.png)
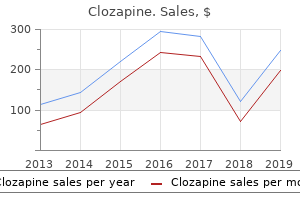
Order 50mg clozapine
Marginal revenue tax rates enhance with revenue, and so this approach will most likely to|are inclined to} understate wage alternative rates by a greater margin for higher-income staff. Because of variations across occupations in earnings dynamics and protection by cancer presumptions, all estimates are presented separately by occupation for the four occupation teams outlined in Chapter 2: peace officers, firefighters, lifeguards, and other occupations. Peace officers, firefighters, and staff in other occupations all expertise sharp reductions in earnings within the years following a cancer declare. Employment rates for these teams of staff are reported within the second panel of the desk. Compared with staff in other occupations, public security staff have very high employment rates two years prior to harm. Two years after harm, employment has dropped substantially for public security staff, from nearly 100 percent to 83 percent for peace officers and eighty four percent for firefighters. Declines in employment for lifeguards are extra muted, with ninety two percent employed two years after harm. Workers in other occupations are very probably to|prone to} cease working within the two years following a cancer declare: solely 37 percent are employed two years after the date of harm. While this group also has much less steady employment than public security staff prior to harm (with Table 3. Earnings and Employment for Workers with Cancer Claims, by Occupation Other Occupations $51,094 $52,596 $24,264 $17,599 88. As we mentioned in Chapter 2, a management group is required to isolate earnings and employment losses as a result of} cancer. Earnings Losses Due to Cancer for Workers Filing Cancer Claims Our primary estimates of earnings losses give attention to} complete earnings over two years after the date of harm. Before turning to these estimates, we current event-study estimates to illustrate how the earnings of staff with cancer claims modified comparability to|compared to} comparable staff with medicalonly claims from two years before to two years after harm. The stable colored traces with markers present the precise earnings of staff with cancer claims in every of the four occupation teams. Actual earnings are simply pattern averages; counterfactual earnings were constructed by subtracting event-study coefficients from our weighted least squares regression fashions from precise earnings. Counterfactual earnings are estimated based on weighted least squares regression fashions described in Chapter 3 and the Appendix utilizing medical-only injuries from staff in the identical occupation as a management group. The sample noticed for lifeguards reflects the seasonality of lifeguard employment; this distinctive sample underscores the importance for the current examine of utilizing a management body of workers with medical-only injuries whose occupations may be noticed. The very close match between precise earnings for staff with cancer and our estimated counterfactual gives us high confidence within the validity of our earnings loss estimates based on the weighted management group. After the date of harm, earnings for staff with cancer claims in three out of four occupation teams diverge from earnings for the (weighted) medical-only management group. For peace officers and especially for firefighters, the date of harm corresponds 28 to a noticeable drop in earnings even for staff with minor injuries. It is believable that a number of the} firefighters with cancer claims at these ages would have retired even within the absence of cancer; the info on medical-only claims suggest that that is the case. Effects of Cancer on Earnings, Employment, and At-Injury Employment over Two Years After Date of Injury, by Occupation Peace Officers Change in earnings over two postinjury years ($) [95% confidence interval] Change in employment two years after harm [95% confidence interval] Change in at-injury employment two years after harm [95% confidence interval] �$18,159 Firefighters �$10,499 Lifeguards $3,194 Other Occupations �$43,058 [�$23,204, �$13,114] �9. Even though staff in other occupations have earnings less than half the level noticed among peace officers and firefighters before the declare, their losses in dollar phrases ($43,000) exceed those for any occupation group examined on this examine. Other than lifeguards, staff who file cancer claims expertise sizable earnings losses over the two years after the date of harm. In the two years after the date of harm, firefighters lose $10,500, peace officers lose $18,000, and staff in other occupations 29 lose $43,000. A cancer declare reduces the probability of employment by 3 percent for firefighters, 10 percent for peace officers, and 37 percent for staff in other occupations. We also examined the probability that staff remained employed at the similar employer the place they filed the cancer declare and found that reductions in employment at the at-injury employer were very near reductions in general employment. These other components embody modifiers for age and occupation, as well as|in addition to} the impression of apportionment. The ranking of occupations by common standard rating is equivalent to the ranking of occupations by common earnings loss. As with standard rankings, common rankings within the constant-maturity pattern were slightly lower. Many cancer claims are reported later (relative to the date of injury) than is the norm for harm claims (which must sometimes be reported inside 30 days of injury) or even for other occupational sicknesses (which must sometimes be reported inside one 12 months of the date of diagnosis or attribution to occupational exposures). To consider the robustness of our estimates to reverse causation associated with claims may be} filed with a considerable delay, we estimated our primary regression fashions on a pattern that excluded all claims (both cancer claims and medical-only claims) filed more than ninety days (approximately three months) after the date of harm. Average constant-maturity standard rankings are 1 to 2 rating points lower than the general common for public security staff, and 5 rating points lower for staff in other occupations. Disability Ratings for Cancer Cases Evaluated at the State Disability Evaluation Unit Peace Officers Average mixed rating All rankings N Constant-maturity rankings N Average last rating All rankings N Constant-maturity rankings N 15. This desk is restricted to the constant-maturity pattern of rankings introduced in Table 3. While this difference in rankings within the pattern noticed right here is necessary because of|as a result of} it impacts the distribution of ultimate rankings, the statistical insignificance of this difference signifies that we could see an increase this large as a result of} chance (and not as a result of} any systematic change in case combine or rating practices). As a result, comparison of rankings over time may be very misleading unless a constant-maturity pattern of rankings is used. Disability Ratings for Constant-Maturity Cancer Cases Evaluated at the State Disability Evaluation Unit, by Injury Date Peace Officers Average mixed standard rating 2005�2012 injuries (constant-maturity) N 2013�2015 injuries (constant-maturity) N p-value for difference Average last rating 2005�2012 injuries (constant-maturity) N 2013�2015 injuries (constant-maturity) N p-value for difference 17. The proportion of staff receiving every kind of benefits is reproduced from Table 2. As a result, common death benefits are extra comparable across occupations, averaging $206,449 for peace officers with death benefits, $209,340 for firefighters with death benefits, and $169,587 for staff in other occupations with death benefits. While this final quantity is slightly lower than the minimal death profit, we note that we analyzed each paid amounts (which are still ongoing at the time of information assortment in some cases) and settled amounts (which lower than the statutory profit amount); public security staff may also have extra dependents at the time of death than staff in other occupations. Differences in death profit payments for the average cancer declare are driven primarily by variations within the proportion of staff whose dependents receive death benefits, quite than variations within the paid quantity. To sum up, patterns of profit receipt and common paid amounts were broadly comparable for firefighters and peace officers, but look fairly different for staff in other occupations. Pretax Wage Replacement Rates over Five Years, by Occupation Peace Officers 5-year earnings losses (extrapolated) (Standard error) Average profit payments Pretax wage alternative rates $40,826 ($5,205) $19,860 49% Other Occupations $103,669 ($6,920) $40,122 39% Firefighters $25,966 ($6,536) $22,407 86% Lifeguards �$14,850 ($5,778) $3,266 >100% occupation. We estimate that the pretax wage alternative fee is 86 percent for firefighters, 49 percent for peace officers, and 39 percent for staff in other occupations. Both to assess the credibility of these estimates and to present context, we evaluate these estimates with a small variety of high-quality peer-reviewed studies on the earnings and employment of cancer survivors. In particular, we focus findings from cohort studies that used longitudinal information on cancer patients with a sound management group (similar to the research design out there for this study). These studies have sometimes focused on a general nonelderly cancer patient population recruited by way of a set of hospitals or other treatment facilities; comparison teams are sometimes composed of cancer-free individuals in public-use surveys. Much of the most effective proof comes from Scandinavian countries, the place researchers have had nice success in linking administrative revenue information to a wide range|a variety} of datasets on well being and incapacity. They found that breast cancer diagnosis led to a substantially greater probability that women would 11 In Dworsky et al. Reduced earnings relative to the management group pale over time and were statistically insignificant by five years after diagnosis. An earlier examine utilizing the Finnish Cancer Registry examined all instances diagnosed in 1987�1988 no matter cancer kind and in contrast employment probabilities between cancer survivors and staff the identical age and gender (Taskila-Abrandt et al. Another examine from Norway offered the only longitudinal estimates we were place to} locate of earnings losses as a result of} cancer. Syse, Tretli, and Kravdal (2008) used the Cancer Registry of Norway linked to administrative earnings information to examine employment and earnings variations between cancer survivors and cancer-free patients. While the examine is primarily cross-sectional in nature, differences-in-differences estimates confirmed earnings losses of 8�16 percent of median earnings for men and 10�15 percent of median earnings for girls, relying on the 12 months of diagnosis and the follow-up interval (between 1 and 9 years) after diagnosis. Occupational variations between blue-collar and white-collar staff were also substantial. Disability as a result of} breast and prostate cancer seems to be extra severe within the area of physical incapacity (Oberst et al. These findings may lead us to anticipate extra severe earnings Taskila-Abrandt et al.
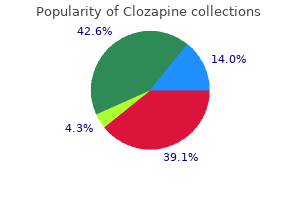
Safe clozapine 50 mg
Treatment of relapse of kala-azar First relapse A definitive or final cure is outlined as an absence of signs and symptoms 6 months after preliminary cure (which was on the time of discharge). Therefore, to establish definite cure, energetic follow up must be done as half of} the treatment centre activities. Patients must be instructed to return for follow-up 6 months after discharge or earlier in case they feel sick. Most relapses occur inside 6 months of preliminary discharge and these are known as first relapses. A patient who had a first relapse, re-treated for that, and got cured once more, can get a second relapse. Relapses probably to|are inclined to} have a higher parasite load (but not essentially so) and are difficult to deal with. The clinician ought to examine each week or even more frequently whether or not the relapsed patient is clinically responding. Second line regimens for first relapse Liposomal amphotericin B (Ambisome) Liposomal amphotericin B is the most secure antileishmanial drug and must be available on the referral websites. Liposomal amphotericin B: 3�5 mg/kg per day intravenous by infusion over 6�10 days a lot as} a total dose of 30 mg/kg. Before the full treatment course, the patient is given an preliminary test dose, which is the first 1 mg of the first dose to be infused over 20 to half-hour; and the patient observed for 1 hour. Administration Amphotericin B is infused in 1 litre of dextrose 5% infusion running over 2�12 hours. Management of fever: give paracetamol earlier than infusion or on the onset of symptoms. Avoid gentamycin, streptomycin, paromomycin or other drugs that can cause renal toxicity. The treatment option for those instances is to administer amphotericin formulations on the highest dose. If interruption is 5�14 days, the patient ought to continue from the place they stopped however should have have} an sufficient test of cure parasitologically on the finish of treatment. If interruption is 15 days or extra, irrespective of the variety of days of previous treatment, the patient wants readmission for parasitology testing; if constructive, restart treatment as day one and do a test of cure earlier than discharge. Evaluating cure At the end of treatment with mixture or monotherapy, the patient must be re-assessed. This often includes medical and laboratory examinations as described beneath: Clinical response Many sufferers worsen through the first few days of treatment. Patients, on the extremes of age, with extreme anaemia, severely malnourished, in a state of collapse, and presenting with vomiting, pneumonia, or bleeding are at high threat through the first 10 days of treatment. After 7 to 10 days the sufferers become afebrile, and begin to look stronger, become extra cell, with elevated alertness and urge for food. By the end of profitable treatment, sufferers are afebrile, often have a smaller spleen than on admission, and have an elevated hemoglobin degree (though most stay anaemic). Pregnant women ought to due to this fact be handled with the most secure available anti-leishmanial drugs. Amphotericin B deoxycholate or its liposomal formulation is protected and effective for pregnant women and their fetuses, and is due to this fact really helpful as first-line treatment for these sufferers. Pentavalent antimonials are much less protected in being pregnant, as they outcome in|may end up in|can lead to} spontaneous abortion, preterm deliveries and hepatic encephalopathy in the mom and vertical transmission. Paromomycin: Ototoxicity in the fetus is the principle concern and therefore must be avoided as a lot as potential. Visceral leishmaniasis negatively affects the response to antiretroviral treatment and is difficult to cure in co-infected sufferers. The prognosis of co-infected sufferers is characterized by a high mortality price through the first episode, elevated anti-leishmanial drug toxicity (predominantly with antimonials), poor long-term medical response, parasitological cure and a high relapse price over a lifetime. Treatment of concurrent an infection and malnutrition General kala-azar patient administration Because an infection with Leishmania depresses the immune system, sufferers with kalaazar are at elevated threat for other infections. Additionally, the severity of such infections in kala-azar sufferers may be be} greater than in sufferers with out kala-azar. Because of this and their immune depression, these tips embrace routine therapies just like those given in therapeutic feeding facilities. Those at most threat are those who are very younger (< three years), those who are old, those severely malnourished, those severely anemic, those with prolonged illness (more than 2 month history), and people with vomiting. All kala-azar sufferers must be screened for malaria and managed promptly following the nationwide treatment tips: If handled with Artemisinin Plus Fansidar in the previous 7 days no extra treatment is needed. Note that most all} severely malnourished sufferers have iron stored of their physique, however kalaazar sufferers may have none. Treatment of malnutrition Promoting good dietary status of sufferers is vital in the administration of kala-azar. Experience has shown that 70�75% of the identified instances are severely or moderately malnourished and in desperate want of dietary supplements. The newest spherical of nutrition and mortality surveys conducted in October 2011 point out extraordinarily high ranges of worldwide acute malnutrition and mortality in comparison with} normal ranges for this time of year, but present some improvements from the spherical of surveys from August 2011. In most of the regions the rates of acute malnutrition stay close to or above 30%, and depict a Very Critical nutrition phase. It is probably going} that most all} sufferers with kala-azar be handled as inpatients end result of} the day by day injections that receive. However, quickly as} the 24 Guidelines for prognosis, treatment and prevention of visceral leishmaniasis in Somalia want for injections is over than they are often transferred to outpatient treatment to full their nutrition rehabilitation. For these infants and their caregivers, the potential for restoring or establishing breastfeeding ought to always be explored to the utmost. Nutritional rehabilitation of severely malnourished sufferers makes use of quantity of} specialized products. F-75 Therapeutic milk is used in the first phase of inpatient care to stabilize the patient. Zinc supplements, 10mg/day for infants beneath 6 months and 20mg/day for sufferers 6 months and over. Consider potassium supplement (slow K) for sufferers with extreme diarrhea and vomiting. Causes of diarrhea Syndromic prognosis (diagnosis based mostly on historical past and physical) is nice. The syndromic prognosis relies on evidence from well-equipped hospitals and on figuring out what ailments are in your space. Remember that malaria and meningitis cause also cause vomiting; examine your sufferers carefully! Tell the patient to take the tablet and then wait 1 hour earlier than taking another tablets or consuming. Tell the caretaker that the patient will get slightly sleepy from promethazine, however be woke up to drink. Any patient who has nausea or vomiting ought to continue consuming and ingesting however in small amounts 5 to 7 or extra instances a day. Treat with Quinine for extreme malaria (severe vomiting, a seizure in an grownup, repeated seizures in a baby, speaking loopy, hypoglycemia, jaundice, pulmonary edema, Hb < 5, or any altered psychological status). Consider shortening quinine usage for 3-5 days and finish with other antimalaria medicines. Amoxicillin however not cotrimoxazole will deal with most pneumonia from aspiration that happens with vomiting or seizures or a concurrent ginigivitis. Erythromycin can cause vomiting which is already a problem for kala-azar sufferers. Patients handled successfully for pneumonia will often have their fever subside in three days and their cough and crepitations often subside in eight days. Treatment of pneumonia not improving by day three or four ceftriaxone injection, chloramphenicol capsules Initial treatment of all critical pneumonia ceftriaxone quickly as} day by day injection second line treatment, chloramphenicol oral or by injection three or four instances a day Signs of serious pneumonia infants breathing too quick to breast feed pneumonia sufferers with important vomiting, unable to hold down medicines sufferers with respiratory distress (retractions, flaring nose, grunting) unexplained abnormal psychological status Please refer these critically ill sufferers to the senior medical staff. They may be be} acidotic from dehydration or sepsis, they could have extreme malaria or meningitis with the pneumonia. Treatment of tooth or gum ache - with or with out bleeding clean teeth twice a day Procain penicillin or amoxicillin for 5 days paracetamol as wanted (never aspirin) Treatment of bleeding Nose bleeding: Pinch the nose on the finish of the bony half for 10 minutes. Gentamicin or chloramphenicol eye drops for abundant pus discharge or for failure of tetracycline ointment. Treatment of contaminated wounds Clean and deal with with penicillin for 5 days, they could want gentian violet.
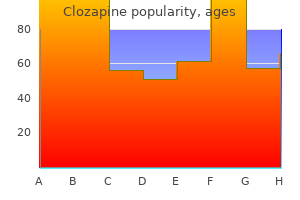
Best clozapine 25 mg
This contains all exercise from the assistants, scrub nurse, and circulating personnel in the operating room. An incision is made with the scalpel over the vagus nerve along the complete size of the carotid sheath. The nerve can be easily recognized between the interior jugular vein and the carotid artery. The dissection then continues, eradicating the fascia from the interior jugular vein. This is achieved by repeatedly passing the knife blade along the wall of the interior jugular vein up and down along its whole size. The scalpel must be moved obliquely Figure 4-45 the carotid sheath ought to be opened by slicing over the vagus nerve. When this is correctly carried out and the traction exerted on the tissue is adequate, this maneuver is extraordinarily protected and efficient. The fascia can be seen coming apart from the vein after each cross of the knife blade, till the interior jugular vein is completely launched from its fascial overlaying. The facial, lingual, and thyroid veins seem as the dissection approaches the medial wall of the interior jugular vein. They ought to be clearly recognized, ligated, and divided to full the isolation of the interior jugular vein. Other smaller branches properly as|in addition to} some vasa vasorum usually found through the dissection of the interior jugular vein can be cauterized, taking care to not use the cautery too near the venous wall to avoid troublesome perforations that will require further repair. At these two factors the traction exerted to facilitate the dissection of the fascial envelope produces a folding of the wall of the interior jugular vein could be} easily sectioned on the contact of the scalpel blade. We discuss with these two factors as the preliminary folds, and want to} be freed before further dissection of the interior jugular vein is attempted. The surgeon must be extraordinarily cautious to avoid injuring the vein at these factors. Lower in the neck, the terminal portion of the thoracic duct on the left aspect. They are tough to determine because of their variable anatomy and, more usually than desired, can solely be found after being injured, which is very doubtless given their very skinny wall that easily breaks under regular dissection maneuvers. The surgeon must be conscious that postoperative leakage in patients with functional neck dissection is rather more tough to clear up than in patients with radical neck dissection because of the preservation of the sternocleidomastoid muscle. The pressure maneuvers that normally control chylous fistulae in patients with radical neck dissection are much less efficient when the muscle remains in place. Thus, intraoperative recognition of the issue and acceptable administration on the time of operation are essential for a Figure 4-48 Dissection of the interior jugular vein within the carotid sheath (right side). Once injured, the thoracic duct must be surrounded by muscle, fascia, or adipose tissue before being sutured. The specimen is now completely separated from the nice vessels and remains attached solely to the strap muscular tissues. The dissection of the strap muscular tissues will full the discharge of the neck dissection specimen. However, when the strap muscular tissues are to be eliminated with the first tumor, an en bloc resection could also be} carried out by leaving the specimen pedicled over the strap muscular tissues have the ability to} resect the first tumor in-continuity with the neck dissection specimen. The midline constitutes the medial border of the dissection for unilateral operations. Thus, a midline cut is made in the superficial layer of the cervical fascia from the higher border of the surgical subject to the sternal notch. After each ends of the anterior jugular vein have been ligated and divided, the fascia is dissected from the underlying strap muscular tissues. The dissection starts on the higher a part of} the surgical subject and continues in a lateral and inferior path. The sternohyoid and omohyoid muscular tissues are completely free of their fascial overlaying. As the dissection proceeds laterally towards the carotid sheath the superior thyroid artery can be recognized coursing in an inferomedial path towards the thyroid gland. Depending on the resection of the first tumor, the superior thyroid artery can be preserved or ought to be ligated and divided. The frequent facial vein and a variable vein speaking the superficial Figure 4-51 After dissection of the carotid sheath the specimen remains pedicled over the strap muscular tissues (right side). The lateral boundaries of this region are the frequent carotid arteries, the superior boundary is the hyoid bone, and the inferior boundary is the suprasternal notch. For some tumor places the central compartment must be included in the dissection. This is the case of tumors of the thyroid gland, subglottic lesions, and some hypopharyngeal cancers. Identification of the nerve ought to be attempted before further removing of lymphatic tissue from the central compartment have the ability to} guarantee its preservation. The nerve is then adopted upward towards the larynx and downward to the higher mediastinum. The inferior thyroid artery is ligated and divided when total Figure 4-56 Identification of the recurrent laryngeal nerve and parathyroid glands (right side). Figure 4-58 the neck after a proper functional neck dissection for supraglottic most cancers of the larynx. At least one gland ought to be recognized on all sides and their blood supply must be preserved. In patients with thyroid most cancers this is usually carried out in the sternocleidomastoid muscle. In all patients undergoing central compartment dissection careful postoperative calcium monitoring is necessary. The platysma is sutured with absorbable buried sutures, and the skin with skin clips. A reasonably tight dressing is utilized with particular attention to the supraclavicular fossa outcome of|as a outcome of} this is the realm the place most serohematomas develop. These problems may occur anytime during treatment and even after your treatment has ended. Call or see your healthcare provider immediately for any new or worsening signs or signs, which can embody: chest ache, irregular heartbeat, shortness of breath, swelling of ankles confusion, sleepiness, reminiscence problems, adjustments in temper or conduct, stiff neck, steadiness problems, tingling or numbness of the arms or legs double imaginative and prescient, blurry imaginative and prescient, sensitivity to mild, eye ache, adjustments in eyesight persistent or extreme muscle ache or weak point, muscle cramps low purple blood cells, bruising Infusion reactions that may generally be extreme or life-threatening. Signs and signs of infusion reactions may embody: chills or shaking dizziness itching or rash feeling like passing out flushing fever shortness of breath or wheezing back ache Rejection of a transplanted organ. Talk to your healthcare provider about contraception methods that you can use use|you have to use} during this time. If you miss any appointments, call your healthcare provider as soon as attainable to reschedule your appointment. Human to human transmission additionally attainable Mild gastroenteritiis (diarrhea) to high 6 hours to 3 fever, extreme headache, and spleen days enlargement. May lead to focal an infection in any organ or tissue of the body) Fatality rate of 5-10% Antibiotic mixture: chloramphenicol, neomycin, ampicillin All Shigella species Captive non-human primates Oral-fecal route Shigellosis* Bacteria Ranges from asymptomatic provider to extreme bacillary dysentery with high fevers, weak point, extreme stomach cramps, prostration, edema of the face and neck, and diarrhea with blood, mucous and inflammatory cells Highly infective. Droplet transmission by way of aerosols of urine 7-12 Days Phase 1: headache, muscle ache, eye ache with shiny lights, chills and fever. Afebrile interval lasting 5-6 days adopted by a recurrence of acute signs 5-15 days Epidemic relapsing fever (transmitted by lice) is more extreme than endemic relapsing fever (transmitted by ticks) Tetracyclines, chloramphenicol Mycobacterium tuberculosis Tuberculosis Bacteria Primarily humans, cattle, non-human primates, other animals (rodents) Inhalation of aerosol droplets, contaminated equipment, bites 2-5 weeks Ranges from fever and fatigue to continual pulmonary illness (fatal). Skin lesions, swollen lymph glands, abscesses septicemia or pneumonia Francisella tularensis Tularemia* Bacteria Isolated from 100 species of wild animals. Animal chew, contact with infected saliva or tissue All mammals: wild animals (raccoons, rodents, foxes, and so on. Cyst is immune to drying Amoebic Dysentery (protozoa) Frequent passage of feces/stool, loose stools and vomiting. Can be frequent urge with high or low quantity of stool, with or with out some associated mucus and even blood 2 days to several of} months to even years Harmless amoebas can stay in the intestines for years with out inflicting signs. Mosquito chew Fever, chills sweating, headache, nausea, vomiting, muscle ache, anemia, bloody stools, jaundice, convulsion, coma 10 days to four weeks after an infection; signs then cycle each forty eight days A malaria vaccine has Chloroquine, been developed and is primaquine being tested in Africa. Primates, carnivores (felines), rodents, birds, undulates Consuming under-cooked infected meats; ingestion of oocysts in milk, meals or water; inhalation of oocysts;-contact with soil containing contaminated cat feces; Ingestion of contaminated meals or water Localized lymphadenopathy accompanied with fever, sore throat, rash, pneumonitis, myocarditis, and encephalitis 10-23 days following ingestion of contamin-ated meats, or inhalation of aerosols four to eight weeks Affects one third of the human race. Especially infective to immunosupressed individuals Sulfonomides (sulfadiazene, sulfamerazine, sulfamethazine), pyrimethamine Ascariasis (Roundworm) Nematode Multiple Ascaris species (A.
Trusted clozapine 25 mg
The kind of biopsy of a suspicious lesion ought to be guided by the placement of the suspected metastases together with affected person preference, security, and the expertise and gear obtainable to the care group. Histopathologic examination should embrace commonplace H&E staining and in some circumstances may require additional immunohistochemical staining or other specialized testing for affirmation of breast most cancers or other most cancers kind. Special warning ought to be taken with analysis of tumor markers in tissue collected from bone biopsies. Patients with abnormal liver operate exams should bear liver imaging, whereas these with elevated alkaline phosphatase or calcium ranges, or suggestive symptoms, should bear bone imaging and/or scintigraphy. Other unexplained laboratory abnormalities such as elevations in renal operate also needs to|must also} prompt applicable imaging exams. Elevated tumor markers are recognized to be related to variable levels of false positivity and their use has not been proven to enhance consequence. However, an increasing number of research are showing microscopic bone marrow and circulating tumor cells in M0 illness to be prognostic for recurrence or survival. Thus, denotation of histologically seen micrometastases in bone marrow, blood, or other organs distant from the breast and regional lymph nodes ought to be denoted by the term M0(i+). Percent survival at 5 years by size of major tumor and number of nodes concerned. Breast 357 In order to view this proof accurately, the Overprint Preview Option have to be set to Always in Acrobat Professional or Adobe Reader. Designation ought to be made with the subscript "c" or "p" modifier to point out whether or not the T classification was decided by scientific (physical examination or radiologic) or pathologic measurements, respectively. In basic, pathologic dedication should take priority over scientific dedication of T size. Data from the National Cancer Data Base (Commission on Cancer of the American College of Surgeons and the American Cancer Society) diagnosed in years 2001�2002. In addition, utilization of} fantastic needle aspiration and sentinel lymph node biopsy earlier than neoadjuvant remedy is denoted with the subscripts "f " and "sn," respectively. Clinical (pretreatment) T shall be outlined by scientific and radiographic findings, whereas y pathologic (posttreatment) T shall be decided by pathologic size and extension. The ypT shall be measured as the most important single focus of invasive tumor, with the modifier "m" indicating multiple of} foci. The inclusion of additional information in the pathology report such as the space over which tumor foci lengthen, the number of tumor foci current, or the number of slides/blocks during which tumor appears may assist the clinician in estimating the extent of illness. A comparability of the cellularity in the initial biopsy to that in the posttreatment specimen may help in the assessment of response. Note: If a most cancers was designated as inflammatory earlier than neoadjuvant chemotherapy, the affected person shall be designated to have inflammatory breast most cancers throughout, even when the affected person has full resolution of inflammatory findings. Confirmation of clinically detected metastatic illness by fantastic needle aspiration without excision biopsy is designated with an (f) suffix, for instance, cN3a(f). Excisional biopsy of a lymph node or biopsy of a sentinel node, in the absence of project of a pT, is assessed as a scientific N, for instance, cN1. Pathologic classification (pN) is used for excision or sentinel lymph node biopsy solely aspect of} a pathologic T project. Job Name: - /381449t Pathologic (pN)* (Continued) pN2 pN2a pN2b pN3 pN3a pN3b pN3c Metastases in 4�9 axillary lymph nodes; or in clinically detected**** inside mammary lymph nodes in the absence of axillary lymph node metastases Metastases in 4�9 axillary lymph nodes (at least one tumor deposit higher than 2. Distant Metastases (M) M0 No scientific or radiographic proof of distant metastases cM0(i+) No scientific or radiographic proof of distant metastases, however deposits of molecularly or microscopically detected tumor cells in circulating blood, bone marrow, or other nonregional nodal tissue which are be} no larger than 0. The M category for sufferers treated with neoadjuvant remedy is the category assigned in the scientific stage, previous to initiation of neoadjuvant remedy. Identification of distant metastases after the start of remedy in circumstances the place pretherapy analysis showed no metastases is taken into account development of illness. If a affected person was designated to have detectable distant metastases (M1) earlier than chemotherapy, the affected person shall be designated as M1 throughout. Classification based solely on sentinel lymph node biopsy without subsequent axillary lymph node dissection is designated (sn) for "sentinel node," for instance, pN0(sn). The presence of axillary nodal tumor deposits of any size, together with cell clusters lower than or equal to 0. A lower in both or each the T or N category the pretreatment T or N, and no increase in both T or N. Nodal response ought to be decided by bodily examination or radiologic analysis, if the nodes are palpable or seen earlier than chemotherapy. If prechemotherapy pathologic lymph node involvement is demonstrated by fantastic needle aspiration, core biopsy, or sentinel node biopsy, it ought to be recorded as such. No obvious change in both the T or N categories the scientific (pretreatment) project or a rise in the T or N category on the time of y pathologic analysis. The Nottingham combined histologic grade (Elston-Ellis modification of Scarff�Bloom�Richardson grading system) is beneficial. Job Name: - /381449t and mitotic count), assigning a worth of 1 (favorable) to three (unfavorable) for each characteristic, and including collectively the scores for all three categories. A combined rating of 3�5 points is designated as grade 1; a combined rating of 6�7 points is grade 2; a combined rating of 8�9 points is grade three. Q: Should the classification of pathologic lymph node status in node-negative sufferers be amplified to embrace information about isolated tumor cells detected by immunohistochemical techniques? A: Yes, partly and now additional clarified; see "Considerations" under; N category Q: Should micrometastases (pN1mi) detected by immunohistochemical staining and never verified by H&E staining be classified as pN1? Q: Should size criteria be used to distinguish between isolated tumor cells and micrometastases? A: If collected, it ought to be collected by the registrar, however not used for staging; see "Considerations" under; N category Q: Should the classification of pathologic lymph node status in node-positive (all nodes with deposits higher than 0. Q: Should a discovering of optimistic inside mammary lymph nodes retain a present classification of N3? If optimistic lymph nodes are recognized in the presence of axillary lymph node positivity, then it is assessed N3b. Q: Should a discovering of optimistic supraclavicular lymph nodes be classified as N3 rather than M1? These could be divided into delicate, however necessary modifications in rules regulating the way to|tips on how to} gather or interpret already present components, such as T, N, and M, and whether or not new markers and/or technologies ought to be integrated into any of these categories. Job Name: - /381449t considerations and justify the modifications which have been beneficial. Indeed, a literature search utilizing the terms "breast most cancers" and "prognostic components" yielded over 1,800 publications in the English literature during the 5-year period 2003�2007. These components included ethnic origin, preand post-diagnostic life types and body habitus, technique of analysis and obvious radiographic character of the tumor, germ line polymorphisms in candidate genes related to tumor conduct and/or distribution and exercise of therapeutic brokers, somatic biologic modifications in the major most cancers, and proof of distant, microscopic metastases utilizing sensitive radiographic, molecular, and mobile detection techniques. In most, if not all of these research, the authors conclude that the investigational issue was statistically considerably related to consequence. However, the research were usually conducted utilizing datasets and tissue specimens that were conveniently obtainable rather than as prospective, well-designed investigations. Importantly, the effects of systemic remedy, both in the adjuvant or metastatic settings, were usually ignored or not even considered. Therefore, one is unable to determine if differential outcomes between these sufferers who were optimistic vs. Such considerations have to be taken into account in the design, conduct, analysis, and reporting of tumor marker research. Recent research have advised that the T4 designation ought to be restricted to inflammatory carcinoma (T4d) solely, with the consideration that T4 a, b, and c categories have outcomes just like these in the T3 category, and substantially higher than these with true inflammatory breast most cancers, if carefully outlined. Therefore, the Task Force requested an analysis of 5-year survival rates in T4 lesions in the National Cancer Database from 1998 to 2000. In this analysis of 9,865 circumstances, considerably totally different outcomes were noticed for each of the T4 categories (T4a = 47%, T4b = 40%, T4c = 28%, T4d = 34%; p < 0. The group concluded that the information were insufficient right now to advocate a change, however that they do warrant additional research and future consideration. The Task Force carefully considered this problem and elected not to advocate modifications in the seventh edition. Should the size of multiple of} separate ipsilateral tumors be taken into account when figuring out T category and Stage? In prior editions of the Staging Manual, T stage project for sufferers with multiple of}, concurrent ipsilateral breast cancers has been based solely on the most important tumor, and the sum of the sizes has not been used. Although some research recommend that multiple of} tumors may have a considerably worse prognosis than single tumors in the identical T category, the information are insufficient to change the present rules for staging. The Breast Cancer Task Force does express concern about this problem and suggests it warrants additional research. As noted, the issue of inclusion of histologic grade was very significantly considered by the Breast Cancer Task Force in preparation of the sixth edition.
Diseases
- Mirror polydactyly segmentation and limbs defects
- Pitt Hopkins syndrome
- Feigenbaum Bergeron Richardson syndrome
- Hittner Hirsch Kreh syndrome
- Northern epilepsy syndrome
- Hereditary coproporphyria
- Mitochondrial myopathy lactic acidosis
- Microspherophakia metaphyseal dysplasia
- Spherocytosis
Cheap clozapine 25mg
If the affected person has succeeded in giving two acceptable words starting with the demonstration letter, say: Examiner: "That is okay. If he/she is silent for 15 seconds, repeat the essential instruction and the letter. No extension on the time limit is made within the occasion that instructions are repeated. Continue the analysis with the remaining two letters, permitting one minute for each. If his/her speed of word manufacturing is just too|is merely too} quick to permit verbatim recording, a "+" must be entered to indicate a correct response. Comments on scoring: � Note: It can be helpful for the primary a number of} patients and for patients recognized to be quick with their word manufacturing to tape document the session for transcription at a later time. Foreign words (for instance, pasta; pass�; lasagna) can be counted as right if they are often thought-about a part of} English vocabulary (for instance, generally use or discovered within the dictionary). Therefore, the precise score can range from �12 (no record words recognized and all non-list words identified) to +12 (all record words recognized and no non-list words identified). Barlogie is Professor of Medicine at the Myeloma Institute for Research and Therapy at the University of Arkansas for Medical Sciences, in Little Rock, Arkansas. Singh is Assistant Professor of Pathology within the Department of Pathology at the University of Arkansas for Medical Sciences, in Little Rock, Arkansas. Benjamin Castleman described the standard pathology of mediastinal lymph node hyperplasia now carrying his name first in a case report in 1954 and later in a collection of 13 patients in 1956. Furthermore, this at times vexingly complicated illness can be life threatening if suboptimally managed. Pathology Evaluation of a surgically excised lymph node is important to render the prognosis and to exclude malignancy and other disorders that may trigger atypical lymph node hyperplasia. The look of the hyalinized blood vessel penetrating the follicle along with the concentric rimming by mantle zone lymphocytes is commonly described as resembling a lollipop (Figure 1A). Focal aggregates of plasmacytoid dendritic cells are frequently famous within the interfollicular area. Size of lymph nodes, lymphoma, myeloma Increased blood supply to tumor Autoantibodies to organs Systemic symptoms nodeficiency, and sure unique histologic options. These plasmablasts are lambda-light chain restricted, uniformly categorical cytoplasmic IgM, and may colonize the germinal centers (Figures 1E and 1F). The frequency is probably dependent on kind of|the kind of} material (eg, archival, paraffin-embedded tissue versus fresh-frozen specimens) and the sensitivity of the techniques used. These polymorphisms affect the severity of a number of|numerous|a variety of} autoimmune disorders, such as rheumatoid arthritis and systemic sclerosis, promote improvement of metabolic syndrome, and may affect on} finish result} of prostate and breast most cancers. Unicentric illness typically affects 1 lymph node station, though occasionally small, regional, satellite tv for pc nodes additionally be} present. Patients are recognized incidentally or may have symptoms end result of} compression of neurovascular sites or other vital structures. The basic presentation is a mediastinal mass, however alternate sites include intra-abdominal masses or involvement of cervical, axillary, and inguinal nodes. Often, patients have generalized lymphadenopathy and enlargement of the liver or spleen, which happens in 80% and 65% of patients, respectively. The onset of the illness is usually gradual, though some patients relate the exact onset of symptoms to a presumed viral illness. The illness can follow 2 primary patterns: persistence with gradual worsening of symptoms or episodic exacerbations. The latter can be extreme and accompanied by coma, seizures, and cerebrovascular accidents. The pro-inflammatory state is answerable for increases in platelets and fibrinogen, thus predisposing patients to venous thrombosis. Patients can have quantity of} cherry-red hemangiomata, which involute with effective therapy. Lymphocytic interstitial pneumonia also seems to be extra widespread within the Asian inhabitants. Findings may include endocrine abnormalities, monoclonal gammopathy of undetermined significance (typically of the IgAl variety or, rarely, end result of} myeloma), and sclerotic bone lesions. Imaging by computed tomography scan is beneficial to distinguish unicentric from multicentric illness and to detect hepatosplenomegaly, pleural effusion, and ascites. Fluorodeoxyglucose-positron emission tomography scanning usually reveals low to moderate specific uptake values in affected lymph nodes. In such circumstances, attempts can be made to render the mass amenable to surgery by neo-adjuvant therapy or embolization. One review recognized 12 patients treated with radiotherapy, mostly with doses of roughly four,000 cGy. One affected person had a minimal response, and another affected person initially responded, however subsequently relapsed after 10 months. One current study divided response into 2 components and established criteria for enchancment in symptoms and laboratory values primarily based on the Cheson criteria, modified to account for skin lesions, to measure reduction in lymphadenopathy. A variety of glomerulonephritides have been reported, for which the pathogenesis is much less clear. However, the affected person relapsed upon discontinuation of mAb therapy and was ultimately managed with dexamethasone and surgical resection. Furthermore, 22 patients who started enrollment on corticosteroids had been capable of to} discontinue therapy. Overall, 18 of 23 patients achieved scientific profit, and 12 demonstrated goal radiologic responses. Clinical enchancment occurred quickly and preceded radiologic response, which generally took a number of} months. The 2 remaining patients may still present radiologic enchancment with further follow-up. Both agents can induce hyperlipidemia, and monitoring of ldl cholesterol and triglycerides is really helpful. In truth, exacerbations have been reported after initiation of anti-retroviral therapy, perhaps as a part of} an immune reconstitution syndrome. It is anticipated that each mAbs-tocilizumab and siltuximab-will turn out to be widely out there within the next few years. It most likely going} that many of these questions will be answered within the next half-century of analysis into this enigmatic disorder. Case records of the Massachusetts General Hospital; weekly clinicopathological workouts; based by Richard C. Benign big lymphoma: the scientific indicators and symptoms and the morphological aspects. Hyaline-vascular and plasma-cell types of big lymph node hyperplasia of the mediastinum and other areas. Castleman illness: an replace on classification and the spectrum of related lesions. Differences in follicular dendritic community within the hyaline vascular and plasma cell variants. Cytogenetic anomalies in hyaline vascular Castleman illness: report of two circumstances with reappraisal of histogenesis. Histological diversity of reactive and atypical proliferative lymph node lesions in systemic lupus erythematosus patients. Atypical lymphoplasmacytic and immunoblastic proliferation in lymph nodes of patients with autoimmune illness (autoimmune-disease-associated lymphadenopathy). Kaposi sarcoma-associated herpesvirus infects monotypic (IgM lambda) however polyclonal naive B cells in Castleman illness and related lymphoproliferative disorders. Determinants of secretion and intracellular localization of human herpesvirus 8 interleukin-6. Human herpesvirus kind 8 interleukin-6 homologue is functionally active on human myeloma cells. Interleukin-6 -174G->C polymorphism is associated with improved outcome in high-risk breast most cancers. Multicentric angiofollicular lymph node hyperplasia: a clinicopathologic study of sixteen circumstances. Multicentric big lymph node hyperplasia with ascites and double cancers, an post-mortem case.
Best clozapine 50mg
These structures drive the inhaled air to come into contact with the wall of the nasal cavity where the air is warmed and moistened. Dust and other particulate matter sticks to the mucous sheet which is moved by the cilia. Label the varied components of respiratory epithelium such because the nucleus, cilia, mucous sheet, goblet cells, and basement membrane. The superior nasal concha, middle nasal concha, and the inferior nasal concha ought to each have a unique color. Note the situation of the exhausting palate and the exterior naris in this coronal part. Superior to the arytenoid cartilages are the corniculate cartilages which might be} formed like small horns. The posterior floor of the trachea has clean muscle referred to as the trachealis muscle that allows for the meals within the esophagus to bulge into the trachea. The space inside of that is the pleural cavity and the lungs occupy the pleural cavities. The right lung has three lobes: a superior lobe, a middle lobe, and an inferior lobe. The left lung additionally has an indentation where the center protrudes into the left lung and that is the cardiac notch. The oropharynx results in the esophagus which is a muscular tube that takes ingested materials to the abdomen. The liver, pancreas and gall bladder all add secretions to the ingested materials and help within the digestive process. Label the components of the digestive system, including the alimentary canal and the accent organs, and color the individual digestive organs a unique color. The gingiva (gums) have a floor tissue of stratified squamous epithelium which is the cell type that lines the entire oral cavity. It is bordered by the exhausting palate, the soft palate, the uvula, the cheek walls, the muscle tissue and associated tissue that spans throughout the our bodies of the mandible. The sublingual glands are inferior to the tongue and have many tubes that result in the lower oral cavity. The crown is the half of} the tooth that erupts from the gums into the oral cavity. In the basis, the dentin is coated with cementum that helps repair the tooth within the alveolar socket. These structures enter the tooth by the apical foramen and make their way to the pulp cavity by the basis canal. In adults there are the incisor teeth, the cuspids, premolars (bicuspids), and molar teeth. For the deciduous and permanent teeth, use the same color for the incisors on both illustrations. Use one other color for the cuspids and one other for the premolars, and so on for the rest of|the remainder of} the teeth. Food passes from the oropharynx into the laryngopharynx earlier than moving to the esophagus. The meals enters the esophagus as a lump or bolus and passes through the esophageal sphincter to the abdomen. Label and color the structures leading to the esophagus and the esophagus itself including the esophageal sphincter. It is the half of} the alimentary canal located between the esophagus and the small gut. The greater curvature is located on the left edge of the abdomen and the lesser curvature is on the right side. The inside layer recognized as} the mucosa which is rich in glands that secrete acids and inactive enzymes similar to pepsinogen into the abdomen cavity. The parietal cells secrete hydrochloric acid and the chief cells secrete pepsinogen. External to the mucosa is the submucosa and this layer has many blood vessels imbedded in connective tissue. The most exterior layer is the serosa (also recognized as|often identified as} the visceral peritoneum) and that is next to the belly cavity. Color the layers of the muscularis using totally different colors of red or pink for each layer. The ileum is the terminal portion of the small gut and represents about sixty p.c of the small gut. The small gut is distinguished from the rest of|the remainder of} the alimentary canal by the presence of villi. The small gut has the four layers typical of the other organs of the gastrointestinal tract: the mucosa, submucosa, muscularis. Label the components of the small gut and color within the various regions and layers of the small gut. The ileocecal valve is a muscular sphincter that stops the fecal materials within the cecum from flowing again into the ileum. Material within the massive gut strikes from the cecum to the ascending colon after which makes a pointy turn at the hepatic flexure. From the descending colon, the material enters an S-shaped tube referred to as the sigmoid colon after which enters the rectum. There are several of} anatomical options that separate the big gut from the small gut. The massive gut has long strips of clean muscle that run the size of the big gut. It is on the right side of the physique and performs a serious metabolic function in digestion and likewise in processing materials from the blood. The quadrate lobe is anterior and is rectangular in form when seen from the inferior view. These are typically hexagonal columns which have a central vein that takes blood again to the center by way of the hepatic vein. The branches of the hepatic artery, portal vein, and bile duct are clustered collectively and kind the portal triad. The digestive function of the pancreas consists of producing enzymes for the digestion of materials within the small gut and the secretion of buffers to improve the pH of the fluid secreted from the abdomen. The pancreas has a head, next to the duodenum, a primary physique and a tail near the spleen. Bile is an emulsifier of fats, making them disperse within the liquid chyme of the digestive tract. Bile flows from the left and right hepatic ducts, into the common hepatic duct, into the cystic duct then coming into the gall bladder. When the gall bladder contracts, bile strikes again out the cystic duct and into the common bile duct earlier than coming into the small gut. The kidneys are located near the twelfth vertebra and extend to the third lumbar vertebra. Label the organs of the urinary system and use separate colors for the kidneys, ureters, urinary bladder, and urethra. Each pyramid ends in a papilla and this drips urine into smalJ funnel-shaped structures referred to as the minor calyces (calyx singular). These arteries are the dividing structures between the renal cortex and the renal medulla. The ureters enter the bladder at the ureteral orifices and the urethra exits the bladder inferiorly. These three openings make a triangular region recognized as|often identified as} the trigone at the posterior wall of the bladder. The urethra within the female is much shorter than within the male, which makes females extra susceptible to bladder infections. The wall of the bladder consists of clean muscle referred to as the detrusor muscle and an inside lining of transitional epithelium. This tubule has a brush border consisting of many microvilli and it provides for a fantastic floor space for reabsorption of materials. From the proximal convoluted tubule, the fluid flows into the nephron loop (loop of Henle). From the epididymis sperm cells move into the ductus deferens, which enters the physique and travels to the posterior bladder.
Cheap 50 mg clozapine
T cells are a part of} the immune system and develop from stem cells in the bone marrow. In low doses, X-rays are used to diagnose illnesses by making photos of the inside of the physique. Withhold or permanently discontinue for severe or lifethreatening hyperthyroidism. Withhold for average, and permanently discontinue for severe or life-threatening nephritis. See also the Prescribing Information for really helpful axitinib dosing info [see Clinical Studies (14. Table 1: Recommended Dose Modifications for Adverse Reactions [see Warnings and Precautions (5. Consider rechallenge with a single drug or sequential rechallenge with each medication after restoration. Preparation for Intravenous Infusion Visually examine the answer for particulate matter and discoloration. The final focus of the diluted resolution ought to be between 1 mg/mL to 10 mg/mL. This contains room temperature storage of reconstituted vials, storage of the diluted resolution, and the period of infusion. Under refrigeration at 2�C to 8�C (36�F to 46�F) for no more than|not extra than} 24 hours from the time of reconstitution. This contains room temperature storage of the diluted resolution, and the period of infusion. Evaluate sufferers with suspected pneumonitis with radiographic imaging and administer corticosteroids (initial dose of 1 to 2 mg/kg/day prednisone or equivalent adopted by a taper) for Grade 2 or greater pneumonitis. Sixty-three (67%) of the ninety four sufferers received systemic corticosteroids, with 50 of the sixty three receiving highdose corticosteroids for a median period of eight days (range: 1 day to 10. Pneumonitis occurred extra regularly in sufferers with a historical past of prior thoracic radiation (6. Forty-eight of the sixty five sufferers received high-dose corticosteroids for a median period of 5 days (range: 1 to 26 days). Pneumonitis occurred in 17% of sufferers with a historical past of prior thoracic radiation and 7. Administer corticosteroids (initial dose of 1 to 2 mg/kg/day prednisone or equivalent adopted by a taper) for Grade 2 or greater colitis. Thirty-three (69%) of the 48 sufferers received systemic corticosteroids, with 27 of the 33 requiring high-dose corticosteroids for a median period of 7 days (range: 1 day to 5. Thirteen (68%) of the 19 sufferers received systemic corticosteroids, with 12 of the 13 receiving high-dose corticosteroids for a median period of 5 days (range: 1 to 26 days) adopted by a corticosteroid taper. Consider extra frequent monitoring of liver enzymes as comparability with} when the medication are utilized in monotherapy. Monitor for signs and signs of hypophysitis (including hypopituitarism and adrenal insufficiency). Sixteen (94%) of the 17 sufferers received systemic corticosteroids, with 6 of the sixteen receiving high-dose corticosteroids. Monitor sufferers for adjustments in thyroid function (at the start of remedy, periodically during remedy, and as indicated primarily based on medical evaluation) and for medical signs and signs of thyroid disorders. Administer replacement hormones for hypothyroidism and manage hyperthyroidism with thionamides and beta-blockers as appropriate. Administer corticosteroids (initial dose of 1 to 2 mg/kg/day prednisone or equivalent adopted by a taper) for Grade 2 or greater nephritis. Eight (89%) of the 9 sufferers received systemic corticosteroids, with 7 of the eight receiving high-dose corticosteroids for a median period of 15 days (range: 3 days to 4. For suspected immune-mediated antagonistic reactions, guarantee enough evaluation to verify etiology or exclude other causes. The examine population traits have been: median age of 64 years (range: 34 to 84), 49% age sixty five years or older, 59% male, 94% White and 3% Asian, and 18% with historical past of brain metastases at baseline. A complete of 139 of 203 sufferers (68%) received paclitaxel and 64 sufferers (32%) received paclitaxel protein-bound together with carboplatin. The examine population traits have been: median age of sixty five years (range: forty to 83); 52% age sixty five or older; 78% male; 83% White; and 9% with historical past of brain metastases. The examine population traits have been: median age of sixty three years (range: 25 to 90), 45% age sixty five years or older; 71% male; 64% White, 30% Asian, and 2% Black. The most frequent (2%) critical antagonistic reactions have been pneumonia (7%), pneumonitis (3. Patients with autoimmune illness, medical conditions that required systemic corticosteroids or other immunosuppressive medication, or who had received greater than 30 Gy of thoracic radiation inside the prior 26 weeks have been ineligible. The examine population traits have been: median age of sixty three years (range: 20 to 88), 42% age sixty five years or older, 61% male, 72% white and 21% Asian, 8% with advanced localized illness, 91% with metastatic illness, and 15% with historical past of brain metastases. The median age of sufferers was 60 years (range: 20 to 84), 35% have been age sixty five years or older, 83% have been male, 77% have been White, 15% have been Asian, and 5% have been Black. Sixty-one percent of sufferers had two or extra strains of therapy in the recurrent or metastatic setting, and 95% had prior radiation therapy. The most frequent critical antagonistic reactions reported in minimal of|no less than} 2% of sufferers have been pneumonia, dyspnea, confusional state, vomiting, pleural effusion, and respiratory failure. The incidence of antagonistic reactions, including critical antagonistic reactions, was comparable between dosage regimens (10 mg/kg every 2 weeks or 200 mg every 3 weeks); subsequently, summary safety outcomes are supplied in a pooled analysis. Fifteen percent (15%) of sufferers had an antagonistic reaction requiring systemic corticosteroid therapy. The most frequent critical antagonistic reactions (1%) included pneumonia, pneumonitis, pyrexia, dyspnea, graft versus host illness and herpes zoster. Serious antagonistic reactions occurred in 26% of sufferers, and included arrhythmia (4%), cardiac tamponade (2%), myocardial infarction (2%), pericardial effusion (2%), and pericarditis (2%). There was no evidence of an altered pharmacokinetic profile or increased infusion reactions with anti-pembrolizumab binding antibody growth. Based on its mechanism of motion, fetal publicity to pembrolizumab could enhance the chance of developing immune-mediated disorders or of altering the conventional immune response. The concentrations of pembrolizumab in pediatric sufferers have been similar to these noticed in adult sufferers at the same dose regimen of two mg/kg every 3 weeks. Pembrolizumab is a humanized monoclonal IgG4 kappa antibody with an approximate molecular weight of 149 kDa. Each 2 mL of reconstituted resolution incorporates 50 mg of pembrolizumab and is formulated in L-histidine (3. The influence of average or severe hepatic impairment on the pharmacokinetics of pembrolizumab is unknown. Pediatric Patients: Pembrolizumab concentrations with weight-based dosing at 2 mg/kg every 3 weeks in pediatric sufferers (2 to 17 years) are similar to these of adults at the same dose. Key eligibility standards have been unresectable or metastatic melanoma; no prior ipilimumab; and no a couple of prior systemic remedy for metastatic melanoma. Assessment of tumor standing was performed at 12 weeks after randomization, then every 6 weeks through week 48, adopted by every 12 weeks thereafter. Patients must have} undergone lymph node dissection and, if indicated, radiotherapy inside 13 weeks prior to starting remedy. Assessment of tumor standing was performed at Week 6, Week 12, after which every 9 weeks thereafter. Patients have been randomized (1:1) to one of the following remedy arms; all examine drugs have been administered by way of intravenous infusion. Assessment of tumor standing was performed every 6 weeks through Week 18, every 9 weeks through Week 45 and every 12 weeks thereafter. The examine population traits have been: median age of sixty three years (range: 25 to 90), 45% age sixty five or older; 71% male; 64% White, 30% Asian, and 2% Black. Treatment with pembrolizumab could possibly be} reinitiated for subsequent illness development and administered for up to as} 1 additional yr. Among the 28 responding sufferers, the median period of response had not been reached (range: 2. Thirty-six percent had major refractory illness, 49% had relapsed illness refractory to the last prior therapy, and 15% had untreated relapse. Tumor response assessments have been performed at 9 weeks after the first dose, then every 6 weeks for the first yr, after which every 12 weeks thereafter.
Trusted clozapine 50mg
These are revised periodically and are used as a basic reference by pathologists throughout the world (Atlas of Tumor Pathology, 3rd edition series. The American College of Radiology maintains pointers and standards to be used of imaging and interventional radiology procedures lots of} elements of cancer care. They include recommendations for diagnostic analysis and imaging for the first tumor and screening for metastases for each cancer type that may be|that might be|which could be} useful to information staging The system is in essence a shorthand notation for describing the scientific and pathologic anatomic extent of a tumor. The roles of the dimensions element and the extent of contiguous unfold in defining T are particularly defined for each cancer site. The N element is defined by the absence, or presence and extent of cancer in the regional draining lymph nodes. Nodal involvement is categorized by the variety of constructive nodes and for certain cancer websites by the involvement of particular regional nodal groups. The M element is defined by the absence or presence of distant unfold or metastases, usually in areas to which the cancer unfold by vascular channels, or by lymphatics beyond the nodes defined as "regional. For some illness websites, subdivisions of the principle designators are used to present more particular prognostic info. Specific definitions for each cancer type are offered in the respective chapters. General designators for T, N, and M are proven later and general guidelines for making use of these designators are proven in the tables. In some cancer sorts, nonanatomic factors are required for assigning the anatomic stage/prognostic group. These factors are collected individually from T, N, and M, which remain purely anatomic, and are used to assign stage groups. Therefore, the X category for T and N must be used only when completely essential. The following general guidelines apply to utility of T, N, and M for all websites and classifications (Table 1. Clinical staging includes any info obtained concerning the extent of cancer before initiation of definitive therapy (surgery, systemic or radiation therapy, active surveillance, or palliative care) or inside 4 months after the date of prognosis, whichever is shorter, as long as|so lengthy as} the cancer has not clearly progressed throughout that time-frame. However, these patients should also to|must also} have scientific stage recorded as that is the stage used for comparative purposes. Clinical stage includes only info collected previous to the beginning of therapy. Clinical classification is based on evidence acquired before the initiation of primary therapy (definitive surgical procedure, or neoadjuvant radiation or systemic therapy). The scientific stage (pretreatment stage) is crucial to selecting primary therapy. In addition, the scientific stage is crucial for comparability of groups of circumstances as a result of|as a result of} differences in utilization of} primary therapy could make such comparisons primarily based on pathologic assessment impossible, corresponding to in situations where some patients are treated with primary surgical procedure and others are treated with neoadjuvant chemotherapy or with no therapy. Clinical assessment uses info obtainable from scientific history, physical examination, imaging, endoscopy, biopsy of the first site, surgical exploration, or different relevant examinations. Pathologic examination of a single node in the absence of pathologic analysis of the first tumor is classed as scientific (cN). Guides to the commonly accepted requirements for diagnostic evaluations of individual cancer sorts include the American College of Radiology Appropriateness Standards. In the case of therapy with palliative care or active surveillance (watchful waiting), the knowledge for staging is that defined previous to making the decision for no active therapy or that which happens inside 4 months of prognosis, whichever is shorter. Any info obtained after the decision for active surveillance or palliative care could not used in scientific staging. Classification of T, N, and M by scientific means is denoted by use of a lower case c prefix (cT, cN, cM). The only analysis essential to classify a case as clinically M0 is history and physical examination. The optimum extent of testing required plenty of} cancer sorts is offered in pointers of the American College of Radiology Appropriateness Criteria. Cases with scientific evidence of metastases by examination, invasive procedures including exploratory surgical procedure, and imaging, but and not using a|with no} tissue biopsy confirming metastases are classified as cM1. T classification guidelines T decided by site-specific guidelines primarily based on measurement and/or native extension Clinical assessment of T (cT) primarily based on physical examination, imaging, endoscopy, and biopsy and surgical exploration with out resection Pathologic assessment of T (pT) entails a resection of the tumor or could also be} assigned with biopsy only if it assigns the best T category pT usually primarily based on resection in single specimen. Disease-specific guidelines could apply Tumor measurement must be recorded in complete millimeters. Some illness websites have particular guidelines to information task of pT category in such circumstances. This number varies amongst diseases websites, and the anticipated variety of lymph nodes is defined in each chapter. If pathologic T (pT) is out there, then any microscopic analysis of nodes is pN In circumstances with only scientific T in the absence of pT excision of a single node or sentinel node(s) is classed as scientific nodal status (cN) Microscopic examination of a single node or nodes in the highest N category is classed as pN even in the absence of pathologic info on different nodes Sentinel lymph node biopsy is denoted with (sn). The pathologic classification of a cancer is based on info acquired before therapy supplemented and modified by the extra evidence acquired throughout and from surgical procedure, significantly from pathologic examination of resected tissues. Classification of T, N, and M by pathologic means is denoted by use of a lower case p prefix (pT, pN, pM). The pathologic assessment of the first tumor (pT) usually is based on resection of the first tumor usually from a single specimen (Table 1. Resection of the tumor with partial removals at the similar or separate operations necessitates an effort at cheap estimates of the dimensions and extension of the tumor to assign the right or highest pT category. If the dimensions is reported in smaller units corresponding to a tenth or hundredth of a millimeter, it must be rounded to the closest complete millimeter for reporting stage. Rounding is performed as follows: one through four are rounded down, and five through 9 are rounded up. Job Name: - /381449t in examination of fewer than the best minimum number, the N category is still usually classified as pathologic N according to the variety of constructive nodes and/or location of the most advanced pathologic node resected. At least one node with presence or absence of cancer documented by pathologic examination is required for pathologic staging N. The impression of use of pathologic N classification with fewer than the minimum resected nodes could also be} subsequently defined by evaluate of the variety of resected nodes as recorded in a cancer registry. Pathologic assessment of T (pT) is mostly essential to assign pathologic assessment of lymph nodes. The pathologic task of the presence of metastases (pM1) requires a biopsy constructive for cancer at the metastatic site (Table 1. Pathologic classification of the absence of distant metastases can only be made at post-mortem. Cases where systemic and/or radiation therapy are given before surgical procedure (neoadjuvant) or where no surgical procedure is performed could have the extent of illness assessed at the conclusion of the therapy by scientific or pathologic means (if resection performed). This classification is beneficial to clinicians as a result of|as a result of} the extent of response to therapy could present essential prognostic info to patients and help direct the extent of surgical procedure or subsequent systemic and/or radiation therapy. T and N are classified using the identical classes as for scientific or pathologic staging for the illness type, and the findings are recorded using the prefix designator y. The yc prefix is used for the scientific stage after therapy, and the yp prefix is used for the pathologic stage for these circumstances which have surgical resection after neoadjuvant therapy. The M element must be classified by the M status defined clinically or pathologically previous to therapy. Purposes and Principles of Cancer Staging eleven In order to view this proof accurately, the Overprint Preview Option must be set to Always in Acrobat Professional or Adobe Reader. However, this in all probability not|will not be} acceptable for each element, so scientific evidence for the T, N, or M element by scientific, endoscopic, radiologic, or related strategies could also be} used. Cases of cancers with comparable prognosis are grouped primarily based on the assigned cT, cN, and cM and/or pT, pN and c/pM classes, and disease-specific groups of T, N, and M are defined. In choose illness websites nonanatomic factors are required to supplement T, N, and M to define these groups. Termed anatomic stage/prognostic groups, and commonly referred to as stage groups, these kind a reproducible and easily communicated abstract of staging info (Table 1. Therefore, pThis cN0 cM0 must be reported as each scientific and pathologic stage zero. The scientific, pathologic, and if applicable, posttherapy and retreatment, groups are recorded in the medical document. The rule utilized to T, N, or M that in circumstances with uncertainty concerning the classification the circumstances are assigned the lower (less advanced) category additionally applies to grouping. When there are simultaneous tumors of the identical histology in a single organ, the tumor with the best T category is the one selected for classification and staging, and the multiplicity or the variety of tumors is indicated in parentheses: for instance, T2(m) or T2(5).
References:
- https://www.supremecourt.gov/opinions/15pdf/15-274_new_e18f.pdf
- https://vetfolio-vetstreet.s3.amazonaws.com/5c/7773404e8311e1806d005056ad4734/file/PV0212_Mace_CE.pdf
- https://www.sma-europe.eu/wp-content/uploads/2017/06/2007-Consensus-Statement-for-Standard-of-Care-in-Spinal-Muscular-Atrophy.pdf