.png)
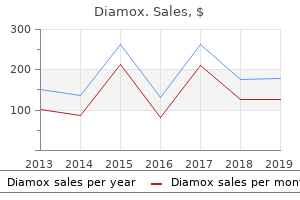
Best diamox 250 mg
Furthermore, each year 20,000 to 30,000 individuals are handled with rabies vaccine, having been bitten by animals that presumably had been rabid, and though the incidence of issues with the newer rabies vaccination is far decrease than before, a number of serious reactions continue to be encountered (see beneath and likewise Chap. Etiology Practically all cases of rabies are the results of transdermal viral inoculation by an animal bite. In undeveloped nations, where rabies is comparatively widespread, probably the most frequent source is the rabid dog. In western Europe and the United States, the most common rabid species are raccoons, skunks, foxes, and bats among wild animals and canine and cats among home ones. Because rabid animals generally bite without provocation, the nature of the attack must be determined. This offers passive immunization for 10 to 20 days, permitting time for active immunization. A thorough trial of the new antiviral brokers in sufferers already symptomatic has not been undertaken. Syndromes of Herpes Zoster Herpes zoster ("shingles," "zona") is a standard viral infection of the nervous system occurring at an overall price of 3 to 5 cases per a thousand individuals per year, with higher charges in the elderly. It is characterised clinically by radicular pain, a vesicular cutaneous eruption, and, much less often, by segmental sensory and delayed motor loss. The pathologic modifications include an acute inflammatory reaction in isolated spinal or cranial sensory ganglia and lesser degrees of reaction in the posterior and anterior roots, the posterior grey matter of the spinal wire, and the adjoining leptomeninges. The neurologic implications of the segmental distribution of the rash had been acknowledged by Richard Bright as way back as 1831. Inflammatory modifications in the corresponding ganglia and associated portions of the spinal nerves had been first described by von Barensprung in 1862 and had been later studied extensively. The concept that varicella and zoster are attributable to the same agent was launched by von Bokay in 1909 and was subsequently established by Weller and his associates (1954, 1958). These and other historic options of herpes zoster have been reviewed by DennyBrown and Adams and by Weller and their colleagues. This hypothesis is consistent with the variations in the medical manifestations of chickenpox and herpes zoster, even though each are attributable to the same virus. Chickenpox is very contagious by respiratory aerosol, has a properly-marked seasonal incidence (winter and spring), and tends to occur in epidemics. The supposition is that in each zoster and varicella infections the virus makes its means from the cutaneous Acute Cerebellitis (Acute Ataxia of Childhood) A particular remark must be made right here regarding the dramatic syndrome of acute ataxia that occurs in the context of an infectious sickness. The syndrome was initially described by Westphal in 1872 following smallpox and typhoid fever in adults, however Batten is credited with drawing attention to the extra widespread ataxic sickness that occurs after sure childhood infections such as measles, pertussis, and scarlet fever. The syndrome, which is actually a "meningocerebellitis," seems comparatively abruptly, over a day or so, and consists of limb and gait ataxia and sometimes dysarthria and nystagmus. The fever of the original infection may have abated, or it might persist via the early stages of the ataxic sickness. Some cases have shown an inflammatory pathology most suggestive of a postinfectious process (see Chap. Multiplication of the virus in epidermal cells causes swelling, vacuolization, and lysis of cell boundaries, resulting in the formation of vesicles and so-known as Lipschutz inclusion bodies. Alternatively, the ganglia might be contaminated through the viremia of chickenpox, however then one would have to clarify why only one or a number of sensory ganglia turn out to be contaminated. Clinical Features As indicated above, the incidence of herpes zoster rises with age. Hope-Simpson has estimated that if a cohort of a thousand individuals lived to eighty five years of age, half would have had one attack of zoster and 10 would have had two attacks. Herpes zoster occurs in as much as 10 percent of sufferers with lymphoma and 25 percent of sufferers with Hodgkin disease- significantly in those who have undergone splenectomy or received radiotherapy. Conversely, about 5 percent of sufferers who current with herpes zoster are found to have a concurrent malignancy (about twice the number that would be anticipated), and the proportion seems to be even higher if more than two adjoining dermatomes are concerned. The vesicular eruption is often preceded for a number of days by itching, tingling, or burning sensations in the concerned dermatome(s), and typically by malaise and fever as properly. The rash consists of clusters of tense clear vesicles on an erythematous base, which turn out to be cloudy after a number of days (due to accumulation of inflammatory cells) and dry, crusted, and scaly after 5 to 10 days. In a small number of sufferers, the vesicles are confluent and hemorrhagic, and therapeutic is delayed for a number of weeks. In most cases pain and dysesthesia last for 1 to 4 weeks; however in the others (7 to 33 percent in numerous sequence) the pain persists for months or, in numerous forms, even for years and presents a troublesome downside in management. Impairment of superficial sensation in the affected dermatome(s) is widespread, and segmental weakness and atrophy are added in about 5 percent of sufferers. In the majority of sufferers the rash and sensorimotor signs are limited to the territory of a single dermatome, however in some, significantly those with cranial or limb involvement, two or extra contiguous dermatomes are concerned. Rarely (and often in association with malignancy) the rash is generalized, like that of chickenpox, or altogether absent. �� Virtually any dermatome could also be concerned in zoster, however some areas are far more frequent than others. The thoracic dermatomes, significantly T5 to T10, are the most common websites, accounting for more than two-thirds of all cases, followed by the craniocervical areas. In the latter cases the disease tends to be extra extreme, with greater pain, extra frequent meningeal signs, and involvement of the mucous membranes. There are two somewhat characteristic cranial herpetic syndromes- ophthalmic herpes and so-known as geniculate herpes. In ophthalmic herpes, which accounts for 10 to 15 percent of all cases of zoster, the pain and rash are in the distribution of the first division of the trigeminal nerve, and the pathologic modifications are centered in the gasserian ganglion. The main hazard on this form of the disease is herpetic involvement of the cornea and conjunctiva, resulting in corneal anesthesia and residual scarring. Palsies of extraocular muscles, ptosis, and mydriasis are frequently related, indicating that the third, fourth, and sixth cranial nerves are affected in addition to the gasserian ganglion. A much less widespread but in addition characteristic cranial nerve syndrome consists of a facial palsy together with a herpetic eruption of the exterior auditory meatus, typically with tinnitus, vertigo, and deafness. Ramsay Hunt (whose name has been hooked up to the syndrome) attributed this syndrome to herpes of the geniculate ganglion. Denny-Brown and Adams found the geniculate ganglion to be solely barely affected in a person who died sixty four days after the onset of a so-known as Ramsay Hunt syndrome (during which era the affected person had recovered from the facial palsy); there was, however, irritation of the facial nerve. Herpes zoster of the palate, pharynx, neck, and retroauricular area (herpes occipitocollaris) is determined by herpetic infection of the upper cervical roots and the ganglia of the vagus and glossopharyngeal nerves. Herpes zoster on this distribution may be related to the Ramsay Hunt syndrome. Encephalitis and cerebral angiitis are uncommon however properly-described issues of cervicocranial zoster, as discussed beneath, and a restricted however destructive myelitis is a equally uncommon however often quite serious complication of thoracic zoster. Devinsky and colleagues reported their findings in 13 sufferers with zoster myelitis (all of them immunocompromised) and reviewed the literature on this subject. The signs of spinal wire involvement appeared 5 to 21 days after the rash after which progressed for the same time period. Asymmetrical paraparesis and sensory loss, sphincteric disturbances, and, much less often, a Brown-Sequard syndrome had been the same old � medical manifestations. The pathologic modifications, which take the form of a necrotizing inflammatory myelopathy and vasculitis, involve not just the dorsal horn but in addition the contiguous white matter, predominantly on the same side and on the identical segment(s) because the affected dorsal roots, ganglia, and posterior horns. Our expertise with the problem contains an elderly man who was not immunosuppressed; he remained with an almost full transverse myelopathy. Many of the writings on zoster encephalitis give the impression of a extreme sickness that occurs temporally remote from the attack of shingles in an immunosuppressed affected person. However, our expertise is extra consistent with that of Jemsek and colleagues and of Peterslund, who described a much less extreme form of encephalitis in sufferers with normal immune techniques. Several of our sufferers, all elderly girls, developed self-limited encephalitis through the latter stages of an attack of shingles. They had been confused and drowsy, with low-grade fever however little meningismus, and a few had seizures. The differential prognosis in these elderly sufferers also features a drowsy-confusional state induced by narcotics given for the management of pain. Angiograms show narrowing or occlusion of the interior carotid artery adjoining to the ganglia; however in some cases, vasculitis is extra diffuse, even involving the contralateral hemisphere. Whether the angiitis outcomes from direct unfold of the viral infection by way of neighboring nerves as postulated by Linnemann and Alvira or represents an allergic reaction during convalescence from zoster has not been settled. Since the exact pathogenetic mechanism is uncertain, remedy with each intravenous acyclovir and corticosteroids could also be justified. In this situation, weeks or months after one or more attacks of zoster, a subacute encephalitis ensues, including fever and focal signs. The vasculitic and other neurologic issues of zoster have been reviewed by Gilden and colleagues.
Syndromes
- A body part that has been completely or partially cut off
- Dyes in drugs and food
- Direct isolation of the SARS virus
- Whitish, pearly bump on gums or roof of mouth (they may look like teeth coming through the gums)
- Overactive thyroid gland
- Poorly organized writing
- Sepsis
- Abnormal connections between the right and left side of the heart
- Abnormal-looking genitals
- Potassium hydroxide
Purchase 250mg diamox
In the case initially described by Dejerine (1892), the disconnection occurred within the pos� terior part (splenium) of the corpus callosum, wherein lie the connections between the visible association areas of the two hemispheres (see. More often the callosal pathways are interrupted within the forceps major or within the paraventricular region (Damasio and Damasio). A uncommon variant of this syndrome takes the type of alexia without agraphia and without hemianopia. A lesion deep within the white matter of the left occipital lobe, at its junction with the parietal lobe, interrupts the projections from the intact (proper) visible cortex to the language areas however spares the geniculocalcarine pathway (Greenblatt). In yet different instances, the lesion is confined to the angular gyrus or the subjacent white matter. In such instances also, a proper homonymous hemianopia shall be absent, however the alexia may be mixed with agraphia and different elements of the Gerstmann syndrome- i. This constellation of signs is sometimes referred to because the syndrome of the angular gyrus. From the time speech becomes audible, language may be syntactically full, displaying neither loss of vocabulary nor agrammatism; or there may be various levels of dysarthria (therefore "cortical dysarthria"), anomia, and paraphasic substitutions, especially for consonants. The most notable characteristic of this sort of speech disorder is its transience; within a number of weeks or months, language is restored to regular. Bastian and extra recently different authors have referred to as this syndrome aphemia, a term that was used initially by Broca in another context- to describe the extreme motor aphasia that now carries his name. Damasio and Geschwind have said that the lesion is anterior and superior to this area. Their patient uttered only some sounds for 4 weeks, after which he recovered rapidly and utterly. From the onset of the stroke, the patient showed no disturbance of comprehension of language or of writing. Anomic (Amnesic, Nominal) Aphasia Some diploma of wordfinding problem is probably part of every sort of language disorder, together with that which happens with the confusional states and dementia. In truth, without an element of anomia, a prognosis of aphasia is often incorrect. Only when this characteristic is essentially the most notable aspect of language problem is the term anomic aphasia employed. In this latter situation, a comparatively unusual type of aphasia, the patient loses only the flexibility to name folks and objects. Or the patient could merely fail to name a shown object, in distinction to the same old aphasic patient, who produces a paraphasic error. When shown a sequence of common objects, the patient could tell of their use, or demonstrate the same, as a substitute of giving their names. The problem applies not only to objects seen however to the names of things heard or felt (Geschwind), however this is harder to demonstrate. Beauvois and coworkers have described a type of bilateral tactile aphasia due to a left parieto-occipital lesion by which objects seen and verbally mentioned could possibly be named, however not those felt with either hand. Recall of the names of letters, digits, and different printed verbal material is almost invariably preserved, and immediate repetition of a spoken name is undamaged. In these instances the lesion has been deep within the basal portion of the posterior temporal lobe or within the center temporal convolution, in place to interrupt connections between sensory language areas and the hippocampal regions involved with studying and memory. Anomia may be a prominent manifestation of transcortical motor aphasia (see under) and may be associated with the Gerstmann syndrome, by which case the lesions are found within the frontal lobe and angular gyrus, respectively. An anomic sort of aphasia is commonly an early signal of Alzheimer and Pick illness (minor levels of it are common in old age) and is a principal characteristic of numerous the degenerative lobar cerebral atrophies (see Chap. Isolation of the Language Areas (Transcortical Aphasias) the identifying characteristic of those language disturbances is a preservation of the flexibility to repeat. Destruction of the vascular border zones between anterior, center, and posterior cerebral arteries- often on account of extended hypotension, carbon monoxide poisoning, or different types of anoxic-ischemic damage- could successfully isolate the intact motor and sensory language areas, all or partly, from the remainder of the cortex of the same hemisphere. In the case reported by Assal and colleagues, for example, multiple infarcts had isolated the entire language area. In transcortical sensory aphasia, so named by Lichtheim and further defined by Goldstein, the patient suffers a deficit of auditory and visible word comprehension, making writing and studying unimaginable. Facility in repetition, in extreme diploma, takes the type of echoing, parrot-like, word phrases and songs which are heard (echolalia). This locale explains the frequent concurrence of transient visible agnosia and hemianopia. The paraphasia is assumed to end result from the weakened management of the motor language areas by the auditory and visible areas, although the direct connection between them, presumably the arcuate fasciculus, is preserved. Preservation of this direct connection is said to account for the flexibility to repeat. In transcortical motor aphasia ("anterior isolation syndrome," "dynamic aphasia" of Luria) the patient is unable to initiate conversational speech, producing only some grunts or syllables. Comprehension is comparatively preserved, however repetition is strikingly intact, distinguishing this syndrome from pure word mutism (see above). Several of our instances have resulted from infarctions within the watershed zone between the anterior and center cerebral arteries, after cardiac arrest or shock. These transcortical syndromes are of great theoretical interest and are probably extra common than is presently appreciated. Foreign Accent Syndrome this uncommon however peculiar (and somewhat amusing) situation defies classification however is worthy of remark as a result of it could be mistaken for hysteria or psychosis. Usually this aberration is encountered as a transient phenomenon throughout recovery from stroke. An extensive analysis of 1 case and references may be found within the article by Kurowski and colleagues. It might be supposed that every one the foundations of language derived from the research of aphasia could be relevant to agraphia. One must be able to formulate ideas in phrases and phrases in order to have something to write in addition to to say; therefore issues of writing, like issues of talking, mirror all the basic defects of language. In speech, only one ultimate motor pathway coordinating the movements of lips, tongue, larynx, and respiratory muscles is out there, whereas if the best hand is paralyzed, one can still write with the left one, or with a foot, and even with the mouth by holding a pencil between the tooth. The writing of a word may be achieved either by the direct lexical technique of recalling its spelling or by sounding out its phonemes and remodeling them into learned graphemes (motor photographs)- i. In help of the latter thought is the fact that studying and writing often develop collectively and are long preceded by the development and elaboration of auditory-articular mechanisms. Pure agraphia because the preliminary and sole disturbance of language operate is a superb rarity, however such instances have been described, as summarized within the review of Rosati and de Bastiani. However, Croisile and associates do cite instances of pure dysgraphia by which a lesion (within the case they reported, a hematoma) was positioned within the centrum semiovale beneath the motor components of the frontal cortex. Quite apart from these aphasic agraphias, by which spelling and grammatical errors abound, there are particular types of agraphia brought on by abnormalities of spatial notion and praxis. Disturbances within the notion of spatial relationships seem to underlie constructional agraphia. In this circumstance, letters and phrases are formed clearly enough however are wrongly organized on the page. Words may be superimposed, reversed, written diagonally or in haphazard arrangement, or from proper to left; within the kind associated with proper parietal lesions, only the best half of the page is used. Usually one finds different constructional difficulties as nicely, similar to inability to copy geometric figures or to make drawings of clocks, flowers, and maps, and so on. Here language formulation is right and the spatial preparations of phrases are respected, however the hand has misplaced its ability in forming letters and phrases. There may be an uncertainty as to how the pen must be held and utilized to paper; apraxias (ideomotor and ideational) are present in the best-hander. In addition to the neurologic types of agraphia, described above, psychologists have defined a group of "linguistic" agraphias, subdivided into phonologic, lexical, and semantic varieties (Roeltgen). These linguistic models are based on loss of the flexibility to write (and to spell) specific lessons of phrases. For instance, the patient may be unable to spell pronounceable nonsense phrases, with preserved ability to spell actual phrases (phonologic agraphia); or there may be preserved ability to write nonsense phrases however not irregular phrases, similar to island (lexical agraphia); patients with semantic agraphia have problem incorporating meaning into the written word. Aphasia has also been described incessantly with dominant striatocapsular lesions, notably in the event that they extend laterally into the subcortical white matter of the temporal lobe and insula. The head of the caudate, anterior limb of the inner capsule, or the anterosuperior aspect of the putamen are the constructions involved in different patients. The aphasia is characterised by nonfluent, dysarthric, paraphasic speech and ranging levels of problem with comprehension of language, naming, and repetition.
Buy 250 mg diamox
It is characterised by quickly rising body temperature, excessive muscular rigidity, and a high mortality fee. Since the original report by Denborough and Lovell in 1960, as larger experience was gained with this entity, it proved to be a metabolic polymyopathy inherited as a dominant trait, rendering the person susceptible to any potent unstable anesthetic agent, significantly halothane, and to the muscle relaxant succinylcholine. The basic trigger in a large proportion of circumstances is an aberration in a part of the calcium channel. Malignant hyperthermia has been estimated to happen approximately once in the midst of each 50,000 administrations of basic anesthesia. The full medical image is hanging but anesthesiologists have turn into adept at detecting its earliest stages. As halothane or an identical inhalational anesthesia is induced or succinylcholine is given for muscular relaxation, the jaw muscles unexpectedly turn into tense quite than relaxed, and shortly the rigidity extends to all the muscles. Circulatory collapse and death could ensue in approximately 10 percent of circumstances, or the patient could survive with gradual restoration. In some circumstances there is identical sequence of events (elevated temperature and acidosis) without muscular spasm. In case of survival for several days, samples of muscle reveal scattered segmental necrosis and phagocytosis of sarcoplasm without inflammation. Pathophysiology the pathogenesis of this reaction has been the topic of a variety of investigations. During the rigor section, oxygen consumption in muscle increases threefold and serum lactate, 15- to 20-fold. Muscle from most affected people is abnormally sensitive to caffeine, which induces contracture in vitro. There is a breed of pigs, inbred for muscular improvement, by which muscle spasm (true contracture) and hyperthermia observe the administration of anesthetic agents. However, considered one of several comparable defects in ryanodine is present in somewhat fewer than 20 percent of human beings. It is presumed that different yet unidentified allelic mutations of this receptor protein or one other that controls the structure of the calcium channel account for the rest of circumstances. Clues as to which patients are in danger for this condition come from several sources. One constellation consists of short stature, ptosis, strabismus, extremely arched palate, dislocated patellae, and kyphoscoliosis, which has been famous in some households (KingDenborough syndrome). This is comprehensible insofar as each problems have been linked to the gene encoding the ryanodine receptor; the 2 ailments are because of allelic variations (Quane et al). It has been pointed out that one other rare muscle illness- Evans myopathy (named after the affected household)- could also be a typical predisposing condition. Diagnostic Testing Various checks for susceptibility to malignant hyperthermia have undergone phases of recognition. The solely currently legitimate take a look at entails in vitro exposure of a muscle biopsy specimen to halothane and to caffeine and the detection of muscle contracture with each agents. The evaluate by Denborough could also be consulted for further particulars on the testing and on the general aspects of the illness. Treatment this consists of discontinuation of anesthesia on the first hint of masseter spasm or rise of temperature. The intravenous administration of dantrolene, which inhibits the release of calcium from the sarcoplasmic reticulum, could also be lifesaving. An infusion of 1 mg/kg is given initially and elevated slowly till symptoms subside, the whole dosage to not exceed 10 mg/kg. Other measures should embrace body cooling, intravenous hydration, sodium bicarbonate infusions to appropriate acidosis, and mechanical hyperventilation to decrease acidosis. Halothane and different unstable anesthesic agents and succinylcholine should thereafter be avoided in such people, and any surgical procedures, if needed, ought to be done beneath nitrous oxide, fentanyl, thiopental (or different barbiturate), or native anesthesia. Only recently has it been appreciated that one form of periodic paralysis, Andersen illness, is associated with the voltagegated potassium channel. In vitro studies indicate that the mutation impairs the power of preformed channels to migrate to the membrane surface and also impedes the present carrying capability of the potassium channel system. This defect could be anticipated to impair repolarization of the muscle membrane, thereby making each skeletal and cardiac muscle hyperexcitable. It is characterised by continuous muscle fiber activity referred to as "neuromyotonia," hyperhydrosis, severe weight reduction, insomnia, and hallucinations. Most circumstances so far described have ended fatally in a matter of months, but plasma change has reversed the syndrome in the case described by Ligouri and colleagues. The condition can also be included in the discussion of the opposite types of continuous muscle fiber activity in the following chapter. Malignant Neuroleptic Syndrome this state, by which hyperthermia happens as an idiosyncratic reaction to neuroleptic medicine, can also be accompanied by widespread myonecrosis. It shares some options with malignant hyperthermia but is a definite entity as mentioned in Chap. Clinical manifestations and inheritance of a kind of periodic paralysis without hypopotassemia. Thus, muscles could go into spasm due to an unstable depolarization of motor axons, which sends volleys of impulses throughout neuromuscular junctions- as happens in myokymia, hypocalcemic tetany, and pseudohypoparathyroidism. In different states, mentioned in the preceding chapter, the innervation of muscle could also be regular but contraction persists regardless of attempts at relaxation (myotonia). Or, after one or a series of contractions, the muscle could also be slow in decontracting, as happens in paradoxical myotonia and hypothyroidism; in the contracture of McArdle phosphorylase deficiency and phosphofructokinase deficiency, muscle, once contracted, could lack the power to relax. Each of those circumstances evokes the grievance of cramp or spasm, which is variably painful and interferes with free and effective voluntary activity. A premium is subsequently hooked up to the medical differentiation of those phenomena. Usually they happen during the night, after a day of unusually strenuous activity; much less usually they happen during the day, both throughout a interval of relaxation or sometimes after a strong voluntary contraction or postural adjustment. The muscle is visibly and palpably taut and painful, and the condition is instantly distinguished from an illusory cramp, by which the feeling of cramp is skilled with little or no contraction of muscle. The latter phenomenon could happen in regular persons as well as in these with certain peripheral nerve ailments. Massage and vigorous stretch of the cramped muscle will trigger the spasm to yield, though for a time the muscle stays excitable and subject to recurrent cramps. Visible fasciculations could precede and observe the cramp, indicating an excessive excitability of the terminal branches of motor neurons supplying the muscle. Sometimes the cramp is so robust that the muscle appears to have been injured; it stays sore to contact and painful upon use for a day or longer. Cramps of precordial chest muscles or diaphragm could arouse worry of coronary heart or lung illness. Cramps are known to enhance in frequency beneath certain circumstances and with certain ailments. Dehydration and sweating predispose to cramping and are a relentless threat to athletes, who try to forestall them by ingesting electrolyte solutions. Exertional cramps are frequent in motor system illness and hypothyroidism and less so in continual polyneuropathies. Patients present process hemodialysis are subject to cramps, which can be suppressed by intravenous hypertonic saline or hypertonic glucose. Focal cramping happens after partial nerve or root injury and with ailments involving anterior horn cells. In one such condition, the calf muscle on one aspect is subject to severe recurrent cramps after decompression of the S1 root in lumbar disc illness; in excessive circumstances, the muscle hypertrophies. In a variety of circumstances with exercise-induced stiffness and muscle ache, sometimes progressing to cramp, below-regular levels of myoadenylate deaminase have been discovered. This enzyme, which is present in high focus in muscle, is assumed to perform primarily throughout aerobic exercise and facilitate the regeneration of adenosine triphosphate from adenosine diphosphate via the action of adenylate kinase. Quinine sulfate- 300 mg at bedtime and repeated in 4 h if needed, or 300 mg tid for diurnal cramping- is an effective medicine; diphenhydramine hydrochloride (Benadryl) 50 mg or procainamide zero. Phenytoin, carbamazepine, propoxyphene, and sometimes clonazepam are much more helpful in alleviating repeated daytime cramping. Tetany, Pseudotetany, and Related Cramp Syndromes As pointed out on web page 1096, a discount in ionizable calcium and magnesium is associated with involuntary cramplike spasms; of their mildest type they appear as distal carpopedal spasms, but they could contain any of the muscles except the extraocular ones. Stimulation of a muscle via its nerve at certain frequencies (15 to 1276 Copyright � 2005, 2001, 1997, 1993, 1989, 1985, 1981, 1977, by the McGraw-Hill Companies, Inc. Indeed, the Trousseau signal- carpal spasms with occlusion of the blood provide to the arm- takes advantage of the latter phenomenon.
Proven diamox 250mg
In such instances the basal ganglia are affected more than the cerebral cortex and white matter as within the case studied by our colleagues Dooling and Richardson. Instances have followed cardiac arrest, drowning, asphyxiation, and carbon monoxide poisoning. In exceptional instances, nevertheless, the supply of sufficient fluid, vasopressor, and respiratory support allows preservation of the somatic organism in a comatose state for longer durations. Posthypoxic Neurologic Syndromes the permanent neurologic sequelae or posthypoxic syndromes noticed most frequently are as follows: 1. With lesser levels of cerebral injury, dementia with or without extrapyramidal indicators 3. Extrapyramidal (parkinsonian) syndrome with cognitive impairment (discussed in relation to carbon monoxide poisoning) 4. A Korsakoff amnesic state If ischemic hypoperfusion dominates, the patient may also show the manifestations of watershed infarctions, situated between the tip territories of the main cerebral vessels. Visual agnosias including Balint syndrome and cortical blindness (web page 406), representing infarctions of the watershed between the center and posterior cerebral arteries. Watershed infarction between the center and posterior cerebral arteries after brief cardiac arrest. All of them incorporate several simple scientific options involving lack of motor, verbal, and pupillary capabilities in numerous combinations. The most often cited and intensive examine of the prognostic aspects of coma following cardiac arrest is the one by Levy and colleagues of a hundred and fifty sufferers who remained in coma for no less than 6 h after cardiac arrest. It has offered the following tips: mortality from this state is high: 20 % died on the first day and sixty four % by the tip of 1 week. In phrases of restoration, 17 % of the sufferers who awakened had carried out so by 3 days, and solely a further 2 % did so by 2 days. At the opposite excessive of the 31 % of sufferers who have been in a vegetative state at 1 day, 70 % survived for 1 week, and solely 3 sufferers recovered. We have never noticed deep coma of this type lasting 5 days in an grownup or more to be attended by full restoration. The question of what to do with sufferers in such states of protracted coma is a societal as a lot as a medical problem. The most that can be expected of the neurologist is to state the extent and diploma of brain harm, its trigger, and the prognosis based on his personal and revealed experience. One prudently avoids heroic, lifesaving therapeutic measures as soon as the character of this state has been decided with certainty. Treatment of Hypoxic-Ischemic Encephalopathy Treatment is directed initially to the prevention of further hypoxic injury. As a clear airway is secured, using cardiopulmonary resuscitation, a cardiac defibrillator, or pacemaker has its place, and each second counts of their immediate utilization. Particular attention is drawn to the randomized trial performed by Bernard and colleagues of gentle hypothermia applied to unconscious sufferers instantly after cardiac arrest. They lowered the core temperature of affected sufferers to 33 C (ninety one F) inside 2 h and demonstrated a doubling of the speed of survival and good outcome. These results have been evaluated by coarse measures of neurologic perform, and these findings have been corroborated within the smaller trial reported by Zeiner et al. Vasodilator medicine, glutamate blockers, and calcium channel blockers are of no proven benefit despite their theoretical attraction and some experimental successes. Oxygen may be of worth in the course of the first hours however is probably of little use after the blood becomes nicely oxygenated. Corticosteroids ostensibly help to allay brain (possibly cellular) swelling, however again, their therapeutic benefit has not been corroborated by scientific trials. For the latter, clonazepam, eight to 12 mg daily in divided doses may be helpful, however the commonly used an- ticonvulsants have little impact in our experience. This state of spontaneous and stimulus-delicate myoclonus as well as persistent limb posturing usually presages a poor outcome. The hanging disorder of delayed movement-induced myoclonus and ataxic tremor that seem after the patient awakens, described by Lance and Adams, is a particular issue, discussed on web page 89. Fever is treated with antipyretics or a cooling blanket combined with neuromuscular paralyzing brokers. The results on the brain for the most part simulate these brought on by cardiac arrest. Early symptoms embody headache, nausea, dyspnea, confusion, dizziness, and clumsiness. These occur when the carboxyhemoglobin degree reaches 20 to 30 % of total hemoglobin. A cherry-pink color of the skin could seem however is definitely an infrequent discovering; cyanosis is more widespread. Only if there has been associated hypotension does one see the identical forms of border-zone infarctions that seem after cardiac arrest. The widespread function among the delayedrelapse sufferers is a protracted period of pure anoxia (before the occurrence of ischemia). Chronic mountain illness, sometimes called Monge illness (after the doctor who described the condition in Andean Indians of Peru), is noticed in long-term inhabitants of high-altitude mountainous regions. Pulmonary hypertension, cor pulmonale, and secondary polycythemia are the primary options. There is usually hypercarbia as nicely, with the expected diploma of gentle mental dullness, slowness, fatigue, nocturnal headache, and sometimes papilledema (see under). Thomas and colleagues have called attention to a syndrome of burning palms and feet in these groups of Peruvians, apparently one other maladaptive response to high altitude. Dexamethasone and acetazolamide prevent and counteract mountain illness to some extent. The most effective preventive measure is acclimatization by a 2- to 4-day stay at intermediate altitudes of 6000 to 8000 ft. The complete scientific syndrome of chronic hypercapnia described by Austen, Carmichael, and Adams includes headache, papilledema, mental dullness, drowsiness, confusion, stupor and coma, and asterixis. The headache tends to be generalized, frontal, or occipital and can be quite intense, persistent, steady, and aching in type; nocturnal occurrence is a function of some instances. The papilledema is bilateral however may be barely higher in a single eye than within the different, and hemorrhages could encircle the choked disc (a later discovering). Intermittent drowsiness, indifference to the setting, inattentiveness, discount of psychomotor activity, inability to perceive all of the items in a sequence of events, and forgetfulness constitute the more delicate manifestations of this syndrome and may immediate the family to search medical help. However, the brain quickly adapts to respiratory acidosis through the generation and secretion of bicarbonate by the choroid plexuses. The solely neurologic residua have been a gentle defect in retentive memory and areas of decreased attenuation within the pallidum bilaterally (arrows). This therapy reduces the incidence of cognitive sequelae from 46 to 25 % in accordance with a trial performed by Weaver and colleagues. High-Altitude (Mountain) Sickness Acute mountain illness is one other particular form of cerebral hypoxia. Headache, anorexia, nausea and vomiting, weak spot, and insomnia seem at altitudes above 8000 ft; on reaching higher altitudes, there may be ataxia, tremor, drowsiness, gentle confusion and hallucinations. At 16,000 ft, in accordance with Griggs and Sutton, 50 % of people develop asymptomatic retinal hemorrhages, and it has been instructed that such hemorrhages also occur within the cerebral white matter. With more extended publicity at these altitudes or with further ascent, affected people endure mental impairment which will progress to coma. Hypoxemia at high altitude is intensified during sleep, as air flow usually diminishes. Oxygen supplementation is, after all, used cautiously in these sufferers so as to keep away from suppressing respiratory drive- marginally compensated sufferers treated with excessive oxygen have lapsed into coma. Treatment of coronary heart failure, phlebotomy to reduce the viscosity of the blood, and antibiotics to suppress pulmonary an infection may be needed. Often these measures result in a surprising diploma of enchancment, which can be maintained for months or years. Unlike pure hypoxic encephalopathy, extended coma as a result of hypercapnia is comparatively uncommon and in our experience has not led to irreversible brain harm. Papilledema and jerky, intermittent lapses of sustained muscular contraction (asterixis) are important diagnostic options. If aminophylline is run for the therapy of the underlying pulmonary airway illness, there may be a bent for seizures.
Generic diamox 250mg
Broad spectrum antibiotics in massive doses must be given initially and the selection of remedy is then refined based mostly on cultures from the abscess or the blood, or on the presumed source of bacteria. Cauda equina epidural abscess without neurologic signs might in lots of cases be treated solely with antibiotics, although some surgeons favor drainage, which must be undertaken in any case if osteomyelitis develops. When osteomyelitis of a vertebral body is the primary abnormality, the epidural extension might implicate only a few spinal sensory and motor roots, leaving long tracts and different intramedullary buildings intact. In some cases with cervical epidural abscesses, stiff neck, fever, and deltoid-biceps weak spot are the principle neurologic abnormalities. Even after apparently profitable drainage and antibiotic remedy of an epidural abscess, there may be a slowly progressive after which stabilizing syndrome of incomplete cord compression. This is the results of formation of a fibrous and granulomatous response at the operative website. Spinal subdural bacterial infections additionally occur and, clinically, are virtually indistinguishable from epidural ones on medical grounds. The pyogenic assortment enhances at the periphery and extends over a number of segments. Subacute pyogenic infections and granulomatous infections (tuberculous, fungal) can also come up in the spinal epidural space, as famous under. In some situations the patient was known to have had systemic bacterial an infection, septicemia, or endocarditis; in others there was a contiguous abscess in the skin or subcutaneous tissues with a fistula to the spinal cord via an intervertebral foramen. Spinal cord abscess is a uncommon complication of spinal dysraphism or of a developmentally open fistulous tract. Woltman and Adson described a patient in whom surgical drainage of an encapsulated intramedullary abscess led to recovery, and Morrison and associates reported a similar case brought on by Listeria monocytogenes, which was successfully drained and the meningeal an infection suppressed by ampicillin and chloramphenicol. Tuberculous Spinal Osteomyelitis (Pott disease) Tuberculous osteitis of the backbone with kyphosis (Pott disease) is well-known in regions of endemic tuberculosis. The osteomyelitis is the results of reactivation of tuberculosis at a website previously established by hematogenous spread. An infectious endarteritis causes bone necrosis and collapse of a thoracic or upper lumbar (less usually cervical) vertebral body leading to a extremely characteristic angulated kyphotic deformity. Most sufferers have some proof of energetic an infection as evidenced by fever, evening sweats, and different consitutional symptoms; the sedimentaion rate is invariably elevated. What is shocking to us about Pott disease is the excellent result which may be obtained by external stabilization of the backbone and long-term antituberculous medication. Tuberculous Myelitis Solitary tuberculoma of the spinal cord as part of a generalized an infection is an extreme rarity. More usually, pus or caseous granulation tissue might extrude from an infected vertebra and offers rise to an epidural compression of the cord (Pott paraplegia, as distinct from Pott disease). Occasionally a tuberculous meningitis might result in pial arteritis and spinal cord infarction. All these types of tuberculosis have become infrequent in the United States and western Europe but we see a brand new case every a number of years in sufferers who spent their earlier life in India or Africa. Meningomyelitis as a result of Fungus and Parasitic Diseases A broad variety of fungal and parasitic agents might contain the spinal meninges. We have cared for 2 sufferers in whom the spinal cord in the low thoracic and lumbar area was infected approximately three weeks after they swam in contaminated water throughout an African trip. The administration of praziquantel arrested the course of the sickness, but the sufferers had been left disabled. Myelitis of Noninfectious Inflammatory Type (Acute and Subacute Transverse Myelitis; See additionally Chap. The crucial factor of their pathogenesis appears to be a disordered immune response, in some cases, to an an infection, and in others, idiopathic. While each of those situations might affect different elements of the nervous system (most often the optic nerves or mind), usually the only manifestations are spinal. Postinfectious and Postvaccinal Myelitides the characteristic features of those illnesses are (1) their temporal relationship to certain viral infections or vaccinations (see page 791); (2) the development of neurologic signs over the interval of some days; and (three) a monophasic temporal course, i. The traditional history in these cases is for weak spot and numbness of the feet and legs (less usually of the arms and arms) to develop over a couple of days, at instances longer, and for the sensory symptoms to ascend from the feet to the trunk. A slight asymmetry of the symptoms and signs, a sensory level on the trunk, or a Babinski sign clearly marks the disease as a myelopathy and serves to distinguish it from a rapidly progressive polyneuropathy such because the Guillain-Barre syndrome. Back ache of varying diploma and head� ache and stiff neck might or will not be present. Cryptococcus, which causes meningoencephalitis and rarely a cerebral granuloma, in our experience seldom causes spinal lesions. Hematogenous metastases to the spinal cord or meninges might occur in each blastomycosis and coccidioidomycosis. Occasionally an echinococcal an infection of the posterior mediastinum might extend to the spinal canal (epidural space) through intervertebral foramina and compress the spinal cord. Schistosomiasis (bilharziasis) is a acknowledged reason for myelitis in the Far East, Africa, and South America. The lesions are harmful of gray and white matter, with ova in arteries and veins resulting in vascular obstruction and ischemia (Scrimgeour and Gajdusek). The sickness evolves over a number of days, typically a single day or on the opposite extreme, over one to 2 weeks. There may be solely three or four cells per cubic millimeter, or none, making the inflammatory side less clear. Clinical variants of this syndrome are frequent in our experience; together with: an virtually pure paresthetic sickness with posterior column dysfunction and the converse; a symmetrical paraparesis with analgesia under a level on the trunk but without involvement of deep sensation (a syndrome usually associated with infarction in the territory of the anterior spinal artery); a syndrome of variable sensory loss involving the leg and groin on one facet or each; a purely lumbosacral or sacral myelopathy (conus syndrome with saddle analgesia and sphincter disturbances); and a partial BrownSequard syndrome. The neurologic signs appeared because the rash was fading, usually with a slight recrudescence of fever. The listing of antecedent infections is in any other case a lot the same as that for the Guillain-Barre syndrome with the notable absence of Campy� lobacter jejuni, which has not led to myelitis. It could be reasonably assumed that pharyngitis, respiratory an infection, or conjunctivitis, and so forth. There is T2 sign change and different images confirmed delicate enhancement after gadolinium infusion. Further dialogue of acute transverse myelitis in relation to different demyelinating illnesses could be discovered under and on pages 778 and 791. The pathologic changes take the form of quite a few subpial and perivenular zones of demyelination, with perivascular and meningeal infiltrations of lymphocytes and different mononuclear cells, and para-adventitial pleomorphic histiocytes and microglia (page 772). We have additionally used plasma change or intravenous immune globulin in a number of sufferers, with uncertain results, although this method was seemingly helpful in a couple of sufferers who had an explosive medical onset. Invariably, the myelitic disease improves, typically to a shocking diploma, but there are examples in which the sequelae have been severe and permanent. Pain in the midthoracic area or an abrupt, severe onset usually indicates a poor prognosis (Ropper and Poskanzer). Also, their relation to antecedent infections is less certain, and in most recorded examples such provocative events had been lacking. The commonest mode of medical expression of demyelinative myelitis is with numbness that spreads over one or each side of the body from the sacral segments to the feet, anterior thighs, and up over the trunk, with coincident but variable and usually asymmetric weak spot after which paralysis of the legs. The sensorimotor disturbance might extend to contain the arms, and a sensory level could be demonstrated on the upper elements of the trunk. Those cases with a necrotic element, Devic disease and the carefully related subacute necrotic myelopathy, might stabilize but then worsen (see under). The differential diagnosis of demyelinative myelitis is taken into account more fully in Chap. Other sufferers, however, show no obvious response, and a a proportion of cases have even continued to worsen while the medication was being given. Plasma change and intravenous immune globulin have reportedly been beneficial in individual cases, significantly in these with an explosive onset (see later). Acute and Subacute Necrotizing Myelitis and Devic Disease (see page 781) In every massive medical heart, occasional examples of this dysfunction are discovered among the many sufferers who present with a subacute paraplegia or quadriplegia, sensory loss, and sphincter paralysis. The neurologic signs might erupt so precipitously that a vascular lesion is assumed. In most different cases, the disease evolves at a slower and usually stepwise pace, over a number of months or years (Katz and Ropper). Necrotizing myelopathy is distinguished from the more common kinds of transverse myelitis by a persistent and profound flaccidity of the legs (or arms if the lesion is cervical), areflexia, and atonicity of the bladder- all reflecting a widespread necrosis that includes each the gray and white matter of the spinal cord over a considerable vertical extent. This image is sudden for a spinal cord lesion and, subsequently, is commonly mistakenly attributed to spinal shock or to a very totally different course of such as Guillain-Barre syndrome. Highly characteristic on imaging studies carried out weeks or more later is severe atrophy of the involved segments of cord. The finding by Lennon and colleagues of a particular serum IgG antibody in half of cases of Devic disease is notable.
Oleum Chaulmoograe (Chaulmoogra). Diamox.
- How does Chaulmoogra work?
- What is Chaulmoogra?
- Skin disorders, psoriasis, eczema, and leprosy.
- Dosing considerations for Chaulmoogra.
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96614
Quality diamox 250mg
Notably, both phenomena are thought of to be symptomatic of "gray matter" illnesses ("polioencephalopthies"). Myoclonus or polymyoclonus might, in sure situations, stand alone as a relatively pure syndrome. The many acquired types of polymyoclonus, such as subacute sclerosing panencephalitis, have been mentioned in Chap. Myoclonic Encephalopathy of Infants (Infantile OpsoclonusMyoclonus Syndrome) Under this title Kinsbourne initially described a form of widespread, continuous myoclonus (except throughout deep sleep) affecting male and female infants whose improvement had been normal until the onset of the disease at the age of 9 to 20 months. The myoclonus evolves over every week or less, affects all the muscles of the physique, and interferes critically with all the natural muscular actions of the kid. Treatment Adrenocorticotropic hormone and dexamethasone, the latter in doses of 1. Some sufferers have recovered from the myoclonus but have been left mentally sluggish and mildly ataxic. Others have required corticosteroid therapy for five to 10 years, with relapse every time it was discontinued. A similar syndrome has been observed in conjunction with neuroblastoma in youngsters and as a transient illness of unknown trigger (in all probability viral or postinfectious) in young adults (Baringer et al; see page 641). It is mentioned here as a result of a similar situation is also recognized in adults, as a paraneoplastic disease with ovarian, breast, gastric, and bronchogenic carcinomas and with other occult tumors. In a broader survey of the pediatric opsoclonus-myoclonus syndrome, Pranzatelli and associates reported their experience with 27 instances, some with neural crest tumors, others with viral infections or hypoxic injury (intention myoclonus). In practically all of their sufferers there was cerebellar ataxia and psychological dysfunction, and 10 % had seizures. Familial Progressive Myoclonus Five major categories of familial polymyoclonus of late childhood and adolescence have been delineated: (1) Lafora- or amyloid-physique sort, (2) juvenile cerebroretinal degeneration, (three) cherry-pink spot� myoclonus (sialidosis or neuraminidosis), (four) mitochondrial encephalopathy, and (5) a extra benign degenerative disease (dyssynergia cerebellaris myoclonica of Hunt). Lafora-Body Polymyoclonus with Epilepsy this disease, which is inherited as an autosomal recessive trait, was first identified by Lafora in 1911 on the premise of the massive basophilic cytoplasmic our bodies that had been discovered in the dentate, brainstem, and thalamic neurons. Beginning in late childhood and adolescence (eleven to 18 years) in a beforehand normal particular person, the disease declares itself by a seizure, a burst of myoclonic jerks, or both. The illness might at first be mistaken for strange epilepsy, but within a number of months it becomes evident that something way more critical is happening. The myoclonus becomes widespread and could be evoked as a startle by noise, an sudden tactile stimulus (even the tap of a reflex hammer), and in addition by excitement, or sure sustained motor actions. An evoked prepare of myoclonic jerks might progress to a generalized seizure with lack of consciousness. Close examination can also reveal an alteration in muscle tone and a slight diploma of cerebellar ataxia. At this time, or even before the onset of myoclonus and seizures, the affected person might experience visible hallucinations or exhibit irritability, odd traits of character, uninhibited or impulsive behavior, and, finally, progressive failure in all cognitive capabilities. Rigidity or hypotonia, impaired tendon reflexes, acrocyanosis, and infrequently corticospinal tract indicators are late findings. Finally the affected person becomes cachectic and bedfast and succumbs to intercurrent an infection. Nonetheless there are isolated stories of Lafora-physique disease by which signs began as late as 40 years, with dying as late as 50 years. These inclusions have been seen in pores and skin and liver biopsies, even though liver operate tests had been normal. Neuropathologic examinations have proven a slight lack of granule and Purkinje cells and lack of neurons in the dentate nuclei, inner segment of globus pallidus, and cerebral cortex in addition to the Lafora our bodies. The latter can also be seen in the retina, cerebral cortex, myocardium, and striated muscles. Polyglycosan Body Disease (See additionally page 914) that is another closely related disease, the options of which have been reviewed by Robitaille and coworkers, by which glycosamine our bodies are discovered in the central and peripheral nervous system. The medical syndrome contains dementia, chorea, and amyotrophy with or with out sensory loss in the limbs. Diagnosis is confirmed by the discovering of the polyglycosan our bodies in the axons of peripheral nerves or liver cells. The causative mutation typically affects the gene for glycogen branching enzyme. Juvenile Ceroid Lipofuscinosis (Cerebroretinal Degeneration) As said earlier, this is among the most variable types of the lipidoses. The salient medical options of the later-onset varieties are severe myoclonus, seizures, and visible loss. In the juvenile sort, the first lesions are seen in the maculae; they seem as yellow-gray areas of degeneration and stand in contrast to the cherry-pink spot and the encircling white ring of Tay-Sachs disease. At first, the particles of retinal pigment are nice and mud-like; later they mixture to resemble extra the bone-corpuscular shapes of retinitis pigmentosa. The usual improvement of those and other manifestations of the disease was outlined by Sjogren, who studied a � giant number of the late infantile and juvenile kinds of instances in Sweden. After roughly 2 years, the onset of generalized seizures and myoclonus, often with irritability, poor control of feelings, and stuttering, jerky speech. Gradual intellectual deterioration (poor memory, reduced psychological exercise, inattentiveness). Stage of severe dementia by which the affected person needs help to walk, no longer speaks, and will scream when disturbed or pressured to move. The muscles are wasted, though the tendon reflexes remain energetic, and the plantar reflexes are extensor. Finally the affected person lies curled up in mattress, blind and speechless, with sturdy extensor plantar reflexes, sometimes adopting dystonic postures. Diagnosis could be confirmed by the appearance of inclusions of a curvilinear "fingerprint" sample in electron microscopic examine of biopsy material, notably of the eccrine sweat glands of the pores and skin. A faulty membrane protein has been identified that varieties the inclusion material in the most common, or basic, juvenile phenotype. Late Juvenile and Adult Ceroid Lipofuscinosis (Kufs disease) the Kufs sort of ceroid lipofuscinosis, which develops later (15 to 25 years of age or older), is usually unattended by visible or retinal modifications and is even slower in its evolution. It is offered here for ease of exposition, however it becomes relevant mostly in relation to dementing illness in young adulthood (page 829). Personality change or dementia is one constellation, the opposite being myoclonic seizures with subsequent dementia and even later pyramidal and extrapyramidal indicators. As the disease progresses, cerebellar ataxia, spasticity and rigidity or athetosis, or mixtures thereof, are combined with dementia. As a measure of the variability of the medical presentation, a current affected person of ours had obscure visible difficulties at age 51 and developed a spastic quadriparesis with disinhibited behavior over 5 years. Further comments regarding the unusual shows of this disease could be discovered additional on, underneath "Adult Forms of Inherited Metabolic Disease. Adams that family members of those sufferers might have retinal modifications with out neurologic accompaniments. Of all the lipidoses, these cerebroretinal degenerations had for many years defied unifying biochemical definition. Our understanding of those illnesses is difficult as a result of they embody both enzymatic defects and structural protein dysfunctions. In a number of of the early childhood varieties, mutations of certainly one of a number of lysosomal enzymes have been identified, as summarized by Mole and by Wisniewski and colleagues. The genetic defects have been tentatively determined for some of the subtypes of neuronal ceroid lipofuscinosis (see Wisniewski et al). Twenty-4 such instances (from 20 kindreds) had been collected from the medical literature by Meek and coworkers. Ataxia and dysarthria had been frequently the presenting signs, adopted by dementia, dysphagia, spasticity, dystonia, seizures, and myoclonus. Degeneration of anterior horn cells with progressive muscular atrophy could also be a function, though that is extra characteristic of the adult-onset variety (see additional on). One of our sufferers is alive at 50 years, the disease having begun in adolescence. Late Gaucher Disease with Polymyoclonus A sort of Gaucher disease is sometimes encountered by which seizures, severe diffuse myoclonus, supranuclear gaze disorders (sluggish saccades, saccadic and pursuit horizontal gaze palsies), and cerebellar ataxia begin in late childhood, adolescence, or adult life. The pathologic and biochemical abnormalities are the identical as these of Gaucher disease of earlier onset (Winkelman et al). Cherry-Red Spot� Myoclonus Syndrome (Sialidosis Type 1, Neuraminidase Deficiency) this can be a comparatively new and genetically distinct class of disease characterized by the storage in nervous tissue of sialidated glycopeptides. In some of the sufferers the onset has been in late childhood or adolescence and in others even later. In one case there was severe episodic ache in the arms, legs, and feet throughout scorching weather, paying homage to Fabry disease.
Effective 250mg diamox
Muscles of the pelvic girdle, lumbosacral spine, and shoulders become weak and wasted, accounting for certain medical peculiarities. Weakness of stomach and paravertebral muscles accounts for a lordotic posture and protuberant stomach when standing and the rounded back when sitting. Bilateral weak point of the extensors of the knees and hips interferes with equilibrium and with activities such as climbing stairs or rising from a chair or from a stooped posture. In standing and walking, the patient places his ft extensive apart in order to increase his base of support. To rise from a sitting position, he first flexes his trunk at the hips, puts his arms on his knees, and pushes the trunk upward by working the arms up the thighs. In getting up from a recumbent position, the patient turns his head and trunk and pushes himself sideways to a sitting position S. Wilson used an alliterative phrase to describe the characteristic abnormalities of stance and gait- the patient "straddles as he stands and waddles as he walks. Many affected boys have a tendency to walk on their toes as a consequence of contractures in the gastrocnemeii muscles. Weakening of the muscles that fix the scapulae to the thorax (serratus anterior, lower trapezius, rhomboids) causes a winging of the scapulae, and the scapular angles can sometimes be seen above the shoulders when one is dealing with the patient. The muscles which might be selectively affected embrace the neck flexors, wrist extensors, brachioradialis, costal a part of the pectoralis major, latissimus dorsi, biceps, triceps, anterior tibial, and peroneal muscles. The ocular, facial, bulbar, and hand muscles are normally spared, although weak point of the facial and sternocleidomastoid muscles and of the diaphragm happens in the late stages of the illness. The house between the lower ribs and iliac crests diminishes with affection of the stomach muscles. The limbs are normally unfastened and slack, but as the incapacity progresses, fibrous contractures appear on account of the limbs remaining in a single position and the imbalance between agonists and antagonists. Early in the ambulatory section of the illness, the ft assume an equinovarus position because of shortening of the posterior calf muscles, which act without the traditional opposition of the pretibial and peroneal muscles. Later, the hamstring muscles become completely shortened due to an absence of counteraction of the weaker quadriceps muscles. Similarly, contractures occur in the hip flexors due to the comparatively higher weak point of hip extensors and stomach muscles. This results in a pelvic tilt and compensatory lordosis to keep standing equilibrium. The consequences of those contractures account for the recurring posture of the patient with Duchenne dystrophy: lumbar lordosis, hip flexion and abduction, knee flexion, and plantar flexion. As they become severe, these contractures contribute importantly to the eventual lack of ambulation. Scoliosis, because of unequal weakening of the paravertebral muscles, and flexion contractures of the forearms appear, normally after walking is now not attainable. The tendon reflexes are diminished and then misplaced as muscle fibers disappear, the ankle reflexes being the final to go. The bones are skinny and demineralized, and the appearance of ossification facilities is delayed. Death is normally the result of pulmonary infections and respiratory failure and, sometimes, of cardiac decompensation. These sufferers normally survive till late adolescence, and no more than 20 to 25 % of sufferers stay beyond the twenty-fifth year. The final years of life are spent in a wheelchair; finally the patient becomes bedfast. Mild degrees of psychological retardation, which is nonprogressive, are noticed in many circumstances. As mentioned earlier, Roses and colleagues have studied the female carriers of the illness. A small variety of female carriers manifest a reasonable diploma of myopathy that will mimic limb-girdle dystrophy (see further on). The muscle fibers of such sufferers (referred to as manifesting or symptomatic carriers) present a novel mosaic immunostaining sample- some fibers containing dystrophin and others missing it (Hoffman et al). The female service may often show the identical abnormalities, but to a a lot milder diploma. Becker-Type Muscular Dystrophy this well-characterized dystrophy is carefully related to the Duchenne kind. It had long been famous that mixed with the Duchenne group of circumstances had been certain comparatively benign ones. In 1955, Becker and Keiner proposed that the latter be separated as a distinct entity, now known as Becker muscular dystrophy. It causes weak point and hypertrophy in the identical muscles as the Duchenne dystrophy, however the onset is way later (imply age, 12 years; vary, 5 to 45 years). We have for instance encountered sufferers who served in the navy with the illness undetected. If maternal uncles are affected by the illness and are nonetheless walking, the diagnosis is comparatively straightforward. Kuhn and associates have reported a genealogy during which early myocardial illness and cramping myalgia had been prominent features. Pathology of Duchenne and Becker Dystrophies In the early stages of Duchenne dystrophy, essentially the most distinctive features are prominent segmental degeneration and phagocytosis of single fibers or teams of fibers and proof of regenerative activity (basophilia of sarcoplasm, hyperplasia and nucleolation of sarcolemmal nuclei, and the presence of myotubes and myocytes). The necrosis excites a regenerative or restorative course of, which explains the forking of fibers and clustering of small fibers with prominent nuclei. The necrotic sarcoplasm and sarcolemma are removed by mononuclear phagocytic (macrophage) cells. There is a hyalinization of the sarcoplasm of many degenerating and nondegenerating fibers. In longitudinal sections, these are seen as "contraction bands," expressive of the irritability of dystrophic muscle. Eventually there are histologic changes which might be common to all kinds of superior muscular dystrophies: lack of muscle fibers, residual fibers of bigger and smaller measurement than normal- all in haphazard association, and the secondary reaction of a rise in lipocytes and fibrosis. Hypertrophy of muscle is believed to be a results of workinduced enlargement of the remaining sound fibers in the face of adjacent fiber injury. But examples of true hypertrophy of complete muscles prior to the first signal of weak point can also occur and are tough to clarify. In these circumstances, giant fibers could also be present when at most there are only some degenerating fibers. Pseudohypertrophy is because of lipocytic replacement of degenerated muscle fibers, but in its earlier stages the presence of many enlarged fibers contributes importantly to the enlargement of muscle, all secondary changes. Smallness of residual fibers (probably atrophy) is a prominent histologic characteristic. It is unsure if this represents a gradual failure of cell metabolism and discount in volume of all sarcoplasmic constituents or a stage in the regeneration of the damaged muscle fiber. The fibers do ultimately degenerate and disappear, owing presumably to an exhaustion of regenerative capability after repeated injuries or increasingly extensive necrosis. In the late stage of the dystrophic course of, only some scattered muscle fibers stay, almost misplaced in a sea of fats cells. It is notable that the late or burned-out stage of continual polymyositis resembles muscular dystrophy in that the fiber inhabitants is depleted, the residual fibers are of variable measurement, and fats cells and endomysial fibrous tissue are elevated; missing solely are the hypertrophied fibers of dystrophy. This resemblance confirms that lots of the typical changes of muscular dystrophy are nonspecific, reflecting solely the chronicity of the myopathic course of. Etiology of Duchenne and Becker Dystrophies crucial development in our understanding of the Duchenne and Becker muscular dystrophies was the discovery by Kunkel of the abnormal gene on the X chromosome and of its gene product, dystrophin (Hoffman et al). The protein is expressed in skeletal, cardiac, and smooth muscle in addition to in brain. The biochemical assay of dystrophin and its histochemical demonstration near the sarcolemma have made attainable the accurate diagnosis of the Duchenne and Becker phenotypes and have clarified the relationship between these two issues. Moreover, phenotypes that falls between the classic Duchenne and Becker types (intermediate or "outlier" circumstances) are characterized by a lower than normal quantity of dystrophin. The Duchenne and Becker dystrophies and their intermediate types are spoken of as dystrophinopathies. A slightly totally different form of dystrophin, originating in a different a part of the gene, is present in neurons of the cerebrum and brainstem and in astrocytes, Purkinje cells, and Schwann cells, at nodes of Ranvier (Harris and Cullen). A deficiency of the cerebral dystrophin may in some but unexplained means account for the delicate psychological retardation. Figure 50-1 is beneficial in understanding the pathogenesis of the dystrophinopathies and certain of the limb-girdle and congenital dystrophies described further on.
Diamox 250 mg
In other words, the attribution of persistent coma and the vegetative state to diffuse axonal damage remains uncertain in our view and disruption of the caudal thalamic and rostral midbrain areas have been often present in our material. Primary brainstem hemorrhages, are distinguished from the secondary hemorrhages resulting from the results of downward displacement of the brainstem (transtentorial herniation). Duret initially emphasized the medullary location of those hemorrhages, but the time period Duret hemorrhage has come to signify any secondary brainstem hemorrhage. In addition to contusions and extradural, subdural, subarachnoid, and intracerebral hemorrhages, there are variable levels of vasogenic edema that increases during the first 24 to 48 h, and zones of infarction because of vascular spasm caused by subarachnoid blood surrounding basal vessels. Marmarou et al have convincingly demonstrated that mind swelling after head damage is essentially the result of edema and never of a rise in cerebral blood quantity, as has long been postulated. In youngsters and in some instances in adults, the cerebral edema could also be huge and lead to secondary brainstem compression. In many emergency wards and intensive care items, the Glasgow Coma Scale is used as a rapid reference to accomplish this purpose (Table 35-1). It registers three elements of neurologic operate: eye opening, verbal response, and motor response to various stimuli. The scores supplied by this scale have been discovered to correspond roughly with consequence of the top damage, as mentioned further on. The scale uses a summed score with a maximum of 15; a score of seven or less is taken into account to mirror extreme trauma and a poor medical state, 8 to 12, moderate damage, and better scores, gentle damage. Patients Who Are Conscious or Are Rapidly Regaining Consciousness (Minor Head Injury) this is probably the most frequently encountered medical scenario. Roughly, two levels of disturbed operate may be recognized inside this class. In one, the affected person was not unconscious in any respect however solely surprised momentarily or "saw stars. There can be slight subarachnoid blood along the tentorium and in the insular cisterns, both typical of traumatic bleeding. There are multiple small hemorrhagic areas (considered one of which is shown by the dark arrow) in the cerebral white matter. Also shown are a contusion in the anterior temporal lobe (white arrow), which frequently accompanies the deep kind of axonal damage, and blood in the ventricle. In the second instance, consciousness was briefly abolished for a few seconds or minutes, i. When such a affected person is first seen, recovery may already be full, or he could also be in one of many phases of partial recovery described earlier, beneath "Clinical Manifestations of Concussion. Thereafter, headache and other symptoms of the posttraumatic syndrome or compensation neurosis may develop. In solely a small group of those patients, mainly in those that are slow in regaining consciousness or have a cranium fracture, is there significant threat of ongoing hemorrhage or other delayed complications. Whether to acquire x-ray movies of the top routinely in such patients is an unresolved drawback. He states that this increases to 1 in 30 in patients with a fracture; however most research, such because the one by Lloyd and colleagues, have discovered that the presence of a cranium fracture in youngsters proves to be a relatively poor indicator of intracranial damage. This is underscored by the outcomes of a research of 215 youngsters with minor head trauma carried out by Simon and colleagues; 34 youngsters with no recognized loss of consciousness and a Glasgow Coma Scale score of 15 nonetheless displayed intracranial lesions, though solely 3 required surgical procedure. These minor and seemingly trivial head accidents may sometimes be followed by a number of puzzling and worrisome medical phenomena, some insignificant, others severe and indicative of a pathologic process aside from concussion. Delayed Fainting after Head Injury Following an accident, the injured individual, after strolling about and seeming to be normal, may turn pale and fall unconscious to the bottom. This is a vasodepressor syncopal assault, possibly related to ache and emotional upset, and differs in no way from the fainting that follows ache and fright without damage. Such syncopal attacks also happen with accidents that spare the top, however with head damage they turn out to be harder to interpret. Again, the affected person seems to be recovering from a blow to the top, which can simply have dazed him or triggered a short interval of unconsciousness, when abruptly, after a interval of several minutes to hours, he collapses and becomes unresponsive for a short time. The most disquieting feature of this medical state is a marked bradycardia, which, coupled with the lucid interval, raises the specter of an evolving epidural hemorrhage (really, bradycardia is a late and inconstant sign of epidural bleeding). A extra severe form of delayed collapse after head damage is described further on, beneath "Concussion Followed by a Lucid Interval. They lie down, are drowsy, complain of headache, and will vomit- symptoms that suggest the presence of an epidural or subdural hemorrhage. There is normally no cranium fracture however, as Nee and colleagues level out, vomiting is related to a rise in the incidence of cranium fracture. The symptoms subside after a few hours, testifying to the benign nature of the condition. Transient Traumatic Paraplegia, Blindness, and Migrainous Phenomena With falls or blows on prime of the top, both legs may turn out to be briefly weak and numb, with wavering bilateral Babinski signs and sometimes with sphincteric incontinence. A concussion of the cervical portion of the spinal cord is one other instructed however improbable mechanism of transient paraplegia. The blindness and paraplegia are normally followed by a throbbing vascular kind of headache. Transient migrainous visible phenomena, aphasia, or hemiparesis, followed by a headache, are noticed sometimes after minimal concussion in athletes who participate in competetive contact sports activities. Possibly all of those phenomena are because of an assault of migraine or migraine equal induced by a blow to the top. Another medical possibility, notably in instances of acute quadriplegia, is cartilagenous embolism of the cervical cord (page 1072). Delayed Hemiplegia In our expertise, most examples of those issues have occurred in male adolescents or young adults who, some hours after a relatively minor athletic or extra extreme highway damage, developed an enormous hemiplegia, homonymous hemianopia, or aphasia (with left-sided lesions). In other instances, notably after a blow to the neck, a mural thrombus varieties in the carotid, which, in turn, may shed an embolus to the anterior or center cerebral artery. In yet other instances, the hemiplegia has no rationalization aside from the blow to the top, perhaps the result of the migraine phenomenon described above. Other causes of delayed hemiplegia are a late evolving epidural or subdural hematoma and, in more extreme accidents, an intracerebral hemorrhage (sometimes from a pre-existent arteriovenous malformation). Fat Embolism With fractures of large bones, there could also be, after 24 to seventy two h, an acute onset of pulmonary symptoms (dyspnea and hyperpnea) followed by coma with or without focal signs or seizures; this sequence is due to systemic fats embolism, first of the lungs and then of the mind. In some instances the onset of pulmonary symptoms is related to a petechial rash over the thorax, and one in three instances is claimed to present fats globules in the urine. Respiratory misery is crucial and infrequently the one feature of the fats embolism syndrome, evident in the chest movie as fluffy infiltrates in both lungs. In the mind, the fats emboli trigger widespread petechial hemorrhages, involving both white and gray matter and a few bigger infarcts. Most patients with fats embolism get well spontaneously in 3 or 4 days, though a mortality rate of as much as 10 percent is quoted, normally related to the underlying accidents. Patients Who Have Been Comatose from the Time of Head Injury Here the central drawback, so ably set forth by Symonds, is the relationship between concussion and contusion. Careful pathologic examination of such instances normally discloses evidence of elevated intracranial strain and of cerebral contusions, lacerations, subarachnoid hemorrhage, zones of infarction, and scattered intrace- rebral hemorrhages- both on the level of damage (coup) and on the alternative side (contrecoup), in the corpus callosum, and between these points, along the line of pressure of the damage. In some patients, the diffuse axonal kind of damage is a outstanding abnormality; most frequently, there are separate however strategically positioned ischemic and hemorrhagic lesions in the higher midbrain and decrease thalamic region, as already mentioned. The tissue across the contusions is swollen, and in postmortem preparations the white matter in these regions seems pale in myelin stains. It must be kept in mind that extreme head damage is related to a direct arrest of respiration and sometimes with bradyarrhythmia and cardiac arrest. The effects on the mind of those systemic adjustments may in themselves be sufficiently profound to trigger coma. Also, head damage often complicates alcohol and drug ingestion, so that the possibility of a poisonous or metabolic encephalopathy because the trigger (or a contributing trigger) of stupor should all the time be considered. Within this class of extreme head damage and protracted coma, three medical subgroups may be recognized: one in which cerebral and other bodily accidents are extreme and could also be incompatible with survival; a second in which improvement sets in inside a few days or per week or two, followed by variable levels of recovery however leaving the affected person with residual neurologic signs; and a 3rd and relatively small group in which the patients remain permanently comatose, stuporous, or profoundly reduced of their cerebral capacities, i. Of course there are many levels of damage that fall between these three arbitrary subgroups. In all of those patients, following the initial interval of stabilization, the matters of curiosity are the medical and radiologic assessments, with the purpose of uncovering a surgically remediable lesion- namely a subdural or epidural hematoma- or a treatable intraparenchymal hematoma. When first seen, such a affected person could also be in shock (possibly from rupture of a visceral organ or damage of the cervical cord), with hypotension, hypoxia, hypothermia, a fast thready pulse, and pale, moist pores and skin. If this state persists together with deep coma, extensively dilated fastened pupils, absent eye movements and corneal and pharyngeal reflexes, flaccid limbs, stertorous and irregular respirations or respiratory failure, death normally follows in a short time. In a few of these patients, the blood strain and respirations stabilize; the degree of cerebral damage can then be evaluated over a interval of hours by observing the depth of coma and the temperature, pulse, and blood strain.
Buy diamox 250 mg
Troglitazone, the primary of a new class of antidiabetic drugs, the glitazones, was additionally marketed in 1994 however withdrawn due to liver injury. Another new class of medication, acting on the incretin system, were introduced in 2005. Tolbutamide, phenformin and insulin were compared within the remedy of maturity-onset diabetes within the first randomized managed trial, the University Group Diabetes Program [73�75]. This much-criticized study concluded that the death rate was greater for both oral brokers than for placebo, and that insulin (whether given in a set or variable dose) was no better than placebo [75]. Long-acting insulins were welcomed by diabetes specialists and sufferers, however their use as a single daily injection in all probability produced worse glycemic management than three or 4 injections of soluble insulin. Indeed, delayed-motion preparations were initially condemned by some diabetes specialists, similar to Russell Wilder of the Mayo Clinic, because the patient could slip without obvious warning into hypoglycemia. The number and variety of insulin preparations proliferated, however the primary advances were in strategies to produce highly purified preparations from porcine or bovine pancreas, which remained the source for therapeutic insulin till the early Nineteen Eighties. From there, genetic engineering has been used to produce "designer" insulins such as the quick-acting insulin analogs lispro and aspart and the "peakless" basal insulins similar to glargine and detemir. The only way of monitoring diabetic management was by testing the urine for glucose, and attempts to keep the urine free from sugar inevitably resulted in extreme hypoglycemia and sometimes psychologic injury. This led to the so-known as "free food regimen" movement � linked notably with Adolf Lichtenstein (Stockholm) and Edward Tolstoi (New York) � which encouraged sufferers to eat no matter they liked and to not fear about glycosuria, nonetheless heavy. Only one-third of diabetes physicians questioned in England in 1953 thought that normoglycemia would stop diabetic issues, and only one-half advised urine testing at home [seventy seven]. Practical monitoring of diabetic management turned feasible within the late Nineteen Seventies with the introduction into clinical practice of check strips for measuring blood glucose in a fingerprick sample and the demonstration that ordinary sufferers could use them at home [78,79]. These strategies in turn made potential the North American Diabetes Control and Complications Trial, which in 1993 lastly established that good management prevents and delays the progression of microvascular issues in type 1 diabetes [81]. By the late Nineteen Nineties it was clear that decreasing glucose ranges, high blood pressure or ldl cholesterol separately would reduce the frequency of heart disease and death and it was pure to wonder whether tackling them concurrently (multiple danger issue intervention) could be even better. The Steno 2 study, which started in Denmark in 1992, enrolled sufferers with type 2 diabetes with microalbuminuria and after thirteen years of observe-up showed that multiple danger issue intervention reduced the danger of death by 20% and the danger of growing nephropathy, retinopathy and neuropathy by 50% [84]. Diabetic issues Apart from the final advantages of controlling blood glucose, some specific remedies have emerged for sure persistent issues. Well-carried out clinical trials during the late Nineteen Seventies showed the effectiveness of laser photocoagulation in preventing visual loss from both maculopathy and proliferative retinopathy [85]. This technique was derived from the xenon arc lamp initially described within the late Nineteen Fifties by Gerd Meyer-Schwickerath (1921�92) of Essen, Germany [86]. The significance of blood pressure management in preventing the progression of nephropathy is now absolutely recognized, and angiotensin-converting enzyme inhibitors could also be notably helpful; that blood pressure management slowed the progression of nephropathy was shown in studies by Carl-Erik Mogensen (b. Diabetic ketoacidosis the introduction of insulin was only one side of the administration of this acute and beforehand fatal complication of diabetes. Of the primary 33 instances handled by Joslin and his colleagues between January 1, 1923 and April 1, 1925, 31 survived � a wonderful end result, even by modern requirements, which Joslin [89] attributed to: "Promptly applied medical care, relaxation in mattress, particular nursing attendance, warmth, evacuation of the bowels by enema, the introduction of liquids into the physique, lavage of the stomach, cardiac stimulants, and above all the exclusion of alkalis. In 1933, the death rate from ketoacidosis in Boston was only 5%, however elsewhere in North America and Europe it averaged 30% and could possibly be as high as 75%. An important advance in administration was the acceptance of relatively low-dose insulin substitute, following the example of Ruth Menzel and colleagues in Karlsburg, Germany [90]. Another step forward was the recognition by Jacob Holler in 1946 of the danger of hypokalemia [92]. Delivery of take care of folks with diabetes From the earliest days of insulin injection and urine testing, it was obvious that individuals with diabetes wanted knowledge and practical expertise to handle their disease successfully. Lip-service was typically paid to the significance of diabetes training, however most sufferers were badly informed. In 1952, Samuel Beaser (1910� 2005) questioned 128 sufferers attending the Boston Diabetes Fair, and found that "all were distinctly poor in knowledge of their disease" [ninety five]; he felt that responsibility lay with both docs and directors. Further studies during the 1960s by Donnell Etzwiler (1927�2003) in Minneapolis showed that many docs and nurses were additionally ignorant about managing diabetes. Since the Diabetic pregnancy As late as 1950, the outcome of pregnancy in girls with diabetes was nonetheless very poor in most units, with perinatal fetal losses of forty five�65%, some 10 times greater than within the basic population. Exceptions to this miserable rule were the units run by Priscilla White on the Joslin Clinic in Boston, who had published wonderful results as early as 1935 [93], and by J�rgen Pedersen in Copenhagen (Figure 1. Pedersen identified the common options underpinning success pretty much as good diabetic management and care (a) (b) Figure 1. Roma by courtesy of Manuel Machado S� Marques and the Associa��o Protectura das Diab�ticos de Portugal. These organizations are devoted to the practice of diabetes care in addition to the fundamental and clinical science of the disease, and have been useful in coordinating remedy targets and methods at international degree; an important example was the St. Pharmaceutice Rationalis; sive, Diatriba de Medicamentorum Operationibus in Humano Corpore [2 components in 1 vol]. An Account of Two Cases of the Diabetes Mellitus, With Remarks as They Arose During the Progress of the Cure. Charles-�douard Brown-S�quard: double hyphenated neurologist and forgotten father of endocrinology. Haemorrhagic retinitis in a patient with diabetes, varicose swellings on a retinal vein in the proper eye. The Treatment of Diabetes Mellitus: with Observations Based upon One Thousand Cases. Diabetes mellitus: its differentiation into insulinsensitive and insulin-insensitive types. Glucose clamp technique: a way for quantifying insulin secretion and resistance. On the relation of persistent interstitial pancreatitis to the islands of Langerhans and to diabetes mellitus. Islet-cell antibodies in diabetes mellitus with autoimmune polyendocrine deficiencies. Cyclosporin will increase the rate and length of remissions in insulindependent diabetes of current onset: results of a multicentre doubleblind trial. A re-evaluation of diabetic glomerulosclerosis 50 years after the discovery of insulin. Localization of glucagon within the A-cells within the pancreatic islet by immunofluorescence. The biosynthesis of insulin and probable precursor of insulin by a human islet cell adenoma. Insulin receptors within the liver: specific binding of [125I] insulin of the plasma membrane and its relation to insulin bioactivity. Affinity chromatography and purification of the insulin receptor of liver cell membrane. Human insulin receptor and its relationship to the tyrosine kinase household of oncogenes. Expression in Escherichia coli of chemically synthesized genes from human insulin. Continuous subcutaneous insulin infusion: an approach to reaching normoglycaemia. �ber synthetisch dargestellte K�rper mit insulinartiger Wirkung auf den normalen und den diabetischen Organismus. A study of the effects of hypoglycemic brokers on vascular issues in sufferers with grownup onset diabetes. The effect of intensive remedy of diabetes on the development and progression of long-term issues in insulin-dependent diabetes mellitus. Long-term antihypertensive remedy inhibiting progression of diabetic nephropathy. Foetal mortality in pregnant diabetics: strict management of diabetes with conservative obstetric administration. Toronto: McClelland and Stewart, 1982; and Edinburgh: Paul Harris Publishing, 1983. The hypoglycaemic sulphonamides: historical past and improvement of the issue from 1942 to 1955. In the symptomatic individual a single irregular value, either casual or fasting, is usually sufficient to verify the prognosis. This is prone to become more widespread Introduction Diabetes mellitus is a disease of antiquity (see Chapter 1). A remedy was described within the Ebers papyrus and as long ago as 600 bc two major types were distinguished. Perhaps the most well-known description was by Arateus the Cappadocian who talked of the melting down of flesh into urine and of the end being speedy.
Best diamox 250mg
These brokers, as well as barbiturates and benzodiazepines, are lipid-soluble and are thought to dissolve in the cell membranes (in direct relation to the diploma of their lipid solubility). With continued ingestion of alcohol, the neuronal membranes ostensibly "rigidify" and turn out to be immune to the fluidizing impact of alcohol (Chin and Goldstein; Harris et al). It is unlikely, however, that these adjustments in the physical properties of cell membranes are in themselves enough to alter cell perform. Probably of greater importance are the effects of alcohol on membrane receptor techniques that regulate ion channels, significantly the chloride and calcium channels. There can be proof that alcohol selectively potentiates serotonin receptor-ion currents, and the exercise of this receptor has been implicated in alcohol- and drug-looking for habits and addiction. The impact of chronic administration of alcohol is to enhance the number of neuronal calcium channels in the cell membrane. Moreover, calcium channel blockers, given throughout chronic administration, stop each the increase in neuronal calcium channels and the event of tolerance to alcohol (Dolin and Little). The significance of these findings has been demonstrated by Little and colleagues, who confirmed that calcium channel blockers, given to chronically intoxicated animals after withdrawal, stop withdrawal convulsions. The molecular mechanisms concerned in the genesis of alcohol intoxication and tolerance are obviously far more advanced than the foregoing remarks would point out (see evaluations by Charness and by Samson and Harris). A unified idea of the function of neurotransmitters and their receptors and modulators in the production of alcohol intoxication and tolerance has but to emerge. The part played by internal mobile messengers, which have attracted much attention in the subject of addiction, can be currently underneath investigation. Some of the early toxic results of alcohol, corresponding to garrulousness, aggressiveness, excessive exercise, and increased electrical excitability of the cerebral cortex- all of them suggestive of cerebral stimulation- are thought to be as a result of the inhibition of certain subcortical constructions (presumably the excessive brainstem reticular formation) that ordinarily modulate cerebrocortical exercise. Similarly, the initial hyperactivity of tendon reflexes could represent a transitory escape of spinal motor neurons from larger inhibitory centers. With increasing quantities of alcohol, however, the depressant action includes the cortical as well as other brainstem and spinal neurons. All manner of motor functions- whether the easy upkeep of a standing posture, the management of speech and eye movements, or extremely organized and sophisticated motor expertise- are adversely affected by alcohol. Alcohol additionally impairs the efficiency of psychological perform by interfering with the speed of perception and the power to persist in psychological processing. Facility in forming associations, whether of words or of figures, and the power to focus, maintain attention, and focus are decreased. The topic is less versatile in directing thought alongside new lines appropriate to the problem at hand. Finally, alcohol impairs the colleges of judgment and discrimination and, all in all, the power to assume and purpose clearly. A scale relating varied levels of functional impairment to blood alcohol ranges in nonhabituated individuals was constructed many years in the past by Miles. At a blood alcohol level of 30 mg/dL, a light euphoria was detectable, and at 50 mg/dL, a light incoordination. At one hundred mg/dL, ataxia was apparent; at 200 mg/dL, there was confusion and a decreased level of psychological exercise; at 300 mg/dL, the themes have been stuporous; and a level of 400 mg/dL- accompanied by deep anesthesia- was doubtlessly fatal. These figures are legitimate supplied that the alcohol content in the blood rises steadily over a 2-h interval. It is widespread data that a habituated person can drink extra and present fewer results than the reasonable drinker or abstainer. This phenomenon accounts for the surprisingly massive quantities of alcohol that the chronic drinker can devour without displaying vital signs of drunkenness. This aspect of tolerance should always be thought-about in judging the importance of a single estimation of the blood alcohol focus as an index of functional capability. The mechanisms that underlie tolerance and addiction are simply starting to be understood. There is little proof that an enhanced rate of alcohol metabolism can adequately account for the diploma of tolerance noticed in alcoholics. The factor widespread to all of them, after all, is the abuse of alcohol, but the mechanism by which alcohol produces its results varies broadly from one group of disorders to another and in lots of circumstances, the important drawback is certainly one of dietary deficiency as discussed in the previous chapter. Traumatic mind lesions consequent to intoxication- subdural hematoma, cerebral contusion, and so on. Now the term is mostly used to designate an outburst of blind fury with assaultive and harmful habits. The attack terminates with deep sleep, which happens spontaneously or in response to parenteral sedation; on awakening, the patient has no reminiscence of the episode. Lesser levels are additionally known whereby the patient, after a number of drinks, repeatedly commits gross social indiscretions. Unlike the usual types of alcohol intoxication and withdrawal, the atypical kind has not been produced in experimental topics, and the analysis relies upon upon the aforementioned arbitrary criteria. However, an analogy could also be drawn between pathologic intoxication and the paradoxical response that sometimes follows the administration of barbiturates or other sedative medication. The major disorders to be distinguished from pathologic intoxication are temporal lobe seizures that sometimes take the form of outbursts of rage and violence and the explosive episodes of violence that characterize the habits of certain sociopaths. The analysis in these circumstances could also be tough and is dependent upon eliciting the other manifestations of temporal lobe epilepsy or sociopathy. Alcoholic "Blackouts" In the language of the alcoholic, the term blackout refers to an interval of time, throughout a interval of extreme intoxication, for which the patient, when sober, has no reminiscence- despite the fact that the state of consciousness, as noticed by others, was not grossly altered throughout that interval. However, a systematic evaluation of psychological perform in the course of the amnesic interval has usually not been made. Blackouts could occur at any time in the midst of alcoholism, even in the course of the first consuming expertise, and they definitely have occurred in individuals who never grew to become alcoholic. Alcoholic Stupor and Coma As has been indicated, the symptoms of alcoholic intoxication are the results of the depressant action of alcohol on cerebral and spinal neurons. In this respect alcohol acts on nerve cells in a fashion akin to the overall anesthetics. Unlike the latter, however, the margin between the dose of alcohol that produces surgical anesthesia and that which dangerously depresses respiration is a narrow one, a fact that provides a component of urgency to the analysis and therapy of alcoholic coma. One should even be alert to the possibility that barbiturates or other sedative- Alcohol Intoxication the usual manifestations of alcohol intoxication are so commonplace that they require little elaboration. They encompass varying levels of exhilaration and excitement, lack of restraint, irregularity of habits, loquacity and slurred speech, incoordination of movement and gait, irritability, drowsiness, and, in advanced circumstances, stupor and coma. There are a number of sophisticated forms of alcohol intoxication, which are thought-about under. Pathologic Intoxication Despite what has been stated earlier, on uncommon events, alcohol has an solely excitatory rather than a sedative impact. This response has been referred to in the past as pathologic, or sophisticated, intoxication and as acute alcoholic paranoid state. Since all types of intoxication are pathologic, atypical intoxication or idiosyncratic alcohol intoxication are extra appropriate designations. Treatment of Severe Alcohol Intoxication Coma as a result of alcohol intoxication represents a medical emergency. The major object of therapy is to stop respiratory melancholy and its problems as described in Chap. The previously favored administration of fructose or of insulin and glucose for this objective is of little worth. The use of hemodialysis ought to be thought-about in comatose sufferers with extraordinarily excessive blood alcohol concentrations (500 mg/dL), significantly if accompanied by acidosis, and in those who have concurrently ingested methanol or ethylene glycol or another dialyzable drug. Pathologic intoxication could require the use of restraints and the parenteral administration of diazepam (5 to 10 mg) or haloperidol (2 to 5 mg), repeated once after 30 to forty min if essential. Methyl, Amyl, and Isopropyl Alcohols and Ethylene Glycol Poisoning with alcohols aside from ethyl alcohol is a comparatively uncommon but catastrophic incidence. Amyl alcohol (fusel oil) and isopropyl alcohol are used as industrial solvents and in the manufacture of varnishes, lacquers, and pharmaceuticals; as well as, isopropyl alcohol is readily available as a rubbing alcohol. Intoxication could follow the ingestion of these alcohols or inhalation of their vapors. Methyl alcohol (methanol, wooden alcohol) is a element of antifreeze and many combustibles and is used in the manufacture of formaldehyde, as an industrial solvent, and as an adulterant of alcoholic beverages, the latter being the commonest supply of methyl alcohol intoxication. Many of the toxic results are like those of ethyl alcohol, but as well as extreme methyl alcohol poisoning could produce critical levels of acidosis (with an anion gap). Survivors could also be left blind or, less typically, with putamenal necrosis and dystonia or Parkinson illness (McLean et al). The most necessary aspect of therapy is the intravenous administration of huge quantities of sodium bicarbonate to reverse acidosis. Hemodialysis and 4-methylpyrazole (see later) could also be useful adjuncts due to the gradual rate of oxidation of methanol.
References:
- http://www.okdhs.org/OKDHS%20Publication%20Library/S11034.pdf
- https://health.baltimorecity.gov/sites/default/files/health/attachments/Baltimore%20City%20CHA%20-%20Final%209.20.17.pdf
- https://deepblue.lib.umich.edu/bitstream/handle/2027.42/75015/j.1540-8167.1993.tb01227.x.pdf;sequence=1
- http://focusontoxpath.com/articles/2/Malarkey-Maronpot-Carcinogenesis-2005.pdf