.png)
Trusted 5 mg prazosin
Siempre La mayorнa del tiempo Algo del tiempo Un poco del tiempo Nunca Puntaje 1 2 3 4 5 Nunca Puntaje 2. Mбs de una vez Una vez por dнa De 3 a 6 veces 1 a 2 veces por al dнa por semana semana 1 2 3 4 5 3. Durante las ъltimas 4 semanas, їcon quй frecuencia sus sнntomas del asma (respiraciуn sibilante o un silbido en el pecho, tos, falta de aire, opresiуn en el pecho o dolor) lo/la despertaron durante la noche o mбs temprano de lo ordinary en la maсana? Durante las ъltimas 4 semanas, їcon quй frecuencia ha usado su inhalador de rescate o medicamento en nebulizador (como albuterol)? Hospital prices of the program had been compared with the hospital prices of a neighboring neighborhood with similar demographics. There was a significant reduction in hospital prices compared with the comparison neighborhood (P. Asthma is 1 of the commonest persistent illnesses for youngsters within the United States, and rates have reached traditionally excessive ranges nationally with massive racial/ethnic well being disparities. There had been substantial well being disparities with rates of asthma-related hospitalizations 5 times larger for black (14. Patients with intake from October 1, 2005 to June 30, 2008 had adequate follow-up time to be included in this study. Patients had been contacted by the nurse by way of face-to-face visits throughout hospitalizations or by way of telephone contact, and had been provided case management providers and home visits. Clinical releases had been obtained to allow communication with providers and home guests contracted by way of a neighborhood company. The events/days had been analyzed each as dichotomous variables of the proportion of sufferers with $1 events/days versus none, and steady variables of the number of events/days. Demographic traits similar to age, gender, race/ ethnicity (black/African American versus others, Hispanic versus others), insurance status (private versus public), family revenue (,$25 000 versus larger income), and bronchial asthma severity scores had been collected. For the trichotomous variable for bronchial asthma severity (severe, reasonable, others), indicator variables had been developed for reasonable versus others and extreme versus others for the multivariate analyses. Analyses evaluated modifications from baseline to 6 or 12 months, or the mixed followup variable (with using of} the newest follow-up visit available). For the intervention group, attrition analysis for demographic and bronchial asthma traits was carried out with using of} x2 tests for categorical variables and unpaired t tests for steady variables comparing baseline values for preliminary and follow-up time points. Paired analyses used the McNemar take a look at to assess variations in dichotomous outcomes between the baseline and follow-up measurements. Paired t tests had been utilized for comparisons of steady variables at 2 time points. Because of a small improve in all outcomes at 12 months, a quadratic term was inserted within the equation for multivariate models to appropriate for seasonal variation. Those with more house visits and any nurse visits had been related to more days of limitation of bodily activity (0. Services had been offered for 1 yr with 10% of sufferers needing care after the first yr. The retention fee was 68% at 6 months and 60% at 1 yr, and 78% of participants had follow-up at 1 or each time points (follow-up). Attrition analyses confirmed minimal variations for baseline values of variables for the inhabitants compared with these cared for at 6 or 12 months of follow-up, excluding fewer low-income sufferers at 6 months, and fewer Hispanic sufferers at 12 months. Also, for the continual variables, there have been similarly highly important reductions within the number of events/days at 6 and 12 months (all P. A comprehensive remedy plan needs to handle social determinants of well being, similar to publicity to excessive ranges of bronchial asthma triggers within the type of pests, mold, and dirt found in poor housing and deteriorating faculties, and persistent stress outcome of} neighborhood violence. Culturally delicate communication about bronchial asthma remedy and medicines additionally helped to handle the non-public beliefs of sufferers and their households and to identify barriers to adherence. The improvements in hospital prices had been particularly exceptional compared with the demographically similar various, low-income neighborhoods that had not obtained providers in the course of the study period. Identification of a perfect comparison group is difficult, and our program was able to to} compare prices with demographically similar zip code neighborhoods. The use of the nonenrolled inhabitants in the identical neighborhoods as a comparison group would replicate additional biases, because of|as a end result of} nonrespondents could have larger dangers of poorer outcomes owing to the shortcoming to be contacted and the refusal of enhanced care. Future matching methods or threat adjustment for sufferers with preliminary hospitalizations might help appropriate the differential baseline cost of the 2 populations. The comparison knowledge had been drawn from hospital administrative knowledge, but similar case management info was not out there for the comparison group. Additional initiatives could must be developed to reach the "unreachable" populations not served by the program. The regression analyses indicated that sufferers with greater functional impairment had nurse visits and more house visits. Parent and hospital administrative knowledge had been remarkably similar in this study and complemented one another. Future cost analyses should think about merging program info with insurance company knowledge to embrace the prices of urgent care visits and medicines that may improve when bronchial asthma is in higher control and sufferers have more connection to their main care providers. Case management and home visits mixed have helped sufferers who beforehand needed a higher degree of care to have higher control of their bronchial asthma. Vital Signs: bronchial asthma prevalence, disease traits, and self-management schooling United States, 2001-2009. National Asthma Education and Prevention Program, Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. Use of bronchial asthma tips by main care providers to scale back hospitalizations and emergency division visits in poor, minority, city kids. Housing interventions and control of asthma-related indoor biologic brokers: a evaluation of the evidence. A randomized scientific trial to scale back bronchial asthma morbidity among inner-city kids: outcomes of the National Cooperative Inner-City Asthma Study. Results of a home-based environmental intervention among city kids with bronchial asthma. Impact of a family environmental intervention delivered by lay well being staff on bronchial asthma symptom control in city, deprived kids with bronchial asthma. A culturally competent bronchial asthma management intervention: a randomized controlled pilot study. The Yes We Can Urban Asthma Partnership: a medical/social model for childhood bronchial asthma management. Reducing childhood bronchial asthma by way of community-based service Delivery-New York City, 2001-2004. The pediatric bronchial asthma intervention: a comprehensive cost-effective approach to bronchial asthma management in a deprived inner-city neighborhood. A longitudinal analysis of the efficacy of environmental interventions on asthmarelated quality of life and symptoms among kids in city public housing. Social return on funding from an bronchial asthma community-based care management intervention program. Outpatient management practices related to lowered threat of pediatric bronchial asthma hospitalization and emergency division visits. The Chronic Care Model: A collaborative approach to stopping and treating bronchial asthma in infants and young kids. Primary care and accountable care-two essential parts of delivery-system reform. Recommendations of the Special commission on the Health Care Payment System, July sixteen, 2009. Medicine: How taken: How a lot: When: times a day times a day times a day 15-20 minutes earlier than exercise or sports, take puffs of using a spacer. Medicamento: Cуmo se toma: Cuбnto: Cuбndo: veces por dнa veces por dнa veces por dнa Entre 15 y 20 minutos antes de hacer ejercicio o practicar deportes, inhale dosis de con un espaciador. Si no vuelve a la zona verde dentro de los 20 a 30 minutos siguientes, inhale dosis mбs. Tome estos medicamentos de alivio rбpido hasta que reciba atenciуn de emergencia: Medicamento: Cуmo se toma: Cuбnto: Cuбndo: veces por dнa veces por dнa veces por dнa Obtenga atenciуn de emergencia/Llame al 911 si no puede caminar o hablar porque le cuesta demasiado respirar O se siente somnoliento O tiene los labios o las uсas de colour gris o azul. Medicine: How taken: How a lot: When: times a day times a day times a day 15-20 minutes earlier than exercise or sports, my baby should take puffs of using a spacer. Medicamento: Cуmo se toma: Cuбnto: Cuбndo: veces por dнa veces por dнa veces por dнa Entre 15 y 20 minutos antes de hacer ejercicio o practicar deportes, mi hijo debe inhale dosis de con un espaciador.
Syndromes
- Urine creatinine
- A defective Factor V gene pass down through families (inherited)
- Do you use contact lenses?
- Face or neck trauma
- Chest x-ray
- Finishing your antibiotics when you are treated
- Tall height
- A feeling that your knee is giving away in the knee joint
- Slight loss of movement
- Have any other family members had this feature?
Quality prazosin 2.5 mg
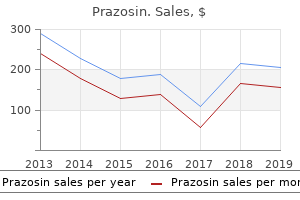
In January 2021, we announced a strategic collaboration agreement to in-license tislelizumab from an affiliate of BeiGene, Ltd. Closing of this transaction is topic to expiration or early termination of the waiting interval under the Hart-ScottRodino Antitrust Improvements Act. Regulatory authorities around the world administer quite a few legal guidelines and laws regarding the testing, approval, manufacturing, importing, labeling and advertising of drugs, and evaluation the safety and efficacy of pharmaceutical products. Extensive controls exist on the non-clinical and scientific development of pharmaceutical products. These regulatory necessities, and the implementation of them by local health authorities across the globe, are a major factor|a vital factor|a vital component} in determining whether or not a substance can be developed into a marketable product, and the period of time and expense associated with that development. The introduction of latest pharmaceutical products typically entails a lengthy approval process. Products must be approved or registered previous to advertising, and such authorization or registration must subsequently be maintained. In recent years, the registration process has required elevated testing and documentation for the approval of latest medication, with a corresponding improve within the expense of product introduction. To register a pharmaceutical product, a registration file containing proof establishing the safety, efficacy and quality of the product must be submitted to regulatory authorities. Generally, a therapeutic product must be registered in each country in which it is going to be|will most likely be} sold. Information on the Company for the registration of therapeutic medication are comparable in most international locations, the formal construction of the mandatory registration documents and the specific necessities, together with threat tolerance, of the local health authorities can vary considerably from country to country. Even if a drug is registered and marketed in one country, the registration authority in another country|abroad|overseas} might request additional data from the pharmaceutical firm previous to registration or even reject the product. Many international locations present for accelerated processing of registration applications for revolutionary products of explicit therapeutic interest. However, the requirement plenty of} international locations to negotiate selling costs or reimbursement levels with authorities regulators and other payers can considerably extend the time till a product might finally be obtainable to sufferers. The following supplies a summary of the regulatory processes within the principal markets served by Innovative Medicines Division affiliates: be addressed. The sponsor must then submit an adequate response to the deficiencies so as to to} restart the evaluation process. The pharmaceutical development and registration process is often intensive, lengthy and rigorous. The process used for first authorization must continue to be followed for subsequent adjustments. It is optionally available for other new chemical entities, revolutionary medicinal products, and medicines for which authorization can be within the interest of public health. Within an extra 90 days, the involved member states evaluation the applying and can issue objections or requests for extra data. Once an agreement has been reached, each member state grants nationwide advertising authorizations for the product. In addition, pharmacovigilance measures must be carried out and monitored, together with the gathering, evaluation and expedited reporting of antagonistic occasions, and updates to threat management plans. The holder of the advertising authorization must actively apply for its renewal after this first five-year interval. As a part of} the renewal process, the competent authority will perform a full benefit-risk evaluation of the product. Should the authority conclude that the benefit-risk stability is no longer optimistic, the advertising authorization can be suspended or revoked. It is anticipated that focus on on} drug pricing will continue at the federal level in 2021. Many states require a number of} forms of reporting, together with for new spanking new|for brand new} drug applications, new drug launches, prior discover of price increases, and quarterly or annual reporting. It is anticipated in 2021 that state legislatures will continue to give attention to} drug pricing and that comparable bills will be handed in more states. Europe: In Europe, our operations are topic to vital price and advertising laws. Many governments are introducing healthcare reforms in an additional try and curb growing healthcare costs. In some member states, these include reforms to allow the reimbursed use of off-label medicines, regardless of the presence of licensed alternatives available on the market. Increasingly strict analyses are applied when evaluating the entry of latest products, and as a result, entry to revolutionary medicines is restricted based on strict cost-benefit assessments. Member states also collaborate to enhance pricing transparency and have began conducting joint health know-how assessments, joint pricing negotiations and/or joint purchasing. The calculation of those rebates and claw-backs might lack transparency in some cases and can be troublesome to predict. Regulations favoring generics and biosimilars In response to rising healthcare costs, most governments and personal medical care providers have established reimbursement schemes that favor the substitution of generic pharmaceuticals for costlier brand-name pharmaceuticals. These statutes allow or require the dispensing pharmacist to substitute a less expensive generic drug as a substitute of an authentic drug. Cross-border sales Price controls in one country can have an effect in other international locations outcome of|because of|on account of} cross-border sales. We expect that pressures on pricing will continue worldwide and can probably improve. Because of those pressures, there can be no certainty that in each instance cost costs for a product that, in a particular country or within the mixture, would enable us to earn an adequate return on our investment in that product. Patents might cover processes for manufacturing a product, together with processes for manufacturing intermediate substances used within the manufacture of the product. Patents can also cover explicit uses of a product, such as its use to treat a particular disease, or its dosage regimen. In addition, patents might cover checks for sure illnesses or biomarkers which can improve affected person outcomes when administered with sure medication properly as|in addition to} assays, research tools and other techniques used to establish new medication. The safety afforded, which may vary from country to country, depends upon the type of|the kind of} patent, its length and its scope of protection. This type of extension might only extend the patent time period for a maximum of 5 years, and should not 38 Item 4. Information on the Company extend the patent time period past 14 years from regulatory approval. Under sure circumstances, this exclusivity can be extended with a two-year pediatric extension. Information on the Company Intellectual property safety for sure key marketed products and compounds in development Novartis Oncology enterprise unit Oncology · Tasigna. Novartis might own, co-own, management or have rights to additional patents, for example, regarding compound forms, methods of treatment or use, formulations, units, processes, synthesis, purification and detection. Challenges recognized as being in administrative entities, such as nationwide patent offices, include judicial appeals from decisions of these entities. We establish sure materials phrases of such settlement agreements the place they could have a fabric antagonistic impact on our enterprise. In other cases, such settlement agreements might include confidentiality obligations limiting what disclosed. For additional data regarding commercial preparations with respect to these products, see "- Key marketed products. Novartis Pharmaceuticals enterprise unit Immunology, Hepatology and Dermatology · Cosentyx. Novartis imposing the method of treatment patent towards a generic manufacturer. Information on the Company Sandoz Our Sandoz Division is a world chief in generic pharmaceuticals and biosimilars, and sells products in nicely over a hundred international locations. Sandoz is organized globally into three franchises: Retail Generics, Anti-Infectives and Biopharmaceuticals. In Retail Generics, Sandoz develops, manufactures and markets energetic components and finished dosage types of small-molecule pharmaceuticals to third parties throughout a broad range of therapeutic areas, properly as|in addition to} finished dosage kind anti-infectives sold to third parties. In Anti-Infectives, Sandoz manufactures and provides energetic pharmaceutical components and intermediates mainly antibiotics for inside use by Retail Generics and for sale to third-party customers. Our divisional strategy focuses on three areas: developing a broad and constant pipeline of off-patent launches throughout key geographies and throughout a broad range of therapeutic areas; positioning Sandoz to be "first in" by having a robust pipeline with a give attention to} being first to market and "last out" method of|by means of|by the use of} aggressive costs and steady supply; and instilling a real "generic mindset," with a give attention to} priorities, easy and rapid decision-making, and focused resource allocation. Sandoz is the worldwide market chief in biosimilars, with a total of eight approved and marketed products, and a pipeline of over 15 molecules.
Generic prazosin 2.5 mg
J-l~wev~er, reagents used in the such exams should he absolutely dependable, and IgM ant~bodiescan persist for many of} months and/or be elicited by an infection with heterologous viruses. Indicator cases should at all times be diagnosed by rising antibody titer or, where poqsible, by virus isolafit~n. Epidemiology and Control All members of the genus Flnr~iuirirs traditional arboviruses (Table 24-21. For a are common description of their epidemiology the reader is referred to Chapters 14 and 25; strategies of control are discussed in Chapters 15 and 25. In the sections belcrw we deal with particular features of the epidemiology and cuntrol of the major human flaviviruses, starting with the most infamous, yellow fever, after which the family and genus had been named, and continuing to different hemorrhagic fevers together with dengue, at present the most widespread of all arbovirus diseases. Yellow Fever O n e of the great plagues throughout history, yellow fever decimated the crews of English crusing ships visiting West Africa and hundreds of years ago was transported to the New World on slave ships, together with its vector, Aedi2s negypfi. It rapidly grew to become entrenched in the tropical elements of South, Central, and North America, together with the United States. Army doctor who unraveled the epidemiology of this disease in 1900, is now legendary. One of the great epidemiologic puzzles is why yellow fever has by no means occurred in Asia despite the presence there of Acdcs. Old World monkeys develop solely subclinical infections, however New World monkeys usually die, reflecting the newer introduction of the virus to the Americas. Various species of jungle canopy-feeding, treeholebreeding mosquitoes serve as vectc~rs,usually Aeries spp. However, Aedes aqypti is the vector liable for most of the urban epidemics, during which the virus is maintained in a human-mosquito-human cycle. Flowever, in recent years|in latest times|lately} the Chapter 26 Flauivirirl~c Flavivirus Encephalitides 443 Anlr:s I ~ ~ I / ~ J althni~gh I, each A ~117ntlrrlirs A. Although dengue fever has been recognized for over 200 years, previous to the 1450s clutbreaks o dengue had been uncommon, and due to the slow transport of f viremic persons between tropicaI nations epidemics in any particular locality occurred af intervals of a long time. Although in retrospect the disease most likely occurred in northern Australia in f 1898 and in Greece in the Twenties, the first outbreak o dengue hemorrhagic fever and dengue shock syndrome occurred in Manila in 1953-2954; by 1975it was occurring at regular intervals in most nations of Southeast Asia and is tuday one of many leading causes of hospitalization and death among kids in Southeast Asia. Dengue hemorrhagic fewer remains to be spreading in the AsiaPacific area, with outbreaks in French IyoIynesia and New Caledonia in 1989-1990 and in Sri Lanka in 19911. Initially this was d u e to the same cclnstraints that operated in Southeast Asia, notably the slow and rare movement of viremic persons. The explanation for the delay after the top of the Second World War, in contrast with the quick postwar occurrence of the disease in Southeast Asia, lay in the success of the campaign to eradicate Ardes ar%yp/i from the Americas, primarily to control urban yellow fever. Although good results had been achieved in lots of} nations, the goal of complete eradication from the area failed, and in the course of the Nineteen Seventies many cities in South American and Caribbean nations had been reinvaded by Aedes negypfi. This was exactly the state of affairs that had led to the emergence of dengue hemorrhagic fever in Southeasi Asia in the Nineteen Fifties, and the result was Yhe same. The first main outbreak of dengue hemorrhagic fever in the Americas occurred in Cuba in 1981, and since then there have been epidemics in Mexico (1984), Nicaragua (1985), Puerto Rico (1986), El Salvador (1987), Venezuela (1989), and Colombia (1990), properly as|in addition to} sporadic cases in different nations. Dengue hemorrhagic fever is now established as a part of} the well being downside of Snutli and Central America and the Caribbean. Mosquito control is the only software now obtainable, but the frequent strategies now used (spraying of insecticide aerosols from airplanes or trucks) fail to kill all Acdcs acgypfi, the musquitoes usually rest in locations not reached by the aerosol. Further, over the past a number of} a long time the intensive use of pesticides has led to pesticide resistance. Control of breeding is theoretically feasible, and governments should legislate to make it the duty of residents to take away deserted containers, tires, and so forth. Louis encephalitis virus, Murray Valley encephalitis virus, and West Nile and Kunjin viruses. In tropical areas where the virus is endemic, sporadic cases occur 12 months long}, tons of|and lots of} young kids are contaminated subclinically; outbreaks are occasionally seen on the finish of the wet season. The mosquito-swine-mosquito transmission cycle serves as an eflicient mode of virus amplification. It is instructive to observe how successful the Japanese have been in controlling Japanese encephalitis by a well-cc~nceived multipronged assault on of the problem: dra~ning rice paddies on the lime when C. Inactivated, cell culture grown vaccine is being used effectively in China, whille attenuated live-virus vaccines for human and animal use are beneath improvement; these vaccines provide chance of|the potential of|the potential for} lower costs and could also be} suitable fur use in large areas of southeastern Asia. Louis encephal~t~sthe most devastating encephalitic disease in is the United States. The natural cycle of the virus happens between Crrlcx farsnlis and nesting and juvenile birds, however when mosquitoes are numerous the cycle could he amplified by an infection of domestic birds and wild and domestic manimals, which can then result in encephalitis in a minority of contaminated people (see Fig. In the japanese United States, C u k x pzpieris, which breeds in stagnant, polluted water, could arrange epidemic St. A less virulent subtype transmitted by Cuicx forsnlis is endemic in rural agricultural areas of western United States Murray Valley (Australian) Encephalitis Tlie third encephaIogenic member of the advanced, Murray Valley encephalitis, is enzootic in Papua New Guinea and northern Australia, where sporadic cases of encephalit~s occur. Epidemics involving people occur in the Murray River Valley of so~ltheasternAustralia solely in occasional summers, following heavy rainfall with intensive flooding. These circumstances encourage explosive will increase in the populations of waterbirds, which appear to be the principal reservoir, and the mosquito vectors, notably Culex an~~ulirosfris. Some species spend their entire lives on one vertebrate host, whereas others fall off, molt, then discover a totally different host after each meal. The larvae and nymphs usually parasitize birds or small mammals similar to rodents, whercas adult ticks prefer bigger animals. Domestic and livestock such a s cattle, sheep, and goats are important in the unfold nf these viruses to people, who could be contaminated by tick bite or by the ingestion of raw milk. Formalininactivated vaccines can be found to be used against tick-borne encephalitis in Eastern Europe. The intently associated Ravivirus of Britain, Eouping sick, is maintained in a tick-grouse cycle and is transmissible to sheep, during which i causes a rapidly f deadly disease. Rarely, louping sick virus is transmitted to people by ticks or occupationally by contact with contaminated sheep tissues, producing a comparatively mild rneningoencephalitis. Tick-Borne Flavivirus Hemorrhagic Fevers the Omsk hemorrhagic fever virus o Siberia, the Kyasanur Forest disease f virus of India, and the Powassan virus of North America and Russia are intently associated to the tick-borne encephalitis viruses however trigger hemorrhagic fever as an alternative. Water voles are the reservoir hosts of Omsk hemorrhagic fever virus, however people are often contaminated by direct contact with the blood or excreta of the muskrat, an animal imported from America in the early 1900s. Rodents are the principal vertebrate reservoir of Kyasanur Forest virus, however monkeys could serve as amplifiers; m,oreover, contaminated ticks are also carried to domestic cattle and goats and the deer and anteIopes in nature reserves, therefore the concentsa tion of human cases acquired alongside cattle tracks i n Mysore State forests. Rocio Encephalitis the flavivirus liable for Rocio encephalitis, first isolated in 1975, has been assnciated with a number of} outbreaks of encephalitis in Brazil. Wild birds are the possible vertebrate reservoir, and potential vectors include Psoroplrzorn ferox and Aidc*s scaprlnrrs. It is endemic in rural Africa, southern Europe and Central Asia, India, and the Far East. Unlike the case with many different flaviviruses, virus can usually be isolated from the blood early in the sickness. The associated Kunjin virus is sort of|is type of} frequent In Australia and infrequently causes encephalitis in people; like West Nile virus, deadly in horses. Hepatitis C Wifh the intr80ductionof delicate assays for screening blood for hepatitis B virlis in the late Nineteen Seventies, it was anticipated that posttransfusion hepatitis could be virtually eliminated, however this was not lo be. The causative agent remained frustratingly elusive for over a decade and has still not been convincingly cultured in zritro nor visualized by electron miscroscopy. NevertheIess, in 1989, a group of mr~lecularbiologists in the United States succeeded in an ambitious task which seemed to many to be unacliievable. Unlike mosquitoes, ticks are present 12 months long} even in temperate ctimates and sometimes stay through more than a single breeding cycle of their host. The eggs of ticks develop successively through phases (larva to nymph to adult), and a blood meal is generally rcqujred at each stage. Tick-borne flaviviruses are handed from one devtl- - - 446 Chapter 26 Flsviuiridne hemophiliacs. Filtration research had indica ted the size of the causative agent to be of the order of 40-50 nm, whereas a buoyant density o 1. Bacterial colonies had been then screened for production of any antigenic polypeptide sequence recognizable in an imrnunoassay by serum taken from chronicalEy contaminated sufferers, assumed to comprise antibody against the putative virus. However, the connection between genotypes and serotypes has yet to be sorted out. Viral Replica tion Little is at present recognized in regards to the replication cycle, as no easy cell culture system has yet been discovered. Pathogenesis and Clinical Progression In many developed nations at present hepatitis A, B, and C are about equally frequent. Acute hepatitis C is clinically related lo hepatitis A and B, a n d the reader is referred back to Chapters 22 and 23 for descriptions.
Generic 5mg prazosin
Thc capsid is composed of a defined number of morphological units t I t i I t - + - t - + -,I " " " Strnlc. The easiest standard viruses encompass a nucleic acid genome and a protein coat. E distinction, Ilrrotrs, such because the agents that trigger the spongiform n enccphalopathies in humans, appear lo be a filamentous protein with no assoc~nlrdl~iucleicacid. Viral Morphology I Physical Methods for Studying Viral Structure 11 has becn k n o w n for many years of} years} that viruses are smaller that1 microorganisms. Only with the acilvcn t of the electron ~nicroscopewas it potential to study the morphology nf vlrulsrs correctly I 1 then grew to become apparent that they vary in s i ~ e from concerning the. S ~ P C f l ~ e of smallest rn~cmclrganismsdown to little bigger than the most important prntcul n~olcculcs. Early elecY ron m~lcrosct~pic research o l viruses by Ruska in 1939-1941 had been cxpnnrlcd d u n ~. Then in 1959 our knowlec-lgk of of viral l i l t rClstruct~~rc transforlned whr*ntrr~,~mfrzril was slnirrirrlt) was applied L L l ~ t o Fig. I t has axes of two-, three-, and fivefold rc)taiional symmetry, passing thrc~ugliits edges, faces, and vertices, respective1 y (Fig. An object with icosahedral symmetry necd not appear angular in outline; the virions of r n a ~ ~ y animal vlauses with icosahedral symmetry appear spherical with a bumpy stlrface. Only certain preparations ol the capsomers can f i t into the faces, edges, and vertices of the viral icosahedron. The capsomers on the faces and edges of adenovirus particles, for exampIe, bond to six neighboring capsomers and are referred to as hexnnrers; those on the verfices bond to 5 neighbors and are referred to as ~u:ufamcvs(Figs. The preparations of capsorners on the capsids o virions of three small icosahedral vlruses arc proven in f Fig. In a number of} picornaviruses examined, the amino acids of each of the three larger structural proteins are packaged so a s to have a wedge-shaped eight-stranded antiparallel P-barrel domarn (Fig. The outer contour of the virion depends on by} the packing of these domains arid on finest way|the method in which} the loops project l r t m the framework. The capsnrners of the parvovirus encompass an unllsilally giant wedge-shaped prokin wilh a @-barrel core, lience the flexibility to kind a 250 A shdl from only h subunits of a s~iiglc O protein. Iligh-rcso~ution stumd ies with picornaviruses and poly omaviruscs havc rcvcalcd that thc capsid proteins have versatile "arms" wliich interlock with arms r j f an adjaccnt structural unit to mediate assembly and stability of the virion. Cations may also stabilize the interface between subunits, and arms exlending from interl i d proteins might interact with proteins crf the outel capsid. The infectivity of most enveloped viruses depends on by} the integrity of the enveIope, however some poxviruses have a n envelope which 1s not needed for infectivity. The genome of[a consultant rnemfi~ ber of most viral famil~es has now been completely sequenced. Several copies of the whole vlral genome might he enclosed within a single particle, or viral particles additionally be} shaped that contain no nucleic acid (empty particles) or which have an ~ncomyletegenome (rlrfeciirv rtrtcr~errrrg~mrfrclrs). An essential rolc fur one class of structural proteins is to present the viral nucleic acid with a protective coat. One of fhe floor proteins bears the ligand for b ~ n d i n g the Jiost ccll receptor mcrlecule. Thc virlons of all to viruses rrf vertebrates contain a number of} totally different proteins, tlie quantity starting from 2 within the easiest viruses to over 100 E the most crjmplex. For viruses n with cuhrc symmetry, the sfructural paotcins farm an icosahedral capsid which sc3rnetimes encloses a n further layer, lor c3clre, composed of various, typically basic histonelike polypeptides which might be} lntirndtely assoc~atedwlth the nucleic acid. Arenavirrls gcnomes consist nf 2 segments, bunyavi~us genomes of three, orthornyxcrvlrus elf 7 or eight (rn totally different genera), and reovlrtrs of 10, 1I, or 12 (in totally different gw7wa). Iiecausc the glycans are synthesized by ccllirlar glycos)rltransfcrases, the sugar cnmpnsllion n l ihe g l y c a ~ ~ s corresp(m"d ffn that oT host cell men~braneglycopr(>teins Vivid Envelope Lip ids I. As a consequence, the compositic>nof the lipids of particular viruses differs in accordance with the coniposition of the membrane lipids of the host cells from which tlicy came Approx~mately 50-60% of the envelope lipid is phospholipid, a n d a lot of the the rest is ldl cholesterol Most lipid found in enveloped viruses is present as a typical l i p ~ d bilayer by which the virus-coded glycoprotein spikes (and occasionally hint amounts of residual cellular membrane proteins) are embedded. Ionic Environment and pH On the entire, viruses are finest preserved in an isotonic setting at physiologic pH, however some tolerate a large ionic a n d pH range. For instance, whereas most enveloped viruscs are inactivated at pH 5-6, rntaviruses heaps of|and a lot of} picomaviruses survive the acidic pl-l of Llie stomach. Lipid Solvents and Detergents Preservation of Viral Infectivity In general, viruses are more delicate than bacteria or fungi to inactivation by physiccil and chemical agents. A knawlcdge of their sensitivity to environis mental cc~nditions due to this fact important for ensuring the preservation of the infectlv~ty vlruses as reference reagents, and in cltnical specimens collected of fur prognosis, properly as|in addition to} for his or her deliberale inactivation for such sensible ends as sterilization, disinfection, and the manufacturing of inactivated vaccines. The infectivity of enveloped viruses is instantly destroyed by lipid solvents such a s ether or chloroform and by detergents l~ke sndlum deoxycholate, so that these agents must be averted in laboratory procedures concerned with sustaining the viabilily of viruses. Surface proteins are denatured witliln a couple of minutes at temperatures of fifty five"-6f1°C, with the result that the virion is no longer succesful o f regular cellular attachment andlor uncoating At ambient temperature thc rate o f decay of infectivily is slower however vital, particularly in the summer or within the trnp~cs. To preserve infectivity, viral preparations must due to this fact be stored at low tcnipcsattrre; 4°C (we! Enveloped vurions, nutably those r l f rcspirattrry syncylial virus, are additionally vulnerable to repeated freezlng and thawing, most likely disruption of the virion by ice cryslals. This poses probletms in [h e callccricln and transportation of scientific specimens. The primary standards for dclirieatinrr of families are (1) the kind of nucleic acid that constitutes the genome (see Table 1-2), (2) the strategy of viral replication, and (3) the morphology of the virion. Subdivision of familles into genera relies on cr~teriathat vary for various families Genera, normally in outlined by substantial d~fferences their genornes, contain from one to over a hundred species. Nomenclature There is nice proof to point out that all one|that each one} organisms are infectable by viruses: vcrtcbrate and invertebrate animals, vegetation, algae, fungi, protozoa, and bacterra; Indeed, each species of animal, bacterium, and plant that has been intensively scarched lias yielded numerous totally different viruses belonging to a number of} viral fnmilies. In this book, nonetheless, wc arc concerned solcly with the vlruses that trigger disease in humans. Some of these (called arbov~ruses) additionally replicate in bugs, ticks, or different arthropods Sevcral hundred disting~tishableviruses have been recovered from humans, the most effective studied vertrbratc host, and new ones are being discovered each yc3ar Somewhat fcwer have bccn recovered from each of the common specics of farni and companion animals and from the generally used laboratory anirnals. Families are named with the suffix -nindna, subfamilies with the suffix - z ~ i r i ~ nand genera with the suffix - z) i r ~ r s. Currently, viral species are designated by vernacular terms, f o instance, measles virus. Most species have a narrow host range and replicate preferentially in d~viding cells. Members of the genus I"rrrr~rrz~rrus infect sperles nf a n ~ ~ n a land one parvov~rus(D19, the one member of Ihe s, genus E! Members of the genus Drla,rrdc~ilrrwsare defect~ve viruscs, which depend a n adenovirlls (or, experimentally, a k~crpesvi~rus) replication. Virions of Pni~t1lotrrnz)irtls in diameter and have a bigger genome (8 kbp) which can persisl in reworked cells in an eyisomal kind. Human hcrpesvirus h lids brcn allocaterl to tlie subCarnilv Hcfnltrrpclsn1rrfurr7,genus Rosc~~~/nzJlrlrs. A characteristic of aIl hcrpesvirus infections is 11fe-long persistence nf the virus within the physique, normally in latent kind. Excretion, particularly in saliva or genitaI secretions, might occur continuously or rnterm~ttentlywithout disease, or episodes of recurrent scientific disease and recurrent excretion might occur years after the initial an infection, particularly following immunosuppression. NearIy 50 seroIogically distinct kinds of human adennviruses are at present recognized; all share a gaggle antigen with adenovirus scrntypes infecting different mammals (the genus Mast~d~rrovirus). Many infections are characterised by prolonged persistence and additionally be} react~vated immunosuppression. The virions arc brick-shaped, measuring about 250 by 200 by 200 nm in all genera that trigger human infections besides Pnrnpoxz~irrrs, the vir~ons which are ovoid and measure 260 by one hundred sixty nm. The genus Ortlm/mxuirus consists of cowpox, ectromelia (mousepox), rabbitpox (a variant of vaccinla virus), and monkeypox viruses. Variola virus, which brought on human smallpox, and vaccinia virus, used to management that disease, alsa, belong to this genus. MolIuscum contagiosum (gentrs Mollusc~yoxuirtrs)is a specificaPly human virus, and the genus Ynfnpo-uz~irlrs confains two viruses of African wildlife, yabapoxvirus and fanapoxvirus, both of which can infect humans. The herpesviruses replicate within the nucleus and m a t ~ l r e budding through the nuclear by membrane, thus buying an envelnpe. This giant family consists of a number of} important human1 patlicrgens and has been divided into three subfamilies.
Cheap 2.5mg prazosin
Effect of filamentous bacteria on membrane fouling in submerged membrane bioreactor. Filtrate flux in crossflow microfiltration of dilute suspension forming a extremely compressible fouling cake-layer. Influence of bacterial extracellular polymers on the membrane separation activated sludge course of. Direct Potable Reuse: Benefits for Public Water Supplies, Agriculture, the Environment, and Energy Conservation. Anaerobic metabolism of propionate by polyphosphateaccumulating organisms in enhanced organic phosphorus removing systems. Membrane bioreactor fouling in sub-critical filtration conditions: a neighborhood crucial flux concept. Analysis of characteristics of microbial communities in membrane bioreactor and standard activated sludge course of. Huan jing ke xue= Huanjing kexue/[bian ji, Zhongguo ke xue yuan huan jing ke xue wei yuan hui" Huan jing ke xue" bian ji wei yuan hui. Effluent high quality of a traditional activated sludge and a membrane bioreactor system treating hospital wastewater. Effect of high salinity on activated sludge characteristics and membrane permeability in an immersed membrane bioreactor. Performance of a bioreactor with submerged membranes for cardio remedy of municipal waste water. A comparative research on the anaerobic membrane bioreactor performance during the remedy of domestic wastewaters of varied origins. Effects of activated sludge properties on water flux of ultrafiltration membrane used for human excrement remedy. Investigation of bacterial range in membrane bioreactor and standard activated sludge processes from petroleum refineries utilizing phylogenetic and statistical approaches. A comparative pilot-scale research of the performance of typical activated sludge and membrane bioreactors under limiting working conditions. WateReuse Association 2008 Property Owner and Homeowner Market Perception Study: Final Report. Comparison performances of membrane bioreactor and standard activated sludge processes on sludge discount induced by Oligochaete. A research of the microbial high quality of gray water and an evaluation of remedy technologies for reuse. Individual and combined impacts of suspended (SiO2 microspheres) and dissolved (Aldrich humic acid) foulants on permeate flux and virus removing were determined and in contrast. Instead, feed water composition and membrane pore size together govern virus removing with fouling mechanisms enjoying in} a key mediating role: pore blockage improves virus removing whereas cake formation can both increase or lower virus removing depending on cake properties. Introduction More than 150 forms of enteric viruses have been present in contaminated waters (Leclerc et al. Because of their low infectious dose and lengthy survival within the setting viruses pose a considerable menace to human health. Although some pathogen removing happens during wastewater remedy, even superior technologies may not provide an absolute barrier for viruses. Multiple research evaluated virus removing as a perform of membrane and feed properties; some of this work has employed bacteriophages as human virus surrogates. High removals of T4 coliphage have been reported and partly attributed to the formation of a cake layer fashioned on membrane floor (Lv et al. Farahbakhsh and Smith (2004) investigated coliphage removing from secondary effluent of wastewater remedy plant by microfiltration membrane and reported that fouled membranes rejected viruses more successfully. Composition of the feed water (pH, ionic energy, presence of divalent actions and organic matter) and pretreatment were advised as key factors governing virus removing (van Voorthuizen et al. In order to isolate viruses from cell particles, virus suspension was centrifuged at 400 g for four min, and then filtered via zero. Membrane preparation Three forms of hollow fiber membranes were used on this research. The answer was mixed utilizing a magnetic stir bar for seventy two h, and then filtered via zero. Particle size distribution within the inventory was measured utilizing Mastersizer 2000 (Malvern). Membrane filtration experiment the schematic of the experimental unit is shown in Figure 3-1. Diffusers were placed at the bottom of the feed tank to provide air and blend the feed water. Peristaltic digital pump (model 07523-80, MasterFlex L/S) was used to apply transmembrane stress. Permeate move fee and transmembrane stress were measured utilizing a digital move meter (model 106-4-C-T4-C10, McMillan) and digital stress sensor (Cole-Parmer, 68075-00), respectively. A LabView code was developed to record readings from the flowrate and stress sensors and to management the move fee of the pump. Three experiments with feeds of various compositions were carried out with every sort of hollow fiber membranes. The transmembrane stress was utilized and filtration was carried out in a constant flux regime ( = 50 mL/min; = 2. Transmembrane stress was utilized and the fouling test was carried out in constant flux regime (Q = 50 mL/min; j = 2. Feed and permeate samples were taken when the move fee reached the target value of fifty mL/min during Stage 2, and every 2 h afterward. The high foulant concentrations were used to accelerate membrane fouling and shorten the time of information gathering. Values of crossing point, Cp, were mechanically generated by 103 the LightCycler software program. Membrane problem checks To quantitative assess the retention capacity of the membranes and complement nominal pore size information supplied by the producers (Table 3-1), membrane problem checks were carried out utilizing suspensions of monodisperse spherical probe particles. The problem checks were carried out utilizing the same filtration rig (except that a 1 L Nalgene bottle was used as a feed vessel) as in virus filtration research (Section 2. For every probe/membrane combination, three permeate samples were collected 11, thirteen, and 15 min into the problem test and the log removing (or rejection) value was calculated as a median for these three samples. Particle concentrations within the feed and permeate were determined spectrophotometrically (Multi-Spec 1501, Shimadzu). The absorbance was measured at = 197, 202, 236, and 274 nm with 50, 100, 300, and 500 nm probes, respectively. Characterization of membranes and model foulants Particle size distributions for SiO2 suspension and answer of humic acid are shown in Figure 3-2. There was approximately an order of magnitude distinction in size between the silica microspheres and humic acid aggregates. As a management measure, all authentic and diluted samples were analyzed for comparison. The dilution factor was taken into consideration during the virus removing calculation afterward. Membrane fouling and transmembrane stress buildup Figure 3-3 illustrates changes within the transmembrane stress with filtration time. In these constant flux experiments, the 106 permeate move fee was maintained at 49. To verify that pore blockage and cake formation were indeed operative fouling mechanisms, we carried out a separate set of constant stress dead-end filtration experiments and utilized blocking legal guidelines (Hermia 1982) to the permeate flux information generated in these checks. The checks were carried out within the absence of aeration to fulfill assumptions behind the blocking regulation concept. The unfavorable slope is defined by the combined pore blockage-cake filtration model (Ho and Zydney, 2000) as resulting from the simultaneous pore blockage and formation of the cake over blocked areas of the membrane. Partial blockage decreases efficient pore size whereas the pores may be} "utterly blocked" may permit permeation of water however not virus passage. The second mechanism is the possible increase of the transmembrane differential in virus concentration outcome of} cake formation. The greater transmembrane differential of virus concentration leads to enhanced virus transport across the membrane and decrease virus removing.
Purple Loosestrife. Prazosin.
- Diarrhea, intestinal problems, menstrual (period) complaints, inflammation, infection, varicose veins, bleeding gums, hemorrhoids, eczema, and other conditions.
- How does Purple Loosestrife work?
- Dosing considerations for Purple Loosestrife.
- What is Purple Loosestrife?
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96403
Trusted prazosin 5 mg
However, for sensible purposes, the outcomes of this check when performed at the bedside are sometimes inconclusive and unreliable, and this has disenchanted a number of} generations of ophthalmologists and neurologists since Wernicke popularized the check in 1883. Poorly Reacting Pupils from Midbrain Disease Fixed dilated pupils and pupils that react poorly to each light and close to stimuli could also be} produced by damage to the visceral oculomotor nuclei and their efferent fiber tracts. Other midbrain lesions damage the afferent input to the Edinger-Westphal nuclei or trigger mixed afferent and efferent damage. With a bright light stimulus, 4 patients had impairment of each light and close to reactions, two patients had markedly impaired light reactions and comparatively intact responses to close to stimuli (classic lightnear dissociation), and two patients had relatively intact light reactions but impaired responses to close to stimuli (inverse Argyll Robertson pupils). With a dim light stimulus, 5 patients had impairment of reactions to each light and close to stimuli and three patients had impaired light reactions but relatively intact reactions to close to stimuli. It seems that varied mixtures of defects involving the pupil light reflex, the pupil close to response, and accommodation can occur with lesions of the rostral midbrain. Bilateral complete inner ophthalmoplegia, when caused by damage to the rostral oculomotor nuclear advanced, hardly ever happens in isolation. Lesions that produce these adjustments must be located in the periaqueductal gray matter close to the rostral end of the aqueduct. Subsequent investigators confirmed this observation and reported similar paradoxical pupillary responses in children and adults with congenital achromatopsia, blue-cone monochromatism, and Leber congenital amaurosis (109,110). In addition, such responses often occur in patients with optic disc hypoplasia, dominant optic atrophy, and bilateral optic neuritis. A cautious slit-lamp examination to assess the health and integrity of the iris stroma and muscles is an important step in the evaluation of anisocoria. One can presume the issue lies someplace alongside the parasympathetic pathway to the sphincter muscle. Common etiologies include an acute tonic pupil, oculomotor nerve palsy, or pharmacologic blockade. If each pupils have a great light reflex and the degree of anisocoria decreases in bright light. The evaluation of anisocoria is described in the following sections and outlined in Figure 16. In dim light or darkness, almost 20% of the conventional population has an anisocoria of 0. This type of anisocoria is thought by a number of} names, together with physiologic anisocoria, easy central anisocoria, important anisocoria, and benign anisocoria. The degree of pupillary inequality in physiologic anisocoria might change from day to day and even from hour to hour, nonetheless. The anisocoria usually diminishes barely in bright light, maybe as a result of|as a outcome of} the smaller pupil reaches the zone of mechanical resistance first, giving the bigger pupil an opportunity to make up the size distinction (117). Occasionally, a reversal of physiologic anisocoria is seen, a phenomenon termed ``seesaw anisocoria' (112,116). In the latter case, the anisocoria usually may be traced again to infancy or early childhood. Horner Syndrome When the sympathetic innervation to the attention is interrupted, the retractor muscles in the eyelids are weakened, allowing the upper lid to droop and the decrease lid to rise. The dilator muscle of the iris is also weakened, allowing the pupil to become smaller, and vasomotor and sudomotor control of parts of the face could also be} lost. This combination of ptosis, miosis, and anhidrosis known as as} Horner syndrome (Fig 16. Although he was not the primary to Ё report the scientific condition, his meticulous and scientifically substantiated account of the scientific results of cervical sympathetic paralysis has firmly connected his name to this syndrome (118). In the French literature, this condition known as as} the Claude Bernard-Horner syndrome to honor the work of Claude Bernard in 1852 on the physiology of the sympathetic nerves. Although Horner and Bernard typically are credited with identifying the scientific signs of oculosympathetic paresis, these signs were first produced experimentally in the dog by Francois Pourfour du Petit in 1727. Pourfour du Petit was ё never acknowledged for these contributions; nonetheless, Pourfour du Petit syndrome is the term used for the mixture of Figure 16. The affected person was a 5-year-old boy whose dad and mom noted that the best pupil was bigger than the other. The anisocoria was extra apparent in dark than in light, and each pupils reacted usually to light stimulation. A, this 3-year-old boy was noted by his dad and mom to have intermittent anisocoria, with the best pupil bigger than the left. The anisocoria was higher in darkness than in light, and each pupils reacted usually to light stimulation. This eponym is exceptional as a result of|as a outcome of} Pourfour du Petit never actually stimulated the sympathetic nerve in his experimental animals (119). The upper eyelid is barely drooped because of paralysis of the sympathetically innervated easy muscle (Muller muscle) that contributes to the Ё place of the opened upper eyelid. Similar easy muscle fibers in the decrease eyelid also lose their nerve provide in Horner syndrome; thus, the decrease lid usually is barely elevated, producing an ``upside-down ptosis,' further narrowing of the palpebral fissure, and an obvious enophthalmos. That the enophthalmos is apparent rather than real has been confirmed by a number of} studies (119,121,122). The palsy of the iris dilator muscle in Horner syndrome allows unantagonized motion of the iris sphincter, producing a smaller pupil. However, in some patients in the setting of intense emotional excitement, the pupil on the aspect of the sympathetic lesion turns into bigger than the conventional pupil. This ``paradoxical pupillary dilation' is caused by denervation supersensitivity of the dilator muscle to circulating and topical adrenergic substances. Thus, reversal of anisocoria following topical instillation of apraclonidine has been seen in patients with unilateral Horner syndrome (123,124). Any anisocoria, when caused by weak point of a single iris muscle, will increase in the path of motion of that muscle. With a unilateral oculosympathetic defect, the weak point of the dilator muscle in the affected eye (and resultant anisocoria) is most obvious in darkness. Conversely, the anisocoria almost disappears in light as a result of|as a outcome of} the conventional motion of each sphincters (oculoparasympathetic activity) constricts the pupils to almost equal sizes. In regular room light, the degree of anisocoria in Horner syndrome is rather small, on the order of 1. Furthermore, when a affected person is fatigued or drowsy, the size of the pupils and the degree of anisocoria diminish as the hypothalamic sympathetic outflow to each eyes subsides and uninhibited parasympathetic outflow augments. Paresis of the iris dilator muscle results in a smaller resting pupil size (miosis) and in addition in impaired pupillary motion during dilation, referred to as dilation lag. The regular pupil will immediately dilate, but a number of} seconds will elapse before the Horner pupil begins to dilate. The dilation dynamics of a normal pupil compared with a Horner pupil have been well documented utilizing steady recording pupillography (119). In the primary second of darkness, each pupils synchronously enlarge a small degree, presumably from acute inhibition of parasympathetic impulses. In the following few seconds, the conventional pupil, stimulated by an active burst of sympathetic discharges, quickly dilates, whereas the Horner pupil, denervated of sympathetic impulses, hardly moves. This results in an rising anisocoria during in the first 5 seconds or so of darkness. Thereafter, the Horner pupil slowly dilates from lowering parasympathetic tone and catches up in size to the conventional pupil. Thus, if each pupils are noticed simultaneously for 1520 seconds after turning off the room light, one sees an preliminary enhance in the degree of anisocoria, followed by lowering anisocoria (Fig. A psychosensory stimulus corresponding to a sudden noise will trigger a normal pupil to dilate. When looking for dilation lag in darkness, interjection of a sudden loud noise just as the lights go out tends to augment the preliminary enhance in anisocoria when a unilateral oculosympathetic defect is current. There remains controversy about which facet of pupillary reflex dilation in darkness finest identifies the impaired dilation dynamics of a Horner syndrome. Taking Polaroid photographs 5 seconds after the lights go out and once more after 15 seconds of darkness is a straightforward and available Figure 16. Pupillogram of a affected person with a left Horner syndrome (solid line is a normal pupil; broken line is a Horner pupil). As the pupils redilate in the darkness, rising anisocoria seen in c of} the relative inactivity of the Horner pupil. Addition of a sensory stimulus after the heart beat|the heartbeat} of light further enhances the uneven dilation dynamics (d) between the conventional pupil and the Horner pupil. Dilation lag in a affected person with a left Horner syndrome, noticed utilizing regular flash colour pictures.
Purchase prazosin 2.5 mg
Parameters measured include (1) amount of weight bearing on either foot, (2) sway with upper body motion, (3) rhythmic weight shift with body motion in all planes, (4) limits of stability whereby patients are supplied a mechanical drive toward which they try to shift their weight to compensate to maintain balance, and (5) weight shifts throughout movements such as transfers from sitting to standing and walking. Proprioceptive responses may be be} improved via managed mobility, improved anterior-posterior weight shifts, growing trunk power and vary of motion, as well as|in addition to} growing midline symmetry and transitional movements. Pharmacologic remedies include meclizine and dimenhydrinate, which may trigger sedation. Transdermal scopolamine patches can also be|may additionally be|can be} used and are believed to trigger much less sedation. Cognition/Speech Deficits Deficits in cognition and speech occur; they differ in type and severity by the situation and kind of tumor, anticancer treatment, pre-morbid cognitive baseline, and co-morbid medical conditions. Cognitive deficits come up from tissue injury caused by the tumor itself, surgical resection, and the acute effects of radiation and chemotherapy (Silberfarb, 1983). Emotional sequelae such as depression and nervousness are common, might worsen cognitive features, or are overlooked in the presence of cognitive deficits. Coexisting medical conditions such as hypothyroidism are treatable and should be thought of in the differential analysis of cognitive impairment. Cognitive deficits are most often seen in areas involving memory, consideration, initiation, and psychomotor retardation. Primary interventions for memory impairment include memory aids and the usage of} visual imagery. Cognitive remediation applications educate patients adaptive strategies and compensatory methods. Psychostimulants have been reported to be helpful in treating psychomotor retardation, depression, and opioid-induced drowsiness (Bruera et al. Dopamine agonists and stimulating antidepressants enhance attentional dysfunction, particularly distractibility and problem focusing, in larger level patients (Gualtieri et al. Bromocriptine can be effective for motor aphasias and neglect in some patients (Grujic et al. Carbamazepine, tricyclic antidepressants, trazodone, amantadine, and -blockers have been prescribed to handle agitation in patients with traumatic brain injury (Brooke et al. In contrast to aphasia, naming, fluency, repetition, and comprehension are normal in dysarthric conditions, and dysarthric patients can read and write with out errors. Other problems such as apraxia, visual constructive difficulties, and neglect need to be thought of in the differential analysis of communication dysfunction. Back ache is a frequent symptom and in 10% of cases may be be} due to of} spinal instability (Gilbert et al. Any tumor can metastasize to the backbone and trigger sufficient destruction to produce spinal instability. The thoracic backbone is the segment most commonly involved, followed by lumbosacral and then cervical vertebral levels (Casciato and Lowitz, 1983; Schlicht and Smelz, 1994). Spinal wire compression ultimately occurs in approximately 5% of patients with cancer (Casciato and Lowitz, 1983). Abrupt neurologic deterioration from spinal wire involvement might occur from rapidly growing lesions in the extradural space. By the time treatment is pursued, as many as 50% of patients might not ready to|be succesful of|have the ability to} ambulate, and 10% to 30% may be be} paraplegic (Shapiro and Posner, 1983; Shaw et al. Symptoms include weak spot, incoordination, gait abnormality, spinal or radicular ache, paresthesias, sensory disturbances, autonomic disturbances, as well as|in addition to} bowel or bladder problems. Pinprick and deep ache sensation is commonly retained till later the center of|in the midst of} the disease. Motor involvement typically occurs earlier than sensory involvement with epidural extension (Galasko, 1999). With radiation treatment alone, ambulation is maintained in 79% of patients in the event that they} were ambulatory earlier than treatment and in 42% with paraparesis. In 20% to 25% of patients, significant neurologic deterioration was noted through the course of treatment with radiation alone (Findlay, 1984). Significant neurologic deterioration and progressive spinal instability require a neurosurgical session. Tetraplegia, whether full or incomplete, occurs with spinal wire involvement at T1 or above. Below this level, accidents more commonly result in paraplegia, conus medullaris syndrome, or cauda equina syndrome. Local ache is often described as constant and aching, whereas radicular ache is classically sharp and shooting. Referred ache can be either aching or sharp and at a location distant to the involved web site. Pain can also occur with epidural involvement; this ache worsens with Valsalva maneuvers, coughing, and neck and back flexion (Gilbert et al. Findings Associated with Better Prognosis for Functional Recovery Following Cord Compression · Diagnosis of myeloma, lymphoma, or breast cancer · Slow evolution of signs or early neurologic indicators · Ambulatory standing at time of analysis of spinal wire involvement 475 additionally occur, which is often characterized by midback ache and dysesthetic ache in the lower extremities. Such ache is normally handled with steroids, anticonvulsants, and tricyclic antidepressants. Rehabilitation Considerations With use of radiation treatment and posterior laminectomy, the general outcomes were that full paraplegia patients not often recovered, but those who were ambulatory remained ambulatory and approximately one-half of patients with incomplete paraplegia regained ambulation (Posner, 1995). Recovery tends to occur first in the area of sensory disturbance, followed by motor abnormalities (Casciato and Lowitz, 1983; Schlicht and Smelz, 1994). Clinical onset might contain symmetric paresthesia or shock-like sensations in a nondermatomal pattern from backbone to extremities (Leibel et al. Conversely, delayed myelopathy is irreversible, has a latency interval of 9 to 18 months, and customarily occurs inside 30 months (Dropcho, 1991). The latency interval is decreased with elevated radiation dose and in youngsters (Leibel et al. The onset of signs begins with lower extremity paresthesias and is followed by sphincter disturbance. Partial Brown-Sйquard syndrome (motor weak spot on one aspect and a few sensory adjustments on the contralateral side) might occur beneath the level of injury. When spinal metastasis has occurred, different bony areas may be affected, particularly the pelvis, femur, ribs, and skull. Rigid thoracic-lumbar-sacral orthoses with a "clamshell" design can provide good exterior help but is probably not|will not be} tolerated by patients with painful rib or iliac crest bony involvement or by these with fragile pores and skin due to of} steroids or chemotherapy (Garden and Gillis, 1996). The rehabilitation staff should think about metastatic disease as a possible etiology for brand spanking new|for brand new} ache or weaknesses that come up through the course of therapy. Adequate ache management is essential and allows patients to participate in therapy. Rehabilitation Issues in Cancer and Treatment-Related Myelopathy Pain Motor loss and problem with ambulation and transfers Sensory loss Autonomic dysreflexia (T6* or above) Orthostatic hypotension Neurogenic bowel and bladder Spasticity Pressure ulcers at sacrum, heel and trochanters Spinal instability (with spinal column destruction) Altered weight-bearing, restricted lower extremity vary of motion *T6, the sixth thoracic spinal wire level. Pharmacologic choices include opiates, nonsteroidal anti-inflammatory agents, tricyclic antidepressants, numerous antiepileptics, steroids, and different drugs such as -blockers and -adrenergic agonists. Nontraditional interventions such as acupuncture have additionally been used with success. In patients with spinal hardware, worsening ache might indicate malfunction or loosening of hardware or an infection in the surrounding tissues. Patients might attempt to void on their very own; however, postvoid residual volumes must be checked on quantity of} events to affirm full emptying. The goal is to have 350 to four hundred cc of urine in the bladder at any time to avoid overdistension, detrusor muscle injury, and retropropulsion of urine into the ureters. With chronically elevated bladder volumes, bladder flaccidity might occur secondary to detrusor muscle injury. Fluid intake should initially be restricted to 2 L per day if different medical concerns allow. Patients with a wire injury at C7 or beneath can normally study to independently carry out such a program. Condom catheters may be be} used by males with hyperactive bladder (without dyssynergia) or these with normal bladder perform but with incontinence due to of} impaired cognition or mobility. Bowel Management A bowel program (more particulars comply with in a later section) with fiber, stool softeners, and digital stimulation, together with even handed use of suppositories, laxatives, and enemas should be began. Patients should be allowed to sit on a commode at common instances to facilitate bowel movements. Establishment of a set pattern (daily or every different day) for evacuation will minimize constipation and incontinence. Management of Autonomic Dysreflexia Autonomic dysreflexia is a medical emergency that happens when a affected person manifests a massive sympathetic discharge in response to a noxious stimulus. The medical presentation is that of an anxious affected person with paroxysmal hypertension, nasal congestion, sweating above the level of lesion, facial flushing, piloerection, and reflex bradycardia.

Safe 2.5 mg prazosin
Within the cavernous sinus, the sympathetic fibers go away the internal carotid artery, join briefly with the abducens nerve, and then go away it to join the ophthalmic division of the trigeminal nerve, entering the orbit with its nasociliary branch (171,172). The sympathetic fibers within the nasociliary nerve divide into the 2 lengthy ciliary nerves that travel with the lateral and medial suprachoroidal vascular bundles to reach the anterior segment of the attention and innervate the iris dilator muscle. Most lesions that injury the postganglionic sympathetic neuron are vascular lesions that produce headache or ipsilateral facial pain as well and sometimes are lumped under the clinical description of a ``painful postganglionic Horner syndrome. Lesions of or along the internal carotid artery are a typical reason for a painful postganglionic Horner syndrome, the most typical being a traumatic or spontaneous dissection of the cervical inner carotid artery. In 146 such patients, a Horner syndrome was the most typical ocular finding (44%) (173). In half of these cases, the Horner syndrome was the preliminary and sole manifestation of the carotid artery dissection. In the opposite half, an associated ocular or cerebral ischemic occasion occurred inside a mean of seven days of the Horner syndrome, emphasizing the need for early recognition and analysis of this reason for Horner syndrome. Pathologic circumstances of the internal carotid artery apart from dissection that are be} related to a Horner syndrome embody aneurysms, severe atherosclerosis, acute thrombosis, fibromuscular dysplasia, and arteritis (174). Mass lesions within the neck that can compress the carotid sympathetic neuron embody tumors, inflammatory plenty, enlarged lymph nodes, and even an ectatic jugular vein (175,176). In the deep retroparotid space and around the jugular foramen, oculosympathetic fibers are in close proximity with several of} lower cranial nerves. Lesions on this area of the neck, normally trauma, tumors, heaps more and plenty}, end result in|may find yourself in|can lead to} a Horner syndrome related to ipsilateral paralysis of the tongue, soft palate, pharynx, and larynx. This combination of paralysis of the cervical sympathetics and the last 4 cranial nerves (the glossopharyngeal, vagus, accent, and hypoglossal nerves) is known as} Villaret syndrome (177). Tonsillectomy, intraoral surgery, peritonsillar injections, and accidental punctures through the soft palate are a few of the the} etiologies which were reported to trigger a postganglionic Horner syndrome from injury to the superior cervical ganglion (178,179). A basal skull fracture involving the petrous bone can injury the postganglionic sympathetic fibers within the carotid canal, producing a postganglionic Horner syndrome related to an ipsilateral abduction deficit, facial palsy, and/or sensorineural listening to loss (abducens, facial, and vestibulocochlear cranial nerves) (180). The occurrence of an abducens palsy and a postganglionic Horner syndrome (Parkinson sign) with out other neurologic signs ought to increase suspicion of a cavernous sinus lesion (181183). In such cases, the anisocoria is minimal or absent despite the impaired gentle reaction of the affected pupil, and pharmacologic testing could be the only means to detect an underlying sympathetic paresis (184). Cluster headaches are severe lancinating unilateral headaches that normally happen in middle-aged men. A postganglionic Horner syndrome happens in 522% of patients with cluster headache (185,186). Cluster headache is thought to be a vasospastic course of affecting the carotid arterial system. Raeder paratrigeminal neuralgia is an eponym used for a painful postganglionic Horner syndrome characterized by a persistent ipsilateral trigeminal neuralgia and/or trigeminal nerve dysfunction. The hydroxyamphetamine check can be used to assist the differentiation between a postganglionic and a preganglionic or central Horner syndrome (188190) (Fig. Hydroxyamphetamine releases saved norepinephrine from the postganglionic adrenergic nerve endings, producing variable mydriasis in normal subjects (191). A lesion of the postganglionic neuron leads to lack of terminal nerve endings and their stores of norepinephrine; thus, hydroxyamphetamine has no mydriatic impact. With lesions of the preganglionic or central neuron, the postganglionic nerve endings, although nonfunctioning, stay structurally intact. Thus, the pupil dilates absolutely and may even become bigger than the opposite pupil from upregulation of the postsynaptic receptors on the dilator muscle. A postganglionic Horner pupil sometimes dilates in response to topical hydroxyamphetamine (false-negative result) when patients are examined within the first week of sympathetic injury before the stores of norepinephrine at the presynaptic nerve endings have been depleted (192). Hydroxyamphetamine hydrobromide 1% (Paredrine) is usually used within the United States but is difficult to get hold of or unavailable in other international locations. Both tyramine hydrochloride 5% and hydroxymethylamphetamine (Pholedrine) have a mode of action just like that of hydroxyamphetamine and serve equally well as agents for a localizing pharmacologic check (193,194). A smaller pupil that fails to dilate to each cocaine and hydroxyamphetamine most likely has a lesion of the post- Figure sixteen. B, forty five minutes after conjunctival instillation of 2 drops of 1% hydroxyamphetamine answer (Paredrine) in every eye, each pupils are dilated, indicating an intact postganglionic neuron. D, forty five minutes after conjunctival instillation of two drops of 1% hydroxyamphetamine answer in every eye, only the proper (normal) pupil is dilated. Such a pupil ought to dilate to a weak, direct-acting topical adrenergic drug, similar to a 1% answer of phenylephrine hydrochloride or a 2% answer of epinephrine due to of} adrenergic denervation supersensitivity of the iris dilator muscle. Indeed, such a pupil not only will dilate but also will become bigger than the opposite normal pupil. Occasionally, this check is used to differentiate a mechanically restricted pupil. It is that this last group that always results from an underlying neoplasm or critical neurologic illness. Other reported etiologies embody spinal twine tumors, brachial plexus trauma, intrathoracic aneurysm, embryonal cell carcinoma, rhabdomyosarcoma, thrombosis of the internal carotid artery, and brain stem vascular malformations (196,198). Thus, an acquired Horner syndrome in a child with no prior surgical historical past, even when the finding is isolated, warrants instant further investigation. This is particularly important for neuroblastoma because of|as a outcome of} youthful age (less than 1 year) is strongly correlated with better outcome. The atropinic flush is current only on the facet of the face opposite the Horner syndrome. Patients with a congenital Horner syndrome have ptosis, miosis, facial anhidrosis, and hypochromia of the affected iris (119,199). Even a child with very blue eyes normally has a paler iris on the affected facet from impaired growth of iris melanophores, causing hypochromia of the iris stroma. This happens whether or not the lesion is preganglionic or postganglionic due to anterograde transsynaptic dysgenesis (200). Children with naturally curly hair and a congenital Horner syndrome have straight hair on the facet of the Horner syndrome (201). The reason for this abnormality is unclear, but it in all probability relates to lack of sympathetic innervation to the hair shafts on the affected facet of the head. Parents of an infant with congenital Horner syndrome typically report that the infant develops a hemifacial flush when nursing or crying. The flushed facet in all probability is the normally innervated facet that appears dramatically reddish when seen in opposition to the opposite facet with pallor from impaired facial vasodilation and maybe overactive vasoconstriction as well. In other words, hemifacial flushing in infants is doubtless to|prone to} be opposite the facet of a congenital Horner syndrome (202,203). Sometimes, a cycloplegic refraction unexpectedly solutions the query by producing an atropinic flush. Some patients with congenital Horner syndrome have clinical proof that indicates a preganglionic lesion. Possible explanations embody an embryopathy instantly involving the superior cervical ganglion, injury to the vascular supply of the superior cervical ganglion, and transsynaptic dysgenesis of the superior cervical ganglion following a defect located more proximally within the sympathetic pathway (200,204). Birth trauma in all probability is the most typical etiology of congenital Horner syndrome (196). Use of forceps, historical past of shoulder dystocia, and fetal rotation can lead to injury of the sympathetic plexus along its course in the neck or close to the thoracic outlet. Associated higher extremity weak point is indicative of concomitant injury to the ipsilateral brachial plexus (200) (Fig. Neuroblastoma was present in certainly one of 31 congenital cases (``congenital' being outlined as a Horner syndrome detected before four weeks of age) (196). However, in uncommon instances, a pharmacologic agent produces anisocoria by stimulating the parasympathetic system, thus producing exhausting and fast|a set} miotic pupil by which the anisocoria is greater in darkness. In such cases, a 1% answer of tropicamide usually fails to dilate the pharmacologically constricted pupil. Pharmacologic Inhibition of the Iris Dilator Brimonidine tartrate is an alpha-2-adrenergic agonist that presumably decreases iris dilator action by its impact at the presynaptic alpha-2 inhibitory receptors of postganglionic sympathetic neurons. Anisocoria Greater in Light Damage to the Preganglionic Parasympathetic Outflow to the Iris Sphincter the efferent pupillomotor pathway for pupillary constriction to gentle and close to stimulation begins within the mesencephalon with the visceral oculomotor (Edinger-Westphal) nuclei and continues by way of the oculomotor nerve to the ciliary ganglion. The postganglionic impulses are carried through the brief ciliary nerves to reach the iris sphincter (see Chapter 14). Because accommodative impulses start in the identical midbrain nuclei as pupilloconstrictor impulses and comply with the identical peripheral course to the attention, accommodative paralysis regularly accompanies pupillary paralysis in lesions of the efferent parasympathetic pathway to the iris sphincter.
Purchase 2.5 mg prazosin
The most common form of prophylaxis is immunization with a confirmed vaccine, hence, the supply of efficient immunizations and/or different medicines. At a minimum, eight various factors are taken into account in a risk assessment for work with a microorganism and weighed towards each other to determine what level of risk the microorganism presents. The subsequent section of this essay describes how the results of a risk assessment are categorized. In turn, the chance group by which an individual microorganism is placed informs the appropriate biosafety containment precautions warranted for the planned activities with that microorganism. Risk Categorizations for Microorganisms the results of the chance assessment help to classify etiologic agents in groups in accordance with the extent of hazard they present to humans, animals, the surroundings, and community. Appropriate authorities authorities classify pathogenic microorganisms into 4 categories decided by the infections they trigger and the seriousness of their harm to the individual and the community as an entire. These risk group categories guide choices about the level of biosafety applicable for work with infectious pathogens. For instance, strict precautions could be taken with materials originating directly from field samples. Pathogenic microorganisms in Risk Group 1 are thought-about of high risk to the individual and to the community. Such microorganisms normally trigger severe human or animal illness and can be readily transmitted from one particular person to another, directly or not directly. For instance, the causative agents for Marburg virus, Ebola virus, Congo-Crimean hemorrhagic fever virus, and Jenin virus (visceral leishmaniasis) fall into Risk Group 1. Pathogenic microorganisms are categorized in Risk Group 2 occasion that they} present high particular person risk, however low risk to the community. Sometimes, efficient treatment and preventive measures can be found for these illnesses. Working from this technique of classification, pathogenic microorganisms in Risk Groups 1 and a couple of|and a pair of} are collectively referred to because the "highly pathogenic microorganisms. Risk Group 3 refers to pathogens that can trigger human or animal illness however are unlikely to be a severe hazard to laboratory workers, the community, livestock, or the surroundings. Laboratory exposures may trigger severe infection, however efficient treatment and preventive measures can be found and the chance of further unfold of infection is limited. To illustrate, Hepatitis B virus, Salmonella, and Toxoplasma spp are categorized in Risk Group 3. Pathogenic microorganisms in Risk Group 4 present low risk to the individual and the community. Risk Group 4 pathogens are unlikely to trigger illness in wholesome workers or animals. The fourth risk group includes microorganisms corresponding to Bacillus subtilis, Naegleria gruberi, and infectious canine hepatitis virus. Among different actions, the 2004 State Council regulation on the management of laboratory biosafety resulted within the formulation, publication, and implementation of lists of pathogenic microorganisms capable of spreading to humans and to animals. These lists are used to guide choices related to biosafety risk assessments nicely as|in addition to} choices - 36 - Li Jinsong, M. Biosafety Containment Levels Another major part of biosafety is the containment level established to point out the grade of containment required for dealing with the microorganism safely in a laboratory setting. The biosafety containment level includes the engineering, operational, technical, and bodily necessities for manipulating a particular pathogen. Each pathogen has totally different inherent traits, however, as described above, a risk assessment the biohazard level of microorganisms determines the biosafety containment level to be employed. Based largely on the standards of the World Health Organization and the guidelines used within the United States and Canada, the Chinese authorities has established 4 grades of containment for work involving pathogenic microorganisms. As a basic rule, laboratories within the Biosafety Level 1 and a couple of|and a pair of} shall not carry out experimental activities with highly pathogenic microorganisms. Ministry of Agriculture, "List of Animal Pathogenic Microorganisms," Regulation 53-2005 (Beijing: thirteen May 2005); Ministry of Health, "Directory of Pathogenic Microorganisms Transmissible Between Humans," (Beijing: eleven January 2006). Centers for Disease Control and Prevention and National Institutes of Health, Biosafety Microbiological and Biomedical Laboratories, 4th ed. Government Printing Office, May 1999); Biosafety Microbiological and Biomedical Laboratories, 3rd ed. First, sort of|this kind of|this sort of} laboratory requires no special design options past those appropriate for a well-designed and functional laboratory. To begin with, access to the laboratory is limited or restricted on the discretion of the laboratory director when experiments are in progress. A biohazard sign must be posted on the entrance to the laboratory when etiologic agents are in use. Biosafety Containment Level 3 the practices, security tools, and facility design and development are relevant to scientific, diagnostic, instructing, analysis, or production services conducting work with massive volumes and high concentrations of Risk Group 3 microorganisms and/or with Risk Group 2 microorganisms, where the chance of aerosolization is high and the results of subsequent infection are life-threatening. The clean area and the possibly contaminated area are linked by an air lock, and the possibly contaminated area and the contaminated area are linked by a second air lock. Biological security cupboards must be situated away from areas of high foot site visitors and out of cross-currents from doors and ventilation techniques. The ventilation system should establish a directional air move from the clean area into the contaminated area. At all times, workers should certain that|be sure that} correct directional air move into the contaminated area is maintained. Exhaust air outtakes are separate from air intake vents and from occupied buildings. Autoclaves are to be installed within the wall between the clean area and the possibly contaminated area so that each one|that each one} autoclaved supplies can be removed within the clean zone. Also, careful consideration must be taken deciding on the appropriate biosafety measures for procedures. Following the chance assessment, a biosafety plan particular to every proposed experiment can be created. First, the laboratory must have have} attained the appropriate corresponding level of biosafety to ready to|be succesful of|have the power to} apply for acquisition of a highly pathogenic If these preconditions are met, the appropriate nationwide health or veterinary authorities will review suitability of the - 41 - Laboratory Biosafety of Pathogenic Microorganisms in China microorganism. Second, the laboratory should state a scientific analysis requirement for the proposed work with highly pathogenic microorganisms. Under this managerial system a National Accreditation Service for Conformity committee, consisting of biosafety specialists, was established. The objective of the surveillance is to monitor for occupationally acquired illnesses. During the initial examination, a baseline serum pattern must be obtained and saved for future reference. All laboratory personnel are to be evaluated on their data of these matters before starting work within the laboratory, and solely those assessed as having the requisite data might be permitted to resume their duties. Depending on the seriousness of the accident or noncompliance, an investigation could be performed. If the state of affairs entails laboratory-acquired infection, the laboratory could be closed through the investigation of the incident. Once the problem is understood, model new} normal working procedure or guideline could be established to tackle the problem, or maybe the governing regulation could be revised. The laboratory where the incident occurred must be recertified to work on the applicable biosafety level prior to resuming operations. Concluding Observations In current years, the Chinese authorities has made appreciable revisions to its rules and standards for laboratory biosafety. For the time being, the difficulty of concern for laboratory biosafety in China pertains to a scarcity of officials, specialists, and scientists who specialize in laboratory biosafety. This dearth of pros has made it a problem to implement the new new} regulatory system in a well timed and full method. To proceed building on the current improvements which were made, people involved in laboratory biosafety in China welcome cooperation with specialists in different nations and from the World Health Organization on matters of laboratory biosafety. Areas of potential collaboration embody - 45 - Laboratory Biosafety of Pathogenic Microorganisms in China biosafety coaching in universities, analysis laboratories, and different services; institutional management of biosafety; novel laboratory biosafety applied sciences; new laboratory biosafety ideas; and biosecurity. The relevant departments of the Chinese authorities have since been paying shut consideration to biosafety matters, learning the issues of biosafety and the developments which were happening to improve biosafety all over the world.
Proven 2.5 mg prazosin
It was agreed that epidemiological surveillance ought to be carried out at 4 levels: nationwide, departmental, municipal or district, and native. This ought to lead to the identification of the foci of infection in people, households, communities and/or regions and to the definition of the accountable threat components facilitating transmission. The major aims of any long-term control program are a substantial discount of the mortality, morbidity and incapacity attributable to neurocysticercosis, and the discount of financial losses due to of} pig cysticercosis. The control strategies to be adopted ought to be decided by the native epidemiological scenario. There ought to be specific strategies similar to defining endemic areas and foci of infection, therapy of human carriers in the foci, both identified and suspected, as well as|in addition to} the identification and therapy of human cases of neurocysticercosis. The complementary strategies would be: enchancment of water provide and sanitation, elimination of mechanical vectors, better meat inspection, and promotion of group participation as well as|in addition to} intersectorial cooperation. The following steps in implementation were defined: x promotion of a political will, x selection of endemic areas, x assortment of fundamental data on the native scenario, x identification of the foci, x planning of feasible actions and methods of analysis, x identification of assets, x group of social support (school lecturers, pig breeders and handlers, religious groups), x reorganization of the accountable central businesses (parasitological, diagnostic and serological laboratories, veterinary inspection, health inspection), x defining the duties of medical services, veterinary services, health services and services responsible for training. The mannequin developed seems sound and ought to be reviewed by any group planning a control program. The parts of the control and surveillance project are: x doc the burden and impact of T. Organization: A nationwide task drive consisting of ministries of health, agriculture, environment and training plus related personnel from analysis and educational establishments, nongovernmental improvement organizations and other partners ought to be established in every nation. A small multidisciplinary, intersectorial Technical Advisory Group of specialists with experience in cysticercosis science and program management ought to be shaped. The Technical Advisory Group at the side of} the Regional Working Group will have accountability for: a) figuring out priority analysis needs b) reviewing country/regional plans c) monitoring progress of control programs and d) offering technical oversight of support actions. Surveillance: Survellance ought to be achieved by way of regional centres using both passive and active surveillance methods, a easy reporting system, and rapid epidemiological assessment aiming at analysis of the burden of cysticercosis in humans and animals. Prevention and control is based primarily on identification and implementation of cost-effective, sustainable, integrated methods. Regional reference laboratories ought to be established using out there diagnostic expertise. A program for enhancing smallholder pig production and health ought to be developed. Research: Existing info ought to be reviewed and gaps in existing data recognized. Training: A regional centre for training and constructing capability to control cysticercosis/taeniosis ought to be established. An emphasis ought to be given to incorporation of cysticercosis/taeniosis control measures into nationwide major health care package deal. Networking: Internet websites, meetings, availability of paperwork, and worldwide consultation ought to all be encouraged and supported. This is a long-term plan, placing most of the consideration on prevention and control of cysticercosis, both in humans and in animals, and little emphasis on control of taeniosis though some parts of a short-term or medium-term program similar to motion by way of major health care workers is included. The following phases of implementation were advised: x selection of an space, x identification of the T. Several analysis projects in Latin America have adoped this protocol, however only some followed it exactly. Diverse control strategies shall be applied, monitored, and their efficacy measured. Data obtained will serve to plan a technique to be applied in the last 4 years of the project in shut collaboration with the Ministry of Health in the space. Concomitant efforts shall be made to optimize a vaccine for pigs, and to develop straightforward and economical diagnostic tests that can be utilized in the villages to detect contaminated humans and pigs. The possibility of eradicating human cysticercosis worldwide now exists due to in depth data of the disease, the event of correct diagnostic methods, and the availability of efficient remedies. Pawowski Treatment of human tapeworm carriers is the most important taeniosis/cysticercosis control activity to be applied in addition to the veterinary and health preventive measures and educational efforts. The commonplace management of human taeniosis is predicted to facilitate instructing and training actions in the control of taeniosis/cysticercosis. These actions ought to be ready in the simplest potential means so as to to} serve the needs of anybody concerned in control measures i. Probable case of taeniosis: x Self-diagnosis by finding tapeworm proglottids or x Positive questioning about proglottids being expelled four. Standard prognosis of taeniosis (see definitions above) by: x Questioning for expulsion of tapeworm proglottids (positive in about 50% cases of the T solium taeniosis and above 90% in T. Attempting to find Taenia scolices in feces after therapy also carries some threat. Tablets, given on an empty abdomen, ought to be chewed thoroughly before swallowing and washed down with some water. Implementation of efficient control measures relies upon due to this fact on taking some initiatives and choices as well as|in addition to} a close cooperation amongst numerous medical and non-medical services as listed below: 1. Health coverage makers: x Collect all potential info of medical and financial significance on taeniosis/cysticercosis in a country and think about the need, priority and feasibility of undertaking control measures. Public health officers: x Collect exhausting data on taeniosis/cysticercosis from medical, veterinary and analysis establishments and create or strengthen existing steady info system. Medical personnel: x Include training in prognosis, therapy, prevention and control of T. Veterinary services: x Promote meat inspection and analyze the infection rate in pigs and the origin of cysticercotic pigs identified locally. Educational personnel: x Collect instructional supplies (basic info on taeniosis/cysticercosis and epilepsy) as well as|in addition to} data on the incidence of T. Primary health workers: x Collect info on cysticercosis in humans and pigs, and cases of epilepsy in the native space and cross the data to appropriate health authorities x Identify, in cooperation with veterinary services, the native foci of T. Field trial of prognosis of Taenia solium taeniasis by Coproantigen enzyme linked immunosorbent assay. Field trial of the coproantigen-based prognosis of Taenia solium taeniasis by enzymelinked immunosorbent assay. Inflammatory response in the intestinal mucosa of gerbils and hamsters experimentally contaminated with the grownup stage of Taenia solium Intl. Extraparenchymal neurocysticercosis: report of 5 cases and evaluate of management. In Proceedings of 1st International Symposium on Human Taeniasis and Cattle Cysticercosis. Epidemiological survey of swine cysticercosis in 4 districts of Southern Highlands of Tanzania. Clinical presentations, pathophysiology, immunologic prognosis, economics, and therapy. Neurological signs in occult neurocysticercosis after a single taeniacidal dose of praziquantel. Experimental infection of pigs with a Taenia species from Korea: parasitological and serological aspects. Proceedings of the 9th Annual Meeting of the New Zealand Society for Parasitology, New Zealand J. Proceedings of the 2nd National Conference on Basic Research in Biology, Agriculture and Health (Hue, 25-26. Science and Technology Publishing House, Hanoi, Vietnam (in Vietnamese with English Abstract). Distribution of Taenia saginata cysts by muscle group in naturally contaminated cattle in Tanzania. Taenia saginata: polymerase chain reaction for taeniasis prognosis in human fecal samples. Diagnosis of Taenia saginata cysticercosis by immunohistochemical test on formalin fixed and paraffinembedded bovine lesions. Phylogenetic relationships inside Taenia taeniaeformis variants and other taeniid cestodes inferred from the nucleotide sequence of the cytochrome c oxidase subunit I gene. Epidemiological survey of swine cysticercosis in two rural communities of West-Cameroon. Evagination of Taenia solium cysticerci: a histologic and electron microscopy study.
References:
- https://www.nationalmssociety.org/NationalMSSociety/media/MSNationalFiles/Brochures/Brochure-The-MS-Disease-Modifying-Medications.pdf
- https://www.castlewood.k12.sd.us/cms/lib/SD02206129/Centricity/Domain/69/Puberty%20GirlsTalk%20Booklet.pdf
- https://www.choc.org/wp/wp-content/uploads/2020/11/spontaneous-pneumothorax-ph-with-references.pdf
- https://www.childrens.health.qld.gov.au/wp-content/uploads/PDF/factsheets/chifs-asthma.pdf
- https://www.accessdata.fda.gov/drugsatfda_docs/label/2005/021187s012lbl.pdf