.png)
Generic 10 mg accupril
This is accomplished by measuring arch perimeter from the mesial of one first molar to the other, over the contact factors of posterior teeth and incisal fringe of anteriors. There are two basic ways to accomplish this manually: (1) by dividing the dental arch into segments that may be measured as straight line approximations of the arch (Figure eleven-forty nine) or (2) by contouring a chunk of wire (or a curved line on the pc screen) to the road of occlusion after which straightening it out for measurement. B, Space required is the sum of the mesiodistal widths of all individual erupted everlasting teeth plus the estimated sizes of the unerupted everlasting teeth. The second step is to calculate the quantity of area required for alignment of the teeth. This is finished by measuring the mesiodistal width of every erupted tooth from contact level to contact level, estimating the dimensions of unerupted everlasting teeth, after which summing the widths of the individual teeth (see Figure eleven-forty nine, B). If out there area is larger than the area required (excess area), gaps between some teeth can be anticipated. Space analysis carried out on this way is predicated on three essential assumptions: (1) the anteroposterior place of the incisors is correct. With regard to the first assumption, it have to be remembered that incisor protrusion is relatively common and that retrusion, although uncommon, does happen. For this purpose, information about how much the incisors protrude have to be out there from medical examination to consider the outcomes of area analysis. This information comes from facial form analysis (or from cephalometric analysis if out there). Even in youngsters with properly-proportioned faces, the place of the everlasting molars changes when primary molars are changed by the premolars (see Chapter 3 for a detailed evaluate). The third assumption can (and should) be checked by medical and radiographic examination, wanting on the teeth as a set somewhat than as individual items. Anomalies in tooth measurement have important implications for area in the dental arches (see Figure 5-23). Estimating the Size of Unerupted Permanent Teeth There are two basic approaches to doing this: 1. Measurement of the Teeth on Radiographs this requires an undistorted radiographic image, which is achieved with individual periapical radiographs. This could be accomplished by measuring an object that may be seen both in the radiograph and on the casts, often a primary molar tooth. Accuracy is truthful to good, depending on the standard of the radiographs and their place in the arch. The method can be used in maxillary and mandibular arches for all ethnic teams, but the radiation burden is justified only in uncommon instances. Estimation from Proportionality Tables There is a fairly good correlation between the dimensions of the erupted everlasting incisors and the unerupted canines and premolars. The measurement of the lower incisors correlates better with the dimensions of the upper canines and premolars than does the dimensions of the upper incisors as a result of upper lateral incisors are extraordinarily variable teeth. Box eleven-1 Tanaka and Johnston Prediction Values One half of the mesiodistal width of the +10. It requires neither radiographs nor reference tables (once the straightforward equation is memorized), which makes it very convenient, however specifically it tends to overestimate the required area for Caucasian females in both arches and underestimate the area required in the lower arch for African-American males. Most computer algorithms for area analysis are primarily based on correlations of tooth sizes, and should be used with warning if the radiographs present something uncommon (except the pc program permits for introduction of radiographic information). Summary Which of those strategies is best for a person patient is determined by the circumstances. The prediction tables work surprisingly properly when utilized to the population group from which they were developed, white school youngsters of northern European descent. On steadiness, the Tanaka-Johnston methodology in all probability is most sensible for manual calculation as a result of no radiographs are required and the straightforward ratio could be printed proper on the area analysis form or memorized, in order that no reference tables have to be consulted. Note that (1) a correction for mesial motion of the lower molars following the exchange of the dentition is included, (2) the Tanaka-Johnston methodology for predicting the dimensions of unerupted canines and premolars is used, and (3) the result from facial form analysis is requested to verify for appropriateness of the analysis and for interpretation of the outcomes. Computer analysis is quicker and easier, however it is important to do not forget that its accuracy will rely upon the accuracy of the digitized input and how properly the patient meets the assumptions that underlie a correlation method. Other area issues, more complex nonetheless, often can be addressed in a specialty apply and are discussed in Chapter 12. Space maintenance is acceptable only when adequate area is out there, and when all unerupted teeth are present and on the regular stage of growth. Several treatment methods can be used successfully for area maintenance, depending on the specific state of affairs. Because these home equipment are in danger for breakage and loss, they have to be monitored rigorously to achieve success. Band-and-Loop Space Maintainers the band and loop is a unilateral mounted appliance indicated for area maintenance in the posterior segments. Although bonding a rigid or flexible wire across the edentulous area has been advocated in its place, this has not proved satisfactory clinically. It also is not thought of advisable to solder the loop portion to a chrome steel crown as a result of this precludes easy appliance removal and alternative. The knowledge for the arch dimensions and tooth widths could be entered by digitizing the already present digital casts. It consists of a band on both a primary or everlasting molar and a wire loop to keep area. A, the loop portion created from 36 mil wire is rigorously contoured to the abutment tooth without proscribing lateral motion of the primary canine and (B) the loop can be contoured to within 1. The solder joints should fill the angle between the band and wire to keep away from meals and particles accumulation. C, A accomplished band-and-loop maintainer in place after extraction of a primary first molar. D, An occlusal relaxation, proven right here on the primary first molar, could be added to the loop portion to stop the banded teeth from tipping mesially. If a primary second molar has been lost, the band could be placed on both the primary first molar or the erupted everlasting first molar. Some clinicians favor to band the primary tooth on this state of affairs because of the danger of decalcification round any band, however primary first molars are challenging to band because of their morphology, which converges occlusally and makes band retention troublesome. A more essential consideration is the eruption sequence of the succedaneous teeth. Before eruption of the everlasting incisors, if a single primary molar has been lost bilaterally, a pair of band-and-loop area maintainers is really helpful instead of the lingual arch that might be used if the patient were older. This is advisable as a result of the everlasting incisor tooth buds are lingual to the primary incisors and sometimes erupt lingually. The bilateral band and loops allow the everlasting incisors to erupt without interference from a lingual wire. At a later time, the two band-and-loop home equipment could be changed with a single lingual arch if needed. It has been judged to be approximately 18 months with cement failure cited as probably the most frequent downside. In these instances, because of the size of the edentulous area, band-and-loop area maintainers are contraindicated, and the doubtless lingual place of the everlasting incisors at initial eruption makes the lingual arch a poor selection. Another indication for this appliance is posterior area maintenance along side alternative of missing primary or delayed everlasting incisors (Figure eleven-53). Distal Shoe Space Maintainers the distal shoe has a singular software and is the appliance of selection when a primary second molar is lost before eruption of the everlasting first molar. At the identical time, it could possibly keep the area of one or more prematurely lost primary molars. Both the clasps and the acrylic need frequent adjustment to stop interference with physiologic adjustment of primary teeth during eruption of everlasting teeth. The C-clasps on the primary canines present limited retention and are good examples of clasps that need continued careful consideration. The information plane is hooked up to a hard and fast or detachable retaining system (Figure eleven-54). When mounted, the distal shoe is often retained with a band instead of a chrome steel crown in order that it can be changed by another type of area maintainer after the everlasting first molar erupts. Unfortunately, this design limits the strength of the appliance and provides no practical alternative for the missing tooth. If primary first and second molars are missing, the appliance have to be detachable and the information plane is incorporated right into a partial denture because of the size of the edentulous span.
Generic accupril 10mg
Much of the periosteal space could be palpated, for example, the anterior partitions of the sinuses, and the palate, and there will be evidence of swelling or tenderness on strain. Temporomandibular joint strain is widespread, and is due to the patient growing an abnormal biting sample, incessantly secondary to orthodontic problems, or because of unwell-becoming or absent dentures. The ache is centralised within the temporal region, however may unfold to the ear, and alongside the pores and skin over the mandible. The temporomandibular joints are tender when the mouth is opened and closed, and a few sideways deviation of the jaw on full opening is apparent. If the patient is seen during an acute episode, slight spasm of the masticatory muscular tissues will be apparent. Radiography demonstrates that it is a useful abnormality, as signs of joint degeneration are absent, however there could be limitation of opening of the joint on one side. Infective pains have a vascular part, for example, the ache of acute sinusitis and a tooth Facial Neuralgia (Pain within the Face) pulp an infection are throbbing in character. In the absence of signs of an infection, one should consider migraine, migrainous neuralgia and temporal arteritis. Migrainous neuralgia is sufficiently totally different from migraine to be recognized as a separate medical entity. The patient is often male, aged between 25 and forty, and the assaults of ache, which final for a short interval various from a couple of minutes to an hour or two, are excruciating in degree, unilateral in distribution, centered around or deep to the attention, and accompanied by ipsilateral nasal obstruction with rhinorrhoea. Attacks can happen at least once in 24 hours, and usually waken the patient about 3 am. A group of very related assaults can happen over a number of weeks or months, and disappear, solely to return in a similar fashion, maybe years later. Temporal arteritis at all times occurs after the age of fifty five and gives rise to acute throbbing vascular-type ache within the temporal region. It is part of a large-cell arteritis affecting lots of the vessels of the pinnacle and neck, and is accompanied by lassitude and slight fever. The temporal arteries are tender to touch and feel thickened, and the overlying pores and skin could be red. Neuralgic ache is sharp and burning in character, and is interspersed with durations which are either free from ache or with a background ache. It occurs in disease affecting the nerves, when there will be evidence of altered sensation either to gentle touch or to a sharp pin prick. Neuralgic ache arising within the absence of evidence of neurological disease occurs in postherpetic neuralgia, when there will be a historical past of earlier shingles, and in trigeminal neuralgia. The trigeminal sensory dermatome at all times encloses the painful parts, and the ophthalmic space is least often affected. The ache is incessantly stimulated by touching a specific part of the face-the trigger space-and initially consists of a sequence of quick sharp spasms of ache, each lasting a couple of minutes, however it can progress to a interval of ache lasting a number of hours. The ache is severe, and if the patient is seen during an acute attack, spasm of the muscular tissues of the ipsilateral side of the face will be famous. Treatment is with carbamazepine (Tegretol) beginning with a dose of one hundred mg twice a day, and growing the dose until relief is obtained. The pure historical past of this condition could be very variable, and the signs can disappear for an extended time frame, solely to recur. Surgical treatment with radio-frequency rhizotomy may be required in patients uncontrolled by medical remedy. These patients have often consulted many specialists and have had innumerable unsuccessful trials of medical or surgical treatment. They are sometimes depressed, however this may be as a lot a function of their unremitting ailment as of psychological imbalance. Treatment is unsatisfactory, a combination of psychotropic medicine and psychotherapy giving the greatest likelihood of success. It is a fibromuscular structure consisting of the next layers from without inwards: 1. The pharynx is split into three parts: (i) nasopharynx, (ii) oropharynx, and (iii) laryngopharynx. Nasopharynx the part of pharynx which lies above the soft palate and behind the nasal cavity known as the nasopharynx. Nasopharyngeal Tonsil It is a set of lymphoid tissue under the mucosa of the nasopharynx located at the junction of the roof and posterior wall of the nasopharynx. Paratonsillar vein emerges on the lateral floor and pierces the superior constrictor muscle to finish within the widespread facial vein and pharyngeal plexus of veins. Lymphatic drainage the efferent lymphatics emerge from the lateral side and finish within the jugulodigastric group of deep cervical nodes. The inner ring consists primarily of the nasopharyngeal tonsil, peri-tubal lymphoid tissues, faucial tonsil and lingual tonsil. The efferents from this ring drain to lymph nodes located across the neck forming the outer ring. Laryngopharynx (Hypopharynx) this part of the pharynx lies behind the larynx and partly surrounds the larynx. Superiorly, it communicates with the oropharynx and begins at the level of the hyoid bone. Inferiorly it extends up to the upper finish of the oesophagus at the decrease border of the cricoid cartilage. It is split into three parts: this is that part of the pharynx which extends from the extent of the soft palate to the extent of laryngeal inlet, under an imaginary horizontal line drawn at the level of the hyoid bone. Anteriorly the oropharynx opens within the buccal cavity at the oropharyngeal isthmus formed by the faucial pillars. Tonsils Tonsils are organised lymphoid structures located between the faucial pillars. The tonsillar fossa is formed by the palatoglossal and palatopharyngeal folds and posterior part of the side of the tongue. A fold of mucous membrane, plica semilunaris connects the palatoglossal and palatopharyngeal folds superiorly. The plica triangularis is another fold of mucous membrane which connects the palatoglossal and palatopharyngeal folds at the decrease pole of the tonsil. An intratonsillar cleft is seen at the upper part of the tonsil and is a remnant of the second pharyngeal pouch. The lateral floor of the tonsil is covered by a fibrous capsule attached loosely to the tonsillar bed. Tonsillar bed It is formed by loose areolar tissue, pharyngobasilar fascia, superior constrictor muscle and buccopharyngeal fascia. Blood provide of tonsil Tonsillar branch of the facial artery is the main artery of provide. It is bounded medially by the aryepiglottic fold, laterally by the thyrohyoid membrane within the upper half and medial floor of the thyroid cartilage within the decrease half. Superiorly the fossa is separated from the vallecula by the pharyngoepiglottic fold. Postcricoid Region the postcricoid region is the decrease part of the laryngopharynx and is formed by mucosa extending from the upper to decrease border of the cricoid cartilage. Posterior Pharyngeal Wall this part of the hypopharynx extends from the extent of the hyoid bone down up to the upper finish of the oesophagus. The round layer is formed by the superior, center and inferior constrictors which kind the side and posterior wall of the pharynx. The longitudinal muscle layer is formed by the palatopharyngeus and stylopharyngeus muscular tissues. While the longitudinal muscular tissues elevate the pharynx, the round group assist in propelling the bolus downwards. Nerve Supply Pharynx is supplied via pharyngeal plexus which lies primarily on the middle constrictor muscle. This is formed by the pharyngeal branches of the vagus and glossopharyngeal nerves and sympathetic fibres across the vessels. The glossopharyngeal is the main sensory nerve however supplies motor fibres to stylopharyngeus. Other muscular tissues which participate in its formation are levator palati, palatoglossus, palatopharyngeus and musculus uvulae. Nerve Supply All the muscular tissues of the soft palate except tensor palati are supplied by the cranial root of the accent via the vagus. The soft palate performs an essential position in closure of the nasopharyngeal isthmus and, subsequently, helps in deglutition and speech. The posterior free border of the soft palate comes in contact with this ridge to shut the nasopharynx during deglutition.
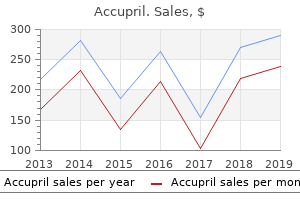
| Comparative prices of Accupril | ||
| # | Retailer | Average price |
| 1 | BJ'S Wholesale Club | 645 |
| 2 | J.C. Penney | 930 |
| 3 | IKEA North America | 385 |
| 4 | Price Chopper Supermkts | 267 |
| 5 | Burger King Holdings | 671 |
Cheap 10 mg accupril
Some children with cerebral palsy find this comforting as a result of it helps them management their actions, however caution have to be used to not forcefully extend contracted limbs. Chil dren with autism have been reported to find more comfort and cooperation in the security and weight of an immobili tive stabilization have to be carefully considered, and oldsters should have all the required info to give informed consent. The writer identified that the technique was positively offered in a have only proven videos with no private experience and no rationalization. Children under sedation must be arousable, inter lively, and profit from communicative habits steerage techniques. Studies that take a look at habits following these modalities help them as effective method of defending the creating psyche of patients. McComb and associates67 concluded that treatment with oral sedation had no important effect on future dental habits at a recall examination performed 2 to heat and caring office surroundings, whereas other research erative treatment, ment to prevent untoward actions by the sedated youngster. Other research have discovered more constructive habits in children after treatment under common anesthesia versus conscious sedation. Sl More lately, nevertheless, Eaton and associates48 discovered sedation or common anesthesia to be the third most acceptable technique after inform-show-do and nitrous oxide. Some mother and father might now even request sedation for their youngster earlier than the dentist has had the opportunity to attempt fundamental habits steerage techniques. In these instances the experienced clinician normally attempts at least one go to earlier than advancing to this level of habits administration. As soon as the youngster indicated he was able to cooperate he was allowed to return to the dental chair. In addition to serving to children purchase new behaviors, it could assist extin guish fear habits via the process of "vicarious extinc tion, " the place children observe other children present process experiences that they fear and turn into much less afraid. For example a younger or fearful patient typically watches a cooperative sibling endure a procedure to extinguish fears. The technique is applicable in children of all ages and in these with excessive and moderate fear. One caveat is that chil dren with earlier experience might profit less than a baby who has no earlier experience with dentistry. It is also useful for the kid to vicariously experience rewards, corresponding to seeing the mannequin obtain praise or a reward. Both reside and filmed modeling can be effective in bringing about posi tive habits. There must even be a delegated plan of observation so that treatment can be applied if the condition worsens. Also these gadgets typically occlude half of the mouth and can make the method for an inferior alveolar block difficult. Although unlikely, aspira tion of these mouth props is a chance and they need to be tied with 1 8 inches of floss to safe them. The practitio ner must use caution as a result of fast opening of the mouth prop on anterior teeth can luxate or avulse them. If the mirror or explorer is used in the mouth, then the patient might inadvertently break them or trigger harm to the patient. It is advisable to substitute these mouth props with McKesson rubber props as soon as adequate opening is obtained. Loose primary teeth can be dislodged and possibly swal lowed or aspirated with any kind of mouth prop. It is advis able to check the dentition as a precaution earlier than using any mouth prop. Documenting Behavior and Use of Behavior Management Techniques the habits of the kid patient is a vital part of the go to that have to be documented. A number of scales for habits exist, and a generally used one is the Frankl score as proven in Table 23-3. Words like "overindulged" or «spoiled" are subjective and will offend mother and father on review of the document. The monitoring and recording requirements for nitrous oxide, oral conscious sedation, and common anesthesia should adjust to state laws. If lively immobilization is used, it is very important document who immobilized the patient, what physique half was immobilized, and for what part of the procedure. If passive immobilization is used the type of Mouth props are routinely used in dentistry to improve the comfort of the patient and high quality of dental care. They may help prevent fatigue from the mouth staying open during lengthy visits, and so they prevent unintended patient closing which will trigger trauma or moisture contamination of the area being treated. However, using a mouth prop on an uncooperative youngster has been interpreted as protecting stabilization that requires informed consent. Multiple types of mouth props are used in pediatric den tistry, as proven in Figure 23-four, and so they all have particular indications, advantages, and disadvantages. It is also prudent to doc that an updated verbal consent was obtained along with the written consent obtained earlier than use. The most modern study on this space discovered that inform-show-do was essentially the most acceptable technique, followed (so as of decreas ing acceptance) by: 1. Sheller31 notes that society, mother and father and their children, the insurance coverage indus attempt, regulatory our bodies, legal system, dental workers, and the edu cation, expectations, and choices of dentists all influence the options available for youngster patient administration. The changing economic and social climate has produced several types of families. There is a development for families to reside more and more isolated and disconnected lives in our society. This is because of young families transferring away from prolonged members of the family, an increased incidence of single mother and father, and free time limitations caused by the work schedules of twin-earnings or single father or mother families. General anesthesia Active restraint Oral premedication Voice management Passive restraint Hand-over-mouth this study concluded that, over the last 20 years, aggressive physical administration techniques, specifically hand-over-mouth and passive restraint, have decreased in acceptability, and pharmacologic techniques have increased in acceptability. General anesthesia and sedation were acceptable for less than extractions and restora tions. Physical restraint by the assistant was acceptable in additional situations than restraint by the dentist, which was judged acceptable just for the injection. Voice management, mouth props, constructive reinforcement, and inform-show-do are acceptable for almost all dental procedures. Passive restraint with the papoose board and hand-over-mouth were unac ceptable to the vast majority of mother and father for all dental procedures. It must be noted that on this study, mother and father watched a video of every technique and had no rationalization of the technique. Havelka and coworkersso discovered that top social groups were more settle for ing than low social groups of lively restraint and inform-show do however much less accepting of using a papoose board and common anesthesia. Additionally, few research have examined the influence of ethnicity and acceptance of habits steerage. Scott and Garcia-Godof2 discovered that Hispanic mother and father had favorable attitudes towards verbal techniques, corresponding to inform-show do and voice control, and unfavorable attitudes toward physical management techniques, such as papoose board, hand-over mouth, and active restraint. One study found few differences between parents of dis abled and fully-abled children in their acceptance of man agement techniques. The only exception was that parents of disabled children were more accepting of restraint for a dental checkup and cleaning than parents of fully-abled children. This form is accompanied by a separate treat ment plan that lists the specific techniques that will be employed. Third-party insurers play an increasingly influential role on practice decisions and are skeptical about paying for services that cannot be measured. Medical sociologists have noted a shift towards a consumerist position on health care and parents are overwhelmed with information, sometimes false, on den tistry. Allen and cowork ers76 found that, compared to video or written presentation, the oral method of delivering information to parents about child behavior management techniques was the best method of ensuring that the average parent felt informed and was likely to consent. Informed consent should be obtained by the practitioner, and written documentation of informed consent is superior to oral consent only. Informed consent is a process of understanding that relies on honest communica tion from the practitioner and willingness to understand by the parent. Misrepresentations for behavior guidance tech niques can cause conflict in the parent-dentist relationship and have legal consequences.
Purchase 10mg accupril
Importantly, roughly one third of affected infants have Down syndrome and a further 20% are premature. Duodenal atresia is related to bilious emesis (vomiting of bile) as a result of the blockage happens distal to the opening of the bile duct. Polyhydramnios also happens as a result of duodenal atresia prevents regular intestinal absorption of swallowed amniotic fluid. The prognosis of duodenal atresia is usually recommended by the presence of a "double bubble" sign on plain radiographs or ultrasound scans. This look is brought on by a distended, gasoline-filled abdomen and proximal duodenum. Figure eleven-5 Progressive stages in the development of the duodenum, liver, pancreas, and extrahepatic biliary apparatus. The pancreas develops from dorsal and ventral pancreatic buds that fuse to type the pancreas. Note that the entrance of the bile duct into the duodenum steadily shifts from its initial place to a posterior one. This explains why the bile duct in the adult passes posterior to the duodenum and the head of the pancreas. C to F, Diagrammatic longitudinal and transverse sections of the duodenum displaying (1) regular recanalization (D to D3), (2) stenosis (E to E3), and atresia (F to F3). Most duodenal atresias happen in the descending (second) and horizontal (third) parts of the duodenum. The liver, gallbladder, and biliary duct system come up as a ventral outgrowth-hepatic diverticulum-from the caudal or distal a part of the foregut early in the fourth week. Based on latest analysis findings, it has been advised that each the hepatic diverticulum and the ventral bud of the pancreas develop from two cell populations in the embryonic endoderm. The diverticulum extends into the septum transversum, a mass of splanchnic mesoderm between the creating heart and midgut. A, An oblique scan displaying the dilated, fluid-filled abdomen (St) entering the proximal duodenum (D), which can be enlarged because of the atresia (blockage) distal to it. The larger cranial a part of the hepatic diverticulum is the primordium of the liver. The proliferating endodermal cells give rise to interlacing cords of hepatocytes and to the epithelial lining of the intrahepatic a part of the biliary apparatus. The hepatic cords anastomose round endothelium-lined spaces, the primordia of the hepatic sinusoids. The fibrous and hematopoietic tissue and Kupffer cells of the liver are derived from mesenchyme in the septum transversum. The liver grows rapidly and, from the fifth to 10th weeks, fills a big a part of the upper abdominal cavity (see. The quantity of oxygenated blood flowing from the umbilical vein into the liver determines the development and functional segmentation of the liver. Initially, the proper and left lobes are roughly the same size, however the proper lobe soon becomes larger. Hematopoiesis begins during the sixth week, giving the liver a bright reddish look. By the ninth week, the liver accounts for about 10% of the entire weight of the fetus. Integration hyperlink: Fetal liver - histology the small caudal a part of the hepatic diverticulum becomes the gallbladder, and the stalk of the diverticulum types the cystic duct (see. The stalk connecting the hepatic and cystic ducts to the duodenum becomes the bile duct. Initially, this duct attaches to the ventral aspect of the duodenal loop; nonetheless, as the duodenum grows and rotates, the entrance of the bile duct is carried to the dorsal aspect of the duodenum (see. The bile entering the duodenum through the bile duct after the 13th week offers the meconium (intestinal contents) a dark green shade. The ventral mesentery, derived from the mesogastrum, also types the visceral peritoneum of the liver. Anomalies of the Liver Minor variations of liver lobulation are common, however congenital anomalies of the liver are uncommon. Variations of the hepatic ducts, bile duct, and cystic duct are common and clinically important. Accessory hepatic ducts could also be present, and awareness of their attainable presence is of surgical importance (Moore and Dalley, 2006). These accent ducts are slim channels running from the proper lobe of the liver into the anterior floor of the body of the gallbladder. In some circumstances, the cystic duct opens into an accessory hepatic duct quite than into the common hepatic duct. Extrahepatic Biliary Atresia page 220 page 221 this is essentially the most critical anomaly of the extrahepatic biliary system and happens in one in 10, 000 to 15, 000 reside births. The most typical type of extrahepatic biliary atresia (present in eighty five% of circumstances) is obliteration of the bile ducts at or superior to the porta hepatis-a deep transverse fissure on the visceral floor of the liver. Biliary atresia could end result from a failure of the reworking process at the hepatic hilum or from infections or immunologic reactions throughout late fetal development. B, Transverse section of the embryo displaying enlargement of the peritoneal cavity (arrows). D, Transverse section of the embryo after formation of the dorsal and ventral mesenteries. Note that the liver is joined to the ventral abdominal wall and to the abdomen and the duodenum by the falciform ligament and lesser omentum, respectively. Development of the Pancreas the pancreas develops between the layers of the mesentery from dorsal and ventral pancreatic buds of endodermal cells, which come up from the caudal or dorsal a part of the foregut. The larger dorsal pancreatic bud seems first and develops a slight distance cranial to the ventral bud. The ventral pancreatic bud develops close to the entry of the bile duct into the duodenum and grows between the layers of the ventral mesentery. As the duodenum rotates to the proper and becomes C formed, the ventral pancreatic bud is carried dorsally with the bile duct (see. The arrow signifies the communication of the peritoneal cavity with the extraembryonic coelom. Because of the speedy development of the liver and the midgut loop, the abdominal cavity temporarily becomes too small to include the creating intestines; consequently, they enter the extraembryonic coelom in the proximal a part of the umbilical twine (see. The ventral pancreatic bud types the uncinate process and a part of the head of the pancreas. As the abdomen, duodenum, and ventral mesentery rotate, the pancreas involves lie alongside the dorsal abdominal wall. The pancreatic duct types from the duct of the ventral bud and the distal a part of the duct of the dorsal bud (see. The proximal a part of the duct of the dorsal bud often persists as an accessory pancreatic duct that opens into the minor duodenal papilla, situated roughly 2 cm cranial to the main duct. In roughly 9% of people, the pancreatic ducts fail to fuse, resulting in two ducts. Integration hyperlink: Pancreas - anatomy Molecular research present that the ventral pancreas develops from a bipotential cell inhabitants in the ventral a part of the endoderm. Histogenesis of the Pancreas the parenchyma of the pancreas is derived from the endoderm of the pancreatic buds, which types a community of tubules. Early in the fetal period, pancreatic acini start to develop from cell clusters around the ends of these tubules (primordial pancreatic ducts). The pancreatic islets develop from groups of cells that separate from the tubules and are available to lie between the acini. The glucagon- and somatostatin-containing cells develop earlier than differentiation of the insulin-secreting cells. The connective tissue sheath and interlobular septa of the pancreas develop from the encompassing splanchnic mesenchyme. As a end result, these cells bear hypertrophy to improve the speed of insulin secretion.
Trusted accupril 10mg
C, After delivery, showing the left recurrent nerve hooked around the ligamentum arteriosum and the arch of the aorta. B, Diagrammatic illustration of the common routes of collateral circulation that develop in association with postductal coarctation of the aorta. E, Sketch of the pharyngeal arch arterial sample in a 7-week embryo showing the areas that usually involute. Note that the distal phase of the best dorsal aorta usually involutes as the best subclavian artery develops. G, Later stage showing the abnormally involuted phase showing as a coarctation of the aorta. This moves to the region of the ductus arteriosus with the left subclavian artery. These drawings (E to G) illustrate one speculation in regards to the embryologic foundation of coarctation of the aorta. B, A large right arch of the aorta and a small left arch of the aorta come up from the ascending aorta and kind a vascular ring around the trachea and esophagus. The right common carotid and subclavian arteries come up individually from the massive right arch of the aorta. Double Pharyngeal Arch Artery this rare anomaly is characterised by a vascular ring around the trachea and esophagus. If the compression is important, it causes wheezing respirations that are aggravated by crying, feeding, and flexion of the neck. The vascular ring outcomes from failure of the distal a part of the best dorsal aorta to disappear (see. Usually the best arch of the aorta is larger and passes posterior to the trachea and esophagus (see. There are two main types: Right arch of the aorta and not using a retroesophageal component (see. Originally, there was most likely a small left arch of the aorta that involuted, leaving the best arch of the aorta posterior to the esophagus. Anomalous Right Subclavian Artery page 324 page 325 the best subclavian artery arises from the distal a part of the arch of the aorta and passes posterior to the trachea and esophagus to provide the best upper limb. A retroesophageal right subclavian artery occurs when the best fourth pharyngeal arch artery and the best dorsal aorta disappear cranial to the seventh intersegmental artery. As growth proceeds, differential growth shifts the origin of the best subclavian artery cranially till it comes to lie near the origin of the left subclavian artery. Figure 13-43 A, Sketch of the pharyngeal arch arteries showing the normal involution of the distal portion of the left dorsal aorta. There can also be persistence of the complete right dorsal aorta and the distal a part of the best sixth pharyngeal arch artery. The abnormal right arch of the aorta and the ligamentum arteriosum (postnatal remnant of the ductus arteriosus) kind a ring that compresses the esophagus and trachea. Good respiration in the new child toddler depends on regular circulatory modifications occurring at delivery, which end in oxygenation of the blood occurring in the lungs when fetal blood circulate by way of the placenta ceases. Fetal Circulation page 325 page 326 Figure 13-forty four Sketches illustrating the potential embryologic foundation of abnormal origin of the best subclavian artery. A, the best fourth pharyngeal arch artery and the cranial a part of the best dorsal aorta have involuted. As a result, the best subclavian artery forms from the best seventh intersegmental artery and the distal phase of the best dorsal aorta. B, As the arch of the aorta forms, the best subclavian artery is carried cranially (arrows) with the left subclavian artery. C, the abnormal right subclavian artery arises from the aorta and passes posterior to the trachea and esophagus. Highly oxygenated, nutrient-wealthy blood returns underneath excessive stress from the placenta in the umbilical vein (see. Here it mixes with the comparatively small quantity of poorly oxygenated blood coming back from the lungs by way of the pulmonary veins. From the left atrium, the blood then passes to the left ventricle and leaves by way of the ascending aorta. The right subclavian artery then courses cranially and to the best, posterior to the esophagus and trachea. Because of the excessive pulmonary vascular resistance in fetal life, pulmonary blood circulate is low. Approximately 10% of blood from the ascending aorta enters the descending aorta; sixty five% of the blood in the descending aorta passes into the umbilical arteries and is returned to the placenta for reoxygenation. The remaining 35% of the blood in the descending aorta supplies the viscera and the inferior a part of the physique. Aeration of the lungs at delivery is associated with a: Dramatic decrease in pulmonary vascular resistance Marked improve in pulmonary blood circulate Progressive thinning of the partitions of the pulmonary arteries; the thinning of the partitions of these arteries outcomes mainly from stretching because the lungs improve in measurement with the primary few breaths Because of elevated pulmonary blood circulate and lack of circulate from the umbilical vein, the stress in the left atrium is larger than in the best atrium. The elevated left atrial stress functionally closes the oval foramen by urgent the valve of the oval foramen against the septum secundum (see. The right ventricular wall is thicker than the left ventricular wall in fetuses and new child infants as a result of the best ventricle has been working tougher in utero. By the top of the primary month, the left ventricular wall thickness is larger than the best as a result of the left ventricle is now working tougher. The right ventricular wall turns into thinner due to the atrophy associated with its lighter workload. The colours point out the oxygen saturation of the blood, and the arrows show the course of the blood from the placenta to the heart. Observe that three shunts allow many of the blood to bypass the liver and lungs: (1) ductus venosus, (2) oval foramen, and (3) ductus arteriosus. The poorly oxygenated blood returns to the placenta for oxygen and vitamins by way of the umbilical arteries. The grownup derivatives of the fetal vessels and structures that turn into nonfunctional at delivery are proven. After delivery, the three shunts that brief-circuited the blood throughout fetal life cease to perform, and the pulmonary and systemic circulations turn into separated. B, Ultrasound scan showing the umbilical cord and the course of its vessels in the embryo. C, Schematic presentation of the connection among the ductus venosus, umbilical vein, hepatic veins, and inferior vena cava. At the top of 24 hours, 20% of ducts are functionally closed, 82% by forty eight hours, and a hundred% at 96 hours. The action of this substance seems to be dependent on the excessive oxygen content material of the blood in the aorta ensuing from aeration of the lungs at delivery. During the transitional stage, there could also be a right-to-left circulate by way of the oval foramen. The closure of fetal vessels and the oval foramen is initially a useful change. Later, anatomic closure outcomes from proliferation of endothelial and fibrous tissues. Derivatives of Fetal Vascular Structures Because of the modifications in the cardiovascular system at delivery, certain vessels and structures are no longer required. Approximately 50% of umbilical venous blood bypasses the liver and joins the inferior vena cava by way of the ductus venosus. The larger stream passes by way of the oval foramen into the left atrium, the place it mixes with the small quantity of poorly oxygenated blood coming from the lungs by way of the pulmonary veins. The smaller stream of blood from the inferior vena cava stays in the best atrium and mixes with poorly oxygenated blood from the superior vena cava and coronary sinus. Umbilical Vein and the Round Ligament of the Liver the umbilical vein stays patent for a considerable period and could also be used for change transfusions of blood throughout early infancy. These transfusions are sometimes done to prevent mind harm and dying in infants with anemia from erythroblastosis fetalis. The intra-stomach a part of the umbilical vein ultimately turns into the round ligament of liver (L. Umbilical Arteries and Abdominal Ligaments Most of the intra-stomach parts of the umbilical arteries turn into the medial umbilical ligaments (see. Oval Foramen and Oval Fossa the oval foramen usually closes functionally at delivery.
Syndromes
- Nephrotic syndrome
- Easily excitable
- Weakness in the face
- Agitation
- Steroid use
- Tricyclic antidepressants
- Multiple myeloma
- Have you noticed a growth, lump, or lesion on the genitals?
- Dry mucus membranes
- Your fingers change color and you do not know the cause.
Proven accupril 10 mg
Peripheral processes of these neurons divide to enter the vestibular mechanism, together with the three semicircular canals. Central processes of these neurons become the vestibular division of the vestibulocochlear nerve responsible for the sense of balance. The modalities inside the glossopharyngeal nerve include: special visceral efferent, general visceral efferent, special visceral afferent, general visceral afferent, and general somatic afferent (see. Because the glossopha- ryngeal nerve is the nerve of the third pharyngeal arch, it serves the one muscle derived from this arch, the stylopharyngeus muscle. Observe the communications with the vagus nerve and the contributions of each to the pharyngeal plexus. General visceral efferents (parasympathetic) sup- ply the parotid gland and different minor salivary glands within the mucous membrane in and about the posterior tongue and adjacent pharynx. Special visceral afferents are distributed to the taste buds positioned on the posterior one third of the tongue, as well as to these positioned within the circumvallate papillae. General visceral afferents supply the posterior one third of the tongue, the fauces, the palatine tonsils, and the pharynx. Other general visceral sensory fibers supply the carotid sinus with blood pressure receptors as well as to chemoreceptors positioned inside the carotid physique. The glossopharyngeal nerve leaves the mind as three or four rootlets adjacent to the vagus nerve along the medulla between the olive and the inferior cerebellar peduncle. The rootlets unite to exit the cranium by way of the jugular foramen in firm with the vagus and accent nerves. Housed within the groove inside the jugular foramen are the superior and inferior ganglia of the glossopharyngeal nerve, containing the cell bodies of the sensory fibers. While passing by way of the jugular foramen, this nerve communicates with the facial nerve, the auricular department and superior ganglion of the vagus nerve, and the superior cervical sympathetic ganglion. Tympanic Nerve the tympanic nerve arises from the inferior ganglion of the glossopharyngeal nerve. Here it types the tympanic plexus with fibers from the carotid plexus and the larger petrosal nerve. Branches from the tympanic plexus serve sensory capabilities to the mucous membranes of the eardrum, oval and spherical windows, mastoid air cells, and auditory tube. The tympanic nerve emerges from the tympanic plexus because the lesser petrosal nerve, providing preganglionic parasympathetic fibers to the otic ganglion (see Tables 18-1 and 18-2), which it reaches by leaving the cranium on the fissure between the petrous portion of the temporal bone and the larger wing of the sphenoid bone. The otic ganglion, described within the section on the mandibular division of the trigeminal nerve, lies just outdoors the foramen ovale, instantly behind the mandibular nerve. This ganglion receives preganglionic parasympathetic fibers from the lesser petrosal Chapter 18 Cranial Nerves 305 Clinical Considerations Unilateral Lesion of the Glossopharyngeal Nerve Outside Brainstem Unilateral lesion of the glossopharyngeal nerve outdoors of the brainstem will trigger loss of taste from the posterior one third of the tongue, loss of salivation from the parotid gland on the ipsilateral facet, loss of gag reflex, and loss of carotid sinus reflex. Postganglionic parasympathetic fibers go away the otic ganglion and are communicated to the auriculotemporal nerve for distribution to the parotid gland, providing it with secretomotor innervation. Pharyngeal Plexus Other fibers of the glossopharyngeal nerve be part of with pharyngeal branches of the vagus nerve and branches from the superior cervical ganglion to kind the pharyngeal plexus, positioned on the wall of the center pharyngeal constrictor muscle (Fig 18-10). Branches from this plexus penetrate the wall of the pharynx and supply the entire muscular tissues of the pharynx (besides the stylopharyngeus) and soft palate (besides the tensor veli palatini) with motor innervation and adjacent mucous membranes with sensory innervation. Glossopharyngeal contributions to the pharyngeal plexus are sensory, whereas the vagal branches are motor. Postganglionic sympathetic fibers contributed from the superior cervical ganglion to the pharyngeal plexus are vasomotor in function. Carotid Sinus Nerve the nerve to the carotid sinus arises as a small filament from the glossopharyngeal nerve subsequent to nerve communications on the jugular foramen. This department descends along the interior carotid artery, ending within the bifurcation of the frequent carotid artery. On its way to the carotid sinus, the nerve communicates with pharyngeal department(es) of the vagus and branches from the superior cervical ganglion (postganglionic sympathetic fibers). Glossopharyngeal and vagus nerves transmit afferent fibers from the chemoreceptors inside the carotid physique. Nerve to the Stylopharyngeus Muscle As the glossopharyngeal nerve courses to the posterior pharyngeal wall, a nerve to the stylopharyngeus muscle arises to supply that muscle. Pharyngeal Branches the principle trunk of the glossopharyngeal nerve terminates as a number of pharyngeal branches to enter the posterior pharyngeal wall. Some of these branches proceed to the tongue as lingual branches, providing general sensation to the posterior one third of the tongue and special sensory fibers to the taste buds on that portion of the tongue as well as to these of the circumvallate papillae. Other branches penetrate the pharyngeal wall as tonsillar branches, communicating with the lesser palatine nerve of the maxillary X. In addition to its locations inside the head and neck, the vagus nerve also enters the thorax to serve the guts and lungs, and continues 306 Chapter 18 Cranial Nerves into the stomach to supply many of the abdominal viscera. The vagus nerve possesses 5 modalities, specifically, special visceral efferent general somatic afferent, general visceral afferent, special visceral afferent, general visceral efferent. The vagus is the nerve of General somatic afferent fibers are provided to the pores and skin about the ear and external acoustic meatus. General visceral afferent supplies the mucous mem- the fourth pharyngeal arch, and its recurrent laryngeal department is the nerve of the sixth pharyngeal arch. Muscles growing from the fourth arch include the pharyngeal constrictors and the cricothyroid muscular tissues. Muscles developed from the sixth arch include the intrinsic muscular tissues of the larynx. General visceral efferent supplies the graceful muscular tissues and glands of the digestive tract from the esophagus to (and together with) many of the intestines, plus the bronchi and trachea. Special visceral afferent is provided to the bottom of the tongue, aryepiglottic fold, and larynx. The vagus nerve exits the mind on the medulla, between the olive and the inferior cerebellar peduncle just posterior to the glossopharyngeal nerve, through a cluster of 8 to 10 rootlets that unite to exit the cranium Figure 18-eleven. Chapter 18 Cranial Nerves 307 by way of the jugular foramen along with the glossopharyngeal and accent nerves. This nerve possesses two sensory ganglia: the superior ganglion, housed within the jugular fossa, and the inferior (nodose) ganglion, showing as a swelling on the nerve just after it exits the jugular foramen. Peripheral processes of the neurons in these ganglia are distributed with the vagus nerve because the sensory element. These ganglia obtain communications from the glossopharyngeal, facial, accent, and hypoglossal nerves. The sympathetic nervous system communicates through a filament from the superior cervical ganglion, and a communication also exists between the vagal ganglia and the first and second cervical nerves. The cranial root of the accent nerve joins the vagus nerve just proximal to the inferior ganglion. Thus, the motor element to the muscular tissues arising from the fourth and fifth pharyngeal arches, typically described as arising from the vagus nerve, are actually from this contribution to the vagus nerve by the accent nerve. However, autonomic motor innervation to the esophagus and the buildings inside the thorax and stomach attributed to the vagus come up from the dorsal motor nucleus of the vagus nerve. Before its exit from the jugular fossa the vagus nerve provides off two branches: the meningeal and auricular branches. Pharyngeal Branches Pharyngeal branches of the vagus come up from the inferior vagal ganglion and move over the interior carotid artery to the pharyngeal constrictor muscular tissues, providing input to the pharyngeal plexus. From this plexus, motor innervation is provided to the pharyngeal but not the stylopharyngeus, as well as to all muscular tissues of the soft palate besides the tensor veli palatini. This nerve descends along the interior carotid artery to terminate within the carotid physique housed within the bifurcation of the frequent carotid artery. Chemoreceptors detect changes in oxygen and carbon dioxide tension as well as hydrogen ion concentration within the blood at this web site. As previously described, sensory fibers from the carotid physique are also transmitted within the glossopharyngeal nerve. Superior Laryngeal Nerve the superior laryngeal nerve arises from the vagus on the inferior end of the inferior ganglion and passes deep to the interior carotid artery, descending to the thyroid cartilage, where it divides into external and internal branches. The smaller external department continues to descend beneath the sternothyroid muscle to enter the cricothyroid and inferior pharyngeal constrictor muscular tissues, which it supplies with motor innervation. This department supplies sensory innervation to the mucous membranes superiorly, to the bottom of the tongue, and to the epiglottis and the larynx as far inferiorly because the vocal folds. It is with this department that the feeling of taste is transmitted to the mind from the bottom of the tongue, epiglottis, and larynx. The internal laryngeal department also contains parasympathetic fibers to the glands related to the mucous membranes of the areas just described.
Effective accupril 10 mg
The oral cavity is lined with mucous membrane composed of stratified squamous epithelium and an underlying dense, irregular, collagenous connective tissue that houses minor salivary glands. For functions of description, the oral cavity is subdivided into two main areas: the outer vestibule and the inner oral cavity proper. They are lined externally with pores and skin that overlies muscle, glands, and connective tissue. The purple portion of the lips, whose coloration is attributable to a wealthy vascular bed visible via the skinny epithelium, is termed the vermilion zone. The superior lip is bounded laterally by the nasolabial groove extending from the ala (wing) of the nose to a brief distance lateral to the nook of the mouth. The two lips are related laterally by the labial commissures, that are skinny folds of tissue which are easily considered when the mouth is barely opened. Occasionally a slight depression is famous in the heart of the labial commissure, often known as the commissural lip pit. The oral fissure (rima of the mouth) is the zone between the superior and inferior lips, which may be opened or, when the two lips are involved with one another, closed. The lips develop from several sources, including the median nasal (intermaxillary section), maxillary, and mandibular processes. Many of the buildings simply described are fusion remnants of these embryologic origins and sometimes turn out to be more pronounced with advancing age. A more detailed description of the development and congenital deformities of the lips is introduced in Chapter 5. The vestibule is the space between the lips and the cheeks external to the tooth in occlusion. The vestibule is the cleft or space between the lips and cheeks externally and the tooth and gingiva of the dental arches internally when the tooth are in occlusion. The vestibule communicates with the exterior via the oral fissure of the lips and with the oral cavity proper by way of the interdental spaces and the interval posterior to the final molar tooth in every dental arch. The mucobuccal and/or mucolabial folds (fornix) represent the placement level at which the regionally named vestibular mucosa turns to turn out to be the alveolar mucosa. Located Chapter four the Oral Cavity, Palate, and Pharynx 33 Clinical Considerations Lips Cleft lip, typically related to cleft alveolar and primary palate, is the result of a developmental defect and happens in approximately 1 in 1, 000 births. The terminology and severity of this and associated defects in the palate are mentioned intimately in Chapter 5. Congenital commissural lip pits could also be observed infrequently at the angle of the mouth in the commissure. Abnormally giant superior labial frenula might invade the interdental space between the maxillary central incisors, thus inflicting a large diastema. If after an inexpensive time the diastema persists, orthodontic treatment could also be essential. Protruding into the roof of the buccal vestibule in the vicinity of the first molar is the zygomatic process of the maxilla. The practically vertical anterior border of the masseter muscle may be palpated in the posterior buccal vestibule because it extends from the angle of the mandible to the zygomatic arch. The region of the maxilla posterior to the zygomatic process and superior to the final molar is the maxillary tuberosity. This is a crucial area anatomically because it serves as an injection web site for anesthesia of the posterior superior alveolar nerve. The parotid gland empties its salivary secretions into the buccal vestibule at a small orifice opposite the second maxillary molar. This opening, which seems elevated in the mucosa, is the parotid papilla (Stenson duct). Several different small minor salivary glands which are regionally named-for example, the 6 7 1 2 three four 5 1 5 three 2 four Figure four-three. Superior labial vestibule indicating regionally named gingiva covering anatomic areas of maxillae. Buccal vestibule with opening of parotid duct opposite the second maxillary molar. In most people, small yellow spots could also be observed in the buccal mucosa lateral to the nook of the lips. These are Fordyce granules, composed of defunct sebaceous glands that became trapped in the mucosa throughout development. Extra reflections of labial mucosa appear as folds of tissue in the midline attaching the superior and inferior lips to the gingiva. Occasionally, the superior labial frenulum is so broadly attached that it interferes with regular eruption of the central incisors, thereby producing a diastema. Correction of this situation often requires surgical elimination of the frenulum between the central incisors to allow the tooth to return to the normal place. The gingiva (gum) is covered by the gingival mucosa, which folds back on itself to form a free edge, often known as the gingival margin, which surrounds the inferior margin of the clinical crowns of the tooth. The vestibular gingiva in this region turns into continuous with the gingiva of the oral cavity proper. The interdental papilla lies between the tooth in the interdental spaces, and the retromolar papilla is that specialised area of the gingiva distal to the final molars in both dental arches. The coronal-most aspect of the interdental papilla of the molar region often possesses a concavity often known as the col. The alveolar mucosa overlies the alveolar processes of both the maxillary and mandibular arches. Its purple hue is attributable to the visibility of its vascularity via the nonkeratinized epithelium of its mucosa. However, a quite sharp, scalloped line, the mucogingival junction, separates the gingival mucosa from the alveolar mucosa. The oral cavity proper is that part of the oral cavity mendacity internal to the dental arches of each jaw and their surrounding gingiva. The oral cavity proper lies internal to the dental arches and their contained dentition and gingiva. It is bounded superiorly by the palate and inferiorly by the muscular tongue and reflections of the mucous membrane extending from the mandibular gingiva in the sublingual sulcus (groove) to the bottom of the tongue. The posterior boundary of the oral cavity proper is formed by the vertical portion of the taste bud superiorly and by the anterior pillar of the fauces (the palatoglossal arch). This arch, which includes the palatoglossus muscle and overlying oral mucosa, extends from the taste bud to the edges of the bottom of the tongue. Chapter four the Oral Cavity, Palate, and Pharynx 35 Clinical Considerations Vestibule A fold of mucosa in the posterior-most boundary of the vestibule connecting the maxillary and mandibular alveolar areas covers the pterygomandibular raphe. The superior labial frenulum incessantly possesses a tag of tissue located on its anterior surface approximately halfway between its attachments at the lip and gingiva. The region of the buccal mucosa adjoining to the mandibular retromolar papilla incorporates an aggregation of accessory buccal glands that results in a prominence in the mucosa. This, along with the retromolar papilla, is often referred to incorrectly because the retromolar pad. Occasionally, a white line, the linea alba, could also be observed on the buccal mucosa representing that area of three 2 1 the mucosa in shut proximity to the occlusal surfaces when the jaws are in the closed place. The space of the vestibule is somewhat lowered when the mouth is opened by the forward motion of the coronoid process of the mandible as its condyle strikes forward and downward. This might interfere with dental radiographic procedures in the maxillary molar area and in getting ready study models and making maxillary dentures. The masseter muscle also impinges on the vestibular space because the mouth is closed and tooth are clenched. The anterior fringe of this muscle could also be palpated in the clenched place by inserting a finger in the buccal vestibule. The presence of this muscle should be taken under consideration when fitting a mandibular prosthesis. Communication of the oral cavity proper with the vestibule has been mentioned previously; now its communication with the pharynx will be described. The oral cavity communicates with the oral pharynx by way of the oropharyngeal isthmus, the fauces. This aperture is bounded by the taste bud superiorly, by the surface of the posterior one third of the tongue inferiorly, and by the palatoglossal arch laterally. For instance, the palatine tonsil lies in a tonsillar crypt between the palatoglossal and palatopharyngeal arches.
Buy accupril 10 mg
It makes use of a pin and tube apparatus to maintain the mandible in an advanced place and is kind of appropriate with the presence of a fixed appliance on anterior enamel (but also can be utilized with bonded or detachable splints). Note that for this patient the pin and tube attaches to steel crowns on the molars, that are sturdier than molar bands, and extensions from the lower crowns are bonded to the lower premolars. For a child with a facial asymmetry, an appliance of the sort shown here could be efficient in improving both the vertical and a-p aspects of the issue. Note that the enamel are free to erupt on the left facet (which requires a lingual in addition to a buccal shield), whereas a chunk block impedes eruption on the opposite. The chunk is taken to convey the jaw to the midline, advancing the deficient facet (here, the left) more than the opposite. The energetic element normally is a jackscrew positioned so that it holds the components of the plate collectively (see Figure 103). The screw offers the advantage that the quantity of movement could be managed, and the baseplate remains rigid despite being minimize into two components. The disadvantage is that the force system could be very different from the best one for transferring enamel. Rather than offering a light however continuous force, activation of the screw produces a heavy force that decays quickly. Activating the screw too quickly results in the appliance being progressively displaced away from the enamel rather than the arch being expanded as desired. Removable Appliances with Springs for Tooth Movement In contrast to the heavy, quickly decaying forces produced by a screw, practically optimum light continuous forces could be produced by springs in a detachable appliance. The guideline for tooth movement with a spring from a detachable appliance subsequently is that this method ought to be used only when a couple of millimeters of tipping movement is suitable. Clear Aligner Therapy Development of Clear Aligners the use of clear aligners in orthodontic treatment for adults grew to become attainable as vacuum-fashioned clear thermoplastic sheets were launched into orthodontics in the Nineteen Eighties. The spring on the mesial of the canine exerts a heavier force than the distal spring, leaving a web force to move the canine distally, whereas the couple essential for management of root place is created by the opposing motion of the two springs. Although bodily movement with a detachable appliance is theoretically attainable with spring preparations of this type, the spring changes and clasp preparations become too complicated for sensible scientific use. C, Creating a divot in the aligner, in this case to enhance movement of one maxillary central incisor. D, the modified aligner in place, with elevated stress in opposition to the central incisor. It grew to become obvious rather quickly, nonetheless, that if enamel were reset barely and the vacuum-fashioned sheet was made to fit the reset enamel, a tooth transferring system rather than a retainer would be the result. The system now could possibly be, and quickly was, referred to as an "aligner" as a result of the everyday use was to convey mildly displaced enamel back into alignment, as, as an example, when delicate irregularity of maxillary or mandibular incisors occurred in an orthodontic patient after retainers were discontinued. Only small amounts of tooth movement are attainable with a single aligner, nonetheless, because of the stiffness of the plastic materials. To get hold of more than minor modifications, it was essential both to reshape the aligner or make a new one on a new forged with the enamel reset to a greater diploma. Because the suck-down materials is softened and turns into moldable when heated, it will be attainable to alter the shape of an aligner with a heated instrument, 2 and in an attempt to lengthen the use of aligners, a particular heated pliers for this type of reshaping was offered as a way to keep away from the price and complexity of having to make a number of new aligners (Figure 10-11). This nonetheless allowed only minor tooth movement, and talent was required to get hold of simply the right amount of change in the aligner. A major limitation is that the plastic can only be stretched a maximum of about three mm (in 1 mm increments) before it turns into too thin to exert force. It grew to become clear that a sequence of a number of aligners, made on a series of casts with some enamel reset in small increments (no more than 1 mm) to a new place, would be needed to appropriate even delicate malalignment. Although a sequence of modified dental casts could be produced by hand and a brief sequence of two to 5 aligners created from these casts works for minor tooth movement, this is prohibitively time consuming and troublesome if more than a few aligners are required. In the late Nineties, a new company, Align Technology, obtained venture capital to computerize the method of manufacturing a sequence of casts with incremental modifications on which aligners could possibly be fabricated. With careful planning, this may end in a sequence of aligners that would appropriate extra complicated problems. This new method was launched with tv publicity for "Invisalign" that was designed to create shopper interest in this new method. The early days of Invisalign treatment were wrought with problems as a result of staging of treatment, optimum charges of tooth movement, and indications for use of attachments on the enamel had not been labored out, and preliminary professional acceptance of the tactic was spotty. The production process begins when the intraoral scan or impressions are used to create an accurate three-dimensional (three-D) digital mannequin of every dental arch (Figure 10-12). These information are transferred electronically to a digital treatment facility (presently in Costa Rica). A clear plastic aligner is fashioned over every mannequin, and the set of aligners is shipped directly to the doctor. In essence, when the ClinCheck is posted for the doctor to look at, the computer technician has sent a draft treatment plan for evaluate (Figure 10-14). The software program used by the computer technicians has default scenarios for various kinds of malocclusions and default charges of tooth movement. These defaults are satisfactory for less complicated cases however not for the extra complicated ones. Considerations in Clinical Use of Clear Aligners Although Invisalign is over a decade old, only a few research of the outcomes of Invisalign treatment have been revealed in refereed professional journals. C, In this view, the seated technician is conferring with one of the orthodontic advisors because the digital dental arches are displayed on the computer display screen. Invisalign (and clear aligners extra usually) do some issues nicely and others not so nicely (Box 10-1). Several different considerations in the use of sequential aligners embrace the following: the use of attachments which might be bonded to chosen enamel greatly extends the attainable tooth movement with aligners. In common, vital root movement (as in the closure of extraction sites) is nearly impossible without the use of attachments, as is closure of open bites by elongation of incisor enamel; with attachments, both are attainable (see Figures 18-40 and 18-forty one). Even with attachments, vital rotation of rounded enamel (canines and premolars) is troublesome. It is possible to bond a button to a rotated tooth so that a rubber band can be utilized to rotate it whereas an aligner is being worn (see Figure 10-14). There is an growing development toward a mix method to complicated treatment, using a brief part of partial fixed home equipment or auxiliaries in addition to the sequence of aligners. If this is done, it is very important remember that tooth movement causes transient pulpitis and so does bleaching. This could be managed by growing the intervals between bleaching sessions, however bleaching normally is better deferred until the retention stage. The scientific use of clear aligners in adjunctive and comprehensive treatment is discussed in greater element in Chapter 18. Fixed Appliances Contemporary fixed home equipment are predominantly variations of the edgewise appliance system. For this patient, bonded attachments are to be positioned as shown in the frontal and maxillary occlusal views. B, Bonded attachments on the facial floor of the enamel (identical patient because the Clincheck kind) are made of clear plastic in a wide range of shapes. These are essential to produce rotation or extrusion and facilitate different forms of tooth movement. For this patient, the higher incisors are to be lowered barely in width to facilitate their alignment. Ligatures from a heavy labial arch were used to convey malposed enamel to the line of occlusion. E-Arch In the late 1800s, a typical orthodontic appliance depended on some kind of rigid framework to which the enamel were tied so that they could possibly be expanded to the arch kind dictated by the appliance. Bands were positioned only on molar enamel, and a heavy labial archwire extended around the arch. The end of the wire was threaded, and a small nut positioned on the threaded portion of the arch allowed the archwire to be superior so that the arch perimeter elevated. This appliance nonetheless could possibly be found in the catalogs of some mail-order orthodontic laboratories as late because the Nineteen Eighties, maybe because of its simplicity, and even though it can ship only heavy interrupted force. To overcome this issue, Angle started placing bands on different enamel and used a vertical tube on every tooth into which a soldered pin from a smaller archwire was positioned. With this appliance, tooth movement was completed by repositioning the individual pins at every appointment.
10mg accupril
This provides some latitude for the tooth to rebound earlier than last settling is achieved. Rebound is a 1 to 2 mm phenomenon; posturing can result in 4 to 5 mm relapse, and clearly you will need to detect it and continue therapy to a true correction. These concerns result in the guidelines for ending therapy when interarch elastics have been used: 1When an acceptable degree of overcorrection has been achieved, the force used with the elastics should be decreased whereas the light elastics are continued full time for an additional appointment interval; 2At that time, interarch elastics should be discontinued, 4 to eight weeks earlier than the orthodontic home equipment are to be removed, so that modifications due to rebound or posturing could be observed. It is best to tell the patient that she or he is getting a vacation from the elastics and that some further elastic put on may be necessary if modifications are observed, quite than saying that elastics are now not wanted. If modifications do occur, that makes it simpler for sufferers to accept that the vacation is over and one other interval of elastics is required. For upper molar and premolar tooth, a band-removing instrument is placed so that first the lingual, then the buccal surface is elevated (Figure sixteen-thirteen). For the decrease posterior tooth, the sequence of force is simply the reverse: the band remover is utilized first on the buccal, then the lingual surface. Bonded brackets should be removed, insofar as possible, without damaging the enamel surface. This is finished by creating a fracture throughout the resin bonding material or between the bracket and the resin and then removing the residual resin from the enamel surface. With metal brackets, applying a slicing pliers to the bottom of the bracket so that the bracket bends (Figure sixteen-14) is the safest method. This has the disadvantage of destroying the bracket, which in any other case could be reused, but defending the enamel normally is a more necessary consideration. Enamel harm from debonding metal brackets is uncommon, but there have been numerous reports of enamel fractures and removal of chunks of enamel when ceramic brackets are debonded (see Chapter 10 for a more detailed discussion). It additionally is straightforward to fracture a ceramic bracket whereas trying to take away it, and if that happens, massive pieces of the bracket should be ground away with a diamond stone in a handpiece. Shearing stresses are utilized to the bracket to take away it, and the mandatory force can turn into alarmingly massive. A, Lower posterior bands are removed primarily with strain from the buccal surface. B, Upper posterior bands are removed with strain primarily against the lingual surface, which is simpler when a lingual tube (as seen here), cleat, or different attachment was welded to the band initially. Most of the ceramic brackets now available on the market have an interface designed to make removal simpler. Chemical bonds between the bonding resin and the bracket could be too good, and most manufacturers now have weakened them or abandoned chemical bonding altogether. One benefit of a metal slot in a ceramic bracket is that then the bracket could be engineered to fracture within the slot area, which makes it a lot simpler to take away. Electrothermal and laser devices to warmth ceramic brackets for removal now are available. Cement left on the tooth after debanding could be removed easily by scaling, but residual bonding resin is tougher to take away. A particular pliers can be used to fracture the bonding resin, which normally ends in a lot of the resin left on the tooth surface. The benefit of this method is that the bracket normally is undamaged; the disadvantage is heavy force that will trigger enamel harm. The first approach is more suitable with recycling of brackets, but the second is safer and normally leaves much less resin to take away from the tooth surface. Topical fluoride should be utilized when the cleanup process has been accomplished, however, since a number of the fluoride-wealthy outer enamel layer may be misplaced with even probably the most careful approach. Positioners for Finishing An alternative to segmental elastics or light round archwires for last settling is a full-arch tooth positioner. A positioner is best whether it is placed immediately on removal of the fastened orthodontic appliance. As part of the laboratory process, bands and brackets are trimmed away, and any band area is closed. This indirect approach permits individual tooth positions to be adjusted with appreciable precision, bringing every tooth into the specified last relationship. Removing extra bonding resin is finest achieved with a smooth 12-fluted carbide bur, followed by pumicing. The use of a tooth positioner quite than last settling archwires has two benefits: (1) it permits the fastened appliance to be removed considerably more quickly than in any other case would have been the case. The gingival stimulation provided by a positioner is an excellent method to promote a rapid return to regular gingival contours (Figure sixteen-17). First of all, these home equipment require a substantial quantity of laboratory fabrication time and therefore are costly. Second, settling with a positioner tends to improve overbite greater than the equivalent settling with light elastics. This is a drawback in sufferers who had a deep overbite initially but could be advantageous if the initial downside was an anterior open chunk. It is an error to take away a modern fastened appliance early and rely upon a positioner to accomplish greater than minimal settling of the occlusion. At current, there are two major indications for use of a positioner: (1) a gingival condition with greater than the same old degree of irritation and swelling on the finish of lively orthodontics or (2) an open chunk tendency, so that settling by delicate despair quite than elongation of posterior tooth is required. Severe malalignment and rotated tooth, a deep chunk tendency, and an uncooperative patient are contraindications for positioner use. Often the positioner impression is taken one month earlier than debanding, with bands and brackets carved off the tooth within the laboratory, so the positioner could be delivered immediately after the appliance is removed. Their use is especially necessary when a positioner is utilized in a maxillary premolar extraction case. A positioner should be worn by the patient a minimum of 4 hours during the day and through sleep. Since the amount of tooth motion tends to decline rapidly after a couple of days of use, an excellent schedule is to take away the orthodontic home equipment, clear the tooth and apply a fluoride therapy, and place the positioner immediately, asking the patient to put on it as almost full time as possible for the primary 2 days. Final (posttreatment) records and retainer impressions could be taken 2 or three weeks after the positioner is placed. Special Finishing Procedures to Avoid Relapse Relapse after orthodontic therapy has two main causes: (1) continued progress by the patient in an unfavorable pattern and (2) tissue rebound after the discharge of orthodontic force. These modifications are due to the pattern of skeletal progress, not simply to tooth motion. Controlling this sort of relapse requires a continuation of lively therapy after the fastened home equipment have been removed. The different, which often is more acceptable to the patient, is to use a useful appliance quite than a traditional retainer after the completion of fastened appliance therapy. Control of Soft Tissue Rebound A main cause for retention is to maintain the tooth till soft tissue reworking can take place. A, Swollen maxillary papillae immediately after band removal, simply earlier than placement of an immediate positioner. This degree of gingival swelling and puffiness occurs solely rarely throughout fastened appliance therapy, but when it does, a positioner is among the finest means to resolve it. There are two ways to cope with this phenomenon: (1) overtreatment, so that any rebound will solely bring the tooth back to their correct place, and (2) adjunctive periodontal surgical procedure to cut back rebound from elastic fibers within the gingiva. Whatever the mechanism used to appropriate crossbite, it should be overcorrected by a minimum of 1 to 2 mm earlier than the force system is released. If the crossbite is corrected during the first stage of therapy, as should be the case, the overcorrection will gradually be misplaced throughout succeeding phases of therapy, but this could enhance stability when transverse relationships are established exactly during the ending part. Just as with crossbites, irregularities and rotations could be overcorrected during the first part of therapy, carrying a tooth that has been lingually positioned barely too far labial, for example, and vice versa. It is sensible to maintain the tooth in a barely overcorrected place for a minimum of a couple of months, during the finish of the primary stage of therapy and the second stage. Maintaining an over-rotated place could be carried out by adjusting the wings of single brackets, or by sustaining a rotation wedge in place with twin brackets. Maintaining overcorrected labiolingual positions of incisors is finished readily with first-order bends in working archwires. Rotated tooth should be maintained in an overcorrected place so long as possible, but even then, these tooth are sometimes candidates for the periodontal procedures described below. Adjunctive Periodontal Surgery Sectioning of Elastic Gingival Fibers A main reason for rebound after orthodontic therapy is the network of elastic supracrestal gingival fibers. As tooth are moved to a new place, these fibers tend to stretch, and so they remodel very slowly.
10 mg accupril
The improve in dimension of the uterus largely outcomes from hypertrophy of preexisting easy muscular fibers and partly from the development of recent fibers. Note that because the conceptus enlarges, the uterus increases in dimension to accommodate the quickly growing fetus. By 20 weeks, the uterus and fetus reach the extent of the umbilicus, and by 30 weeks, they reach the epigastric area. Labor is the sequence of involuntary uterine contractions that end in dilation of the uterine cervix and expulsion of the fetus and placenta from the uterus. The fetal hypothalamus secretes corticotropin-releasing hormone, which stimulates the anterior hypophysis (pituitary) to produce adrenocorticotropin. Adrenocorticotropin causes the secretion of corticol from the suprarenal (adrenal) cortex. Peristaltic contractions of uterine easy muscle are elicited by oxytocin, which is launched by the neurohypophysis of the pituitary gland. Oxytocin also stimulates launch of prostaglandins from the decidua that stimulate myometrial contractility by sensitizing the myometrial cells to oxytocin. Estrogens also improve myometrial contractile exercise and stimulate the discharge of oxytocin and prostaglandins. From research carried out in sheep and nonhuman primates, it appears that evidently the period of pregnancy and the process of birth are underneath the direct management of the fetus. During this part, regular painful contractions of the uterus happen lower than 10 minutes aside. Expulsion begins when the cervix is fully dilated and ends with supply of the infant. During the second stage of labor, the fetus descends through the cervix and vagina. The average period of the second stage is 50 minutes for primigravidas and 20 minutes for multigravidas. The placental stage begins as soon because the baby is born and ends with the expulsion of the placenta and membranes. The period of the third stage of labor is quarter-hour in roughly 90% of pregnancies. A retained placenta is one which has not been expelled within 60 minutes of supply of the infant. Integration hyperlink: Routine examination of the new child infant Retraction of the uterus reduces the realm of placental attachment (see. A hematoma, a localized mass of extravasated blood, soon types deep to the placenta and separates it from the uterine wall. The placenta separates through the spongy layer of the decidua basalis (see Chapter 2). The myometrial contractions constrict the spiral arteries that provided blood to the intervillous space. The Placenta and Fetal Membranes after Birth the placenta and fetal membranes are extruded from the uterus after birth. The placenta commonly has a discoid shape, with a diameter of 15 to 20 cm and a thickness of two to three cm. It weighs 500 to 600 g, which is roughly one sixth the burden of the average fetus. The margins of the placenta are continuous with the ruptured amniotic and chorionic sacs. As the placenta develops, chorionic villi normally persist only the place the villous chorion is in touch with the decidua basalis. When villi persist on the complete surface of the chorionic sac (an unusual occurrence), a skinny layer of placenta attaches to a large area of the uterus. When villi persist elsewhere, a number of variations in placental shape happen: accessory placenta. Gestational Choriocarcinoma Abnormal proliferation of the trophoblast ends in gestational trophoblastic disease, a spectrum of lesions including highly malignant tumors. The cells invade the decidua basalis, penetrate its blood vessels and lymphatics, and may metastasize to the maternal lungs, bone marrow, liver, and other organs. Gestational choriocarcinomas are highly delicate to chemotherapy, and cures are normally achieved. Maternal Surface of the Placenta the attribute cobblestone look of the maternal surface is produced by barely bulging villous areas-cotyledons-which are separated by grooves that were formerly occupied by placental septa. The surface of the cotyledons is covered by skinny grayish shreds of decidua basalis that separated from the uterine wall when the placenta was extruded. These shreds of tissue are recognizable in sections of the placenta which are examined underneath a microscope. Most of the decidua is temporarily retained in the uterus and is shed with the uterine bleeding. Examination of the placenta prenatally by ultrasonography or magnetic resonance imaging. C to E, the fetus is passing through the cervix and vagina through the second stage of labor. Separation of the placenta ends in bleeding and formation of a giant hematoma (mass of blood). Episiotomy, surgical incision of the perineum to facilitate birth, may be performed because the fetal head distends the perineum. Fetal Surface of Placenta the umbilical twine normally attaches to the fetal surface of the placenta, and its epithelium is continuous with the amnion adhering to the fetal surface. The chorionic vessels radiating to and from the umbilical twine are clearly seen through the clear amnion. The umbilical vessels branch on the fetal surface to kind chorionic vessels, which enter the chorionic villi and kind the arteriocapillary-venous system (see. Placental Abnormalities Abnormal adherence of chorionic villi to the myometrium is called placenta accreta. When chorionic villi penetrate the full thickness of the myometrium to or through the perimetrium (peritoneal overlaying), the abnormality is called placenta percreta. Third-trimester bleeding is the frequent presenting signal of these placental abnormalities. When the blastocyst implants near or overlying the inner os of the uterus, the abnormality is called placenta previa. The fetus has to be delivered by cesarean part when the placenta fully obstructs the inner uterine os. The Umbilical Cord the attachment of the umbilical twine to the placenta is normally near the middle of the fetal surface of this organ (see. For example, insertion of it on the placental margin produces a battledore placenta (see. The umbilical twine is normally 1 to 2 cm in diameter and 30 to 90 cm in length (average, 55 cm). A very quick twine might cause untimely separation of the placenta from the wall of the uterus throughout supply. Each cotyledon consists of numerous major stem villi with their many branch villi. The grooves were occupied by the placental septa when the maternal and fetal elements of the placenta were collectively (see. B, Fetal surface displaying blood vessels operating in the chorionic plate deep to the amnion and converging to kind the umbilical vessels on the attachment of the umbilical twine. D, Placenta with a marginal attachment of the twine, typically referred to as a battledore placenta because of its resemblance to the bat used in the medieval recreation of battledore and shuttlecock. Because the umbilical vessels are longer than the twine, twisting and bending of the vessels are frequent. They incessantly kind loops, producing false knots which are of no significance; nonetheless, in roughly 1% of pregnancies, true knots kind in the twine, which can tighten and cause fetal dying resulting from fetal anoxia. In most instances, the knots kind throughout labor as a result of the fetus passing through a loop of the twine. In roughly one fifth of deliveries, the twine is loosely looped around the neck with out elevated fetal threat.
References:
- http://porphyria.eu/sites/default/files/files/2014%20Porphyria%20safe%20list%20only.pdf
- https://www.cityofmadison.com/fire/documents/frf-intro-to-firefighter-fitness.pdf
- https://www.dcms.uscg.mil/Portals/10/CG-1/PSC/PSD/docs/VBA-21%20-%20Mental%20health%20DBQ%20form.pdf?ver=2017-03-28-110138-457