.png)
Effective nolvadex 20mg
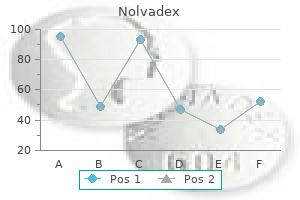
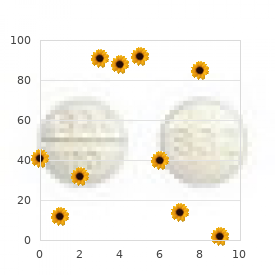
Coarsening of the skin of the face and scalp, often known as cutis verticis gyrata, could also be noticed in addition to seborrheic dermatitis and palmoplantar hyperhidrosis. The scientific manifestation patterns are variable, ranging from the total syndrome (periostitis, pachydermia, and cutis verticis gyrata) or a partial expression (no involvement of the head) to a "forme fruste" (pachydermia with out periostitis) (3). Primary hypertrophic osteoarthropathy usually exhibits a progression of about 10 years, when it arrests spontaneously. The life expectancy is normal, but disabling can occur if the axial skeleton is concerned with stiffness, kyphosis, and neurological manifestations as spinal nerve roots get compressed by new bone formations. In 1890, Bamberger and Marie independently described secondary hypertrophic osteoarthropathy as a syndrome of digital clubbing and periostitis in sufferers suffering from chronic coronary heart and lung diseases (4, 5). Secondary hypertrophic osteoarthropathy exhibits an even distribution between men and women with no racial preference. In secondary hypertrophic osteoarthropathy, the periostitis is often related to a deep, burning ache. Arthritis is more frequent (as much as 40% of sufferers) and can mimic symptoms of rheumatoid arthritis when affecting small joints. However, with an extended length of secondary hypertrophic osteoarthropathy, like in congenital cyanotic coronary heart disease, symptoms and findings can absolutely correlate with those noticed in major hypertrophic osteoarthropathy. In more advanced phases, osteolysis can seem at the distal phalanges and ossification of ligaments can be noticed. Synostosis can develop, notably between carpal and tarsal bones, in addition to at the symphysis pubis. In a sophisticated stage of major hypertrophic osteoarthropathy, synovialitis could have an effect on joints causing limited movement because of periosteal appositions near the joint. In secondary hypertrophic osteoarthropathy, the appositions are linear thin traces separated from the cortical bone. They can also have an "onion-skin"-like look, but are usually not as irregular as in major hypertrophic osteoarthropathy. In a later stage of the disease, the new periosteal bone fuses with the original cortex. Besides the tibia, fibula, radius, and ulna, periosteal appositions can even seem at the femur, humerus, metacarpalia, metatarsalia, and the phalanges. Rarely an involvement of the scapula, the clavicle, rips, backbone, or cranium is discovered. As in rheumatoid arthritis, joint effusion can be discovered in addition to osteoporosis near the joint. In contrast to arthritis, no joint area narrowing or erosive bony lesions are seen. Nuclear Medicine Radionuclide bone scanning utilizing technetium Tc99m polyphosphate can reveal the disease in an early stage, where plain films are nonetheless unfavorable. It exhibits elevated uptake of the tracer in the cortex of diaphysis and metaphysis. Clubbed digits and related synovitis can both present elevated activity, notably in an early part of the scan. Diagnosis and Differential Diagnosis Differential analysis between major and secondary hypertrophic osteoarthropathy can be achieved primarily based on radiographic findings (irregular, with epiphyseal involvement in major hypertrophic osteoarthropathy), scientific presentation. Other differential diagnoses to think about are thyroid acropachy, venous stasis, hypervitaminosis A, childish cortical hyperostosis, acromegaly, and endosteal hyperostosis. In thyroid acropachy, pretibial myxedema and a Imaging Periostitis is the characteristic characteristic of the disease (6). Periosteal appositions usually begin creating at the distal finish of the diaphysis. Figure 2 Radiograph of the proper distal tibia and fibula in an anteroposterior and lateral view. Figure 3 Radiograph of the proper distal tibia and fibula in a lateral and anteroposterior view of a 59-12 months-old affected person with pachydermoperiostitis. Multiple regions of periosteal reaction are recognized involving the diaphysis, metadiaphysis, metaphysis, and epiphysis of the tibia and fibula. Presse Med forty three:1820�1824 � Bamberger E (1891) Uber Knochenveranderugen bei chronishen Lungen und Herzkrankheiten. Saunders, Philadelphia historical past of thyroid dysfunction are current; the typical speculated periosteal appositions have a predilection for small tubular bones. Venous stasis exhibits a predilection for the decrease extremity with indicators of phlebolitis, gentle tissue swelling, and ulceration. In hypervitaminosis A, gentle tissue nodules could also be current with epiphyseal deformities. Infantile cortical hyperostosis is characterized by cranial destructions and skeletal deformities. Martinez-Lavin M, Matucci-Cerinic M, Jajic I et al (1993) Hypertrophic osteoarthropathy: consensus on its definition, classification, evaluation and diagnostic criteria. J Rheumatol 20(eight):1386�1387 Hippocrates (1849) Hippocrene Books: Prognostic: Regimen in Acute Diseases, Sacred Disease, Art, Breaths, Law, Decorum, Physician, Dentition. Congenital Abnormalities, Pancreatic Synonyms Birth asphyxia; Hypoxic-ischaemic Neonatal; Perinatal; Seizures encephalopathy; Hypotelorism Definitions Narrowed intercanthal space. There could also be a clear sentinel occasion such as a wire prolapse or uterine rupture that precedes indicators of foetal distress detected as abnormalities in foetal coronary heart rate seen on cardiotocograph with or with out meconium stained liquor. The analysis of hypoxic-ischaemic encephalopathy is made when such neonates require resuscitation at start, having low Apgar scores <5 at 1 min and often <5 at 5 min, after which develop irregular neurological indicators such as seizures, irregular tone, irritability and poor feeding. The pattern of injury sustained in the brain is determined by the length and nature of the hypoxic-ischaemic insult. Hypothenar Hammer Syndrome Symptoms occurring in sufferers who use the palm of the hand for pushing, pounding, or twisting (mechanics, carpenters, and so on. Ischemia, Brachial Hypothyroidism Aetiology the physiological manifestation of elevated thyroid function, hormone production or insensitivity of the tip organs to thyroid hormone. There is an elevated incidence of thrombophilic disorders in neonates with perinatal infarction. Factor V Leiden has been related to more in depth infarction and poorer outcomes. Neonates could require assisted ventilation because of respiratory melancholy secondary to the injury or to anticonvulsant medication administered to management seizures. In infants with marked basal ganglia lesions feeding stays tough for weeks or months. Sequences could have to be adapted to the neonatal brain with its higher water content material and longer T1 and T2 values. A venogram is useful in delineating related thrombosis from subdural haemorrhage throughout the major sinuses. By the time most neonates are imaged, haemorrhage is evident on conventional T1 and T2 weighted sequences. Feeding and wrapping neonates can sometimes produce a natural sleep for long enough to picture. The subcortical white matter adjacent to these areas of "cortical highlighting" develops an extended T1 and long T2 according to ischaemic change. This tissue usually atrophies and appears gliotic at follow up after 1 12 months of age. The medial temporal lobe may present obvious cortical and subcortical abnormalities. It subsequently atrophies leading to poor head progress and a secondary microcephaly. Ultrasound is complimentary but must be performed serially for no less than the first week to detect lesions. It should still be tough to determine peripheral infarction and delicate but clinically vital basal ganglia lesions. The timing is important whilst early imaging could also be required in order that decisions about continuing intensive care can be made the severity of injury will not be obvious unless diffusion weighted sequences are used. T1 weighted images showing a standard look, mild, reasonable and severe basal ganglia lesions in neonates presenting with hypoxic-ischaemic encephalopathy. Infant with established severe basal ganglia lesions showing cystic breakdown and a few atrophy. There is irregular cortical highlighting alongside the interhemispheric fissure and the central sulcus. They do nevertheless develop cognitive impairment the severity of which is said to the severity of white matter abnormality.
Quality 20 mg nolvadex
Infection normally demonstrates extra widespread uptake on delayed bone scan compared to the focal uptake of a stress fracture. In oncology sufferers, an damage may represent a pathological fracture via a metastasis or an insufficiency fracture from radiation or osteoporosis. The presence of endosteal scalloping and marked muscle edema supports the analysis of a pathologic fracture. Early stress injuries are characterised by small resorption cavities and osteopenia in the cortex. Periosteal and endosteal bony proliferation is characteristically seen in therapeutic lesions. An early stress response demonstrates excessive T2-weighted signal inside the medullary cavity or cortex. Progression to a stress fracture results in the characteristic appearance of a low signal intensity, transverse linear band on T1- and T2-weighted images. Fayad L, Kamel I, Kawamoto S et al (2005) Distinguishing stress fractures from pathological fractures: a multimodality method. Radiology 235:553�561 Lassus J, Tulikoura I, Konttinen Y et al (2002) Bone stress injuries in the decrease extremity: a evaluate. Acta Orthop Scand 73(three):359�368 Nuclear Medicine Bone scintigraphy demonstrates glorious sensitivity however restricted specificity in detecting stress fractures. The represent physiologic, not-disease-related cysts and happen as a normal strategy of ovulation normally disappearing inside eight�12 weeks with out remedy. Free Fragment A free fragment is a fraction of disk that has separated from the disk of origin. The most typical causes are fulminant viral hepatitis, drug toxicity (acetaminophen, isoniazid, antidepressant), chemical toxicity (mycotoxins of the mushroom Amanita phalloides), ischemia or shock. A lobe could also be spared or patchy necrotic areas could also be dispersed all through the liver. The scientific situation is dominated by jaundice, encephalopathy, coagulopathy and bleeding, renal failure, cardiovascular failure. Hepatitis Department of Radiology, Childrens Hospital, Nancy University Hospital, Vandoeuvre les Nancy, France m. Renal function includes at least two successive physiological processes: glomerular filtration (which is determined by the variety of nephrons and on blood perfusion) and reabsorption/secretion in the tubules. Second, as a result of current technical enhancements, the kidneys can be studied with excessive temporal and spatial decision, permitting analysis of blood perfusion, for example. Different tracers can be found, permitting analysis of the different processes leading to urine formation. This radiopharmaceutical can also be useful for measuring cut up function because the ratio of activity measured in each kidney, after correction for background activity, corresponds to cut up function. Dynamic imaging protocols normally involve different phases: acquisition of 60 one-second images to observe the vascular section, and comply with-up of the medullar focus and excretion during 20�forty five min, sensitized by injection of furosemide. Renal perfusion is calculated from the vascular section by dividing both the upslope of the kidney by that of the aorta (Kirchner index) or the world beneath the curves (Hilson index). After the vascular peak, activity continues to enhance till a peak previous excretion. Indeed, if correction for background activity and for each kidney quantity is utilized, it may be derived from the ratio both of the world beneath the curve or the upslope between 1 and three min after injection. The cortex, containing the glomerulus, is the extra exterior one and is comprised of the glomerulus, the proximal and distal convoluted tubules, and the start of the accumulating ducts. The internal layer corresponds to the medulla, which is constituted by the loops of Henle and the distal parts of the accumulating ducts. But this method permits analysis of renal perfusion, including regional blood quantity and circulate, in several pathologic conditions similar to renal artery stenosis and continual obstruction. However, absolute quantification remains difficult because of the quite a few parameters and changes, and exploration remains to be restricted to a single slice or to a small quantity. Iodinated Contrast Media and Gadolinium Chelates After intravenous injection, these clinically out there distinction media, generally known as nonspecific agents, have an unrestricted interstitial diffusion and are freely filtered via the glomerulus with out secretion or reabsorption by the tubule. Second, these measurements are related to a excessive radiation dose because of the quite a few acquisitions required. Intravenous Urography Intravenous urography was the first renal practical imaging method, nevertheless it offers just some primary physiological knowledge that add to morphologic knowledge. Abdominal X-rays are performed earlier than and at various instances after intravenous injection of an iodinated distinction medium (normally at the end of injection and at 4, eight, 12, and 20 min). Nephrographic: this phrase begins with the arrival of the distinction medium in the cortex (vascular nephrogram), which lasts just a few seconds, adopted by the focus of the distinction medium in the medulla, which reaches its maximum between 5 and 10 min after injection in regular kidneys earlier than wash-out. Urographic: this section begins about 2 min after injection, when the distinction medium is excreted in the renal calyces and pelvis. Functional analysis is subsequently restricted to a visual appreciation of a delayed nephrogram and/or urogram, with none specificity (renal artery stenosis, continual obstruction). Some are common to all imaging techniques regarding kidneys: their intraabdominal scenario results in respiratory motions between two acquisitions in breath-maintain or if the acquisition lasts too lengthy, and movement artifacts created by digestive peristalsis. Thus, conversion of signal intensities into concentrations based mostly on phantom studies is preferable. The y-axis corresponds to the comparison between the evolution of the attenuation in areas of interest placed in the aorta (A) and in the kidney (K) (K(t)/A(t)), when a �R t � normalized time is on the x-axis zero A�t �=A�t� (three). The clearance corresponds to the slope of this line, and the fractional vascular quantity corresponds to the y-axis intercept. First, the use of iodinated distinction media may worsen a preexisting renal insufficiency, however this danger is decreased by the small quantity of distinction Renal Blood Volume and Flow Evaluation of renal perfusion is especially interesting in renal artery stenosis, in illnesses with renal microvasculopathy, or in estimation of effects of remedy. Arterial spin labeling is one other method with out distinction media, but the in vivo accuracy of this system has but to be demonstrated. Perfusion parameters can be evaluated utilizing strategies with distinction agents; this is named dynamic distinction-enhanced imaging. Signal�time curves are derived from areas of interest placed in the aorta and kidney. Various mathematic models have been evaluated; the choice of the suitable one is determined by the distinction agent used. Indeed, clinically out there gadolinium compounds have a vast interstitial diffusion and are freely filtered via the glomerulus, theoretically requiring resort to a 3-compartment mannequin-notwithstanding that this third compartment, representing less than 10% of renal parenchyma, is normally neglected. Other gadolinium chelates, generally known as rapid-clearance blood pool agents, have a better molecular weight that limits their interstitial diffusion with out compromising their glomerular filtration; thus, use of a twocompartmental mannequin is possible with out making any assumption. Moreover, conversion of signal intensities into focus is simpler because decrease doses of gadolinium are injected because of their properties. With these gadolinium chelates, T1-weighted sequences are used, similar to quick gradient echo with spoiler. Semiquantitative approaches based mostly on T1-weighted sequences have proven similar results to renal scintigraphy for parameters measured on signal�time curves, similar to vascular upslope, time to peak, and area beneath the curve. Parenchymal signal�time curves start with a vascular upslope corresponding to the arrival of the distinction medium in the vessels and the glomerulus, adopted by a brief decrease and then by a second upslope corresponding to glomerular filtration and tubular function, till a peak previous excretion. T (to be suppressed) Signs of nephropathy are extra marked on the latter with decreased quantity of parenchyma and sinus lipomatosis. Br J Radiol 69:989�995 Prigent A Piepsz A (eds) (2005) Functional Imaging in NephroUrology. Fundoplication this antireflux process is indicated in the surgical remedy of gastroesophageal reflux. The fundus is wrapped posteriorly across the distal esophagus and decrease esophageal sphincter. The fundus is sutured anteriorly, making a complete 360� wrap (Nissen Fungal, Abscess, Hepatic 755 fundoplication) or incomplete 270� wrap (Toupet fundoplication) that lies below the level of the diaphragm. Stomach and Duodenum in Adults Postoperative Fungal, Abscess, Hepatic Fungal abscesses are most frequently caused by Candida albicans, they usually happen in immunocompromised people. Hepatic abscesses caused by Cryptococcus infection and Aspergillus species have also been reported. Hepatic fungal microabscesses in immunosuppressed sufferers have a miliary distribution and appear as multiple small, often subcentimetric, lesions scattered all through the liver. After therapy the lesions are inclined to decrease in dimension and enhance in echogenicity, leading to the fourth pattern which consists of echogenic foci with variable levels of posterior acoustic shadowing. These microabscesses normally present central enhancement, though peripheral enhancement may happen.
Generic nolvadex 20 mg
Renalexcretionisreduced by the low glomerular filtration rate, which will increase thehalflifeofsomedrugs,e. Discharge from hospital Childrenshouldbedischargedfromhospitalassoonas clinically and socially applicable. Beforedischargefromhospital, parentsandchildrenshouldbeinformedof: 72 � Thereasonforadmissionandanyimplicationsfor thefuture Box 5. Donotavoid difficultissuesbecauseparentshavenotthought toask Follow-up � Offerearlyfollowup � Suggesttofamiliesthattheywritedown questionsinpreparationforthenext appointment � Ensureadequatecommunicationofcontentof interviewto: � othermembersofstaff � generalpractitionerandhealthvisitor � otherprofessionals,e. Theaimisto Definitions of the principles of medical ethics � Non-maleficence�donoharm(psychologicaland/ orphysical) � Beneficence�positiveobligationtodogood(these twoprincipleshavebeenpartofmedicalethics sincetheHippocraticOath) 1 2 three 4 Care of the sick youngster seventy three 5 Detailsofmedicationandothertreatment Anyclinicalfeatureswhichshouldpromptthemto seekmedicaladvice,andhowthisshouldbe obtained � Theexistenceofanyvoluntaryselfhelpgroupsif applicable Problemsorquestionslikelytobeaskedbyother � familymembersorinthecommunity. School 5 Care of the sick youngster Child psychiatrist Psychologist Physiotherapist Occupational therapist Speech and language therapist General practitioner Health visitor Community paediatric services Consultants in other specialities Child development group Hospital inpatient keep and discharge planning Paediatric residence care group Social services Tertiary centre Dietician Figure 5. Consent Validconsent is required forall medical interventions otherthanemergenciesorwhenurgentinterventionis necessary to prevent critical threat of present or future hurt. It supplies the moral and legal authority for actionwhichwouldotherwisebeacommonassaultor intervene with the proper of individuals to decide what must be done to them (autonomous choice). Clinicians haveadutytoprovidesufficientinformationtoenable a reasonable person to make the choice and must answer all questions actually. The proper of children under this age to give consentdependsontheircompetenceratherthantheir age. Whenachildlacksthematurityandjudgementto giveconsent,thiscapacityisgiventoapersonhaving parentalresponsibility�usuallyanaturalparent,orto Application of moral principles to paediatrics Non-maleficence Children are extra vulnerable to hurt. Justice this entails ensuring a complete youngster well being service, including the prevention of illness, and equal access to healthcare, even when poverty, language barriersandparentaldisabilityarepresent. Whenagirllessthan16yearsofagerequestscon traceptionwithoutparentalknowledge,aprofessional canprovideitifsatisfiedthatshecannotbepersuaded toinformherparents,thatsheislikelytohavesexwith orwithoutcontraceptionandthatreceivingcontracep tion is in her best pursuits. Whatever the end result, children ought to have their viewsheardandbegivenreasonsastowhytheyare beingoverridden. Yet with the total and anxious approvalofhisparents,yougoaheadanddothese issues anyway. They are given the privilege and duty of makingdecisionsonbehalfoftheirchildrenlargely becausetheyaremostlikelytoprotectandpromote theinterestsoftheirchildren. Thenormalassump tion in paediatric practice is that medical doctors ought to work carefully with mother and father and give advice that parentsmayormaynotaccept. Whereverpossible, amutuallytrustingandrespectfulworkingrelation ship must be developed and maintained, each because it will be in the best pursuits of the child andbecauseitwilltendtoleadtofarbetterexperi encesofmedicalcareforallinvolved. Confidentiality Childrenareowedthesamedutyofconfidentialityas adults, regardless of their legal capacity. In common, personalinformationaboutthemshouldnotbeshared withouttheirconsentoragreementunlessitisneces sary for their well being or to shield them from critical hurt,e. Best pursuits It is a common moral and legal maxim that the best interestsofthechildareparamount. Doctorstherefore have a duty to save life, restore well being and prevent illness by treatments that confer maximum profit andminimalharmandwhichrespecttheautonomyof thechildasfaraspossible. Parentshavetheethicaland legal duty to make decisions on behalf of their youngster, providedthattheyactintheirbestinterests. Disputes might come up over what constitutes best pursuits and whoshoulddecideaboutthem;theymayrequirelegal intervention,especiallywhenthewithholdingorwith drawingoflifesustainingtreatmentisinvolved. Childrendifferfromadults in their anatomy, physiology, illness patterns and responses to remedy however many drugs in present use havenotbeentestedonthem. However,childrenare perhaps extra vulnerable to the hurt which may be produced by analysis and must be protected againstit. Research that fails to profit people could also be moral supplied that it involvesanacceptablelevelofrisk. It is the opinion of her paediatric advisor thatnofurthermedicaltreatmentislikelytobecura tive. Jane asks one of the junior paediatric medical doctors whyherparentshadbeensoupsetfollowingarecent discussionwiththeconsultant,atwhichshehadnot beenpresent. The mother and father have heard of a new drug which is claimed,insomereportsontheinternet,tohelpsuch children. In such conditions, additional discussion between the parentsandstaffwhomtheytrustisusuallythekey to resolving the scenario. The mother and father might want to understandthemutualbenefitsofadoptingasopen apatternofcommunicationaspossible. Both could be ethicallyjustifiedprovidedthattheprocedureinques tion carries no extra threat than generally encountered andacceptedineverydaylife. However,suchdecisions have usually been made intuitively, given as clinical opinion, which is tough to generalise, scrutinise or problem. Evidencebasedpracticeprovidesasystem aticapproachtoenableclinicianstoefficientlyusethe bestavailableevidence,usuallyfromresearch,tohelp them remedy their clinical issues. The distinction betweenthisapproachandoldstyleclinicalpracticeis thatcliniciansneedtoknowhowtoturntheirclinical problemsintoquestionsthatcanbeansweredbythe analysis literature, to search the literature effectively, and to analyse the proof, utilizing epidemiological and biostatistical guidelines (Figs 5. Sometimes, the bestavailableevidencewillbeahighqualitysystem atic evaluation of randomised controlled trials, that are directly relevant to a specific patient. Theimportant issue is that, for any choice, clinicians know the strengthoftheevidence,andthereforethedegreeof uncertainty. Asthisapproachrequiresclinicianstobe explicitabouttheevidencetheyuse,othersinvolvedin the selections (patients, mother and father, managers and other clinicians) can debate and choose the proof for themselves. Each group member needstounderstandtherationalefordecisionsandthe probabilityofdifferentoutcomesinordertomaketheir ownclinicaldecisionsandtoprovideconsistentinfor mationtopatientsandparents. Management protocols of virtually all children with cancerarepartofmulticentretrialsdesignedtoiden tify which treatment offers the best possible results. The trials are nationwide or, increasingly, international, andincludeshortandlongtermfollowup. There are many examples from the previous the place, by way of lack of proof, clinicians have harmed children,e. For evidencebased practice to turn into extra widespread,cliniciansmustrecognisetheneedtoask 1 2 three 4 Care of the sick youngster seventy seven 5 Application of proof-based medication to clinical issues Clinical downside 5 Care of the sick youngster What proof is needed to reach your choice Clinical issues are sometimes advanced and the completely different elements (aetiology, prognosis, remedy, prognosis) must be tackled as separate questions. Most clinical questions could be structured into these three elements: Frame query Patient inhabitants A inhabitants similar to your patient Intervention. For randomised clinical trials and systematic reviews of interventions, go to Cochrane Library. Appraise the proof Appraise the validity (closeness to the reality) and usefulness (relevance to your patient) of the proof. If about prognosis, you want a study that follows a group of patients similar to your patient (cohort), over an sufficient period of time, to see what occurs to them. This is dependent upon judgements in regards to the validity and relevance of the proof, the probability of the completely different outcomes, and the values assigned to them by the patient, clinician and wider society. We will usually agree on the validity of the proof and the probability of the completely different outcomes, however decisions might differ because the individuals involved maintain completely different values. Evaluate your efficiency Ensure that proof-based decisions are translated into practice and measure the wider effects of implementation on healthcare. You explain to the father or mother that antibiotics: � would cut back the chance of ache lasting 2�7 days however about 17 children must be treated for one to profit, and this would not reduce the chance of listening to loss � would increase the chance of minor aspect-effects. One method can be to give this information and a prescription for antibiotics to mother and father and ask them to wait 2�three days and use their prescription only if the child continues to be unwell. Clear proof of profit 5 Care of the sick youngster Surfactant remedy in pre-time period infants the metaanalysis (see. This proof was rapidly produced and intro ducedintopracticeas: � Respiratorydistresssyndromeisacommon causeofdeathandmorbidityinaneonatal intensivecareunit � Thereisaclearlyunderstooddisease mechanismforrespiratorydistresssyndrome, i. Clear proof, however must stability benefits and harms Antibiotic treatment for children with otitis media AsshowninFigure5. No clear proof Bulk-forming laxatives for constipation Bulkforming laxatives, corresponding to methylcellulose or ispaghula husk, are used in children with constipa tion. Some attainable causes for the dearth of proof ontheuseoftheselaxativesinthiscommoncondi tionare: � constipationisnotalifethreateningdisorder � thecausesaremultifactorialandthedisease mechanismisnotclearlydefined � thereisabeliefthattherearelikelytobefew sideeffectstotheuseofbulkforming laxativesandcliniciansarepreparedto prescribethemwithoutclearevidence � thereislimitedsupportforstudiesfromthe pharmaceuticalindustry � theresearchagendaisnotdrivenbysuch clinicalproblems. Summary Evidence-based paediatrics � requiresclinicalproblemstobeframedinto questions,tosearchtheliteratureandthen appraisetheevidenceinordertomakea choice � islesswelldevelopedthaninadultmedicine � shouldbeadoptedwheneverpossible; nonetheless,clinicaldecisionsarecomplexand theevidencebaseusuallyinformsratherthan determinesclinicaldecisionmaking. This chapter outlines a primary method to the emergency managementofseriouslyillchildren.
Buy 20mg nolvadex
Permethrin cream (5%) ought to be applied beneath the neck to all areas and washedoffafter8�12h. Benzylbenzoate emulsion(25%)appliedbelowtheneckonly,indiluted formaccordingtoage,andleftonfor12h,isalsoeffec tive however smells and has an irritant action. Parasitic infestations Scabies Scabies is attributable to an infestation with the eight leggedmiteSarcoptes scabiei,whichburrowsdownthe epidermis alongside the stratum corneum. In older kids, burrows, papules and vesicles involvetheskinbetweenthefingersandtoes,axillae, flexor features of the wrists, belt line and around thenipples,penisandbuttocks. Pediculosis Pediculosis capitis (head lice infestation) is the most commonformofliceinfestationinchildren. Presentation may be itching of the scalp and nape or from figuring out reside lice on the scalp or nits (emptyeggcases)onhairs(Fig. Louseeggsare cementedtohairclosetothescalpandthenits(small whitishovalcapsules)remainattachedtothehairshaft as the hair grows. There may be secondary bacterial infection,oftenoverthenapeoftheneck,leadingtoa misdiagnosis of impetigo. Once infestation is confirmed by findinglivelice,treatmentisbyapplyingasolutionof zero. Wet combing to take away reside lice (bugbusting) every 3�four days for a minimum of 2 weeks is a helpful and secure bodily treatment, notably when parentstreatwithenthusiasm. Other childhood skin problems Psoriasis Thisfamilialdisorderrarelypresentsbeforetheageof 2 years. Afterafew days,numeroussmallerdullpinkmaculesdevelopon the trunk, upper arms and thighs. Acne vulgaris Acnemaybegin1�2yearsbeforetheonsetofpuberty following androgenic stimulation of the sebaceous glandsandanincreasedsebumexcretionrate. Thereareavarietyoflesions, initiallyopencomedones(blackheads)orclosedcome dones (whiteheads) progressing to papules, pustules, nodules and cysts. Topical treatment is directed at encouraging the skintopeelusingakeratolyticagent,suchasbenzoyl peroxide, applied once or twice day by day after washing. For more severe zits, oral antibiotic remedy with tetracyclines (only when over 12yearsold,becausetheymaydiscolourtheteethin youthful kids) or erythromycin is indicated. Alopecia areata this is a common form of hair loss in kids and, understandably,acauseofmuchfamilydistress. Hair less, single or a number of noninflamed smooth areas of skin, usually over the scalp, are present. Examples are: Granuloma annulare Lesions are usually ringed (annular) with a raised fleshcoloured nonscaling edge (unlike ringworm). Theymayoccuranywherebutusuallyover bony prominences, especially over palms and feet. Papularurticariaisadelayedhypersensitivityreac tionmostcommonlyseenonthelegs,followingabite from a flea, bedbug, or animal or bird mite. Hereditary angioedema is a uncommon autosomal domi nant disorder attributable to a deficiency or dysfunction of C1esterase inhibitor. Available free from the British Association of Dermatologists, London 25 Endocrine and metabolic problems Diabetes mellitus Hypoglycaemia Hypothyroidism Hyperthyroidism Parathyroid problems Adrenal cortical insufficiency 433 441 442 443 444 445 Cushing syndrome Inborn errors of metabolism Newborn screening Disorders presenting acutely within the neonatal interval Hyperlipidaemia 445 446 446 447 448 1 Points of notice regarding endocrine and metabolic disordersinchildrenare: Aetiology of type 1 diabetes Both genetic predisposition and environmental pre cipitantsplayarole. Inheritedsusceptibilityisdemon stratedby: � Thenumberofchildrendevelopingdiabetes mellitusisincreasing � Themostcommoncauseofhypothyroidismis congenital,whichisdetectedonroutine biochemicalscreeningshortlyafterbirth � Inbornerrorsofmetabolismareindividuallyvery rareandmanagedbyafewspecialistcentres. It has been estimatedthattheincidenceofchildhooddiabeteswill double by 2020 in developed international locations. This is most probably to be a results of adjustments in environmental risk factors, although the exact causes stay obscure. Thereisconsiderableracialandgeographicalvariation �theconditionismorecommoninnortherncountries, with high incidences in Scotland and Finland. Type2diabetesduetoinsulinresistanceis beginning to occur in childhood, as severe obesity turns into more common and in some ethnic teams. Almost all kids with diabetes have insulin-dependent (type 1) diabetes, although type 2 diabetes is more and more common. Most childhood diabetes: � Destructionofpancreaticcellsbyan autoimmuneprocess � Type 2. Insulin resistance followed later by -cell failure: � Usuallyolderchildren,obesityrelated, positivefamilyhistory,notasproneto ketosis,commonerinsomeethnicgroups. Environment one hundred% Autoimmune islet cell destruction Genes Trigger � viral infection � diet. Molecular mimicry in all probability occurs between an envi ronmentaltriggerandanantigenonthesurfaceof cells of the pancreas. Ingeneticallypredisposedindividuals,thisresults inanautoimmuneprocesswhichdamagesthepancre atic cells and leads to increasing insulin deficiency. Thereisanassociation with other autoimmune problems similar to hypothy roidism,Addisondisease,coeliacdiseaseandrheuma toidarthritisinthepatientorfamilyhistory. Diagnosis the diagnosis is usually confirmed in a symptomatic youngster by finding a markedly raised random blood Box 25. In distinction to adults,childrenusuallypresentwithonlyafewweeks of polyuria, excessive thirst (polydipsia) and weight reduction;youngchildrenmayalsodevelopsecondarynoc turnal enuresis. Advanceddiabetic ketoacidosishasbecomeanuncommonpresentation 434 Smellofacetoneonbreath Vomiting Dehydration Abdominalpain Hyperventilationduetoacidosis(Kussmaul respiration) � Hypovolaemicshock � Drowsiness � Comaanddeath. Wherethereisanydoubt,a fasting blood glucose (>7mmol/L) or a raised glyco sylatedhaemoglobin(HbA1c)arehelpful. The data provided for the kid should be appropriate for age, and updated frequently. The specialist nurse ought to liaise with the college (lecturers, those who prepare faculty meals, bodily educationteachers)andtheprimarycareteam. Thetypesofinsulininclude: Initial administration of type 1 diabetes As type 1 diabetes in childhood is rare (1�2 kids per massive secondary faculty), much of the initialandroutinecareisdeliveredbyspecialistteams (Box25. Most newly presenting kids are alert and able to eat and drink and could be managed with subcutaneous insulin alone. Inmost centres with adequate assets, kids newly pre sentingwithdiabeteswhodonotrequireintravenous therapyarenotadmittedtohospitalbutaremanaged entirelyathome. Insulin may be injected into the subcutaneous tissueoftheupperarm,theanteriorandlateralaspects ofthethigh,thebuttocksandtheabdomen. Breakfast Lunch Dinner Bedtime Snack Breakfast Continuous pump insulin Basal pump fee = blue Boluses for meals Insulin 1 2 3 four 5 6 7 8 9 10 eleven 12 13 14 15 16 17 18 19 20 21 22 23 24 Clock time 436 oftheinjectionsitesisessentialtopreventlipohyper trophyor,morerarely,lipoatrophy. Patientsandfami lies are also taught tips on how to appropriate any sugar above 10mmol/L between ordinary meal instances by additional quick appearing insulin injections. However, the input required bytheteamstostarttheseintensiveregimensishigh, asistheneedforasupportiveschoolenvironment,and somepatientsandfamiliesstillrelyontwicedailytreat mentwithpremixedinsulin. A nutritious diet is recom mended,withahighcomplexcarbohydrateandrela tivelylowfatcontent(<30%oftotalcalories). Thediet shouldbehighinfibre,whichwillprovideasustained launch of glucose, somewhat than refined carbohydrate, whichcausesrapidswingsinglucoselevels. Learning this balancing act requires lots of academic input fol lowedbyrefinementinthelightofexperience. Blood glucose monitoring Regular blood glucose profiles and blood glucose measurements,whenaloworhighlevelissuspected, are required to regulate the insulin routine and learn how adjustments in life-style, meals and train have an effect on control. A report ought to be saved in a diary or transferred from the memory of the blood glucose meter. In follow, in order also to avoid hypoglycaemic episodes, this means levels of four�10mmol/L in kids and four�8mmol/L in Hypoglycaemia Increase Omission of insulin Food (especially refined carbohydrates) Illness Menstruation (shortly before onset) Growth hormone Corticosteroids Sex hormones at puberty Stress of an operation Decrease Insulin Exercise Alcohol Some medicine Marked anxiousness/ excitement Figure 25. Continuousglucosemonitoring sensorsalsoallowthedetectionofunexpectedasymp tomaticepisodesofnocturnalhypoglycaemiaortimes of poor control in the course of the day. Blood ketone testing (often utilizing the same meter as for blood glucose) is mandatoryduringinfectionsorwhencontrolispoorto trytoavoidsevereketoacidosis. The measurement of glycosylated haemoglobin (HbA1c) is particularly useful as a information of overall control over the earlier 6�12 weeks and ought to be checkedatleast3timesperyear. Thelevelisrelatedto the chance of later problems in a nonlinear fashion, such that the chance of problems will increase more rapidlywithhigherlevels,butmaybemisleadingifthe redbloodcelllifespanisreduced,suchasinsicklecell trait or if the HbA molecule is irregular, as in thalas saemia.
Trusted nolvadex 10mg
With progressive pulmonary hypertension, the proper coronary heart will ultimately fail and proper coronary heart failure indicators and signs will develop, together with pitting edema, ascites, raised jugular vein stress, tachycardia, enlarged pulsating liver, loud P2 sound and/or pansystolic murmur, proper ventricular heave and pleural effusions. Imaging Chest radiography will help distinguish issues which will mimic signs, similar to pneumonia, tuberculosis, and coronary heart failure. In sufferers with established pulmonary hypertension, the heart configuration and the primary pulmonary arteries are often (but not at all times! Right coronary heart catheterization is currently the reference methodology for measurements of pressures, stress gradients and mixture with stress checks helps to assess the potential response to therapy. Echocardiography will reveal proper ventricular overload, consisting of proper ventricular hypertrophy, wall movement abnormalities, bowing of the interventricular septum to the left and tricuspid valve regurgitation. Echocardiography is capable of giving an estimate of the pulmonary artery stress. Nuclear Medicine Traditionally, perfusion (-ventilation) lung scintigraphy was the primary diagnostic take a look at for pulmonary vascular Hypertension, Pulmonary 923 Hypertension, Pulmonary. Notice the high septal defect, the distended proper atrium and the proper ventricular hypertrophy. Notice giant central pulmonary arteries, a number of caliber modifications within the segmental branches, in keeping with webs and stenoses after recanalization of pulmonary emboli. Nevertheless, perfusion scintigraphy continues to be considered a useful adjunct to assess the severity of pulmonary hypertension and to monitor disease development and response to therapy. Echocardiography is a primary line investigation, and can increase additional suspicion of elevated pressures and will reveal proper ventricular dysfunction. These instruments are also more and more being developed to help monitoring disease development and response to therapy. Diagnosis the prognosis of pulmonary hypertension is commonly delayed because of the insidious onset of signs. Interventional Radiological Treatment There is an, albeit limited, position for interventional radiological therapy. First, inferior vena cava filters may be inserted in sufferers who bear surgical corrections. Only the stenoses that cut back the interior diameter by >60% produce a significant lower in renal blood flow. They may be atherosclerotic (ninety% of cases) or dysplastic (fibromuscular dysplasia, 10% of cases), ostial or not, and be situated on primary or accessory arteries. Figure 4 Perfusion scintigraphic findings in several etiologies of pulmonary hypertension. Notice that there are a number of wedge-shaped defects, similar to that seen in acute pulmonary embolism. The lungs present inhomogeneous tracer uptake, with photopenic central hilar areas because of pulmonary artery dilatation. Notice that the kidneys are seen; quantification of the shunt may be carried out by calculating the precise uptake as a share of the entire injected dose. J Magn Reson Imaging 22:sixty seven�72 Hypertension, Renal 925 atherosclerotic arterial disease, atheroembolism, diabetes, elevated oxidative stress, medullary hypoxia, endothelial dysfunction, inflammatory response, and proteinuria. This multiplicity of causal components explains the great heterogeneity of renal injury. Characteristics Clinical distinction between renovascular and important hypertension is difficult and based on classical criteria similar to, amongst others, the onset of hypertension earlier than or after the age of fifty years, the absence of a family historical past of important hypertension, an belly bruit, duration of hypertension of less than 1 year, hypokalemia, and decreased renal function (Table 1). The prevalence will increase with age, significantly in sufferers with diabetes, aorto-iliac occlusive disease, Hypertension, Renal. Hypertension � Abrupt onset earlier than the age of fifty year or after the age of 55 year � Accelerated or malignant hypertension � Refractory to therapy with three medication 2. Other findings � Abdominal or flank bruit � the presence of various atherosclerotic manifestations and/or belly aortic aneurysm � Unexplained left ventricular hypertrophy � Flash pulmonary edema � Severe retinopathy coronary artery disease, or hypertension. Progression of the diploma of stenosis occurs in approximately 51% of renal arteries 5 years after prognosis, and three�sixteen% of renal arteries progress towards occlusion. Most of those stenoses are situated at the ostium of the renal arteries and are actually perirenal aortic plaques extending into the ostia. When atherosclerotic disease progresses unilaterally, the scale of the ipsilateral kidney, its cortical thickness, and its blood flow lower, whereas the serum creatinine concentration and glomerular filtration rate remain normal due to compensatory modifications inside the contralateral kidney. When the disease progresses bilaterally, both kidneys current with progressive shrinkage and cortical thinning and irregularities. Because the cardiovascular threat mainly depends on the diploma of hypertension, improving blood stress control has been a significant task. Today, we all know that medical therapy can obtain this control with out renal revascularization in lots of cases. The examination consists of measurement of both kidneys, spectral sampling of two or three interlobar or segmental arteries of every kidney, and spectral sampling of both renal arteries. Ultrasound distinction brokers might improve the feasibility of the take a look at in sufferers with a high body mass index or with decreased renal function. Sensitivity (92%) and specificity (99%) in detecting vital stenoses are high. Fluoroscopic steering of arrival of the bolus within the aorta improves the reproducibility of the approach. Parallel acquisition methods allow improved spatial decision with out rising the acquisition time and yield an isotropic decision of 1 mm3 in a single breath-maintain. These improvements are responsible for an improved grading of stenoses, which has the identical interobserver variability as conventional angiography, and better detection of accessory arteries. A renal flow index-renal flow (mL/min) divided by renal volume (cm3)-less than 1. Renal Anatomy modifications the renal anatomy modifications when the renal blood flow is significantly decreased. If the renal length is <eight cm, revascularization is contraindicated as a result of the affected person is much less more likely to get profit from it. Measurement of cortical thickness and cortical area: A threshold of eight mm for cortical thickness and 800 mm2 for cortical area permits one to distinguish control kidneys from poststenotic kidneys. It is possible to separate normal velocity�time curves and abnormal curves evocative for average or high grade stenoses. After captopril, the proper kidney reveals a normal tubular part (arrow) and normal excretion (double arrow) whereas tubular part is delayed on the left but then enhances with time, extending inside the cortex and providing a complete low sign depth of the left kidney; this effect is said to a severe retention of the distinction agent inside the whole left kidney induced by captopril. Hyperthyroidism the physiological manifestation of elevated thyroid function, hormone manufacturing or insensitivity of the top organs to thyroid hormone. Congenital malformations, Thyroid, and Functional Disorders Thyroid Autoimmune Diseases Renal Perfusion Absolute quantification of parenchymal perfusion may be assessed with diffusible (as gadolinium chelates) or purely intravascular distinction brokers (as iron oxide particles). A 50% lower in cortical perfusion (from 400 to 200 mL/ min/a hundred g) has been noticed below tight (80%) stenoses. Hypertrophic Arthropathy, Secondary Secondary hypertrophic arthropathy is one of the extra frequent and specific paraneoplastic ailments which will current as an oligoarthritis or polyarthritis of the distal joints with clubbing, painful periostitis of the distal long bones, and noninflammatory synovial effusions. Linear ossification of the distal long bones separated by a radiolucent zone from the underlying cortex may be seen in radiographs. Ann Intern Med 135:401�411 Radermacher J, Chavan A, Bleck J et al (2001) Use of Doppler ultrasonography to predict the result of therapy for renal artery stenosis. Hypertrophic, Osteoarthropathy 929 Hypertrophic Pyloric Stenosis Thickening of the muscle wall and mucosa within the pylorus of the stomach resulting in gastric outlet obstruction and typically occurring in younger infants and resulting in traditional projectile vomiting. Figure 1 Radiograph of the proper distal tibia and fibula in an anteroposterior and lateral view. The affected person suffered from lung cancer and severe, burning ache in both distal legs. The periosteal appositions (white) have a linear appearance typically present in secondary hypertrophic osteoarthropathy. Primary hypertrophic osteoarthropathy may be hereditary or idiopathic and may be very rare (three�5% of all cases of hypertrophic osteoarthropathy). Secondary hypertrophic osteoarthropathy is commonly related to intrathoracic neoplastic or inflammatory conditions. Pathology/Histopathology Periostitis with new periosteal deposition of bone is the hallmark of the disease. While the brand new surface is tough in primary hypertrophic osteoarthropathy, it has a extra linear appearance in secondary hypertrophic osteoarthropathy. In histologic cross sections, the delineation between the old and new periosteal bone is much less distinct in primary in comparison with secondary hypertrophic osteoarthropathy, the place the brand new bone is commonly much less dense than the unique cortex.
Citronella Oil. Nolvadex.
- What is Citronella Oil?
- Worm infestations, fluid retention, spasms, and other conditions.
- Preventing mosquito bites when applied to the skin. Citronella oil is an ingredient in some commercial mosquito repellents. It seems to prevent mosquito bites for a very short amount of time. Other mosquito repellents, such as those containing DEET, are usually preferred because these repellents last much longer.
- What other names is Citronella Oil known by?
- Are there safety concerns?
- Dosing considerations for Citronella Oil.
- How does Citronella Oil work?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96619
Safe nolvadex 20 mg
Ampicillin is principally indicated for the treatment of exacerbations of chronic bronchitis and middle ear infections. Co-amoxiclav consists of amoxicillin with the -lactamase inhibitor clavulanic acid, which extends the spectrum of activity of amoxicillin. The mixture has activity in opposition to many Gram-constructive and Gram-adverse pathogens and anaerobes including Pseudomonas aeruginosa. Flucloxacillin Capsules: 250 mg, 500 mg; Solution: 125 mg/5 mL, 250 mg/5 mL; Injection: 250 mg vial. Amoxicillin Capsules: 250 mg, 500 mg; Suspension: 125 mg/5 mL, 250 mg/5 mL; Injection: 250 mg vial. Side effects Hypersensitivity reactions embody urticaria, fever, rashes and anaphylaxis. Encephalopathy with fits results from excessively excessive doses or in patients with extreme renal failure. Other effects are interstitial nephritis, hepatitis, cholestatic jaundice, reversible neutropenia and eosinophilia. Cautions/contraindications Contraindicated in penicillin hypersensitivity (see above); macrolides are an alternative in these patients. Therapeutics sixty three Cephalosporins Mechanism of action Cephalosporins inhibit bacterial wall synthesis in a way just like the penicillins. Indications Broad-spectrum antibiotics � used for treatment of septicaemia, pneumonia, meningitis, biliary tract infections, peritonitis and urinary tract infections. Succeeding generations are likely to have elevated activity in opposition to Gram-adverse bacilli, often on the expense of Gram-constructive activity, and elevated capability to cross the blood� brain barrier. Cefuroxime Tablets: 125 mg, 250 mg; Suspension: 125 mg/mL; Injection: 250 mg, 750 mg, 1. Cautions/contraindications Penicillin hypersensitivity apart from with a minor rash solely. Indications Aminoglycosides are lively in opposition to many Gram-adverse bacteria (including Pseudomonas species) and some Gram-constructive bacteria however are inactive in opposition to anaerobes. Aminoglycosides are often used for serious Gram-adverse infections after they have a complementary and synergistic action with agents that disrupt cell wall synthesis. Preparations and dose Examples: gentamicin (the most broadly used), amikacin, neomycin, netilmicin, streptomycin, tobramycin. Side effects Most unwanted effects are dose associated and are in all probability associated to excessive trough concentrations of the drug. Ototoxicity can lead to both vestibular and auditory dysfunction, which lead to often irreversible disturbances of stability or deafness. Other side effects are renal toxicity, acute neuromuscular blockade, nausea, vomiting, rash and antibiotic-associated colitis. Cautions/contraindications Aminoglycosides are contraindicated in myasthenia gravis. Monitor serum concentrations in all patients and reduce the dose in renal impairment. In patients with normal renal operate, serum aminoglycoside concentrations should be measured after three to four doses (earlier and extra frequent measurements in patients with renal failure), 1 hour after i. Macrolides Mechanism of action Macrolides interfere with bacterial protein synthesis by binding reversibly to the 50S subunit of the bacterial ribosome. Azithromycin has barely less activity than erythromycin in opposition to Gram-constructive bacteria however enhanced activity in opposition to Gram-adverse bacteria. Preparations and dose Clarithromycin Tablets: 250 mg, 500 mg; Injection: 500 mg vial. Oral 250 mg every 12 hours; elevated in extreme infections to 500 mg every 12 hours. Side effects Gastrointestinal upsets (epigastric discomfort, nausea, vomiting and diarrhoea) are common with the oral preparation of erythromycin; azithromycin and clarithromycin are higher tolerated. Erythromycin and clarithromycin inhibit P450 drug-metabolizing enzymes and might elevate levels of drugs. Only some anaerobes and some protozoa contain the enzyme (nitroreductase) that converts metronidazole to its toxic metabolite. Indications Anaerobic infections, protozoal infections, Helicobacter pylori eradication, C. Preparations and dose Metronidazole Tablets: 200 mg, 400 mg; Suspension: 200 mg/5 mL; Intravenous infusion: 5 g/5 mL; Flagyl suppositories. Oral 400 mg every 8 hours; for surgical prophylaxis, 400 mg earlier than surgery and three further doses of 400 mg every 8 hours for high-risk procedures. Side effects Nausea, vomiting, metallic taste, disulfiram-like response (unpleasant hangover symptoms) with alcohol, pores and skin rashes, and abnormal liver biochemistry. With prolonged remedy, peripheral neuropathy, transient epileptiform seizures and leucopenia can happen. Cautions/contraindications Caution with alcohol ingestion; reduce dose in extreme liver disease and keep away from in porphyria. Indications Ciprofloxacin has a broad spectrum of activity and is especially lively in opposition to Gram-adverse bacteria. Ciprofloxacin Tablets: 100 mg, 250 mg, 500 mg, 750 mg; Suspension: 250 mg/5 mL; Intravenous infusion: 2 mg/mL. Cautions/contraindications Contraindicated in patients with a history of tendon problems associated to quinolone use; risk of tendon rupture is elevated by corticosteroids. Dyspeptic symptoms are brought on by problems of the oesophagus, stomach, pancreas or hepatobiliary system, however the most common cause is practical dyspepsia. Other causes embody peptic ulceration, gastro-oesophageal reflux disease or not often a gastro-oesophageal most cancers. Dysphagia Dysphagia is issue in swallowing and suggests an abnormality within the passage of liquids or solids from the oral cavity via the oesophagus and into the stomach. Vomiting Vomiting happens as a result of stimulation of the vomiting centres within the medulla. This might result from stimulation of the chemoreceptor set off zones or from intestine vagal afferents. Vomiting is associated with many gastrointestinal circumstances, however nausea and vomiting with out belly ache are incessantly non-gastrointestinal in origin. Persistent nausea and vomiting with out some other symptoms can also be practical in origin (p. Extrinsic pressure Mediastinal glands Goitre Enlarged left atrium Intrinsic lesion Benign stricture Malignant stricture Oesophageal internet or ring Foreign physique Pharyngeal pouch Flatulence Flatulence describes extreme wind, presenting as belching, belly distension and the passage of flatus per rectum. Diarrhoea and constipation these are common complaints and never often as a result of serious disease. Diarrhoea implies the passage of elevated amounts of free stool (stool weight >250 g/24 h) (p. This must be differentiated from the frequent passage of small amounts of stool (that patients often discuss with as diarrhoea), which is usually seen in practical bowel problems. Steatorrhoea Steatorrhoea is the passage of pale cumbersome stools that contain fat (>17 mmol or 6 g per day) and signifies fat malabsorption as a result of small bowel, Investigation of gastrointestinal disease 69 pancreatic disease (resulting in lipase deficiency), or cholestatic liver/biliary disease (resulting in intestinal bile salt deficiency). The stools are offensive, often float because of elevated air content and are troublesome to flush away. They are in a position to distinguish natural from non-inflammatory practical disease with excessive diagnostic accuracy. The tip of the endoscope can be angulated in all directions and channels within the instrument are used for air insufflation, water injection, suction, and for the passage of equipment similar to biopsy forceps or brushes for acquiring tissue, snares for polypectomy and needles for injection therapies. Mucosal biopsy is usually an integral a part of the examination; a number of biopsies (8�10) are taken in suspected most cancers to reduce sampling error and a false-adverse result. Patients quick for 6 hours prior to the process and must not drive for 24 hours after intravenous sedation. Duodenal biopsies can be obtained to establish a analysis of coeliac disease, and therapeutic choices embody arresting higher gastrointestinal bleeding, dilatation of oesophageal strictures and stent insertion for palliation of oesophageal malignancy. Sigmoidoscopy that is carried out with a inflexible instrument to look at the rectum and distal sigmoid, or with a versatile instrument to look at the whole of the left colon. Intravenous analgesia (with fentanyl) and sedation (with midazolam) could also be required. Colonoscopy is helpful for the investigation of patients with altered bowel habit, rectal bleeding or as a screening software for colorectal most cancers. Therapeutic choices embody removal of polyps (polypectomy) or diathermy of bleeding lesions similar to angiodysplasia. Perforation happens in 1: one thousand examinations, however that is greater (as much as 2%) after polypectomy and endoscopic mucosal resection.
Trusted 10 mg nolvadex
This picture is a derivative work, adapted from the following supply, out there under Yale Rosen. See also Insulin Detrusor instability, 569 Developmental delays renal failure and, 571 Developmental milestones, 258 Dexamethasone. See Growth-hormonereleasing hormone Giant cell arteritis, 302 Giant cell pneumonia, 166 Giant cells in persistent inflammation, 207 Giant cell tumors, 438 Giant cell tumors of bone, 660 Giardia spp watery diarrhea, a hundred seventy five Giardia lamblia, 151 Giardiasis, 151 Giemsa stain, 122 Borrelia, 142 chlamydiae, 146 Gigantism, 317, 333 Gilbert syndrome, 376, 377 Gingival blue line, 652 Gingival hyperplasia calcium channel blockers, 304 cyclosporine, 116 as drug reaction, 241 epilepsy medicine and, 514 Gingivostomatitis, 160 Gitelman syndrome, 556 markers in, 560 Glans penis, 593 cancer of, 617 lymphatic drainage of, 591 Glanzmann thrombasthenia, 393, 405 Glargine insulin, 340. Tao subsequently went on to cofound Medsn, a medical training technology venture, and served as its chief medical officer. He is at present chief of adult allergy and immunology on the University of Louisville. His eclectic pursuits embody technology, data design, pictures, South Asian diasporic tradition, and avoiding a day job. Always discovering the lengthy shortcut, Vikas is an adventurer, information seeker, and occasional innovator. He enjoys novice standing as a kiteboarder and single father, and strives to increase his kids as global residents. He completed medical school in 2013 at Brown University and is a 2008 graduate of the University of Massachusetts, Amherst, the place he studied biochemistry and the classics. Pastimes embody snowboarding, cooking/baking, touring, the company of pals/loved ones (especially his great wife), the Spanish language, and laptop/video gaming. Yash has many pursuits outside of medicine and enjoys spending time together with his loved ones. He is a developing photographer, former net/graphic designer (who nonetheless dabbles), video gamer, foodie, and avid explorer who desires to travel the world (whenever he truly will get an opportunity). He was born in Karachi, Pakistan, grew up in Toronto, Canada, and pursued medication upon completing high school. In his restricted leisure time, Mehboob enjoys playing or watching soccer, lengthy drives, and family gatherings. Andrew Zureick Andrew is a medical scholar on the University of Michigan and is at present conducting analysis in radiation oncology. In his spare time, he enjoys playing the piano, golf, tennis, and inventive writing. The matters range from writing fashion to the completion of required forms and the fee of fees. The majority of students submit an digital model of their thesis or dissertation to the Graduate School. There are instructions on the Graduate School web site for guidance via this course of. Style There is a definite distinction between submitting a manuscript to a writer and offering a completed thesis or dissertation to the Graduate School. A manuscript represents a pre-publication format; a thesis or dissertation is a ultimate, utterly edited, revealed document. Students ought to use these pointers, not other fashion manuals, as the final authority on problems with format and style. Areas not covered in this document or deviation from any of the specifications ought to be discussed with a Graduate School format editor. Do not use previously accepted theses and dissertations as particular models for fashion. Composition and Structure Manuscripts consist of four major sections and ought to be placed in the order listed: Preliminary Pages Title Page (required) Copyright (elective, Ph. The maximum size of the dissertation abstract is 350 phrases, together with the dissertation title. Spacing between text on the title page will range according to the size of the title. Sample title pages, together with one revised for digital submission, are on pages 15-sixteen. It is permissible to change level dimension in tables, figures, captions, footnotes, and appendix material. Italics are acceptable for book and journal titles, international terms, and scientific terminology. Boldface may be used inside the text for emphasis and/or for headings and subheadings. Margins Measure the top margin from the sting of the page to the top of the primary line of text. Measure the underside page margin from the underside of the final line of text to the underside fringe of the page. Page margins ought to be a minimum of 1-half inch from top, backside, left and proper. Right margins may be justified or ragged, depending upon departmental necessities or scholar preference. Block quotations, footnotes, endnotes, table and figure captions, titles longer than one line, and particular person reference entries may be single-spaced. Double spacing ought to comply with chapter numbers, chapter titles and major section titles (Dedication, Acknowledgements, Table of Contents, List of Tables, List of Figures, List of Abbreviations, Appendices, and References). Double spacing should also occur before every firstlevel and second-degree heading, and before and after tables and figures embedded in the text. Numbering Schemes Chapters may be identified with uppercase Roman numerals or Arabic numbers. Tables, figures, and equations ought to be numbered consecutively all through the manuscript with Arabic numerals. Equation numbers ought to be placed to the proper of the equation and contained within parentheses or brackets. Utilize this function to assist in the proper division of sentences from one page to another. Headings and Subheadings Use headings and subheadings to describe briefly the material in the section that follows. Be constant with your choice of "ranges" and refer to the instructions on spacing, above, for proper spacing between headings, subheadings, and text. Acronyms/Abbreviations/Capitalization Abbreviations on the title page ought to appear as they do in the physique of the thesis or dissertation. Capitalize only the primary letter of phrases of significance, distinction, or emphasis in titles and headings. Use the traditional fashion for Latin phrases (Examples: in vitro, in vivo, in situ). Capitalize the primary letter of the Genus, however not that of the Species name (Example: Streptococcus aureus). Tables and Figures Figures commonly refer to pictures, photographs, maps, charts, graphs, and drawings. These items ought to appear as close as attainable to their first mention in the text. Tables and figures may be placed in appendices, if this can be a departmental requirement or normal in the field. Tables and figures ought to be numbered with Arabic numerals, both consecutively or by chapter. Table knowledge and figure knowledge should be stored collectively, if the data suits on one page. These instructions permit the pc to proper align the page numbers and accurately place the "dots". The title of the thesis or dissertation ought to be written in the international language on the title page and abstract. Multi-Part and Journal Article Format A multi-half presentation format may be used for combining analysis that has been conducted in two or extra associated or non-associated areas, or for presentation of combined journal articles (revealed or submitted for publication). Each dissertation ought to embody the appropriate preliminary pages, an introduction presenting the final theme of the analysis and literature review, and a conclusion summarizing and integrating the main findings. Each "chapter" ought to include nicely-outlined "subheadings," corresponding to introduction, methods, outcomes, and discussion. Tables and figures ought to be placed inside the text, not on the end as is customary in articles prepared for journal publication. Permission to Use Copyrighted Material the standard provisions of copyright laws regarding quoted material under copyright apply to digital publication.
Safe nolvadex 20mg
Some syndromes such as radiologists are involved with imaging interpretation and with supervision of juniors in training. Pathology and Histopathology Hemangioma Hemangioma is the most typical benign primary neoplasm of the spleen. It arises from the sinusoidal epithelium, normally appearing on gross examination as a small, encapsulated, intraparenchymal bluish-pink spongy tumor. Histopathologic analysis reveals a nonencapsulated proliferation of vascular channels of variable dimension, ranging from capillary to cavernous, which are lined with a single layer of endothelium crammed with pink blood cells. Areas of infarction, hemorrhage, thrombosis, and fibrosis may be noticed inside the lesion (1, 2). Interventional Radiological Treatment Interventional radiology is basically for potential intervention with intraarterial chemotherapy in specific circumstances or embolization prior to surgery to lower blood loss. Eur Radiol 14(three):506�513 Hamartoma Hamartoma is a rare benign lesion consisting of an anomalous combination of normal splenic pink pulp elements. Microscopically it seems as a combination of unorganized vascular channels lined by endothelial cells and surrounded by fibrotic cords of predominant splenic pink pulp. Focal necrosis, cystic components, and minute calcifications may be noticed inside the lesion (1, 2). These lesions are inclined to occur in subcapsular areas, reflecting the anatomic distribution of splenic lymphatics. On minimize part, lymphangiomas range in appearance and may include large macroscopic interconnecting cysts (cystic lymphangioma) or microscopic cysts (cavernous lymphangioma). Histologically, lymphangioma consists of multiple endothelium-lined vascular channels crammed with eosinophilic proteinaceous materials. The supporting stroma consists of collagen and may include lymphocytes and lymphoid aggregates (1, three). N 2nd Department of Radiology, University Hospital of Pisa, Pisa, Italy 2 Department of Diagnostic and Interventional Radiology, University of Pisa, Pisa, Italy p. This very rare neoplasm has attribute morphologic and immunophenotypic features (vascular and histiocytic antigens) that distinguish it from different vascular splenic tumors. Morphologically it consists of multiple nodules composed of vascular channels 1310 Neoplasms, Splenic, Benign of pink pulp and normally involves the spleen in a diffuse method, though a focal type has been described (four). Hemangiopericytoma Hemangiopericytoma is a rare neoplasm with a comparatively high-malignant potential. Gross examination reveals a well-defined, stable tumor with a pseudocapsule, which has a wealthy vascularization. At histopathologic analysis, pericytes proliferating around vascular channels lined with endothelium are noticed (1). Hemangioendothelioma Hemangioendothelioma is a very rare primary vascular tumor of the spleen and has variable malignant potential. Hemangioendotheliomas are well-circumscribed and nonencapsulated stable splenic masses. Microscopically, hemangioendothelioma consists of vascular and stromal elements, and a number of other histologic patterns, ranging from well differentiated to extremely undifferentiated, have been described (1). Splenic Cysts Cysts are relatively common benign splenic lesions and can be divided into primary or true cysts and secondary or false cysts based on their etiology and pathophysiology. Primary cysts have a cellular lining and can be brought on by either a congenital occasion (epithelial cyst) or parasitic infestations (hydatid cyst). However, bigger and multiple lesions may manifest with splenomegaly and belly ache. Thrombocytopenia, anemia, and coagulopathy may occur from sequestration of hematopoietic cells either in large hemangiomas (Kasabach-Merritt syndrome) or hamartomas, whereas malignant degeneration has been reported in splenic hemangiopericytoma and hemangioendothelioma. Associations between a number of benign splenic tumors and generalized multisystem issues such as tuberous sclerosis, Wiskott�Aldrich syndrome, lymphangiomatosis and Klippel�Trenaunay�Weber syndrome, have been not often reported (1, 2, three). However, high T1 sign depth due to inside bleeding or to the proteinaceous nature of the intracystic fluid can also be noticed. The fibrous septa appear as hypointense bands on each T1- and T2-weighted images (1). On ultrasound, splenic hemangioma seems as a well-defined hyperechoic nodule (a). Littoral Cell Angioma Sonographic characteristics of littoral cell angioma embody splenomegaly with a diffuse heterogeneous echo texture of the spleen. This focal lesion shows high blood flow on color Doppler ultrasound (a, b), reflecting the hypervascularity of the pink pulp inside the hamartoma. Diagnosis Although benign focal lesions of the spleen are relatively unusual, they have to be correctly characterised and differentiated from malignancies. A cystic lesion normally reveals a fluid content and a well-defined outline without stable components, however dependable differentiation between primary and secondary cysts is normally not possible at imaging. The characterization of the opposite benign lesions, including splenic hemangioma, hamartoma, and a number of other rare vascular tumors, is normally tough. Although the most typical hypervascular mass in an asymptomatic affected person is splenic hemangioma, the imaging appearance of that lesion is commonly complicated, and differentiation from hamartoma or malignancies, significantly angiosarcoma, may not be possible. Large subcapsular solitary lobulated cystic abnormalities discovered incidentally in pediatric patients are typical for lymphangioma; nevertheless, differential diagnosis can also embody echinococcal or different splenic cysts. In conclusion, a number of imaging modalities are necessary to enhance focal splenic lesion characterization and position out malignancies. However, splenectomy is important for definitive analysis of a splenic mass with atypical imaging features (1). Nonenhanced computed tomography scans (a, b) show a spherical, low-attenuating cystic splenic lesion with multiple daughter cysts and peripheral calcifications. No enhancement is seen within the lesion after intravenous contrast materials administration (c, d). Radiographics 24:1137�1163 Robertson F, Leander P, Ekberg O (2001) Radiology of the spleen. Radiographics sixteen:107�129 Definition Malignant neoplasms of the spleen embody primary lymphoreticular tumors (lymphomas and persistent myeloproliferative issues), primary nonlymphoreticular tumors (hemangiosarcoma, leiomyosarcoma, and fibrosarcoma), and splenic metastases. Pathology and Histopathology Lymphoma Splenic lymphoma is the most typical malignant tumor of the spleen and can be primary (when limited to the spleen and hilar lymph nodes) or secondary (when the spleen is involved as a part of a disseminated disease). Grossly, an enlarged spleen with one or more intraparenchymal tumor nodules, typically lower than 1 cm in diameter, is normally noticed; nevertheless, a diffuse, infiltrative tumor development and single large lesions have also been described. Generally, malignant lymphomas show a homogeneous, extremely cellulated histologic construction missing fibrous septa (1). All of those issues are thought to outcome from a hematopoietic stem cell lesion. However, nonspecific signs (fever, weight loss, and night sweats) due to the systemic disease are normally also noticed (1, 2). Chronic Myeloproliferative Disorders Hemangiosarcoma Although very rare, splenic hemangiosarcoma is the most typical nonlymphoreticular malignant tumor of the spleen. It arises from splenic sinus endothelial cells, and at gross examination it normally seems as a big, poorly defined, nodular pink mass diffusely involving the spleen. Microscopically the tumor consists of irregular anastomosing vascular channels lined by malignant endothelial cells. The persistent myeloproliferative issues are persistent diseases that typically convert to an acute myeloid leukemic part. Most patients are over 60 years of age at diagnosis, and one-third of patients are asymptomatic at presentation. Hemangiosarcoma Unlikely hepatic hemangiosarcomas, no associations with exposure to thorium, vinyl chloride, or arsenic have been noticed. The most frequent medical findings are splenomegaly, belly ache, fever, fatigue, weight loss, anemia, and consumptive coagulopathy. Major problems embody rupture of the spleen, which often leads to deadly hemoperitoneum. The lymphatic system, liver, lungs, and bone are probably the most frequent metastatic sites. Leiomyosarcoma Splenic leiomyosarcoma is a particularly rare nonlymphoreticular malignant tumor that originates from muscular cells. Even in poorly differentiated examples, actin and myosin are current within the tumor cells (three).
References:
- https://multimedia.3m.com/mws/media/795755O/toxic-anterior-segment-syndrome-may2012.pdf
- http://www.parentsmedguide.org/ParentGuide_English.pdf
- https://www.faa.gov/data_research/research/med_humanfacs/oamtechreports/2000s/media/200623.pdf
- https://internal.medicine.ufl.edu/files/2012/07/5.18.03.01.-Gluten-Free-Diet-review.pdf
- https://www.avma.org/sites/default/files/resources/javma_221_10_1413.pdf