.png)
Cefuroxime 250mg
Insurers such as the Washington Dental Service need to target assets appropriately. This in flip may minimize more pricey complications as a result of} superior disease (bridges, partials, dentures, implants) and contribute to improved oral quality of life for sufferers. If it has value in letting dentists know which sufferers will want care in the future, why not authorize and provide treatment now? Slavkin favors the next analogy: "Like the Periodic Table of Elements from the 19th century, the Human Genome Project is without values per se, but raises profound ethical points concerning the makes use of of this information base. Marks her medical and dental historical past and genetic information on a conveyable health card with a computer chip. In any case, neither supply will allow copying or a printout for security and authorized purposes, although reports of bypassing technology floor. From it they develop tests utilizing organisms like yeast and lab animals, and sometimes plan to put them by way of clinical trials on people. Dentists at some point could supply or even recommend sufferers take tests that go nicely past dental diseases. Patients could come into the workplace already having taken such a take a look at at one other medical or dental workplace and know the total spectrum of their health-related susceptibilities. Marks" may see a brand new} fifteen-year-old dental patient, Sophia, who made her appointment through the Internet. Marks she has the gene for juvenile onset periodontal disease, to not mention alcoholism, "which suggests I have have} to stop at two drinks, or else" she opines, sighing with adolescent drama. However, after reading about full-site hackings utilizing passwords, she decided would see it, expediency will trump public opinion. Surabian stated he has noticed a development in a loosening of privateness safeguarding, "Our nation became diverted from the limitation for widespread generalized use of the social security quantity. But Americans have a responsibility to hold informed as to Journal of the American College of Dentists 2003 19 Implications of the New Biology ities and alert the doctor to any significant points to evaluation, or order up prior take a look at outcomes and digital images-also stored on the net. Genetic susceptibilities for circumstances corresponding to oral most cancers and periodontitis could also be} info shared among family members. Likewise, he doubts that a dental genetic specialty group would in a position to|be capable of|have the power to} acquire acknowledged dental specialty status. The National Coalition for Health Professional Education in Genetics is developing a device for eliciting a comprehensive, multigenerational household historical past. More and more, health care suppliers shall be making judgments about genetic take a look at outcomes. Computer programs could even be created that assign weights to risk components (including genes and residential hygiene pattern), disease, treatment, therapy administered, and genetic reception to that therapy. Genes responsible for defective tooth enamel formation, decreased salivary gland operate, and immune dysfunction and others are related to caries. After all of the gamers are decided in the subsequent few years, researchers can study method to|tips on how to} modulate the cascade to enhance therapeutic in reconstructive surgery, change operate, and more. Likewise, he thinks there may be geneticists with special knowledge of oral health. Activities eligible for funding embrace developing courses, conferences, and curriculum tons of|and lots of} other means for bettering professional and lay understanding about genetics, related technology, and its ethical, authorized and social implications. James Lipton, assistant director of the workplace, may be reached at(301)594-2618 or James Lipton@nih. Dental researchers are working at a breakneck pace to study not solely genetic susceptibilities, but additionally pharmacogenetics and tissue engineering/biomimetics in vitro and in vivo. In his analysis on laboratory animals, he has proved his theory and already transferred therapeutic genes to salivary glands with good outcomes. He has used this method to repair irradiationdamaged salivary glands, kill an azole-resistant Candida species utilizing a therapeutic course of gene expression (ten to fourteen days). The glands then can produce and secrete "transgene-encoded proteins" systemically so that they circulate in the bloodstream to deal with sure single-protein deficiency diseases corresponding to human growth hormone deficiency or hemophilia. If salivary gland gene switch proves highly efficient and efficient, not just for oral disease but additionally as a modality for therapeutic gene switch for systemic disease in people, chance of|the potential of|the potential for} dentists administering gene therapy for health purposes past the oral cavity is real. Besides injection into the salivary glands, genes may be injected into the mucosa, gingivae, tongue and muscula- ture. The gene supply has typically been developed to mimic the ways in which viruses invade cells; adenoviruses are superb at coming into oral and nasal cells. Meanwhile, antagonistic effects do appear in clinical trials, and common public} needs to understand that clinical trials for lifethreatening diseases do have dangers. Everything else is made from somatic cells, and each somatic cell contains the same human genome encased in twenty-three pairs ofchromosomes. Gene-mediated therapy may be performed in germ somatic Dental researchers are working at a breakneck pace to study not solely genetic susceptibilities, but additionally pharmacogenetics and tissue engineeringlbiomimetics in vitro and in vivo. In 1999, Jesse Gelsinger, an eighteen-year-old student on the University of Pennsylvania died from a poisonous response 4 days after beginning experimental gene therapy treatment. His liver had been injected with virus-bearing genes to appropriate his genetic liver disorder. Still, this system was quickly halted, and federal and Congressional scrutiny has begun in the fledgling area. Slavkin sees the accident this way: "In important clinical analysis, individuals can die and do die. In the case of the teenager in Pennsylvania, all accounts indicate poor handling of the clinical cells. The gene-mediation could final for days or weeks weeks|days or even weeks}, or may final for a lifetime if inserted in to stem cells. There is consolation in understanding if therapy for a potential problem linked to a polymorphism is botched or if unwanted side effects effects} emerge, the gene therapist should in a position to|be capable of|have the power to} change off the gene or carry out therapy with the other impact to reverse course-even if it was to be a "permanent change" to stem-type somatic cells. Integrating With Medicine In the era of biodentistry, lengthy run} model of the dental practice is being debated. Parts of dentistry will probably Journal of the American College of Dentists 2003 21 Implications of the New Biology overlap with drugs, as they do now. Many assume that dental practices that provide genetic testing for a number of systemic diseases past oral diseases shall be "networked" with genetic counseling and treatment. Perhaps common dentists will nonetheless be solo or group practitioners who check with specialists. Or maybe dentists will turn out to be part ofa broader group health model-the multidisciplinary health clinic owned by one health care system that provides a full vary of providers: medical, nursing, dental, podiatric, ophthalmic, obstetric/embryology, pediatric, audiology, oncology, and so on. At such a website, genetic tests for every aspect of human health shall be provided with genetic and psychological counseling as nicely. The idea is to provide a full-spectrum of health care suppliers within close proximity to more simply deal with the patient along a seamless continuum of care. In truth, in mation from all dental colleges on how a 1998 study on offering genetic take a look at many clock hours they spend on primary outcomes reported in a Journal of the science and clinical science. American Medical Association article, "We have a graph with totally different disonly one in five sufferers received the ciplines within primary science. The imply average variety of clock Genetics Curriculum In a New England Journal of Medicine hours of genetics taught during dental report years ago, physicians had school for all colleges is thirteen. The Survey Center lately surveyed misinterpreted one-third of predictive dental colleges again. Physicians want more genetic training and so do are released later this 12 months, it is going to be|will probably be} interesting to see if genetics is taught in dentists. The first primary genetic course anybody more colleges and coated more thorcan recall being provided in a dental oughly. Rachel Morrissey, supervisor of educa- lishing genetics analysis articles but tion and institutional surveys on the have yet to produce any consensus statements or patient schooling materials on Genetic Web Sites · the National Human Genome Research Institute: By 2010, all dentists will understand how Both dental colleges and professional how these competencies could be be} inteto interpret genetic take a look at outcomes and their societies must play a central function in edu- grated into their curricula. At the same time, present Leaps in science and technology knowldental professionals want schooling and edge imply the completed map of the Conclusion updates on "the rising importance, human genome shall be completed forward this article discussed the adjustments and benefits, and dangers for his or her sufferers of of schedule. Originally set for 2005, challenges in how oral health will soon genetic info and gene-based researchers are now are|are actually} saying 2003 is an actual be managed in the rising era of therapies," Tabak stated. The precept of genetic problem a set ofcore competencies in genetWhat researchers can sequence in one manipulation to counter cellular growing older ics that will outline the minimal minute at present, took twenty minutes is yet another vista for analysis. Our knowledge, abilities, and attitudes necesthree years ago,and a 12 months or more twen- genome-a genetic thumbprint-will sary for health professionals, including provide health professionals with the ty years ago.
Buy cefuroxime 500 mg
Microcirculatory dysfunction and defects in oxygen utilization at the mobile degree may play a job in hypoxia. Shock affects a number of} organ techniques, and early recognition of the indicators and symptoms of shock may aid in lowering morbidity and mortality. As an example, as many as one-third of patients in septic shock even have a point of myocardial dysfunction, and post-cardiac surgical procedure patients may endure from postcardiopulmonary bypass vasoplegia along with cardiogenic shock. The classification, along with particular pathologic subtypes, is as follows in Figure 1 and Table 2. Initial administration could be broadly separated into institution of efficient circulating quantity, achievement of an adequate minimum blood strain, optimization of cardiac operate, and restoration of oxygen supply. Hypovolemic Shock Characterized by low filling pressures, decreased cardiac output, and elevated systemic vascular resistance, hypovolemic shock 182 could be categorized into hemorrhagic and non-hemorrhagic shock. Initial resuscitation should focus on to} restoration of circulating quantity, with the type of|the sort of} resuscitation fluid geared in the direction of|in direction of} the underlying process. In these instances, avoidance of hypothermia, acidosis, and coagulopathy, the so-called "lethal triad" of trauma, is of important significance. Source control for bleeding should be obtained surgically, endoscopically, or through interventional radiology. Nonhemorrhagic hypovolemia can happen secondary to elevated fluid losses (eg: vomiting or diarrhea, burn injury) and/or inadequate intake. Cardiogenic Shock Characterized by low cardiac output, high filling pressures, and elevated systemic vascular resistance, cardiogenic shock could be categorized into arrhythmogenic, myopathic or valvular etiologies. Additional lack of coordination between atrial and ventricular contraction (atrial fibrillation) may result in important decreases in cardiac output. In the unstable patient, electrical cardioversion could also be} essential to restore perfusion. Bradyarrhythmias leading to cardiogenic shock may require temporary or permanent pacing. Electrolyte abnormalities, hyper- and hypovolemia, ischemia, and different physiologic stressors can all result in development of arrhythmias. Patients with myopathic disease, together with acute myocardial ischemia, exacerbations of coronary heart failure, or myocardial gorgeous post-cardiopulmonary bypass, may profit from inotropic help with related preload or afterload reduction. Severe acute or continual valvular abnormalities may cause hemodynamic derangements. The sequelae of aortic or mitral stenosis could also be} insidious and never present until the patient experiences extra physiologic stresses or reserve is exhausted. Acute aortic insufficiency could also be} end result of|the results of} endocarditis or aortic dissection, while new onset extreme mitral regurgitation could also be} secondary to an acute myocardial insult. Treatment refractory to medical administration may include 183 percutaneous or open surgical repair/replacement. Initial targets of remedy include fluid resuscitation, sometimes with a 30mL/kg bolus of crystalloid answer, followed by the addition of vasopressor administration if quantity fails to resolve hypotension. Vasopressin is added as a second line remedy for escalating vasopressor necessities. Rapid therapy with broad spectrum antibiotics is equally essential in enhancing outcomes in septic shock. Source control, via surgical or interventional radiology procedures, is vital for chosen infections (necrotizing gentle tissue infection, urinary obstruction, intraabdominal abscess). Anaphylactic shock is recognized by physical exam findings preserving with} vasoplegic shock physiology and a temporal affiliation with administration of an inciting agent. Patients may exhibit indicators of bronchospasm, airway and mucosal edema, rash, tachycardia and hypotension. Treatment hinges on discontinuation of the offending agent and supportive care, together with the administration of epinephrine (intramuscular or intravenous) with antihistamines, steroids, and bronchodilators. Adrenal crisis may present as end result of|the results of} acute stress in an already adrenally suppressed patient or de novo in the case of adrenal infarction (as could be seen with extreme meningococcal infections). Rapid recognition in at-risk patients is critical and therapy consists of stress-dose steroid administration (hydrocortisone). Neurogenic shock is end result of|the results of} a blockade of sympathetic outflow, most commonly from high spinal wire harm or brain damage. In addition to low systemic vascular resistance, these patient may endure from potentially deadly bradyarrhythmias. If unresponsive to pharmacologic therapies such as atropine or epinephrine, these patients may require temporary or permanent pacing. Neurogenic shock is sometimes listed as a separate category of shock, though the physiology is just like different sources of distributive shock. Obstructive Shock Characterized by low cardiac output, high filling pressures, and elevated systemic vascular resistance, obstructive shock is physiologically just like cardiogenic shock, and is sometimes considered a subcategory of cardiogenic shock. Though less common, obstructive shock has the potential for fast reversal depending on etiology. Classifications include cardiac tamponade, tension pneumothorax, huge pulmonary embolism, and restrictive pericarditis. Management for all 184 etiologies include fluid resuscitation to preserve intravascular quantity and cardiac preload, and inotropic help as indicated until definitive therapy could be undertaken. Cardiac tamponade is end result of|the results of} elevated pericardial strain causing decreased diastolic cardiac filling and finally outflow obstruction. Causes include hemorrhage into the pericardial area, especially in post-cardiothoracic surgical patients, or pericarditis leading to large quantity accumulation. Definitive therapy is drainage of the effusion, both by pericardiocentesis or a pericardial window procedure. Tension pneumothorax is brought on by the buildup of air in the pleural area, leading to compression of the great vessels with decreased cardiac filling and cardiac output. Constrictive pericarditis could also be} end result of|the results of} quantity of|numerous|a variety of} infectious, rheumatologic or oncologic sources. Treatment consists of administration of the underlying disease process, preload optimization, and occasionally surgical consultation. Monitoring Response to Treatment Active and continuous evaluation of therapy response is vital to ongoing remedy. A number of different modalities have been developed to measure preload responsiveness, though each has its limitations. Invasive cardiac output monitoring with a pulmonary arterial catheter is not routinely beneficial though could also be} useful in certain conditions (post-cardiac surgical procedure or in mixedshock states). Dynamic response measurements such as pulse strain variation and stroke quantity variation are increasingly 185 utilized at the bedside, however are greatest validated in mechanically ventilated patients without spontaneous respiratory effort. Serial evaluation is advantageous, however could be costly, time intensive and operator dependent. Cecconi M, De Backer D, Antonelli M, et al: Consensus on circulatory shock and hemodynamic monitoring. An 89 year-old lady presents from a nursing house with altered psychological status, tachycardia, tachypnea, hypotension and fever. The following hemodynamic parameters are most characteristic of her shock subtype. Which of the following instruments could also be} used as a stand-alone monitor of preload responsiveness in shock? None of the above 187 Section 2 Management of Dysrhythmias Key Points: · Dysrhythmias are common in the intensive care unit. Surgery is a serious threat factor in the development of post-operative dysrhythmias due to of} ache, inflammation, electrolyte abnormalities, and anemia. It is characterised by symptomatic bradycardia, frequent sinus pauses, sinus arrest, junctional escape rhythms, and sinus bradycardia with paroxysmal atrial fibrillation. Common pharmacologic offenders are adenosine, calcium channel blockers, beta blockers, amiodarone, and digoxin. This rhythm additionally be|can be} a known complication following aortic or mitral valve surgical procedure. Asystole refers to the whole absence of electrical and mechanical exercise of the center.
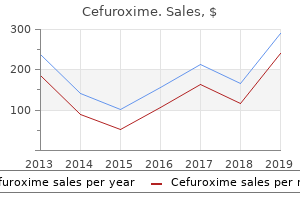
| Comparative prices of Cefuroxime | ||
| # | Retailer | Average price |
| 1 | Costco | 832 |
| 2 | Meijer | 835 |
| 3 | Army Air Force Exchange | 126 |
| 4 | Lowe's | 863 |
| 5 | SonyStyle | 970 |
| 6 | Williams-Sonoma | 394 |
| 7 | Delhaize America | 206 |
| 8 | OfficeMax | 506 |
| 9 | Big Lots | 839 |
| 10 | Winn-Dixie Stores | 443 |
Order cefuroxime 250 mg
Cleveland Clinic was awarded the rating based on knowledge comparisons from January 2009 by way of December 2011. Cleveland Clinic performs the biggest variety of aortic valve operations in the nation. Ninety-one percent were valve replacements (N = 1,553), 5 percent were valve repairs (N = 101) and four percent were valve-sparing operations (N = 85). Replacement 2007 2011 Percent 80 60 40 20 0 2007 2008 2009 2010 2011 Repair Replacement Cleveland Clinic surgeons carried out mitral valve repairs before it was the preferred treatment for patients with mitral valve illness. The majority of mitral valve repairs at Cleveland Clinic are carried out using a minimally invasive approach. Sydell and Arnold Miller Family Heart & Vascular Institute 29 Valve Disease (continued) Valve Replacement Prostheses Volume and Type 2007 2011 Volume 2,000 1,500 1,000 500 0 2007 2008 2009 2010 2011 Mechanical Allografts Bioprostheses the bulk (92. Surgical Treatment of Infective Endocarditis Infective endocarditis is a life-threatening illness. It causes bacterial or fungal growths on the heart valves that can result in perforation, rupture and subsequent valve regurgitation. Cleveland Clinic surgeons deal with selection of|quite lots of|a big selection of} patients with infective endocarditis, including these with superior illness and prosthetic valve endocardititis. Volume and Hospital Mortality (N = 128) 2007 2011 Volume one hundred eighty 150 a hundred and twenty 90 60 30 0 2007 2008 2009 2010 2011 Mortality (%) Reoperation Primary 24 20 16 12 8 four 0 In 2011, we carried out 128 surgical procedures to deal with infective endocarditis and maintained low mortality charges. The mortality price is consistently 0 percent with this process, and patients experience a shorter restoration than those that have traditional surgery. Robotically Assisted Valve Surgery (N = 160) Cleveland Clinic performs extra robotically assisted mitral valve surgeries than any major academic hospital in the United States. Robotically Assisted Mitral Valve Repair Volume 2007 2011 Volume 300 200 100 0 Cleveland Clinic surgeons carried out a hundred and sixty robotically assisted mitral valve repairs in 2011. Compared with comparable hospitals, mortality charges for valve surgery are far decrease. Percutaneous Valve Treatments Cleveland Clinic stays devoted to developing and using greatest possible|the absolute best|the very best} percutaneous methods to deal with patients with valve illness. Transcatheter Aortic Valve Replacement Volume and 30-Day Mortality 2007 2011 Volume a hundred and twenty 80 40 0 Expected Mortality (%) Mortality (%) 15 10 5 0 2007 2008 2009 2010 2011 In 2011, Cleveland Clinic carried out a hundred and five percutaneous aortic valve replacements. United States Feasibility Study of Transcatheter Insertion of a Stented Aortic Valve by the Left Ventricular Apex. Transcatheter Aortic-Valve Implantation for Aortic Stenosis in Patients Who Cannot Undergo Surgery. Researchers are finding out using of} percutaneous aortic valve alternative on this patient inhabitants. The process is completed by way of the transfemoral or left subclavian artery or by way of a transapical approach. Research additionally includes an approach by way of the ascending aorta by way of a mini-J incision. Sydell and Arnold Miller Family Heart & Vascular Institute 33 Aortic Disease 43,199 Estimated variety of patients who die yearly from aortic illness, according to the Centers for Disease Control and Prevention. This is larger than the number folks who|of people that} die yearly from breast cancer, homicides, pancreatic cancer, colon cancer, prostate cancer or motorcar accidents. Cleveland Clinic makes use of a comprehensive, multidisciplinary approach to deal with patients with aortic illness. Using typical, minimally invasive and endovascular strategies, our surgeons deal with all sections of the aorta, from the aortic valve to the blood provide to the pelvic vasculature. Aortic Surgery Volume and Type (N = 1,173) 2002 2011 Volume 1,500 Open Ascending/Arch Repair (N = 707) Open Descending/Thoracoabdominal Repair (N = 110) Endovascular Descending/ Thoracoabdominal Repair (N = 210) 1,000 500 Open Abdominal Repair (N = 59) Endovascular Abdominal Repair (N = 87) 0 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 A whole of 1,173 aortic surgeries were carried out at Cleveland Clinic in 2011. Ascending Arch Descending thoracic aorta Thoracoabdominal aorta Abdominal aorta 34 Outcomes 2011 Open Ascending Aorta and Arch Disease Surgery Volume 2007 2011 Volume 800 600 four hundred 200 0 2007 2008 2009 2010 2011 In 2011, Cleveland Clinic carried out 707 elective and emergency procedures to deal with patients with issues of the ascending aorta and arch. More than one-third of the patients transported were handled in the Miller Family Heart & Vascular Institute, and lots of|and a lot of} had acute aortic syndromes. In 2011, we carried out 209 of those procedures and maintained a low mortality price of 7. Elective Ascending Aorta and Arch Surgery Volume, Stroke and Mortality 2007 2011 Volume 500 four hundred 300 200 100 0 2007 2008 2009 2010 2011 Stroke (%) Hospital Mortality (%) 10 8 6 four 2 0 Cleveland Clinic carried out 498 elective ascending aorta and arch surgeries. Sydell and Arnold Miller Family Heart & Vascular Institute 35 Aortic Disease (continued) Aortic Arch Aneurysm Repairs In 2011, Cleveland Clinic surgeons carried out 222 procedures to restore aortic arch aneurysms. We use open and endovascular procedures that incorporate using of} fenestrations, branches or hybrid strategies. Despite the complexity of those procedures, the speed of death and stroke remained low. Elective Arch Aneurysm Operations Volume, Stroke and Mortality 2007 2011 Volume 200 150 100 50 0 2007 2008 2009 2010 2011 Stroke (%) Hospital Mortality (%) 20 15 10 5 0 3-D reconstruction of aortic arch aneurysm complicating a persistent aortic dissection. Emergency and Urgent Arch Aneurysm Operations Volume, Stroke and Mortality 2007 2011 Volume 150 a hundred and twenty 90 60 30 0 2007 2008 2009 2010 2011 Stroke (%) Hospital Mortality (%) 25 20 15 10 5 0 3-D reconstruction of an aortic arch department graft. This technique permits treatment of very complicated anatomy with out opening the chest. Outcomes 2011 36 Cleveland Clinic surgeons are internationally recognized as besttrained surgeons to deal with patients with extensive thoracic aneurysmal illness. We use a comprehensive, multidisciplinary approach that allows every patient to receive greatest possible|the absolute best|the very best} individual treatment. Novel Technique for Chronic Extensive Dissection with Aneurysm Patients who survive an acute dissection that involves segments of the aorta typically require major operations to eliminate the risk of rupture and death. A novel approach combining open "elephant trunk" restore with a fenestration process of the distal aorta supplies a dependable endovascular answer to complete the restore in these complicated circumstances. Distal touchdown zone fenestration facilitates endovascular elephant trunk completion and false lumen thrombosis. First-stage elephant trunk and distal fenestration Second-stage stent graft Coarctation and Late Complications in Adults and Adolescents A rising variety of adults and adolescents are identified with aortic coarctation after childhood. Our multidisciplinary group has extensive experience using open, hybrid and endovascular procedures to deal with patients on this inhabitants. During a 10-year study of a hundred and ten patients handled with these procedures, there was no incidence of hospital mortality. Open, hybrid, and endovascular treatment for aortic coarctation and postrepair aneurysm in adolescents and adults. We have demonstrated 100 percent success in treating patients with Takayasu arteritis using an endovascular approach to place stent grafts. Newer endovascular strategies have allowed us to use alternate treatment methods which will result in better outcomes than traditional, open surgery to deal with patients with this complicated illness. Endovascular administration of patients with Takayasu arteritis; stents versus stent grafts. Cleveland Clinic surgeons deal with patients with these circumstances using both open and endovascular procedures. Mortality (%) 20 2008 2010 2011 15 10 5 0 Emergency Open Elective Emergency Endo Elective 38 Outcomes 2011 Protection of Spinal Function the restore of thoracoabdominal aneurysms has traditionally been related to a threat of spinal wire damage or paralysis. In circumstances of thoracoabdominal aneurysm restore, this means incessantly staging the restore so the impression on the spinal wire is gradual, somewhat than sudden. We have additionally incorporated superior strategies to shield the spinal wire throughout open thoracoabdominal aortic repairs. This includes adding papaverine to the intrathecal area throughout surgery, which helped reduce the speed of paraplegia to three. Spinal wire protective strategies throughout descending and thoracoabdominal aortic aneurysm restore in the modern period: the function of intrathecal papaverine. The goal of treatment with a bifurcated-bifurcated system is to eliminate the method of inserting branched grafts into internal iliac arteries whereas permitting the preservation of blood move to the pelvis. Preserving pelvic blood move is essential as a result of|as a outcome of} it contributes to spinal wire, buttock muscle and sexual operate. Fewer elements are needed to complete complicated repairs when the bifurcated-bifurcated system is used. Because of this, many research support population-based, one-time ultrasound screening for patients at excessive threat (usually these over age 65).
Safe 250 mg cefuroxime
En este sentido, se deberнa garantizar la accesibilidad de estos productos a los afectados, mediante la regulaciуn normativa asн como por medio de la cobertura por parte de la sanidad pъblica de estos productos, Los tratamientos disponibles para la poblaciуn con enfermedades raras, presentan un tipo de respuesta excesivamente orientado hacia los sнntomas. Ello, si bien es resultado de la ausencia de tratamientos eficaces para la eliminaciуn de la enfermedad, tambiйn se relaciona con el ofrecimiento de respuestas parciales en un contexto de desconocimiento sobre su existencia, descoordinaciуn entre especialistas o la simple necesidad de dar una respuesta a cada necesidad de forma independiente. Ademбs de la ausencia de un sistema fiable de recursos de referencia adecuados (que mediante la Estrategia Nacional de Enfermedades Raras del Sistema Nacional de Salud se estб intentando articular), se detectan problemas de descoordinaciуn entre diferentes servicios (sanitarios, sociales, educativos, etc. En este sentido la reclamaciуn mбs evidente parece ser la necesidad de mayor especializaciуn de determinados servicios o profesionales clave. Es necesario, en este бmbito, avanzar en criterios objetivos de planificaciуn de los servicios y actividades, basando el trabajo en la exigencia a estas instituciones de un anбlisis riguroso de la demanda que expresan familias y afectados. Las peculiares caracterнsticas de dispersiуn de casos influyen en el acceso a los recursos, generalmente servicios lejanos al lugar de residencia. Este acceso se complica no sуlo por cuestiones relacionadas con el propio desplazamiento sino con problemas burocrбticos sobre todo entre бmbitos de gestiуn de los sistemas sanitarios (comunidades autуnomas, en general). La dispersiуn de casos determina a su vez la estructura y desarrollo de las orga151 nizaciones de afectados y familiares y en la consolidaciуn y funcionamiento del movimiento asociativo, como veremos. La relaciуn entre enfermedad (discapacidad) y condiciуn socioeconуmica Las personas con enfermedades raras presentan necesidades de apoyo muy variables tanto en бreas de actividad para las que las precisan, como en la frecuencia e intensidad de dichos apoyos. Como hemos visto, estas limitaciones en la actividad van a condicionar la situaciуn de salud y socioeconуmica de los afectados, por lo que se requieren medidas que garanticen esos apoyos necesarios por motivo de su discapacidad (y, en algunos casos, por su "situaciуn de dependencia"), las cuales precisan primero del reconocimiento de la misma. En common, estб mucho mбs generalizado el reconocimiento por discapacidad que por situaciуn de dependencia, cuestiуn que parece lуgica teniendo en cuenta el nivel de desarrollo de ambos sistemas; el acceso a ellos resulta fundamental para tener oportunidades de apoyo desde los servicios pъblicos, sobre todo entre aquellos que tienen menos ingresos como para poder proveйrselos en el mercado. Mбs allб de estos, parece que las ayudas tйcnicas estбn mбs generalizadas que la asistencia private, que sigue siendo una labor extensamente asumida por las familias y en concreto por las mujeres. Independientemente de los apoyos disponibles, las familias se ven sometidas a importantes costes (econуmicos y de oportunidad) como consecuencia de las necesidades de atenciуn y apoyo que asumen que, como dijimos, van a reducir su capacidad monetaria para adquirir los recursos para satisfacer sus necesidades en igualdad de condiciones que el resto de los ciudadanos. Se ha de plantear en el futuro cуmo valorar la dependencia en determinadas enfermedades raras en las que no se visibilizan con nitidez las dificultades, que actualmente pueden suponer valoraciones inadecuadas, igual que en la valoraciуn de la discapacidad. Determinadas enfermedades no presentan ningъn sнntoma ni rasgo seen, incluso para pruebas no especializadas, lo que repercute negativamente a lo largo de muchos momentos de la vida de las personas (debido al desconocimiento y la incomprensiуn): la relaciуn con la familia y el бmbito laboral entre los mбs destacados, sobre todo si estas enfermedades se acompaсan de crisis o fases agudas. Con respecto a la poblaciуn afectada en edad escolar y su relaciуn con el sistema educativo, se observan aъn grandes posibilidades de mejora. No se han generalizado apoyos y adaptaciones especнficas en la escuela y mбs de la mitad de la poblaciуn escolarizada no tiene cubiertas adecuadamente las ayudas que precisa, mediante apoyos en la escuela ordinaria o a travйs de centros de educaciуn especial. Cabe destacar que, especialmente en el бmbito escolar, la mejora no pasa tanto por la generaciуn de nuevos recursos como por un aprovechamiento eficiente de los que el sistema prevй para la poblaciуn con necesidades educativas especiales, asн como por la sensibilizaciуn de profesorado y alumnado acerca de las necesidades especнficas de los alumnos afectados por enfermedades raras (y otras discapacidades). En el бmbito laboral, el problema radica especialmente en la inactividad obligada de los afectados mбs que en los bajos niveles de ocupaciуn entre los que efectivamente se consideran activos laboralmente hablando. Es llamativamente baja la tasa de actividad para la poblaciуn en edad de trabajar, en ocasiones como efecto de unas no bien atendidas necesidades de adaptaciуn de los puestos o flexibilizaciуn de las condiciones laborales: jornada, ubicaciуn del puesto, conciliaciуn de la vida laboral con las necesidades de tratamiento, etc. Como 152 hemos visto, la inactividad laboral, mбs que ser un hecho, es un proceso al que se ven abocados muchos de los afectados por la falta de apoyos, de adaptaciуn del puesto de trabajo y de la incomprensiуn del sistema productivo hacia los trabajadores que son "diferentes". Las (pocas) personas con enfermedades raras que trabajan, por el contrario, lo hacen en una situaciуn de estabilidad laboral correcta y no destacan las altas tasas de desempleo (en relaciуn con el resto de la poblaciуn). Pero es imprescindible tambiйn analizar la relaciуn con la actividad laboral no sуlo del afectado, sino de su nъcleo acquainted: la familia del afectado encuentra limitaciones aсadidas en el terreno laboral, sobre todo los que prestan asistencia private a la persona con enfermedad rara en el hogar como cuidadores principales, que segъn el tipo y la gravedad de la enfermedad, revelan costes de oportunidad laborales que van desde la reducciуn de la jornada laboral a la imposibilidad de continuar trabajando. Igualmente, se observan otros costes de oportunidad a nivel formativo, asн como en cuanto a las posibilidades de disfrute del ocio y tiempo libre. Todo ello, va a afectar directamente a su nivel de ingresos y a su capacidad para adquirir los servicios y recursos que necesitan. Las personas con enfermedades raras y quienes conviven con ellas en el hogar sufren restricciones econуmicas directamente relacionadas con la atenciуn deficiente de sus necesidades de apoyo y la insuficiente cobertura pъblica de los recursos que necesitan. Se ha constatado una menor capacidad para generar ingresos asн como obligaciуn de asumir mбs costes que la poblaciуn common, tanto mбs graves cuanto mayores son las necesidades de apoyo. Como hemos observado, esto repercute negativamente en sus niveles de integraciуn, tanto real como percibida, existiendo una gran mayorнa de poblaciуn afectada que se ha sentido discriminada en diferentes бmbitos de la vida social y cuya valoraciуn subjetiva de su situaciуn private es bastante baja, tanto mбs cuanto peores son las condiciones socioeconуmicas en las que viven. Esos niveles de malestar y desigualdad pueden reducirse mediante una adecuada cobertura del sistema de bienestar pъblico y/o bien amortiguarse mediante las redes de apoyo informales, circunscritas al entorno private, pero tambiйn (aunque en menor medida al tratarse de un movimiento incipiente) al entorno asociativo. La informaciуn obtenida permite afirmar que las personas con enfermedades raras y sus familias cuentan con redes de apoyo muy limitadas y circunscritas habitualmente a personas de su entorno private. Las familias sufren consecuencias graves en su bienestar emocional, en su capacidad para mantener vнnculos y relaciones sociales y en sus oportunidades para mantener una vida laboral activa. La apariciуn de la enfermedad en un hogar puede suponer un alto impacto emocional para la persona con enfermedad rara y su entorno mбs нntimo. El aislamiento social puede llegar hasta la familia extensa, y las relaciones sociales se ven afectadas. Los sentimientos de frustraciуn hacia las personas y las instituciones son generalizados, sobre todo en personas con grandes necesidades de apoyo no cubiertas o con dificultades para acceder a diagnуstico y tratamiento adecuado. Son personas, por ejemplo, frecuentemente sometidas a periodos largos de falta de sueсo, obligadas a generar conocimiento tйcnico sobre especialidades complejas (genйtica, biologнa, medicina), renunciar a logros personales, uso del tiempo libre, etc. Como hemos podido comprobar, la pertenencia a las asociaciones de atenciуn y apoyo a afectados por enfermedades raras o, mбs genйricamente, a personas con discapacidad, mejora los niveles de bienestar subjetivo de los afectados, independientemente de la condiciуn socioeconуmica de los mismos, pues sirven de ayuda mutua y apoyo psicolуgi153 co entre afectados con problemas similares, que les ayudan a afrontar situaciones anбlogas en diferentes escenarios sociales: la atenciуn sanitaria, el apoyo social, la inserciуn laboral y educativa, etc. Segъn familias y profesionales, las entidades especializadas en la atenciуn a personas con enfermedades raras (bбsicamente asociaciones de afectados, familias y tambiйn recursos pъblicos) constituyen un punto de apoyo muy bien valorado. Aъn asн, resulta evidente que la poblaciуn con enfermedades raras y sus familias forman un colectivo, como decнamos, en situaciуn de vulnerabilidad, por lo common con grandes necesidades de apoyo en todos los бmbitos de la vida. El fortalecimiento de las asociaciones y las macro-estructuras que las agrupan (federaciones regionales, estatales y supranacionales) suponen un incremento en recursos ъtiles para las personas con enfermedades y sus familias (informaciуn, contacto con otros afectados, coordinaciуn, sensibilizaciуn y apoyo), asн como un recurso poderoso para hacer valer sus derechos y reivindicar ante los poderes pъblicos que se garanticen unos niveles dignos de atenciуn sociosanitaria e inclusiуn social. Las iniciativas de informaciуn, sensibilizaciуn y coordinaciуn de servicios, junto con las mejoras en investigaciуn generan grandes posibilidades de mejora que las personas perciben con optimismo. La articulaciуn de esfuerzos, autonуmicos, nacionales e internacionales, pъblicos y privados, de profesionales y de afectados y familiares, es la herramienta mбs poderosa y eficaz que se puede emplear para empezar a mejorar la situaciуn sanitaria de los afectados y sus familias y garantizar su inclusiуn y no discriminaciуn en la sociedad. Este es el camino que se ha tomado en los ъltimos aсos y, como los datos de este estudio demuestran, estб obteniendo unos resultados (si bien aъn incipientes) claramente favorables. En este бmbito es fundamental la unificaciуn de las pruebas genйticas entre diferentes comunidades, cuyo catбlogo ha de ser revisado periуdicamente. Una vez que las familias identifican servicios o profesionales realmente capacitados para intervenir en el diagnуstico y tratamiento de las personas con enfermedades raras, encuentran mъltiples dificultades para acceder a ellos. Estas dificultades se relacionan con la dispersiуn geogrбfica y las trabas burocrбticas principalmente, por lo que resulta necesario desmontar las barreras administrativas, sobre todo entre Comunidades Autуnomas, para la atenciуn a personas ajenas al sistema regional de salud. En el medio rural, las dificultades de acceso a recursos (sobre todo especializados) se incrementan. Mejorar el registro e intercambio de informaciуn entre personas afectadas y profesionales. De igual manera, es preciso incorporar la informaciуn que las familias cuidadoras disponen sobre su experiencia en la relaciуn y apoyo al afectado, asн como poner a su disposiciуn la informaciуn contenida en la historia clнnica. La atenciуn a una persona con enfermedad rara puede requerir la aplicaciуn de muchos recursos, mбs allб de los farmacolуgicos. Independientemente de si los medicamentos son financiados whole o parcialmente (lo cual suponen un coste muy alto para muchas familias), el tratamiento adecuado a muchas personas requiere la adquisiciуn de otros materiales, servicios y recursos que no estбn financiados, por lo que se hace necesario contemplar el reembolso de los mismos. Para ello, es indispensable una regulaciуn normativa que garantice el acceso como derecho fundamental, asн como medidas eficaces para que esa cobertura se haga efectiva. Determinadas caracterнsticas de las enfermedades raras implican necesidades o servicios de apoyo muy concretos que, aunque existen, en ocasiones no se puede acceder por cuestiones formales de diseсo de los servicios o no contemplar limitaciones en la actividad muy especнficas de algunas enfermedades raras. Resulta recomendable flexibilizar y adaptar estos mecanismos, por ejemplo en los servicios de valoraciуn de la discapacidad o de la incapacidad laboral. Atenciуn integral en educaciуn, con los apoyos necesarios dentro y fuera del entorno escolar. Las personas con enfermedades raras precisan de una adaptaciуn de los recursos educativos que les permitan acceder a estos servicios en igualdad de oportunidades. Las adaptaciones precisas para su escolarizaciуn trascienden en muchos casos de las meramente curriculares: eliminaciуn de barreras, disposiciуn de profesionales de apo- 2 three 4 5 6 156 yo, adaptaciуn de horarios y exбmenes. Asimismo, deberнa extenderse la aplicaciуn de los apoyos al бmbito domйstico, para favorecer el mejor seguimiento de los cursos escolares. La principal carga de atenciуn a personas con enfermedades raras muy dependientes recae sobre las mujeres, que ven asн perjudicadas sus posibilidades de desarrollo private, social y laboral. Un diseсo adecuado de los mecanismos de apoyo en el бmbito acquainted, asн como de los recursos sociales destinados a ello, deben contemplar actuaciones destinadas a cambiar esta realidad.
Proven 500 mg cefuroxime
D u r i n g t h i s t i me, the r i s k f o r g r o s s s t r u c t u r a l d e f e c t s b e i n g i n d u c e d d e c r e a s e s, b u t o r g a n s y s t e ms ma y s t i l l b e a f f e c t e d. F o r e xa mp l e, the b r a i n c o n t i n u e s t o d i f f e r e n t i a t e d u r i n g the f e t a l p e r i o d, s u c h t h a t t o xi c e xp o s u r e s ma y c a u s e l e a r n i n g d i s a b i l i t i e s o r me n t a l r e t a r d a t i o n. E n vi r o n m e n t a l F a c t o r s U n t i l the e a r l y 1 9 4 0 s, i t w a s a s s u me d t h a t c o n g e n i t a l d e f e c t s w e r e c a u s e d p r i ma r i l b y h e r e d i t a r y f a c t o r s. G r e g g t h a t G e r ma n me a s l e s a f f e c t i n g a mo the r d u r i n g e a r l y p r e g n a n c y c a u s e d a b n o r ma l i t i e s i n the e mb r y o, i t s u d d e n l y b e c a me e v i d e n t t h a t c o n g e n i t a l ma l f o r ma t i o n s i n h u ma n s c o u l d a l s o b e c a u s e d b y e n v i r o n me n t a l f a c t o r s. L e n z l i n k e d l i mb d e f e c t s t o the s e d a t ih a l i d o m i d e n d ma d e i t c l e a r t h a t d r u g s c o u l d a l s o c r o s s ve a the p l a c e n t a a n d p r o d u c e b i r t h d e f e cF sg (s8. L i mb d e f e c t s c h a r a c t e r i ze d b y l o s s o f 2 the l o n g b o n e s o f the l i mb. T h e s e d e f e c t s w e r e c o mmo n l y p r o d u c e d b y the d r u g t h a l i d o mi d. S u s c e p t i b i l i t y t o t e r a t o g e n e s i s d e p e n d s e n otth e e o f the c o n c e p t u s g on y p a n d the ma n n e r i n w h i c h t h i s g e n e t i c c o mp o s i t i o n i n t e r a c t s w i t h the e n v i r o n me n t. T h ea t e r n a l g e n o m s a l s o i mp o r t a n t w i t h r e s p e c t t o d r u g m ie me t a b o l i s m, r e s i s t a n c e t o i n f e c t i o n, a n d o the r b i o c h e mi c a l a n d mo l e c u l a r processes that have an effect on} the conceptus. S u s c e p t i b i l i t y t o t e r a t o g e n s v a r i e s w ie h e ho p m e n t a l s t a g e a t the t i m e d t v tl e o f e x p o s u r eT h e mo s t s e n s i t i v e p e r i o d f o r i n d u c i n g b i r t h d e f teh itrsd i s t h. F o r e xa mp l e, c l e f t palate could be induced on the blastocyst stage (day 6), during gastrulation (day 1 4), a t the e a r l y l i mb b u d s t a g e (f i f t h w e e k), o r w h e n the p a l a t a l s h e l v e s a r e f o r mi n g (s e v e n t h w e e k). F u r the r mo r e, w h i l e mo s t a b n o r ma l i t i e s a r e p r o d u c e d d u r i n g e mb r y o g e n e s i s, d e f e c t s ma y a l s o b e i n d u c e d b e f o r e o r a f t e r t h i s p e r i o d; n o s t a g e o f d e v e l o p me n t i s c o mp l e t e lF i g. M a n i f e s t a t i o n s o f a b n o r ma l d e v e l o p me n t o n p e ns e a n d d u r a t i o n o f de do d e x posure o a teratogen. The r a t o g e n s a c t i n s p e c i f i c (w ae c h a n i s m s)n d e v e l o p i n g c e l l s a n d m ys o t i s s u e s t o i n i t i a t e a b n o r ma l e mb r y o g e n eh io g e n e s i. M a n i f e s t a t i o n s o f a b n o r ma l d e v e l o p me n ta the m a l f o r m a t i o n, g r o w t h de ar, r e t a r d a t i o na n df u n c t i o n a l d i s o r d. R u b e l l au s e d t o b e a ma j o r p r o b l e m, b u t the a b i l i t y t o d e t e c t s e r u m a n t i b o d y t i t e r s a n d d e v e l o p me n t o f a v a c c i n e h a v e s i g n i f i c a n t l y l o w e r e d the i n c i d e n c e o f b i r t h d e f e c t s f r o m t h i s c a u s. O f t e n, the mo the r h a s n o s y mp t o ms, b u t the is results on the fetus could be devastating. H e r p e s s i m p l e x v i r u s, v a r i c e l l a v i rdhs m a n i m m u n o d e f i c i e n c y v i r u s, an u u (H I V) c a n c a u s e b i r t h d e f e c t s. H e r p e s - i n d u c e d a b n o r ma l i t i e s a r e r a r e, a n d u s u a l l y i n f e c t i o n i s t r a n s mi t t e d a s a v e n e r e a l d i s e a s e t o the c h i l d d u r i n g d e l i v e r y. In f e c t i o n w i t h v a r i c e l l a c a u s e s a 2 0 % i n c i d e n c e o f b i r t h defects. Othe r V iral Infe ctions and Hy pe rthe rm ia M a l f o r ma t i o n s f o l l o w i n g ma t e r n a l i n f e c t i o n w i t h me a s l e s, mu mp s, h e p a t i t i s, p o l i o my e l i t i s, e c h o v i r u s, C o xs a c k i e v i r u s, a n d i n f l u e n za v i r u s h a v e b e e n d e s c r i b e d. P r o s p e c t i v e s t u d i e s i n d i c a t e t h a t the ma l f o r ma t i o n r a t e f o l l o w i n g e xp o s u r e t o the s e a g e n t s i s l o w i f n o t n o n e xi s t e n t. A c o mp l i c a t i n g f a c t o r i n t r o d u c e d b y the s e a n d o the r i n f e c t i o u s a g e n t s i s t h a t mo s t a r e p y r o g e n i,ca n d e l e v a t e d b o d y t e mp e r ahu rp e r the r m i as t e r a t o g e n i c. In a d d i t i o n t o f e b r i l e i l l n e s s e s, u s e o f h o t t u b s a n d s a u n a s c a n p r o d u c e s u f f i c i e n t t e mp e r a t u r e elevations to cause start defects. P o o r l y c o o k e d me a t; d o me s t i c s c a n i ma l s, e s p e c i a l l y c a t s; a n d f e c e s i n c o n t a mi n a t e d s o i l c a n c a r r y the p r o t o zo a n p a r a s i t e opl as mos i s gondi ic. Radiation I o n i z i n g r a d i a t i oinl s r a p i d l y p r o l i f e r a t i n g c e l l s, s o i t i s a p o t e n t t e r a t o g e n, k l producing virtually any sort of start defect relying upon the dose and stage of d e v e l o p me n t o f the c o n c e p t u s a t the t i me o f e xp o s u r. R a d i a t i o n f r o m n u c l e a r e xp l o s i o n s i s a l s o t e r a t o g e n i c. Amo n g w o me n s u r v i v o r s p r e g n a n t a t the t i me o f the a t o mi c b o mb e xp l o s i o n s o v e r H i r o s h i ma a n d N a g a s a k i, 2 eight % a b o r t e d, 2 5 % g a v e start to youngsters who died of their first year of life, and 25% gave start to youngsters w h o h a d s e v e r e b i r t h d e f e c t s i n v o l v i n g the c e n t r a l n e r v o u s s y s t e m. R a d i a t i o n i s a l s o a mu t a g e n i c a g e n t a n d c a n l e a d t o g e n e t i c a l t e r a t i o n s o f g e r m c e l l s a n d s u b s e q u e n t ma l f o r ma t i o n s. A N a t i o n a l (In s t i t u t e s o f H e a l t h s t u d y d i s c o v e r e d t h a t p r e g n a n t w o me n t o o k 9 0 0 d i f f e r e n t d r u g s f o r a n a v e r a g e o f 4 p e r w o ma n. O n l y 2 0 % o f p r e g n a n t w o me n u s e d n o d r u g s d u r i n g the i r p r e g n a n c y. E v e n w i t h t h i s w i d e s p r e a d u s e o f c h e mi c a l a g e n t s, r e l a t i v e l y f e w o f the ma n y d r u g s u s e d d u r i n g p r e g n a n c y h a v e b e e n p o s i t i v e l y i d e n t i f i e d a s b e i n g t e r a t o g e n i c. O n e e xa mp t e a si d o m i d ea n a n t i n a u s e a n t a n d s l e e p i n g p i l l. In l h il, 1 9 6 1, i t w a s n o t e d i n W e s t G e r ma n y t h a t the f r e a me nl c aa o f m e r o m e l i a qu e i y nd (t o t a l o r p a r t i a l a b s e n c e o f the e xt r e mi t i e s), a r a r e h e r e d i t a r y a b n o r ma l i t y, h a d s u d d e n l y i n c r e a s e dg(. T h e c a u s a l r e l a t i o n b e t w e e n t h a l i d o mi d e a n d me r o me l i a w a s d i s c o v e r e d o n l y b e c a u s e the d r u g p r o d u c e d s u c h a n u n u s u a l a b n o r ma l i t y. If the d e f e c t h a d b e e n a mo r e c o mmo n t y p e, s u c h a s c l e f t l i p o r h e a r t ma l f o r ma t i o n, the a s s o c i a t i o n w i t h the d r u g mi g h t e a s i l y h a v e b e e n o v e r l o o k e d. Other drugs with teratogenic potential include the anticonvulsants d i p h e n y l h y d a n t o i n (p h e n y t o i n), v a l p r o ia natcriid e t h a d i o n e h i c h a r e, c d m, w u s e d b y p i l e p t i c o me n. S p e c i f i c a l l y, t r i me t h a d i o n e a n d d i p h e n y l h y d a n t o i n e w p r o d u c e a b r o a d s p e c t r u m o f a b n o r ma l i t i e s t h a t c o n s t i t u t e d i s t i n c t p a t t e r n s o f d y s mo r p h o g e n e s i s k n o w n a s r ti h ee t h a d i o na n df e t a l h y d a n t o i n s y n d r o. Va l p r o i c a c i d a l s o c a u s e c r a n i o f a c i a l a b n o r ma l i t i e s b u t h a s a p a r t i c u l a r p r o p e n s i t y f o r p r o d u c i n g n e u r a l t u b e defects. A n t i p s y c h o t ia n da n t i a n x i e t y a g e n(tma j o r a n d mi n o r t r a n q u i l i ze r s, c s r e s p e c t i v e l y) a r e s u s p e c t e d p r o d u c e r s o f c o n g e n i t a l ma l f o r ma t i o n s. T h e a n t i p s y c h o t i c s e n o t h i a z i na n dl i t h i u mh a v e b e e n i mp l i c a t e d a s t e r a t o g e n s. In a n y c a s e, i t h a s b e e n s t r o n g l y advised that use of those brokers during pregnancy carries a excessive risk. S i mi l a r o b s e r v a t i o n s h a v e b e e n ma d e f o r the a n t i a n xim the pa o e n tm a t e, e y r gba s c h l o r d i a z e p o x i,da n dd i a z e p a m (V a l i u. L i k e w i s e, r e t r o s p e c t i v e s t u d i e s d e mo n s t r a t e u p t o a f o u r f o l d i n c r e a s e i n c l e f t l i p w i t h o r w i t h o u t c l e f t p a l a t e i n o f f s p r i n g w h o s e mo the r s t o o k d i a ze p a m d u r i n g p r e g n a n c y. T h e a n t i c o a g u l a n t w a r f air i n e r a t o g e n i c, w h e rh e p a r i nd o e s n o t a p p e a r t o s t eas b. A n t i h y p e r t e n s i v e a g e tn ta t i n h i ba tn g i o t e n s i n - c o n v e r t i n g e n z y m e (A C E hs i i n h i b i t o r sp r o d u c e g r o w t h r e t a r d a t i o n, r e n a l d y s f u n c t i o n, f e t a l d e a t h, a n d) o l i g o h y d r a mn i o s. C a u t i o n h a s a l s o b e e n e xp r e s s e d r e g a r d i n g a n u mb e r o f o the r c o mp o u n d s t h a t ma y d a ma g e the e mb r y o o r f e t u s. F i n a l l y, the r e i s i n c r e a s i n g e v i d e n c e t h a ts p i r i n(s a l i c y l a t e s), the mo s t c o mmo n l y i n g e s t e d d r u g d u r i n g p r e g n a n c y, ma y h a r m the d e v e l o p i n g o f f s p r i n g w h e n u s e d i n l a r g e d o s e s. In the c a s e o f L S D, l i mb a b n o r ma l i t i e s a n d ma l f o r ma t i o n s o f the c e n t r a l n e r v o u s s y s t e m h a v e b e e n r e p o r t e d. A c o mp r e h e n s i v e r e v i e w o f mo r e t h a n 1 0 0 p u b l i c a t i o n s, h o w e v e r, l e d t o the c o n c l u s i o n t h a t p u r e L S D u s e d i n mo d e r a t e d o s e s i s n o t t e r a t o g e n i c a n d d o e s n o t c a u s e g e n e t i c d a ma g. A s i mi l a r l a c k o f c o n c l u s i v e e v i d e n c e f o r t e r a t o g e n i c i t y h a s b e e n d e s c r i b e d f o r ma r i j u a n a a n d P C P. T h e r e i s a w e l l - d o c u me n t e d a s s o c i a t i o n b e t w e e nama t h r ni a lg e s t i o n a n d lco eol n c o n g e n i t a l a b n o r ma l i t i e s. S i n c e a l c o h o l ma y i n d u c e a b r o a d s p e c t r u m o f d e f e c t s, r a n g i n g f r o m me n t a l r e t a r d a t i o n t o s t r u c t u r a l a b n o r ma l i t i charge t,a tl ha l c e rh o l s e to m s p e c t r u m d i s o r d(e r S D)i s u s e d t o r e f e r t o a n y a l c o h o l - r e l a t e d F e tf a lc t s. A l c o h o l - r e l a t e d n e u r o d e v e l o p m e n t a l d i s o r d e r r eA R N D n t s a l e s s s e v e r e (prese) e xa mp l e o f a l c o h o l - r e l a t e d a b n o r ma l i t i e s. F u r the r moo e,o l i s the l e a d i n g c a u s e o f m e n t a l alc r h re tardation. C i g a r e t t e s m o k i n g s n o t b e e n l i n k e d t o ma j o r b i r t h d e f e c t s, b u t i t d o e s ha c o n t r i b u t e t o i n t r a u t e r i n e g r o w t h r e t a r d a t i o n a n d p r e ma t u r e d e l i v e r y. I s o t r e t i n o i n (1 3s- r e t i n o i c a c i, da n a n a l o g u e v ift a m i n,A h a s b e e n s h o w n t o ci) o c a u s e a c h a r a c t e r i s t i c p a t t e r n o f ma l f o r ma t i o n s k n os o t r e t itn o i n i wn as he e m b r y o p a t h y r v i t a m i n A e m b r y o p a. E v e n t o p i c a l r e t i n o i d s, s u c h a s e t r e t i n a t e, ma y h a v e the p o t e n t i a l t o c a u s e a b n o r ma l i t i e s. In the p a s t, s y n the t i c p r o g e s t i n s w e r e f r e q u e n t l y u s e d during pregnancy to stop abortion. The progestins ethisterone and n o r e t h i s t e r o n e h a v e c o n s i d e r a b l e a n d r o g e n i c a c t i v i t y, a n d ma n y c a s e s o f ma s c u l i n i za t i o n o f the g e n i t a l i a i n f e ma l e e mb r y o s h a v e b e e n r e p o r t e d.
Syndromes
- Taking a photo of the inner lining of the eye (fundus photography)
- Loss of appetite
- Most often feels sharp or stabbing
- What kind of shampoo, hair spray, gel, or other product do you put on your hair?
- Wear sunglasses with UV protection.
- DTap-HepB-IPV
Trusted cefuroxime 250mg
It then passes out to the lateral surface of the cerebral hemisphere at the insula of the lateral sulcus. Clinical options the center cerebral artery may be be} occluded by embolus or thrombus. The clinical image relies upon upon the location of occlusion and whether dominant or non-dominant hemisphere is affected. Occlusion at the insula Contralateral hemiplegia (leg comparatively spared) Contralateral hernianaesthesia and hemianopia All cortical branches are involved Aphasia (dominant) Neglect of contralateral limbs (non-dominant) Dressing issue When cortical branches are affected individually, the clinical image is much less extreme. The deep branches (perforating vessels) of the center cerebral artery may be be} a source of haemorrhage or small infarcts (lacunes see later). The vertebral artery runs from its origin through the foramen of the transverse processes of the mid-cervical vertebrae. It then passes laterally through the transverse means of the axis, then upwards to the atlas accompanied by a venous plexus and across the suboccipital triangle to the vertebral canal. After piercing the dura and arachnoid matter, it enters the cranial cavity through the foramen magnum. At the lower border of the pons, it unites with its fellow to form the basilar artery. The vertebral artery and its branches provide the medulla and the inferior surface of the cerebellum before forming the basilar artery. Clinical options Occlusion of the vertebral artery, when low within the neck, is compensated by anastomotic channels. When one vertebral artery is hypoplastic, occlusion of the other is equal to basilar artery occlusion. The shut relationship of the vertebral artery to the cervical backbone is necessary. Rarely, damage at intervertebral foramina or the atlanto-axial joints following subluxation may lead to intimal damage, thrombus formation and embolisation. Vertebral artery compression during neck extension may trigger signs of intermittent vertebrobasilar insufficiency. Stenosis of the proximal left or proper subclavian artery may lead to retrograde circulate down the vertebral artery on exercising the arm. This is often asymptomatic and demonstrated by the way by Doppler strategies or angiography. Anterior inferior cerebellar artery Vertebral artery Posterior inferior cerebellar artery Basilar artery the basilar artery supplies the brain stem from medulla upwards and divides eventually into posterior cerebral arteries as well as|in addition to} posterior speaking arteries which run forward to join the anterior circulation (circle of Willis). Clinical options Prodromal signs are widespread and should take the form of diplopia, visual subject loss, intermittent memory disturbance and a complete constellation of different brain stem signs: vertigo ataxia paresis paraesthesia Anterior spinal artery the whole basilar syndrome following occlusion consists of: impairment of consciousness coma bilateral motor and sensory dysfunction cerebellar indicators cranial nerve indicators indicative of the level of occlusion. Abnormal actions (hemiballismus) are related to visual loss, pupillary abnormalities, gaze palsies, impaired aware stage and disturbances of behaviour. Small perforating branches provide midbrain buildings, choroid plexus and posterior thalamus. Cortical branches provide the undersurface of the temporal lobe temporal department; and occipital and visual cortex occipital and calcarine branches. Occlusion of cortical vessels will produce a unique image with visual subject loss (homonymous hemianopia) and sparing of macular vision (the posterior tip of the occipital lobe, i. Posterior cortical infarction within the dominant hemisphere may produce issues in naming colors and objects. Cerebellum dysarthria, ipsilateral limb ataxia, vertigo and nystagmus (due to damage to vestibulo-floccular connections). The patient is paralysed and unable to discuss, though some facial and eye actions are preserved. The syndrome often follows basilar artery occlusion and carries a grave prognosis. Clinical syndromes are distinctive and usually end result from long-standing hypertension. In 80%, infarcts occur in periventricular white matter and basal ganglia, the remaining in cerebellum and brain stem. Lacunar or subcortical infarction accounts for 17% of all thromboembolic strokes and knowledge of commoner syndromes is crucial. Dysarthria/clumsy hand Lesion in dorsal pons Thalamus Clinical: Equal weak spot of contralateral face, arm and leg with dysarthria Vessel(s): Lenticulostriate A. Clinical: Dysarthria weak spot of ipsilateral face and tongue related to clumsy however sturdy contralateral arm. Ataxic hemiparesis Lesion in ventral pons (interruption of pontocerebellar fibres) Clinical: Mild hemiparesis with extra marked ipsilateral limb ataxia Vessel(s): Perforating department of Basilar A. Severe dysarthria with facial weak spot Lesion in anterior limb of inner capsule Clinical: Dysarthria, dysphagia and even mutism occur with gentle facial and no limb weak spot or clumsiness. Confirmation of lacunar stroke may save sufferers from unnecessary investigations for carotid and cardiac embolic source. Careful management of blood pressure and the use of of} aspirin often prevents recurrence. The prognosis of embolic infarction is determined by}: the identification of an embolic source. Symptoms are referable to the attention (retinal artery) and to the anterior and middle cerebral arteries, and take the form of: Visual loss transient, i. Focal or generalised seizures may persist for a while after the ischaemic episode. The majority of all cerebral emboli come up from ulcerative plaques within the carotid arteries (see page 244). Emboli arising from the aorta (atheromatous plaque or aortic aneurysm) often involve both hemispheres and systemic embolisation. Arrhythmias: Non-rheumatic (non-valvular) atrial fibrillation is the commonest explanation for cardioembolic stroke Bacterial endocarditis may give rise to septic cerebral embolisation with ischaemia an infection abscess formation. Non-bacterial endocarditis (marantic endocarditis): related to malignant disease fibrin and platelet deposition on heart valves. Patent foramen ovale may lead to paradoxical embolisation; suspect in patient with deep venous thrombosis who develops cerebral infarction. Onset is acute; if the patient survives the first 30 minutes, prognosis is superb. Tumour emboli lead to metastatic lesions; the onset is often slow and progressive. Acute stroke-like presentation may occur, adopted weeks or months later by the mass effects. Lung Melanoma Testicular tumours Lymphoblastic leukaemia Prostate Breast Renal generally metastasise to brain. Subtle changes occur within three hours in some artery) sufferers; most scans turn into irregular within 48 hours. Cardiac ultrasound (transthoracic or transoesophageal): this often reveals a cardiac embolic source in young people with stroke. Whilst of worth in sufferers with heavily calcified carotid plaques, immune to Doppler, it tends to overestimate the severity of stenosis. Its non-invasive nature makes it helpful in investigating the intracranial circulation. In sufferers where uncommon aetiologies are suspected and less invasive imaging has not been diagnostic for instance young sufferers or when cerebral vasculitis is suspected. The treatment of stroke has been the subject of many clinical trials and the following is a digest of the current advice primarily based on those studies. Treatment goals Recanalise blocked vessels Prevent progression of present occasion Prevent immediate complication Prevent the event of subsequent occasions Rehabilitate the patient. General measures Around the edge of an infarct, ischaemic tissue is at risk, however is potentially recoverable. This compromised however viable tissue should be protected by making certain an sufficient provide of glucose and oxygen. Factors which might have an effect on} this should be maintained hydration, oxygenation (maintain oxygen saturation over 95%), blood pressure (consider treatment if 185/110), glucose (maintain between 411 mmol/l).
Purchase 500 mg cefuroxime
Advanced technique for the identification of patients with inherited hypercholesterolemia. Development of a high-resolution melting technique for mutation detection in familial hypercholesterolaemia patients. The effect of pravastatin on coronary occasions after myocardial infarction in patients with common cholesterol levels. Hospitalizations for coronary artery illness amongst patients with systemic lupus erythematosus. Tonelli M, Keech A, Shepherd J, Sacks F, Tonkin A, Packard C, Pfeffer M, Simes J, Isles C, Furberg C, West M, Craven T, Curhan G. Collins R, Armitage J, Parish S, Sleigh P, Peto R; Heart Protection Study Collaborative Group. Wenke K, Meiser B, Thiery J, Nagel D, von Scheidt W, Steinbeck G, Seidel D, Reichart B. Simvastatin reduces graft vessel illness and mortality after heart transplantation: a four-year randomized trial. The efficacy and tolerability of ezetimibe in cardiac transplant recipients taking cyclosporin. Knowledge and attitudes relating to heart problems threat and prevention in patients with coronary or peripheral arterial illness. Basic data concerning related coronary illness in peripheral vascular patients. Effects of statin therapy on the progression of carotid atherosclerosis: a systematic review and meta-analysis. Statins in stroke prevention and carotid atherosclerosis: systematic review and up-to-date meta-analysis. Do lipids, blood strain, diabetes, and smoking confer equal threat of myocardial infarction in girls as in men? Impact of gender in primary prevention of coronary heart illness with statin therapy: a meta-analysis. Gransbo K, Melander O, Wallentin L, Lindback J, Stenestrand U, Carlsson J, Nilsson J. Cardiovascular and most cancers mortality in very elderly post-myocardial infarction patients receiving statin therapy. Ten-year threat of cardiovascular indidence related to diabetes, prediabetes, and the metabolic syndrome. Overproduction of very low-density lipoproteins is the hallmark of the dyslipidaemia within the metabolic syndrome. Effects of fenofibrate therapy on heart problems threat in 9,795 people with type 2 diabetes and various elements of the metabolic syndrome. Effect of lifestyle intervention on the occurrence of metabolic syndrome and its elements within the Finnish diabetes prevention research. Influence of low high-density lipoprotein ldl cholesterol and elevated triglyceride on coronary heart illness occasions and response to simvastatin therapy in 4S. Fibrates within the prevention of heart problems in patients with type 2 diabetes mellitus-a pooled meta-analysis of randomized placebo-controlled clinical trials. Benefits of niacin by glycemic status in patients with healed myocardial infarction (from the Coronary Drug Project). Mortality from heart illness in a cohort of 23,000 patients with insulin-treated diabetes. The effects of simvas tatin on the incidence of heart failure in patients with coronary heart illness. Relation of atherosclerotic changes in retinal arteries to the extent of coronary artery illness. Can statins reduce perioperative morbidity and mortality in patients undergoing non-cardiac vascular surgery? Reduction in cardiovascular occasions after vascular ~ surgical procedure with atorvastatin: a randomized trial. Lipid administration within the prevention of stroke: review and updated meta-analysis of statins for stroke prevention. Quantifying effect of statins on low density lipoprotein ldl cholesterol, ischaemic heart illness and stroke: systematic review and meta-analysis. Final conclusions and recommendations of the National Lipid Association Statin Safety Assessment Task Force. Relationship between adherence to evidence-based pharmacotherapy and long-term mortality after acute myocardial infarction. In view of its significance in spinal ischemia, an analysis is required of the anatomic vocabulary used to describe the spinal twine blood provide to enhance understanding of the topic. The major provide is the Adamkiewicz artery, also known as|also called|also referred to as} nice anterior radicular artery. The literature was reviewed to equate the totally different nomenclatures employed and an accurate description of present data on spinal twine vascularization was prepared. Resumo A intrincada anatomia tridimensional da irrigaзгo medular й frequentemente explanada na literatura com diferentes nomenclaturas e devido a sua alta relevвncia no estudo da isquemia medular, o estudo da terminologia se faz necessбrio para melhor compreensгo do tema. A artйria de Adamkiewicz, tambйm chamada de artйria radicular magna, й a through principal. Foi realizada a revisгo da literatura com equiparaзгo das nomenclaturas utilizadas e elaboraзгo de descriзгo acurada e sumarizada do conhecimento atual sobre a vascularizaзгo medular. Conflicts of curiosity: No conflicts of curiosity declared concerning the publication of this article. However, the vasculature involved is complicated and difficult to research because of the small caliber of arteries, which make up an intricate three-dimensional network with a large diploma of anatomic variation. Most frequent Aorta Segmental Arteries Vertebral branch Dorsal branch Radiculomedullary artery anterior radicular artery Posterior branch of the radicular artery Posterolateral spinal artery Anterior spinal artery Artery of Adamkiewicz Lumbar arteries Intercostal arteries Sulcal arteries Pial plexus the intercostal and lumbar arteries that provide the spinal marrow originate within the aorta, as do the subclavian and hypogastric branches. The intercostal and lumbar arteries divide thrice before reaching the spinal twine. The first branch is the spinal branch, which divides into the anterior and posterior radicular arteries and, farther on, bifurcates into the dorsal and vertebral branches. The last bifurcation of the spinal branch is fixed for anterior and posterior provide of the vertebral canal, of the nerve roots and of the dura mater, at some ranges only, and the anterior and posterior radicular arteries pass via the dura mater and attain the marrow. Generally, one of many anterior radicular arteries is dominant phrases of|when it comes to|by way of} caliber and identified as|is called|is named} the nice anterior radicular artery or Adamkiewicz artery (Figure 2). Arteries that provide the spine are divided between a central system, fed by the sulcal arteries, and a peripheral system, the pial plexus, which supplies origin to perforant branches (Figure 2). Posteriorly, there simply one|is only one} posterior spinal vein, somewhat than two smaller posterolateral veins, and that is regularly of smaller caliber than the anterior median vein. There is an axial network of small arteries within the spinal canal, in paravertebral tissues and in paraspinal muscle tissue that anastomose with one another and with the arteries supplying the spinal marrow; the entry to this network contains segmental vessels (intercostal and lumbar arteries), subclavian arteries, hypogastric arteries and their branches (Figure 4). All of those vessels are interconnected and anastomose with the subclavian arteries cranially and the hypogastric arteries caudally. Alexandre Campos Moraes Amato, Noedir Antфnio Groppo Stolf this collateral network can present compensatory move to the spinal twine within the event of occlusion of the bigger caliber routes,31 and the move from one source can increase when one other is decreased; or vice versa: move can reduce if a low resistance alternative route is opened, i. Standardization of the terminology is critical and the recommendations for use in Portuguese made on this research are based on present anatomic terminology. The clinical significance of anatomic data of this region lies in planning for endovascular surgical procedure procedures on the aorta, so as to to} reduce the chance of ischemia, avoiding pointless occlusion of the spinal blood provide. The mathematical algorithm employed identified intraoperative hypotension and simultaneous exclusion of a minimum of|no much less than} two spinal provide territories as related to the genesis of ischemia, and it was concluded that extensive exclusion of the intercostal arteries alone was not related to symptomatic spinal ischemia. The mechanism of spinal ischemia after endovascular repair of thoracic aorta aneurysms has not been totally elucidated and is outwardly related to an intricate mechanism of several of} different factors, and never completely to everlasting interruption of provide through the segmental artery. However, in acute conditions, similar to surgical procedures, spinal perfusion relies on the gradient of arterial blood strain and of cerebrospinal fluid. Albert Adamkiewicz (1850-1921)-his artery and its significance for the retroperitoneal surgeon. Albert Wojciech Adamkiewicz: the discoverer of the variable vascularity of the spinal twine.
Best cefuroxime 250mg
Free tissue transfer ("free flap") for breast reconstruction following mastectomy. For details, see Grafts & Flaps (Chapter 6), Gender Affirmation Surgery (Chapter 23), Composite Tissue Allotransplantation (Chapter 25), and Lymphedema (Chapter 26) 165 Figure 2. Free tissue transfer of three toes, including bone, tendon, artery, vein, and nerve reconstruction. Other indications for microvascular techniques (magnification, precision tools) 1. Bleeding / clotting disorders (hypercoagulable state will increase flap failure rate) D. Begin with dissection of tissue for transfer (+vessels) and exposure of recipient vessels C. Magnification is used during dissection, anastomosis (of artery, vein, and/or lymph vessels), and nerve coaptation F. The end of each vein has been pulled by way of the rings and everted onto the sharp pins. As the coupler is closed, opposing pins will interdigitate to seal the veins collectively. Clinical photograph (left) and sketch (right) of a free flap with 1 artery and a couple of|and a pair of} veins attached. Preoperative picture (upper left) and postoperative picture at 28 months (lower left). Probe positioned round artery or vein during surgical procedure, connects to exterior move monitor (Figure 7) B. A small silastic cuff probe (left lower) is positioned around the vessel (right) and connected to an exterior move monitor (upper left). May be integrated into residency training or offered as a stand-alone course 171 Figure 8. Albany Medical Center residents practicing microsurgical techniques with surgical loupes (foreground) and operating microscope (background). Implantable Venous Doppler Monitoring in Head and Neck Free Flap Reconstruction Increases the Salvage Rate. Distinct entity from these people with congenital disorders of sexual development/ambiguous genitalia C. Desire to costume and reside as reverse gender (and make his/her physique a more in-depth} resemblance to the alternative gender) 2. Feminization by way of suppression of androgens and induction of feminine traits i. Special consideration must be taken for adolescents, and puberty suppression may be be} indicated four. Current debate about whether or not or not may be a|it is a} biological or psychosocial dysfunction H. Transsexualism is recorded throughout historical past, significantly in Greek and Roman literature B. Publishes "Standards of Care for the Health of Transsexual, Transgender, and Gender Nonconforming People" which is now in its seventh version three. Frontonasal-orbital complex is biggest defining characteristic of male vs feminine face 2. Increased supraorbital bossing, distinguished brow and glabella, brow more angled b. A more acute glabellar angle, a more acute nasal tip angle, a less open nasolabial angle, and a more pronounced chin are preferred in males. Skin graft creation of a vaginal canal, similar to McIndoe operation or with use of grafts from penile skin i. Pedicled penile and scrotal flaps for creation of neovagina and labia (from deep exterior pudendal, superficial perineal, and funicular arteries) iv. Anterior penile flap and posterior scrotal flap to create vaginal canal a) Can add skin graft for more length v. Cons: Need for dilation, need for pre-op hair elimination, might have revisions/labiaplasty for additional feminization Figure 2. Surgical Outcome after Penile Inversion Vaginoplasty: A Retrospective Study of 475 Transgender Women. Pros: vascularized vagina with moist lining, lowering the necessity for dilation and lubrication iii. Cons: intraabdominal operation, constant lubrication (sometimes excessive) that may be} malodorous, diversion colitis, stricture and cancer of the reconstruction Figure three. Long-Term Outcomes of Rectosigmoid Neocolporrhaphy in Male-to-Female Gender Reassignment Surgery. Subcutaneous keyhole or periareolar mastectomy for small breasts with minimal skin extra ii. Double incision mastectomy with free nipple grafts for medium and large/ptotic breasts Figure four. Stretching the hormonally hypertrophied clitoris, lengthening urethra with local flaps ii. Pros: tactile and erogenous sensate clitoral tissue, sustained erectile rigidity with out prostheses, minor donor site scarring, shorter hospitalization v. Cons: very small phallus so unlikely to ready to|be capable of|have the flexibility to} provide penetration, impaired standing urination 182 Figure 8. Result of metaoidioplasty and scrotum construction in a slim, 30-year-old feminine transsexual who has been on hormonal therapy for six years. Inferiorly based mostly abdominal flaps a) Less aesthetic and better complication price b) Easier to cover donor site scars c) Diminished sensation d) Variability in vascular pattern e) Limited capability to void standing and unable to provide sexual penetration v. Pedicled groin flaps a) Similar to abdominally based mostly flaps b) Insensate c) Functional issues the same as abdominal flaps vi. Gracilis flap a) Bipedicled design with two flaps b) Urethra produced from skin graft 183 Figure 9. The internal conduit becomes the neourethra, and the outer tubularized tissue represents the neophallus. The semicircular extension at the distal portion of the flap more accurately approximates the circumcised male phallus. Radial forearm a) Most generally used b) Tube within a tube neourethra c) Can be sensate d) Pros: aesthetic reconstruction, standing urination, tactile and erogenous sensation e) Cons: donor site morbidity, urinary fistulas/strictures, requires prosthesis ii. Osteocutaneous fibula a) Can be made sensate b) Does not require a prosthesis iii. Can be made practical with inclusion of muscle/nerve and find a way to|could possibly|might find a way to} have erectile operate Figure 10. Illustration of the radial forearm free flap and the fibula osteocutaneous free flap. In the osteocutaneous free fibula flap, the fibula is harvested with a cuff of muscle, the peroneal artery, and either the lateral or posterior sural nerve to create the sensate phallus. In the radial forearm free flap, the tube-in-tube design is used to create a neophallus and neourethra in a single flap. The radial artery and the antebrachial nerves are harvested to create the sensate phallus. A distal circumferential portion of the neophallus shaft is elevated and rolled to create the corona. Once joined collectively round a skin graft used for the neourethra, another skin graft is positioned around the muscle. The groin flap with or with out the iliac bone could be performed in either one or two phases. The twostage process relies on the superficial circumflex iliac artery and the deep circumflex iliac artery. The lateral and medial skin edges of the flap are sutured collectively, constructing a tube nonetheless attached to the physique. The neourethra is reconstructed utilizing a full thickness skin graft from the contralateral groin. Gender-confirming facial surgical procedure: issues on the masculinity and femininity of faces. LongTerm Outcomes of Rectosigmoid Neocolporrhaphy in Male-to-Female Gender Reassignment Surgery. Monstrey S, Selvaggi G, Ceulemans P, Van Landuyt K, Bowman C, Blondeel P, Hamdi M, De Cuypere G.
Generic 250 mg cefuroxime
Effectiveness of cricoid pressure in preventing gastric aspiration throughout rapid sequence intubation in the emergency division: research protocol for a randomised managed trial. Adverse hemodynamic effects of interrupting chest compressions for rescue breathing throughout cardiopulmonary resuscitation for ventricular fibrillation cardiac arrest. Guidelines for the acute medical management of severe traumatic mind harm in infants, kids, and adolescentssecond edition. Phase three (72 to 96 hr):returnofnonspecificsymptomsaswellas evidenceofliverfailure. Acetaminophen plasma concentration 2 le ib ss he pa tic to ty ci xi 26 Part I Pediatric Acute Care three. Provide schooling about decreasing environmental lead exposure and decreasing dietary lead absorption* Perform environmental assessment in homes constructed earlier than 1978 Follow repeat blood lead testing tips (see Table 2. Advisory Committee on Childhood Lead Poisoning Prevention of the Centers for Disease Control and Prevention. Diphenhydramine and dimenhydrinate poisoning: An evidence-based consensus guideline for out-of-hospital management. Pharmacology, pathophysiology and management of calcium channel blocker and beta-blocker toxicity. Laundry detergent "pod" ingestions: a case collection and discussion of current literature. Acute toxicity due to of} the confirmed consumption of artificial cannabinoids: scientific and laboratory findings. Sedation and analgesia must be deliberate prematurely, and the dangers of such explained to the father or mother and/or affected person as applicable. Proper sterile method is important to attaining good wound closure, decreasing transmittable illnesses, and preventing wound contamination. Ultrasound caveats important for sure procedures are famous under, where relevant. Linear transducers use high frequencies to produce high decision images and are primarily used for procedures in pediatrics. Though they provide a large space of pores and skin contact to facilitate procedures near concave and convex surfaces, larger curvilinear probes are troublesome to use in young children. Ensure sufficient contact by using enough ultrasound gel and making use of comfy pressure on the pores and skin. Depth: Adjust to visualize construction of curiosity and a minimum of|no much less than} a centimeter of tissue under that construction. Indications: Blood sampling in infants for laboratory research much less affected by hemolysis. Alternate between squeezing blood from the leg toward the heel (or from the hand toward the finger) after which releasing the pressure for several of} seconds. After eradicating tourniquet, connect a syringe and apply mild adverse pressure to withdraw blood for serum sampling. Perform this by sliding the probe along the course of the vessel and figuring out its course and branching. Infiltration round deeper vessels is also be|can be} a risk, as a shorter length of catheter resides in the vessel after insertion. Insert the needle into the pores and skin at a shallow (usually <30-degree) angle to the pores and skin at the midline of the probe near where it contacts the pores and skin. Restrain affected person securely and place with head turned away from facet of cannulation. Position with towel roll under shoulders or with head over facet of mattress to prolong neck and intensify the posterior margin of the sternocleidomastoid muscle on the facet of venipuncture. The exterior jugular vein will distend if its most proximal phase is occluded or if the kid cries. With continuous adverse suction on the syringe, insert the needle at a couple of 30-degree angle to the pores and skin. Indications: Arterial blood sampling or frequent blood fuel and continuous blood pressure monitoring in an intensive care setting. It is optionally available to infiltrate the world over the point of maximal impulse with lidocaine. Once the sample is obtained, apply agency, constant pressure for five minutes after which place a pressure dressing on the puncture web site. Prepare the wrist with sterile method and infiltrate over the point of maximal impulse with 1% lidocaine. Alternatively, cross the needle and catheter by way of the artery to transfix it, after which withdraw the needle. After the sterile field has been prepped, apply gel to the probe and place within a sterile cover. Place the ultrasound probe transverse to the artery on the radial, posterior tibial, or dorsalis pedis pulse. With the probe visualizing the vessel transversely, slowly advance the needle and observe the tip of the needle by sliding the probe away. Indications: Arterial blood sampling when radial artery puncture is unsuccessful or inaccessible. Posterior tibial artery: Puncture the artery posterior to medial malleolus whereas holding the foot in dorsiflexion. Complications: Infection, bleeding, arterial or venous perforation, pneumothorax, hemothorax, thrombosis, catheter fragment in circulation, air embolism. Ultrasound guidance: Has turn out to be commonplace apply to facilitate placement of internal jugular vein central venous catheters. Subclavian vein: Risks embody pleural harm, pneumothorax, hemothorax, or pleural infusion causing hydrothorax nicely as|in addition to} subclavian artery harm. It is technically very troublesome in patients with cervical collars and tracheostomies and discouraged in these cases if one other route is available. Patient is supine in slight Trendelenburg position, with neck prolonged over a shoulder roll and head rotated away from facet of approach. Introducer needle enters along anterior margin of sternocleidomastoid about halfway between sternal notch and mastoid process and is directed toward the ipsilateral nipple. Introducer needle enters at the point where exterior jugular vein crosses posterior margin of sternocleidomastoid and is directed under its head toward sternal notch. The guidewire may be seen as a shiny, hyperechoic line (G) crossing the wall of the vein after which remaining in the lumen of the jugular vein. Insert the needle simply lateral to the proximal angle of the clavicle, had been the medial third and lateral two-thirds of the clavicle meet. The ultrasound may be placed longitudinally over the vessel to view the guidewire, if desired. This may be very useful throughout cardiopulmonary arrest, shock, burns, and life-threatening standing epilepticus. Complications embody extravasation of fluid from incomplete or by way of and thru cortex penetration, infection, bleeding, osteomyelitis, compartment syndrome, fat embolism, fracture, epiphyseal harm. In apply, cannulation of the femoral vein should take place distal to the inguinal ligament. Insertion point is in the midline on medial flat floor of anterior tibia, 13 cm (2 fingerbreadths) under tibial tuberosity. Medial floor of the distal tibia 12 cm above the medial malleolus (may be a more effective web site in older children). Proximal humerus, 2 cm under the acromion process into the higher tubercle with the arm held in adduction and internal rotation. If the kid is conscious, anesthetize the puncture web site down to down to} the periosteum with 1% lidocaine (optional in emergency situations). Marrow may be despatched to decide glucose levels, chemistries, blood types and cross-matches, hemoglobin levels, blood fuel analyses, and cultures. It is contraindicated in the presence of potential necrotizing enterocolitis or intestinal hypoperfusion. A high line could also be} recommended in infants weighing less than 750 g, in whom a low line might easily slip out. Identify the one massive, thin-walled umbilical vein and two smaller, thick-walled arteries. If resistance is encountered, attempt loosening umbilical tape, making use of regular and delicate pressure, or manipulating the angle of the umbilical wire to the pores and skin.

Best cefuroxime 500 mg
Varicocele Varicosities of the testicular veins could develop in boys around puberty. Treat ment is indicated for symptoms (dragging, aching), impairedtesticulargrowthand,inlaterlife,forinfertil ity. Obliterationofthetesticularveinscanbeachieved by standard surgery, laparoscopic strategies or radiological embolisation. Torsion of testicular appendage A hydatid of Morgagni is an embryological remnant discovered on the upper pole of the testis. The ache could improve over 1 or 2 days and infrequently the tortedhydatidcanbeseenorfelt(thebluedotsign). Surgical exploration and excision of the appendage leadstorapidresolutionoftheproblem. Other causes Viral or bacterial epididymoorchitis or epididymitis could trigger an acute scrotum in infants and toddlers, and scrotal exploration is commonly necessary to confirm thediagnosis. Ifanassociatedurinarytractinfectionis current, antibiotic remedy and full investigation of the urinary tract shall be required. Other conditions which can trigger scrotal symptoms and indicators are idi opathic scrotal oedema (usually painless, bilateral the acute scrotum Torsion of the testis Testiculartorsionismostcommoninadolescentsbut could happen at any age, including the perinatal interval. When his testes are examined, the right testis is foundtobeslightlyswollenandlyinghigherinthe scrotumthanthelefttestis(Fig. Althoughhe has not complained of testicular ache, the testis is tender on palpation. Thiscasehighlights: · Theclinicalfeaturesoftesticulartorsionarevaria ble and may be potentially deceptive, with ache predominantly referred to the stomach or inguinalregionandminimalpainfeltinthetestis itself · Abdominalexaminationisnevercompletewithout inspectionandgentlepalpationofbothtestes · Withtorsion,thetestisisalwaystender. Abnormalities of the penis Hypospadias In the male fetus, urethral tubularisation occurs in a proximaltodistaldirectionundertheinfluenceoffetal testosterone. Failure to complete this process leaves theurethralopeningproximaltothenormalmeatuson the glans and that is termed hypospadias. Hypospadiasconsistsof: Glanular hypospadias may be be} a solely beauty con cern, but more proximal varieties could trigger func tional issues including an incapability to micturate in a traditional path and erectile deformity. Surgery · · A ventral urethral meatusinmostcasesthe urethraopensonoradjacenttotheglanspenis, butinseverecasestheopeningmaybeonthe penileshaftorintheperineum(Fig. Infants with hypospadias must not be circumcised, because the foreskin is commonly needed for later reconstructive surgery. Genitalia 351 1 Correction is commonly undertaken before 2 years of age, oftenasasinglestageoperation. Theaimsofsurgery aretoproduce: Hypospadias 19 Genitalia Commonest sorts Increased incidence of different genitourinary abnormalities Normal urethral meatus Urethral groove Glanular Coronal Midshaft Types of hypospadias Urethral meatus Penoscrotal Figure 19. These adhesions separate spontaneously with time, allowing the foreskin to become more cellular and ultimately retractile. At 1 yr of age, roughly 50% of boys have a non-retractile foreskin,butby4yearsthishasdeclinedto10%,andby16 yearstoonly1%. Anonretractileforeskinoftenleads to ballooning on micturition, which is physiological. Gentleretractionoftheforeskinatbathtimeshelpsto keep hygiene, but forcible retraction of a healthy nonretractileforeskinshouldbeavoided. Circumcision is one of the|is among the|is probably considered one of the} earliest recorded operations and stays an necessary tradition within the JewishandMuslimreligions. Unlikecircum cision, preputioplasty conserves the foreskin and resultsinlesspostoperativediscomfortandfewercom plications. However, regular retraction of the foreskin isrequiredinthefirstfewweeksaftersurgeryandfor this cause, preputioplasty is better suited to older boyswhoarewillingtodothis. Topical corticosteroids Applicationofatopicalsteroidointmenttotheprepuce has been shown to facilitate retraction of a non retractile prepuce, with success rates of as much as} 80%. Different remedy regimens have been described but typically the ointment is utilized twice day by day for 23months. Surgery Circumcision for medical indications is carried out underageneralanaestheticasadaycase. Theforeskincanusuallybe reduced, but sufficient analgesia (often a common anaesthetic)isneededtoachievethis. Summary Genital conditions in male infants and children Inguinal hernia: · Presentation intermittent swelling within the groin or scrotum on crying or as an irreducible lump · Repair promptly to avoid the risk of strangulation · If irreducible sustained mild compression with analgesia to reduce, followed by delayed surgery An undescended testis: · Is current in about 4% of full-term male infants but only one. Parents should be advised about hygiene, the avoidance of bubble bathtub and scented soaps and the usage of} loosefitting cotton underwear. Swabs should be taken to establish any pathogens, whichcanthenbespecificallytreated. Oestrogen cream utilized sparingly to the vulva could relieve the issue in resistant circumstances by increasingvaginalresistancetoinfectionasprepuber taltissuestendtobeatrophic. Ifthereareanyconcerns about sexual abuse, the child have to be seen by a paediatrician(seeCh. Rarely,androgeninsensitivity syndrome (testicular feminisation) can current as a herniainaphenotypicfemalewhoactuallyhasamale genotype. In extended (persistent) neonatal jaundice, check if it is conjugated hyperbilirubinaemia, as this as a result of|as a result of} of} liver illness. Hepatic dysfunction Encephalopathy Jaundice Epistaxis Varices with portal hypertension Spider naevi Muscle wasting from malnutrition Bruising and petechiae Splenomegaly with portal hypertension Hypersplenism Hepatorenal failure Liver palms Peripheral neuropathy Rickets secondary to vitamin D deficiency Clubbing Loss of fat shops secondary to malnutrition Neonatal liver illness Many newborn infants become clinically jaundiced. This is usually an unconjugated hyperbilrubinaemia, which resolves i spontaneously(Box20. Prolongedneonataljaundice caused by liver illness is characterised by a raised conjugated bilirubin (>20µmol/L) and is usually accompaniedby: Cholestasis: · fat malabsorption · deficiency of fat-soluble nutritional vitamins · pruritus · pale stools · darkish urine Ascites Hypotonia · · · · Palestools Darkurine Bleedingtendency Failuretothrive. There is an urgency to diagnose liver illness as early aspossibleintheneonatalperiod,becauseearlydiag nosisandmanagementimprovesprognosis. Babies with biliary atresiahaveanormalbirthweightbutfailtothriveas the illness progresses. They are usually mildly jaun dicedand,followingpassageofmeconium,theirstools are pale and their urine darkish. Although stool colour mayfluctuate,palestoolsisanimportantabnormality and warrants investigation, even within the absence of scientific jaundice. Hepatomegaly is commonly current and splenomegaly will develop secondary to portal hypertension. Afastingabdominalultrasound could demonstrate a contracted or absent gallbladder, though it could be regular. Liver biopsy demonstrates features of extrahepatic biliaryobstruction,althoughfeaturesmayoverlapwith thoseofneonatalhepatitis,especiallyifcarriedoutat an early stage of the illness. The prognosis is con firmed at laparotomy by operative cholangiography whichfailstooutlineanormalbiliarytree. Treatmentconsistsofsurgicalbypassofthefibrotic ducts, hepatoportoenterostomy (Kasai procedure), in which a loop of jejunum is anastomosed to the reduce surfaceoftheportahepatis,facilitatingdrainageofbile fromanyremainingpatentductules. Ifsurgeryisper shaped before the age of 60 days, 80% of kids obtain bile drainage. Postoperativecomplicationsinclude cholangitis and malabsorption of fat and fatsoluble nutritional vitamins. Biliary atresia is the one commonest indication for liver transplanta tioninthepaediatricagegroup. Choledochal cysts these are cystic dilatations of the extrahepatic biliary system. Intheolderagegroup,choledochalcystspresentwith stomach ache, a palpable mass and jaundice or cholangitis. Treatmentisbysurgicalexci sionofthecystwiththeformationofaRouxenYanas tomosis to the biliary duct. In distinction to biliary atresia, these infants mayhaveintrauterinegrowthrestrictionandhepato splenomegalyatbirth. There are many phenotypes of the protease inhibitor (Pi)whicharecodedonchromosome14. The majority of kids who current with 1 antitrysindeficiencywilleitherhaveprolongedneona taljaundiceor,lesscommonly,bleedingduetovitamin K deficiency (haemorrhagic illness of the newborn). At 5 weeks of age, he pre sentedwithpoorfeedingandvomitingandahistory of bruising on his brow and shoulders. In persistent neonatal jaundice, early prognosis of biliary atresia improves the prognosis.
References:
- https://iuristebi.files.wordpress.com/2011/07/law-for-non-law-students.pdf
- https://www.acc.org/~/media/Non-Clinical/Files-PDFs-Excel-MS-Word-etc/Tools%20and%20Practice%20Support/Quality%20Programs/Heart%20Failure%20Roundtable%202016/Heart%20Failure%20Guidelines/HFG%203%202013%20ACCFAHA%20Guideline.pdf
- https://lms.rn.com/getpdf.php/2058.pdf