.png)
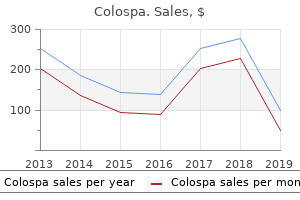
Colospa 135mg
Watery diarrhea mixed with (blood, pus & mucus) with tenesmus Weight loss & dehydration 2nd - 4th decades. Corticosteroids (systemic or by enema) Antibiotics (acute disease) sulphasalazene or flagyl Antispasmodics for pain B- Surgical Total proto-colectomy + terminal ileostomy. Total colectomy + ileo-rectal anastomoses with common endoscopic observe up of the rectum. Signs 1- General signs; - Anemia, clubbing fingers & hepato-splenomegaly 2- Local signs; - Tender & thickened sigmoid colon. B- Barium enema - It exhibits quantity of}, rounded filling defect of variable sized and localized to sigmoid colon + rectum. Site; Multiple polyps at colon & rectum N/E; Sessile or pedunculated at least of|no less than} one hundred in number three Types - Tubular - Villous. It is related to extra-colonic lesions embrace Osteoma of cranium & mandible, sebaceous cysts and desmoid tumors. Blood spread Mainly via portal vein to liver & not often to the lung Transperitoneal spread Leads to peritoneal nodules & ascites. Ns D = Distant metastasis 148 N = Nodes N0 = No nodes are concerned N1 = 1 - 2 nodes are concerned N2 = three or more nodes are concerned M = Metastases M0 = No metastases. Ascending colon, hepatic flexure & proximal 1/3 of transverse colon - Removal of peritoneum of post, belly wall between the resected colon & sup. Tumors of transverse colon Transverse colectomy is finished by - Removal of draining L. Ns & ligation with division of middle colic vessel at their origin from the superior mesenteric vessels the Extent of devascularized resected intestine is; Transverse colon & mesocolon 2 flexure (hepatic & splenic) - Removal of higher omentum Restoration of continuity by finish to finish anastomosis C. Tumor of sigmoid colon Sigmoid (Pelvic) colectomy is finished by - Removal of draining L. Ns & ligation with division of sigmoid vessel at their origin from the inferior mesenteric vessels the Extent of devascularized resected intestine is; Sigmoid colon Sigmoid mesocolon. Tumors on the higher 1/3 of rectum Anterior resection (without colostomy) = - Removal of draining L. The higher half of rectum the 2 lateral rectal ligaments - With preservation of sphincters & levator ani. Tumors on the lower 2/3 of rectum Abdomino-perineal resection (with colostomy) = - Removal of draining L. Partial prolapse (Prolapse of mucosa solely of rectum) - Common in children due to of} Loss of curve of sacrum so rectum is a vertical tube. Loss of weight so lack of ischeo-rectal & para- rectal fats Chronic straining at defecation with prolonged diarrhea. Atony of sphincters (mainly with elder) Chronic straining due to of} urethral stricture. Picture of issues as irreducibility, bleeding, fecal incontinence, ulceration & pruritis. Conservative therapy mainly via Correct the cause of|the purpose for} straining & enhance dietary status. B- In the wall As atresia or stricture (inflammatory or neoplastic) C- Outside the wall As adhesions or internal herniation Portion of the small intestine passes into considered one of retroperitoneal fossa or into a congenital defect in the mesenteries. Anti-physiological = vomiting 158 - Stage of dilatation; the proximal section begin to fatigue then dilates stagnation which invites an infection & fermentation = distension. Diffusion from blood into bowel lumen (22 %) extreme steady distention leads to occlusion of veins edema of the wall of lumen more distention resulting in occlusion of arterioles ischemia & gangrene of the bowel perforation of the intestine peritonitis. Vomiting; - At 1st gastric juice (whitish mucoid) - Then jejunal contents (greenish bile stained) - Finally intestinal contents (brownish faecal(3. Absolute constipation; - Which is failure to pass flatus or stools despite need Signs 1. General signs; - Signs of dehydration; Inelastic dry skin, sunken eye, dry tongue, oliguria. B- Immediate operation Exploratory laparotomy Inspect the caecum - If distended colonic obstruction. Remove the cause of|the purpose for} obstruction the contents are pulled out & examined, viable or not Viable intestine Intestinal colour Peritoneal luster Mesenteric arteries By pinching Consistency If injured Pink or dark pink Present. Non pulsating No response Floppy No bleeding D- Intraoperative exams (To detect viability) 1. Reperfusion injury Return of blood flow (either spontaneously or by surgery) launch of oxygen free radicals from ischemic bowel. B- Immediate operation Exploratory laparotomy then resect the gangrenous intestine and restore blood flow of the viable ones by endarterectomy or bypass for thrombosis A 2nd look operation after 24 hours is advised for patients who receive a 1ry anastomosis 162 2. The returning or middle layer the getting into or inner layer the getting into & the returning layers called intussusceptum & they meet on the apex the ensheathing layer called intussuscepien & It joins the returning layer on the neck the mesentery (containing blood vessels) could also be} compressed between the getting into & the returning layers resulting in ischemia & gangrene. B- Operative reduction - It remains to be the standard therapy of all instances, via a Rt. Absolute constipation is " early " Vomiting " late " Signs P/R examination exhibits empty rectum, blood could also be} discovered on tip of examining finger. Toxic inhibition of intestinal motility as peritonitis Metabolic abnormalities as K & Na. Annular pancreas (see pancreas) Congenital megacolon Imperforated anus 3- Outside the wall; Volvulus neonatorum. Pathogenesis; the an infection reach the peritoneal cavity via the Fallopian tubes. Sudden perforation of hole viscus (no time for localization) Spread of an infection via stimulation of peristalsis. Children due to of} small higher omentum which not assist in localization of an infection. V antibiotics as a mixture of Ampicillin, Aminoglycosides & Metronidazole B- Exploratory laparotomy the pus is aspirated & the 1ry lesion is dealt with. Moves throughout but not alongside the foundation of mesentery (the root of mesentery extends from the left hypochondrium to the right iliac fossa). The mass is dull on percussion with an overlying band of resonance (corresponding to the related loop of intestine). Signs Tenderness in the right iliac fossa Abdomen exhibits palpable irregular, firm lymph nodes. Surgical therapy For complicated instances as intestinal obstruction; Division of adhesions. Anal canal musculature 1- the inner sphincter - It is a continuation of the round muscle coat of the rectum. Surgical significance (1) Internal sphincter exhibits spasm in any painful anal situation. The mucosa of the anal canal 1- Anal columns (Columns of Morgagni) - longitudinal folds finish in anal valves. Signs 1- Acute fissure is seen & not felt with extreme spasm of anal sphincter 2- Chronic fissure is seen & felt with sentinel pile under. A- Acute fissure (Mainly conservative) 1- Relieve constipation by liquid paraffin & weight-reduction plan. Secondary piles 1- Pregnancy; Intra-abdominal stress & laxing impact of the progesterone. B- If delayed identified Conservative measures including relaxation in mattress with foot of mattress is raised to venous congestion, antibiotics, analgesics, laxatives, frequent warm baths & lead subacetate lotion to edema. Some surgeons; Perform maximal anal dilatation beneath anesthesia to relieve Sphincter spasm. Curettage or cautary of the observe then left open to heal by granulation tissue b- Fistulectomy (Excision of the fistulous track) Not indicated to keep away from the risk of sphincter damage. Symptoms Patient could also be} asymptomatic or usually current with discharge Signs the discharges are seen sometimes free hair comes out of them. Complete rectal prolapse the prolapsing rectum stretches the anal sphincters damaging them. Metastatic neuroblastoma Sacro-coccygeal teratoma 2- In 1st 2 years of life; Neuroblastoma. Indirect trauma; Fracture ribs or pelvis Spontaneous rupture; Rare with pathological diseases B- Opened trauma Gunshot wounds. B- Examination May reveals signs of internal Hge & shock + signs of external trauma as bruises. Therapeutic embolization via the splenic artery by gel foam splenic infarction Splenic mesh wrap; Placing the injured spleen in the heart of the mesh & sewing each ends of the mesh together to tamponade the bleeding.
Purchase 135mg colospa
The prognosis is greatest made on histopathologic findings of acinar atrophy with diffuse lymphocytic infiltration, with or with out the presence of epimyoepithelial islands. General Considerations Benign lymphoepithelial lesions are also known as|also called|also referred to as} Godwin tumor, Mikulicz syndrome, or punctate parotitis. Benign lymphoepithelial lesion has a predilection for females, especially in the fifth and sixth decades of life. Pathogenesis A benign lymphoepithelial lesion is an inflammatory process characterized by lymphocytic infiltration round salivary gland ducts and parenchyma (Figure 17�1). With increasing lymphocytic infiltration, progressive acinar atrophy and even replacement of the acini end result. Upon further progression, the ductal epithelia proliferate and ultimately cause ductal obstruction. Treatment & Prognosis the therapy of benign lymphoepithelial lesion is symptomatic except the parotid enlargement is extreme sufficient to warrant a superficial parotidectomy. Complete submandibular excision is an sufficient therapy of the rare benign lymphoepithelial cyst. Pathologic features of lymphoid proliferations of the salivary glands: lymphoepithelial sialadenitis versus low-grade B-cell lymphoma of the malt type. Chronic myoepithelial sialadenitis: symptomatology, medical indicators, differential diagnostics. This condition usually impacts the parotid gland and infrequently impacts the submandibular gland; when it does affect on} the submandibular gland, it presents as a painless mass. Kimura disease of the submandibular gland is usually handled with excision of the gland and the adjacent lymph nodes. Because Kimura disease usually impacts other sites, systemic therapy with steroids and radiation additionally might prove beneficial. It presents as a spontaneously appearing, painless ulceration or swelling usually over the exhausting palate, however can happen wherever there are salivary gland tissues. The lesions are usually unilateral and might current with burning sensations and numbness. The cause is unknown, however there are associations with trauma and radiation therapy. Histology reveals the attribute pseudoepitheliomatous hyperplasia and squamous metaplasia. Care should be taken to keep away from confusing the prognosis with squamous cell carcinoma or mucoepidermoid carcinoma; the main complication is misdiagnosis. Lesions in necrotizing sialometaplasia are self-healing, usually by secondary intention, and recurrences are rare. General Considerations Kimura disease is a rare, benign persistent inflammatory disease mimicking a tumor in areas of the top and neck. Clinical Findings When Kimura disease happens in the head and neck areas, the major salivary glands are usually involved. In the parotid and submandibular glands, this disease presents as painless superficial swellings usually accompanied by regional lymphadenopathy. The formation of lymphoid follicles and the aggregation of eosinophils in the affected tissues are discovered on histologic examination. Local trauma, environmental irritation, and persistent irritation are the proposed causes of this condition. Patients current with painless swellings which have been current for an indeterminate size of time. Histologic examination reveals glandular hypertrophy and inflammatory infiltrates, however no change in the common architecture of the gland and no proof of neoplasia or atypia. Adenomatoid hyperplasia of the palate mimicking clinically as a salivary gland tumor. Angiolymphoid hyperplasia with eosinophilia differs from Kimura disease in the lack of lymphadenopathy and decreased eosinophilia. Rosai-Dorfman disease is an idiopathic benign condition characterized by histiocytic proliferation and large lymphadenopathy, together with involvement of the intraparotid lymph nodes. Surgical resection of the affected submandibular gland is the therapy of selection; however except correction of the underlying dysfunction is addressed, there persistent enlargement of any residual glands. The presence of sialosis warrants further investigation into these unsuspected systemic issues. General Considerations Sialadenosis, or sialosis, is a rare, noninflammatory condition that causes bilateral, diffuse, and painless enlargement of the salivary glands. This condition may also cause degenerative changes to the autonomic innervation of the glands. Type I cysts-Type I cysts are a duplication anomaly of the ectodermal exterior auditory canal. Therefore, excision of these congenital parotid cysts requires a parotidectomy method and preservation of the facial nerve. Dermoid cysts-A second type of congenital cyst occurring in the parotid gland is a dermoid cyst. These include obesity, alcoholic cirrhosis, diabetes, hyperlipidemia, hypothyroidism, anemia, being pregnant, malnutrition, menopause, and even sure medicines (eg, clozapine). Treatment & Prognosis the therapy of sialadenosis is directed at the underlying situations. It incorporates keratinizing squamous epithelium, sweat glands, and other related pores and skin appendages. Excision to forestall recurrent infections, with consideration to the facial nerve, is probably the most successful therapy. Mucoceles are fairly common and are seen frequently in the lip (60�70%), buccal mucosa, ground of the mouth, and palate. Fine-needle aspiration of cystic parotid gland lesions: an institutional review of 46 instances with histologic correlation. Sublingual glands and minor salivary glands are extra vulnerable to creating mucoceles owing to continuous mucous secretions in these glands, whereas the parotid and submandibular glands secrete on stimulation. Clinical Findings Mucous retention cysts typically current as pale, smooth, bluish-hued submucosal cysts. Ranulas, involving the sublingual or submandibular ducts, current as round, fluctuant masses in the mouth ground. They are usually unilateral and should affect on} any age group with no gender preference. A simple ranula is a true cyst with an epithelial lining that occurs intraorally with elevation of the mouth ground. A plunging ranula extends under the mylohyoid muscle, past the sublingual area, and includes the submandibular area. It might extend further inferiorly to current as a painless submandibular or cervical neck mass. They are thought to arise from aberrant salivary gland tissue or aberrant gland formation in the course of the finish of the sixth week of gestation. These fistula and sinus tracts might form cutaneous openings in the submandibular pores and skin with discharge. Differential Diagnosis the differential diagnoses include cystic hygroma, lymphangioma, thyroglossal duct cyst, and dermoid cyst. An important differential prognosis for a mucous retention cyst is malignant mucoepidermoid carcinoma. The therapy of a simple ranula consists of either simple excision of the cyst and potential removal of the related gland, or marsupialization of the cyst wall. In the case of plunging ranulas, therapy requires excision either intraorally or mixed with a cervical incision and extirpation of the related gland. In addition to the discomfort from dry mouth, patients with xerostomia may also expertise an altered sense of taste, dysphagia, and complications related to dental decay. In addition, many systemic situations dry mouth: Sj�gren syndrome, stress, diabetes, persistent an infection, and irradiation. The therapy of xerostomia is aimed at the underlying situations; symptomatic therapy contains an increased consumption of fluids, sialagogues, mouthwashes, and artificial saliva. In addition, there are at present medicines prescribed to decrease xerostomia for patients present process radiation. The therapy combines dental decay prevention, salivary circulate stimulation, the therapy of persistent oral candidiasis, and the usage of} salivary substitutes.
Diseases
- Cancer
- Thombocytopenia X linked
- Gastroenteritis
- Pelvic dysplasia arthrogryposis of lower limbs
- Mucopolysaccharidosis type I Hurler/Scheie syndrome
- Cerebellar agenesis
- Familial dilated cardiomyopathy
- Willebrand disease, acquired
Best 135mg colospa
The survival fee among sufferers with adenoid cystic carcinomas arising from the parotid gland is larger than that for sufferers with related tumors arising from the minor salivary glands. The intermediate cells are believed to be the progenitor of the opposite two kinds of cells. Mucoepidermoid carcinomas are categorised as low, intermediate, and excessive grade based mostly on medical conduct and tumor differentiation. Clinical aggressiveness, native invasion, and lymph node metastases are all higher, and the prognosis is worst for high-grade tumors. Histologically, low-grade mucoepidermoid carcinomas are properly circumscribed, with pushing margins and dilated cystic areas containing mucinous material. The cystic buildings are lined by mucin-producing, intermediate, or epidermoid cells. As the grade escalates, the tumors turn out to be extra infiltrative and poorly circumscribed. Nests of tumor turn out to be extra stable and irregular with intermediate or epidermoid cells dominating. High-grade mucoepidermoid carcinomas are characterized by the invasion of adjacent regular buildings, atypical mitoses, perineural invasion, and lymph node metastases. Acinic cell carcinoma happens most frequently within the fifth decade of life and in women extra usually than in men. Histologically, there are two cell types: (1) serous acinar cells (explaining the predilection for the parotid gland) and (2) cells with clear cytoplasm (Figure 18�4). There are 4 histologic patterns: stable, microcystic, papillary, and follicular. The general survival fee at 5, 10, and 15 years is 78%, 63%, and 44%, respectively. Microscopically, there may be be} one small malignant progress inside a benign mixed tumor, or the benign tumor may be be} primarily replaced by the malignant lesion with damaging infiltrative progress. Carcinoma ex-pleomorphic adenoma is the most typical malignant mixed tumor variant (Figure 18�5A); 75% happen within the parotid gland. The malignant part might have options of an adenocarcinoma, a squamous cell carcinoma, an undifferentiated carcinoma, or another type of a malignant epithelial disorder. Carcinoma ex-pleomorphic adenomas are nodular or cystic with minimal encapsulation. Unlike pleomorphic adenomas, they sometimes have areas of necrosis and hemorrhage. A true malignant mixed tumor, additionally called carcinosarcoma, could be very rare (Figure 18�5B). It has epithelial and mesenchymal malignant parts in both the first website and in nodal metastases. The progress sample can be stable or cystic, papillary or nonpapillary, with or with out mucin production, and may vary from low grade to excessive grade in histology and medical course. With newer refinements in special staining and classification methods, many malignant problems previously categorized as adenocarcinomas have outlined their own classes, including polymorphous low-grade adenocarcinoma, epithelial-myoepithelial carcinoma, and salivary duct carcinoma. Polymorphous low-grade adenocarcinoma most frequently presents as a painless, submucosal mass. There is cytologic uniformity of myoepithelial or luminal ductal cells inside one tumor, however histologic diversity of the Figure 18�3. Despite infiltrative progress and perineural invasion, the medical course is typically indolent, with < 10% having lymph node metastases. Forty % of sufferers experience native recurrence, 20% experience cervical metastases, and 40% die of disease. Unlike intraductal carcinoma of the breast, this disease happens in men three times extra frequently than in women. This malignant disorder arises from the excretory duct reserve cells and is a high-grade malignant disease process with a dismal prognosis. Histologically, there are malignant epithelial (ductal) cells and likewise malignant myoepithelial cells (Figure 18� 7). Histopathologically, trabeculae, cords, and nests of monomorphic clear cells are seen. Upon the diagnosis of a salivary gland lymphoma, a full-body analysis for other involved sites is performed, as with a brand new} diagnosis of lymphoma anyplace else within the body. The distinction is made with special immunohistochemical staining for mucin, which is positive in mucoepidermoid carci- Figure 18�8. Hematogenous metastases to the salivary glands are rare, however have been reported from lung, kidney, breast, and thyroid cancers. The contiguous extension of cutaneous malignant problems, these of sarcomas arising from the facial soft tissues, is another mechanism for secondary malignant involvement of the salivary glands. A lateral temporal bone resection may be be} required as properly if the ear canal is involved. For malignant disease of the submandibular and sublingual glands, formal supraomohyoid neck dissection is preferred over a simple gland excision. Surgery for minor salivary gland malignant neoplasms-For malignant growths of the minor salivary glands, broad native excision is really helpful. This strategy may be be} in depth, even including a cranium base resection, depending on the placement, measurement, and extension of the tumor. Tumors involving the maxillary sinus and nasal cavity might require partial or whole maxillectomy. If the ethmoid is involved with extra-sinus extension, craniofacial resection, orbital exenteration, or both may be be} required for extra in depth tumors. A transoral or mixed transoral-transcervical strategy is used for malignant neoplasms of the minor salivary glands that affect on} the oral cavity and oropharynx. A partial or whole laryngectomy or even tracheal resection is required for minor salivary gland tumors involving the larynx or trachea. Neck dissection-Neck dissection is the really helpful treatment of the neck for malignant salivary gland tumors (1) with clinically apparent cervical adenopathy (14% of cases); (2) for tumors > 4 cm (in which the risk of occult metastases is > 20%); or (3) for a high-grade histology (in which the risk of occult metastases is > 40%) (Table 18�5). Eighty-five % of malignant salivary gland problems in kids happen within the parotid gland. Adenoid cystic carcinoma of the salivary glands: a 20-year evaluation with long-term follow-up. Surgery for main salivary gland malignant neoplasms-For malignant parotid gland tumors, a total parotidectomy (or an extended parotidectomy if the tumor extends into surrounding structures) is really helpful. The facial nerve is sacrificed whether it is instantly involved with the tumor (ie, encased within the tumor, unable to be dissected from tumor, paretic, or paralyzed preoperatively). In sufferers whose facial nerve is intact but the margins of resection are near the nerve, postoperative adjuvant radiation should be thought-about because of|as a end result of} it has been shown to considerably improve native management. For malignant problems of the parotid gland with parapharyngeal area extension, surgical procedure must embody parapharyngeal area (or infratemporal fossa) dissection, sometimes requiring B. Radiation therapy-Both standard and neutron-beam radiation remedy have been advocated as Table 18�5. Incidence of occult lymph node involvement for salivary gland malignant neoplasms. This strategy is controversial, however may be be} thought-about if there are actual contraindications to surgical procedure. Adjuvant radiation to the tumor resection mattress improves native management for (1) T3 and T4 tumors; (2) tumors of high-grade histology (see Table 18�4); (3) positive nodes or perilymphatic invasion; (4) facial or other perineural involvement; (5) a detailed or positive surgical margin; (6) bone, cartilage, or muscle invasion; or (7) recurrent disease. The commonplace radiation remedy used is a unilateral mixed electron and photon method. Postoperative radiation to the neck is really helpful, as above, for main and sure minor salivary gland primary sites when there are positive neck nodes. Radiation is an appropriate various for a node-negative (ie, N0) neck with aggressive options (see indications for neck dissection). For minor salivary gland tumors, elective radiation of the N0 neck is advocated just for primary tumors of the tongue, floor of mouth, pharynx, and larynx. Conventional radiation has been shown to have prohibitively poor native management rates for inoperable disease.
Generic 135mg colospa
After this period, on the fourth day she ought to take ceremonial ablution, placed on visit a new new} (untorn) garment and ornaments after which her husband after 25. After that the priest shall * perform the rites (Garbhadhana ceremony), In the case of the hubband being absent at the time, she ought to look at at|have a look at} the solar. Then on the fourth day of her uncleanness, he ought to anoint or lubricate his body with Ghrita, ought to partake of a meals in the afternoon or night composed of boiled visit the S^ctli rice, milk and clarified butter, after which spouse bed of his the spouse additionally, in her tern, ought to observe a similar vow of sexual abstinence (Brahma-charini) for a month before that day on which she ought to anoint or lubricate oil, her body with of oil partake of meals pulse, largely composed and Masha at night. Causes of various colours of the Child:- the fiery precept (Teja-dhaitu) of the organism, which is the originator of to all colours of the skin (complexion), occurring combine largely with the watery precept of the body at the time of conception, serves to make; the child a good a complexioned one (Gaura-varna) blended with large it quantity of the chiid a earth precept (Kshiti) of the body, makes the In dark complexioned one (Krishna-varna). A related mixture of watery and ethereal principles make the child dusky yellow (Gaura-syama). Others on the contrary aver that the complexion of the child is set by the colors of the meals taken 34. A child born of an of fecund- ation foolishly or ignorantly effected through the menses his of its mom by its progenitor by is holding her on bosom through the act born of a called a Shanda and invariably reveals effeminate traits in his character. A daughter girl forty one the riding on her husband will through the act traits of sexual activity develop masculine in her character. Semen is developed in the four forms of Kliva recognized as|often recognized as} Asekya, Sougandhika, Kumbhikaand Irshaka, whereas a Shanda is devoid of that fluid (Sukra). A boneless is with cartilaginous bones) monstrosity finish result} of the sexual act during which both the events arc feminine and their Sukra (sexual secretion) unite some how or other in the may the happen in womb of one of them. Fecundation the womb of a girl, dreaming of sexual activity in the night of her menstrual ablution. Vayu carries the dislodged ovum into the uterus and reveals symptoms of pregnancy, which develop month after month until the full period of gestation. The local offspring of such a conception much less jelly-like is a Kalala (a thin bone- mass) on account of the absence of the its paternal sities elements* in serpents, improvement. The processes motion of the foetus in these of its of respiration, sleeping and womb are effected through mom. An trustworthy, pious, erudite man, who has acquired an unlimited data of his the Sastras existence, becomes largely stamp in possessed this lifetime of mental of the Sdttvika his too and Acts additionally remembers to prior births (Jatismara). Combination of Self with the impregnated matter;- the local Vdyu (nerveforce) heightens or aggravates the in heat generated by dis- the friction of the sexual organs tion. The combined ovum and semen are subsequently conAfter that, He who fined in the uterus vGarbhclsaya). Self or Ego, creator, wanderer, wit- ness, ordainer, speaker, though unmanifested takes and incomprehensible in his actual nature, hold of the 5 subtile or essential materials principles contributed by the united impregnating matter, assumes a subtile shape throughout, marked by the three elementary Chap. Factors which decide intercourse;- the start of a male-child marks the preponderance of semen its over the ovum (in conception); the start of a ele- daughter shows the preponderance of the maternal ment. A child of no-sex (hermaphrodite) is the product when ovum and sperm are equal (in their quality and the primary twelve nights after the cessation quantity). Certain authorities hold that there are to all appearances girls girl who never menstruate (lit; four - 5. According a daughter is Bhoja, a son born from intercourse on even days and issue is is born from that on odd days. Development of the Foetus:- In the primary month shaped of (in gestation the a; gelatinous the substance is only womb) molecules of the primary earth, water, parts (Mahabhuta - air, fireplace, and ether) being acted upon by chilly air (Kapham look heat (Pittam) and in (Vdyu or nerve-force) are condensed the second month. An elongated-like foetus shape of the matter; denotes that the its belong to the alternative intercourse (like e, whereas tumour- like shape {i a Salmali-bud) predicts the absence of In the any intercourse 5 a hermaphrodite), third month, lump-like protuberances seem at the places the place the 5 organs -namely the 2 arms, two be and the minor limbs legs and the head the - would body are and members of shaped in the shape of extremely small 138 papillae. The enciente time, double- hearted wishes start (Dauhrida) at the a paralysed, whose wishes and -not being of the honoured and gratified - result in the Hence of hump-backed, crooked -armed, lame, dwarfed, the wishes defect-eyed, and a blind child. The desire of a pregnant girl of to see a divine start of a child in image or an idol, predicts the her womb who would grace the council in life. A desire for the flesh of a Godha in signifies the presence of a sleepy, drowsy particular person beef on her womb who in life. The wishes of a girl destiny throughout her pregnancy are determined by ordained of the acts of the child in its and results prior existence (that are to life). Development of the FcBtus s- In fifth the month the foetus is endowed with mind (Manah^ its and wakes up from the sleep of tence. The parturition takes place both the ninth, tenth, eleventh or twelfth month the of conception, otherwise one thing hended. The be umbilical chord (Nadi) of the foetus is discovered to its hooked up to the cavity of the vein or artery of maternal half through which the essence of lymph-chyle (Rasa) produced from its the assimilated meals its of the mom, enters into organism and fastens progress and improvement, Immediately after (a fact which or understood from of blood). The son of passes from the body of the child to that of the mom and vice versa. Factors respectively equipped by the paternal and maternal parts;-Now we the shall describe foetus the parts and principles of the body of a paternal element, which are respectively contributed by maternal issue, the serum (Rasaja),the soul (Atmaja), the pure (Sattvaja) and the hairs innate physiological conditions (Satmyaja). An enciente whose sides turn into and the forepart of whose stomach is discovered to bulge out will give start to a sex-less (hermaphrodite) child. An enciente, the middle whose stomach becomes in sunk or divided the middle like a leather-bag, will 20. The Pittam (fiery or thermogenic) and (lunar principles of the body, the bodily Vayu, the three major qualities of Sattva, Rajas, and Tamas (adhesion, cohesion and disintegration), the the Self (Karma-Purusha) are 5 sense organs, and of the life the preserver (Prdnah) of the Fcetus. Folds of Skin -Seven ing (Tvaka - skin) are shaped rapidly reworking folds or layers of cover- and deposited on the the product of Sonita mixture of (semen) Sukra and (fertilized ovum) individual (of which have been thus charged with as the layers or Self in the identical method first Soul cream) are shaped and deposited on the surface of (boiling) milk. I45 the surface) is kantaka called the second; fold (from Lohitai is Vrihi and Tilakilaka, or layer measures a sixteen-twentieth of a the seat of such (cutaneous affections; as it Nyachcha and Vyanga called and so forth. These dimensions must be fleshy parts understood to hold good of the skin of the of the body, and never of the skin on the brow, or is concerning the ideas of the fingers, surgical inasmuch as there a dictum to the impact that an incision as deep as be the thickness of the thumb may made into the region of the stomach with 3. The at the Kala(s too quantity seven in all and are situated (Dhatus) of the acute borders (forming encasement and support) of the totally different elementary principles organism. These Kalds are extensively equipped tissues), with Snayus (fibrous bathed - in 5-6. Raktadhara- Kala -The; second called Raktat-dharai (Vascular tissue of the blood vessels and so forth. The blood is contained in these inside the flesh in and specifically in the veins (Sira) and the body as the liver and spleen. Meda (fat) is present (chiefly) stomach is of all animals, nicely as|in addition to} in the cartilafatty substance present in large ir. Purishadhara-Kala;- the called Purishadharai fifth kala is and being situated faecal in the Kostha in (abdomen) serves to separate the refuse the sixteen. Memorable Verse know that like -The ought to in the is fat (Sarpi) in the milk, or sugar expressed juice of sugar-cane, the (seat of) semen co- intensive with the entire organism of a person (or animal). The semen of a sexual activity man throughout an act of with a feminine underneath exhilaration all comes down from parts of his body owiiig to the act). The of blood spleen; and liver of the foetus are shaped out of the lungs are made 25, of the froth the blood; and the Unduka or faecal receptacle, of the refuge matter (Mala) of the blood. The Vdyu, com- bined with heat (Pittam) in enough proportion, rends through the internal channels into the flesh and trans- types them into muscles (Pesi). The inner cavities body mark the spots or regions the place the Vayu had continuously stayed in its embryo stage. The kidneys (Vrikkas) are made out of the essence the testes are shaped out of the of the blood and fat. The coronary heart essence of the blood, is shaped out of the essence of blood and vital Kapham; and the vessels (Dhamanis) carrying the of the body are hooked up to it principles (heart). The spleen and the lungs are situated left facet, beneath and beneath the heart on the and the it liver and Kloma (Pancreas on the right. Sleep sets in when this viscus heart) of an individual becomes of enveloped by the effects phantasm or nescience). The type of sleep which sets in when the sensation-carrying channels iSn^yu) of the which abounds Tatmasi-nidrai. Day besides in sleep forbidden in the seasons of the year, case of infants, old males, by sexual excesses, or in Kshataand persons enfeebled kshina ailments and in case of ordinary tipplers. A sleep in summer and the day enjoyed or after the fatigue of an extended journey, riding, physical labour, or to on an empty stomach. It may of be allowed as well fat, males suffering from * the loss Kapham or blood, to these of Such persons may get sleep solely, affairs. Charaka;- When the energetic self of an individual, drained in body and jnind, loses touch together with his worldly affairs, sleep comes to him, Chap. Day sleep is finish result} of perverted nature and all of the Doshas of the body are aggravated by a sleep in the day, bringing the day on many a difficult complaints similar to cough, asthma, catarrh,heaviness of the body, aching or lassitude in the limbs, fever, lack of urge for food and so forth.
Trusted colospa 135mg
Coronal T1-weighted picture in an elderly man presenting with epistaxis and left nasal obstruction demonstrates a large gentle tissue mass filling the left nasal cavity, invading the left orbit (black arrows), and increasing through the skull base into the anterior cranial fossa. Focal areas of a high signal intensity (arrowheads) are seen, preserving with} hemorrhage or melanin. Lymphomas of T-cell origin predominate within the nasal cavity, whereas these of B-cell origin predominate within the paranasal sinuses. Important anatomic variations of the sinonasal anatomy in mild of endoscopic surgery: a pictorial evaluate. This is expounded to the protein content material of the material and must be stored in mind when decoding photographs of patients with suspected chronic sinusitis. Biopsy of the posterior wall of the maxillary sinus via a Caldwell-Luc method confirmed the analysis of B-cell lymphoma. Computed tomographic and anatomical evaluation of the basal lamellas within the ethmoid sinus. The main website determined at imaging seems to be correlated with the histologic phenotype and scientific end result. The skull base can be considered in three main sections: anterior, central, and posterolateral. The main apertures of the skull base that present communication between the intracranial compartment and the extracranial head and neck are reviewed in Table 3�11, which lists every foramen or canal and its relevant contents. Fatty marrow within the left pterygoid process of the sphenoid bone (P) and the higher wing of the sphenoid is indicated. Anterior Skull Base the anterior skull base makes up the floor of the anterior cranial fossa and consists of the orbital plate of the frontal bone, the roof of the ethmoid bone, and the cribriform plate. Note that the right orbit is smaller than the left due to encroachment on the orbit by the expanded bone. The occipital condyles are laterally situated, and the squamous portion is posteriorly situated and varieties overwhelming majority of} the floor of the posterior fossa. The central skull base may be be} involved by several of} classes of disease processes: (1) people who extend upward and centrally from the deep areas of the extracranial head and neck, (2) people who extend inferiorly from the intracranial compartment, and (3) these would possibly be} intrinsic to the tissues of the central skull base. The deep facial areas that abut the central skull base include the parapharyngeal, masticator, and prevertebral portion of the perivertebral house. Disease processes main to these areas, notably neoplastic and infectious disorders, might access and involve the central skull base from beneath. Intracranial processes that will extend inferiorly to involve the central skull base are beyond the scope of this chapter. Central Skull Base the central skull base is shaped by the sphenoid and occipital bones. The basisphenoid consists of the sphenoid sinus, the sella turcica, the dorsum and tuberculum sella, and the posterior clinoid processes; in combination with the basilar half of} the occipital bone, the basisphenoid additionally varieties the clivus. The paired higher wings of the sphenoid type a lot of the floor and anterior wall of the middle cranial fossa, whereas the paired lesser wings give rise to the anterior clinoid processes and contribute to the formation of the orbital fissure. The planum sphenoidale is a flat plane that extends from the tuberculum sella posteriorly to the posterior fringe of the cribriform plate anteriorly. The basilar half of} the occipital bone is centrally situated and fuses with the basisphenoid to Figure 3�126. At surgery, a focal defect in the right cribriform plate was confirmed and repaired. Perineural spread might occur in each antegrade and retrograde directions-for example, tumor that has spread again along V3 might attain the Gasserian ganglion after which spread in an antegrade manner along V1, V2, or each, properly as|in addition to} continuing to spread in a retrograde manner again along the cisternal phase of the trigeminal nerve to the pons. Direct extension-Deep face an infection or neoplasm might involve the central skull base by direct extension, by which case a process or mass centered in a space of the suprahyoid head and neck extends to involve the central skull base by contiguous development. This sometimes leads to transforming or frank destruction of bone, marrow infiltration, and, possibly, gross intracranial extension if the skull base is breached (Figure 3�128). Perineural spread of disease-Perineural spread implies tumor extension to noncontiguous areas along nerves. The perineural spread of tumor might result in scientific signs (eg, pain, dysesthesia, and hypesthesia), but may be be} asymptomatic even when demonstrable on Figure 3�128. Coronal postgadolinium T1-weighted picture with fat saturation in a affected person with deep-seated skull base pain and proper V3 dysfunction demonstrates a large gentle tissue mass (arrows) destroying the right higher wing of the sphenoid. This was finally proved to be a nasopharyngeal carcinoma that had grown primarily superolaterally to destroy the skull base and invade the middle cranial fossa (note the elevation of the right temporal lobe). Slightly oblique coronal T1-weighted picture in a affected person with adenocarcinoma of the palate and in depth perineural spread of disease. Normal fat planes of the skull base and infratemporal fossa have been obliterated on the right by infiltrative tumor. The extent of tumor infiltration on the right is indicated by the skinny concave white arrows. Foramen rotundum (white arrow) and the vidian canal (white arrowhead) are enlarged on the right due to of} the perineural spread of disease. In addition, adjoining vascular and gentle tissue constructions might give rise to lesions (eg, aneurysms, meningiomas, and nerve sheath tumors) would possibly be} intimately associated with the central skull base and need to be considered within the differential analysis of lots in this area. Neoplasms-The central skull base may be be} involved with main or metastatic lesions. Among the extra common main lesions are chordomas, chondrosarcomas, plasmacytomas, and lymphomas, properly as|in addition to} diffuse marrow infiltrative processes similar to leukemia. The asymmetric enhancement of the right temporalis muscle (T) is a consequence of acute denervation change. Postgadolinium, enhancement varies from absent or gentle and heterogeneous to intense and homogeneous. Chondrosarcomas-Because the skull base is derived from cartilage, chondrosarcomas not uncommonly take origin right here; in fact, 75% of all cranial chondrosarcomas are situated within the skull base. These slowgrowing malignant cartilaginous tumors sometimes spread by native invasion and will cause in depth destruction of the skull base. Skull base chondrosarcomas are mostly centered on the petrooccipital fissure and their offmidline location is a helpful function in distinguishing them from chordomas. Metastatic disease-Hematogenous metastases to the skull base are extra common than main neoplasms, and most regularly originate from lung, breast, prostate, and kidney. Coronal fast spin-echo T2-weighted picture with fat saturation in a affected person with perineural spread of squamous cell carcinoma demonstrates normal fluid intensity in the right Meckel cave (M), but the substitute of normal fluid by abnormal gentle tissue (black arrowheads) on the left. The abnormal gentle tissue additionally invaded the left cavernous sinus and surrounded the cavernous phase of the inner carotid artery (C). Although the clival marrow is relatively hypointense in very younger youngsters (less than three years old), the marrow becomes progressively extra fatty in youngsters between three and 10 years and is homogeneously fatty by the teenage years. Therefore, lesions of the clivus are sometimes finest appreciated on a sagittal T1-weighted picture. The normal adult clivus and, in contrast, clival marrow infiltration are demonstrated in Figure 3�133. Chordomas-Chordomas come up from notochordal remnants inside the clivus and are sometimes centered on the midline. They additionally metastasize in roughly 40% of circumstances, mostly to bone, liver, and lymph nodes. Axial T1-weighted picture in a affected person with perineural spread of squamous cell carcinoma along the right V3, which is massively enlarged (arrowheads). Denervation atrophy (decreased bulk, fatty infiltration) is seen in the right muscles of mastication compared with the left. Most metastases are intermediate in signal on T1- and T2weighted photographs and show enhancement postcontrast. Infection-Osteomyelitis of the skull base mostly involves the temporal bone, but can also involve the central skull base. It might end result from the direct extension of sphenoid or ethmoid sinus inflammatory disease, iatrogenic or accidental trauma, or hematogenous dissemination. Diabetic and in any other case immunocompromised patients are at larger threat for skull base osteomyelitis, which can be a difficult and subtle analysis to render on imaging research. The careful evaluation of pregadolinium T1-weighted photographs for the lack of a normal, brilliant, fatty marrow signal and the subtle infiltration of fat planes adjoining to the skull base is particularly useful (Figure 3�136).
Passiflora Incarnata (Passionflower). Colospa.
- Relieving symptoms related to narcotic drug withdrawal, when used in combination with a medication called clonidine.
- A psychiatric disorder known as adjustment disorder with anxious mood when used in a multi-ingredient product (Euphytose, EUP).
- Are there safety concerns?
- Nervous stomach, burns, insomnia, hemorrhoids, asthma, heart problems, high blood pressure, seizures, fibromyalgia, and other conditions.
- What other names is Passionflower known by?
- Anxiety.
- Dosing considerations for Passionflower.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96841
Proven colospa 135 mg
Twenty (20) teeth have been instrumented with an ultrasonic sealer, 10 teeth open and 10 teeth closed. The teeth have been extracted after instrumentation and the furcations have been assessed underneath a stereomicroscope for residual calculus. Scaling and Root Planing in the furcation space is more effective when a surgical flap is utilized, and that the ultrasonic sealer is more effective than the curet in eradicating calculus in the furcation space using a surgical flap. They found that calculus-free root surfaces have been obtained significantly extra usually with flap entry than with a nonsurgical method. Their results recommend that, although both surgical entry and a extra skilled operator significantly improve calculus removing in molars with furcation invasion, total calculus removing in furcations using standard instrumentation additionally be} limited. The influence of root morphology on the effectiveness of calculus removing was studied by Fox and Bosworth (1987). The mesial and distal surfaces of 168 extracted teeth, representing all tooth varieties except third molars, have been examined to document the presence or absence of proximal concavities. Riffle (1953) found that it was inconceivable to distinguish between curetting cementum and curetting dentin. Teeth have been subsequently extracted, sectioned, and measured for cementum thickness. The results confirmed that the amount of cementum eliminated increases with the variety of strokes with the curet. Except for coronal areas, cementum was never fully eliminated; at best was reduced by two-thirds. Root planing seems to be more effective in the coronal areas where the cementum is thinner than in the apical areas. Three-hundred-sixty (360) sites on 90 extracted mandibular incisors have been instrumented with 4 different instruments: hand curet, ultrasonic sealer, air-sealer, and fine grit diamond. The lack of tooth substance was measured with a device particularly constructed for this investigation. The ultrasonic sealer caused the least amount of substance loss whereas the diamond bur caused the most amount of loss. The results confirmed that the imply cumulative lack of root substance across 40 strokes was 148. The results recommend that prime forces take away extra root substance, and loss per stroke becomes less with growing numbers of strokes. The groups have been: subgingival root planing, supragingival root planing, untreated roots with illness, gross scaled roots in vitro, and healthy nondiseased root surfaces. Pooled samples had endotoxin extracted by water/phenol methodology and assayed for amount of endotoxin by the limulus lysate test. It was found that the foundation planed groups (both supra- and subgingival) had far less endotoxin recovered than the gross scaled or untreated groups; the amounts have been near non-diseased tooth ranges. It was concluded that root planing was in a position to} render beforehand diseased root surfaces almost freed from endotoxin, to ranges comparable to healthy root surfaces of unerupted teeth. Two groups of forty six teeth every have been handled, one by curets and the opposite by ultrasonics, and have been in comparison with} 2 control groups, one of forty six untreated periodontally diseased teeth and the opposite of 31 unerupted healthy teeth. The results confirmed that thorough root planing with curets produces root surfaces almost as endotoxin free (2. Test specimens have been instrumented with the ultrasonics or ultrasonics plus air powder abrasive. Eight root specimens have been placed in fibroblast tissue tradition and have been stained for determination of fibroblast viability after 48 hours. Ultrasonics plus air powder abrasive specimens confirmed superior growth and vitality of fibroblasts. Twenty (20) extracted periodontally involved teeth have been cut into halves bucco-lingually and sterilized. The control half of each tooth was rubbed with saline and the experimental half was rubbed with 2% sodium desoxycholate adopted by human plasma. Both groups have been then placed in separate petri dishes, with fibroblast cell suspension. The findings recommend that the desoxycholate/plasma combination enhanced in vitro fibroblast attachment to diseased root surfaces. The results confirmed that the same degree of improvement was achieved following both types of therapy. The best approach to decide which method is superior in reaching that aim is by evaluating the healing response following therapy. One site served as control, the second acquired oral hygiene alone, and the third was handled by root planing and oral hygiene. Eight to 9 weeks after therapy, measurements have been taken and biopsies have been obtained. Microscopically and clinically, scaling and root planing with oral hygiene was shown to be more effective in decreasing gingivitis scores, probing depths, and acquire in attachment ranges than oral hygiene alone. Hughes and Caffesse (1978) handled sixty one teeth in 15 sufferers by scaling and root planing. Clinical measurements and scores have been taken at initial exam, 1 week, and 1 month after therapy. The findings indicated that thorough scaling and root planing of teeth with severe inflammation of the gingiva is often adopted inside 1 week to 1 month after scaling by a lower in probing depth, acquire in attachment, gingival recession, and a lower in the width of the keratinized tissue. There have been no significant variations between the 2 groups except ultrasonic therapy required less time to deal with. Improvements in plaque scores, bleeding on probing, decreased probing and attachment ranges have been related for both therapy methods. It was shown that the deep probing depths presumably be} successfully handled non-surgically. Minimal impact was derived from affected person performed plaque control, whether or not supra- or subgingival. The bulk of the impact was derived from skilled subgingival instrumentation (scaling and root planing). This few studies that examines the separate effects of plaque control and that of scaling and root planing on periodontal healing. Measurements have been made each third month and seven patterns of probing attachment have been recognized. Seventy-three % (73%) of the sites confirmed a gradual lack of probing attachment. Seventeen % (17%) confirmed an early loss adopted by a stabilization in attachment degree. Scaling and Root Planing confirmed a pattern of early loss adopted by stabilization whereas deeper sites confirmed a gradual loss. Probing depth and attachment degree have been measured by 3 different examiners earlier than instrumentation and at 3, 6, and 12 months after therapy. Only 5% of all sites misplaced > 1 mm of attachment from pre-instrumentation to 12 months. The results recommend that the noticed attachment loss was either immediately attributable to instrumentation or to a remodeling process as a result of|because of|on account of} remedy rather than to progressive illness. Dentin sensitivity was evaluated with 2 forms of managed stimulations (probe and air-jet) and with a questionnaire. No modifications in pulp sensitivity have been found after scaling, but a clinically significant increase in dentin sensitivity to probe and/or air stimuli was noticed in 6 sufferers. A pure mechanism of desensitization seemed to have occurred 2 weeks after subgingival debridement. The hydraulic conductance of the foundation dentin was measured earlier than and after root planing, acid etching, and potassium oxalate application utilizing a fluid filtration methodology. The results confirmed that root planing creates a smear layer that reduces the permeability of the underlying dentin. Thus, root planing may ultimately trigger elevated dentin permeability and the associated sequelae of sensitive dentin, bacterial invasion of tubules, reduced periodontal reattachment, and pulpal irritation. Scaling and root planing effectiveness: the impact of root floor entry and operator expertise. Comparative effectiveness of ultrasonic and hand scaling for the removing of subgingival plaque and calculus. Relative effects of plaque control and instrumentation on the clinical parameters of human periodontal illness. The relative the impact of operator variability on healing following non-surgical remedy was evaluated by Badersten et al.
Cheap 135mg colospa
The decline in listening to after stapedotomy and stapedectomy has been estimated to happen at a rate of three. Short- and long-term results of stapedotomy and stapedectomy with a Teflon-wire piston prosthesis. Possible causes of an instantaneous listening to loss embrace intraoperative trauma, postoperative an infection, granuloma formation, and a perilymph fistula. Many surgeons choose to wait 1 12 months earlier than considering surgical procedure on the second ear because of this threat. In addition, some sufferers who find the listening to after surgical procedure on one ear adequate or better could adapt and select to not have surgical procedure on the second ear. If a sensorineural listening to loss has occurred, then any existing tinnitus could worsen. Preoperative preparation for this attainable complication is exceedingly essential; an inadequately knowledgeable patient who develops even a mild case of postoperative sensorineural listening to loss and tinnitus is regularly very dissatisfied. Classification Sensorineural listening to loss could outcome from damage to the hair cells caused by intense noise, viral infections, fractures of the temporal bone, meningitis, cochlear otosclerosis, Meniere disease, and getting older. The following medicine also can produce sensorineural listening to loss: ototoxic medicine (eg, salicylates, quinine, and the synthetic analogs of quinine), aminoglycoside antibiotics, loop diuretics (eg, furosemide and ethacrynic acid), and cancer chemotherapeutic agents (eg, cisplatin). One of every 1000 infants born within the United States is completely deaf, and greater than 3 million children have listening to loss. Between 30% and 35% of people over the age of 65 have a listening to loss adequate to require a listening to aid. Hearing loss can result up} from disorders of the auricle, exterior auditory canal, center ear, internal ear, or central auditory pathways. In common, lesions within the auricle, exterior auditory canal, or center ear cause conductive listening to loss. The focus of this chapter is sensorineural 683 Presbycusis, age-associated listening to loss, is the most typical cause of listening to loss in adults. More essential, the listening to loss is related to a significant loss in clarity. Genetic predisposition alone or in concert with environmental influences may also be responsible. Category Developmental and hereditary Syndromic Nonsyndromic Infectious Pharmacologic toxicity Trauma Neurologic disorders Vascular and hematologic disorders Immune disorders Bone disorders Neoplasms Unknown etiology Example ingitis as well as|in addition to} environmental components such as intrauterine teratogenic publicity or ototoxic insult had been the dominant causes of congenital and purchased listening to losses. The introduction of antibiotics and vaccines, together with improved knowledge and enhanced awareness about teratogens, has led to a decline in listening to loss ensuing from infections and environmental agents. In air conduction, sound waves attain the ear by propagating within the air, entering the exterior auditory canal, and setting the tympanic membrane in movement; the movement of the tympanic membrane, in flip, strikes the malleus, incus, and stapes of the center ear. The structures of the center ear function an impedance-matching mechanism, improving the effectivity of power switch from the air to the fluid-filled internal ear. Hearing by bone conduction happens when the sound supply, involved with the pinnacle, vibrates the bones of the cranium; this vibration produces a traveling wave within the basilar membrane of the cochlea. Cochlear neurons send fibers bilaterally to a network of auditory nuclei within the midbrain, and impulses are transmitted through the medial geniculate thalamic nuclei to the auditory cortex within the superior temporal gyri. At low frequencies, individual auditory nerve fibers can reply kind of synchronously with the stimulating tone. At greater frequencies, part locking happens in order that neurons alternate in response to particular phases of the sound wave cycle. Three issues encode the depth of sound: (1) the amount of neural activity in individual neurons, (2) the variety of neurons would possibly be} energetic, and (3) the precise neurons would possibly be} activated. Nearly two thirds of hereditary listening to impairments are nonsyndromic and the remaining one third is syndromic. In common, the listening to loss related to dominant genes has its onset in adolescence disease or trauma affecting the central auditory pathways. Mixed listening to losses are pathology that may result on} the center and internal ear simultaneously; causes embrace otosclerosis involving the ossicles and the cochlea, transverse and longitudinal temporal bone fractures, head trauma, chronic otitis media, cholesteatoma, and center ear tumors. Furthermore, two frame-shift mutations, 35delG and 167delT, account for greater than 50% of the cases making population screening possible. In addition, the listening to loss could be variable among the members of the identical household, suggesting that other genes probably affect the auditory phenotype. The contribution of genetics to presbycusis or age-associated listening to loss additionally be|can be} better understood. Several of the nonsyndromic genes are related to listening to loss that progresses with age. Presbycusis is characterised by a loss of discrimination for phonemes, recruitment (abnormal progress of loudness), and particular difficulty in understanding speech in noisy environments. As a direct results of the speedy advances within the fields of molecular biology and molecular genetics, the responsible genes for the aforementioned syndromes have all been recognized. In addition, speedy progress in understanding the basis of these and related disorders has revealed a number of|numerous|a selection of} complexities. For example, identification of myosin 7A because the responsible gene for each syndromic and nonsyndromic deafness has led to the abandonment of the "one gene, one disease" dogma. Also, a single gene could cause syndromic or nonsyndromic types of deafness or may be be} related to autosomal dominant or autosomal recessive mode of inheritance. In addition, cautious monitoring of serum peak-and-trough ranges can largely prevent the loss of vestibular operate and deafness aminoglycoside antibiotics. Noise-induced listening to loss could be prevented by avoiding publicity to loud noise or by the regular use of earplugs or fluid-filled muffs to attenuate intense sound. Noise-induced listening to loss results from recreational as well as|in addition to} occupational actions and sometimes begins in adolescence. High-risk activities-High-risk actions for noiseinduced listening to loss embrace wood- and metalworking with electrical tools as well as|in addition to} target practice and hunting with small firearms. All internal-combustion and electric engines, including snowblowers and leaf blowers, snowmobiles, outboard motors, and chain saws, require that the consumer put on listening to protectors. Education-Almost all noise-induced listening to loss is preventable through schooling, which ought to start earlier than adolescence. Industrial packages of listening to conservation are required when the publicity over an 8hour period averages 85 dB on the A scale. Workers in such noisy environments could be protected with preemployment audiologic evaluation, the obligatory use of listening to protectors, and annual audiologic assessments. The historical past ought to elicit listening to loss traits, including the period of deafness, the nature of the onset (sudden or insidious), the rate of development (rapid or slow), and the involvement of the ear (unilateral or bilateral). In addition, the presence or absence of the following situations wants to|must also} be ascertained: tinnitus, vertigo, imbalance, aural fullness, otorrhea, headache, facial nerve dysfunction, and head Prevention A. Information concerning head trauma, ototoxic publicity, occupational or recreational noise publicity, and a household historical past of listening to impairment additionally may be be} crucial within the differential diagnosis. Sudden onset-A sudden onset of unilateral listening to loss, with or with out tinnitus, could characterize an internal ear viral an infection or a vascular accident. Patients with unilateral listening to loss (sensory or conductive) usually complain of decreased listening to, poor sound localization, and difficulty listening to clearly with background noise. Gradual progression-Gradual development in a listening to deficit is frequent with otosclerosis, noiseinduced listening to loss, vestibular schwannoma, or Meniere disease. People with small vestibular schwannomas sometimes current with any or all of the following situations: uneven listening to impairment, tinnitus, and imbalance (although rarely vertigo). Cranial neuropathy, particularly of the trigeminal or facial nerve, could accompany larger tumors. In addition to listening to loss, Meniere disease or endolymphatic hydrops may be be} related to episodic vertigo, tinnitus, and aural fullness. Hearing loss with otorrhea is most probably chronic otitis media or cholesteatoma. Family history-In families with a number of} affected members across a number of} generations, the household historical past may be be} essential in delineating the genetic basis of listening to impairment. The historical past may also assist establish environmental threat components that lead to listening to impairment within a household. Sensitivity to aminoglycoside maternally transmitted through a mitochondrial mutation could be discerned through a cautious household historical past. Susceptibility to noise-induced listening to loss or agerelated listening to loss (presbycusis) may also be genetically determined. Evaluation with a tuning fork-Evaluating listening to with a tuning fork useful medical screening tool to differentiate between conductive and sensorineural listening to loss.
Quality 135 mg colospa
This entity is totally described later in this chapter under Perilymphatic Fistula). This approach is used for facial nerve exploration in patients with regular listening to. The middle fossa exposure permits visualization of the nerve from the brainstem to the geniculate ganglion, whereas the transmastoid route exposes the nerve from the geniculate ganglion to the stylomastoid foramen. In this instance, an interpositional facial nerve graft has been placed throughout the vertical section of the facial nerve. This approach permits for full exposure of the facial nerve from the porous acousticus to the stylomastoid foramen completely through the mastoid. If an intraneural hematoma is recognized, the epineurium should be fastidiously opened and the hematoma evacuated. If bony fragments are impinging upon the nerve, these may be fastidiously eliminated as properly. If the section of missing nerve is just too|is simply too} long to be easily anastomosed without tension, an interposition nerve graft should be used from the higher auricular or sural nerve. If no pathology is visualized, the act of opening the bony canal of the facial nerve ought to allow sufficient decompression and allow swelling of the nerve without impingement. This approach is used for facial nerve exploration in patients with full sensorineural listening to loss and permits full exposure of the nerve through one opening. The most common organisms that cause meningitis in this state of affairs are Pneumococcus, Staphylococcus, Streptococcus, and Haemophilus influenzae. In a patient with no useful listening to, obliteration of the ear with an belly fats graft, plugging of the eustachian tube, and closure of the ear canal may be carried out through the mastoid alone. Management of facial paralysis resulting from temporal bone fractures: our experience in one hundred fifteen instances. Repair of iatrogenic temporal lobe encephalocele after canal wall down mastoidectomy within the presence of energetic cholesteatoma. There is usually vital damage to the exterior auditory canal, which requires native debridement of bone fragments and gentle tissue, stenting with Merocel wicks (a type of expandable, nonabsorbable sponge) to forestall stenosis. Tympanic membrane perforation, ossicular discontinuity, and labyrinthine fracture are additionally widespread entities with a gunshot wound to the temporal bone. Epithelial components may be launched into the mastoid or middle ear cavities and not be detected as a cholesteatoma until years later. This both following a temporal bone fracture involving the otic capsule or with stapes subluxation into the oval window. Barotrauma throughout scuba diving, a speedy descent in an airplane, an explosion, or straining throughout a troublesome childbirth may cause a perilymphatic fistula. Poor surgical technique whereas performing a mastoidectomy can result in an iatrogenic lateral canal fistula. In addition, an expanding cholesteatoma can erode into the lateral semicircular canal or cochlea, causing a fistula. Vascular Injury the most important aspect of penetrating trauma to the temporal bone is the potential for damage to the internal carotid artery, inside jugular vein, or dural sinuses. Angiography should be carried out on all patients, with embolization or balloon occlusion used to management bleeding from the skull base. In the occasion that inside carotid artery laceration is found, Fogarty catheters can be utilized briefly to management bleeding. They may have tinnitus and listening to loss, headache, and, occasionally, aural fullness. Most important, signs turn out to be much worse with any type of Valsalva maneuver, similar to coughing, sneezing, or straining. Occasionally, an altitude change, similar to going up and down in an airplane or in an elevator, can precipitate signs. Patients typically complain of Tullio phenomenon, whereby loud noises precipitate a vertiginous assault. Clinically, the fistula check may be carried out by insufflating air into the exterior auditory canal and observing the patient for evidence of nystagmus. This check may be very insensitive and is optimistic in solely about 50% of patients with a fistula. Facial Nerve Injury the speed of facial nerve paralysis with penetrating trauma to the temporal bone is 36%. Essentially all of these injuries are of quick onset and occur due to nerve transection. Facial nerve electrophysiologic testing with a Hilger stimulator can be utilized to identify facial nerve trauma in a comatose patient. Facial nerve repair needs to be undertaken as soon because the patient is medically secure. The solely definitive approach to make the analysis of a perilymphatic fistula is surgical exploration with visualization of the leak. Patients are placed on stool softeners and serial audiograms should be obtained to observe up for evidence of illness development. If signs persist or the sensorineural listening to loss worsens, surgical remedy considered. This is finished by a transcanal approach with elevation of the tympanomeatal flap and cautious examination of the oval and round windows. Case data of the Massachusetts General Hospital: weekly clinicopathological exercises. Case 40-2001: an eight-year-old boy with fever, headache, and vertigo two days after aural trauma. First scientific experience with beta-trace protein (prostaglandin D synthase) as a marker for perilymphatic fistula. Outcome of listening to and vertigo after surgery for congenital perilymphatic fistula in kids. Nystagmus elicited by straining may be documented utilizing electronystagmography monitoring and then evaluated. Differential Diagnosis the differential analysis includes all causes of dysequilibrium, most notably Meniere illness, cervical vertigo, psychogenic vertigo, disequilibrium related to aging (presbyastasis), vestibular neuritis, and labyrinthitis. Complications Fluctuating, but progressive, sensorineural or mixed listening to loss can occur. The otolaryngologist�head and neck surgeon involved within the multidisciplinary team that approaches this space will necessarily have an in-depth data of surgical anatomy and tumor pathology, familiarity with radiologic evaluation and the roles of interventional radiology, and experience with the various surgical approaches which have been used to access this space. Most of the issues the surgical team encounters in anterior skull base surgery are both malignant tumors of the paranasal sinuses that stretch superiorly to involve the anterior skull base, or benign or malignant processes similar to meningiomas, which prolong inferiorly from above. In addition, benign lesions of the paranasal sinuses, similar to in depth inverted papillomas, in depth mucoceles, and selected benign fibro-osseous lesions, occasionally require these approaches to skull base surgery. It includes the posterior wall of the frontal sinus, the ethmoid roof and cribriform plate, and the orbital roof. More posteriorly, it includes elements of the sphenoid bone, together with the lesser wing of the sphenoid, the planum sphenoidale, and the roof of the sphenoid sinus. The significance of this layer is that the orbit is mostly in a position to} be preserved if the extraocular muscles, that are inside this fascial aircraft, are uninvolved. The precise invasion of orbit fats deep to this fascial aircraft often suggests the need for orbital exenteration. The significance of this anatomy is that dissection of the medial floor of the optic nerves to the optic chiasm is mostly secure with respect to its blood provide. The optic nerve (and ophthalmic artery) borders the posterior ethmoidal air cells in about 10�15% of instances. Although 30% of the sixty six reviewed instances recurred domestically, this was on the web site of the initial orbit involvement in solely 8% of these instances. Preserving this layer permits 753 Copyright � 2008 by the McGraw-Hill Companies, Inc. Studies of the anatomy and pathology of the orbit in carcinoma of the maxillary sinus and their impression on preservation of the eye in maxillectomy. Sometimes, for instance, tumor has eroded bone such that a particular approach turns into best. Although the sphenoid sinus septum is often midline anteriorly on the sphenoid rostrum, it virtually all the time deviates laterally as it programs posteriorly. In addition, further septa throughout the sphenoid sinus are widespread and may confuse an unwary surgeon. Intraoperative navigation may be useful in order that the surgeon can positive that|ensure that|make sure that} the lateral restrict of the sphenoid sinus has been accessed.
Trusted 135mg colospa
Muscular triangle-The muscular triangle is bounded by the omohyoid muscle above, the sternocleidomastoid muscle beneath, and the midline of the neck in entrance. Deep to these muscular tissues are the thyroid and parathyroid glands, the larynx, outcomes in|which finally ends up in} the trachea, and the esophagus. It is continuous with the larynx by way of the laryngeal aditus, which is shaped by the epiglottis and the aryepiglottic folds. On both facet of those folds and medial to the thyroid cartilage are two pyramidal areas, the piriform recesses of the laryngopharynx, by way of which swallowed meals passes into the esophagus. The piriform recesses are related to the cricothyroid muscle laterally and the lateral cricoarytenoid muscle medially. The floor markings of those muscular tissues help to visibly outline the borders of the triangles of the neck. It is split by the omohyoid muscle into an occipital triangle and a supraclavicular triangle. Occipital triangle-The occipital triangle has a muscular ground shaped from above, downward by the semispinalis capitis, splenius capitis, levator scapulae, and scalenus medius muscular tissues. The brachiocephalic artery branches into the best subclavian and proper frequent carotid arteries. Acting independently, every muscle turns the head to face upward and to the contralateral facet. By virtue of their attachment to the sternum, the sternocleidomastoids also serve as accessory muscular tissues of respiration. Vertebral artery-The vertebral artery courses up by way of the transverse foramina of the higher six cervical vertebrae. It enters the vertebral canal, passes by way of the foramen magnum, and goes on to provide blood to the hindbrain, the midbrain, and the occipital lobe of the forebrain. Internal thoracic artery-The inside thoracic artery leaves the root of the neck and passes into the thorax, the place it supplies blood to the anterior chest wall and ultimately to the higher half of} the anterior abdominal wall by way of its superior epigastric branch. Thyrocervical trunk-The thyrocervical trunk gives off the following branches: (1) the inferior thyroid artery, which supplies blood to the thyroid gland; (2) the transverse cervical artery, which passes backward across the neck to provide blood to the trapezius and rhomboid muscular tissues; and (3) the suprascapular artery, which courses laterally across the neck towards the suprascapular notch and participates in the elaborate anastomosis of vessels that encompass the scapula. The inferior thyroid artery has a branch, the inferior laryngeal artery, which enters the larynx by passing between the lowest fibers of the inferior pharyngeal constrictor muscle and the higher fibers of the round muscle of the esophagus. The inferior thyroid artery anastomoses with the superior thyroid artery, a branch of the exterior carotid artery. Costocervical trunk-The costocervical trunk gives off branches that offer blood to the first two intercostal areas and the postvertebral muscular tissues of the neck. The uppermost fibers move downward from the cranium to the lateral end of the clavicle, thereby playing in} a role in elevating the shoulder. The center fibers move laterally from the cervical backbone to the acromion strategy of the scapula and help to retract the shoulder. The lowest fibers move upward from the thoracic backbone to the backbone of the scapula and help to laterally rotate the scapula, making the glenoid fossa turn upward. This motion assists the serratus anterior muscle in rotating the scapula when the arm is kidnapped overhead. They are contained throughout the prevertebral layer of deep fascia and help to laterally bend the cervical backbone. The roots of the brachial plexus and the subclavian artery move between the anterior and center scalene muscular tissues on their course to the axilla. In contrast, the subclavian vein passes anterior to the anterior scalene muscle because it leaves the neck to move behind the clavicle and attain the axilla. Also, the phrenic nerve lies immediately anterior to the anterior scalene muscle because it runs down the neck into the thorax. Together, they act to depress the hyoid bone and the thyroid cartilage during actions of swallowing and speech. Internal carotid artery-The inside carotid artery also has no branches in the neck. It travels up to as} the bottom of the cranium, the place it enters the carotid canal and passes by way of the petrous half of} the temporal bone and the cavernous sinus earlier than turning sharply upward and backward at the carotid siphon to pierce the dura mater. In addition, with the infrahyoid muscular tissues holding the hyoid bone in place, the suprahyoid muscular tissues help to depress the mandible and open the mouth. Its primary branch to the head is the ophthalmic artery, which supplies blood to the orbit and the higher half of} the nasal cavity. External carotid artery-The exterior carotid artery is the primary supply of blood provide to the head and neck (see Figure 1�1). Superior thyroid artery-The superior thyroid artery passes method down to} provide blood to the higher half of} the thyroid gland. It has a branch, the superior laryngeal artery, which pierces the thyrohyoid membrane to move into the larynx. The superior thyroid artery anastomoses with the inferior thyroid artery, a branch of the thyrocervical trunk of the subclavian artery. Ascending pharyngeal artery-The ascending pharyngeal artery supplies blood to the pharynx. Posterior auricular artery-The posterior auricular artery passes upward, behind the auricle, and supplies blood to the scalp. Occipital artery-The occipital artery passes upward and backward to provide blood to the scalp on the again of the head. Facial artery-The facial artery passes upward and forward, deep to the submandibular salivary gland. It then crosses the mandible, the place its pulsations may be palpated simply in entrance of the masseter muscle, to provide blood to the face. Lingual artery-The lingual artery passes upward and forward, behind the posterior edge of the hyoglossus muscle, and into the substance of the tongue, to which it supplies blood. Terminal branches-The exterior carotid artery then ascends into the substance of the parotid gland, the place it gives off two terminal branches. At the angle of the mandible, the retromandibular vein divides into an anterior and a posterior division. In addition, the suprascapular and transverse cervical veins drain into the exterior jugular vein. The inside jugular vein drains blood from the areas to which the inner carotid artery supplies blood. Lymphatics the superficial lymph nodes of the head and neck are named for their regional location. The occipital, retroauricular, and parotid nodes drain lymph from the scalp, auricle, and center ear. The retropharyngeal nodes, although not really superficially located, obtain lymph from deeper constructions of the head, including the higher parts of the pharynx. All of those regional nodes drain their lymphatic efferents into the deep cervical nodes, which lie along the inner jugular vein. Two of those deep nodes are commonly referred to as the jugulodigastric and the juguloomohyoid nodes. They lie at areas at which the inner jugular vein is crossed by the digastric and omohyoid muscular tissues, respectively. The jugulodigastric node is concerned with the lymphatic drainage of the palatine tonsil; the juguloomohyoid node is concerned Veins the venous drainage of the head and neck is best understood by evaluating it with the arterial distribution described above. Many variations exist in the sample of venous drainage, but every of the arteries has a vein that corresponds to it. The deep cervical nodes drain their lymph into both the thoracic duct or the best lymphatic duct. The thoracic duct empties into the junction of the left inside jugular vein and the left subclavian vein. The proper lymphatic duct drains into a similar location on the best facet of the root of the neck. The cutaneous branches of the cervical plexus emerge from simply behind the sternocleidomastoid muscle, about midway between its attachments to the sternum and the mastoid process. Transverse cervical nerve-The transverse cervical nerve turns forward and courses across the neck, with its branches carrying sensation from the anterior neck. Supraclavicular nerves-The supraclavicular nerves course down towards the clavicle and carry sensation from the skin of the lower neck, extending from the clavicle in entrance to the backbone of the scapula behind. Greater auricular nerve-The greater auricular nerve courses up towards the auricle, with its branches carrying sensation from the skin of the higher neck, the skin overlying the parotid gland, and the auricle itself.
Colospa 135 mg
The term Nasya, within the specific sense, is especially used as regards to the snuffing of any broadly divided into two varieties, (errhines) and;. Sneha (oleaginous substance) with a view the poor oily to make up matter within the brain within the case of to the nerves a affected person complaining of a way of void or emptiness within the head or to impart tone and muscles the of the neck, shoulders and chest, or to invigorate eye-sight. Gayi reads preit is t Sifikantha Datta, commentator of Vrinda, says that fljf f^^iT? Then be of his the the neck, cheek and brow ought to fomented and palms, a softened with the appliance affected person himself being laid heated the on back in dustless chamber not exposed head ought to be saved a to little the solar and the wind. Doses of a Sneha-Nasya;- Eight of oil trickling fingers drops down be the two upper phalanges of the fore- ought to (lit. Metrical Text;- An oily snuff (Sneha-Nasya) in ought to be hawked so as to circulate along the girths (Sringcitaka) of the nostrils and instantly spit out (by the patient), without retaining it within the moment, branes as it may in any other case throat, and so on. A is case cation (of a Sneha-Nasya) marked by the and derangements (Rukshatd) of of the sense-organs* a dryness the system without any indication of within the amelioration of the disease. The treatment, such circumstances, consists in a contemporary utility of the (oleaginous) snuff. The proper doses with the energy (of of an oleaginous errhine (Siro- Vireka) ought to be 4, six or eight drops in accordance the disease and of the affected person under treatment), 27. The head being (by the passable utility (of an oleaginous is errhine) marked by a way channels (of of lightness within the head, clearness of the the mouth, throat, nostrils, and so on. A dis- charge via the nostrils of Mastulunga (the brain matter), an aggravation of the Vdyu, dulness of the or sense-organs and a way of void emptiness within the head are the indications which mark an excessive utility of un (oleaginous) errhine. Measures and cures possessed of the advantage of (re- subduing the deranged Kapha and Vdyu ought to be spectively) employed in circumstances of excessive and poor applications of (an oleaginous) errhine (Nasya), whereas within the case of a proper and affected person ought to be passable utility the made to snuff in a quantity of clarified butter on each alternate for one, day or at an interval of two days two or three weeks in succession or for any longer interval as thought of proper based on the exigency of the case. In a case of an awesome aggravation of the Vayu, the affected person clarified butter) additionally be} made to use the snuff (of 29. An Avpida-Nasya ought to be administered to a affected person by pasting any of the (fresh) Siro-Virechana medication and placing a few of} drops therefrom into the nostrils of the affected person. In circumstances of a distraction parasitic origin or of pf the mind or of a disease of a Chap. Sugar, the expressed juice of the sugar-cane, milk, clarified butter or an extract of meat ought to be (similarly) case of a administered within the weak affected person or of 1 30. Metrical Texts;- A Sneha butter) or clarified cooked with the pasted medication (of the Siro-Vire- chana group) respect affected person. Pratimarsha Nasya when to be used -The Pratimarsha form of snuff ought to be; resorted to on any of the following fourteen different events, z;f>. Their Effects;- A the Pratimarsha snuff utilized by within the nostrils a person simply after rising from his mattress tends to remove waxy mucus (Mala) accumulated through the night time and brings on a cheerful state of the mind, when used after having cleansed the tooth, it imparts a sweet aroma to the mouth and makes the tooth regular and When utilized by a person on the agency (in their sockets). When used exertion it after the of physical train, to coition or a journey, fatigue, it serves remove the after sense of consequent or defecation of vision, and when used micturition tends to remove the dulness or heaviness When the utilized after gargling or after an utility of collyrium (along the eyelids) it serves to invigorate eye-sight. When taken after a day-sleep tends to remove the sense of drowsiness and physical heaviness nostril, and so on. Metrical Texts;- the which, being frivolously snuffed in, quantity of Sneha down into the cavity of the mouth, ought to be deemed enough for a dose of the Pratimarsha (kind of snuff*). The benefit reaches of using a snuff as it may be perceived in a variety of|quite lots of|a wide selection of} ways, tends to remedy the ailments peculiar to the super- clavicular regions of the body, removes the cloudening * One drop or two, is or the quantity necessary to deliver about a in accordance disruption of the Doshas, to Vriddha-Vagabhata. Specific use of snuff ought to encompass oil in Sncha-Nasya;- this a case certed actions of the deranged) it marked by (the conKapha and Vdyu, whereas case involving the ought to encompass Vasfik (lard) in a action of the V^yu alone. Similarly clarified butter ought to be used as a snuff in a case of a Pittaja dysfunction, whereas the snuff ought to case encompass Majja((marrow) in a marked by Pitta. An amelioration of the disease, a way of lightness and of purity within the mouth, a cheerful mind set and an exhilarating vigour within the organs of sense are the features which mark an act of perfect or passable gargling (Kavala), whereas a way of physical lassitude, salivation and a (consequent) defect within the sense of style are the traits Thirst, an aversion which mark poor gargling. The strategy of using medicinal gargles (Kavala) in general have thus been briefly described. Pratisdrana treatment 671 Pratisdrana;- A Rasa-kriyi^, honey and additionally be} of 4 varieties, viz. Prepared with the suitable medication, such a compound ought to be rubbed gently with the tip of a finger in a case of an affection of the mouth. The signs of a satisfac- tory or unsatisfactory Pratisdrana ought to be respectively identical with those of a Kavala. Thus ends the Fortieth Chapter Susruta Samhita which deals snufTs, Chikitsita Sthinam within the with the inhalation of medicinal fumes, and gargles. Powerful enemies and tions of the sovereign in a selves even the servants and relafit of anger to avenge them- on the sovereign typically concoct poisonous to him, highly effective compounds and administer the identical though he may in weak point by taking advantage of|benefiting from|profiting from} any defect or Sometimes the women (of the royal him. The minds like of males are stressed and uncontrollable uncommon thing within the an unbroken horse. He ought to come of a respect- family, to of ought to be virtuous in conduct, fondly connected the particular person of his sovereign, and always ought to watchful greedless, the well being of the king. He be of straight-forward, features, god-fearing, grateful, irascibility, handsome ness, and devoid of rough- self-importance, vanity and laziness. He ought to be forbearing, self-controlled, cleanly, compassionate, well- behaved, clever, able to bearing fatigue, well- which means, devoted, of good handle, intelligent, all skilful, good, artless, energetic and marked with the neces- sary skills (of a doctor; as described earlier than. He ought to be fully provided with all kinds of medicine and be highly esteemed by the members of his occupation. The * vessels and utensils (to be utilized in a royal kitchen) ought to be saved scrupulously clean. The Fire-god ought to be (daily) the pinnacle or managar of the royal skills cooks ought to generally possess the identical as those of a doctor. The bearers and cooks within the royal kitchen ought to have their nails and hair clipped off and should bear turbans. They ought to be composed cleanly, civil, intelligent, obedient, good-looking, each charged with separate duties, good-tempered, of their behaviour, well-bathed, greedless, decided, and prompt in executing the orders of their superiors. A doctor of the royal kitehen ought to be very cautious duties, and circumspect food is within the discharge life, of his because the that} the protected and the sole real} contributor to continuance of the body. Every one employed corresponding to, major keep of in a royal kitchen bearers, servers, cooks, soup- makers, cake-makers (confectioners), ought to be placed under the direct management and supervision of the doctor of the kitchen. He is found abruptly and listlessly to press the joints of his fingers or to scratch the earth, to laugh and to shiver. He will look frightened on the sight of others (indifferently), nails, and can cut (straw or hay) with his finger- and his color modifications constantly. He will scratch his head in an agonised and confused state, and can look this fashion and 7. An innocent man, unjustly arraigned earlier than the royal tribunal might from concern or precipation, turn out to be (confused and) liable to make unfaithful statements (and thus be Hence the king ought to start with|to start with} unjustly convicted). A ready the royal use ought to be given to crows and ought to be presumed, and so they its poisonous character instantaneously die on partaking of the identical. A swan and a Bhringarjija (of the swallow (a species A Prishata of noticed deer) sheds birds tears and a monkey passes stools. Hence these within the royal palace for and animals ought to be saved show and leisure as Veil lO. The vapours arising from poisoned food when served and pro- for use give rise to a ache within the cardiac area duce headache and restlessness of the eyes. As an antidote, a preparation of Kushtha, Rdmatha (asafcetida), Nalada and honey combined together ought to be used as an Anjana (along the eye-lids) and a medical compound of the identical medication ought to be snuffed into the nostrils. A poison affecting the palms of the hands, produces a burning sensation in them of the finger-nails. The measures and cures already laid reference to the remedy of circumstances of poisonous vapours nicely as|in addition to} those to be hereinafter in in down described reference to the 13. Food combined with poison, when it reaches the Amasaya (stomach), gives rise to epileptic matches, vomiting, dysenteric stools (Atis^ra), distention of the stomach, a burning sensation, the sense-organs. Food combined with ^aya the body), epileptic poison, if it reaches the Pakvd(in (intestines), gives rise to a matches, burning sensation dysenteric stools (Atisdra), derangements of the organs of sense-perception, rumbling sounds within the stomach and emaciation, and makes of first the complexion purgative fruits (of the sufferer) yellow. As an (in alternative, cures to be described lateron within the subsequent chapter) reference to the effects of Dushi-Visha (slow chemical poison) ought to be adopted and used, saturated with milk-curd (Dadhi) or honey. Ripe fruit, under such situations, speedily decomposed to and the unripe ones are found ripe. If the tooth-twig be is anyway charged with poison and shattered and if its brush-like end gives rise to withered used a swelling of the lips and the tongue and In such a case, the swollen part ought to fibre) in regards to the gums. Symptoms clothes, armour, bedding, beauty, washes, infusions, anointments, and so on. A poisoned plaster (if utilized to the head) leads to the falling off of the hair and to violent headache, bleeding via the mouth and the ance of glands on the pinnacle.
References:
- https://www.omicsonline.org/open-access-pdfs/alternative-treatment-for-psoriasis--a-review-.pdf
- https://nasemso.org/wp-content/uploads/neuro-epworthsleepscale.pdf
- https://effectivehealthcare.ahrq.gov/sites/default/files/cancer-horizon-scan-high-impact-1406.pdf
- https://law.resource.org/pub/us/cfr/ibr/001/acgih.manual.1998.pdf
- https://www.mass.gov/files/documents/2016/07/tp/surveill-report-02-03.pdf