.png)
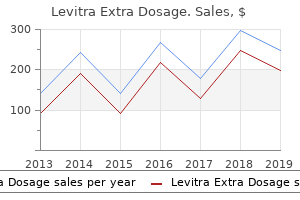
Buy levitra extra dosage 60mg
Criteria for both treatment and prognosis are affected by the presence of goal organ disease. Pre-treatment laboratory checks can be restricted to these usually carried out as a part of a routine medical checkup analysis: complete blood rely; urinalysis; serum potassium, sodium, and creatinine levels; fasting blood glucose; low- and high-density lipoprotein cholesterol levels; and a 12-lead electrocardiogram. These checks assist assess the presence and severity of goal organ disease and other cardiovascular risk components and can be used as a baseline for monitoring the effects of antihypertensive treatment. Serial electrocardiograms and echocardiograms (see Chapters 42 and forty three) might assist assess the effects of hypertension and antihypertensive treatment on the center, however their scientific utility in managing an individual affected person is unclear. Consensus tips stratify hypertensive patients into risk groups for therapeutic choices (Table 55-5) (Table Not Available). For these with stage 2 or stage three hypertension, immediate drug remedy is warranted. If a number of risk components are current, immediate drug remedy should be thought-about. Lifestyle modification and administration of reversible risk components should accompany drug treatment. This concern appears to be most related to hypertensive patients with pre-existing coronary artery disease and to these with a pulse pressure larger than 60 mm Hg. Beneficial results include protection from stroke, coronary occasions, coronary heart failure, development of renal disease, development to more extreme hypertension, and most importantly, all-trigger mortality. The benefits of antihypertensive treatment in aged patients are even larger than the benefits in youthful patients. A meta-evaluation of thirteen randomized scientific trials with sixteen,000 individuals 60 years of age and older confirmed that forty three individuals needed to be handled for five years to prevent one stroke and 61 individuals needed to be handled for five years to prevent one coronary occasion. Only 18 individuals needed to be handled to prevent one cardiovascular (cerebrovascular or cardiac) occasion. Furthermore, solely 15 individuals with isolated systolic hypertension needed to be handled for five years to prevent a cardiovascular occasion. Comparison with 12 trials involving 33,000 center-aged and youthful hypertensive individuals revealed that for all outcomes besides cardiac mortality, two to four occasions as many youthful as older individuals needed to be handled for five years to prevent morbid and mortal cardiovascular occasions. Therapy should be tailor-made to the person characteristics of every affected person, similar to weight discount and exercise for an obese affected person and moderation in alcohol consumption for a heavy drinker. A reasonable generalized method for all patients contains (1) reduced dietary sodium and elevated calcium and potassium from food sources, (2) weight loss for obese patients, (three) common bodily exercise, (4) moderation of alcohol consumption, and (5) smoking cessation. The same lifestyle modification strategies which are efficient in treating hypertensive patients may be useful within the main prevention of important hypertension. This effect is impartial of dietary sodium restriction and is seen in both obese and non-obese hypertensive individuals. Moreover, the appetite suppressant medication fenfluramine and phentermine have been withdrawn from the market because of cardiovascular toxicity, together with severe mitral, aortic, and tricuspid regurgitant lesions and, not often, pulmonary hypertension. Weight discount via a combination of dietary caloric restriction and elevated bodily exercise is really helpful for all obese hypertensive individuals. Additional benefits of standard bodily exercise include weight loss, enhanced sense of nicely-being, improved practical health standing, and reduced risk of heart problems and all-trigger mortality. Accordingly, common aerobic bodily exercise is really helpful for all hypertensive individuals, together with these with goal organ damage. Patients with superior or unstable heart problems might require medical analysis earlier than initiation of exercise or a medically supervised exercise program. Furthermore, excessive alcohol consumption appears to trigger resistance to antihypertensive remedy. Moderate alcohol consumption might cut back general cardiovascular risk within the basic inhabitants, however whether any risk discount also occurs within the hypertensive inhabitants is uncertain. An observational study of a big cohort of hypertensive individuals, all of whom were advised to restrict their sodium consumption, confirmed that males within the lowest quartile of sodium excretion had a four-fold larger risk of coronary heart assault than did these within the highest quartile. This observation, as but unconfirmed in potential, managed trials, raises the likelihood that sodium restriction could also be dangerous for some hypertensive individuals. Moderate sodium restriction (4 to 6 g of salt per day) can usually be really helpful to hypertensive patients, with the belief that solely a subset will benefit. Such sodium restriction can be completed by not adding salt to food throughout preparation or on the desk and avoiding processed foods containing salt as the preservative. Furthermore, seventy five to ninety% of adults within the United States fail to consume the really helpful day by day allowance of calcium (a thousand mg for adults youthful than 65 years; 1500 mg for adults older than 65 years). Maintaining the really helpful calcium consumption, ideally from food sources, is also beneficial for preventing osteoporosis and perhaps gastrointestinal malignancy. Hypertensive patients should keep enough potassium consumption (50 to ninety mmol/day) by eating contemporary fruit and veggies. Potassium supplementation should be avoided or used solely with extreme warning in patients with renal insufficiency, in diabetics, and in patients receiving potassium-sparing diuretics. Hypokalemia should be particularly avoided in patients receiving digoxin and in patients with known coronary artery disease inasmuch as it predisposes to arrhythmia. Furthermore, modifications in or discontinuance of treatment is frequent: several large studies of hypertensive patients have proven that 50 to 70% of recent remedies were changed or discontinued within the first 6 months. Non-adherence to prescribed remedy is a serious problem within the administration of hypertensive patients, and maximizing adherence is more important than selecting a particular drug routine. Clues to non-compliance include regularly missed appointments, failure to manifest the expected biologic results of prescription drugs similar to coronary heart rate slowing with beta-adrenergic blockers, and alcohol and substance abuse. The establishment of a great relationship with the affected person and free and open communication about hypertension, its issues, 266 and the targets and pitfalls of treatment are important in enhancing compliance. The initial selection of antihypertensive drug treatment is a topic of great curiosity and controversy for a wide range of causes, together with the development of recent medication with actual or perceived benefits over existing agents, cost points, the lack of morbidity and mortality data for the newer agents, and a paucity of information comparing the efficacy and tolerability of agents from completely different courses. In the Captopril Prevention Project, captopril and traditional antihypertensive remedy with diuretics or beta-blockers had related efficacies in preventing cardiovascular morbidity and mortality in practically eleven,000 randomized patients. Neither study had the ability to evaluate the effects of the remedies on cardiovascular outcomes. Clinical trials in progress around the world, with a projected affected person enrollment of 200,000, are addressing this problem. Current data point out that quick-acting dihydropyridine calcium channel blockers are related to an elevated risk of opposed cardiovascular outcomes when compared with other drugs and should be avoided. For the minority of hypertensive patients without co-morbid conditions, goal organ damage, or concomitant cardiovascular risk components, drug remedy should begin with a diuretic or a beta-blocker (see. For most patients, nevertheless, co-morbid conditions might dictate the selection of one other class of drug and/or avoidance of diuretics and beta-blockers for initial remedy (see. For patients with coexistent diabetes mellitus or heart problems, randomized managed trials have provided compelling indications for initial drug decisions from particular drug courses. When monotherapy is unsuccessful, a second agent, usually of a special class, should be added. Recommended dose ranges for individual medication are listed in Table 55-8 (see Table 55-7 for dose ranges for combination agents); frequent opposed results are summarized in Table 55-9. Re-analysis for secondary causes of hypertension and possible referral to a hypertension specialist are indicated. Doses should be titrated slowly downward and drugs discontinued separately, if possible. Clues from the medical historical past, bodily examination, initial laboratory analysis and scientific course assist establish the 5% of hypertensive patients with particular causes for the dysfunction (see Table 55-three. Patients with the more frequent and treatable forms of secondary hypertension share the characteristics outlined in Figure 55-6. The indicators, signs, and bodily and laboratory findings that time to a particular secondary etiology for hypertension might appear as a part of the initial analysis or might emerge in the midst of comply with-up, especially in conjunction with a disappointing response to ordinary medical remedy. Renovascular disease is the commonest (1 to 2%) cause of curable/treatable secondary hypertension. Any lesion that obstructs either large or small renal arteries could cause renovascular hypertension. The commonest and clinically important of those are intrinsic lesions of the massive vessels (see Chapter 112) as a result of they are often physically handled and the hypertension either cured or ameliorated. Of patients with renovascular hypertension, atherosclerotic disease is found in seventy five% general and in practically all aged patients, whereas fibrous or fibromuscular disease is found in 25%, together with the overwhelming majority of youthful patients. The usefulness of screening checks for renovascular hypertension is extremely variable, so patients should be referred to high-volume centers for testing. Patients more than likely to have renovascular hypertension include these with hypertension of abrupt onset, especially within the young or in late center-aged or aged patients; these with malignant hypertension or sudden acceleration of benign hypertension; and those that fail to reply to medical remedy. A definitive prognosis of renal artery stenosis is made by selective renal angiography, which defines the anatomy of the stenotic renal artery and hence provides data needed to plan the method to revascularization.
Purchase 100 mg levitra extra dosage
Atropine, in doses much like these given within the prehospital phase, may increase blood pressure if hypotension displays bradycardia or extra vagal tone. High concentrations could also be counterproductive due to vasoconstriction and lack of augmented myocardial oxygen delivery in normoxemic sufferers. Patients requiring mechanical air flow require special measures (see Chapter ninety three). Lower-threat sufferers with out apparent ischemia ought to be noticed and monitored in both a step-down/intermediate care unit or a chest pain analysis/statement unit (see above). Alternatives for coronary recanalization embrace intravenous thrombolytic agents or catheter-based approaches. Thrombolysis could be accomplished with a variety of intravenous medications and regimens (see Chapter 188), with or with out the use of adjunctive therapies. Catheter-based approaches also avoid the risk of bleeding, including intracerebral bleeding, seen with thrombolytic medications. It is clearly the treatment of selection in sufferers with contraindications to thrombolytic agents (see beneath). First-generation drugs invariably elicit a systemic lytic state characterized by depletion of circulating fibrinogen, plasminogen, and hemostatic proteins, and by marked elevation of concentrations of fibrinogen degradation merchandise in plasma. In optimum regimens, they induce clot lysis with out inducing a systemic lytic state, are much less vulnerable to predispose to hemorrhage that requires transfusion compared with non-clot-selective agents, and are efficient in inducing recanalization in 80 to ninety% of infarct-associated arteries within ninety minutes. The risks of coronary thrombolysis embrace bleeding, a lot of which is confined to websites of vascular entry. Marked depletion of fibrinogen or prolongation of the bleeding time could also be markers of pharmacologic results that lead to bleeding. With thrombolysis, the incidence of hemorrhagic stroke is elevated, however the threat of thrombotic or embolic stroke is somewhat reduced, and general any small increase in fatal cerebrovascular accidents is more than offset by the favorable impact on survival. Relative contraindications embrace prolonged or traumatic cardiopulmonary resuscitation, peptic ulcer illness, remote cerebrovascular accident, and hepatic failure. Safety has not been established for pregnant girls, though it has been for menstruating girls. Treatment could also be useful in some sufferers first seen 6 to 12 hours after the onset of symptoms, particularly these with stuttering infarcts. Clinical efficacy of coronary thrombolysis is dependent upon the frequency, rapidity, and persistence of recanalization, all of which depend not only on the intensity of fibrinolysis, but in addition on the inhibition of coagulation and platelet-induced thrombosis, which undoubtedly happen concomitantly. Presently, intravenous heparin is the agent of selection, coupled with orally administered aspirin. These and related agents are undergoing intense analysis for assessment of their potential utility alone or in numerous mixtures with fibrinolytic agents. They are particularly promising because platelet activation leads to profound augmentation of thrombin generation. Even optimally efficient coronary thrombolysis is compromised by early thrombotic reocclusion in 6 to 20% of sufferers with preliminary recanalization unless vigorous conjunctive anticoagulation is initiated instantly. Treatment may require use of thrombolytic medications and mechanical revascularization. Contrary to preliminary expectations, not all sufferers handled with thrombolytic drugs ought to be subjected to compulsory early cardiac catheterization and angioplasty. A technique comprising arteriography and angioplasty in only these sufferers who exhibit recurrent or persistent symptoms and signs of ischemia appears to be safer (Table 60-6) and as efficient as compulsory angiography for all sufferers in preserving ventricular operate and lowering mortality. Patients with insulin-dependent diabetes mellitus and peripheral vascular illness could be handled with caution. Death, nonfatal reinfarction, intracranial hemorrhage, or coronary bypass grafting after angioplasty. Appropriate treatment of fluid standing to optimize left ventricular filling pressures (see beneath), preserve oxygen saturation, and management coronary heart rate by avoiding reflex sympathoadrenal stimulation can be helpful. Intravenous nitroglycerin, titrated to avoid hypotension (10 to 200 mug/minute), reduces peripheral arterial resistance and ventricular afterload. Higher doses diminish systemic venous tone and blood pressure, thereby potentially (paradoxically) exacerbating ischemia. Tolerance to repeatedly administered intravenous nitrates happens rapidly, often within hours. General measures generally embrace use of stool softeners to avoid constipation, straining, and consequent circulatory derangements. Electrical countershock ought to be implemented instantly, somewhat than deferred until after implementation of endotracheal intubation and different emergency measures. If true electrical asystole is documented, immediate external, transvenous, or transthoracic cardiac pacing is important, though prognosis on this situation is grim. Other promising antifibrillatory drugs are presently being investigated within the United States. Assessment and treatment should focus on electrolyte and pH derangements and their correction. Flecainide, encainide, and sotalol suppress the arrhythmia, however in addition they appear to increase mortality. If severe dysfunction is clear, treatment ought to be guided by outcomes of electrophysiologic research (see Chapter 50). Treatment of those arrhythmias is the same as that used when they happen underneath different circumstances (see Chapter 51) and is indicated when they impair hemodynamics or compromise myocardial viability by augmenting oxygen requirements. In the absence of the Wolff-Parkinson-White syndrome, these circumstances ought to be handled with beta-blockers, calcium channel blockers, or digitalis glycosides (see Chapters 51 and 54). Calcium channel blockers are, nonetheless, potentially hazardous, particularly within the presence of hypotension or poor left ventricular operate. A quick-appearing beta-adrenergic blocker similar to esmolol could also be useful initially to management ventricular rate. When decompensation is clear, speedy atrial pacing (to terminate atrial flutter) or electrical cardioversion (to terminate both atrial fibrillation or flutter) ought to be used (see Chapter fifty three). Nevertheless, short-term transvenous pacing may stabilize hemodynamics, and lengthy-time period pacing could also be justified prophylactically in sufferers at excessive threat. Hemodynamic Manifestations Hemodynamic observations could be useful in guiding therapy (Table 60-7). Patients are categorized with respect to cardiac output (elevated, regular, or diminished), systemic arterial blood pressure (elevated, regular, or diminished, with or with out elevated or decreased systemic vascular resistance), and the presence or absence of pulmonary venous hypertension (elevated pulmonary arterial wedge pressure). Patients with out diminished systemic arterial blood pressure or pulmonary venous hypertension may have regular or hyperdynamic hemodynamics (the latter mirrored by a excessive cardiac output, with or with out hypertension brought on by sympathoadrenal stimulation). Rarely, it displays decreased peripheral vascular resistance brought on by vagotonia or sepsis. The noncompliant left ventricle requires augmented filling pressure to sustain cardiac output. Accordingly, relative hypovolemia may exist regardless of reasonably elevated left ventricular filling pressure. Right ventricular failure, with or with out concomitant tricuspid regurgitation, results in elevated central venous pressure with out concomitantly elevated pulmonary venous or pulmonary arterial occlusive pressure, which is indicative of left atrial pressure. Clinical findings often resemble these of pericardial effusion or constriction, however echocardiography can simply make the excellence. Central venous (systemic venous) pressure is often markedly elevated (upper restrict of regular = 6 mm Hg). Profound hypotension and pulmonary venous hypertension are manifestations of cardiogenic shock (see Chapter ninety five). Initial impairment of ventricular performance may exceed that attributable to irreversible damage due to myocardial stunning. Right ventricular involvement may compromise cardiac output greater than anticipated from the extent of left ventricular damage alone. Patients with peripheral hypoperfusion regardless of preliminary administration of fluids to replete or broaden vascular quantity and those with severe, refractory, or progressive coronary heart failure, refractory arrhythmias, persistent pain, or hemodynamic instability ought to be evaluated by balloon flotation right-sided coronary heart catheter hemodynamic monitoring. Patients with pulmonary congestion indicative of pulmonary venous hypertension, mirrored by bodily findings or chest roentgenographic abnormalities, often could be managed conservatively. They should remain in place for not more than seventy two hours to avoid the risk of an infection, and so they can often be removed much more promptly. Sometimes, ascertaining systemic and pulmonary venous pressure, cardiac output, and peripheral vascular resistance is adequate for subsequent administration with out the necessity for continuous monitoring. In different instances, the consequences of vasodilators, diuretics, agents with constructive inotropic results, and therapeutic alterations of vascular quantity ought to be monitored over the following 48 to seventy two hours.
Safe 100mg levitra extra dosage
These adjustments happen in a patchy style in gentle intermittent asthma and turn into more widespread because the disease turns into more persistent and severe. Morphometric studies of airways from asthmatic topics have demonstrated airway wall thickening of enough magnitude to improve airflow resistance and enhance airway responsiveness. In severe asthma, the airway wall is thickened markedly; in addition, patchy airway occlusion happens by a combination of hyperviscous mucus and clusters of shed airway epithelial cells. The episodic airway narrowing that constitutes an asthma assault outcomes from obstruction of the airway lumen to airflow. Three possible, but not mutually unique, links have been postulated: (1) constriction of airway clean muscle, (2) thickening of the airway epithelium, and (three) the presence of liquids throughout the confines of the airway lumen. Among these mechanisms, the constriction of airway clean muscle as a result of the local launch of bioactive mediators or neurotransmitters is probably the most extensively accepted explanation for the acute reversible airway obstruction in asthma assaults. Several bronchoactive mediators are thought to be the brokers inflicting airway obstruction within the asthmatic. Acetylcholine released from intrapulmonary motor nerves causes constriction of airway clean muscle through direct stimulation of muscarinic receptors of the M3 subtype. The potential function for acetylcholine within the bronchoconstriction of asthma primarily derives from the observation that atropine and its congeners have proven therapeutic efficacy in asthma. Histamine, or beta-imidazolylethylamine, was identified as a potent endogenous bronchoactive agent greater than 90 years in the past. Mast cells, that are outstanding in airway tissues obtained from patients with asthma, represent the most important pulmonary source of histamine. Clinical trials with novel potent antihistamines 388 Figure 74-1 Schematic renderings of airway anatomy from a normal topic (prime) and a mildly allergic asthmatic topic (backside). The airway within the asthmatic patient displays subepithelial fibrosis, edema, and inflammatory cell infiltration. Bradykinin and related molecules are cleaved from plasma precursors by the actions of enzymes known as kallikreins; no less than one kind of kallikrein is released from activated mast cells. It can also be unique among asthmatic mediators in that the sensation of dyspnea evoked by exogenous administration of bradykinin has been proven to mimic the subjective sensations reported by patients throughout spontaneously occurring asthmatic episodes. Clinical trials with leukotriene receptor antagonists or synthesis inhibitors have proven vital scientific efficacy within the treatment of persistent persistent asthma, leading to the conclusion that the leukotrienes are essential mediators of the asthmatic response. Two prophlogistic peptides, substance P and neurokinin A (substance K), are found within the terminal axon dendrites of certain sensory nerves. When these nerves are stimulated by acceptable sensory stimuli, their peptides are released into the airway microenvironment. In distinction to these contractile peptides, vasoactive intestinal peptide, a bronchodilator peptide also present in pulmonary nerves, is believed to play a homeostatic function within the airways. The contractile/inhibitory action of substance P, neurokinin A, and vasoactive intestinal peptide is regulated by particular peptidases located at or near the site of their action or launch. As a consequence, inhibition of the function of these peptidases enhances the biologic results of these peptides. The availability, as experimental instruments, of nonpeptide antagonists at neuropeptide receptors might result in elucidation of the function of these peptides within the asthmatic response; for the present, their function in asthma is speculative. Physiologic Changes in Asthma the consequence of the airway obstruction induced by clean muscle constriction, thickening of the airway epithelium, or free liquid throughout the airway lumen is an increased resistance to airflow, which is manifested by increased airway resistance (Raw) and decreased flow rates all through the very important capability. At the onset of an asthma assault, obstruction happens at all airway ranges; because the assault resolves, these adjustments reverse-first within the large airways (i. This anatomic sequence of onset and reversal is mirrored within the physiologic adjustments observed throughout decision of an asthmatic episode. Specifically, as an asthma assault resolves, flow rates first normalize at a excessive level within the very important capability, and only later at a low level within the very important capability. Because asthma is an airway disease, no primary adjustments happen within the static pressure-volume curve of the lungs. This closure leads to a change of the pressure-volume curve such that, for a given contained fuel volume throughout the thorax, elastic recoil is decreased, which in flip further depresses expiratory flow rates. Additional elements affect the mechanical habits of the lungs throughout an acute assault of asthma. During inspiration in an asthma assault, the pleural pressure drops far beneath the 4 to 6 cm H2 O subatmospheric pressure usually required for tidal airflow. The expiratory phase of respiration also turns into energetic because the patient tries to force air from the lungs. As a consequence, peak pleural pressures throughout expiration, which normally are only some centimeters of water above atmospheric pressure, may be as excessive as 20 to 30 cm H2 O above atmospheric pressure. The low pleural pressures throughout inspiration are likely to dilate airways, whereas the excessive pleural pressures throughout expiration are likely to slender airways. This tachypnea is pushed not by abnormalities in arterial blood fuel composition, but somewhat by stimulation of intrapulmonary receptors with subsequent results on central respiratory centers. One consequence of the mix of airway narrowing and rapid airflow rates is a heightened mechanical load on the ventilatory pump. During a severe assault, the load can improve the work of respiratory by an element of 10 or more and can predispose to fatigue of the ventilatory muscle tissue. The patchy nature of asthmatic airway narrowing leads to a maldistribution of air flow (V) relative to pulmonary perfusion (Q). A shift happens from the normal preponderance of V/Q models, with a ratio of near unity, to a Figure 74-2 Schematic flow-volume curves in numerous stages of asthma; in each determine the dashed line depicts the normal flow-volume curve. Variants of asthma exist during which cough, hoarseness, or an incapability to sleep through the night time is the one symptom. Identification of a scary stimulus through careful questioning helps to establish the prognosis of asthma and may be therapeutically useful if the stimulus can be averted. Most patients with asthma complain of shortness of breath when uncovered to rapid adjustments within the temperature and humidity of impressed air. For instance, during the winter months in much less temperate climates, patients generally turn into wanting breath when leaving a heated home; in warm humid climates, patients might complain of shortness of breath when coming into a chilly dry room, similar to an air-conditioned theater. The tendency of air flow with chilly dry air to induce airway narrowing types the premise of one of the widespread diagnostic checks for asthma. An essential factor to consider when taking a historical past from a patient with asthma is the potential for occupational exposures leading to the asthmatic diathesis (Table 74-1) (Table Not Available). However, reversal of asthmatic symptoms might not happen when the patient is faraway from the offending surroundings. Common options of acute asthma assaults embody a rapid respiratory rate (usually 25 to 40 breaths per minute), tachycardia, and pulsus paradoxus (an exaggerated inspiratory fall within the systolic pressure). The chest is usually hyperinflated, and the expiratory phase is prolonged relative to the inspiratory phase. Percussion of the thorax demonstrates hyperresonance, with lack of the normal variation in dullness as a result of diaphragmatic motion. Wheezing, generally louder throughout expiration but heard throughout inspiration as nicely, is characterized as polyphonic in that multiple pitch may be heard concurrently. Accompanying adventitious sounds might embody rhonchi, that are suggestive of free secretions within the airway lumen, or rales, that are indicative of localized an infection or heart failure. The lack of depth or the absence of breath sounds in a patient with asthma is an indication of severe airflow obstruction. A decrease in airflow rates all through the very important capability is the cardinal pulmonary function abnormality throughout an asthmatic episode. In very severe asthma, dyspnea may be so severe as to forestall the patient from performing a whole spirogram. If the asthma is of enough severity to advantage prolonged observation, nonetheless, blood fuel evaluation is indicated; in such cases, hypoxemia and hypocarbia are the rule. At the onset of the assault, an acceptable pure respiratory alkalemia is usually evident; with assaults of prolonged length, the pH normalizes because of a compensatory metabolic acidemia. In addition, elevated serum ranges of IgE are sometimes documented; epidemiologic studies point out that asthma is uncommon in topics with low IgE ranges. In uncommon situations throughout severe asthma assaults, serum concentrations of aminotransferases, lactate dehydrogenases, muscle creatine kinase, ornithine transcarbamylase, and antidiuretic hormone may be elevated. Severe asthma is related to hyperinflation, as indicated by depression of the diaphragm and abnormally lucent lung fields. Complications of severe asthma, together with pneumomediastinum or pneumothorax, may be detected radiographically.
Trusted levitra extra dosage 60mg
The only proven therapy is to stop the insult by even handed use of high oxygen concentrations. The physician usually faces a dilemma in that growing concentrations of oxygen are wanted to save the affected person immediately however can finally kill the affected person. Alternative strategies to improve arterial oxygen content must be used whenever potential; these strategies embrace a number of maneuvers primarily based on strategies related to mechanical assist of ventilation (see Chapter ninety three) and transfusion of packed pink cells to maintain the hematocrit near 30%. Cardiac output must be maintained and accompanied by measures to decrease the tissue oxygen demand by decreasing fever or agitation. Little or no harm occurs in regular animals or human volunteers breathing oxygen concentrations of 40 to 50% for extended periods. When oxygen (O2) is reduced incompletely, toxic oxygen species are formed corresponding to singlet oxygen (1 O2), superoxide anion (O- 2), and hydrogen peroxide (H2 O2). Quenchers react with reactive oxygen species or with oxidized cellular molecules to stop additional oxidation. A rational therapy is to use only enough oxygen to provide sufficient arterial blood saturation. If the affected person survives oxygen toxicity, some residual injury to the lung parenchyma may remain, with septal fibrosis changing areas where the pulmonary capillary bed was destroyed by the hyperoxia. Ionizing radiation produces oxidant lung harm related to the diploma of the radiation exposure. The clinical prevalence of radiation pneumonitis is set by the entire radiation dose, the variety of fractions, and the length of time over which the radiation is given. Chemotherapeutic drugs that produce oxidant-primarily based lung toxicity, corresponding to bleomycin, may potentiate lung harm from radiation. The alveolar partitions turn out to be infiltrated with mononuclear inflammatory cells and fibroblasts. Alveolar fibrosis and capillary sclerosis are its predominant histologic features. If massive volumes of lung have been irradiated, or if high radiation doses have been given over quick periods, the affected person can develop dyspnea, tachypnea, and fever. These signs can either progress to severe dyspnea and dying or progressively subside, leaving various degrees of respiratory impairment because of lung fibrosis. Permanent fibrosis takes 6 to 24 months to evolve, and it then often remains stable if no additional exposure occurs. Auscultation of the chest is often regular, though rales, signs of consolidation, and pleural rubs could also be found. Laboratory findings embrace a gentle leukocytosis and an elevated erythrocyte sedimentation rate. The affected areas are usually demarcated by a "straight edge" defining the margins of the radiation portal, and they have a "floor-glass appearance"-a hazy increase in density with vague pulmonary markings. In the later phases of the radiation harm, fibrosis and contraction of the irradiated region are the predominant radiographic findings. The prognosis of acute radiation pneumonitis could also be tough to set up due to coincidental illness. The clinical image is often complicated by the immunocompromised state of most of the sufferers, leading to elevated threat of bacterial or opportunistic pneumonias. Radiation pneumonitis in elements of the lung outside the radiation portal has been suspected in a number of sufferers on the idea of typical clinical and radiographic features. Complications of radiation pneumonitis embrace small pleural effusions and, occasionally, spontaneous pneumothorax. The affected person who develops radiation pneumonitis requires supportive care, together with cough suppression, antipyretics, and supplemental oxygen for hypoxemia. Corticosteroids (prednisone, 1 mg/kg of body weight) have been advocated for treating severe instances of radiation pneumonitis, though no managed clinical trials have been undertaken. No evidence supports the purely prophylactic use of corticosteroids, however using them at the very onset of pneumonitis appears to be more effective than later therapy. On occasion, the response could also be dramatic, with complete decision of signs within 24 hours. Corticosteroids must be tapered rigorously after achieving maximal clinical profit. Recurrent pneumonitis has been reported occasionally after withdrawal of steroids. Antibiotic therapy must be reserved for sufferers in whom the clinical findings recommend infection. Because the lesion involves occlusion and thrombosis of many small blood vessels, anticoagulation has been tried, however no evidence of its effectiveness has been compiled. Injury to the respiratory system by aspiration may be categorized by the nature of the aspirate as (1) infectious materials (see Chapter eighty two), (2) chemical or inflammatory substances, and (3) inert materials. Aspirating gastric acid is the commonest instance of chemical aspiration in adults; hydrocarbon aspiration occurs predominantly in youngsters however is encountered occasionally in adults. By distinction, lipids (mineral oil, vegetable and animal fat) most frequently provoke a chronic inflammatory response. Food particles may cause a fibrotic, granulomatous lesion or, if massive enough to occlude the larynx or trachea, sudden dying by asphyxiation ("cafe coronary"). Aspiration Pneumonitis Aspiration pneumonitis refers to pulmonary harm caused by acidic abdomen contents. This condition is in distinction to "aspiration pneumonia," an infectious process caused by oropharyngeal flora contaminating the tracheobronchial tree. Aspiration of gastric acid can occur during vomiting or regurgitation, and within the latter occasion the occasion may go unnoted (i. The regular protecting mechanisms of the higher airway embrace epiglottic closure during deglutition, glottic closure on contact with solids or fluids, the cough reflex, and esophageal sphincters. Altered states of consciousness, anesthesia and surgery, neuromuscular illness, gastrointestinal illness, and medical devices (nasogastric tubes or tracheostomy tubes) impair these defenses. Using low-stress, high-volume cuffs on endotracheal tubes reduces the extent of aspiration of gastric contents in sufferers in danger. The primary elements figuring out the extent of sickness caused by gastric acid aspiration are as follows: 1. The acidity of the fabric is the one most essential contributor to lung harm. Aspiration of gastric meals substances causes a severe pneumonitis and peribronchial inflammatory response within the absence of acid. Aspirating as little as 30 mL of gastric acid is sufficient to cause pneumonitis within the adult. Many sufferers who aspirate immediately start to cough, which can partially shield the lung from harm or may improve dispersion of the acid over a greater area and create a diffuse harm. Acid within the trachea is quickly distributed within the lungs and might reach the pleura in 12 to 18 seconds. It is quickly neutralized by bronchial secretions; in less than 30 minutes, the pH at the bronchial floor returns to regular. Acid causes chemical burns of the bronchi, bronchioles, and alveolar partitions, with subsequent exudation of fluid into the lungs. Plasma volume may decrease by as a lot as 35% in severe harm without fluid substitute, and cardiac output and systemic arterial blood stress may fall. Pulmonary capillary wedge stress is regular or low, indicating a nonhydrostatic explanation for the pulmonary edema. The characteristics of phospholipids within the alveolar floor lining layer (surfactant) are altered, growing floor forces and selling early alveolar collapse. Lung compliance decreases secondary to the increase in interstitial fluids and altered floor forces. These disturbances of airways, alveoli, and vascular elements profoundly unbalance the normal ventilation-perfusion relationships. Some sufferers aspirate a large volume of gastric acid and virtually immediately turn out to be apneic and hypotensive and die. More usually, the affected person survives the preliminary disaster however later develops a fulminant sickness marked by dyspnea, cough, and frothy sputum. Alternatively, aspiration may not be accompanied by immediate coughing and agitation. After such silent aspiration, the affected person may develop acute respiratory failure without an apparent reason for a precipitous deterioration in fuel exchange. Within 1 to 5 hours after aspiration of gastric acid, tachypnea, rales, and rhonchi occur, and wheezing, cyanosis, cough, and hypotension could also be present. Abnormalities on chest roentgenograms are extremely variable, and no attribute pattern is present.
Generic levitra extra dosage 100 mg
These cells secrete surfactant and carry out a variety of different biologic functions, together with regeneration of the alveolar epithelium, transport of electrolytes and fluids across the epithelium to keep "dry" alveolar air areas, and secretion of substances that help regulate immune and inflammatory functions within the lung. The lung has an intensive lymphatic system that clears fluid from both the pleural area and the lung. The pleural network lies within the visceral pleura lining the outer lung surface and connects to the deep or parenchymal plexus, which follows the bronchovascular bundles and the lobular septa. The two systems join at the boundaries between lobes or lobules and the pleura, and both systems drain towards hilar lymph nodes by way of larger lymphatic channels outfitted with valves. The pleural area can be lined by a parietal pleura, which is the pleural membrane on the chest wall aspect. The steadiness of oncotic and hydrostatic pressures within the capillaries lining the parietal and visceral pleuras is completely different owing to the fact that parietal pleura capillaries are provided by the systemic vasculature. The visceral pleura capillaries, which derive primarily from the low-strain pulmonary vascular circuit, have a imply capillary strain of 5 to 10 cm H2 O. Under regular conditions, the oncotic strain in blood is 384 approximately 15 cm H2 O greater than that within the surrounding extravascular tissues; thus, the oncotic strain gradient is the first force transferring fluid back into the capillaries. The effects of the traditional hydrostatic and oncotic strain variations in pleural capillaries lead to fluid motion from systemic capillaries within the parietal pleura into the pleural area. The pleural fluid may be absorbed either into low-strain visceral or parietal pleural lymphatics or into pulmonary capillaries lying throughout the visceral pleura. The adverse intrathoracic pressures in the course of the respiratory cycle additionally contribute to the presence of a big fluid flux out of the parietal pleura. The low-strain pulmonary vascular circuit creates a good larger constructive gradient favoring resorption of fluid from the pleural areas (and, in a similar way, from the alveolar air areas). Unless disturbed by disease, fluid strikes continuously into and out of the pleural areas, however the pleural areas are maintained free of extra fluid by the excessive absorptive capability of the visceral pleura and of lymphatics. In an analogous manner, any fluid in alveolar air areas is rapidly absorbed by the pulmonary capillary bed, and the alveolar air areas are stored "dry" and thereby obtainable for gas trade. Diseases that affect the permeability barrier created by pulmonary capillary walls, disturb pulmonary lymphatic drainage, or enhance pulmonary hydrostatic strain can alter these forces, resulting in rapid accumulation of pleural effusions and/or intraalveolar flooding. More than ninety nine% of the mass of particles inhaled under regular conditions are cleared by the nasopharynx and bigger airways within the lung. Particles impacting the upper airways are primarily cleared by the epithelial mucociliary escalator. Airway epithelial cells are coated by a mucous coat that will increase in thickness because it strikes upward. This mucous coat is frequently moved proximally by the ciliated cells lining all levels of the airways. Small particles (<10 mum in aerodynamic diameter) have a finite probability of reaching alveolar gas trade surfaces. Once particles deposit within the alveolar area, clearance is primarily via alveolar macrophages. In the traditional lung, each alveolus incorporates about 12 macrophages, and this quantity could also be 2 to 10 occasions greater within the proximal alveoli of a smoker or a person uncovered to excessive levels of environmental air pollutants. These free-transferring cells on the alveolar surface course of inhaled particles, antigens, micro organism, and viruses by phagocytosis. A critical function of the lung is to clear and/or course of inhaled antigens and infectious brokers or different poisonous materials without stimulating an amplified immune response. Although the alveolar surface is continually bombarded with inhaled supplies, the thin, delicate alveolar septa are generally maintained in a noninflamed state, and gas trade is undisturbed. A variety of chemical and structural elements contribute to regulation of immune processes within the lung, creating a milieu in which extensively dispersed inhaled particulate materials or infectious brokers may be processed without creating an exaggerated or unnecessary immune response. Disorders in these immune regulatory pathways, that are at the present time poorly understood, are prone to be necessary elements of hyperimmune or inflammatory lung ailments. Although gas trade is the plain major function of the lung, the lung additionally has a number of critical metabolic functions. The lung incorporates the one capillary bed within the physique by way of which one hundred% of the blood passes on each circulation. Thus, the lung is in a critical position to act as a mechanical filter of the blood and to regulate vascular levels or responses to a wide range of small peptides. The lung has an energetic uptake pathway for a wide range of vasoactive amines or peptides. The lung vascular bed can be a major site where circulating polymorphonuclear leukocytes are sequestered. Under regular conditions, approximately half of the circulating polymorphonuclear leukocytes are sequestered within the pulmonary capillary bed. They can be used to assess both coronary heart and lung function, establish basic functional categories of lung issues, assess responses to a wide range of inhalation accidents, and assess lung damage occurring via the pulmonary circulation. Although an enormous array of pulmonary function parameters may be measured, the first parameters of worth to the working towards doctor (Table seventy three-1) embrace basic measurements of lung volumes. Spirometric examination is essentially the most generally used take a look at and consists of measurement of the sample of air motion into and out of the lungs during managed ventilatory maneuvers. The lungs and the chest wall are elastic constructions that function in parallel to determine the gas quantity within the lungs at relaxation and the work concerned in numerous respiration maneuvers. The gas remaining within the lung at the end of a maximal exhalation maneuver is termed residual quantity. In wholesome persons, lung volumes vary in accordance with gender, age, peak, and ethnic group. Using ninety five% confidence intervals for the anticipated regular values is really helpful as the best index for determining whether or not a given subject is within or exterior the anticipated regular range. A simple and generally used substitute for ninety five% confidence intervals is to define as irregular a measured lung functional parameter that falls beneath 80% of its predicted regular. Thus, ±20% of predicted regular is a crude estimator of the range of values of pulmonary function present in a normal inhabitants. Total gas within the lungs is usually measured by one of three strategies: (1) washout of an inert gas (N2), (2) equilibration with an inert take a look at gas, or (3) entire-physique plethysmography. Accurate measurements of lung quantity done by washing out nitrogen (N2) or by equilibrating with an inert take a look at gas (helium) require that the take a look at gas communicate to or from all compartments of the lung. Lung volumes can be measured by physique plethysmography, which involves inserting the subject in a big air-tight field and having him or her breathe by way of a mouthpiece related to the skin. A shutter occludes the mouthpiece, and because the subject pants against the closed shutter, the volume of gas within the chest is compressed and expanded, creating an analogous change in gas quantity within the field. By measuring either changes in strain within the field or flow by way of a calibrated orifice within the field, the total quantity of gas within the thorax may be calculated. Finally, posteroanterior and lateral chest radiographs can be used to estimate lung volumes utilizing planimetry. This technique estimates thoracic gas quantity from the projected area of the lungs on two perpendicular views of the chest. With common computerized tools, more than 20 spirometric variables are sometimes reported. The use of enormous numbers of variables can lead to false-constructive findings, and it is recommended that just a few basic variables from the lung spirogram be used. Spirometric measurements of lung function are most useful when the patient has physical findings, symptoms, or threat components suggesting pulmonary disease. Lung functional research can be used to define the basic class of a lung dysfunction, consider the severity of the abnormality being quantitated, or comply with the progression of the disease course of. Age-associated declines in lung function should be considered in evaluating take a look at outcomes. In people who smoke youthful than 35 years, quitting smoking may end up in an increase in lung function. In people who smoke older than 35 years who stop smoking, the speed of decline of lung function generally slows to the traditional fee associated with growing older. The magnitude of functional impairment in obstructive lung disease may be assessed utilizing pulmonary function testing (Table seventy three-2). Mild exercise limitation means that the subject is able to Figure seventy three-4 A portion of a normal spirogram showing the forced exhalation from whole lung capability. It is necessary to correlate predicted functional capability by pulmonary function testing with the historical past of exercise limitation described by the patient. A vital difference within the functional capability predicted by pulmonary function testing with that described by the patient may be an necessary indicator of the presence of nonpulmonary disease processes.
Stabilized Liquid Oxygen (Vitamin O). Levitra Extra Dosage.
- Arthritis; asthma; constipation; depression; diabetes; dizziness; headaches; increasing energy; improving alertness, concentration, immune function, and memory; irritability; lung disease; menopause; mouth sores; muscle aches and pains; obesity; premenstrual syndrome; sexual problems; and many other uses.
- Dosing considerations for Vitamin O.
- How does Vitamin O work?
- What is Vitamin O?
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96461
100mg levitra extra dosage
Clinical presentation · Wheezing A musical, excessive-pitched whistling sound produced by airflow turbulence. Naga Foreign body aspiration Oropharyngeal dysphagia with aspiration Cystic fibrosis, immunodeficiency Cystic fibrosis, immotile cilia syndrome Cystic fibrosis, immotile cilia syndrome Vocal cord dysfunction Bronchiectasis Immunodeficiency · Cough Usually nonproductive and nonparoxysmal. Diagnosis · Pulmonary perform tests: Spirometry: obstructive pattern with response to bronchodilators. Education: self-management schooling ought to give attention to teaching patients the importance of recognizing their very own stage of control and indicators of progressively worsening bronchial asthma symptoms. Educational methods must also give attention to environmental control and avoidance methods, in addition to on treatment use and adherence. Expert Panel Report three: Guidelines for the Diagnosis and Management of Asthma, 2007. Asthma Medications 2-Agonists · Relieve the constriction by binding to specific receptors on airway clean muscle tissue cells. Leukotriene Antagonists · They block inflammatory pathways which are energetic within the illness. Prognosis of Asthma · Children at significant threat of getting bronchial asthma symptoms later in life - Children with early onset bronchial asthma < three years of age: Who had three or more episode of wheezing per year and a minimum of one major criterion (Eczema or parental eczema). Or a minimum of two minor criteria (allergic rhinitis, wheezing unrelated to colds, or blood eosinophil count > four %). Inhaled Corticosteroids · Inhaled corticosteroids are the most generally prescribed upkeep therapy for bronchial asthma. Naga · Absence of fever, tachypnea, elevated work of respiration, and auscultatory abnormalities, bacterial pneumonia is unlikely. Respiratory Disorders 303 · Possible causes: an infection, chyle, blood, malignancy, and drug exposures. Prolonged remark (minimal 8 h) in setting in a position to manage respiratory failure is perfect. Pneumothorax Causes · Primary spontaneous pneumothorax Occurs with out trauma or underlying cause More regularly in tall, thin male, thought to have subpleural bleb Family historical past is optimistic in many patients · Secondary pneumothorax Underlying lung illness Trauma Loud music (air stress) Catamenial pneumothorax (uncommon condition related to menses due to passage of intra stomach air by way of a diaphragmatic defect) Clinical presentation · the onset is abrupt, and the severity is dependent upon lung collapse. Foreign Body Aspiration Background · Nuts especially peanuts are one 1/three of cases. Complications · Retained overseas body is related to bronchiectasis, hemoptysis and lung abscess. Congenital Pulmonary Malformations Sequestration · Extralobar: more frequent in males; sixty five % within the left lung, coated by pleura, fed by systemic artery and drained through systemic vein, may be related to diaphragmatic hernia and colonic duplication. Pulmonary Abscess Background · Cystic space due to necrotic lung tissue a minimum of 2 cm in diameter. Clinical presentation · Fever · Cough · Sputum manufacturing · Hemoptysis Respiratory Disorders 305 · Treatment is surgical removing. Vascular ring/sling · May contain airway and or esophagus · Variable severity and timing of presentation · May cause stridor, cough, apnea, and dysphagia · Imaging chest is useful, more frequent with right aortic arch Congenital pulmonary adenomatoid malformation, lobar emphysema, and diaphragmatic hernia · Least frequent · May be seen on fetal imaging (U/S) and then resolve spontaneously · May cause extreme respiratory distress and require surgery · Consult pulmonology - Involvement of paranasal sinuses. Clinical presentation · Productive cough is the most typical symptom of bronchiectasis. Diagnosis · Pulmonary perform testing might present obstruction, restriction, and mixtures depending on etiology. Clinical presentation · Hundred percent of children have productive cough, sinusitis, and otitis media. Diagnosis · the gold normal check is documentation of irregular cilia ultrastructure (absent, irregular dynein arms, radial spokes, doublet arrangements) on nasal and bronchial biopsies or scraping considered on electron microscope. Treatment and prognosis · Establishing the primary cause is of important importance and is best undertaken with direction from a pediatric pulmonologist. Pulmonary Hemosiderosis Background · Repeated episodes of intra-alveolar bleeding that lead to irregular accumulation of iron as hemosiderin in alveolar macrophages. Bronchopulmonary Dysplasia Background · Recognized since 1960 following invention of optimistic stress ventilation for premature infants and their survival. Cystic Fibrosis Genetics · the most typical life shortening autosomal recessive illness due to mutation on the lengthy arm of chromosome 7. The passive movement of water is decreased and airway secretions are dehydrated with very low surface liquid layer. Cilia turn out to be compressed inhibiting ciliary clearance and cough clearance, micro organism thrive; immune perform can also be irregular on the airway surface. Repeated and persistent an infection leads to airway injury and bronchiectasis within the lung and dysfunction of other organs. Clinical presentation · Pulmonary: Cough is the most constant symptom dry at instances, regularly productive. Sarcoidosis Background · Sarcoidosis is a noncaseating granuloma multisystem illness. Clinical presentation · Approximately 5 % of cases are asymptomatic and incidentally detected by chest radiography. Respiratory Disorders 309 · Pancreatic perform testing: fecal elastase most popular technique. Naga · the disorder can happen at any age however is most typical within the preschool age group (26 years) and adolescents. Risk factors and associated circumstances · Adenotonsillar hypertrophy · Obesity · Craniofacial abnormalities, specifically midface hypoplasia and micrognathia · Hypotonia. Clinical presentation · Loud nightly snoring with observed apnea spells · Parents might notice that the kid is a restless sleeper · Sweats while sleeping · Sleeps in an irregular place with the neck prolonged · Chronic mouth respiration with persistent nasal congestion · Morning headaches · Excessive daytime sleepiness is more frequent among older kids. Overnight saturation monitoring could be very helpful to recognize issues that require extra assist. Usefulness of chest radiographs in kids with acute lower respiratory tract illness. Long-time period complication of congenital esophageal atresia and/or tracheaoesophageal fistula. Image gently, step lightly: promoting radiation security in pediatric interventional radiology. Cardiac problems related to chest ache · Coronary artery illnesses (ischemia or infarction) - History of Kawasaki illness (coronary arteritis) - History of transposition of great arteries s/p arterial change - Anomalous origin of the coronary arteries - Coronary artery fistula - Cocaine abuse - Coronary calcinosis - Takayasu arteritis · Infections/autoimmune problems - Pericarditis - Myocarditis - Systemic lupus erythematosus, juvenile rheumatoid arthritis · Arrhythmias - Supraventricular tachycardia - Ventricular tachycardia · Other cardiac abnormalities - Aortic stenosis - Aortic dissection (collagen vascular illness corresponding to Marfan syndrome) J. Hsu Respiratory circumstances causing chest ache · Asthma · Pneumonia · Pulmonary embolism - History of oral contraceptive use · Pneumothorax - Marfan syndrome · Pleural effusion/hemothorax · Clinical presentation - Tachypnea - Dyspnea - Hypoxia - Fever - Pleuritic ache - Cough - Hemoptysis Psychogenic problems · Anxiety · Stress · Recent major tense event - Separation from friends - Divorce within the household - School anxiousness/phobia - Death within the household Gastrointestinal problems · Recent overseas body ingestion · Reflux esophagitis · Clinical presentation - Burning, substernal in location - Worsened by reclining or consuming spicy meals - Pain is expounded to meals Miscellaneous causes · Sickle cell illness might lead to vaso-occlusive crises or acute chest syndrome. Idiopathic chest ache · No identifiable cardiac, pulmonary, or musculoskeletal cause · 20forty five % of cases of pediatric chest ache; no prognosis could be determined with certainty Clinical approach to chest ache · Comprehensive historical past - Characteristics of the ache Frequency, location, high quality, and severity of the ache Timing: daily activity, sleep, train - Associated symptoms: train intolerance, fatigue, tachycardia, shortness of breath, dizziness, or syncope - Family historical past for heritable illnesses affecting the center or lungs; for instance, sudden dying, deafness, seizures, cardiomyopathy, or bronchial asthma - A prior historical past of structural or acquired coronary heart illness - Prior historical past of cardiac surgery - Medication use · Physical examination - Vital indicators - Signs of coronary heart failure or congestion - Abnormal cardiac findings - Chest wall palpation · Electrocardiogram · Further testing as indicated by historical past, physical examination and electrocardiogram: blood tests, echocardiogram, train stress testing, pulmonary perform testing, 24-h Holter monitor Syncope Background · Syncope is a brief loss of consciousness which may be due to generalized cerebral hypoperfusion or neurologic problems. Causes of Syncope · Vasovagal: impaired response of the autonomic nervous system · Cardiac structural defects - Hypertrophic obstructive cardiomyopathy - Aortic stenosis - Pulmonary hypertension - Coronary artery anomalies · Cardiac arrhythmias; for instance, ventricular tachycardia (torsades de pointes), complete coronary heart block, atrial fibrillation · Noncardiac mechanisms, corresponding to seizures, hypoglycemia, or psychologic problems Vasovagal or neurocardiogenic syncope · the most typical type of syncope in kids Cardiovascular Disorders 315 · Neurally mediated syncope hardly ever is related to sudden dying · Mechanism of vasovagal syncope (hypersensitive autonomic response) - Decreased systemic venous return - Decreased left ventricular end diastolic volume - Increased mechanical contractility leads to stimulation of cardiac vagal fibers - Bradycardia, vasodilation, and hypotension · Clinical Presentation - Occurs with standing or sitting prodrome: tachycardia, diaphoresis, blurred vision - Brief interval of unconsciousness - Orthostatic hypotension - Normal physical examination · Red flags for cardiac syncope - Sudden onset of palpitation, shortness of breath, or chest ache before syncope - Syncope throughout exertion, swimming, or supine - Episode brought on by sudden startle - Exercise intolerance and fatigue - Young age < 10 years (specially less than 6 years) - Previous coronary heart illness - Family historical past of cardiomyopathy and channelopathy - Abnormal physical examination - Bradycardia Initial analysis · Electrocardiography - Rhythm - Left or right ventricular hypertrophy Cardiology consultation is indicated · Syncope with train. Further analysis · 24-h Holter or 30-day event monitoring if historical past suggests tachyarrhythmia · Echocardiogram if physical examination or electrocardiogram irregular Treatment of vasovagal syncope · Increase fluid and salt consumption · Fludrocortisone · Midodrine · Beta-blockers · Pacemaker - Documented bradycardia unresponsive to medical therapy Murmur Background · A murmur is heard in most youngsters at one or more of their examinations. Pathologic murmurs · Systolic ejection murmurs: crescendodecrescendo murmur heard best with the diaphragm. Clinical presentation · Feeling a "skipped beat" or "pause," usually adopted by a powerful beat. Atrial Flutter Background · Atrial charges of 300four hundred beats/min with variable conduction so that the ventricular rate is slower than the atrial rate. Sinus Rhythm and Sinus Arrhythmia Background · Sinus arrhythmia is a traditional discovering in wholesome kids. Management · the affected person should be referred for pressing cardiac analysis and remedy. Clinical presentation · Family historical past of unexplained sudden dying (50 % in symptomatic patients). Chest radiography · Cardiomegaly and pulmonary congestion in infants with extreme coarctation. Associated syndromes · Turner syndrome (the most typical lesion related to Turner syndrome is bicuspid aortic valve). Indication for prophylaxis · All dental procedures that contain manipulation of gingival tissue or the periapical region of enamel, or perforation of the oral mucosa. Prophylactic antibiotics · Ampicillin or first- or second-generation oral cephalosporins are beneficial in nonallergic patients.
Trusted levitra extra dosage 40 mg
The mind radioisotopic tracer distribution retains this fixed cerebral distribution in essence completely, dissipating only as dictated by the bodily half-lifetime of the tracer (tЅ = 6 hours). Owing to compromised cerebral blood flow, evaluation for a surgical revascularization procedure was performed. B, An acetazolamide (Diamox) vascular stress check was performed to determine if the viability of the left inside carotid vascular territory was in jeopardy. This case exemplifies the ability of the mind to present effective vascular collateral provides to the territory of a major arterial blockade. The cerebrovascular stress check clearly revealed the limitations of this collateral circulation. Only barely decreased perfusion is seen within the medial left temporal lobe (arrowhead). The major present limitation is that these scans have relatively low decision as a result of the low counts per pixel acquired within the speedy scanning procedure and the low vitality photon emission of Xe-133. Functional mind imaging can now be prolonged to measure the subtle changes in mind exercise associated with pondering. These procedures have the potential to detect congnition and thought as well as irregular mind activation patterns attributable to psychiatric disease and will eventually result in a extra correct anatomically-primarily based categorization of psychiatric illness. Pharmacologic manipulation to detect cerebrovascular insufficiency is also possible using the cerebral vasodilator acetazolamide (Diamox). This illustrates the excessive sensitivity for detecting metastases that may be obtained using indium-111-labeled monoclonal antibody tracers. During the stress scan the vascularly comprised territories of mind blood flow show a relative lower in tracer uptake compared with the remaining scan. Fluorine-18 has adequate half life (109 minutes) to be distributed regionally, additional permitting its widespread routine use in diagnostic nuclear medication. This injection and scan procedure is most revealing in extra-temporal lobe epilepsy patients without clear localization by another laboratory or imaging standards. Functional imaging of metabolic exercise allows clear distinction between new, recurrent, or residual, viable, excessive-grade glioblastoma and mind necrosis. Functional imaging not only can determine tumor grade and viability status but in addition can measure tumor dimension. The central benzodiazepine receptor distribution in epilepsy patients has been evaluated with iodine-123-labeled iomazenil. These tracer studies have elucidated the role of neurochemical receptors within the pathogenesis of neurologic and psychiatric disorders; this understanding is important for the development of pharmacologic therapies specifically targeted for these receptors. Monoclonal antibodies have performed an important role within the growth of this goal-specific imaging methodology. A, Projection picture (2D) of the torso of a affected person with main colorectal carcinoma (lower arrow) with metastases to the liver (higher arrow). Selected coronal tomographic sections (B and C) and transaxial (D) images are from a breast most cancers affected person with metastases to the backbone (B, a number of lesions at stage of arrow and under) and the cerebellum (C and D). E, Coronal tomographic picture illustrating abdominal metastases (arrows) in a affected person with ovarian carcinoma. F, Coronal and sagittal tomographic picture by way of the torso and head of a affected person with a main bronchogenic carcinoma (arrow). H, Coronal tomographic picture of a affected person with metastatic melanoma to the liver and spleen (arrows). Review of the present scientific applications of positron emission tomography in oncology. Genetics as an experimental science owes its origins to Gregor Mendel and his cross-breeding of garden peas in 1865. He identified specific bodily characteristics (phenotypes), corresponding to seed shade and plant height, that might be transmitted from one era to the next. Each phenotype was ascribed to hereditary factors, later designated genes, that have been inherited in pairs, one every from the male and female father or mother. True-breeding plants (homozygotes) inherited similar factors from the parental plants, whereas non-true-breeding plants (hybrids or heterozygotes) inherited different factors (alleles) from every father or mother. Some alleles have been shown to have a larger impact on the phenotype of hybrids than others. In the case of a dominant allele, a single copy of the gene was adequate to produce the same phenotype seen in homozygous organisms. Detecting these genes within the hybrid required breeding the plants and demonstrating the presence of offspring that bore the recessive phenotype. These laws have been first utilized to human disease by Sir Archibald Garrod in his studies of "inborn errors of metabolism" in 1908 (see Chapter 32). Each purine or pyrimidine pairs with a complementary base (A:T and G:C) (Table 31-1) to kind two antiparallel polynucleotide strands which might be twisted into a double helix. There are 23 pairs of chromosomes per somatic nucleus, 22 pairs of autosomes numbered by descending dimension, and 1 pair of intercourse chromosomes (X + X, feminine; X + Y, male). Only one of many allelic pair of chromosomes is allowed to segregate into the gamete. Thus, a diploid germ cell provides rise to a haploid sperm or egg that accommodates an assortment of one of every of the 23 pairs of allelic chromosomes within the parental cell. During fertilization, sperm and egg unite to create a zygote with a complete set of 46 chromosomes. The central dogma of molecular genetics holds that each gene encodes one polypeptide. The first base within the codon is identified on the left, the second base is identified on the top of the chart, and the third base is identified on the proper. Ala = alanine; Arg = arginine; Asn = asparagine; Asp = aspartic acid; Cys = cysteine; Gln = glutamine; Glu = glutamic acid; Gly = glycine; His = histidine; Ile = isoleucine; Leu = leucine; Lys = lysine; Met = methionine; Phe = phenylalanine; Pro = proline; Ser = serine; Thr = threonine; Trp = tryptophan; Tyr = tyrosine; and Val = valine. During the method of meiosis, allelic chromosomes are brought into shut juxtaposition. Single-strand breaks happen within the chromosomes and allow bridges, or chiasmata, to kind between homologous parts of the chromosomes. Although recombination can happen wherever within the chromosome, only a limited number of chiasmata kind during every meiosis. Two genes which might be on opposite ends of the chromosome could thus behave as if they have been on different chromosomes, whereas recombination is much less doubtless between genes which might be very shut of their main sequence to each other. The increased frequency of the joint inheritance of two genes which might be intently linked on a chromosome is termed linkage disequilibrium. Distances between genes on a chromosome may be quantified by their bodily distance from each other in hundreds of thousands of base pairs (megabases) or by their genetic distance, as measured by the frequency of recombination between the two genes per era. Recombination frequencies in selected regions of the genome differ in male and female gametes, implying that segments of chromosomes may be handled in another way by testicular and ovarian cells. This disparity can result in differences within the operate of alleles, depending on whether they have been inherited from the mother or the daddy, a process termed imprinting. From the standpoint of evolution, mutations are essential to generate adequate genetic diversity to allow species to adapt to their setting by way of the mechanism of "pure choice. A, During meiosis, homologous chromatids are attached to each other at websites of sequence id. Somatic mutations in oncogenes, for example, underlie the development of many cancers (see Chapter 191). Mutations could contain hundreds of thousands of base pairs within the structure of a chromosome, as in duplications, deletions, and translocations of a portion of 1 chromosome to one other (see Chapter 34). At the opposite extreme, a mutation may be minute and contain a small deletion or insertion or it may be a alternative of only a single base pair (level mutation). Deletions or insertions that happen in a coding region can alter the studying body distal to the mutation (frameshift mutations). Frameshift mutations regularly alter the protein sequence and might result in untimely peptide termination by producing a cease codon. The useful penalties of mutations could differ depending on the placement of the mutation. The catalytic site is exquisitely delicate, and a single mutation could abrogate operate. Finally, parts of the hydrophilic exterior could serve primarily to promote solubility, and changes in amino acid sequence that preserve polarity could have minimal penalties.
Trusted levitra extra dosage 60 mg
As our understanding of life has expanded, the connotation of poisoning has undergone substantial evolution. New analytical strategies can promptly and completely establish poisonings and have uncovered the causes of such numerous entities as Minamata disease (teratogenesis consequent to methyl mercury), an outbreak of ascending paralysis affecting greater than 4000 with greater than 400 deaths in Iraq (also caused by methyl mercury), the "gray syndrome" in premature infants (caused by chloramphenicol), mesotheliomas induced by asbestos, and an epidemic of angiosarcoma of the liver amongst industrial staff (caused by vinyl chloride). Nevertheless, many unknowns remain and justify careful potential monitoring of business, of the home, and of the surroundings. Many metals and non-metals in trace amounts are able to inflicting human disease, especially after continual or repetitive exposure. In others, the disease outcomes from using prescription or non-prescription medicines or as an antagonistic impact of medical procedures such as hemodialysis. Over the previous few a long time, increased awareness of the well being penalties of commercial substances, extra stringent federal and state laws, and worry of lawsuits have resulted in a healthier workplace. Knowledge of the refined penalties of continual, low-degree trace element exposure is still grossly insufficient. For example, copper smelter staff are uncovered not only to copper but in addition to lead, zinc, arsenic, gold, silver, cadmium, and mercury; in these staff, pneumonitis or other acute sicknesses might result from two or extra metals acting in concert. In other cases, excesses or deficits of a trace element might act not directly by inducing deficiency or toxicity of another trace element. In the previous, lead poisoning was ascribed to pica (abnormal ingestion) amongst children residing in dilapidated houses with peeling layers of lead-based mostly paints. In the previous 20 years lead intoxication has occurred with lowering frequency, partially related to less use of lead in paint and leaded gasoline. Several studies relate environmental lead contamination to traffic density patterns, with leaded gasoline the most important wrongdoer. It is estimated that greater than 800,000 American staff have potentially important lead exposure. Lead and other metallic smelter staff or miners, welders, storage battery staff, and pottery makers are particularly closely uncovered. Workers in auto manufacturing, ship constructing, paint manufacture, and printing industries are also at substantial threat, as are house painters and those that repair old houses. Lead-soldered kettles and cans and lead-glazed pottery can release lead when acidic fluids are stored or cooked in them. Demolition staff and those employed in firing ranges have turn out to be poisoned from intensive aerosol exposure. In the southern United States, moonshine whiskey is an important reason for poisoning. The stills are linked with lead solder, and old radiators containing lead are used as condensers; 20 to ninety% of moonshine samples comprise lead within the potentially toxic vary. In previous centuries, lead acetate was added to wine to sweeten it, a deception that was eventually made punishable by death. Recently, including result in varied natural and folks medicines has resulted in poisoning. Retained bullets can result in lead poisoning, especially if a joint is involved, as a result of synovial fluid seems to be an excellent solvent for lead. The interval between lodging of the bullet and scientific proof of lead poisoning has ranged from 2 days to forty years. Children have been poisoned by swallowing lead family objects, such as lead curtain weights, that are then retained within the gastrointestinal tract for a protracted time. Gasoline sniffing can produce lead poisoning; the organic tetraethyl lead seems to have a proclivity for the nervous system. Each day, an average of 150 to 250 mug is ingested, 5 to 10% of which is absorbed. The main toxic effects of lead are referable to the stomach, the blood, and the nervous system. The crampy, diffuse, often intractable belly pain may be accompanied by nausea, vomiting, anorexia, constipation, or occasionally diarrhea. The pain may be confined to the epigastric, periumbilical, or other areas of the stomach and should simulate a wide range of surgical and non-surgical diseases. Lead interferes with a wide range of red cell enzyme techniques, including delta-aminolevulinic acid dehydratase and ferrochelatase. Anemia is frequent in extreme acute lead poisoning and may be normocytic normochromic but usually is microcytic hypochromic. Moreover, an inherited deficiency in delta-aminolevulinic acid dehydratase may cause lead intoxication at modest blood lead ranges. These manifestations embrace irritability, incoordination, reminiscence lapses, labile affect, sleep disturbances, restlessness, listlessness, paranoia, headache, lethargy, and dizziness. In extra severe instances, manifestations embrace syncope-like attacks, disorientation, flaccidity, extreme psychological impairment, ataxia, vomiting, cranial nerve palsies, localized neurologic signs, psychosis, somnolence, seizures, blindness, and coma. The cerebrospinal fluid may be beneath increased stress and should show an increased protein content. Papilledema has been reported, as have grayish deposits surrounding the optic disc and optic atrophy. Frank encephalopathy is an ominous prognostic sign for each mortality and chronic mind harm. Most children who experience two or extra bouts of clinically evident encephalopathy have neurologic residua. Tetraethyl lead (organic lead) poisoning causes euphoria, nervousness, insomnia, hallucinations, convulsions, and frank psychosis. Wristdrop and footdrop happen most often; the previous, depending on sort of occupation, may be asymmetric, and there may be paresthesias. The spinal cord may also be involved, with manifestations having some similarity to these of amyotrophic lateral sclerosis. Over the previous era, increasing proof has arisen of refined mind harm within the absence of scientific proof of encephalopathy. Inordinate physique burdens of lead might end in mentation difficulties, emotional lability, deficits in intelligence and reminiscence, impaired psychomotor and visible motor perform, slowed nerve conduction, and behavioral aberrations in each children and adults, even within the absence of overt proof of poisoning. These modifications are postulated to happen at blood ranges of forty mug/dL (and even less in young children). However, the scientific neighborhood is sharply divided in regards to the scientific significance of those observations. In adults, the kidneys are often involved (see Chapter 107), the characteristic lesion being interstitial seventy two nephritis; as the disease progresses, glomerular filtration price falls. Occasionally, arrhythmias and cardiomegaly have been reported, as have abnormalities of liver perform. In the grownup, a excessive index of suspicion and a careful examination of the peripheral blood for basophilic stippling are obligatory; for occupational staff, lead screening is warranted. Blood lead ranges are readily decided by atomic absorption spectrophotometry or anodic stripping voltometry. Urinary coproporphyrin ranges are increased as a result of lead interferes with incorporation of iron into heme. Currently, 26 states have lead registries to monitor all lead analytic determinations within the state in an attempt to curtail issues. Three agents have been used to form tight complexes with lead and thus promote its biologic inactivation and elimination from tissues (Table 21-2). Chelation must be undertaken only after careful consideration for these with milder proof of poisoning, as a result of every of the agents may be related to important antagonistic effects. Newer, less toxic oral dimercaprol analogues dimercaptosuccinic acid and dimercaptopropanesulfonate have been introduced with the hope of enhancing efficacy and reducing issues. More than 60 occupations involve mercury exposure, including chloralkali work; manufacture of pesticides, pesticides, and fungicides; manufacture of mercury-containing instruments, lamps, neon lights, batteries, paper, paint, dye, electrical gear, and jewellery; and dentistry. In the previous, mercury was administered medicinally as a component of cathartics, teething powders, and antihelminthics. Elemental mercury is a liquid at environmental temperatures but vaporizes with agitation in addition to gentle heating. Bulk mercury is utilized in dental amalgams; as much as 10% of dental offices have extreme mercury vapor ranges; and unintended spillage can result in mercury poisoning. Heavy aerosol exposure to mercury produces chills, fever, cough, chest pain, and hemoptysis; roentgenograms show diffuse pulmonary infiltrates. Oxidized elemental mercury is readily absorbed from the alveoli; subsequently it could enter the mind. With gentle exposure, the manifestations are prone to be refined and diagnosis is troublesome.
References:
- https://pathology.oit.duke.edu/siteParts/avaps/02.15.1_Thrombosis_I_or_Hemostasis_FINAL.pdf
- https://www.ventegra.com/medpolicies/Medication%20Policy_Provigil.pdf
- https://www.aphrs.org/attachments/article/97/Pre-excitation%20patient%20when%20not....pdf
- https://www.govinfo.gov/content/pkg/GPO-STYLEMANUAL-2016/pdf/GPO-STYLEMANUAL-2016.pdf