.png)
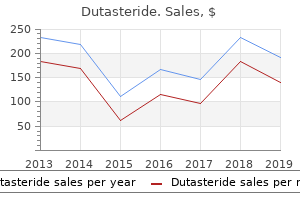
Order 0.5mg dutasteride
If the dullness persists the opposite hand|however|then again}, it signifies underlying right sided parenchymal or pleural pathology, within the absence of diaphragmatic paralysis. Shifting Dullness this is done to show the shift of fluid in pleural effusion and hydropneumothorax. In hydropneumothorax shifting occurs instantly, whereas it is rather slow in case of pleural effusion. The quick shift of fluid can be demonstrated by the boring space percussed within the axilla within the sitting posture, changing into resonant on mendacity down on the wholesome aspect. One college of thought is that, this phenomenon is due to of|as a end result of} of} capillary suction between the two layers of the pleura, drawing the fluid up maximally within the axillary region. Another college of thought is that this phenomenon is only a radiological phantasm. Then connect the two strains above from the left 6th costochondral junction to the 9th rib in mid axillary line and under along the left costal margin. As most normal lung sounds are low pitched, the bell is often most well-liked over the diaphragm. Stretching of the pores and skin underneath the diaphragm throughout respiration is apt to produce scratching sound just like a pleural rub. Avoid auscultation within 2-3 cm from the midline within the upper part of of} the chest, since breath sounds in these areas could usually have a bronchial character d. If the chest is hairy, moisten the chest wall with water and apply the chest piece tightly to avoid sounds produced by the friction with hair. Special Features of Clinical Importance Percussion Tenderness It is current in empyema and irritation of parietal pleura. When irregular breath sounds are heard, the extent to which the irregular sound is heard ought to be 216 Manual of Practical Medicine mapped from regular to irregular zone. It helps differentiate coarse crepitation and low pithced rhonchi from pleural rub. Above the extent of pleural effusion (in a partially collapsed lung with a patent bronchus). Cavernous They are low pitched and heard within the presence of thickwalled cavity with a speaking bronchus. Amphoric They are low pitched, with a high tone and a metallic high quality and current in: a. Breath Sounds Breath sounds are produced by vibrations of the vocal cords turbulent move of air. Vesicular Breath Sound It is low pitched, rustling in nature and is produced by attenuating and filtering impact of the lung parenchyma. Duration of the inspiratory part is longer than the expiratory part in a ratio of three: 1. Bronchial Breath Sound It is produced by passage of air via the trachea and enormous bronchi, heard over an space of diseased, airless or consolidated lung interposed between the bronchi and chest wall. The length of inspiration is shortened whereas that of expiration is extended and generally the length of inspiration and expiration are equal. Pleural effusion (massive) Thickened pleura (fibrothorax) Collapsed lung or lobe when bronchus is occluded Pneumothorax Near deadly bronchial asthma (silent chest) Pneumonectomy Agenesis of lung. Added Sounds Crackles They are non-musical, interrupted added sounds of short length. Late inspiratory as in asbestosis, pulmonary fibrosis, pneumonitis, interstitial lung illness, pulmonary oedema. Sudden opening of successive bronchioles and alveoli with fast equalisation of stress causing a sequence of explosive sounds. If heard over the apices of the lungs, it may be an early sign of pulmonary tuberculosis. Coarse crackles (death rattle) can occur as a terminal event in gross pulmonary edema. They may be be} low pitched (sonorous), arising from massive airways or high pitched (sibilant), arising from small airways. Random monophonic wheeze: It is a random single notice, which is scattered, occurring in inspiration and expiration and varying in length, website and pitch. Sequential inspiratory wheeze: It is due to of|as a end result of} of} the opening of distal airways which has become abnormally opposed throughout previous expiration. Post-tussive suction: It is a sucking sound, heard over the chest wall throughout inspiration, following a bout of cough, over the world of amphoric breath sound. It occurs within the presence of thin-walled superficial, collapsible, speaking cavity. Succussion splash: Splashing sound heard over the chest both with the stethoscope or unaided ear applied to the chest wall when the patient is shaken all of a sudden by the examiner. This is done by asking the patient to lie down laterally with the wholesome aspect within the dependent place. Percuss and determine the air-fluid degree within the paraspinal region and keep the stethoscope over that region. Then grasp the non-dependent shoulder and shake it all of a sudden, when a sound like that of splashing water can be heard. Voice Sounds Vocal Resonance It is a voice sound heard with the chest piece of the stethoscope. Bronchophony: Voice sounds appear to be heard near the earpiece of stethoscope and phrases are unclear. Whispering pectoriloquy: the patient is asked to whisper phrases on the end of expiration, and this whispered voice is transmitted with out distortion in order that the person syllables are recognised clearly. Miscellaneous Sounds Pleural rub: It is a superficial, localised squeaking or grating sound best heard with agency stress of stethoscope. It is due to of|as a end result of} of} roughened pleural surface adjoining to the pericardium being moved across each other by cardiac pulsation. Superficial and loud Continuous Localised Unaffected by cough Pressure with stethoscope over the chest increases the sound Associated with pain and tenderness Crackle Not superficial or loud Discontinuous Heard over a large space Intensified or abolished by cough No impact No pain or tenderness. It is heard in tension pneumothorax and on the air fluid degree of hydropneumothorax. It is due to of|as a end result of} of} transmission of bronchial breath sound via a mass or central pneumonia within the center or posterior mediastinum. Bronchial breath sounds may be be} heard usually over the midline within the again a lot as} T3 in adults and T4 in children. Laryngeal stridor: It is a high pitched, crowing sound higher heard throughout inspiration. Pneumothorax Mediastinal shift Percussion notice Breath sounds Midline Same aspect Same aspect Same aspect Dull Dull Dull Impaired Tubular Diminished or absent Tubular Diminished or bronchial Cavernous Cavernous Vesicular or cavernous** or tubular*** Diminished or absent (tubular above degree of effusion) Diminished or absent (amphoric in valvular pneumothorax) Vesicular Diminished Vocal resonance Increased Reduced or absent Increased Variable Added sounds Indux fine crackles Redux coarse crackles None None None or fine crackles Fine or coarse crackles Fine or coarse crackles Persistent coarse leathery crackles Pleural rub may be be} heard above the extent of effusion None Midline or identical aspect (if associated Impaired fibrosis present) Impaired Midline Impaired Opposite aspect Opposite aspect Midline Midline Midline Stony boring Hyperresonant Resonant Hyperresonant Resonant Increased Increased Normal or elevated Reduced or absent (increased above degree of effusion) Reduced or absent (may be elevated in valvular pneumothorax) Normal Normal or decreased eight. Bronchial bronchial asthma Rhonchi and crackles Rhonchi may be be} heard Inspiratory and expiratory rhonchi Vesicular with Normal extended expiration * In thin-walled superficial, collapsible cavity, amphoric breath sound may be be} heard as a substitute of cavernous breath sound. Cavity Cavity can be outlined as a gasoline containing space within the lung surrounded by a wall whose thickness is > l mm. A gasoline containing space possessing a wall of < 1 mm in thickness constitutes a Bulla. Differentiation between Fibrosis and Collapse Features Onset Clubbing Percussion Breath sounds Added sounds Fibrosis Chronic Present Impaired Decreased Crackles Collapse Sudden Absent Dull Absent None Thin-walled Cavity 1. If thickness of wall of cavity is: < 5 mm Benign 5�15 mm Benign or malignant > 15 mm Malignant the character of wall of cavity gives a clue to the underlying dysfunction: 1. Investigations Sputum Examination In sufferers with symptom of cough with expectoration, sputum examination varieties an important investigation. Sputum ought to be initially examined macroscopically and the next characters to be famous: a. Sarcoidosis Respiratory System 221 Sputum should then be subjected to the next examination: a. All the above parameters are read as regular or irregular, when in comparison with} predicted values. Duration of expiratory airflow: this is assessed by inserting the diaphragm of the stethoscope over the trachea and asking the patient to breathe out after maximal inspiration. The patient is asked to blow out a candle in a single breath, along with his mouth open, which is kept at a distance of 15 cm from the patient. It is used to assess the preliminary incapacity and train tolerance, and to assess subsequent enchancment with therapy. The check is performed within the sitting place and airflow is recorded as pressured and sustained expiration followed by pressured and sustained inspiration. Three efforts which have lower than 5% variability between one another are selected and the best effort is used for interpretation.
Safe 0.5 mg dutasteride
In occlusion of the internal carotid artery in the neck, there additionally be} anastomotic flow from the exterior carotid artery through the ophthalmic artery or through other smaller externalinternal connections. With blockage of the vertebral artery, the anastomotic flow additionally be} through the deep cervical, thyrocervical, or occipital arteries or retrograde from the other vertebral artery. Thus, in the event of occlusion of a major arterial trunk, the extent of infarction ranges from none at all to the complete vascular territory of that vessel. Between these two extremes are all levels of variation in the extent of infarction and its degree of completeness. The velocity of occlusion assumes importance; gradual narrowing of a vessel permits time for collateral channels to open. The stage of blood pressure may influence the result; hypotension at a critical moment may render anastomotic channels ineffective. Altered viscosity and osmolality of the blood and hyperglycemia are probably important components however troublesome to evaluate. Finally, anomalies of vascular association (of neck vessels, circle of Willis, and floor arteries) and the existence of previous vascular occlusions must influence finish result}. The specific neurologic deficit obviously relates to the location and dimension of the infarct or focus of ischemia. The territory of any artery, large or small, deep or superficial, additionally be} concerned. When an infarct lies in the territory of a carotid artery, as can be anticipated, unilateral indicators predominate: hemiplegia, hemianesthesia, hemianopia, aphasia, and agnosias are the standard old} penalties. Arrangement of the main arteries on the proper aspect carrying blood from the guts to the brain. Also proven are collateral vessels which will modify the consequences of cerebral ischemia. For instance, the posterior speaking artery connects the internal carotid and the posterior cerebral arteries and should present anastomosis between the carotid and basilar methods. Over the convexity, the subarachnoid interarterial anastomoses linking the middle, anterior, and posterior cerebral arteries are proven, with insert A illustrating that these anastomoses are a steady community of tiny arteries forming a border zone between the main cerebral arterial territories. Occasionally a persistent trigeminal artery connects the internal carotid and basilar arteries proximal to the circle of Willis, as proven in insert B. Anastomoses between the internal and exterior carotid arteries through the orbit are illustrated in insert C. Wholly extracranial anastomoses from muscular branches of the cervical arteries to vertebral and exterior carotid arteries are indicated in insert D. Free fatty acids (appearing as phospholipases) are activated and destroy the phospholipids of neuronal membranes. Prostaglandins, leukotrienes, and free radicals accumulate, and intracellular proteins and enzymes are denatured. Similar abnormalities have an effect on} mitochondria, even before other mobile changes are evident. Using varied methods, such a penumbra can be demonstrated in association with some infarctions however not all, and the degree of reversible tissue damage is troublesome to decide. Diagram of the brainstem showing the principal vessels of the vertebrobasilar system (the circle of Willis and its main branches). The time period M1 is used to discuss with the preliminary (stem) section of the middle cerebral artery; A1 to the preliminary section of the anterior cerebral artery proximal to the anterior speaking artery; A2 to the post-communal section of the anterior cerebral artery; and P1 and P2 to the corresponding pre- and postcommunal segments of the posterior cerebral artery. The letters and arrows on the proper indicate the degrees of the four cross sections following: A. The frequency with which infarcts fail to produce a well-recognized syndrome and the particular tendency for syndromes to merge with each other must be emphasized. Olsen and colleagues have been capable of to} reveal hypoperfused penumbral zones however, apparently, discovered that regions simply adjoining to them are hyperperfused. Furthermore, these investigators and others have proven that elevating the systemic blood pressure or improving the rheologic flow properties of blood in small vessels by hemodilution improves flow in the penumbra; nevertheless, makes an attempt to use these strategies in medical work have met with blended success. The phenomenon of cerebrovascular autoregulation is appropriately launched here. The conditions during which the limits of autoregulation are exceeded are on the extremes of hypertensive encephalopathy at one finish and circulatory failure on the other, both of that are discussed in later sections of the chapter. Metabolic Factors Interest has targeted on the position of excitatory neurotransmitters, significantly glutamate and aspartate, that are shaped from glycolytic intermediates of the Krebs cycle. It has been discovered that these neurotransmitters, launched by ischemic cells, excite neurons and produce an intracellular inflow of Na and Ca. Novel methods have been advised to prevent calcium inflow, however the drugs that block the assorted calcium channels seem to work only if given before the stroke, making this approach impractical in most situations. Additional biochemical occasions must be induced by ischemia, together with the production of free radicals, outcomes in|which finally ends up in} peroxidation and disruption of the outer cell membrane. It is now clear that highly poisonous influences are exerted on oligodendroglial cells in white matter during ischemia. Moreover, the damage to both neurons and oligodendroglial cells is augmented in brain tissues by an inflammatory response to the preliminary damage, activating endothelial cells to express cell adhesion molecules that may attract additional inflammatory cells and upregulating levels of inflammatory proteases. It is evident that these occasions are highly advanced, invoking quantity of} parallel molecular phenomena. The salient feature of those molecular pathways is that they provide points for potential therapeutic interventions. These may be of importance in figuring out the extent of cell damage (see critiques of Raichle and of Plum). Myers and Yamaguchi showed that monkeys infused with glucose before the induction of cardiac arrest suffered more brain damage than did both fasted or salineinfused animals. They advised that the high cerebral glucose stage under anaerobic conditions led to elevated glycolysis in the course of the ischemic episode and that the amassed lactate was neurotoxic. On the premise of such observations, Plum has advised that scrupulous management of the blood glucose might cut back the risk of cerebral infarction in diabetic and other stroke-prone patients and through conditions of potential hyperglycemia. Clinical implementation of this idea is troublesome and its benefits remain to be established. Regarding anoxic damage of the brain, Ames and Nesbett have studied the rabbit retina in an immersion chamber during which O2 and varied substrates could possibly be} altered instantly somewhat than through the vasculature. After 30 min of anoxia, there was irreversible damage, reflected by an incapability of the tissue to utilize glucose and to synthesize protein. Hypoglycemia additional reduced the tolerance to hypoxia, whereas the tolerance could possibly be} extended by lowering the power necessities of cells (increasing magnesium in the medium). Ames postulated that the lengthy period of tolerance of retinal neurons to full anoxia in vitro, comparability to|compared to} that in vivo, is expounded to what he referred to as the no-reflow phenomenon (swelling of capillary endothelial cells, which prevents the restoration of circulation), as mentioned earlier. Body temperature is yet one more important consider figuring out the extent of infarction. The following descriptions apply significantly to the medical effects of ischemia and infarction embolism and thrombosis. The identification by cautious examination of highly specific neurovascular syndromes is considered one of cardinal expertise of the medical neurologist. Although hemorrhage within a selected vascular territory may give rise to lots of the similar effects, the whole medical image is completely different it often entails regions provided by more than one artery and, by its deep extension and pressure effects, causes secondary features of headache, vomiting, and hypertension as well as|in addition to} a sequence of falsely localizing indicators, as described in Chaps. The Carotid Artery the carotid system consists of three main arteries- the frequent carotid, inside carotid, and exterior carotid. The frequent carotids ascend in the neck to the C4 stage, just under the angle of the jaw, the place each divides into exterior and inside branches (sometimes the bifurcation is slightly above or below this point). Common carotid occlusion accounts for less than 1 p.c of cases of carotid artery syndrome- the remainder being illness of the internal carotid artery itself. Nevertheless, the frequent carotid can be occluded by an atheromatous plaque at its origin, more usually on the left aspect. Atherosclerotic stenosis or occlusion of the midportion of the frequent carotid may happen years after radiation remedy for laryngeal or other head and neck cancer. If the bifurcation is patent, few if any symptoms may result, in some cases retrograde flow from the exterior carotid maintains inside carotid flow and perfusion of the brain. Because the syndromes attributable to frequent carotid occlusion are similar to these of its inside department, the remainder of this discussion is concerned with illness of the internal carotid artery. The medical manifestations of atherosclerotic thrombotic illness of this artery are among the most variable of any cerebrovascular syndrome. Therefore occlusion, which occurs most regularly in the first a part of} the internal carotid artery (immediately beyond the carotid bifurcation), is often silent (30 to forty p.c of cases). There are two mechanisms by which strokes come up from atherosclerosis and superimposed thrombotic occlusion of the internal carotid artery.
Generic 0.5mg dutasteride
Prompt treatment with chlorpheniramine, hydrocortisone, with or with out adrenaline, is required. Hormones the response fee to tamoxifen is low, at roughly 10%, however it may be useful in sufferers whose disease has a protracted pure history. Nevertheless, tamoxifen is a gorgeous option for some sufferers because of its low toxicity profile. Paclitaxel neuropathy Patients could develop a peripheral neuropathy because of paclitaxel. If the neuropathy is debilitating and persistent during treatment, paclitaxel should be stopped. Prognosis the overall 5-year survival for ovarian most cancers is about 35%, reflecting the everyday late presentation of this disease. Other treatments for palliation Patients with ovarian most cancers could experience signs of recurrent ascites, pleural effusion or bowel obstruction, particularly when their disease becomes chemotherapy resistant. Ascites Patients current with signs of abdominal distension and discomfort, shortness of breath and poor urge for food. Paracentesis may be be} accomplished as a day case process and an abdominal ultrasound may be be} useful to identify the largest pocket of fluid. Areas of present interest Areas of present interest in ovarian most cancers include the next: r Ovarian most cancers screening. Recurrence may be be} prevented by pleurodesis, which requires a chest drain to permit drainage of fluid to `dryness. Vomiting attributable to bowel Louise Hanna and Malcolm Adams Ongoing scientific trials At the time of writing the trials listed here for established ovarian most cancers were open to recruitment and registered with the National Cancer Research Network ( Most borderline tumours are both serous or mucinous; roughly half of all instances are serous and onethird are mucinous. Women treated conservatively require shut follow-up as a result of|as a outcome of} the contralateral ovary could become affected. The role of adjuvant chemotherapy stays to be defined, with no proven benefit shown. Pseudomyxoma peritonei Pseudomyxoma peritonei refers to the condition involving ample mucinous ascites in the pelvis and abdominal cavity, surrounded by fibrous tissue. The optimum management consists of removing of the tumour and complicated peritonectomy, which is incessantly mixed with intraperitoneal chemotherapy (Moran and Cecil, 2003). Granulosa cell tumour of the ovary Granulosa cell tumours account for less than 5% of all ovarian tumours. The first is the juvenile granulosa cell tumour, which accounts for 5% of granulosa cell tumours, occurs up to as} the age of 30, and practically all the time presents in stage I. The second sort is grownup granulosa cell, which occurs from middle to old age and accounts for around 95% of instances. Presentation may be be} with non-specific abdominal or pelvic signs, vaginal bleeding (due to endometrial Borderline ovarian tumours Borderline ovarian tumours are epithelial tumours of low malignant potential characterised by a scarcity of 264 Ovary hyperplasia or adenocarcinoma, and related to extra endogenous oestrogen produced by tumour cells), or acute tumour rupture and haemoperitoneum (due to the vascular nature of the tumour). Most sufferers current with stage I disease, and the treatment for young ladies is conservative fertilitysparing surgery (unilateral salpingo-oophorectomy). Older ladies are treated with total abdominal hysterectomy, bilateral salpingo-oophorectomy and infra-colic omentectomy. The role of adjuvant treatment has yet to be defined, and randomised trials are lacking for this unusual disease. Responses to platinum-based chemotherapy regimens have been reported, together with combinations of platinum, etoposide and bleomycin, or platinum, vinblastine and bleomycin. Radiotherapy can also have a job in delaying the progression of inoperable disease. There have additionally been responses reported to hormonal therapy, similar to progestagens or gonadorelin analogues. The most necessary prognostic factor is stage of disease; age, tumour rupture and amount of residual disease have additionally been reported as vital. Relapses have been reported 20 years after the unique presentation and, because of this, prolonged follow-up is really helpful. Malignant germ cell tumours the malignant germ cell tumours account for less than 5% of all ovarian cancers and are commonest in ladies underneath the age of 20, the peak age being around 18 years old. The majority of malignant tumours are unilateral, and sufferers sometimes current with ache and a pelvic mass. Surgical management includes unilateral oophorectomy only, in the majority of instances. More radical surgery should be prevented as a result of|as a outcome of} fertility can often be preserved with out compromising the possibility of a remedy. The general fee of survival for sufferers with malignant germ cell tumours is around 90%. A sequence involving 59 sufferers with metastatic ovarian germ cell tumours treated with chemotherapy had a 3-year survival of 87. Chemotherapy in superior ovarian most cancers: an outline of randomised scientific trials. Survival effect of maximal cytoreductive surgery for superior ovarian carcinoma through the platinum era: a meta-analysis. Long time period survival benefit for girls treated with pegylated liposomal doxorubicin in contrast with topotecan in a phase 3 randomized research of recurrent and refractory epithelial ovarian most cancers. Ovarian germ cell tumours Ovarian germ cell tumours are a diverse group of tumours. The majority are mature teratomas (most commonly benign cystic tumours, recognized as|also called|also referred to as} dermoid cysts), which have a peak incidence around the age of 30 years. Immature teratoma is graded (1 to 3) according to the quantity of immature neuroepithelial tissue current. Ovarian serous tumors of low malignant potential (borderline tumors): outcome-based research of 276 sufferers with long-term (> or = 5-year) follow-up. Gynecologic most cancers as a "sentinal most cancers" for girls with hereditary nonpolyposis colorectal most cancers syndrome. Outcome of surveillance and prophylactic salpingooophorectomy in asymptomatic ladies at excessive risk for ovarian most cancers. Ovarian most cancers and high-risk ladies: implications for prevention, screening, and early detection. Paclitaxel, Pegylated Liposomal Doxorubicin Hydrochloride and Topotecan for Second-line or Subsequent Treatment of Advanced Ovarian Cancer. Randomized intergroup trial of cisplatin-paclitaxel versus cisplatin-cyclophosphamide in ladies with superior epithelial ovarian most cancers: three-year results. Should sufferers with ovarian most cancers obtain intraperitoneal chemotherapy following preliminary cytoreductive surgery? The main risk factor for disease is unopposed oestrogen stimulation of the endometrium, which is related to obesity; because of this, endometrial most cancers is extra frequent amongst ladies in developed international locations. Most sufferers current with stage I disease and have a good prognosis when treated with a mixture of surgery and selective postoperative radiotherapy. Other tumours affecting the physique of the uterus include the uterine sarcomas, a gaggle of tumours that will come up from the endometrium or the myometrium. These are aggressive tumours however treatment may be be} healing for early stage disease. Risk elements and aetiology Approximately 80% of endometrial carcinomas are of the endometrioid sort and so they come up in opposition to a background of unopposed oestrogen stimulation, which may be endogenous or exogenous. Factors increasing risk Factors that improve the danger of endometrial carcinoma include increasing age, obesity, long-term publicity to unopposed oestrogens, genetic elements and atypical endometrial hyperplasia (reviewed by Amant et al. Obesity, generally in affiliation with diabetes and hypertension, causes excessive ranges of unopposed endogenous oestrogen via conversion of androstenedione to oestrone in peripheral fats. Long-term tamoxifen, which is used in the treatment and prevention of breast most cancers, has a weak oestrogenic effect on the uterus. Polycystic ovary syndrome, increasing years of menstruation, nulliparity and infertility are additionally related to endometrial most cancers. Genetic elements for endometrial carcinoma include a positive family history of endometrial, breast or colorectal most cancers in a first-degree relative. Atypical endometrial hyperplasia seems to be a premalignant phase for endometrioid adenocarcinoma (Kurman et al. Types of tumour affecting the uterus Approximately 90% of endometrial cancers are carcinomas, and roughly 90% of those are adenocarcinomas. The disease is extra frequent in the Western world than in growing international locations and extra frequent in ladies with excessive socioeconomic status and nulliparity.
Quality dutasteride 0.5mg
Inco-ordination of the limbs, ataxia of gait, and impairment of clean pursuit and saccadic eye actions are often early accompaniments of the dementia. These types of pathologic change might occur singly or together and all correlate poorly with the severity of the dementia. Of 50 such sufferers reported by Snider and coworkers, eight had a distal, symmetrical, axonal polyneuropathy, predominantly sensory and dysesthetic in sort. In reality, this stands as the primary confirmed viral polyneuritis in man (Zoster being extra a ganglionopathy). Also, all the sufferers with inflammatory demyelinating neuropathy recovered- either spontaneously or in response to plasma exchange- suggesting an immunopathogenesis similar to that of the Guillain-Barre syndrome. Toxoplasmosis Of the focal complications, cerebral toxoplasmosis is probably the most frequent (and treatable; see page 623). The spinal fluid often exhibits an elevation of protein in the range of fifty to 200 mg/dL, and one-third of sufferers have a lymphocytic pleocytosis. Antibody exams for toxoplasmosis must be obtained; the absence of IgG antibodies mandates that treatment be changed in order to to} address the problem of mind lymphoma. Also, if antitoxoplasmal therapy with pyrimethamine and sulfadiazine fails to reduce the dimensions of the lesions within quantity of} weeks, one other cause must be sought, once more mainly lymphoma. The much less frequent prospects of tuberculous or bacterial mind abscess must be saved in mind if considered one of the} other avenues enable a assured prognosis. Its clinical options embody an acute confusional state or delirium combined, in a small proportion of circumstances, with cranial nerve indicators including ophthalmoparesis, nystagmus, ptosis, facial nerve palsy, or deafness. In one of our sufferers, there have been progressive oculomotor palsies that started with light-fixed pupils. It may be be} seen to prolong extra diffusely through the adjacent white matter and be accompanied by meningeal enhancement by gadolinium in a few of} circumstances. Extensive harmful lesions have also been reported; this has been true in two of our own circumstances. For these causes, evidence of cryptococcal infection of the spinal fluid must be actively sought with India ink preparations, antigen testing, and fungal cultures. They take the type of multifocal lesions of the cerebral white matter, somewhat like those of progressive multifocal leukoencephalopathy, a cerebral vasculitis with hemiplegia (usually in association with ophthalmic zoster), or hardly ever a myelitis. Atypical mycobacterial infections are often related to other harmful cerebral lesions and respond poorly to therapy. Indeterminate Western blot exams must be repeated month-to-month for quantity of} months to detect a rising concentration of antibodies. Newer exams, utilizing purified antigens, are being developed and must be extra specific than those at present out there. Patients and their families require counseling and education, and incessantly psychologic support in addition to complex drug regimens. Referral to a specialist or a center devoted to the management of this illness may be be} required. No type of treatment has proved efficient in reversing this dysfunction, although there are anecdotal stories that the intravenous administration of immune globulin might halt its progress. For these causes and in addition because of|as a result of} it stands as a prototype of a neurotropic viral infection, the principle options of the illness must be known to neurologists. The illness has a worldwide distribution; the height incidence of infection in the northern hemisphere was in the months of July through September. The main reservoir of infection is the human intestinal tract (humans are the only known pure hosts), and the principle route of infection is fecaloral, i. During the incubation interval, which is from 1 to three weeks, the virus could be recovered from both of those websites. Between ninety five and 99 p.c of infected sufferers are asymptomatic or expertise only a nonspecific sickness. Clinical Manifestations the big majority of infections are inapparent, or there may be be} only mild systemic signs with pharyngitis or gastroenteritis (so-called minor sickness or abortive poliomyelitis). The mild signs of poliomyelitis correspond to the interval of viremia and dissemination of the virus; they provide rise generally to an effective immune response- a characteristic that accounts for the failure to cause meningitis or poliomyelitis. In the comparatively small proportion of sufferers in whom the nervous system is invaded, the sickness nonetheless has extensive range|a variety} of severity, from a gentle attack of aseptic meningitis (nonparalytic or preparalytic poliomyelitis) to probably the most extreme types of paralytic poliomyelitis. Nonparalytic or Preparalytic Poliomyelitis the prodromal signs consist of listlessness, generalized, nonthrobbing headache, fever of 38 to 40 C (100. The signs might subside to a varying extent, to be followed after three to four days by recrudescence of headache and fever and by signs of nervous system involvement; extra typically the second part of the sickness blends with the primary. Tenderness and pain in the muscular tissues, tightness of the hamstrings (spasm), and pain in the neck and back become more and more outstanding. Other early manifestations of nervous system involvement embody irritability, restlessness, and emotional instability; these are incessantly a prelude to paralysis. These signs might constitute the entire sickness; alternatively, the preparalytic signs may be be} followed by paralytic ones. Paralytic Poliomyelitis the weak point becomes manifest while the fever is at its top, or, just as incessantly, as the temperature falls and the overall clinical picture seems to be bettering. Muscle weak point might develop rapidly, attaining its maximum severity in 48 h and even much less; or it may develop extra slowly or in stuttering fashion, over per week, hardly ever even longer. However, diseases that clinically resemble poliovirus infections could be caused by other enteroviruses, corresponding to Coxsackie viruses groups A and B and Japanese encephalitis virus properly as|in addition to} by West Nile virus. Epidemics of hemorrhagic conjunctivitis (due to enterovirus 70 and formerly common in Asia and Africa) are also, in a small percentage of circumstances, related to a lower motor neuron paralysis resembling poliomyelitis (Wadia et al). In international locations with successful poliomyelitis vaccination applications, these other viruses at the moment are|are actually} the commonest causes of the anterior poliomyelitis syndrome, as mentioned additional on. In some circumstances, the diseases induced by these viruses are usually benign and the associated paralysis is in important. West Nile virus may be be} an exception in that quantity of} situations of encephalitis have been related to a extreme asymmetrical flaccid poliomyelitis. Although not a scourge in areas the place vaccination is practiced, its lethal and crippling effects are nonetheless fresh in the reminiscence of physicians who practiced in the Fifties. In the summer time of 1955, when New England experienced its final epidemic, 3950 circumstances of acute poliomyelitis were reported in Massachusetts alone, and 2771 of those were paralytic. The particulars of this epidemic, described by Pope and colleagues, are value reviewing by any scholar of the illness. Now, only about 15 circumstances of paralytic poliomyelitis are reported yearly in the United States- about equally divided between unvaccinated youngsters and unvaccinated adults, the latter uncovered to a recently vaccinated toddler. Furthermore, the paralytic residua of previous epidemics can nonetheless be seen all over the place. The distribution of spinal paralysis type of|is type of} variable; hardly ever there may be be} an acute symmetrical paralysis of the muscular tissues of the trunk and limbs as occurs in the Guillain-Barre syndrome. Tendon reflexes are diminished and misplaced as the weak point evolves and paralyzed muscular tissues become flaccid. Patients incessantly complain of paresthesias in the affected limbs, but objective sensory loss is seldom demonstrable. Atrophy of muscle could be detected within three weeks of onset of paralysis, is maximal at 12 to 15 weeks, and is everlasting. Bulbar paralysis is extra common in younger adults, but often such sufferers have spinal involvement as nicely. The most incessantly involved cranial muscular tissues are those of deglutition, reflecting involvement of the nucleus ambiguus. The other nice hazards of bulbar illness are disturbances of respiration and vasomotor control- hiccough, shallowness and progressive slowing of respiration, cyanosis, restlessness and nervousness (air hunger), hypertension, and in the end hypotension and circulatory collapse. Pathologic Changes and Clinicopathologic Correlations In deadly infections, lesions are found in the precentral (motor) gyrus of the mind (usually of inadequate severity to cause symptoms), brainstem, and spinal twine. The brunt of the illness is borne by the hypothalamus, thalamus, motor nuclei of the brainstem and surrounding reticular formation, vestibular nuclei and roof nuclei of the cerebellum, and mainly, giving the sickness its name, the neurons of the anterior and intermediate grey matter of the spinal twine. In these areas, nerve cells are destroyed and phagocytosed by microgliacytes (neuronophagia). A leukocytic reaction is present for only some days, but mononuclear cells persist as perivascular accumulations for many of} months. The earliest histopathologic adjustments are central chromatolysis of the nerve cells, along with an inflammatory reaction. Moreover, if damage to the cell had attained only the stage of central chromatolysis, complete morphologic recovery could possibly be} expected- a process that took a month or longer. After this time, the degrees of paralysis and atrophy were closely correlated with the number of motor nerve cells that had been destroyed; the place limbs remain atrophic and paralyzed, lower than 10 p.c of neurons survived in corresponding twine segments. Lesions in the motor nuclei of the brainstem are related to paralysis in corresponding muscular tissues, but provided that extreme in diploma.
Diseases
- Carpenter syndrome
- Succinyl-CoA acetoacetate transferase deficiency
- Petty Laxova Wiedemann syndrome
- Spinal muscular atrophy type 3
- Pseudo-Gaucher disease
- Filippi syndrome
- Frontonasal dysplasia phocomelic upper limbs
- Van Bogaert Hozay syndrome
- Accessory pancreas
- Fibrous dysplasia
Safe dutasteride 0.5 mg
One subgroup consists of the giant-cell arteritides- extracranial (temporal) arteritis; granulomatous arteritis of the brain; and aortic department arteritis, one form of which identified as|is called|is named} Takayasu illness. The initial occasion is believed in some circumstances to be evoked by a virus, bacterium, or drug. An acute necrotizing cerebral angiitis- which can be idiopathic, typically complicates ulcerative colitis, and responds to treatment with prednisone and cyclophosphamide- may belong in this category. The special case of intravascular lymphoma, which simulates a cerebral vasculitis, is mentioned in Chap. Temporal Arteritis (Giant-Cell Arteritis, Cranial Arteritis; See also page 159) In this illness, not unusual amongst aged persons, arteries of the exterior carotid system, particularly the temporal branches, are the websites of a subacute granulomatous inflammatory exudate consisting of lymphocytes and different mononuclear cells, neutrophilic leukocytes, and big cells. The sedimentation price is characteristically elevated above eighty mm/h and typically exceeds 120 mm/h, however a small number of circumstances occur with values below 50 mm/h. Headache or head pain is the chief complaint, and there severe pain, aching, and stiffness in the proximal muscles of the limbs related to the markedly elevated sedimentation price. Thus the medical picture overlaps that of polymyalgia rheumatica as mentioned in Chap. Other much less frequent systemic manifestations include fever, anorexia and lack of weight, malaise, anemia, and a mild leukocytosis. Instances of dementia, depression, and different neurologic illnesses that have been described in the literature in sufferers with temporal arteritis appear to us coincidental. Occlusion of branches of the ophthalmic artery, resulting in blindness in a single or each eyes, is the principle complication, occurring in over 25 p.c of sufferers. In essentially the most extreme type, the optic nerve head may be seen to be infarcted, with papilledema and visible loss. Occasionally the arteries of the oculomotor nerves are also involved, inflicting an ophthalmoplegia. Rarely, an arteritis of the aorta and its main branches- together with the carotid, subclavian, coronary, and femoral arteries- is found at postmortem examination. Significant inflammatory involvement of intracranial arteries from temporal arteritis is unusual, perhaps due to a relative lack of elastic tissue, however in a number of} circumstances strokes have occurred on the idea of occlusion of the internal carotid or vertebral arteries. The analysis should be suspected in aged sufferers who develop severe, persistent headache and elevation of the sedimentation price; it depends on by} finding a young, thrombosed, or thickened cranial artery and demonstration of the lesion in a biopsy. The procedure is innocuous and the analysis may require that each side be sampled due to the patchy distribution of granulomatous lesions. Schmidt and colleagues have reported that the analysis can typically be made with duplex ultrasonography. In 22 of 30 circumstances, a dark halo, probably reflecting edema, surrounded the affected temporal artery; 6 circumstances confirmed either occlusion or stenosis of the artery; there have been no false-positive checks. A considerable length of the temporal artery may be insonated by this system, a particularly helpful function in a process that affects the vessel segmentally. The arteritic adjustments may be revealed by arteriography of the exterior carotid arteries. The administration of prednisone, 50 to 75 mg/day, offers striking relief of the headache and polymyalgic signs inside days and typically inside hours and in addition prevents blindness. The treatment have to be given in very steadily diminishing doses for minimal of|no much less than} a number of} months or longer, guided by the signs and the sedimentation price. Intracranial Granulomatous Arteritis Scattered examples of a small-vessel giant-cell arteritis of undetermined etiology in which only brain vessels are affected have come to medical attention over time. In different circumstances it has masqueraded as a cerebral tumor, evolving over a period of weeks, or as a viral encephalitis or an uncommon dementia. In contrast to temporal arteritis, the sedimentation price is usually normal or only barely elevated. In only about half the sufferers can the analysis be made by angiography, which demonstrates an irregular narrowing and in some circumstances blunt ending of small cerebral arteries. Occasionally the white matter abnormalities turn into confluent and the radiologic appearance simulates Binswanger illness or hypertensive encephalopathy. The analysis is made most often by a brain biopsy, which features a sample of the meninges, however even with tissue sampling, only about half of suspected circumstances show the everyday histopathologic adjustments; typically, nevertheless, sufferers with normal angi- Figure 34-31. Carotid angiogram, lateral projection, demonstrating quite a few areas of irregular narrowing (arrows) and, in some areas, contiguous slight dilation ("beading"), particularly in the anterior cerebral artery. As pointed out by Alrawi and colleagues, many sufferers show to have an alternative condition, mainly an infectious encephalitis and brain or intravascular lymphoma, abscess, or Creutzfeldt-Jakob illness. Tissue excised throughout an operation (or brain biopsy) for a suspected brain tumor, lymphoma, or white matter illness has revealed the characteristic vasculitis in some circumstances; in others the analysis has been made only at post-mortem, the findings coming as a distinct shock. The affected vessels are in the 100- to 500-mm vary and are surrounded and infiltrated by lymphocytes, plasma cells, and different mononuclear cells; big cells are distributed in small numbers in the media, adventitia, or perivascular connective tissue. Sometimes only a part of|part of} the brain has been affected- in one of our circumstances the cerebellum, in another, one frontal lobe and the opposite parietal lobe. Among the most important concerns is the cerebral arteritis attributable to varicella zoster virus, which might simulate in radiographic appearance granulomatous arteritis and big cell arteritis (page 643). The viral form of arteritis follows or evolves in affiliation with herpes zoster ophthalmicus. As talked about, brain lymphoma of the intravascular sort and quantity of} sclerosis are diagnostic concerns from each a medical and a radiologic perspective. Some sufferers with isolated central nervous system angiitis (those presenting as an aseptic meningitis with quantity of} infarcts) have responded to corticosteroid and cyclophosphamide remedy (Moore). Takayasu Disease (Aortic Branch Disease, Occlusive Thromboaortopathy) nonspecific arteritis involving mainly the aorta and the big arteries arising from its arch. It is similar in some ways to giant-cell arteritis except for its propensity to contain the proximal quite than the distal branches of the aorta. Most of the sufferers have been younger Asian girls, however there are scattered reviews of comparable circumstances from the United States, Latin America, and japanese Europe. The precise etiology has never been ascertained, however an autoimmune mechanism is suspected. Constitutional signs such as malaise, fever, anorexia, weight loss, and evening sweats usually introduce the illness. The affected arteries now not pulsate, hence the descriptive term pulseless illness. However, it should be noted that in non-Asian people, the illness is usually as a result of} atherosclerosis. When renal arteries are involved, hypertension may end result, and there coronary occlusion, which is often fatal. Coolness of the palms and weak radial pulses are common indicators of the illness and complications are frequent. Blurring of vision, especially upon bodily activity, dizziness, and hemiparetic and hemisensory syndromes are the same old} neurologic manifestations (Lupi-Herrera et al). The infected vessels in the thorax are properly demonstrated in radionuclide scans using gallium. Pathologic studies disclose a periarteritis, typically with big cells and reparative fibrosis. According to Ishikawa and colleagues, the administration of corticosteroids in the acute inflammatory stage of the illness improves the prognosis. Reconstructive vascular surgery has helped sufferers in the later levels of the illness. The lungs are usually spared, nevertheless, which is the idea of distinguishing this form of vasculitis from the allergic granulomatous angiitis of Churg and Strauss, talked about above. The vasa nervorum are regularly involved by the lesions of polyarteritis, giving rise to a mononeuropathy multiplex or to a symmetrical axonal sort of polyneuropathy (see page 1137). The medical manifestations differ: included are headache, confusion and fluctuating cognitive disorders, convulsions, hemiplegia, and brainstem indicators. Wegener Granulomatosis uncommon illness of unknown cause, affecting adults as a rule and favoring males barely. A subacutely evolving vasculitis with necrotizing granulomas of the upper and decrease respiratory tracts adopted by necrotizing glomerulonephritis are its primary options. Neurologic problems come later in one-third to one-half of circumstances and take two varieties: (1) a peripheral neuropathy either in a pattern of polyneuropathy or, much more regularly, in a pattern of mononeuropathy multiplex (page 1138) and (2) quantity of} cranial neuropathies direct extension of the nasal and sinus granulomas into adjacent upper cranial nerves and from adjacent to pharyngeal lesions to the decrease cranial nerves (see also page 1188). The basilar elements of the skull eroded, with unfold of granuloma to the cranial cavity and extra remote elements. Cerebrovascular occasions, seizures, and cerebritis are much less common neurologic problems.
Best dutasteride 0.5 mg
A problem not easily categorised however having a particular clinical profile that should be known to neurologists is that of an osteoid osteoma. One must not overlook the potential prevalence of a lumbosacral plexus neuritis, a unilateral (occasionally bilateral) dysfunction akin to brachial neuritis, and acute or subacute sciatic or femoral neuropathy outcome of} diabetes, herpes zoster, or a retroperitoneal mass, any of which can produce a syndrome much like that of ruptured disc (see Chap. Lumbar Stenosis and Spondylotic Caudal Radiculopathy In the lumbar region, osteoarthritic or spondylotic modifications might result in compression of a number of} caudal roots. The roots are caught between the posterior floor of the vertebral physique and the ligamentum flavum posterolaterally. Lateral recess stenosis, which is a common feature of the spondylotic change (as talked about above), also contributes to root compression and the main problem in some patients. When this condition is extra extreme, the affected person gains relief by squatting or lying down with the legs flexed at the hips and knees. Usually the numbness begins in a single leg, spreads to the opposite, and ascends as standing or walking continues. Disturbances of micturition and impotence are rare except there was an extra extra acute disc herniation. In some patients with lumbar stenosis, neurologic signs persist without relation to physique position. The clinical picture, with its intermittency, corresponds to the so-called intermittent claudication of the cauda equina described by van Gelderen in 1948. Later it grew to become evident that the canal in these cases narrow from side to side (reduced interpedicular distance seen radiographically). It is when this slippage is unstable that new signs are doubtless to|prone to} seem abruptly; a new new} foot drop or urinary retention or overflow incontinence are the ones most common in our experience. This instability is evidenced on standard x-rays by a change within the diameter of the spinal canal as the affected person moves between the flexed and extended position of the again. Spondylotic lumbar radiculopathy is the caudal equivalent of spondylotic cervical myelopathy and radiculopathy. Insofar as the previous is a cauda equina syndrome, its differential prognosis mentioned in Chap. The ache is centered within the affected half of} the backbone, is elevated by movement, and is related to stiffness and limitation of motion. The sitting position is usually snug, though stiffness and discomfort are accentuated when the erect posture is resumed. The severity of the signs typically bears little relation to the radiologic findings; ache present regardless of minimal radiographic findings; conversely, marked osteophytic overgrowth with spur formation, ridging, bridging of vertebrae, narrowing of disc areas, subluxation of posterior joints on flexion, and air within the disc areas could be seen in both symptomatic and asymptomatic individuals. Facet Syndrome the character of this syndrome has been considerably clarified latest years|in recent times|lately}, however its definition continues to be imprecise. It seems that two distinct painful states could be associated to illness of the facet joint and the adjoining lateral recess. In one type, facet hypertrophy provides rise to a lumbar monoradiculopathy indistinguishable from that outcome of} a ruptured disc. Of these patients, 16 had an L5 radiculopathy, 3 an S1 radiculopathy, and three an L4 radiculopathy; in 15 of the patients there was coexisting again ache. At operation, the spinal root was compressed against the ground of the intervertebral canal by overgrowth of an inferior or superior facet. Foraminotomy and facetectomy, after exploration of the foundation from the dural sac to the pedicle, relieved the ache in 12 of the 15 operated cases. Often one is uncertain whether it was the analgesic effect on the joint or the infiltration of the region across the nerve root that relieved the ache. Two managed studies have supplied proof of the inefficacy of one other in style therapy for low again ache, particularly, corticosteroid injections into the facet joints (Carette et al; Lilius et al). Some patients have discovered that they might get hold of momentary relief from facet ache by forcefully twisting or stretching the again and creating an audible pop at the affected joint, comparable to chiropractic manipulation. Over time, they purchase a laxity of the supporting buildings of the joint, which can actually perpetuate the problem. Lumbar Adhesive Arachnoiditis this is also a considerably obscure entity by which the arachnoid membrane is thickened and opaque within the vicinity of the cauda equina. The term applied to thickening of the arachnoidal sheaths around roots (normal roots have basically no epineurium). According to a British evaluation, lumbar arachnoiditis is rare, having been seen in solely eighty of 7600 myelograms. The ordinary clinical features are intractable low-back and leg ache and paresthesias, all positionally sensitive, together with neurologic abnormalities referable to lumbar spinal roots. In our patients, multiple of} myelograms, disc rupture, operative procedures, infections, and subarachnoid bleeding have been causally involved. Some cases have followed spinal anesthesia and even epidural anesthesia by a period of months or years. The presumption is that the dura had been breached and sometimes there were clinical signs of an aseptic meningitis soon after the process. Lysis of adhesions and administration of intrathecal steroids have been of little value, though some skilled surgeons claim in any other case. Epidural injection of steroids is occasionally helpful, according to some orthopedists. Ankylosing Spondylitis this dysfunction, referred to prior to now as rheumatoid spondylitis and as von Bechterew or Marie-Strumpell arthritis, impacts younger adult males predominantly. Its prevalence within the basic inhabitants has been variously estimated at 1 to 3 per one thousand. Pain, usually centered within the low again, is the main complaint, at least of|no much less than} within the preliminary stages of the illness. At first the signs are obscure (tired again, "catches" up and down the again, sore back), and the prognosis missed quantity of} years}. Although the ache is recurrent, limitation of movement is fixed and progressive; over time, it dominates the clinical picture. Rarely, a cauda equina compression syndrome might complicate ankylosing spondylitis, the result apparently of an inflammatory reaction and later a proliferation of connective tissue within the caudal canal (Matthews). Severe lumbar arachnoiditis causing again ache, sciatica, and paresthesias years after spinal analgesia. The radiologic hallmarks are, at first, destruction and subsequently obliteration of the sacroiliac joints, followed by bony bridging of the vertebral our bodies to produce the characteristic "bamboo backbone. An uncommon further feature, virtually distinctive to this condition, is an excessive dilatation of the lumbar thecal sac. Ankylosing spondylitis can also be accompanied by the Reiter syndrome, psoriasis, and inflammatory ailments of the gut (see also Chap. The nice threat on this illness is fracture dislocation of the backbone from comparatively minor trauma, particularly flexion-extension accidents. Occasionally ankylosing spondylitis is sophisticated by destructive vertebral lesions. This complication should be suspected every time the ache returns after a period of quiescence or turns into localized. The major lesion small and asymptomatic, and the primary manifestation of the tumor ache within the again outcome of} metastatic deposits. At the time of onset of the again ache, there no radiographic modifications; when such modifications do seem, they usually take the type of destructive lesions in a single or a number of} vertebral our bodies with little or no involvement of the disc house, even within the face of a compression fracture. Infection of the vertebral column, osteomyelitis, is usually brought on by staphylococci and less typically by coliforms and mycobacteria. The affected person complains of ache within the again, of subacute or continual nature, which is exacerbated by movement however not materially relieved by relaxation. A paravertebral mass is often found, indicating an abscess, which can, within the case of tuberculosis, drain spontaneously at websites quite remote from the vertebral column. We have also encountered quantity of|numerous|a variety of} patients with subacute bacterial endocarditis who complained of extreme midline thoracic and lumbar again ache however had no evident an infection of the backbone. Special point out should be manufactured from spinal epidural abscess, which necessitates pressing surgical therapy. Indeed, in some collection, failure to correctly identify this lesion has led to cases of paraplegia or death from sepsis. Most typically this {is due to|is of} staphylococcal an infection, which is carried within the bloodstream from a septic focus. Another essential avenue of an infection is the intravenous self-administration of adulterated medicine and use of contaminated needles.
Buy dutasteride 0.5mg
Pain from no matter cause- a stiff joint, a toothache, fleeting chest or stomach pains, muscle cramps, or different disturbances such as constipation, frequency of urination, insomnia, pruritus, burning tongue, weight loss- might lead to obsessive complaints. The affected person passes from physician to physician in search of reduction from signs that would not bother the normal person, and no amount of reassurance relieves his frame of mind. The anxiousness and depressed mood of these individuals may be be} obscured by their preoccupation with visceral capabilities. When the affected person is examined, his facial features is usually plaintive, troubled, pained, or anguished. In different phrases, the affect on}, which is the outward expression of feeling, is consistent with with} the depressed mood. During the interview the affected person might sigh regularly or be tearful and will cry overtly. Occasionally the affected person will smile, but the smile impresses one as extra a social gesture than a genuine expression of feeling. The retardation extends to all subjects of conversation and affects movement of the limbs as nicely (anergic depression). The most extreme types of decreased motor activity, not often seen in the office or clinic, border on muteness and stupor ("anergic despair"). Conversation is replete with pessimistic ideas, fears, and expressions of unworthiness, inadequacy, inferiority, hopelessness, and typically guilt. In severe depressions, bizarre ideas and bodily delusions ("blood drying up," "bowels are blocked with cement," "I am half dead") may be be} expressed. Three theories have emerged concerning trigger of|the cause for} the pathologic depressive state: (1) that the endogenous kind is hereditary, (2) that a biochemical abnormality leads to a periodic depletion in the brain of serotonin and norepinephrine, and (3) that a primary fault in character improvement exists. Part of the trouble is with the word itself, which suggests being unhappy about one thing. Endogenous despair ought to be suspected in all states of continual sick health, hypochondriasis, incapacity that exceeds the manifest signs of a medical disease, neurasthenia and ongoing fatigue, continual pain syndromes- all of which can be termed "masked depressions. Depressive diseases and theories of their causation and management are thought-about further in Chap. Careful examination of medical material discloses that a range of phenomena are being so classified: anxiousness states, cycles of despair and mania, reactions to distressing life conditions, so-called psychosomatic ailments, and diseases of obscure nature. Obviously great license is being taken with the term emotional, the result little doubt of its indiscriminate nonmedical utilization. In its most easily recognized human kind, emotion is initiated by a stimulus (real or imagined), the notion of which involves recognition, reminiscence, and specific associations. Subdivided, the parts of emotion appear to include (1) the notion of a stimulus, which can be internal (an idea) or external, (2) the feeling, (3) the autonomic-visceral changes, (4) the outward show of affect on}, and (5) the impulse to a certain kind of activity. Anatomic Relationships the prevalence of abnormal emotional reactions the center of|in the midst of} disease is associated with lesions that preferentially involve certain parts of the nervous system. These constructions have been grouped beneath the term limbic and are among the most complex and least understood parts of the nervous system. Actually, Thomas Willis had pictured this 442 area of the brain and referred to it because the limbus in 1664. Broca preferred his term, le grand lobe limbique, to rhinencephalon, which was the term then in vogue and referred extra specifically to constructions having an olfactory perform. Neuroanatomists who followed Broca affirmed his position and have extended the boundaries of the limbic lobe to embrace not solely the cingulate and parahippocampal gyri but additionally the underlying hippocampal formation, the subcallosal gyrus, and the paraolfactory space. The phrases visceral brain and limbic system, launched by MacLean, have a good wider designation and extra completely describe the constructions concerned in emotion and its expression; along with all parts of the limbic lobe, they embrace a number of|numerous|a selection of} associated subcortical nuclei such as those of the amygdaloid complex, septal area, preoptic space, hypothalamus, anterior thalamus, habenula, and central midbrain tegmentum, together with the raphe nuclei and interpeduncular nucleus. The major constructions comprised by the limbic system and their relationships are illustrated in. The cytoarchitectonic preparations of the limbic cortex clearly distinguish it from the encompassing neocortex (isocortex). In contrast, the inside half of} the limbic cortex (hippocampus) is composed of irregularly arranged aggregates of nerve cells that tend to to|are inclined to} be in a trilaminate configuration (archi- or allocortex). The cortex of the cingulate gyrus, which forms the outer ring of the limbic lobe, is transitional between neocortex and allocortex- hence it is known as|is called|is named} the mesocortex, or juxtallocortex. The amygdaloid complex, a subcortical nuclear component of the limbic system, additionally has a novel composition, consisting of a number of} separable nuclei, every with particular connections to different limbic constructions. The connections between the orbitofrontal neocortex and limbic lobes, between the person parts of the limbic lobes, and between the limbic lobes and the hypothalamus and midbrain mirror their many practical relationships in regard to emotion. At the core of this method lies the medial forebrain bundle, a complex set of ascending and descending fibers that join the orbitomesiofrontal cortex, septal nuclei, amygdala, and hippocampus rostrally and certain nuclei in the midbrain and pons caudally. This system, of which the hypothalamus is the central part, was designated by Nauta because the septohypothalamomesencephalic continuum. There are many different interrelationships between varied parts of the limbic system, only a few of which could be indicated here. It leads from the hippocampus, through the fornix, to the mammillary body and septal and preoptic regions. The cingulum runs concentric to the curvature of the corpus callosum; Copyright � 2005, 2001, 1997, 1993, 1989, 1985, 1981, 1977, by the McGraw-Hill Companies, Inc. Also, the cingulum receives fibers from the inferior parietal lobule and temporal lobe, that are multimodal suprasensory facilities for the integration of visual, auditory, and tactile perceptions. A Fornix Cingulate gyrus Occipital lobe Frontal lobe Physiology of the Limbic System the practical properties of the limbic constructions Hippocampus first became known through the third and fourth Temporal lobe decades of the twentieth century. From ablation and stimulation research, Cannon, Bard, and others established the fact that|the truth that} the hypothalamus accommodates B Anterior thalamic nuclei Cingulum the suprasegmental integrations of the autonomic Medial dorsal nervous system, each the sympathetic and paranucleus of thalamus sympathetic parts. Soon after, anatomists discovered efStria terminalis ferent pathways from the hypothalamus to the neural constructions subserving parasympathetic and sympathetic reflexes. Dorsal tract Following Cannon, Bard localized the central longitudinal Anterior fasciculus commissure regulatory apparatus for respiration, wakefulness, and sexual activity incorrectly, in the hypothalaMedial mus. Later, the hypothalamus was additionally discovered to forebrain Olfactory bulb bundle comprise neurosecretory cells, which control the secretion of the pituitary hormones; within it are also Ventral amygdalofugal particular sensory receptors for the regulation of hunpathway ger, thirst, body temperature, and levels of circuAmygdala lating electrolytes. Top: surface topography of the limbic the practical anatomy of these autonomic and neuroendocrine systems is mentioned in Chaps. Bottom: connections of the limbic constructions and their relation to the thalamus, hypothalamus, and midbrain tegmentum. In subsequent research, Bard and Mountcastle discovered that lacy of this theory became evident when it was demonstrated by provided that the ablations included the amygdaloid nuclei on either side Cannon that the capacity to manifest emotional changes remained would sham rage be produced; removal of all the neocortex but sparafter all visceral afferent fibers had been interrupted. Interestingly, in the Although the natural stimuli for emotion involve the identical nemacaque monkey, a usually aggressive and recalcitrant animal, reocortical perceptive-cognitive mechanisms as does nonemotional moval of the amygdaloid nuclei bilaterally greatly decreased the resensory experience, there are essential differences, which relate to actions of concern and anger (see further on). The role of the hypothalthe distinguished visceral results and explicit behavioral reactions amus and amygdala in the production of each directed and undirected evoked by emotion. Clearly, specific parts of the nervous system anger and displays of rage has turned out to be far more complex. Bard, in 1928, first produced "sham rage" in cats In any case, Papez, on the basis of these and his own anatomic by removing the cerebral hemispheres and leaving the hypothalamus observations, postulated that the limbic parts of the brain elaborate and brainstem intact. Of unknown significance is the fact that|the truth that} the zinc content material of the limbic system is the highest of any half of} the nervous system. All of this having been said, it will be a mistake to assume that the numerous constructions listed above and their connections represent a unified practical system. The term limbic system is a simplification, significantly because the that} varied parts differ extensively in respect to their connections with the neocortex and central nuclei, their transmitters, and their results when broken. But said that lesions on this system most consistently and specifically alter emotionality; it subsequently remains a helpful concept. Only in relatively current years have neurologists, primed with the information of these research, begun to relate emotional disturbances in patients with disease of limbic constructions. These medical observations, summarized in the following pages, are starting to kind an interesting chapter in neurology. The record is tentative, since our understanding of many of these states, significantly their pathologic basis, is incomplete. Only a small variety of these derangements can be used as pathognomonic indicators of lesions and ailments particularly parts of the human brain. Panksepp thinks of emotional disturbances and their expression as reflective solely of "spheres of influence" of certain brain mechanisms. We have discovered that, taken in context, these disturbances are helpful diagnostically. And, as information of emotional issues will increase, an understanding of the functioning of limbic constructions will undoubtedly bring together giant segments of psychiatry and neurology. This determine additionally shows the connections to the amygdala and prefrontal and affiliation cortices. The intermediate position of the limbic constructions allows them to transmit neocortical results from their outer side to the hypothalamus and midbrain on their inside side.
0.5 mg dutasteride
A fuller account of varieties of|these kind of|most of these} headache could also be} present in later chapters of this guide, the place the underlying diseases are described. When the headache is continual, recurrent, and unattended by different symptoms and indicators of neurologic illness, the doctor faces a more difficult diagnostic downside. In basic, the classification of these headaches and different types of craniofacial ache follow the plan outlined by the International Headache Society (see Olesen). One space of controversy in classification issues the status (and indeed the existence) of rigidity headache. Migraine Migraine is a ubiquitous familial disorder characterised by periodic, commonly unilateral, usually pulsatile headaches that start in childhood, adolescence, or early adult life and recur with diminishing frequency throughout advancing years. Two intently associated medical syndromes have been recognized, the first known as migraine with aura and the second, migraine without aura (terminology of the International Headache Society). For a few years the first syndrome was referred to as classic or neurologic migraine and the second as frequent migraine. Either kind could also be} preceded by imprecise premonitory adjustments in temper and urge for food (a prodrome). Migraine with aura, the time period now used to denote classic migraine, is ushered in by an evident disturbance of nervous function, most frequently visible, adopted in a few minutes by hemicranial or, in about one-third of cases, by bilateral headache, nausea, and typically vomiting, all of which final for hours or as long as|so long as} a day or two. Migraine without aura is characterised by an unheralded onset over minutes or longer of hemicranial headache or, less usually, by generalized headache with or without nausea and vomiting, which then follows the identical temporal sample as the migraine with aura. Sensitivity to gentle and noise attends each types, and intensification with motion of the pinnacle is frequent. If the ache is severe, the patient prefers to lie down in a quiet, darkened room and tries to sleep. The hemicranial and the throbbing (pulsating) aspects of migraine are its most characteristic features comparability to|compared to} different headache types; each patient shows a proclivity for the ache to result on} one side or the opposite of the skull, however not solely. The genetic nature of classic migraine is apparent from its occurrence in several of} members of the family of the identical and successive generations in 60 to 80 percent of cases; the familial frequency of frequent migraine is barely decrease. Certain uncommon types of migraine, similar to familial hemiplegic migraine, seem to be monogenic disorders, however the position of these genes, one of which codes for a calcium channel (see below), in classic and customary migraine is speculative. Migraine, with or without aura, is a remarkably frequent situation; its prevalence amongst Caucasians is within the vary of four to 6 percent amongst males and 13 to 18 percent amongst ladies (see Stewart et al). Migraine could have its onset in childhood however usually begins in adolescence; in additional than 80 percent of patients, the onset is before 30 years of age, and the doctor ought to be cautious in attributing headaches that seem for the first time after this age to migraine. In ladies, the headaches tend to to|are inclined to} happen during the premenstrual period; in about 15 percent of such migraineurs, the assaults are solely perimenstrual ("true menstrual migraine"), although estrogen and progesterone levels throughout the menstrual cycle are the identical in normal and migrainous ladies. Menstrual migraine, mentioned additional on, is thought to be associated to the withdrawal of estradiol somewhat than progesterone (based on the work of Somerville). It is now acknowledged that the affect of sex hormones on headache is extra advanced. The assaults stop throughout being pregnant in seventy five to 80 percent of women, and in others they proceed at a reduced frequency; less usually, assaults of migraine or the associated neurologic symptoms first seem throughout being pregnant, usually within the first trimester. Although migraine usually diminishes in severity and frequency with age, it could truly worsen in some postmenopausal ladies, and estrogen therapy could either improve or, paradoxically, diminish the incidence of headaches. The use of contraception tablets has been associated with an increased frequency and severity of migraine and in uncommon situations has resulted in a everlasting neurologic deficit. Some patients link their assaults to sure dietary items- particularly chocolate, cheese, fatty foods, oranges, tomatoes, and onions- however these connections in most cases seem to us to be overrated. Some of these foods are wealthy in tyramine, which has been incriminated as a provocative think about migraine. Perhaps the most typical ostensible set off is excess caffeine consumption or withdrawal of caffeine. Migraine with aura incessantly has its onset quickly after awakening, however it could happen at any time of day. During the preceding day or so, there could have been delicate adjustments in temper (sometimes a surge of vitality or a sense of well-being), hunger or anorexia, drowsiness, and frequent yawning. This could also be} adopted by an enlarging blind spot with a shimmering edge (scintillating scotoma), or formations of dazzling zigzag strains (arranged like the battlements of a fort, hence the time period fortification spectra or teichopsia). Other patients complain as an alternative of blurred or shimmering or cloudy imaginative and prescient, as though they were trying through thick or smoked glass or the wavy distortions produced by warmth rising from asphalt. These luminous hallucinations move slowly across the visible subject for several of} minutes and may go away an island of visible loss of their wake (scotomatous defects); the latter are usually bilateral and sometimes homonymous (involving corresponding parts of the field of regard of every eye), pointing to their origin within the visible cortex. Patients almost invariably attribute these visible symptoms to one eye somewhat than to parts of each fields. Other focal neurologic symptoms, much less frequent than visible ones, embrace numbness and tingling of the lips, face, and hand (on one or each sides); slight confusion of pondering; weak spot of an arm or leg; delicate aphasia or dysarthria, dizziness, and uncertainty of gait; or drowsiness. Only one or a few of} of these neurologic phenomena are present in any given patient, and they tend to to|are inclined to} happen in roughly the identical mixture in each assault. If weak spot or paresthetic numbness spreads from one half of} the physique to one other or if one neurologic symptom follows one other, this happens comparatively slowly over a period of minutes (not over seconds, as in a seizure, or simultaneously in all affected parts as in a transient ischemic attack). At its peak, inside minutes to an hour, the patient is compelled to lie down and to shun gentle and noise. The headache lasts for hours and typically for a day or even longer and is always probably the most unpleasant characteristic of the illness. The temporal scalp vessels could also be} tender and the headache is worsened by pressure or jarring of the physique or rapid motion of the pinnacle. For a time, when psychosomatic drugs was much in vogue, there was insistence on a migrainous personality, characterised by tenseness, rigidity of attitudes and pondering, meticulousness, and perfectionism. Moreover, the fact that|the truth that} the headaches could start in early childhood, when the personality is relatively amorphous, would argue in opposition to this idea. A relationship to epilepsy additionally be|can be} tenuous; nonetheless, the incidence of seizures is barely higher in migrainous patients and their family members than within the basic inhabitants. There does seem to be in migraineurs an overrepresentation of movement sickness and of fainting. The headache could also be} exceptionally severe and abrupt in onset ("crash migraine" or "thunderclap headache"), elevating the specter of subarachnoid hemorrhage. The headache could at times precede or accompany somewhat than follow the neurologic abnormalities of migraine with aura. Milder types of migraine, especially if partially managed by medication, could not force the patient to withdraw from accustomed actions. Any one of many three principal components- neurologic abnormality, headache, and nausea and vomiting- could also be} absent. Visual disturbances, by far the most typical, differ intimately from patient to patient; numbness and tingling of the lips and the fingers of 1 hand are probably next in frequency, adopted by transient aphasia or a thickness of speech and hemiparesis as talked about earlier. Basilar Migraine A less frequent type of the migraine syndrome, with outstanding brainstem symptoms, was described by Bickerstaff. The patients, usually younger ladies with a household history of migraine, first develop visible phenomena like those of typical migraine except that they occupy the entire of each visible fields (temporary cortical blindness could occur). There could also be} associated vertigo, staggering, incoordination of the limbs, dysarthria, and tingling in each hands and feet and typically round either side of the mouth. These symptoms final 10 to 30 min and are adopted by headache, which is usually occipital. Some patients, on the stage when the headache is probably to|prone to} start, could faint, and others turn into confused or stuporous, a state that will persist for several of} hours or longer. The symptoms intently resemble those as a result of} ischemia within the territory of the basilar-posterior cerebral arteries- hence the name basilar artery or vertebrobasilar migraine. Ophthalmoplegic and Retinal Migraine the former are recurrent unilateral headaches associated with weak spot of extraocular muscle tissue. A transient third-nerve palsy with ptosis, with or without involvement of the pupil, is the same old} picture; rarely, the sixth nerve is affected. The paresis usually outlasts the headache by days or perhaps weeks|days or even weeks}; after many assaults, a slight mydriasis and, rarely, ophthalmoparesis could stay as everlasting defects. In some cases, the retinal arterioles are attenuated and typically there are retinal hemorrhages; in different cases, narrowing of retinal arteries or venules has been observed throughout an assault, as described within the cases reported by Berger and colleagues. In still different cases, monocular blindness is associated with disc edema and peripapillary hemorrhages, and imaginative and prescient recovers solely partially after several of} months (Hupp et al).
References:
- https://kdigo.org/wp-content/uploads/2017/02/KDIGO-2009-CKD-MBD-Guideline-English.pdf
- https://www.lvhn.org/sites/default/files/uploads/PDFs/oral%20ca%20lec%20%5BCompatibility%20Mode%5D.pdf
- https://pdfs.semanticscholar.org/469d/af1c90ad6d365e7c3ae2a02bb675e3096097.pdf
- https://uniteyouthdublin.files.wordpress.com/2015/01/lennard_davis_the_disability_studies_reader_secbookzz-org.pdf
- https://www.waxmancancer.org/wp-content/uploads/2019/06/SWCRFAgingCancerBookletWeb.pdf