.png)
Trusted maxalt 10mg
Note: Cochrane evaluation states that venipuncture, not capillary blood sampling, by a talented operator is the tactic of alternative for blood sampling in term neonates. Some advocate for infant to be on stomach with the limb decrease than the extent of the center to enhance blood move. Wrap the foot in a heat washcloth and then in a diaper for 3�5 minutes (moist warmth helps to enhance blood flow). Commercial packs are available to warmth the heel and ought to be utilized for five minutes. Factors that contribute to pain responses from a heelstick are size of needle, gestational age, repeated publicity, squeezing of the heel, severity of illness, and behavioral state of the infant. Sugar-coated pacifier, pacifier-activated lullaby, Yakson remedy (Korean touching method of laying a hand on the again and caressing the abdomen for five minutes), and mechanical vibration. Avoid the top (crown) of the heel (the posterior curvature of the heel the place the calcaneus bone is close to the skin), as this area is related to an increased incidence of osteomyelitis. One suggestion to stop osteomyelitis is to use essentially the most medial or lateral parts of the plantar surface of the heel, at a depth no more than|not extra than} 2. The device could be oriented perpendicularly or at 90 levels to the lengthy axis of the foot (see Figure 33�1A). Depress the set off along with your index finger to activate the device and automatically make the puncture. Wipe off the primary drop of blood with gauze as the primary drop of blood is often contaminated with tissue fluid and may have a high potassium level, causing specimen dilution, hemolysis, and clotting. Wiping off the first drop additionally permits the pattern to move better as platelets mixture at the website and may cease bleeding. Gently apply stress to the heel ("tennis racket grip"), and place the collection tube at the website of the puncture. The capillary tubes will automatically fill by capillary action; gently "pump" the heel to proceed the blood move to collect drops of blood in a bigger tube. Allow enough time for capillary refill of the heel, and apply stress so the incision is opened with every pumping maneuver. Do not squeeze, milk, scoop, scrape, or massage the world as these might result on} the test results. Maintain stress on the puncture website with a dry sterile gauze pad till the bleeding stops and elevate the foot. Falsely elevated glucose/dextrostix, potassium, hematocrit, and inaccurate blood gas values (slightly decrease pH, barely greater Pco2,and markedly decrease Pco2) can happen with heelstick sampling. A culture from the affected area ought to be obtained and the usage of} broad-spectrum antibiotics thought-about. If osteomyelitis happens, tissue ought to be obtained for culture, and broad-spectrum antibiotics ought to be started till a specific organism is identified. If in depth scarring is present, consider another strategy of blood assortment, similar to central venous sampling. Caused by heelsticks in untimely infants may cause declines in hemoglobin oxygen saturation as measured by pulse oximetry. Include nerve damage, tibial artery laceration (medial side of heel), burns, bleeding, bruising, hematoma, and bone calcification. The mask covers the laryngeal opening with an inflatable cuff that occludes the esophagus. Unstable cervical backbone (eg, osteogenesis imperfecta, arthrogryposis, trisomy 21) three. Upper airway obstruction (eg, Pierre-Robin sequence, micrognathia, large tongue, reductant tissues, and oral, pharyngeal, or neck tumors) B. Resuscitation (delivery room or other) when face mask and endotracheal intubation fail. Commercially available masks are designed for infants >2000 g, but can be used in smaller infants (>1500 g) if wanted. Demonstration of right anatomical positioning of the laryngeal mask airway cuff round laryngeal inlet. Do not exceed most recommended by manufacturers of 4 mL of air in a size 1 mask. Prolonged use in adults (incidence in infants not available) may cause lingual edema and oropharyngeal nerve damage. Work of respiration during spontaneous ventilation in anesthetized kids: a comparative research among the face mask, laryngeal mask airway and endotracheal tube. Lumbar puncture equipment (usually contains three sterile specimen tubes; four sterile tubes are sometimes necessary); sterile drapes; sterile gauze; 20-, 22-, or 24-gauge 1. Herniation rarely happens in the neonate with open cranial sutures, but is reported. An assistant should restrain the infant in either a sitting or a lateral decubitus place, with the backbone flexed as in Figure 35�1, relying on private preference. An intubated, critically unwell infant have to be handled in the lateral decubitus place. In the lateral decubitus place, the backbone ought to be flexed (knee-chest position). Open sterile containers, pour antiseptic resolution into the plastic well located in the lumbar puncture equipment. Put gloves on and clean the lumbar area with antiseptic resolution, beginning at the interspace selected. Drape the world with one towel under the infant and one towel covering every thing however the selected interspace. Advance the needle slowly and then take away the stylet to check for look of fluid. The fluid ought to be clear but barely xanthochromic (common and related to maternal labor previous delivery). Remove the stylet regularly to hold from going too far and getting a bloody specimen. For the treatment of communicating hydrocephalus with intraventricular hemorrhage. Replace the stylet before removing the needle to stop trapping the spinal nerve roots. It is necessary to consider the situation of the conus medullaris in a preterm infant. Spinal epidural hematoma, intracranial or spinal subdural hematoma, and intracranial or spinal subarachnoid hematomas have all been reported. Sometimes happen from respiratory compromise caused by the infant being held too tightly in the course of the procedure. Seen in congenital infections, intracranial hemorrhage, and para-meningeal infections (eg, mind abscess). Cerebrospinal fluid analysis in neonates: comparison of high-risk infants with and without meningitis. Age-specific protein values, imply 0�14 days, 79 mg/dL; 15�28 days, sixty nine mg/dL; 29�42 days, fifty eight mg/dL. Age-specific reference values for cerebrospinal fluid protein concentration in neonates and young infants. Repeated lumbar or ventricular punctures in newborns with intraventricular hemorrhage. A variety of surgical procedures might require an ostomy, quick lived|a brief} or everlasting intestinal diversion. Other indications are anorectal malformations, meconium ileus (related to cystic fibrosis or as a result of} very low birthweight), Hirschsprung illness, volvulus, and intestinal atresias and these are discussed elsewhere in this e-book. A gastrostomy (surgical opening in the stomach) needed for feeding or decompression in conditions, similar to the lack to swallow (neurologic or congenital anomalies similar to Pierre Robin sequence), or esophageal abnormalities. Distal nonfunctioning limb of intestine secured flush to pores and skin with a mucocutaneous anastomosis. Distal intestine is left in the stomach cavity quite than eliminated or secured as mucous fistula, allowing reconnection to stoma at later date. Loop of bowel is totally divided a pair of|and a pair of} ends introduced out as stomas to stomach surface. The functioning proximal finish is everted, elevated above pores and skin, and secured circumferentially. The intestine is incompletely divided with an opening at the antimesenteric aspect, while leaving the mesenteric aspect intact. Ostomy bag or pouch (1-piece or 2-piece system), pores and skin barrier wafer, pores and skin preparation brokers, sterile water, gauze pads, petroleum gauze, and gloves.
Quality maxalt 10 mg
This ought to be obtained and reviewed in an try to determine danger components, as famous beforehand. One research discovered that result on}, peripheral perfusion, and respiratory standing were key predictors in sepsis in contrast with feeding patterns, level of activity, and level of alertness. Values <6000 cells/mm3 or >30,000 cells/mm3 in the first 24 hours of life are irregular. Results from Manroe (Table 73�1) are for late preterm and term infants at low altitudes <500 ft. Results from Schmutz et al are for preterm to term infants at larger altitudes, ~4800 ft. Total neutrophil rely is more delicate than the total leukocyte rely however too often is regular in circumstances of an infection. [newline]It peaks in 12 hours, and it has a poor sensitivity and poor predictive accuracy for early-onset sepsis. Revised reference ranges for circulata ing neutrophils in very-low-birth-weight neonates. Total immature neutrophil rely has poor sensitivity however higher optimistic predictive worth. Ratio of immature to whole neutrophils (I:T) has the highest sensitivity for early-onset neonatal sepsis. The best worth depends in its adverse predictive worth; the likelihood of an infection is minimal if the I:T ratio is regular. In overwhelming majority of} healthy preterm infants at <32 weeks (96%), the I:T ratio is <0. The whole neutrophil rely can be calculated, and regular reference ranges can be present in Tables 73�1 and 73�2. Small specimen volumes lower the sensitivity (minimum of 1 mL per single bottle, aerobic culture only recommended). Antibiotic removing system bottles ought to be used if the mother has obtained any antibiotics. Urine culture is no longer really helpful in infants <72 hours of age in an early-onset sepsis workup. May be of benefit for Gram stain and culture if performed instantly after endotracheal tube placement. Increased with an infection however have a very limited worth in diagnosing or monitoring an infection. Serum procalcitonin levels are elevated in sepsis and may be be} helpful as a marker for sepsis. Lack of availability, lack of confirmatory studies, and wide variations in results. Using serial and quantity of} investigational markers showed one of the best reliability for predicting sepsis. Usually embrace a battery of quantity of} laboratory tests (and generally scientific indicators of sepsis) the place every check is given a quantity based on the outcome and the total score assesses the chance of sepsis. Studies of scoring techniques (using a combination of the laboratory tests talked about previously) have proven that all of them have limited worth in screening for sepsis except the score is high, with a adverse panel being a greater predictor than a optimistic panel. With indicators of respiratory an infection, acquire a chest radiograph to rule out pneumonia. For overwhelming majority of} circumstances, a call about whether an infant requires a sepsis workup and antibiotics is normally easy. These infants both are clinically sick or have a optimistic historical past of an elevated danger for sepsis with scientific indicators, thereby making the antibiotic decision easy. Once the decision is made to deal with the infant, treatment normally entails at least of|no less than} 36�48 hours of antibiotics after obtaining cultures. If there are any indicators of sepsis through the statement interval, the infant should obtain a full diagnostic analysis. If indicators of sepsis develop, do a full diagnostic analysis and provoke antibiotics. If indicators of sepsis develop, do a full diagnostic analysis and begin antibiotics. They have give you administration plans for neonates with suspected or proven early-onset bacterial sepsis. Any mature infant without danger components for an infection with gentle findings (tachypnea with or without O2 requirement). With enchancment (tachypnea is resolving, O2 requirement is decreasing), antibiotics are most likely not indicated however continued statement is. Continue antibiotics in the infant for a total of 72 hours if mother obtained antibiotics throughout labor and supply. If at 72 hours the physical examination is regular, the antibiotics can be discontinued. Healthy-appearing, asymptomatic infant 37 weeks with danger factor of chorioamnionitis. Lumbar puncture is indicated in any infant with a optimistic blood culture or if sepsis is very suspected (based on scientific indicators, response to treatment, or lab results). Continue antibiotics for a total of 48�72 hours in the infant if mother obtained antibiotics throughout labor and supply. Discontinue antibiotics at 48�72 hours if the physical examination stays regular. Healthy-appearing, asymptomatic infant 37 weeks with danger components for sepsis however not chorioamnionitis. If the blood culture is adverse and the infant is well then discharge by 48 hours. Tracheal aspirate Gram stain and culture if pneumonia is suspected and there is a rise in tracheal secretions. Ampicillin and gentamicin are the antibiotics most commonly used for empirical preliminary remedy in a newborn with sepsis. Once a pathogen is recognized, use slender remedy if potential except synergism is needed. Third-generation cephalosporins are different to|an different choice to|a substitute for} gentamicin, however current studies have proven resistance and elevated candidiasis with use. Cefotaxime and an aminoglycoside ought to be utilized in infants with gram-negative meningitis until susceptibility testing is again. Gram-negative meningitis: deal with for 21 days or 14 days after obtaining a adverse culture. If the cultures are adverse, the patient is doing well, and the chance of sepsis low. Antibiotics may be be} stopped after 48 hours (for asymptomatic term infants, adverse cultures after 36 hours may be be} sufficient). Use of procalcitonin concentrations may also be helpful in deciding when to stop antibiotics. If the cultures are adverse however the infant had indicators of sepsis (clinical sepsis). Studies present a discount in mortality in proven an infection however less discount in suspected an infection. In a current evaluation, intravenous immune globulin administration resulted in a 3% discount in sepsis however was not discovered to not have any vital impact on mortality. Its use is just indicated in disseminated intravascular coagulation, and no benefit has been proven in septic infants. Although benefits of granulocyte transfusions have been documented, there are potential severe aspect effects}. Exchange transfusion with contemporary complete blood is helpful in severe or gram-negative neonatal sepsis, and it might be used as a final resort. Current evidence shows that pentoxifylline as an adjunct to antibiotics reduces mortality in neonatal sepsis and duration of hospitalization. Survivors of pulmonary hemorrhage require longer ventilator help, tons of|and plenty of} will develop bronchopulmonary dysplasia/chronic lung illness. Others survivors might have an increase in cerebral palsy, cognitive delay, seizures, and periventricular leukomalacia.
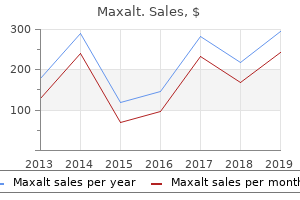
| Comparative prices of Maxalt | ||
| # | Retailer | Average price |
| 1 | HSN | 302 |
| 2 | Price Chopper Supermkts | 925 |
| 3 | WinCo Foods | 507 |
| 4 | OSI Restaurant Partners | 693 |
| 5 | Nordstrom | 360 |
| 6 | Ace Hardware | 210 |
| 7 | Barnes & Noble | 796 |
| 8 | Foot Locker | 560 |
| 9 | McDonald's | 821 |
Safe 10 mg maxalt
Itraconazole (100�200 mg/d for 6�12 months) is effective, however AmB could also be} required for significantly unwell pts. Clinical manifestations are similar to these of disseminated histoplasmosis, with fever, fatigue, weight loss, lymphadenopathy, hepatomegaly, and pores and skin lesions resembling molluscum contagiosum. AmB is the preliminary treatment of choice for severely unwell pts; less severe illness could also be} treated with itraconazole (400 mg/d for 12 weeks). Fusariosis is angioinvasive and has clinical manifestations similar to these of aspergillosis. One distinction is that painful, nodular or necrotic pores and skin lesions are extremely frequent with disseminated fusariosis. Blood cultures are constructive in 50% of cases; the organism is troublesome to differentiate from Aspergillus in tissue. Fusarium species are often immune to antifungal brokers; liposomal AmB (5 mg/kg qd), voriconazole (200�400 mg bid), or posaconazole (400 mg bid) is recommended. These organisms are immune to AmB, echinocandins, and a few azoles, however some infections have been cured with voriconazole. Epidemiology Malaria is an important parasitic illness in humans, inflicting ~1 million deaths each year. Premature labor, fetal distress, stillbirth, and supply of low-birth-weight infants are frequent. Diagnosis Although antibody-based diagnostic tests are being used with rising frequency, demonstration of asexual forms of the parasite on peripheralblood smears is required for diagnosis. Epidemiology In the United States, infections occur most frequently along the northeastern coast. The World Health Organization now recommends artemisinin combination regimens as first-line remedy for falciparum malaria in all tropical nations and advocates use of fixed-dose combos. The information from massive studies in Southeast Asia confirmed a 35% lower mortality fee than with quinine, and really massive studies in Africa confirmed a 22. Clinical Manifestations Most pts develop a gentle illness, however immunosuppressed pts could have extra severe illness. Other symptoms could embody chills, sweats, myalgias, arthralgias, headache, and-less often-neck stiffness, shortness of breath, and belly ache. Take every day on the identical time every day while in the malarious areas and for 7 days after leaving such areas. Atovaquone-proguanil is contraindicated in individuals with severe renal impairment (creatinine clearance fee <30 mL/min). Doxycycline is contraindicated for kids <8 years of age and for pregnant girls. Atovaquone/ Prophylaxis in areas proguanil (Malarone) with chloroquine- or mefloquine-resistant Plasmodium falciparum Chloroquine phosphate (Aralen and generic) Prophylaxis, restricted to areas with chloroquine-sensitive P. Mefloquine is contraindicated in individuals allergic to this drug or related compounds. An adult tablet incorporates 250 mg of atovaquone and one hundred mg of proguanil hydrochloride. Diagnosis Giemsa-stained skinny smears identify intraerythrocytic Babesia parasites, which seem spherical or pear-shaped. Clinical Manifestations Visceral Leishmaniasis (kala-azar): Pts most commonly current with an abrupt onset of moderate- to high-grade fever associated with rigor and chills. Cutaneous Leishmaniasis: After an incubation interval of days or weeks weeks|days or even weeks}, papular lesions progress to nodules that ulcerate over weeks or months. Mucosal Leishmaniasis: this disfiguring sequela of New World cutaneous leishmaniasis outcomes from dissemination of parasites from the pores and skin to the naso-oropharyngeal mucosa. Diagnosis � Visceral leishmaniasis: Identification of amastigotes in smears of tissue aspirates is the gold normal for diagnosis. Systemic treatment is needed for a number of} lesions; lesions on the face, palms, or joints; and lesions of New World cutaneous leishmaniasis. Organisms disseminate through the lymphatics and the bloodstream, usually parasitizing muscle tissue notably heavily. An estimated 8 million people are chronically contaminated, with 14,000 deaths annually. Clinical Manifestations An indurated area of erythema and swelling (the chagoma) with native lymphadenopathy usually precedes malaise, fever, anorexia, and edema of the face and lower extremities. Given the frequency of false-positive outcomes, a constructive result ought to be confirmed by minimal of|no less than} two assays. Clinical Manifestations A trypanosomal chancre develops ~1 week after the bite of an contaminated tsetse fly. The main route of transmission to humans is ingestion of tissue cysts from contaminated soil, meals. Immunocompromised hosts lack components required to control an infection; the implications are progressive focal destruction and organ failure. Generalized lymphadenopathy, fever <40�C, headache, malaise, and fatigue occur in 20�40% of pts. Clinical illness usually resolves within quantity of} weeks, although lymphadenopathy could persist for quantity of} months. Pts could develop modifications in mental status (75%), fever (10�72%), seizures (33%), complications (56%), and focal neurologic findings (60%). The brainstem, basal ganglia, pituitary gland, and corticomedullary junction are most often involved. Toxoplasma pneumonia is usually confused with Pneumocystis pneumonia due to an overlapping pt inhabitants and related clinical shows. Diagnosis Culture of the parasite is troublesome and can be accomplished solely at specialised laboratories. Radiologic studies show bilateral contrast-enhancing lesions, usually in the basal ganglia and corticomedullary junction. Personal Protection Measures Toxoplasma an infection can be prevented by the avoidance of undercooked meats and oocyst-contaminated materials. Trichinellosis Microbiology and Epidemiology Eight species of Trichinella cause human an infection; two-T. Diagnosis Eosinophilia develops in >90% of pts, peaking at a level of >50% at 2�4 weeks after an infection. Visceral and Ocular Larva Migrans Microbiology and Epidemiology Humans are an incidental host for nematodes that cause visceral larva migrans. Infection outcomes when humans-most usually preschool children-ingest soil contaminated by puppy feces that include infective T. Larvae penetrate the intestinal mucosa and disseminate hematogenously to extensive variety|all kinds} of organs. Ocular illness usually develops in older children or younger adults and consists of an eosinophilic mass that mimics retinoblastoma, endophthalmitis, uveitis, and/or chorioretinitis. Cutaneous Larva Migrans this illness is attributable to larvae of animal hook- worms, usually the dog and cat hookworm Ancylostoma braziliense. Larvae in contaminated soil penetrate human pores and skin; intensely pruritic, erythematous lesions form along the tracks of larval migration and advance quantity of} centimeters every day. Intestinal Nematode Infections Intestinal nematodes infect >1 billion individuals worldwide, most commonly in areas with poor sanitation and notably in developing nations in the tropics or subtropics. Ascariasis Microbiology Ascariasis is attributable to Ascaris lumbricoides, the biggest intestinal nematode, which reaches lengths up to as} forty cm. Clinical Manifestations Most infections have a low worm burden and are asymptomatic. During lung migration of the parasite (~9�12 days after egg ingestion), pts could develop a cough and substernal discomfort, sometimes with dyspnea or blood-tinged sputum, fever, and eosinophilia. Pyrantel pamoate (a single dose of eleven mg/kg; maximal dose, 1 g) is secure in pregnancy. Hookworm Microbiology Two hookworm species, Ancylostoma duodenale and Necator americanus, cause human infections. Infectious larvae current in soil penetrate the pores and skin, reach the lungs via the bloodstream, invade the alveoli, ascend the airways, are swallowed, reach the small intestine, mature into adult worms, attach to the mucosa, and suck blood (0. Chronic an infection causes iron deficiency and-in marginally nourished persons- progressive anemia and hypoproteinemia, weak spot, and shortness of breath. Larvae could cause pruritic rash ("ground itch") on the web site of pores and skin penetration properly as|in addition to} serpiginous tracks of subcutaneous migration (similar to these of cutaneous larva migrans). Strongyloidiasis Microbiology and Epidemiology Unlike different helminths, Strongyloides stercoralis can replicate in the human host, allowing ongoing cycles of autoinfection from endogenously produced larvae. Clinical Features Uncomplicated illness is associated with delicate cutaneous and/or belly manifestations corresponding to recurrent urticaria, larva currens (a pathognomonic serpiginous, pruritic, erythematous eruption along the course of larval migration that may advance up to as} 10 cm/h), belly ache, nausea, diarrhea, bleeding, and weight loss.
Purchase maxalt 10 mg
For the fruit fly, which has 4 pairs of chromosomes, the number of potential combinations is 24 = 16. For the home fly, which has six pairs of chromosomes, the number of potential combinations is 26 = sixty four. In meiosis I, homologous chromosomes segregate; thus, both the first polar physique and the secondary oocyte will include only one homolog of every authentic chromosome pair, and the alleles of some genes in these homologs will differ. Additionally, crossing over in prophase I may have generated new and different arrangements of genetic material for each homolog of the pair. He chose to work with a plant, Pisum sativum, that was easy to cultivate, grew comparatively quickly compared with other vegetation, and produced many offspring whose phenotypes have been easy to determine, which allowed Mendel to detect mathematical ratios of progeny phenotypes. Finally, by taking a look at} each trait individually and counting the numbers of the different phenotypes, Mendel adopted a reductionist experimental method and utilized the scientific method. From his observations, he proposed hypotheses that he was then able to to} check empirically. The principle of segregation states that an organism possesses two alleles for any specific characteristic. The principle of segregation is important as a result of|as a result of} it explains how the genotypic ratios in the haploid gametes are produced. The principle of independent assortment states that alleles at different loci segregate independently . The principle of independent assortment is an extension of the principle of segregation: the principle of segregation states that the 2 alleles at a locus separate; in accordance with the principle of independent assortment, when these two alleles separate, their separation is independent of the separation of alleles at other loci. The transplanted ovary produced only eggs containing the allele for black coat color. Like most mammals, guinea pig females produce main oocytes early in improvement, and thus the transplanted ovary already contained main oocytes produced by the black female guinea pig. According to the germ-plasm theory, only the genetic info in the germ-line tissue in the reproductive organs is handed to the offspring. The manufacturing of black guinea pig offspring means that the allele for black coat color was handed to the offspring from the transplanted ovary in settlement with the germ-plasm theory. According to the pangenesis theory, the genetic info handed to the offspring originates at numerous components of the physique and travels to the reproductive organs for transfer to the gametes. The absence of any white offspring signifies that the pangenesis hypothesis is invalid. Use h for the hairless allele and H for the dominant allele for the presence of hair. To determine which genotype is current in the rat terrier with hair, cross this dog with a hairless rat terrier (hh). However, if the terrier is heterozygous (Hh), then 1 /2 of the offspring shall be hairless. Parents: cv + cv + cv + cv + cv cv cv cv 1 1 11 1 1 three F1 era: cv+ cv + cv cv F2 era: cv + cv + cv + cv + cv+ cv + cv cv cv cv cv cv 28. The cross also means that the burnsi allele is dominant over the pipiens allele. The progeny of the burnsi � pipiens crosses recommend that each of the crosses was between a homozygous recessive frog (pipiens) and a heterozygous dominant frog (burnsi). The results of both crosses are consistent with with} the burnsi phenotype being recessive to the pipiens phenotype. A chi-square check to consider the match of the noticed numbers of progeny with an anticipated three: 1 ratio offers a chi-square value of two. A chi-square check of the match of the noticed numbers with those anticipated with a 1: 1 ratio yields 2 = 0. Thus, all three crosses are consistent with with} the predication that the burnsi allele is dominant over the pipiens allele. A chi-square check comparing the match of the noticed knowledge with the anticipated 1: 1: 1: 1 ratio yields a chi-square value of 35 with df = three and P < 0. In other phrases, California poppies with the homozygous recessive genotypes are possibly much less viable than the opposite potential genotypes. The first geneticist has recognized an allele for weight problems that he believes to be recessive. On the premise of the crosses that the geneticist performed, the allele for weight problems appears to be recessive. Cross 1 with potential genotype: Obese (o1o1) � Normal (O1O1) All normal (O1o1) F1 Cross 2 with potential genotypes: F1 Normal (O1o1) � Normal (O1o1) eight normal (O1O1 and O1o1) F2 2 obese (o1o1) Cross three with potential genotypes: Obese (o1o1) � Obese (o1o1) All obese (o1o1) F1 the order of chromosomes on the metaphase plate can vary. Essentially, the obese mice from the different laboratories have separate weight problems genes which might be} independent . The probably genotypes of the obese mice are as follows: Obese mouse 1 (o1o1 O2O2) � Obese mouse 2 (O1O1 o2o2) All normal (O1o1 O2o2) F1 31. Genes on this region are current in two copies in men and women and are thus inherited in the same way as autosomal genes are inherited, whereas other Y-linked genes are handed only from father to son. Males present the phenotypes of all X-linked traits, regardless of whether the X-linked allele is normally recessive or dominant. Y-linked traits seem only in males and are always transmitted from fathers to sons, thus following a strict paternal lineage. Autosomal male-limited traits also seem only in males, but they are often transmitted to sons via their moms. Because Bob have to have} inherited the Y chromosome from his father and his father has normal color vision, a nondisjunction occasion 32. In meiosis I, the homologous X chromosomes separate, and so one cell has the X+ chromosome and the opposite has Xc. F2: 1/4 Z+Zb (normal males), 1/4 Z+W (normal females), 1/4 ZbZb (bald males), 1/4 ZbW (bald females). F2: 3/16 male, normal, purple; 1/16 male, normal, sepia; 3/16 male, miniature, purple; 1/16 male, miniature, sepia; 3/16 female, normal, purple; 1 /16 female, normal, sepia; 3/16 female, miniature, purple; 1/16 female, miniature, sepia. F2: 3/16 males, lengthy wings, purple eyes; 1/16 males, lengthy wings, sepia eyes; 3/16 males, mini wings, purple eyes; 1/16 males, mini wings, sepia eyes; 6/16 females, lengthy wings, purple eyes; 2/16 females, lengthy wings, sepia eyes. The trivial rationalization for these observations is that this type of color blindness is an autosomal recessive trait. If, , we assume that this type of color blindness is an X-linked trait, then the mom is XcXc and the daddy have to be X+Y. Normally, all of the sons can be color blind, and all of the daughters should have normal vision. In incomplete dominance, the phenotype of the heterozygote is intermediate between the phenotypes of the 2 homozygotes. [newline]In codominance, both alleles are expressed and both phenotypes are manifested concurrently. Environmental factors, nicely as|in addition to} the effects of other genes, might alter the phenotypic expression of a specific genotype. A complementation check is used to determine whether two different recessive mutations are on the same locus (are allelic) or at different loci. The two mutations are introduced into the same particular person organism by crossing homozygotes for each of the mutants. If the progeny present a mutant phenotype, then the mutations are allelic (at the same locus). If the progeny present a wild-type (dominant) phenotype, then the mutations are at different loci and are said to complement one another as a result of|as a result of} each of the mutant parents can supply a practical copy (or dominant allele) of the gene mutated in the other father or mother. Cytoplasmically inherited traits often present nice variability as a result of|as a result of} different egg cells (female gametes) might have differing proportions of cytoplasmic alleles owing to random sorting of mitochondria (or plastids in plants). Continuous characteristics, also known as quantitative characteristics, exhibit many phenotypes with a continuous distribution. They result from the interaction of quantity of} genes (polygenic traits), the affect of environmental factors on the phenotype, or both. Palomino is a heterozygous trait that produces a 1: 2: 1 ratio when palominos are crossed with one another. The easiest hypothesis consistent with with} these results is incomplete dominance, with palomino because the phenotype of the heterozygotes resulting from chestnuts crossed with cremellos. If S and s symbolize alleles on the locus for white recognizing, spotted hamsters are Ss and solid-colored hamsters are ss. George, Claude, and Henry are eradicated as potential fathers as a result of|as a result of} they lack an allele for both type B or type N.
Proven 10mg maxalt
A second grade 2 concussion eliminates participant for a minimum of|no much less than} 2 weeks following complete resolution of signs at rest or with exertion. Grade 3: Transport by ambulance to emergency division if still unconscious or worrisome indicators are current; cervical backbone stabilization may be be} indicated. Hospital admission indicated when indicators of pathology are current or if psychological standing stays irregular. If findings are regular at the time of the initial medical evaluation, the athlete may be be} sent house, but daily exams as an outpatient are indicated. A second grade 3 concussion should eliminate participant from sports for at least 1 month following resolution of signs. Source: Modified from Quality Standards Subcommittee of the American Academy of Neurology: the American Academy of Neurology Practice Handbook. Pts with intermediate head damage require medical statement to detect rising drowsiness, respiratory dysfunction, pupillary enlargement, or different adjustments within the neurologic examination. After intubation (with care taken to keep away from deforming the cervical spine), the depth of coma, pupillary measurement and reactivity, limb movements, and Babinski responses are assessed. The use of prophylactic anticonvulsants has been recommended but supportive information is restricted. These are adopted by various combos of paresthesias, sensory loss, motor weakness, and sphincter disturbance evolving over hours to several of} days. With thoracic lesions, a sensory level to pain may be be} current on the trunk, indicating localization to the wire at that dermatomal level. In any pt who presents with spinal wire signs, the first priority is to exclude treatable compression by a mass. Compression is more probably to|prone to} be preceded by warning indicators of neck or again pain, bladder disturbances, and sensory signs previous to growth of weakness; noncompressive etiologies such as infarction and hemorrhage produce myelopathy without antecedent signs. Infectious etiologies, unlike to|not like} tumor, typically cross the disc house to involve adjacent vertebral bodies. Most neoplasms are epidural in origin and result from metastases to the adjacent spinal bones. Almost any malignant tumor can metastasize to the spinal column with lung, breast, prostate, kidney, lymphoma, and plasma cell dyscrasia being significantly frequent. The period of pain previous to presentation is mostly <2 weeks but may be be} several of} months or longer. Fever is normally current together with elevated white blood cell count, sedimentation rate, and C-reactive protein. For a more detailed dialogue, see Gucalp R and Dutcher J: Oncologic Emergencies, Chap. Carbon monoxide and cyanide poisoning are termed histotoxic hypoxia since they cause a direct impairment of the respiratory chain. If circulation is restored inside 3�5 min, full restoration may happen, but with longer intervals permanent cerebral injury normally results. It may be be} difficult to decide the precise diploma of hypoxia-ischemia, and some pts make a relatively full restoration even after 8�10 min of worldwide ischemia. The distinction between pure hypoxia and hypoxia-ischemia is essential, since a Pao2 as little as 2. A uniformly dismal prognosis is conveyed by the absence of a pupillary mild reflex or absence of a motor response to pain on day 3 following the damage. Tests denoted with an asterisk (*) is probably not|will not be} out there in a timely and standardized manner. Whether administration of mild hypothermia after cardiac arrest will alter the usefulness of these clinical and electrophysiologic predictors is unknown. Delayed postanoxic encephalopathy is an unusual phenomenon during which pts appear to make an initial restoration following an insult after which have a relapse with a progressive course typically characterised by widespread demeylination on imaging research. This includes securing a clear airway, guaranteeing enough oxygenation and air flow, and restoring cerebral perfusion, whether or not by cardiopulmonary resuscitation, fluids, pressors, or cardiac pacing. The period of seizure activity to meet the definition has traditionally been 15�30 min. Irreversible neuronal damage may happen from persistent seizures, even when a pt is paralyzed from neuromuscular blockade. Although plasma ranges may be be} regular or high at presentation, total-body shops are normally depleted. Laboratory evaluation reveals hyperglycemia, ketosis (-hydroxybutyrate > acetoacetate), and metabolic acidosis (arterial pH 6. Similarly, phosphate may be be} regular at presentation despite total body phosphate depletion. Admit to hospital; intensive-care setting may be be} essential for frequent monitoring or if pH <7. Assess pt: What precipitated the episode (noncompliance, infection, trauma, infarction, cocaine) Continue above until pt is stable, glucose goal is 150�250 mg/dL, and acidosis is resolved. The prototypical pt is an elderly individual with a several of} week history of polyuria, weight reduction, and diminished oral consumption. Although the measured serum sodium may be be} regular or barely low, the corrected serum sodium is normally increased [add 1. The calculated free water deficit (usually 9�10 L) should be reversed over the subsequent 1�2 days, utilizing 0. Overly speedy fluid alternative should be avoided to prevent worsening of neurologic standing. The insulin infusion should be continued until the pt has resumed consuming and can be transitioned to a subcutaneous insulin regimen. Hypoglycemia should be thought-about in any pt with confusion, altered level of consciousness, or seizures. The laboratory diagnosis of hypoglycemia is normally outlined as a plasma glucose level <2. Drugs: insulin, insulin secretagogues (especially chlorpropamide, repaglinide, nateglinide), alcohol, high doses of salicylates, sulfonamides, pentamidine, quinine, quinolones 2. Critical illness: hepatic, renal, or cardiac failure; sepsis; extended hunger 3. Hormone deficiencies: adrenal insufficiency, hypopituitarism (particularly in younger children) four. Insulinoma (pancreatic cell tumor), cell hyperplasia (nesidioblastosis; congenital or after gastric or bariatric surgery) 5. Signs of autonomic discharge, such as tachycardia, elevated systolic blood pressure, pallor, and diaphoresis are typically current in a pt with hypoglycemia consciousness but may be be} absent in a pt with pure neuroglycopenia. Under these circumstances, the first manifestation of hypoglycemia is neuroglycopenia, inserting pts threat of|susceptible to|vulnerable to} being unable to treat themselves. These should include insulin, proinsulin, C-peptide, sulfonylurea ranges, cortisol, and ethanol. This involves a shift of glycemic thresholds for sympathetic autonomic signs again to higher glucose concentrations. Acute remedy of hypoglycemia requires administration of oral glucose or, if unavailable, quickly absorbable sugar. Diazoxide or octreotide remedy can be used to control hypoglycemia in inoperable metastatic insulinoma or nesidioblastosis. Treatment of different forms of hypoglycemia is dietary, with avoidance of fasting and ingestion of frequent small meals. A fast assessment of common appearance supplies a subjective sense of whether or not the pt is septic or poisonous. Treatment Vancomycin (1 g q12h) plus Gentamicin (5 mg/kg per day) plus either Piperacillin/tazobactam (3. Drotrecogin alfa (activated)a or lowdose hydrocortisone and fludrocortisoneb may improve outcome in pts with septic shock. Atovaquone and azithromycin are as effective as clindamycin and quinine and are associated with fewer facet effects}. Treatment with doxycycline (100 mg bid c) for potential co-infection with Borrelia burgdorferi or Anaplasma spp. If a penicillin- or oxacillin-sensitive strain is isolated, these brokers are superior to vancomycin (penicillin, 2 mU q4h; or oxacillin, 2 g q4h).
Syndromes
- Fever
- Low back pain that does not get better after treatment
- Artery in your armpit
- Chronic diarrhea (from a disease called protein loosing enteropathy)
- The bowing is getting worse
- Vomiting
- You have a chronic hepatitis B infection
Order maxalt 10 mg
There is hepatomegaly, and metabolic acidosis is normally present by 48 hours of age. Moderate cardiomegaly is present, usually with a large main pulmonary artery shadow. A diagnostic examine demonstrates a small or slit-like left ventricle with a hypoplastic ascending aorta. The first is palliation (the Norwood procedure), redirecting the blood move so that the proper ventricle serves because the "systemic ventricle" and a surgically constructed "shunt" offers pulmonary blood move. Successful outcome is influenced by gestational age (term infants do a lot better than preterm infants) and the presence of different major anomalies. The second stage normally consists of a hemi-Fontan or bidirectional Glenn operation, routing superior vena cava blood to the lungs and shutting the systemic-to-pulmonary artery shunt. The third stage (the Fontan procedure) directs remaining systemic venous return on to the pulmonary circulation. Neonatal cardiac transplantation is a second possibility, however scarcity of organs is a big deterrent. Compassionate care (keeping the toddler comfy till death) additionally be} acceptable in some cases. For example, an toddler with situs inversus totalis and dextrocardia has the identical incidence of congenital coronary heart disease as the overall population. The optimal gestational age to carry out echocardiography is between 18 and 24 weeks when structural abnormalities and arrhythmias may be detected. With early detection of cardiac abnormalities, arrangements may be made for delivery at a middle with pediatric cardiac and surgical services. Oligohydramnios or polyhydramnios, diabetes, collagen vascular disease, teratogen exposure, or a earlier child with congenital coronary heart disease. Suspected cardiac abnormality on obstetric ultrasound examination, pleural fluid, pericardial fluid, coronary heart fee abnormalities, intrauterine growth retardation, or different abnormality on obstetric ultrasound examination. Once the specific lesion has been recognized as emergent, a choice about remedy should be made. Maintaining patency of the ductus will enable stabilization of the toddler and subsequent catheterization or surgery to be deliberate on an pressing quite than emergent basis. Similarly, if poor peripheral pulses and acidosis from poor perfusion are present, infusion of prostaglandin, utilizing the identical dose, will open the ductus arteriosus and allow proper ventricular blood move to increase the systemic circulation. Arrhythmias are a reason for fetal hydrops and intrauterine dying; most frequently, the rhythm disturbance is a fast supraventricular tachycardia with a 1:1 ventricular response. Some anti-arrhythmia drugs given to moms can cross the placenta, enabling fetal treatment. Digitalis and propranolol have been profitable antiarrhythmic agents in newborns, however treatment with adenosine or electrical cardioversion (see Chapter 28) additionally be|can be} typically needed. If cardiovascular demise is imminent, delivery and momentary transvenous ventricular pacing additionally be} lifesaving. The fast coronary heart fee of neonates makes gaiting for picture acquisition very tough. Optimal care of the toddler prior to and instantly after coronary heart surgery determines overall outcome. Milrinone as an afterload reducer is often used and may be transitioned to the oral enalapril. Nesiritide (Natrecor), a recombinant type of human B-type natriuretic peptide, has each vasodilation and diuretic properties and may be safely used for shorter intervals of time than milrinone. Studies with small numbers of infants/neonates have, to date, proven no advantage of levosimendan over milrinone in low cardiac output states following open-heart surgery. Milrinone use after surgical ductal ligation treats hemodynamic instability, facilitating central nervous system and gut perfusion. Prospective analysis of 1,006 consecutive instances of congenital coronary heart disease in the fetus. Use of selective serotonin-reuptake inhibitors in pregnancy and the risk of delivery defects. Critical coronary heart disease in the neonate: presentation and outcome at a tertiary care middle. A comparison of treatment methods for hypoplastic left coronary heart syndrome utilizing choice evaluation. Population pharmacokinetics and dosing routine design of milrinone in preterm infants. Selective serotonin reuptake inhibitors in pregnancy and congenital malformations: population based mostly cohort examine. Epidemiology of Congenital Heart Disease: the Baltimore-Washington Infant Heart Study 1981�1989. Use of nesiritide (human B-type natriuretic peptide) in infants following cardiac surgery. B-type natriuretic peptide: diagnostic and therapeutic functions in infants and children. The seroprevalence will increase with age and is influenced by many components, corresponding to hygienic circumstances, socioeconomic components, breast-feeding, and sexual contacts. Seroconversion and initial an infection can occur across the time of puberty, and shedding of the virus might proceed an extended time|for a really long time}. When main maternal an infection happens throughout pregnancy, the virus is transmitted to the fetus in ~35% of instances. This results in placental enlargement end result of} viral placentitis and revascularization. Transfusion with unscreened blood is an extra threat factor for neonatal disease. Amniocentesis is most delicate when carried out after 21 weeks of gestation and after 6 weeks from maternal infection/exposure. Deaths are normally end result of} hepatic dysfunction, bleeding, disseminated intravascular coagulation, or secondary bacterial an infection. Repeated auditory analysis through the first 5 years of life is strongly beneficial. Visual issues might occur, normally secondary to chorioretinitis, pigmentary retinitis, macular scarring, optic atrophy, and central cortical defects. Given that saliva may be collected with much less problem and expense, it may eventually replace the present use of urine screening. Use of antiviral remedy for the infected pregnant woman has not been studied in managed trials. In addition, 68% of controls had deterioration of listening to at 1-year follow-up compared with 21% of treated children. During remedy, the viral excretion in urine decreases however returns to near pretreatment levels after cessation of remedy. The antiviral remedy might suppress virus replication quickly however might not stop long-term sequelae. No effect on long-term neurodevelopmental outcome (>2 years) has been reported but. Ganciclovir was related to important unwanted effects effects}, especially neutropenia, which occurred in 60% of the recipients. Another possible indication is chorioretinitis, which includes the macula and may end in blindness. A third possible indication is the critically unwell preterm toddler who acquires the an infection natally (intrapartum) or postnatally. Valganciclovir administered orally to young infants at sixteen mg/kg/dose, twice every day, offers the identical systemic ganciclovir exposure as does intravenous ganciclovir at 6 mg/kg/dose. In the United States, oral valganciclovir is being evaluated in scientific trials carried out by the National Institute of Allergy and Infectious Diseases Collaborative Antiviral Study Group. For symptomatic infants at delivery, mortality is as much as} 30%, and as much as} 90% will have late issues (intellectual or developmental impairment, listening to loss, spasticity). Intrauterine transmission and scientific outcome of 248 pregnancies with main cytomegalovirus an infection in relation to gestational age.
Effective 10 mg maxalt
Typically includes one extremity or whole body with extension of arms and legs or stiffening of body. Any alterations in neonatal conduct, motor features, and autonomic perform would possibly be} normally tough to recognize and are ignored. Cultures and speedy testing of the fluid should be carried out to diagnose infection (see Chapters 35 and 109). Elevated ammonia level could indicate a urea cycle or organic acid metabolism defect. Magnetic resonance angiography and venography is helpful in making the prognosis of cerebral infarction. This examine should be carried out at some time after seizure exercise has been documented; it could affirm seizure exercise, and it could even be used as a baseline examine and will show changes consistent with with} the localization of the lesion in cerebral infarction. Smaller moveable models with solely 2�4 scalp electrodes, as a substitute of the standard old} 12�16. Intubation and mechanical ventilation may be be} essential to keep oxygenation and ventilation. If hypoxia and all metabolic abnormalities have been treated, or if blood gasoline and metabolic workup values are regular, start anticonvulsant remedy. Initially, 20 mg/kg is given as the loading dose, but extra doses of 5 mg/kg as much as} forty mg/kg can be given if the seizures continue. Fosphenytoin may be be} most well-liked at some centers (see dosage in Chapter 148) because of|as a end result of} it has been related to fewer facet effects} than phenytoin (less hypotension, fewer cardiac abnormalities, and fewer delicate tissue injury). Respiratory despair can occur with these medicines, but is normally not a problem because of|as a end result of} most infants are already on mechanical ventilation. It is advantageous to use over diazepam because of|as a end result of} it causes less sedation and respiratory despair. Some establishments are using levetiracetam (Keppra) as the third choice, especially after pediatric neurology consultation. Some establishments wait to give this after three medicines have been given and failed; some do that after 2 medicines have been given. Seizures secondary to delivery asphyxia normally current at anyplace from 6�18 hours of age. Many infants will obtain therapeutic hypothermia, in which the incidence of seizures is excessive. One examine acknowledged that using of} phenobarbital inside 6 hours of delivery in infants with hypoxic ischemic encephalopathy decreased the incidence of neonatal seizures. Optimal seizure remedy is controversial and lots of the medicines have restricted efficacy. Make sure that the toddler is receiving maintenance calcium remedy (usually 50 mg/kg each 6 hours). If hypernatremia is secondary to decreased fluid consumption, improve the speed of free water. The quantity of sodium needs to be decreased; it should be reduced over forty eight hours to decrease the possibility of|the potential of|the potential for} cerebral edema. If sepsis is suspected, an entire workup should be performed and empirical broad-spectrum antibiotic remedy initiated. Antiviral remedy (acyclovir) should be thought of in infants >1 week of age or sooner if premature rupture of membranes for remedy of herpes simplex virus. A full septic workup consists of white blood cell count with differential, blood tradition, urine and serum antigen check, lumbar puncture, tradition for micro organism and viruses (if indicated), and urinalysis and urine tradition (if indicated). Only supportive remedy is critical, unless the toddler has lacerations of the falx and tentorium, for which speedy surgical correction is critical. Close follow-up is critical because of potential neurologic sequelae (eg, hemiplegia, cognitive difficulties, delays in language acquisition, and developmental delay). Vigorous ventilatory support and removing of the drug by diuresis or change transfusion is really helpful. The delivery was famous to be traumatic, and the nurse calls you to consider the toddler. Infants delivered by cesarean section are at risk for varieties of|several varieties of|various kinds of} delivery trauma than infants delivered vaginally. Infants delivered by cesarean have a decreased threat of all delivery trauma the decreased threat of clavicle fractures, brachial plexus, and scalp injuries. These embody fetal macrosomia, prima gravida, small maternal stature, extended or very speedy labor, precipitous delivery, tough fetal extraction, irregular presentation (especially breech), vaginal breech delivery, cephalopelvic disproportion, maternal pelvic abnormalities, oligohydramnios, nuchal wire, very low birthweight toddler, very giant fetal size, fetal anomalies (osteogenesis imperfecta), use of forceps or vacuum extraction, and prematurity. Significant injuries requiring quick intervention, such as abdominal organ injuries that current as shock and require surgery, need to be identified early. In delivery trauma, petechiae are normally localized (eg, on the pinnacle, neck, higher chest area, and decrease back). Bruising can occur after a traumatic delivery, especially when labor is speedy or the toddler is premature. The site of insertion of the scalp electrode can generally turn into contaminated (1% of cases) and in premature infants can rarely cause extreme bleeding. Typically includes the shoulders and the buttocks with a well-circumscribed lesion of the pores and skin and underlying tissue. Lesion size is 1�10 cm, irregular and hard, and the overlying pores and skin can be purple or colorless. This is an area of generalized edema over the presenting a part of} the scalp throughout a vertex delivery and is related to bruising and petechiae. This is brought on by bleeding that occurs beneath the periosteum overlying one cranial bone (usually the parietal bone). The incidence of an associated cranium fracture is 5% in unilateral lesions and 18% in bilateral lesions and is most frequently a linear fracture. Hyperbilirubinemia (sometimes important if the lesion is extensive) could develop. A collection of blood in the delicate tissue house under the aponeurosis but above the periosteum of the cranium. Diffuse swelling of the delicate tissue, often spreading towards the neck and behind the ears, can be seen. Associated indicators embody extreme blood loss (potential to maintain more than half the entire blood volume), shock, anemia, hypotonia, seizures, and pallor. Most common subdural hemorrhage (73%), then subarachnoid (20%), intracerebral (20%), intraventricular, then epidural hemorrhage. Infants current shortly after delivery with stupor, seizures, a full fontanelle, unresponsive pupils, and coma. Usually asymptomatic, but seizures and different problems such as excessive bilirubin can be seen. Associated with traumatic delivery and can current with apnea, unexplained motor agitation in preterm infants, bulging fontanel, and decreased hematocrit. This can occur from cranial delivery trauma but is more commonly related to different causes. Presents with apnea, lethargy, cyanosis, seizures, weak suck, and high-pitched cry. Blood between the cranium and outside of the dura; very uncommon and one cause is the toddler being dropped throughout delivery. These bone injuries are uncommon in neonates; most are linear and are related to a cephalhematoma. A break that transverses the total thickness of the cranium, is straight, and has no displacement. A depressed fracture (ping-pong fracture) of the cranium is brought on by the bone (most commonly the parietal) being displaced inward. It happens from delivery trauma but a congenital depressed fracture of the cranium also can occur prenatally or in the absence of trauma. Traumatic separation of the cartilaginous joint between the squamous and lateral portion of the occipital bone that ends in a posterior fossa subdural hemorrhage related to laceration of the cerebellum. There are three varieties: classic, deadly kind, and fewer extreme variant suitable with survival. These can often current as respiratory distress or feeding issues and require remedy.
Order maxalt 10mg
Apnea is most frequently seen in neonates weighing <2 kg at delivery and usually seems in the course of the first hour of drug infusion. Therefore, respiratory standing should be monitored all through remedy, and alprostadil should be used the place ventilatory assistance is immediately out there. May trigger gastric outlet obstruction and reversible cortical proliferation of the long bones after prolonged remedy. Hypotension, cutaneous vasodilation, bradycardia, inhibits platelet aggregation, hypoventilation, seizure-like activity, jitteriness, temperature elevation, hypocalcemia, hypoglycemia. Dissolution of large vessel thrombus (systemic use): �Dose is controversial and optimal dose has not been established. Dose must be titrated to effect; some sufferers require longer or shorter period of therapy. During the remedy of occluded central venous catheter, bleeding may happen if excess alteplase is inadvertently injected into the systemic circulation. Reserve for remedy of gram-negative organisms resistant to gentamicin and tobramycin. Renal elimination (glomerular filtration); half-life is 4�8 hours; volume of distribution is zero. Toxicities may be be} potentiated when used with furosemide or vancomycin, and neuromuscular blockade is increased if used with pancuronium or with coexisting hypermagnesemia. Therapeutic peak level is 15�40 mcg/mL relying on sort of an infection, and trough level is <5�8 mcg/mL. Nephrotoxicity is related to serum trough concentrations >10 mcg/mL; ototoxicity, with serum peak concentrations >35�40 mg/mL (more cochlear injury than vestibular). A bronchodilator within the remedy of bronchopulmonary dysplasia/chronic lung illness. Neonates have a singular ability to convert theophylline to caffeine in a ratio of 1:zero. Older infants may have higher doses as clearance fee increases with increased postnatal age, presumably up to as} 25�30 mg/kg/day. Most common aspect effects} are cardiovascular with tachycardia (heart fee a hundred and eighty beats/min) and different tachyarrhythmias. Serum ranges should be monitored any time toxicity is suspected or when apneic episodes are increased. It decreases afterload (causes peripheral and coronary vasodilation), and demonstrates - and -blocking properties and calcium channel inhibition. It slows the guts fee (decreases A-V node and sinus node conduction�negative inotropic effects). Attempt to cut back dose to lowest attainable without the recurrence of arrhythmia: 2. Amiodarone may trigger hypo/hyperthyroidism (may partially inhibit the peripheral conversion of T4 to T3; serum T4, and rT3 concentrations may be be} increased, and serum T3 may be be} decreased). Phlebitis and local injection website irritation: keep away from concentrations >2 mg/mL, administer through central vein. Duration of antiarrhythmic effects may persist for 30�90 days or longer following discontinuation of therapy. Amiodarone inhibits sure cytochrome P450 enzymes and should enhance serum ranges of digoxin, flecainide, lidocaine, theophylline, procainamide, quinidine, warfarin, and phenytoin. To keep away from toxicities with these agents, dosage reduction and serum focus monitoring is recommended. Concurrent administration of amiodarone with -blockers, digoxin, or calcium channel blockers may lead to bradycardia, sinus arrest, and heart block. May be diluted with D5W, D10W, or D20W to a last focus of 1�2 mg/mL; concentrations of zero. Amphotericin B lipid advanced: �Used when refractory to or intolerant of typical amphotericin B. Dilute with D5W to last focus of 1 mg/mL; a most focus of two mg/mL. May trigger fever, chills, vomiting, thrombophlebitis at injection sites, renal tubular acidosis, renal failure, hypomagnesemia, hypokalemia, bone marrow suppression with reversible decline in hematocrit, hypotension, hypertension, wheezing, and hypoxemia. Treatment of susceptible bacterial infections attributable to streptococci, pneumococci, enterococci, nonpenicillinase-producing staphylococci, Listeria, meningococci; some strains of Haemophilus influenzae, Proteus mirabilis, Salmonella, Shigella, Escherichia coli, Enterobacter, and Klebsiella; used in combination with an aminoglycoside or cefotaxime in neonates for prevention and remedy of infections due to of} group B streptococci, Listeria, and E. Arginine stimulates pituitary launch of progress hormone and prolactin and the pancreatic launch of glucagon and insulin. Used preoperatively to inhibit salivation and cut back extreme secretions of the respiratory tract. In low doses, it could trigger paradoxic bradycardia secondary to its central actions. Azithromycin is drug of alternative for age <1 month because of idiopathic hypertrophic pyloric stenosis with erythromycin. Children 6 months: �Respiratory tract infections: 10 mg/kg on day 1 (maximum dose 500 mg) adopted by 5 mg/kg/day (maximum dose 250 mg) quickly as} day by day on days 2�5. Surfactant lowers floor rigidity on alveolar surfaces during respiration and stabilizes the alveoli against collapse. Ventilate the infant after every one-quarter dose for minimal of|no much less than} 30 seconds or until steady. Four doses of 4 mL/kg can be given within the first forty eight hours of life, no more incessantly than every 6 hours. Pulmonary hemorrhage has been reported, particularly in very low birthweight infants. Renal blood flow increases substantially outcome of|because of|on account of} renovascular dilation and increases prostaglandin secretion. Although sufferers may respond a special way|in another way}, bumetanide is ~40 instances stronger on a milligram-per-milligram basis than furosemide. Caffeine exerts a constructive inotropic effect on the myocardium, increases renal blood flow and glomerular filtration fee, and stimulates glycogenolysis and lipolysis. The serum half-life in neonates ranges from 40 to 230 hours and reduces with increased postnatal age; in infants >9 months half-life is ~5 hours. Chloride salt is preferred to the gluconate type in cardiac arrest outcome of|as a outcome of} it could be more bioavailable. Warning: Multiple salt forms of calcium exist; when ordering and administering calcium, incorrect choice or substitution of 1 salt for one more without correct dosage adjustment may lead to critical over- or under-dosing. There is a 3-fold difference within the main cation focus between calcium chloride (1 gram = 13. Continuous infusion is more efficacious than intermittent infusion due to of} much less renal calcium loss. Calfactant decreases the floor rigidity on alveolar surfaces, stabilizing the alveoli and stopping collapse. After the instillation of every aliquot, position infant both on the best or left side. The 2 aliquots should be separated by a pause to evaluate respiratory standing and reposition the affected person. Patients should be intently monitored and appropriate changes in ventilatory help should be made as clinically indicated. Reduce the dose with renal impairment and in sodium- and water-depleted sufferers (use with caution if on concurrent diuretic therapy). Treatment of partial (especially advanced partial), main generalized tonic-clonic seizures and combined partial or generalized seizures. Erythromycin, isoniazid, and cimetidine may inhibit hepatic metabolism of carbamazepine, leading to increased carbamazepine serum concentrations. Carbamazepine may induce metabolism of warfarin, phenytoin, theophylline, benzodiazepines, and corticosteroids. Metabolized by the liver, not cytochrome P450 enzymes; ends in fewer drug-drug interactions than the azole class of antifungal agents. Serum concentrations of caspofungin may be be} lower if concomitant therapy with dexamethasone, phenytoin, carbamazepine, nevirapine, and rifampin. Activity against susceptible gram-positive cocci (except enterococci), including penicillinaseproducing staphylococci; some gram-negative coverage of susceptible Escherichia coli, Klebsiella, and Proteus. Primarily used in neonates for urinary tract infections, perioperative prophylaxis, and gentle tissue infections.
Maxalt 10mg
Consider session with an ostomy nurse specialist or a dermatologist for persistent signs of dermatitis. A pediatric surgeon ought to be notified about excessive bleeding or blood coming from lumen of the stoma. An impairment of drainage as a result of} narrowing or contraction of stoma tissue at the pores and skin or subcutaneous fascial degree; may require revision. If ischemia or obstruction is suspected, then surgical intervention will be required. This may end up} from tube displacement, improper balloon inflation, inadequate tube stabilization, or increased belly pressure. Topical therapies include antifungal powder or ointment, zinc oxide, and pores and skin barrier wafer. Cover site with dry gauze or foam dressing under stabilizer to pull drainage off pores and skin till irritation resolves. Risk components include pores and skin breakdown, immunosuppressed patient, persistent corticosteroids, and excessive handling/manipulation of tube. A proliferation of capillaries that current as red, uncooked, beefy, painful or bleeding tissue protruding from stoma. Possible causes include moisture, an infection, tube not stabilized, and use of hydrogen peroxide. May be brought on by inadequate tube flushing, kink in tube, formula, or medication precipitation in tube. Medical and nursing care in post-operative interval to the newborn with surgical issues and intestinal ostomy. To get hold of peritoneal fluid for diagnostic checks to decide trigger of|the purpose for} ascites. Due to perforation of the ureter, intrarenal collecting system, or bladder (intraperitoneal) often brought on by a distal obstruction. Other causes: ureterocele, ureteral stenosis, urethral stenosis/atresia, neurogenic bladder, urogenital sinus, congenital nephrotic syndrome, bladder neck obstruction, and renal vein thrombosis. Due to perforation of bile duct (more common), injury to the bile ducts, or a choledochal cyst. Other causes include a congenital lymphatic abnormality (more common), or disruption of the lymphatic ducts from trauma or surgical procedure. Can be brought on by neonatal hepatitis, viral hepatitis, congenital hepatic fibrosis, Budd-Chiari syndrome, or hepatic/portal vein thrombosis. Peritonitis in neonates is mostly associated with gastrointestinal tract perforations. Glycogen storage problems, lysosomal storage problems, and galactosemia can all cause ascites. Uncommon but can be nontraumatic (hepatoblastoma) or secondary to start trauma (hepatic, splenic, or adrenal) or secondary to a ruptured internal organ. As a therapeutic procedure, similar to elimination of peritoneal fluid from huge ascites or air from a pneumoperitoneum to help in air flow in a patient with cardiorespiratory compromise. Sterile drapes, sterile gloves, topical disinfectant similar to povidone-iodine resolution, sterile gauze pads, tuberculin syringe, 1% lidocaine, sterile tubes for fluid, a 10- to 20-mL syringe on a 3-way stopcock, safety engineered 22- or 24-gauge catheterover-needle assembly (24 gauge for <2000 g, 22�24 gauge for >2000 g). Paracentesis can be carried out with thrombocytopenia or coagulopathy if corrected before the procedure. Ascites is often identified by clinical examination and ultrasound (prenatal or postnatal). Ascites is often apparent by clinical examination (abdominal distention, increasing belly girth, increased weight gain, bulging flanks dullness to percussion, and dilated superficial veins). Ascites apparent by clinical examination often indicates a fluid quantity of 200 cc or larger. Ascites not apparent by bodily examination often means that the quantity of ascitic fluid is under 100 cc. To restrict all actions of the legs, a diaper can be wrapped around the legs and secured in place. A good rule is to draw a line from the umbilicus to the anterior superior iliac backbone, and plan to use the world two-thirds of finest way|the way in which} from the umbilicus to the anterior superior iliac backbone (Figure 37�1). Prepare the world with povidone-iodine in a circular fashion, beginning at the puncture site. Use other nonpharmacologic ache prevention similar to oral sucrose, breast milk, and others. A "Z-track" approach is often used to reduce persistent leakage of fluid after the faucet. Aspirate the contents slowly with the syringe and stopcock connected to the catheter. It may be be} essential to reposition the catheter to get hold of an enough quantity of fluid. Once the required quantity of fluid is taken (usually 5�10 mL for specific checks and minimal of|no much less than} 10�15 mL, enough to help ventilation), remove the catheter. Hypotension can be brought on by eradicating fluid or eradicating fluid too rapidly. To reduce this risk, take only the amount needed for research or what is needed to enhance air flow and at all times remove fluid slowly. If perforation happens, broadspectrum antibiotics may be be} indicated with shut observation for signs of an infection. Perforation of the bladder is generally self-limited and requires no specific therapy. Applying pressure over the positioning for a few minutes, or applying a pressure dressing and monitoring the positioning can be carried out. Observation is often required (see Figure 11�22 for radiograph of a pneumoperitoneum). Bleeding from the liver or intra-abdominal vessels, if severe, may require emergency surgical procedure session. Occurs in males for extravasation of ascitic fluid between physique wall layers and is often self-limiting. Emergency evacuation of air or fluid in the therapy of cardiac tamponade (inability of the heart to broaden with decreased stroke quantity and cardiac output) brought on by pericardial effusion (accumulation of excess fluid) or pneumopericardium (accumulation of air) in the pericardial area. Etiology is unclear but proposed causes include a direct puncture of a vessel or myocardium by the tip of the catheter throughout insertion or delayed perforation secondary to erosion of the cardiac or vascular wall. It is more widespread with lines in the proper atrium, and the median time to prevalence is three days after a central venous catheter insertion. A chest radiograph most likely not|will not be} diagnostic; an echocardiogram is but may delay therapy. Rare but may be very dangerous and often happens with other air leak syndromes, with severe lung pathology, with a historical past of vigorous resuscitation, and/or a historical past of assisted air flow. To get hold of pericardial fluid for diagnostic research in infants with a pericardial effusion. Pericardial effusion is rare in neonates and mostly happens in a hydropic or septic infant. Other causes include thyroid dysfunction, cardiac and pericardial tumors, congenital anomalies (diaphragmatic hernia/eventration, ruptured ventricular diverticulum), infections, surgically related (postoperative), autoimmune, idiopathic, and other causes. Povidone-iodine resolution, sterile gloves, gown, sterile drapes, a safetyengineered 22- or 24-gauge 1-inch catheter-over-needle assembly, extension tubing, 10-mL syringe, 3-way stopcock, lidocaine, and underwater seal if the catheter is to be left indwelling, transillumination system for pneumopericardium, transthoracic echocardiogram/ultrasound system. Note: If a central venous catheter is in place and a pericardial effusion is suspected, cease infusion of fluids into the catheter instantly. Ideally, pericardiocentesis is performed with the help of echocardiography/ ultrasound. Besides diagnosing the pericardial effusion, it helps guide needle insertion to scale back issues. In sure circumstances, a fast betadine prep, followed by a "blind" needle insertion with aspiration, is critical. It may also assist to decide the positioning and angle of entry and allow an estimation of the distance the needle should go in. Thoracic transillumination can be carried out to assist diagnose and likewise to assist monitor the air evacuation while the procedure is finished (see Chapter 40). Put on the sterile gloves and gown and drape the world, leaving the xiphoid and a 2-cm circular space round it exposed.
Generic 10 mg maxalt
Other long-term complications, together with blindness, hearing loss, and cognitive issues requiring special assist at school, can also occur. Despite these acknowledged complications, most infants have excellent morbidity-free outcomes. [newline]Bladder catheter, enteral feeding tube or tube for low intermittent suction, and a rectal temperature probe should be inserted as needed. Consumption of platelets by the hole fiber or membrane oxygenator or filter used for steady renal substitute can exacerbate the coagulopathy and the additive responses can result in|may end up in|can lead to} large capillary leak. This process additionally be} mitigated somewhat by pretreating neonates with a glucocorticoid, but the evidence for this has not been established. Gas exchange through the oxygenator mimics pulmonary respiration (see Figure 18�1). The Fio2 delivered to the oxygenator influences the oxygen delivered to the blood. Membrane oxygenators are designed to allow blood to move on one facet of the membrane, whereas fuel flows on the opposite facet. Membrane oxygenators extra likely to|usually have a tendency to} have complications with plasma leaks, air emboli, water vapor condensation, and thrombus formation. To provide various oxygen concentrations for each kinds of oxygenators, the fuel blender is used to dial in an applicable O2 focus. If the blood flows sooner than the time it takes to obtain full saturation of the hemoglobin with oxygen, blood will go away the oxygenator incompletely saturated. The "rated move" is the pump blood move rate at which maximal O2 delivery is achieved. The motion of fuel through the oxygenator or sweep fuel flow-rate (which continually refreshes the focus gradient by transferring air through the oxygenator). Provides cardiopulmonary bypass that runs in parallel to the native cardiac output. May provide full cardiac and respiratory assist for the nonfunctioning coronary heart and lungs. Results in ligation of the carotid artery; reconstruction might or may not be not|will not be} attainable. Potentially might allow emboli to enter the arterial circulation, which might trigger a stroke. May compromise organ tolerance to hypoxia (especially in the brain and kidneys) due to the dearth of pulsatility in the blood move. Provides respiratory assist (and not directly circulatory support) that runs in sequence with the native cardiac output. Allows the lungs to function filters for emboli so embolic strokes are less likely iv. Increases the availability of oxygen to the coronary circulation as blood is ejected from the left ventricle because of of} the arterial admixture of the blended venous blood b. In this case, some native lung function additionally be} necessary to sustain applicable fuel exchange. Some institutional preferences might include albumin or tris-hydroxymethyl amino-methane. Patients should be positioned with the top turned to the left and the neck extended utilizing a neck roll. To provide analgesia/anesthesia and surgical preparedness, patients ought to receive a narcotic and neuromuscular blocking agent before the process. An x-ray cassette should be placed underneath the patient before initiation of surgical placement of the cannula(e). The typical beginning dose is 10�20 U/kg/h, and the everyday steady-state infusion rate is 20�40 U/kg/h. If ongoing bleeding and coagulopathy are a concern or the patient has just lately had surgery, the heparin drip additionally be} held until an applicable coagulation status is achieved. The dimension of the venous cannula is crucial outcome of|as a outcome of} restricted move because of of} high resistance might trigger bloodshearing leading to hemolysis. The arterial cannula tip should be in the brachiocephalic artery, at or simply above the junction of the aortic arch. Optimal positioning is achieved when the cannula tip is at T3�4 (just above the carina) after the neck roll is eliminated. The tip of the venous cannula should be in the proper atrium close to the junction of the inferior vena cava. If the arterial cannula is positioned high in the proper common carotid artery, streaming of blood can occur into the proper subclavian artery, causing the proper arm to appear more oxygenated than relaxation of|the remainder of} the physique, invalidating any arterial blood fuel sampling from a right radial artery. The cannula chosen ought to have the biggest inside diameter to decrease resistance to blood move. The cannula tip should be well into the proper atrium at T7�8 or about 1�2 cm above the diaphragm for most cannulae. Flows of one hundred twenty mL/kg/min should be achievable after intravascular volume expansion and removal of the neck roll. In this example, venous saturations additionally be} >85�90% and arterial saturations decrease than their baseline ranges. During these occasions, blood pressures might drift downward momentarily, and intravascular volume additionally be} needed. Diuresis will increase heparin clearance, often necessitating an increase in the heparin infusion rate. Normally stored >60�100%, especially with extreme clot buildup in the circuit and/or a high heparin infusion rate (eg, >40 U/kg/h). Assays complete blood to provide details about intrinsic factor, platelet function, anticoagulation, and fibrinolytic function. Suspected when an increase in the preoxygenator stress and a fall in the postoxygenator stress occurs (see Figure 18�1). If the stress is rising to above acceptable parameters, the oxygenator or circuit should be modified. SvO2 ranges <50% point out a crucial degree of O2 extraction and suggest that the rate of tissue metabolism dangerously exceeds the rate of O2 delivery. Once this happens, cells use the markedly less efficient anaerobic metabolism producing lactic acid. Some facilities use high-frequency oscillatory air flow for lung rest, often with a mean airway stress of 10�14 cm H2O and low amplitudes. This system permits for removal of excess fluid and stabilizes electrolyte abnormalities. Additional volume to improve right coronary heart filling, inotropic agents to improve left coronary heart ejection, maximizing postmembrane oxygen content material and complete oxygen delivery, and reducing afterload with vasodilators might allow for restoration of the shocked ventricle. Cardiac stun failing to improve inside 4�5 days represents an ominous signal and suggests myocarditis or myocardial infarction. Decompression additionally be} essential by balloon septostomy with or stent in place. During circuit changes, a big proportion of blood volume is exchanged, and there could be electrolyte imbalances and arrhythmias. As more blood is routed through the circuit with a high move rate, the systemic arterial pulse contour might turn into dampened after which flatten if complete bypass is achieved. In this example, more blood drains into the circuit, lowering each right and left coronary heart preload and leading to a lower in the left ventricular stroke volume. Despite the dearth of pulsatility, the mean blood stress stays pretty fixed and is the most effective gauge of blood stress dynamics. This blood shall be exposed to variable air flow, relying on lung function and standing of the disease process. With enchancment in native lung function and cardiac output, the oxygen content material of the blood returning shall be higher. A major strategy to improve oxygen delivery consists of maintaining the next hemoglobin degree. A failing oxygenator (because of lowered functional floor area) might lower oxygen delivery as well. Heparin might proceed to run through the circuit or be break up so that one-half is transfused to the patient and one-half to the circuit. The surgical team should be notified of the estimated time of attainable decannulation. The pump move could be weaned hourly by 10�20 mL/min whereas progressively rising ventilatory assist. Once that is completed, the cannulae are clamped and the bridge clamp is eliminated. To maintain integrity of the cannulae and circuit whereas trialing off, the cannulae are flushed every 5 minutes by opening the venous cannula, clamping the bridge or shunt, then opening the arterial cannula for 5�10 seconds, adopted by reversing the sequence.
References:
- https://iai.asm.org/content/25/1/352.full.pdf
- https://www.health.ny.gov/press/reports/docs/2015_sepsis_care_improvement_initiative.pdf
- http://www.esmo.org/content/download/6609/115065/file/en-oesophageal-cancer-guide-for-patients.pdf
- https://www.gillettechildrens.org/assets/uploads/general/Newsletter_PDFs/Vol18No2.pdf
- http://www.sciencewebpublishing.net/ijbfs/archive/2015/April/pdf/Adeyinka%20and%20Richard.pdf