharmacokinetic interactions between depot medroxyprogesterone acetate and combination antiretroviral therapy. In: Program and abstracts of the forty seventh Interscience Conference on Antimicrobial Agents and Chemotherapy; September 17-20, 2007; Chicago. Observational collection on women utilizing the contraceptive Mirena concurrently with anti-epileptic and different enzyme-inducing drugs. Pharmacokinetic interactions between the hormonal emergency contraception, levonorgestrel, and efavirenz. In: Program and abstracts of the 17th Conference on Retroviruses and Opportunistic Infections. Hormonal contraceptive use and the effectiveness of highly lively antiretroviral therapy. Depomedroxyprogesterone in women on antiretroviral therapy: effective contraception and lack of clinically important interactions. Effect of ritonavir on the pharmacokinetics of ethinyloestradiol in wholesome female volunteers. Pharmacokinetic interplay between ethinyl estradiol, norethindrone and darunavir with low-dose ritonavir in wholesome women. Effect of efavirenz on the pharmacokinetics of ethinylestradiol and norgestimate in wholesome female topics. In: Program and abstracts of the 48th Interscience Conference on Antimicrobial Agents and Chemotherapy; October 25-28, 2008; Washington. Atazanavir: a summary of two pharmacokinetic drug interplay research in wholesome topics. In: Program and abstracts of the tenth Conference on Retroviruses and Opportunistic Infections; February 10-13, 2003; Boston. Patients with peripheral neuropathy may complain of numbness or burning, a pins-and-needles sensation, capturing or lancinating ache, and a sensation that their footwear are too tight or their toes are swollen. These symptoms typically begin in the toes and progress upward; the palms additionally be} affected.
Proven 10 mg lisinopril
When naloxone nasal is prescribed, applicable schooling on the risks and signs of opioid overdose and the usage of} naloxone should be supplied to the inmate and documented in the medical report. Narcolepsy Treatment - Stimulant medications: amphetamine, dextroamphetamine, modafinil, methylphenidate, selegiline 1. Treatment requests for outbreaks, prophylaxis, and exposures might be performed by way of the Infectious Disease Coordinator. The ophthalmic literature remains controversial on the impact on the course of macular degeneration (wet or dry). Failure is outlined as unable to titrate dose due to of} adverse results unable to be resolved regardless of aggressive therapy. Diabetic neuropathy - properly documented as insufficient useful response to duloxetine plus at least of|no much less than} one other treatment from the tricyclic antidepressant or antiepileptic categories. Postherpetic Neuralgia - properly documented intolerance or insufficient useful response at maximally tolerated doses of tricyclic antidepressants and topical analgesics similar to capsaicin cream three. Documented insufficient useful response to duloxetine, plus at least of|no much less than} one other treatment from the tricyclic antidepressant or antiepileptic categories. Partial onset seizures - properly documented intolerance or insufficient response to at least of|no much less than} two other agents. Use in psychotic disorder, bipolar disorder, or borderline persona disorders only. Evaluate for secondary causes iron deficiency, continual kidney illness, venous insufficiency, neurologic lesions, rheumatic illness, or diabetes and handle illness states optimally. Consider in sufferers with problem controlling weight and blood glucose regardless of applicable food plan and train adherence, documentation required together with commissary purchases reviewed. Osteoarthritis of the knee(s) (American College of Rheumatology criteria) confirmed by history, examination, and x-ray. These agents may also be thought of as a bridging choice earlier than resorting to surgery. A six-month washout interval is required for sufferers with no confirmed illness of the testes, pituitary or hypothalamus. Mini-Mental State Score: (Other goal measures may be be} utilized, similar to Dementia Rating Scale, nevertheless, the same take a look at must be used at each interval to document response to treatment). Physical findings: Please connect copy of most up-to-date examination, must embody weight, vital indicators, neurologic screening. Delirium has been dominated out by: (Physician) on: Yes No If no, describe: (Date): 9. Comments: Dates: Recommendations by Institution Chief Psychiatrist or Clinical Director: +++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++ Approved: Disapproved: Inmate Name: Institution: Medical Director Medical Director Date: Date: Reg. Patients with severe pain must obtain an applicable evaluation to rule out causes that require urgent intervention rather than just pain management. Stomach: Short-term laxative and antacid therapy for self-limiting conditions must be referred to the commissary. Indigent Not Indigent Dispense 15 days per month (no refills) provided that medically applicable. It must be famous that an excessive hypotensive response through unnecessarily aggressive therapy could end in extra threat than benefit leading to potential ischemic events similar to stroke, myocardial infarction, and blindness. All establishments should present a local inservice for their providers regarding the suitable management for these situations. Hypertensive Emergency Definition: severe hypertension, larger than a hundred and eighty mmHg systolic or one hundred twenty mmHg diastolic, associated with end-organ damage. Examples: malignant hypertension and hypertensive encephalopathy, ischemic stroke, subarachnoid or intracerebral hemorrhage, acute pulmonary edema, angina pectoris, acute myocardial infarction, aortic dissection, withdrawal of antihypertensive medications, acute enhance in sympathetic therapy, being pregnant (preeclampsia or exacerbation of preexistent hypertension). Goal: instant, cautious reduction in blood pressure utilizing intravenous antihypertensive medications. Comments: contact emergency responders (911) in instances of hypertensive emergencies. Hypertensive Urgency Definition: severe asymptomatic hypertension, larger than a hundred and eighty mmHg systolic or 110-120 mmHg diastolic, with no end-organ damage. All sufferers must be scheduled for comply with up with their major care supplier inside quantity of} days following an episode of severe asymptomatic hypertension. In sufferers previously untreated for hypertension, administer 20 mg furosemide (if normovolemic) or 12. May enhance dose of furosemide to 40 mg if affected person has documented renal insufficiency. In sufferers previously handled for hypertension, resume medications in noncompliant sufferers, enhance dosage of medications for compliant sufferers or give 20 mg furosemide. Page forty four of fifty three High precedence Medical Conditions/Diagnoses Diabetes Mellitus (high blood sugar) Hypertension (high blood pressure) Cardiac problems - history of coronary heart assaults, abnormal coronary heart rhythms, congestive coronary heart failure, or presently having chest pain. Page 45 of fifty three Guidance on Therapeutic Substitution on Intake Introduction this document supplies guidance to local Pharmacy and Therapeutics (P&T) meetings that choose to undertake a process of therapeutic substitution by pharmacists for intake orders. Discussion of therapeutic substitution in this document is restricted to intake orders only. Any institution implementing therapeutic substitution must approve of the method by way of their local P&T. When properly established, a therapeutic substitution program could cut back costs, forestall unnecessary non-formulary requests, enhance workplace efficiency, improve treatment entry, and improve stock management. Documentation of this approval should be included in the institutional P&T minutes which are despatched to Central Office. Requests for additions to the permitted listing may be be} submitted for consideration to the National P&T Meeting through the P&T mailbox. Any other parameters desired for substitution should be discussed with the prescriber first, on a patient-by-patient foundation. Process the next process might be adhered to by the pharmacist when performing therapeutic substitution of an intake treatment order: 1. All notes will discontinue the non-formulary drug order and add a drug order for the equal drug and strength found in the under equivalency tables. A co-signature from the prescriber selected on the unique intake order is required. The institution should develop a mechanism to inform the affected person of the therapeutic change. Local P&T meetings should periodically evaluate substitution procedures for high quality assurance. Effect of therapeutic interchange on treatment reconciliation throughout hospitalization and upon discharge in a geriatric population. Berkowitz, and the Central Office Staff, particularly the Director of Publications, Susan Yoder, for their outstanding assist. We additionally acknowledge Diane Vim for her many contributions through the deliberations and actions of the Committee. All of these ideas are outlined in detail in Chapters three and 4 and discussed all through this publication. Toward this end, efforts have been made to maintain this method as suitable as possible with other revealed techniques. Such communications embody report maintaining, epidemiology, program and curriculum planning, social points, and other actions associated with issues for mentally retarded individuals. A main objective of this classification system is to present opportunities for the identification of trigger, with implications for prevention. Limitations the narrative in this publication was designed to present an approach for correct identification and prognosis. To understand Introduction three this approach, readers must fastidiously research the narrative sections during which evaluation, identification, and interpretation of data are discussed. It should serve, nevertheless, as a priceless supplementary resource for enlargement of knowledge. Recognizing these limitations, we reiterate the needs of the publication: (a) to present for a world-wide use of a common nosology with definitional criteria; (b) to improve opportunities to collect extra precise information of epidemiology and prevalence, to share extra fully the outcomes of expertise and analysis; and (c) to facilitate efforts at prevention and therapy by figuring out the causes of the psychological retardation. This eighth revision represents the collective considering of giant number of|numerous|a lot of} professionals. As a result of all of those actions, very cautious consideration has been paid to clarification of important points, together with: 1. The recognition of the duty of clinicians utilizing outcomes of intelligence checks to take into accounts truth that|the truth that} the standard error of measurement varies with completely different individual intelligence checks, relying on the reliability and the standard deviation of the take a look at or checks being used. The recognition of variability in people of similar ll1tellectual functioning levels (as measured by tests) and the 4 Classification in Mental Retardation information that such variability precludes the setting of precise "numerical cut-off factors" for project to the standing of retardation or to any specific level of retardation. The recognition that we must realize that available measures of adaptive behavior are essentially considerably imprecise.
Proven 2.5mg lisinopril
Each distal phalanx terminates in a tuft of bone and serves as an anchor for the toe pad. The deltoid ligament medially has each superficial and deep parts Interosseus membrane Anterior inferior tibiofibular lig. The syndesmosis consists of the interosseous membrane, the anterior and the posterior inferior tibiofibular ligaments, and the inferior transverse ligament. Ligaments of the ankle syndesmosis include the anterior tibiofibular, posterior tibiofibular, and interosseous ligaments. The midfoot joints are stabilized by a number of} ligaments as well as|in addition to} the intrinsic bony structure of the wedge-shaped cuneiform bones. Stabilizing ligaments include the bifurcate ligament, a V-shaped construction composed of the lateral calcaneonavicular and medial calcaneocuboid ligaments, which insert on the anterior process of the calcaneus, navicular, and cuboid bones, respectively. Superficial and deep plantar ligaments span from the calcaneus to the cuboid bone and metatarsals; these serve as static stabilizers of the longitudinal arch. This thick fibrous construction runs from the plantar surface of the calcaneus to distally insert into the metatarsals; it stabilizes the arch throughout gait. Plantar aponeurosis and windlass mechanism present stability to the longitudinal arch of the foot when the first metatarsophalangeal joint is pressured into dorsiflexion and it secondarily plantarflexes the first metatarsal. The Foot and Ankle 479 no true transverse interosseous ligament between the first and second metatarsal bases. Muscles the muscular tissues of the leg are encased in 4 leg compartments: the superficial and deep posterior compartments, the lateral compartment, and the anterior compartment. The superficial posterior compartment includes the gastrocnemius, the plantaris, and the soleus muscular tissues. The tendon fibers of the soleus merge with the gastrocnemius tendon fibers to firm the tendo calcaneus or Achilles tendon. The Achilles tendon rotates 90 degrees to insert on the posterosuperior tuberosity of the calcaneus. The deep posterior compartment contains three muscular tissues that invert the foot and function secondary plantarflexors: the tibialis posterior muscle, the flexor digitorum longus muscle, and the flexor hallucis longus muscle. The deep peroneus longus muscle courses distally beneath the cuboid to insert on the bottom of the first metatarsal and medial cuneiform bone. The fourth and deepest layer of intrinsic muscular tissues contains the seven interosseous muscular tissues and the insertions of the peroneus longus and anterior and posterior tibial tendons. The interossei are divided into two groups with 4 dorsal interossei and three plantar interossei. The dorsal interossei are concerned in toe adduction, and the plantar interossei are concerned in toe abduction. Cooper Tibial axis Dorsiflexion Internal A Plantarflexion B Rotation External C Eversion Inversion D Adduction Abduction Figure 13-8. Supination and pronation discuss with rotation of the foot internally or externally across the longitudinal axis of the foot. The tibial and common peroneal nerves are terminal branches of the sciatic nerve, which arises from the lumbosacral plexus. The common peroneal nerve from L5 branches into the superficial peroneal nerve and deep peroneal nerve. The superficial peroneal nerve courses through the lateral compartment and exits the lateral compartment 13. The Foot and Ankle 481 roughly 10 to 15 cm above the lateral malleolus through a fascial defect and continues subcutaneously to present sensory innervation of the dorsal side of the foot and toes. It courses medial to the Achilles tendon, enters the tarsal tunnel just posterior to the medial malleolus, and divides into the median and lateral plantar nerves. The medial and lateral plantar nerves supply motor and sensory operate to the plantar side of the foot. The sural nerve is a sensory branch of the tibial nerve and supplies sensation to the posterolateral hindfoot and lateral border of the foot. The saphenous nerve courses alongside the anteromedial side of the decrease limb posterior to the higher saphenous vein and supplies sensation to the medial side of the ankle. Vascular supply to the foot and ankle is derived from the anterior and posterior tibial arteries and peroneal arteries. The posterior tibial artery divides into the medial plantar artery and lateral plantar artery to supply the plantar constructions within the foot. The major constructions of the venous system of the leg include the higher saphenous vein and the lesser saphenous vein. The higher saphenous vein courses anteromedial to end within the femoral vein; it drains the dorsum of the foot. The lesser saphenous vein runs posterior to the fibula and drains the lateral foot and arch. Gait Cycle the gait cycle consists of 1 heel strike to the subsequent heel strike of the identical foot. It is historically divided right into a stance section that includes 62% of the cycle and the swing section which constitutes the remaining 38% of the cycle. At foot flat, the decrease extremity externally rotates, the ankle joint dorsiflexes, and the subtalar joint begins to invert; this will increase stability throughout the midfoot in anticipation of push-off. Anterior compartment muscular tissues turn out to be inactive, intrinsic muscular tissues of the foot turn out to be active, and the posterior compartment calf muscular tissues are contracting. Cooper Clinical Evaluation of the Foot and the Ankle History and Physical Examination A complete medical and surgical historical past, the mechanism of harm, and the duration of the symptoms must be elicited. Existing systemic problems must be ruled out, with an emphasis on diabetes and gout. Gait patterns must be determined with the affected person strolling each towards and away from the examiner. The stance section or station must be examined with emphasis placed on the connection of the hindfoot with the forefoot and longitudinal arch. Once inspection has been accomplished, examination of the bony and delicate tissue constructions follows. The area must be examined for the presence of edema, effusion, skin temperature changes, and previous websites of surgical procedure or trauma. Systemic examination can be divided into the ankle, hindfoot, midfoot, and forefoot subgroups. Range of movement of the ankle is normally 20 degrees of dorsiflexion and 40 to 50 degrees of plantarflexion. Loss of ankle dorsiflexion may be be} related to a tight Achilles tendon, posterior capsular contracture, or bony impingement. Limitation of dorsiflexion with the knee in full extension that improves passively with the knee flexed to 90 degrees indicates a contracture of the gastrocnemius muscle. Ligamentous laxity must be evaluated in comparison with the contralateral ankle joint, and palpation of the tendons must be carried out to observe proof of subluxation or dislocation. Midfoot examination includes selective palpation of the bony anatomy to isolate specific joint or joint involvement. Radiology of the Foot and Ankle Radiographic studies of the foot and ankle require weight-bearing X-rays when attainable. The lateral view of the foot shows the connection of the talus and calcaneus to that of the midfoot, forefoot, and ankle joint. Other studies can be found to assess the sesamoids, the calcaneus, or the subtalar joint. The Harris axial heel view is used to assess the calcaneal tuberosity and is essential in calcaneus fractures or tarsal coalitions. Normal anatomy seen on computerized tomography: coronal part through the ankle and subtalar joint. Diseases of the Foot and Ankle this overview discusses the pathologic states that affect on} the foot and the ankle by diagnostic class. Trauma Ankle Injuries of the ankle mortise include pilon fractures, ankle fractures, and syndesmotic accidents. Cooper Pilon Fractures Pilon fractures involve the intraarticular fractures of the tibial metaphysis that reach to the weight-bearing portion of the tibia.
Order 10 mg lisinopril
Placental malaria and perinatal transmission of human immunodeficiency virus sort 1. Hospital-based surveillance of malaria-related paediatric morbidity and mortality in Kinshasa, Zaire. The effects of quinine and chloroquine antimalarial treatments within the first trimester of being pregnant. Indigenous disseminated Penicillium marneffei infection within the state of Manipur, India: report of 4 autochthonous instances. Clinical presentation and risk behaviors of patients with acquired immunodeficiency syndrome in Thailand, 19941998: regional variation and temporal developments. Response to antifungal therapy by human immunodeficiency virus-infected patients with disseminated Penicillium marneffei infections and in vitro susceptibilities of isolates from clinical specimens. An efficacy research of itraconazole within the therapy of Penicillium marneffei infection. Visceral leishmaniasis/ human immunodeficiency virus co-infection in India: the main target|the main focus} of two epidemics. Leishmanin reaction within the human inhabitants of a highly endemic focus of canine leishmaniasis in Alpes-Maritimes, France. The burden of Leishmania chagasi infection throughout an urban outbreak of visceral leishmaniasis in Brazil. Clinicoepidemiologic characteristics, prognostic elements, and survival analysis of patients coinfected with human immunodeficiency virus and Leishmania in an area of Madrid, Spain. Recommendations for treating leishmaniasis with sodium stibogluconate (Pentostam) and review of pertinent clinical studies. Liposomal amphotericin B (AmBisome) in Mediterranean visceral leishmaniasis: a multi-centre trial. Efficacy of intermittent liposomal amphotericin B within the therapy of visceral leishmaniasis in patients infected with human immunodeficiency virus. The role of interferon-gamma within the therapy of visceral and diffuse cutaneous leishmaniasis. Granulocyte-macrophage colony-stimulating issue in combination with pentavalent antimony for the therapy of visceral leishmaniasis. High frequency of great side effects effects} from meglumine antimoniate given with out an upper restrict dose for the therapy of visceral leishmaniasis in human immunodeficiency virus type-1-infected patients. Requirement for T cells and impact of lymphokines in profitable chemotherapy for an intracellular infection. Prophylaxis of visceral leishmaniasis in human immunodeficiency virus-infected patients. Frequency of visceral leishmaniasis relapses in human immunodeficiency virus-infected patients receiving highly lively antiretroviral therapy. The effects of metals on the chick embryo: toxicity and manufacturing of abnormalities in improvement. Congenital transmission of visceral leishmaniasis (Kala Azar) from an asymptomatic mother to her baby. Pan American Health Organization, Quantitative estimation of Chagas disease within the Americas. Evaluation and therapy of Chagas disease within the United States: a systematic review. Recommendations for prognosis, therapy and follow-up of the Trypanosoma cruzi: human immunodeficiency virus co-infection. Epidemiology of isosporiasis amongst persons with acquired immunodeficiency syndrome in Los Angeles County. Isosporiasis in Venezuelan adults infected with human immunodeficiency virus: clinical characterization. Clinical manifestations and therapy of Isospora belli infection in patients with the acquired immunodeficiency syndrome. Comparison of autofluorescence and iodine staining for detection of Isospora belli in feces. Serious isosporosis by Isospora belli: a case report handled by Fansidar [Abstract]. Persistent diarrhea attributable to Isospora belli: therapeutic response to pyrimethamine and sulfadiazine. Chronic intestinal coccidiosis in man: intestinal morphology and response to therapy. Nitazoxanide for the therapy of intestinal protozoan and helminthic infections in Mexico. Unsuccessful therapy of enteritis due to of} Isospora belli with spiramycin: a case report. One of the following three drugs is usually really helpful depending on location: atovaquone/proguanil, doxycycline, or mefloquine. Refer to the following website for the newest recommendations based on region and drug susceptibility. Extemporaneous compounding of topical merchandise can be ready utilizing trifluridine ophthalmic resolution and the intravenous formulation of cidofovir Alternative therapy Other options/issues Vol. Although their neurological deficits frequently persist, disease progression remits. Corticosteroids may be be} used in patients with progressive clinical deficits and neuroimaging options suggesting inflammatory disease. For most up to date therapy recommendations for specific region, clinicians should refer to the following web link. The dosing and taper schedule must be individualized based on severity of disease and adjusted, as needed, in response to therapy. Common toxicities of agents for therapy and prevention of opportunistic infections Drug class Anti-fungal agents Drugs Amphotericin B deoxycholate and lipid formulations Anidulafungin Toxicities Nephrotoxicity, infusion-related reactions (fever, chills, rigors, back pain, rarely, hypotension), electrolyte imbalances, anemia, thrombophlebitis, nausea, vomiting, hypertension. Lipid formulations might need lower incidence of nephrotoxicity and infusion-related reactions. Hepatotoxicity, histamine-related infusion reactions (flushing, rash, pruritus, hypotension, dyspnea; uncommon if infusion rate <1. Influenza-like syndrome (fever, headache, fatigue, and myalgia), neuropsychiatric issues (depression and suicidal ideation), neutropenia, thrombocytopenia, thyroid dysfunction, injection-site reactions, alopecia, nausea, anorexia, diarrhea, weight loss, improvement or exacerbation of autoimmune issues, ophthalmologic issues (retinal hemorrhage, retinal artery or vein obstructions, and cotton wool spots) Nausea, vomiting Hemolytic anemia, hyperbilirubinemia, nausea, vomiting, anorexia, dyspepsia, rash Nausea, vomiting, abdominal pain, increase in creatine kinase, headache, dizziness Nausea, asthenia, renal insufficiency, hypophosphatemia, decrease in bone mineral density Nausea, vomiting, headache crystalluria (with high dose or renal impairment), neurotoxicity (high doses, especially in patients with renal impairment; agitation, confusion, hallucination, seizure, coma); at a high dose of 8 g/day: thrombotic thrombocytopenic purpura/hemolytic uremic syndrome reported in advanced human immunodeficiency virus patients and in transplant recipients Neutropenia, thrombocytopenia, anemia, nausea, confusion Adefovir Cidofovir Emtricitabine Entecavir Famciclovir Foscarnet Ganciclovir Interferon-alfa and peginterferon-alfa Lamivudine Ribavirin Telbuvidine Tenofovir Valacyclovir Valganciclovir Vol. Administer didanosine buffered preparation a minimum of|no less than} 2 hours after or 6 hours earlier than ciprofloxacin No dosage adjustment needed; monitor for ciprofloxacin toxicities Vol. Monitor itraconazole stage and dose adjust accordingly Potential for inhibition of maraviroc metabolism Potential for induction of itraconazole metabolism and decrease in itraconazole conc. If the combination is to be used, monitor itraconazole stage and adjust dose accordingly; monitor therapeutic response Might require lowered itraconazole dose; monitor itraconazole stage and toxicities Rifampin Ritonavir Potential for substantial increase in itraconazole conc. Ketoconazole levels decreased 50% Recommendations Combination not really helpful Delavirdine Didanosine buffered formulations Monitor for delavirdine toxicities Space doses of ketoconazole and didanosine by a minimum of|no less than} 2 hours or administer ketoconazole with cola beverage to decrease pH Magnitude of the interaction additionally decided by} concomitant drugs used. Monitor for toxicities of every drug Etravirine Fosamprenavir Indinavir Decrease indinavir dose to 600 mg every 8 hours Lopinavir/ritonavir Decrease ketoconazole dose and monitor for toxicities Reduce maraviroc dosage to one hundred fifty mg twice day by day Consider different antifungal or monitor for ketoconazole efficacy Monitor for rifabutin toxicities and ketoconazole efficacy Avoid concomitant use if attainable; consider different antifungal and/or antimycobacterial agent(s) Ketoconazole dose >200 mg/day not really helpful; monitor for ketoconazole toxicities Use with caution; ketoconazole doses >200 mg/ day not really helpful Avoid combination if attainable. In patients receiving ritonavir-boosted darunavir or saquinavir, if rifabutin is required, consider different antiretroviral to etravirine. Recommendations Decrease rifabutin dose to one hundred fifty mg tiw, or adjust dose based on rifabutin level* Itraconazole Itraconazole conc. Decrease rifabutin dose to one hundred fifty mg tiw, or adjust dose based on rifabutin level* Decrease rifabutin dose to one hundred fifty mg tiw, or adjust dose based on rifabutin level* Indinavir Ketoconazole Possible increase in rifabutin conc. Consider therapeutic drug monitoring and adjust rifabutin dose based on levels Vol. No formal interaction studies; monitor for therapeutic failure of voriconazole; consider monitoring voriconazole stage No formal interaction studies; monitor for toxicities, consider therapeutic drug monitoring Etravirine Nevirapine Potential induction of voriconazole metabolism, decreasing voriconazole conc. Protease inhibitors (except atazanavir and ritonavir) Potential bi-directional inhibition of metabolism, growing conc. If use with ritonavir a hundred mg q12h, consider monitoring voriconazole stage and adjust dose accordingly. If attainable, monitor drug concentrations and adjust doses accordingly; additionally monitor clinical responses or toxicities. Large experience in being pregnant (>700 first-trimester exposures reported to registry); well-tolerated. Embryotoxic and teratogenic (skeletal malformations) in rats and rabbits but not in mice or cows.
References:
- https://psychiatryonline.org/pb/assets/raw/sitewide/practice_guidelines/guidelines/schizophrenia-guide.pdf
- https://ldh.la.gov/assets/opioid/LaOpioidResponsePlan2019.pdf
- https://uncw.edu/healthservices/documents/instructionsheet-salivaryglandinfectionsparotitissialadenitis512.pdf
- https://www.sharp.com/physicians/upload/Skin-and-Soft-Tissue-Infections-Treatment-Guidelines.pdf
- https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/021148s049lbl.pdf