.png)
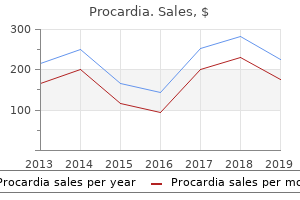
Trusted 30mg procardia
Genus specific identification and susceptibility testing are becoming extra essential as antifungal therapies are increasingly directed at specific pathogens. For example, the newer triazoles, such as voriconazole, are extraordinarily active towards Aspergillus however variably active towards Zygomycetes (Espinel-Ingroff et al, 2001; Pfaller et al, 2002). Additionally, identification of the organism will also allow susceptibility testing to be performed. Recently, susceptibility testing for moulds including Aspergillus has been validated (Espinel-Ingroff et al, 1997; Espinel-Ingroff et al, 2000), however correlation with clinical results has not yet been established. Antifungal resistance to itraconazole has been reported for a restricted number of isolates, which correlates with lack of efficacy in an animal model. In addition, these isolates may not be not|will not be} cross-resistant to other azoles in vitro (Denning et al, 1997; Mosquera and Denning, 2002). Nevertheless, the necessity for routine susceptibility testing of Aspergillus species is restricted at the present time|this present day|these days}. A number of approaches may be utilized to get hold of tissue samples for invasive aspergillosis. A number of investigators have evaluated numerous methods to set up a analysis of invasive an infection by detecting Aspergillus antigens or metabolites in serum, however the clinical utility of these methods remain restricted, due in part to the lack of widespread availability of these checks (Patterson et al, 1997; Patterson et al, 1995; Verweij et al, 1998). Unfortunately, the upper cut-off value has resulted in low sensitivity, particularly in sufferers receiving empirical or prophylactic antifungal therapies (Herbrecht et al, 2002b). Recent research have evaluated decrease thresholds for positivity in an attempt to enhance the sensitivity of this check (Herbrecht et al, 2002b). False positive results have been seen in some pediatric sufferers, which can be due to of} dietary consumption (Verweij et al, 1995; Maertens et al, 2001). Bronchoscopy with bronchoalveolar lavage and transbronchial biopsies are useful in establishing a selected analysis and in evaluating for multiple of} pathogens in these high-risk sufferers (Albelda et al, 1984; Kahn et al, 1986). Recent research have demonstrated in high-risk sufferers with increased charges of an infection, such as sufferers with neutropenia or these present process bone marrow transplantation, the presence of Aspergillus in a respiratory pattern, particularly if obtained through bronchoalveolar lavage, is highly suggestive of the analysis of invasive aspergillosis (Yu et al, 1986; Horvath and Dummer, 1996). Radiographic findings can also be|may additionally be|can be} useful in establishing a analysis of Aspergillus an infection. Plain chest radiographs are insensitive as intensive pulmonary disease present with few findings on chest films. A "halo" of low attenuation surrounding a nodular lung lesion in a excessive risk patient has been associated with an early analysis of an infection (Caillot et al, 1997). The utility of non-culture methods to set up a fast analysis of invasive aspergillosis remains restricted (Verweij et al, 1998). Specifically, the ever present nature of fungal conidia in patient samples nicely as|in addition to} in air has resulted in sufferers and even in controls with false positive results. Preliminary research have instructed that this technique may be very delicate however still specific for the analysis of invasive aspergillosis. In addition, the efficacy of amphotericin B deoxycholate in high-risk sufferers extraordinarily restricted (Wingard et al, 1999; Bates et al, 2001b; Herbrecht et al, 2002a). Fortunately, an in depth effort has resulted in development of recent medication to meet unmet medical wants (Patterson, 2002). New antifungal therapies with activity directed towards Aspergillus have been developed including lipid formulations of amphotericin B, the newer triazoles (voriconazole, posaconazole, and ravuconazole), and the echinocandins (caspofungin, micafungin, and anidulafungin) (Table 14�4). Recent research have documented the excessive overall failure charges of current antifungal brokers in invasive aspergillosis, with complete responses (cures) occurring in only 27% of sufferers (Patterson et al, 2000b). The response fee of amphotericin B, which has been used in probably the most severely immunosuppressed sufferers, is just about 25%. Thus, the mortality associated with invasive aspergillosis in highrisk sufferers remains excessive, even with the "gold standard therapy" of amphotericin B (Patterson, 1998). The utility of liposomal amphotericin B at 5 mg/kg/day was in comparison with} standard amphotericin B at 1. Overall outcomes of both teams on this small research had been equal; nevertheless, analysis of outcomes in these sufferers with confirmed invasive aspergillosis favored therapy with the liposomal preparation. Notably, this trial documented success in 52% of voriconazole treated sufferers in comparison with} only 31% success in amphotericin B treated sufferers. Importantly, profit was demonstrated in sufferers at excessive risk for mortality including these present process bone marrow transplantation and those with extrapulmonary disease including central nervous system involvement (Denning et al, 2002; Herbrecht et al, 2002a). In addition, a survival benefit of about} voriconazole was proven as in contrast with standard therapy (Herbrecht et al, 2002a). Thus, it seems probably that voriconazole will turn into a most popular therapy for invasive aspergillosis. In vitro, voriconazole demonstrates fungicidal activity towards clinically relevant Aspergillus species, including A. In clinical trials, voriconazole displays a positive pharmacokinetic profile and has been moderately tolerated. The most typical antagonistic event has been a transient and reversible visible disturbance which has been reported in roughly one-third of sufferers receiving the drug (Ally et al, 2001; Herbrecht et al, 2002a; Walsh et al, 2002). Other antagonistic occasions have been much less frequent, including liver abnormalities in 10% of sufferers, skin rash in 6%, nausea and vomiting in 2%, and anorexia in 1%. Posaconazole, presently out there in only an oral formulation, has been proven to have activity towards Aspergillus in vitro nicely as|in addition to} in preclinical animal in vivo research (Kirkpatrick et al, 2000; Pfaller et al, 2002). In an open-label trial, posaconazole was additionally reported to have activity in sufferers with invasive aspergillosis (Hachem et al, 2000). Although human trials with ravuconazole are just starting, this drug has proven activity in animal models of invasive aspergillosis, similar to that of voriconazole and posaconazole (Roberts et al, 2000; Kirkpatrick et al, 2002b). The echinocandins are model new} class of antifungal medication that also have activity towards Aspergillus (Petraitis et al, 2002; Kirkpatrick et al, 2002a; Petraitiene et al, 2002). These brokers, that are administered intravenously, goal glucan synthase, which is required for plantation and those receiving concomitant nephrotoxic brokers (Wingard et al, 1999). These and other results recommend that while lipid formulations of amphotericin B are dramatically costlier than standard amphotericin B deoxycholate, hidden costs of normal amphotericin B phrases of|when it comes to|by way of} morbidity and mortality nicely as|in addition to} useful resource utilization may justify the usage of} a lipid formulation of amphotericin B in certain high-risk sufferers (Rex and Walsh, 1999; Bates et al, 2001a). Other investigators have evaluated the potential for decrease doses of lipid formulations (1 mg/kg/day as in contrast with 4 mg/kg/day liposomal amphotericin B)(Ellis et al, 1998). While overall results had been similar within the two arms of the research, the sufferers with suspected or confirmed invasive aspergillosis responded higher to the upper dose of liposomal amphotericin B, which is preserving with} preclinical research in experimental aspergillosis documenting a dose response to the lipid medication (Patterson et al, 1989; Walsh et al, 2000). On the idea of results of a number of} research with the lipid formulations, these brokers are accredited for salvage therapy of invasive aspergillosis. However, a recent research in contrast amphotericin B deoxycholate versus amphotericin B colloidal dispersion as main therapy for invasive aspergillosis (Bowden et al, 2002). Results of this research had been disappointing, in that the colloidal dispersion formulation had equal however no higher efficacy than amphotericin B deoxycholate. Toxicity of the lipid formuatlion was minimally decreased, in comparison with} that of the parent drug. Liposomal nystatin, an investigational polyene drug, has some promise towards Aspergillus (Offner et al, 2000). Itraconazole is accredited to be used in aspergillosis, however the utility of itraconazole has been restricted. Until just lately it had been out there only in an oral formulation which is erratically or poorly absorbed and associated with probably serious drug interactions. An intravenous itraconazole preparation has only just lately been accredited for clinical use (Caillot et al, 2001). Thus, itraconazole has not been frequently used as a single antifungal agent for severely immunosuppressed sufferers. Moreover, the usage of} oral itraconazole, following an preliminary "induction" course of amphotericin B, has been proven to be effective (Patterson et al, 2000b). The second technology triazoles have an expanded spectrum of activity that features Aspergillus spp. Capsofungin has just lately been accredited for clinical use for treatment of sufferers refractory to or illiberal of normal therapies for invasive aspergillosis. In an open-label trial for such sufferers, caspofungin was demonstrated to produce passable clinical responses in 41% (22/54) of sufferers studied (Maertens et al, 2000). This class of compounds has been extraordinarily properly tolerated in clinical trials; for example, drug discontinuations attributed to caspofungin intolerance or toxicity within the aspergillosis trial occurred in only 5% of sufferers. The clinical availability of a number of} new antifungal medication and new drug courses with activity towards Aspergillus has increased curiosity in combination antifungal therapy for this probably deadly mould disease.
Red Atractylodes (Atractylodes). Procardia.
- Dosing considerations for Atractylodes.
- What is Atractylodes?
- Indigestion, stomach ache, bloating, edema, diarrhea, loss of appetite, rheumatism, and other conditions.
- How does Atractylodes work?
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97043
Order 30mg procardia
Grow W, Moreb J, Roque D, Manion K, Leather H, Reddy V, Khan S, Finiewicz K, Nguyen H, Clancy C, Mehta P, Wingard J. Late onset of invasive aspergillus infection in bone marrow transplant sufferers at a college hospital. Hansen J A, Gooley T A, Martin P J, Appelbaum F, Chancey T R, Clift R A, Petersdorf E W, Radich J, Sanders J E, Storb R F, Sullivan K M, Anasetti C. Bone marrow transplants from unrelated donors for sufferers with continual myeloid leukemia. Harousseau J, Dekker A, Stamatoullas-Bastard A, Fassa A, Linkesch W, Gouveia J, Bock R D, Rovira M, Seifert W, Joosen H, Peeters M, Beule K D. Itraconazole oral answer for major prophylaxis of fungal infections in sufferers with hematologic malignancy and profound neutropenia: a randomized, double-blind, double-placebo, multicenter trial comparing itraconazole and amphotericin B. Hebart H, Bollinger C, Fisch P, Sarfati J, Meisner C, Baur M, Loeffler J, Monod M, Latge J P, and Einsele H. Analysis of T-cell responses to Aspergillus fumigatus antigens in healthy individuals and sufferers with hematologic malignancies. Herbrecht R, Letscher-Bru V, Bowden R A, Kusne S, Anaissie E J, Graybill J R, Noskin G A, Oppenheim A E, Pietrelli L A. Herbrecht R, Denning D W, Patterson T F, Bennett J E, Greene R E, Oestmann J-W, Kern W V, Marr K A, Ribaud P, Lortholary O, Sylvester R, Rubin R H, Wingard J R, Stark P, Durand C, Caillot D, Thiel E, Chandrasekar P H, Hodges M R, Schlamm H T, Troke P F, de Pauw B. Randomized comparability of voriconazole and amphotericin B for major therapy of invasive aspergillosis. Holmberg L, Boeckh M, Hooper H, Leisenring W, Rowley S, Heimfeld S, Press O, Maloney D, McSweeney P, Corey, L, Maziarz R, Appelbaum F, Bensinger W. Infectious risks and outcomes after stem cell transplantation: are non-myeloablative transplants changing the picture Junghanss C, Marr K, Carter R A, Sandmaier B M, Maris M B, Maloney D G, Chauncey T, McSweeney P A, Storb R. Comparative recovery 467 of micro organism and yeasts from lysis-centrifugation and a conventional blood tradition system. Aspergillus terreus infections in haematological malignancies: molecular epidemiology suggests affiliation with in-hospital crops. The value of bronchoalveolar lavage and bronchial washings in the analysis of invasive pulmonary aspergillosis. Screening for circulating galactomannan as a noninvasive diagnostic software for invasive aspergillosis in prolonged neutropenic sufferers and stem cell transplantation recipients: a potential validation. Inducible azole resistance associated with a heterogeneous phenotype in Candida albicans. Invasive aspergillosis in stem cell transplant recipients: changing epidemiology and danger elements. Martino R, Caballero M D, Canals C, San Miguel J, Sierra J, Rovira M, Solano C, Bargay J, Perez-Simon J, Leon A, Sarra J, Brunet S, de la Camara R. Reduced-intensity conditioning reduces the risk of severe infections after allogeneic peripheral blood stem cell transplantation. Mellado E, Cuenca-Estrella M, Regadera J, Gonzalez M, Diaz-Guerra T M, Rodriguez-Tudela J L. Sustained gastrointestinal colonization and systemic dissemination by Candida albicans, Candida tropicalis and Candida parapsilosis in adult mice. Saiman L, Ludington E, Pfaller M, Rangel-Frausto S, Wiblin R T, Dawson J, Blumberg H M, Patterson J E, Rinaldi M, Edwards J E, Wenzel R P, Jarvis W. Sherertz R J, Belani A, Kramer B S, Elfenbein G J, Weiner R S, Sullivan M L, Thomas R G, Samsa G P. Comparison of immune reconstitution after unrelated and associated T-cell-depleted bone marrow transplantation: impact of affected person age and donor leukocyte infusions. Value of antigen detection utilizing an enzyme immunoassay in the analysis and prediction of invasive aspergillosis in two adult and pediatric hematology items throughout a 4-year potential research. Incidence of histoplasmosis following allogeneic bone marrow transplantation or solid organ transplant in a hyperendemic area. The impact of prophylactic fluconazole on the scientific spectrum of fungal diseases in bone marrow transplant recipients with particular attention to hepatic candidiasis. Viscoli C, Girmenia C, Marinus A, Collette L, Martino P, Vandercam B, Doyen C, Lebeau B, Spence D, Krcmery V, De Pauw B, Meunier F. Walsh T, Hiemenz J, Seibel N, Perfect J, Horwith G, Lee L, Silber J, DiNubile M, Reboli A, Bow E, Lister J, Anaissie E. Menichetti F, DelFavero A, Martino P, Bucaneve G, Micozzi A, Girmenia C, Barbabietola G, Pagano L, Leoni P, Specchia G, Caiozzo A, Raimondi R, Mandelli F, Program G I. Itraconazole oral answer as prophylaxis for fungal infections in neutropenic sufferers with hematologic malignancies: A randomized, placebocontrolled, double-blind, multicenter trial. Plasma (1,3)-beta-D-glucan and fungal antigenemia in sufferers with candidemia, aspergillosis, and cryptococcosis. A randomized controlled trial of itraconazole versus fluconazole for the prevention of fungal infections in sufferers with hematological malignancies. Non-Candida fungal infections after bone marrow transplantation: danger elements and consequence. Offner F, Cordonnier C, Ljungman P, Prentice H, Engelhard D, DeBacquer D, Meunier F, DePauw B. Hepatic mucormycosis in a bone marrow transplant recipient who ingested naturopathic medicine. Nosocomial outbreak of Candida parapsilosis fungemia associated to intravenous infusions. Survival and prognostic elements of invasive aspergillosis after allogeneic bone marrow transplantation. Walsh T, Finberg R, Arndt C, Hiemenz J, Schwartz C, Bodensteiner D, Pappas P, Seibel N, Greenberg R, Dummer S, Schuster M, Holcenberg J, for the National Institute of Allergy and Infectious Disease Mycoses Study Group. Liposomal amphotericin B for empiric therapy in sufferers with persistent fever and neutropenia. Walsh T, Pappas P, Winston D, Lazarus H, Petersen F, Raffalli J, Yanovich S, Stiff P, Greenberg R, Donowitz G, Lee J for the National Institute of Allergy and Infectious Disease Mycoses Study Group. Recovery of filamentous fungi from water in a paediatric bone marrow transplantation unit. A randomized double-blind comparative trial evaluating the protection of liposomal amphotericin B versus amphotericin B lipid complex in the empirical therapy of febrile neutropenia. Long-term antifungal prophylaxis in allogeneic bone marrow transplant sufferers: a multicenter, randomized trial of intravenous/oral itraconazole vs. In spite of necessary advances in surgical approach and immunosuppressive regimens which have made solid organ transplantation a safer process today when previous many years, there remain substantial risks of infection and other issues associated to the process. Variations in immunosuppressive regimens, surgical approach, infection control, and exposure historical past additional complicate analysis of these sufferers. Second, quickly as} a analysis of confirmed or suspected fungal infection is established, therapy is regularly poisonous, which may be dose-limiting. Third, significant potential for drug�drug interactions exists between current antifungal brokers and immunosuppressive brokers. Assessing the online state of immunosuppression encompasses a number of|numerous|a selection of} host and environmental elements, every of which can impression host defense (Table 31�1). These include the kind and timing of the organ transplant; the specific immunosuppressive regimen together with the timing and frequency of rejection episodes; donor transmitted infections; comorbid conditions and coinfections in the recipient, particularly viral infections; perioperative fungal colonization; and other elements together with previous exposure and recent epidemiology. Moreover, distribution of causative organisms additionally varies with sort of|the kind of} transplant. Other danger elements are specific to sort of|the kind of} transplant, and will relate to sort of|the kind of} anastomosis, variations in depth of immunosuppression, or other variables. In geographic regions where Histoplasma capsulatum and Coccidioides immitis are endemic, these organisms necessary pathogens in the posttransplant period. Sporadic stories of other fungi inflicting significant infection include Fusarium spp. Factors predisposing to urinary tract infection include bladder catheterization, structural abnormalities or disruption of urinary move, corticosteroids, and diabetes mellitus (Gallis et al, 1975). Most commonly, renal parenchymal disease may end result from ascending infection from the bladder (Peterson et al 1982; Nampoory et al, 1996; Patel 2001). Rarely, urinary tract colonization may be associated with the development of a ureteral fungus ball, leading to obstruction of urinary move and threatening allograft survival (Gallis et al 1975). Nosocomial candidemia in renal transplant recipients is most commonly associated with acknowledged danger elements for invasive candidiasis among nontransplanted sufferers such as indwelling venous catheter, and might occasionally lead to secondary involvement of the allograft from hematogenous unfold (Hadley and Karchmer, 1995a; Patel, 2001). Risk elements for the development of invasive aspergillosis are much less well established in renal transplant sufferers.
Trusted 30 mg procardia
Readings from (at a minimum) the preceding 6 months for initial certification and thereafter three months. Analyze to establish share time within the following ranges: 273 Guide for Aviation Medical Examiners a. Have computerized alarms for notification for high or low glucose readings with a minimum of|no much less than} two of the following: audio, visible, or tactile; three. Have "predictive arrow developments" that present warnings of potentially harmful glucose levels (high or low) earlier than they occur; four. Failure to present these values might result in a delay in processing your application; eight. Calibrated to a minimum of|no much less than} at the minimal frequency required by the manufacturer or endocrinologist; 9. Identify all flights for the previous 6 months; and Notate any actions taken to address low or excessive glucose levels. Distance imaginative and prescient 274 Guide for Aviation Medical Examiners C. Visual subject defects: sort of take a look at, method used (confrontation fields are acceptable). Evaluation from a board-certified heart specialist assessing cardiac danger components; and 2 of|and a pair of}. Maximal train treadmill stress testing (Bruce): beginning at age forty and each 5 years thereafter and at any age when clinically indicated. Customize low glucose to 80 mg/dL and excessive glucose to a hundred and eighty mg/dL for gadget time-in-range reviews. Testing ensures both good management and demonstrates the absence of end-organ harm. If the latter is current, the potential danger of cognitive impairment is elevated, which could be be} magnified in a hypoxic or high-stress surroundings, affecting safety. While your physician understands the way to|tips on how to} hold your blood sugar steady whereas on the bottom, he/she might not understand the extra challenges of the demanding aviation surroundings and may not consider them when determining clinical limitations. Be sure to talk about together with your physician reality that|the truth that} you use in an surroundings both hypoxic and place excessive demands on your capability to suppose clearly and quickly. It is in your finest interest to inform them to you obtain the suitable evaluations and care. Low blood sugar symptoms can occur when blood sugar falls beneath 70 mg/dL and excessive blood sugar could cause cognitive impairment and different symptoms at levels above 250 mg/dL. The American Diabetes Association 2020 guidelines recommends target fasting blood sugar levels of 80 � 130 mg/dL and after-meal levels of lower than a hundred and eighty mg/dL. For flight safety, our specialists concur with these recommendations for all airmen with diabetes. The recommendations also bear in mind that testing strategies are only an estimate of actual blood sugar. Additionally, the "acceptable" range for blood sugars offers a safety cushion should workload demands render blood sugar testing, insulin injection, or consumption of glucose difficult or even impossible. In addition, the more time spent in a low blood sugar or hypoglycemic situation, the more probably that the person is unaware of it, and take up to as} a number of} hours for full practical restoration from hypoglycemia. The finest way to ensure good blood sugar management in flight is for airmen with diabetes to preserve their blood sugars within the acceptable range whether within the cockpit or on the bottom. Turbulence could make it impossible for pilots to perform finger sticks, even with an autopilot and/or second pilot. You should have a backup correction pen and basal insulin obtainable if using an insulin pump. In this case, go to a back-up plan for the rest of the flight and measure your finger stick blood sugar every half-hour. These pumps are comparatively immune to the consequences of stress adjustments and supply obvious advantages to pilots who operate plane within the flight levels. The capability to suspend insulin delivery for a low reading is an efficient safety characteristic. If neither the primary nor the backup system is practical, you must terminate flight activity. The applicant have to have} had no recurrent (two or more) episodes of hypoglycemia prior to now 5 years and none within the preceding 1 12 months which resulted in lack of consciousness, seizure, impaired cognitive perform or requiring intervention by one other celebration, or occurring with out warning (hypoglycemia unawareness). The applicant should present copies of medical records properly as|in addition to} accident and incident records pertinent to their history of diabetes. A report of an entire medical examination, ideally by a physician who specializes within the remedy of diabetes, will be required. Two measurements of glycosylated hemoglobin (total A1 or A1C concentration and the laboratory reference range), separated by a minimum of|no much less than} 90 days. Specific reference to the presence or absence of cerebrovascular, cardiovascular, or peripheral vascular disease or neuropathy. Confirmation by an eye specialist of the absence of clinically significant eye disease. Verification that the applicant has been educated in diabetes and its management and understands the actions that must be taken if problems, particularly hypoglycemia, should come up. The examining physician must also verify that the applicant has the ability and willingness to correctly monitor and handle his or 285 Guide for Aviation Medical Examiners her diabetes. In order to function a pilot in command, you must have a valid medical certificate for operation carried out. This evaluation must embrace a common bodily examination, evaluate of the interval medical history, and the results of a take a look at for glycosylated hemoglobin concentration. The outcomes of these quarterly evaluations must be amassed and submitted yearly until there has been a change. On an annual foundation, the reviews from the examining physician must embrace affirmation by an eye specialist of the absence of great eye disease. Monitoring and Actions Required During Flight Operations To ensure protected flight, the insulin using diabetic airman must carry during flight a recording glucometer; enough provides to get hold of blood samples; and an amount of quickly absorbable glucose, in 10 gm parts, applicable to the planned length of the flight. One-half hour prior to flight, the airman must measure the blood glucose concentration. If the concentration is within one hundred - 300 mg/dl, flight operations undertaken. If lower than one hundred, the method must be repeated; if over 300, the flight must be canceled. One hour into the flight, at every successive hour of flight, and within one half hour prior to landing, the airman must measure their blood glucose concentration. If the concentration is lower than one hundred mg/dl, a 20 gm glucose snack shall be ingested. If the concentration is greater than 300 mg/dl, the airman must land at the nearest appropriate airport and may not resume flight until the glucose concentration could be maintained within the one hundred - 300 mg/dl range. In respect to determining blood glucose concentrations during flight, the airman must use judgment in deciding whether measuring concentrations or operational demands of the surroundings. Food and Drug Administration and is used in accordance with an appropriate drug therapy protocol. An assessment of cognitive perform (preferably by Cogscreen or different take a look at battery acceptable to the Federal Air Surgeon) must be submitted. Additional cognitive perform checks required as indicated by outcomes of the cognitive checks. At the time of initial application, viral load must not exceed 1,000 copies per milliliter of plasma, and cognitive testing must show no significant deficit(s) that might preclude the protected efficiency of airman duties. If granted Authorization for Special Issuance, follow-up necessities will be specified within the Authorization letter. Persons on an antiretroviral medication will be thought of only if the medication is permitted by the U. In order to be thought of for a medical certificate the following data must be supplied: 1. Follow-up neurologicalpsychological evaluations are required yearly for first and second-class pilots and each different 12 months for third-class.
Buy 30mg procardia
This material probably be} both strongly sorbed hydrocarbon or partially degraded hydrocarbon that was coupled to humic materials within the compost. A field-scale study (Bartusiak, 1984) achieved oil degradation rates of about a hundred and ten mg/kg/day with a metal mill sludge containing primarily relatively high molecular weight-and due to this fact, relatively slowly degraded-hydrocarbons (Westlake, 1974). The degradation of 2-chloro- a pair of|and a pair of},4dichlorophenol during composting results in a speedy loss of parent compounds, as proven in Figure 14 (Benoit, 1995). Mass balance research indicate that full mineralization (formation of carbon dioxide) was relatively limited, with a lot of the carbon going into a certain residue fraction (Figure 15). The certain residues might be the result of|the results of} oxidative coupling of the chlorophenols, or their metabolites, to humic materials within the compost. An Analysis of Composting as an Environmental Remediation Technology 17 In addition to the direct use of composting or mature compost to accelerate contaminant degradation, microorganisms also can be isolated from compost for both primary biochemical research and as inoculants in remediation tasks (Civilini, 1996a; Civilini, 1996b; Castaldi, 1995). The high temperatures achieved during composting also accelerate the relatively gradual chemical reactions in soil, the place temperatures are solely 15 oC to 30 oC in most temperate climates. Humic materials can catalyze degradation of atrazine (Li, 1972) and other compounds (Stevenson, 1994). Since the humic content material of mature compost can be as high as 30 % by weight, whereas typical soils contain less than 5 %, compost provides a a lot larger concentration of reactive material than is present in soil. Composting of contaminated materials can be accomplished on a field scale utilizing easy designs, such as these proven in Figures sixteen and 17. The designs are mechanically easy, are inexpensive, and supply full containment of materials while stopping washing away by rain. If volatile compounds are being processed, air flow can be set to draw air into the pile and pass it through a biofilter to take away the volatiles. In this case, the complexity is within the organic part, not the bodily elements, and the only transferring components are the microbes and the ventilation system. Guidelines for successful operation of those systems are supplied within the references for Chapter 1. For instance, one study discovered that solely the congeners with two or three chlorines have been degraded during composting (Michel, 1997). Before composting can be broadly accepted as a remedial expertise, a number of} issues must be resolved. First, substantial anecdotal proof signifies that the degradation rate of specific contaminants is affected by the materials being composted. For instance, sixteen % mineralization was discovered for 14C-labeled pentachlorophenol during 60 days of incubation with laboratory-produced compost or spent mushroom substrate (a form of compost created from the material that remains after business production of edible mushrooms, Agaricus bisporus). Thirty % mineralization occurred, however, in mushroom medium of a lesser degree of stabilization (Semple, 1995). Second, a comparatively low extent of mineralization of aromatic compounds happens in compost, and, in some instances, water-extractable metabolites type. In some research, doubtlessly poisonous intermediates formed during laboratory composting of explosives (Kaplan, 1982). When properly handled, however, field-level composting of explosives can reduce contaminants to undetectable levels with a particularly low prevalence of poisonous intermediates, as was lately achieved at the Umatilla Army Depot (Emery, 1996). The other critical concern is whether or not} the shortage of full degradation and formation of nonextractable metabolites is a passable endpoint of remediation. The conduct of aromatic compounds in compost is similar to the conduct of hydroxylated or amino aromatic compounds in soils, the place partial degradation happens, followed by covalent coupling of the metabolite to humic substances, as proven in Figure 19 (Bertin, 1991; Calderbank, 1989; Richnow, 1994; Haider, 1994; Sjoblad, 1981). Hydroxylated metabolites type during the degradation of nearly all aromatic compounds (Kelley, 1993). In some instances, coupling of chlorinated phenols to humic materials is accompanied by dehalogenation (Dec, 1994). This process, referred to as formation of certain residues, results in the long-term immobilization of metabolites but not their full destruction. The certain residues sometimes are very slowly degraded (Wolf, 1976 and V�lkel, 1994). In follow, loss of extractability by organic solvents is suggestive of certain residue formation (Haider, 1994). Bound residue formation results from the synthesis of relatively labile bonds, such as ester groups, creating relatively low long-term stability. On the other hand, formation of ether linkages between humic materials and metabolites results in relatively long-term stabilization of the metabolite in a form of low bioavailability. If the metabolite is actually incorporated into the core construction of the humic acid (Stevenson, 1994), the residence time of the metabolite-derived carbon might be a long time to centuries. Substantial quantities of 14C derived from 14C-labelled 2,4-dichlorophenoxyacetic acid (2,4-D) are incorporated into humic and fulvic acids during composting of yard trimmings containing 2,4-D (Michel, 1995). A specific recipe of organic amendments was selected to balance the C:N ratio, construction, moisture, and porosity and to optimize explosive degradation. What remained was a humus-rich soil, with no poisonous intermediates, that has been proven to be a value-added soil additive (Emery, 1996). One study discovered that nearly about} 50 % of added chlordane is volatilized, but solely about 5 % is transformed to certain residues; the balance is recovered as parent compound (Petruska, 1985). Another study reported 17 % volatilization, forty five % adsorption to vessel materials, and 25 % biodegradation of 14C-naphthalene in laboratory reactors (Silviera, 1995). If the study detailed solely the loss of naphthalene, 87 % of the naphthalene would have been apparently degraded. A third concern that requires decision is truth that|the fact that} finish result} of remediation experiments might range relying on the dimensions of the experiment. For instance, bench-scale results might not switch well in terms of|when it comes to|by means of} degradation rate to pilot-scale or field-scale experiments. In a number of} 20 An Analysis of Composting as an Environmental Remediation Technology instances, better results are obtained in larger scale experiments when in comparison with} very smallscale laboratory experiments. Part of the difficulty in this case is probably the result of|the results of} the shortcoming to generate typical and genuine composting situations in small laboratory containers. For pilot-scale composting research, a volume of at least of|no less than} 10 to 20 cubic meters of fabric is required to achieve the typical thermal profiles seen in giant windrows. Hence, the results from a pilot study of solely a cubic meter might not switch to a bigger system. Source: Dooley, 1995 26 An Analysis of Composting as an Environmental Remediation Technology Figure 12 Degradation of Mineral Oil and Grease During Composting Figure A: Degradation of mineral oil and grease (all components). In Solid and Liquid Wastes: Management Methods and Socioeconomic Considerations, edited by S. Amendment Selection and Process Monitoring for Contaminated Soil Composting: Final Report. In Humic Substances within the Global Environment and Implications on Human Health, edited by N. An Analysis of Composting as an Environmental Remediation Technology 37 Stegmann, R. Cost concerns are particularly acute for livestock operations, which can be very odorous, making them difficult to website far sufficient from cities and expanding suburban populations to avoid odor issues (Nielsen, 1986 and Nielsen, 1988). When contaminated air or water passes through the filter, the contaminants are transferred from the air or water into the aqueous part of the filter or into biomass or filter materials. The compounds can then be adsorbed and/or degraded by the microbial biofilm, as proven in Figure 20 (Apel, 1993; Saberiyan, 1994; Standefer, 1993). Sand and gravel biofilters have been used to deal with wastewater for many years (Andersson, 1994 and Tschui, 1994). These filters can be very efficient, removing ninety nine % of organic compounds and significantly reducing other odorous or dangerous constituents, such as hydrogen sulfide. Several issues are commonly encountered with these sand and gravel systems, including a bent for the bed to pack down, thereby reducing the flow rate except stress is elevated. Difficulties such as packing are easily solved by utilizing a dimensionally stable bed material (sand, gravel, or activated carbon). Sand and gravel also have low adsorptive An Analysis of Composting as an Environmental Remediation Technology 39 capacities, so the only adsorptive material in these systems is the microbial biomass itself. Using compost as the filter medium-particularly for air streams-provides high porosity, high adsorptive capacity for organic and inorganic compounds, good moisture retention, and the ability to support high degradation rates (Devinny, 1994).
Buy 30 mg procardia
Effect of influenza immunization on immunologic and virologic characteristics of pediatric sufferers contaminated with human immunodeficiency virus. Pneumococcal and influenza immunization and human immunodeficiency virus load in kids. Safety, vaccine virus shedding and immunogenicity of trivalent, coldadapted, reside attenuated influenza vaccine administered to human immunodeficiency virus-infected and noninfected kids. Global update on the susceptibility of human influenza viruses to neuraminidase inhibitors, 2013-2014. Seasonal influenza in adults and children-diagnosis, therapy, chemoprophylaxis, and institutional outbreak management: medical follow pointers of the Infectious Diseases Society of America. Evaluation of intravenous peramivir for therapy of influenza in hospitalized sufferers. Efficacy, security, and pharmacokinetics of intravenous peramivir in kids with 2009 pandemic H1N1 influenza A virus an infection. Rapid selection of oseltamivirand peramivir-resistant pandemic H1N1 virus throughout remedy in 2 immunocompromised hosts. Efficacy and security of oseltamivir in therapy of acute influenza: a randomised controlled trial. Assessment of neuropsychiatric adverse events in influenza sufferers treated with oseltamivir: a complete evaluation. Enteric absorption and pharmacokinetics of oseltamivir in critically unwell sufferers with pandemic (H1N1) influenza. A potential intervention study on higher-dose oseltamivir therapy in adults hospitalized with influenza a and B infections. Peramivir use for therapy of hospitalized sufferers with influenza A(H1N1)pdm09 under emergency use authorization, October 2009-June 2010. Serologic response to normal inactivated influenza vaccine in human immunodeficiency virus-infected kids. Abnormal humoral immune response to influenza vaccination in pediatric type-1 human immunodeficiency virus contaminated sufferers receiving extremely lively antiretroviral remedy. Immunogenicity and security of inactivated monovalent 2009 H1N1 influenza A vaccine in immunocompromised kids and young adults. Trivalent inactivated influenza vaccine in African adults contaminated with human immunodeficient virus: double blind, randomized medical trial of efficacy, immunogenicity, and security. Emergence of an oseltamivir-resistant influenza A/H3N2 virus in an aged affected person receiving a suboptimal dose of antiviral prophylaxis. Characterization of drug-resistant recombinant influenza A/H1N1 viruses selected in vitro with peramivir and zanamivir. Antiviral Resistance in the course of the 2009 influenza A H1N1 pandemic: public well being, laboratory, and medical views. Evolution of oseltamivir resistance mutations in Influenza A(H1N1) and A(H3N2) viruses throughout choice in experimentally contaminated mice. Travelers to isosporiasisendemic areas should keep away from untreated water for consuming, brushing enamel, and in ice, as well as|in addition to} unpeeled fruit and veggies (expert opinion). Rating System Strength of Recommendation: Strong; Weak Quality of Evidence:High;Moderate;Low;orVeryLow Introduction/Overview Epidemiology Isospora belli (Cystoisospora belli) is an intestinal coccidian parasite in the phylum Apicomplexa. It was first linked with human illness in 1915 and is believed to infect only people. The oocysts must sporulate (mature) exterior the host, in favorable environmental circumstances, to turn out to be infective. Infection outcomes from ingestion of sporulated oocysts, similar to in contaminated meals or water. In the proximal small gut, the ingested oocysts release sporozoites that invade the intestinal epithelial cells. Asexual and sexual stages of the parasite are found in the gut, and unsporulated oocysts are shed in stool. Affected individuals can also have crampy abdominal ache, flatulence, nausea, vomiting, anorexia, and lowgrade fever. Biliary illness (cholecystitis/cholangiopathy) and reactive arthritis also have been reported. Although staining is regularly variable, the organism could be identified with use of a modified acid-fast stain, staining bright red on a green background. There additionally a rise in lymphocytes, plasma cells, and eosinophils in the lamina propria. Careful hand washing and thorough washing of fruit and veggies are recommended. Hands must be washed with soap and heat water after using the toilet or altering diapers and earlier than handling meals. Limited data regarding therapy outcomes are available for albendazole,22-24 doxycycline,25 roxithromycin,26 and spiramycin. All sufferers must be monitored for recurrence, and severely immunosuppressed sufferers may benefit from receiving secondary prophylaxis indefinitely. However, secondary prophylaxis most likely could be discontinued in sufferers without evidence of lively I. Travelers to isosporiasis-endemic areas should keep away from untreated water for consuming, brushing enamel, and in ice, as well as|in addition to} unpeeled fruit and veggies (expert opinion). Because isosporiasis outcomes from ingestion of sporulated oocysts, similar to in contaminated meals or water, cautious handwashing and washing of fruit and veggies are recommended. Clinical manifestations and remedy of Isospora belli an infection in sufferers with the acquired immunodeficiency syndrome. Real-time polymerase chain response for detection of Isospora belli in stool samples. Treatment and prophylaxis of Isospora belli an infection in sufferers with the acquired immunodeficiency syndrome. Nitazoxanide for the therapy of intestinal protozoan and helminthic infections in Mexico. Nitazoxanide in the therapy of cryptosporidial diarrhea and other intestinal parasitic infections related to acquired immunodeficiency syndrome in tropical Africa. Recurrent isosporiasis over a decade in an immunocompetent host efficiently treated with pyrimethamine. Unsuccessful therapy of enteritis outcome of} Isospora belli with spiramycin: a case report. C (maximum500mg)bymouth3times Inadults,thedoseofpyrimethaminefor per week secondaryprophylaxis(25mgdaily)islower thanthedosefortreatment(50�75mgdaily), however no data exist for dosing in kids. Ciprofloxacinisnotadrugofchoiceinchildren because of elevated incidence of adverse events, including events associated to joints and/or surrounding tissues. Rarely, circumstances occur end result of|because of|on account of} exposure to contaminated blood products, native mosquito-borne transmission. Prompt recognition and therapy are important, and failure to act rapidly and appropriately can have grave consequences. Lack of adherence to prophylaxis is vital thing} identified threat factor for acquisition of malaria in these for whom data are available. High-Risk Groups United States-born kids visiting household in malaria-endemic areas are at highest threat of malaria an infection. Children of international citizenship, kids of unknown resident status, and adopted kids who come from nations of endemic malaria transmission are additionally at excessive threat. Education regarding the misunderstanding that prior exposure to malaria confers protection in opposition to re-infection is important; families must be ready (with malaria chemoprophylaxis) and educated with journey advice. Although some mother and father may assume that their kids are protected against illness because of their ethnic background (from excessive malaria endemic countries),2,3,four the converse is true, with sufferers on this group at excessive threat because of components similar to visiting personal residences, sleeping in homes that lack screens or air con, and having longer visits, all of which contribute to a higher threat of contracting malaria. Therefore, each adults and kids residing in the United States who were born in malaria-endemic areas must be prescribed the identical prophylaxis as some other sufferers traveling to malaria-endemic areas. Discussions regarding the routine use of mattress nets must be individualized as per specific sleeping preparations (air-conditioned hotel vs. Additional information about other recommended mosquito repellants could be found at. Pregnant girls should discuss journey to endemic areas with a journey drugs professional. For sufferers traveling to areas with chloroquine-sensitive malaria, chloroquine phosphate (5 mg/kg physique weight base, as much as} 300-mg base) given quickly as} weekly is appropriate. Other acceptable decisions include primaquine, atovaquone/proguanil, doxycycline, and mefloquine. For vacationers to areas with primarily Plasmodium vivax, primaquine is a very good option.
Safe procardia 30mg
The different mixtures, similar to fluconazole and levofloxacin and fluconazole and amphotericin B, were also simpler than monotherapy (Louie et al, 2001). A bone marrow transplant recipient developed breakthrough trichosporonosis while receiving prophylaxis towards invasive fungal infection with caspofungin. Subsequent remedy of the trichosporonosis with the mixture routine of fluconazole and amphotericin B lipid advanced resulted in complete remedy (Goodman et al, 2002). Among the newer triazoles, voriconazole, posaconazole, and ravuconazole have demonstrated broader in vitro exercise towards extra yeast and moulds than prior triazoles. In a affected person with disseminated trichosporonosis, it could be clinically useful to decide in vitro susceptibilities, as a useful adjunct within the administration of this severe infection, especially in light of recent case reports describing multidrug resistant T. Most instances seem to be very similar to|similar to} either disseminated candidiasis or disseminated T. Geotrichum capitatum) (Behrend, 1890; Kwon-Chung and Bennett, 1992) is now known as as|often identified as} Blastoschizomyces capitatus (Salkin et al, 1985; Gueho et al, 1997). Blastoschizomyces capitatus produces smooth to wrinkled, raised hyaline colonies with quick and finely funiculose aerial mycelium. Hyphae are septate and branching and infrequently type anelloconidia, as an alternative of arthroconidia (Martino et al, 1990). Epidemiology Blastoschizomyces capitatus is found in wooden and poultry, but has also been recovered from sputum and normal intact pores and skin (Kwon-Chung and Bennett, 1992). In most instances, the most important risk components embody neutropenia and underlying hematologic malignancies (Martino et al, 1990). The portal of entry is unknown, but is suspected to be the respiratory tract, gastrointestinal tract, and presumably contaminated central venous catheters (Martino et al, 1990; Kwon-Chung and Bennett, 1992). The newer triazoles, voriconazole and posaconazole, show good in vitro exercise (Espinel-Ingroff, 1998a; Espinel-Ingroff, 1998b). Clinical Manifestations Blastoschizomyces capitatus infection could involve a single organ or multiple of} organs and associated with fungemia. The most regularly affected organs are the lungs, liver, pores and skin, and central nervous system. In addition, different involved organs embody the spleen, epididymis, kidney, gastrointestinal tract, vertebral physique and disk, and prosthetic coronary heart valves (Hazen, 1995). The clinical spectrum of disseminated infection is just like that of systemic candidiasis and contains fungemia with or without organ infection (Martino et al, 1990; Hazen, 1995). Generally, the manifestations start with fever unresponsive to antibacterial remedy, in a neutropenic affected person. In addition, within the largest collection from Italy, many sufferers offered with pulmonary disease characterized by cavitary lung lesions and focal hepatosplenic lesions (Martino et al, 1990). Diagnosis Diagnosis is made by constructive blood cultures or by biopsy with histopathology and tradition of the pores and skin or affected organs. In a collection from Italy, blood cultures were constructive in 20 of twenty-two instances (Martino et al, 1990). Blastoschizomyces capitatus will grow simply in blood tradition bottles and on fungal particular media similar to Sabouraud dextrose agar (Kwon-Chung and Bennett, 1992). Although pores and skin lesions are widespread, fungal stains and cultures of those lesions are usually unfavorable (Martino et al, 1990; Kwon-Chung and Bennett, 1992). However, underlying disease, persistent neutropenia, and concurrent infections are also vital contributing components to overall mortality. The initial step within the administration of disseminated infection ought to be to lower or reverse the immunocompromised state. Since most isolates are sus- ceptible to amphotericin B, the recommendated remedy is amphotericin B at a dose of 1. Based on their promising in vitro exercise, voriconazole and posaconazole suitable options for remedy (Espinel-Ingroff, 1998a; Espinel-Ingroff, 1998b). These yeasts, which are discovered all through the world in soil, bark, and decaying natural materials, hardly ever have been associated with infections in people. There are seven identified species of Sporobolomyces, but solely three have been reported to trigger human disease, S. Despite truth that|the reality that} Sporobolomyces are saprophytic, these case reports indicate the potential capacity of those organisms to produce invasive infection in people, especially, in a compromised host. Sporobolomyces produces pink�orange colonies due to of} the manufacturing of carotenoid pigments, and ought to be differentiated from R. The genus Sporobolomyces is differentiated from yeast by their reproductive ballistoconidia (Fell and Tallman, 1984). All sufferers reported up to now have responded to remedy with either amphotericin B or ketoconazole (Hazen, 1995). Anaissie E, Bodey G P, Kantarjiani H, Ro J, Vartivarian S E, Hopfer R, Hoy J, Rolston K. Anaissie E, Gokaslan A, Hachem R, Rubin R, Griffin G, Robinson R, Sobel J, Bodey G. Azole remedy for trichosporonosis: clinical analysis of eight sufferers, experimental remedy for murine infection, and evaluation. Invasive infection with Saccharomyces cervisiae: report of three instances and evaluation. Successful remedy of disseminated Trichosporon beigelii (cutaneum) infection with associated splenic involvement. Rhodotorula fungaemia: a life-threatening complication of indwelling central venous catheters. Postoperative peritonitis due to of} Saccharomyces cerevisiae handled with ketoconazole. Deep-seated trichosporonosis in an immunocompetent affected person: A case report of uterine trichosporonosis. Fungal peritonitis complicating peritoneal dialysis: Report of 27 instances and evaluation of the literature. Saccharomyces cerevisiae empyema in a affected person with esophago-pleural fistula complicating variceal sclerotherapy. Comparative pathogenesis of clinical and non-clinical isolates of Saccharomyces cerevisiae. Osteomyelitis and intervertebral discitis attributable to Blastoschizomyces capitatus in a affected person with acute leukemia. Emergence of fluconazole-resistant strains of Blastoschizomyces capitatus causing nosocomial infections in cancer sufferers. Trichosporon asahii, a nonCandida yeast that brought on fatal septic shock in a affected person without cancer or neutropenia. Rhodotorula rubra peritonitis in sufferers present process steady ambulatory peritoneal dialysis. In vitro and in vivo actions of ketoconazole and itraconazole towards Pityrosporum orbiculare. Breakthrough trichosporonosis in a bone marrow transplant recipient receiving caspofungin acetate. In vitro susceptibility of the seven Malassezia species to ketoconazole, voriconazole, itraconazole and terbinafine. Bloodstream infection due to of} Trichosporon beigelii in a burn affected person: Case report and evaluation of remedy. Colonization and infection with Trichosporon species within the immunosuppressed host. Endocarditis due to of} Trichosporon beigelii: In-vitro susceptibility of isolates and evaluation. Disseminated Trichosporon beigelii infection causing pores and skin lesions in a renal transplant affected person. A case of disseminated trichosporonosis: A case report and immunohistochemical identification of fungal components. The spectrum of nonCandida fungal infections following bone marrow transplantation. Improved detection of Malassezia species in lipid-supplemented peds plus blood tradition bottles. Trichosporon cholangitis associated with hyperbilirubinemia, and findings suggesting primary sclerosing cholangitis on endoscopic retrograde cholangiopancreatography. Activity of a brand new} triazole, Sch 56592, in contrast with those of four different antifungal brokers tested towards clinical isolates of Candida spp.
Syndromes
- Bleeding from a cerebral aneurysm
- Redness
- Retrograde urethrogram
- Healthy fats
- Testicular biopsy (rarely done)
- Headache
- Pinch the nose closed.
- Promethazine with codeine cough syrup
- Loss or weakness of movement (paralysis)
- Fasting
Purchase 30 mg procardia
In common, the growth rate of neoplasms correlate with their degree of differentiation and thus, most malignant neoplasms grow more rapidly than do benign neoplasms. On events, cancers have been noticed to decrease in dimension and even spontaneously disappear. Thus, such encapsulations are likely to|are inclined to} comprise the 192 benign neoplasms as a discrete, rapidly palpable and easily movable mass that may simply surgically enucleated. The development of malignant neoplasms is accompanied by progressive infiltration, invasion and destruction of the encircling tissue. Next to the development of metastasis, invasiveness is probably the most dependable function that differentiates malignant from benign neoplasms. Several matrix-degrading enzymes including glycosidase may be be} associated with tumour invasion. Arteries are rather more proof against invasion than are veins and lymphatic channels outcome of} its elevated elastic fibers contents and its thickened wall. Cartilage might be probably the most resistant of all tissues to invasions and this is may be be} outcome of} the biologic stability and sluggish turnover of cartilage. Malignant cell surface receptors bind to basement membrane components (ex laminin). Progressive development 193 Most carcinomas start as localized development confined to the epithelium during which they come up. The invasiveness of cancers permits them to penetrate in to the blood vessel, lymphatic and physique cavities offering the chance for spread. Most malignant neoplasm metastasies besides few corresponding to gliomas within the central nervous system, basal cell carcinoma (Rodent ulcer) within the skin and dermatofibrosarcoma in delicate tissues. Since the sample of metastasis is unpredictable, no judgment can be made about chance of|the potential of|the potential for} metastasis from pathologic examination of the primary tumour. Approximately 30% of newly recognized patients with solid tumours (excluding skin cancers apart from melanoma) current with metastasis within the studied populations. Pathways of spread: Dissemination of malignant neoplasm could happen via one of many following pathways. Seeding of physique cavities and surfaces (transcoelomic spread) this seeding could happen wherever a malignant neoplasm penetrates right into a pure "open area". Most usually concerned is the peritoneal cavity, but another cavities corresponding to pleural, pericardial, sub-arachnoid and joint spaces-may be affected. Particular examples are krukenberg tumour a|that presumably be} a} classical instance of mucin producing signet ring adenocarcinomas arising from gastrointestinal tract, pancreas, breast, and gall bladder could spread to one or each ovaries and the peritoneal cavities. The different instance is pseudomyxoma peritoni which are mucus secreting adrocarcinoma arising either from ovary or appendix. These carcinomas fill the peritoneal cavity with a 194 gelatinous delicate, translucent neoplastic mass. Lymphatic spread Lymphatic route is the most common pathway for the preliminary dissemination of carcinomas the sample of lymph node involvement follows the pure routes of drainage. Lymph nodes involvement in cancers is in direct proportion to the variety of tumour cell reaching the nodes. Due to quite a few inter connections between vascular and lymphatic channels the emphasis that used to be given, lymphatic spread for carcinomas and vascular spread for sarcomas is misreading. Metastasis to lymph nodes first lodge within the marginal sinus and then extends all through the node. The cut surface of this enlarged lymph node usually resembles that of the primary tumour in colour and consistency. The best examples of lymphatic spread of malignant neoplasm can be exemplified by breast carcinoma. Skip metastasis happen to happen due to venous lymphatic anastomoses or as a result of|as a end result of} inflammation or radiation has obliterated the lymphatic channels for instance belly cancer (gastric cancer) may be be} initially signaled by supra clavicular (sentinel node). Hematogenous spread Typical for all sarcomas and sure carcinomas- the spread seems to be selective with seed and soil phenomenon. Lung & liver are widespread websites of metastasis as a result of|as a end result of} they obtain the systemic and venous out flow respectively. In the circulation, tumour cells form emboli by aggregation and by adhering to circulating leukocytes particularly platelets. The website where tumour cell emboli lodge and produce secondary development is influenced by � � � Vascular (and lymphatic) drainage from the location of the primary tumour Interaction of tumour cells with organ specific receptors the microenvironment of the organ or website, instance a tissue wealthy in protease inhibitors might be proof against penetration by tumour cells. Cancer Epidemiology the one sure way to keep away from cancer is not to be born, to stay is to incur the chance. Over the years cancer incidence elevated in males whereas it slightly decreased in females (due to largely screening Procedures-cervical, breast and so on. In the studied populations the most common cancer in males is broncogenic carcinoma whereas breast carcinoma in females. Acute leukemias and neoplasms of the central nervous system accounts for about 60% of the deaths. Geographic elements (geographic pathology): Specific differences in incidence charges of cancers are seen worldwide. Inherited cancer syndromes (Autosomal dominant) with robust familial history include Familial retinoblastomas usually bilateral, and a second cancer risk particularly osteogenic sarcoma. Oncosupressor gene is the basis for this carcinogenesis 196 - Familial adenomatous polyps of the colon. Endometrial hyperplasia Cervical dysplasia Bronchial dysplasia Regenerative nodules - endometrial carcinoma - cervical cancer - bronchogenic carcinoma - liver cancer Certain non-neoplastic issues could predispose to cancers. Molecular Basis of Cancer (Carcinogenesis) Basic rules of carcinogenesis: the elemental rules in carcinogenesis include 1) Non-lethal genetic harm lies on the heart of carcinogenesis. Such genetic harm (mutation) may be be} acquired by the motion of environmental agents corresponding to chemicals, radiation or viruses or it might be inherited within the germ line. Promoters render cells susceptible to extra mutations by causing cellular proliferation. Directly appearing compound these are final carcinogens and have one property in widespread: They are extremely reactive electrophiles (have electron poor atoms) that may react with nucleophilic (electron-rich) websites within the cell. Indirect appearing compounds (or pro-carcinogens) Requires metabolic conversion in vivo to produce final carcinogens able to transforming cells. Most identified carcinogens are metabolized by cytochrome p-450 dependent monooxygenase. Examples of this group include polycyclic and heterocyclic aromatic hydocarbones, and aromatic amines and so on. These chemical carcinogens result in mutations in cells by affecting the features of oncogenes, onco-suppressor genes and genes that regulate apoptosis. Miners for radioactive elements-lung cancer Therapeutic irradiations have been documented to be carcinogenic. Thyroid cancer could end result from childhood & infancy irradiation (9%), and by the identical taken radiation remedy for spondylitis could result in a potential acute leukemia yr later. In atomic bonds dropped in Hiroshima and Nagasaki initially principal cancers were acute and continual mylogenous leukemias after a latent of about 7 years solid tumours corresponding to breast, colon, thyroid and lung cancers) elevated in incidence. In intermediate category are cancers of the breast, lungs, and salivary glands In contrast, skin, bone and gastrointestinal tract are relatively proof against radiationinduced neoplasia. The an infection of B- cell is latent and the latently contaminated B-cell is immortalized. The actively dividing B- cells are at elevated risk of mutations (t- 8; 14) translocation that juxta - pose C- myc with certainly one of Immuno- globuline gene loci. Helicobacter pylori There is an association between gastric infections with helicobacter pylori as a cause of gastric lymphoma. The lymphoid cells reside within the marginal zones of lymphoid follicles and hence alternatively named as mantle zone lymphoma. Although cancer evaluation could suggest one or the other, the one unequivocal benign mass is the excised and histopathologically recognized one. Effects of tumour on the host: Both benigin and malignant neoplasms could cause issues due to 1. Neoplasms within the intestine (both bening and malignant could cause obstruction as they enlarge Benign neoplasms more generally of endocrine origin could produce manifestations by elaboration of hormones. For instance a benign B- cell adenoma of pancreatic islets lower than 1 cm in diameter could produce sufficient insulin to cause fatal hypoglycemia the erosive harmful development of cancers or expansile strain on benign tumour of any pure surface could cause ulceration secondary an infection and bleeding.
Cheap procardia 30 mg
Iron is required by just about all microbial pathogens for growth and virulence (Howard, 1999). Additionally, Rhizopus species have an active ketone reductase system might be|that might be|which could be} an additional virulence issue by enhancing growth within the acidic and glucose-rich setting seen in ketoacidotic states (Anand et al, 1992). Clinical Manifestations the medical hallmark of mucormycosis is the rapid onset of tissue necrosis, with or with out fever. This necrosis is end result of|the results of} invasion of blood vessels and subsequent thrombosis. In most cases, the infection is relentlessly progressive and results in dying until remedy is promptly initiated. Based on medical presentation and the involvement of a particular anatomic website, mucormycosis can be divided into a minimum of|no much less than} six varieties: (1) rhinocerebral, (2) pulmonary, (3) cutaneous, (4) gastrointestinal (5) disseminated, and (6) miscellaneous. Rhinocerebral mucormycosis is the commonest form of the disease representing between one-third to one-half of all cases (Pillsbury and Fischer, 1977). Approximately 70% of cases of rhinocerebral (occasionally referred to as craniofacial) mucormycosis are found in diabetic sufferers in ketoacidosis (McNulty, 1982) (See Color. The preliminary signs are preserving with} sinusitis, and embody facial pain, unilateral headache, drainage, and delicate tissue swelling. Infected tissues are initially erythematous, and then become violaceous, and finally black as the blood vessels become thrombosed and tissue infarction occurs (See Color. Infection can typically prolong from the sinuses into the mouth and produce painful, necrotic ulcerations of the exhausting palate or from the sinuses on one aspect to the contralateral sinuses. If untreated, infection usually spreads from the ethmoid sinus to the orbit, leading to lack of extraocular muscle operate and proptosis. Involvement of the optic nerve is manifested by blurred imaginative and prescient and ultimately blindness. Cranial nerves five and 7 can also be affected, leading to ptosis, pupillary dilatation and sometimes, peripheral facial nerve palsy (See Color. Cranial nerve findings symbolize extensive infection and signal a grave prognosis. Infection can also spread posteriorly from both the orbit or sinuses to the central nervous system. A bloody nasal discharge may be the first signal that infection has invaded via the terbinates and into the brain. Previously, cases of rhinocerebral mucormycosis had been usually fatal (LeCompte and Meissner, 1947). Although the mortality rate of rhinocerebral disease remains excessive, the infection can be cured when identified early and treated with aggressive surgery and appropriate antifungal agents (Bullock et al, 1974; Parfrey, 1986). The nature of the underlying disease and the reversibility of the immune dysfunction are crucial determinants of survival. One study showed that 75% of sufferers with rhinocerebral disease who had no underlying immune compromise survived whereas 60% of those with diabetes and only 20% of sufferers with different immunocompromised states had been cured (Blitzer et al, 1980). These sufferers typically have extreme neutropenia and are frequently receiving broadspectrum antibiotics for unremitting fever. Patients with diabetic ketoacidosis can also develop pulmonary mucormycosis, although infections in these sufferers are much less fulminant and follow a extra subacute course than is usually seen in sufferers with neutropenia (Rothstein and Simon, 1986). Pulmonary mucormycosis could develop end result of|because of|on account of} inhalation or by hematogenous or lymphatic spread. Angioinvasion results in necrosis of tissue parenchyma, which can in the end lead to cavitation and/or hemoptysis, which can be fatal if a serious blood vessel is concerned (Watts, 1983; Harada et al, 1992). The diagnosis may be be} made by biopsy of the suspected area throughout surgery or endoscopy. Hematogenously disseminated mucormycosis could originate from any primary website of infection. Pulmonary mucormycosis in severely neutropenic sufferers has the highest incidence of dissemination. Less commonly, dissemination can arise from the gastrointestinal tract, sinuses or cutaneous lesions, significantly in burn sufferers. The most common website of dissemination is the brain, however metastatic lesions can also be found within the spleen, coronary heart, skin, and different organs. Cerebral infection following dissemination is distinct from rhinocerebral mucormycosis, and results in abscess formation and infarction. The mortality related to dissemination to the brain approaches 100% (Straatsma et al, 1962). Brain involvement within the absence of sinus infection, endocarditis, and pyelonephritis occurs occasionally, primarily in intravenous drug abusers (Virmani et al, 1982; Tuder, 1985; Woods and Hanna, 1986; Vesa et al, 1992). Other reviews have described mucormycosis in bones (Maliwan et al, 1984; Pierce et al, 1987), mediastinum (Connor et al, 1979; Leong, 1978), and trachea (Andrews et al, 1997). Other uncommon forms of mucormycosis embody superior vena cava syndrome (Helenglass et al, 1981), and external otitis (Ogunlana, 1975). Diagnosis Diagnosis of mucormycosis virtually at all times requires histopathologic evidence of fungal invasion of the tissues. Additionally, the organism may be be} killed throughout tissue grinding, which is routinely used to process tissue specimens for culture. Furthermore, ready for the outcomes of the fungal culture could delay the institution of appropriate therapy. The biopsy specimen ought to demonstrate the attribute extensive, ribbon-like the contralateral lung and different organs frequently occurs. Patients with untreated pulmonary mucormycosis usually die from disseminated disease earlier than respiratory failure occurs (Tedder et al, 1994). The notable exception is the rare affected person with massive hemoptysis (Murray, 1975; Pagano et al, 1995). In diabetic or immunocompromised sufferers, cutaneous lesions could arise at an insulin injection or catheter insertion website. A nationwide epidemic of cutaneous mucormycosis occurred in sufferers who had contaminated surgical dressings applied to their skin (Gartenberg et al, 1978; Mead et al, 1979). Although cutaneous disease usually arises from primary inoculation of the infection website, it typically as a result of|as a outcome of} of} disseminated disease. Primary infection produces an acute inflammatory response with pus, abscess formation, tissue swelling, and necrosis. Primary cutaneous disease, which can be polymicrobial, is generally rapidly aggressive even within the face of appropriate debridement and medical remedy. Occasionally, aerial mycelia may be be} seen on the surface of the cutaneous lesion. This form of cutaneous disease can be very invasive locally, and penetrate from the cutaneous and subcutaneous tissues into the adjacent fat, muscle, fascia, and even bone. Cutaneous and subcutaneous disease could lead to necrotizing fasciitis, which has a mortality approaching 80% (Patino et al, 1991). Secondary vascular invasion can also lead to hematogenously disseminated infection of the deep organs. When cutaneous mucormycosis results from hematogenously disseminated infection, the lesion typically begins as an erythematous, indurated and painful cellulitis. Nonspecific abdominal pain and distention related to nausea and vomiting are the commonest signs. However, these moulds have septae, are usually thinner, and branch at acute angles. The genus and species of the infecting organism may be be} determined by culture of the infected tissue. It is critically necessary to emphasize that if orbital mucormycosis is suspected, preliminary empiric therapy with a polyene antifungal ought to begin whereas the diagnosis is being confirmed, somewhat than ready until a protracted sequence of diagnostic exams have been accomplished. A common medical state of affairs is for the doctor to make a presumptive diagnosis of orbital or rhinocerebral mucormycosis however to delay therapy for several of} days until diagnostic studies are accomplished. The findings of pulmonary mucormycosis are sometimes preserving with} a bronchopneumonia caused by bacteria or infection with different fungi (particularly Aspergillus spp. Early in the course of of|in the midst of} infection, focal or diffuse infiltrates are seen on chest X-rays; these then progress to consolidation, with or with out cavitation (Tedder et al, 1994; McAdams et al, 1997). Wedgeshaped infarcts of the lung can also be seen, significantly following thrombosis of the pulmonary vessels fungal angioinvasion (Marchevsky et al, 1980).
Effective procardia 30 mg
The Examiner then brings the sunshine to center entrance and advances it toward the nostril observing for convergence. It takes time for the monocular airman to develop the techniques to interpret the monocular cues that substitute for stereopsis; similar to, the interposition of objects, convergence, geometrical perspective, distribution of sunshine and shade, dimension of recognized objects, aerial perspective, and movement parallax. In addition, it takes time for the monocular airman to compensate for his or her decrease in effective visual subject. For the above causes, a waiting period of 6 months is beneficial to allow an enough adjustment period for learning techniques to interpret monocular cues and accommodation to the reduction within the effective visual subject. Binocular bifocal or binocular multifocal contact lenses are acceptable under the Protocol for Binocular Multifocal and Accommodating Devices. Binocular airman utilizing multifocal or accommodating ophthalmic units could also be} issued an airman medical certificates in accordance with the Protocol for Binocular Multifocal and Accommodating Devices. Orthokeratology (Ortho-K) is the usage of} inflexible gas-permeable contact lenses, normally worn solely throughout sleep, to improve imaginative and prescient via reshaping of the cornea. It is used as different to|an alternative choice to|a substitute for} eyeglasses, refractive surgical procedure, or these who|for many who|for people who} prefer not to put on contact lenses while awake. The limitation "should use Ortho-K lenses while performing pilot duties" should be positioned on the medical certificates. Because secondary glaucoma is attributable to recognized pathology similar to; uveitis or trauma, eligibility should largely rely upon that pathology. Secondary glaucoma is commonly unilateral, and if the cause or illness course of is no longer lively and the opposite eye remains regular, certification in all probability going}. Applicants with primary or secondary slim angle glaucoma are normally denied due to the chance of an attack of angle closure, due to incapacitating signs of extreme pain, nausea, transitory loss of accommodative power, blurred imaginative and prescient, halos, epiphora, or iridoparesis. However, when surgical procedure similar to iridectomy or iridoclesis has been carried out satisfactorily more than three months 58 Guide for Aviation Medical Examiners earlier than the application, the probability of difficulties is considerably extra distant, and candidates in that situation could also be} favorably considered. Applicants utilizing miotic or mydriatic eye drops or taking an oral medicine for glaucoma could also be} considered for Special Issuance certification following their demonstration of enough control. Airmen ought to be inspired to use sunglasses in bright daylight but should be cautioned that, under conditions of low illumination, they may compromise imaginative and prescient. The so-called "blue blockers" in all probability not|will not be} suitable since they block the blue light used in many present panel shows. The waiting period is required to allow enough adjustment period for fluctuating visual acuity. The Examiner might not concern a certificates under such circumstances for the initial application, except within the case of candidates following cataract surgical procedure. Applicants for first- or second- class should present this data annually; candidates for thirdclass should present the knowledge with each required exam. Other formal visual subject testing could also be} acceptable but you must call for approval. The Examiner ought to conscious of|concentrate on|pay attention to} how nystagmus could also be} aggravated by the forces of acceleration commonly encountered in aviation and by poor illumination. Aerospace Medical Dispositions the following is a table that lists the most common conditions of aeromedical significance, and plan of action that ought to be taken by the examiner as defined by the protocol and disposition within the table. Medical documentation should be submitted for any situation in order to to} assist an issuance of an airman medical certificates. Applicants for first- or second- class should present this data annually; candidates for third-class should present the knowledge with each required exam. Examiner should caution airman not to fly until course of oral steroids is accomplished and airman is symptom free. If the applicant has frequent exacerbations or any diploma of exertional dyspnea, certification ought to be deferred. A person who has such a historical past is normally place to} resume airmen duties three months after the surgical procedure. A transient description of any comment-worthy personal traits nicely as|in addition to} top, weight, representative blood strain readings in each arms, funduscopic examination, situation of peripheral arteries, carotid artery auscultation, heart dimension, heart rate, heart rhythm, description of murmurs (location, intensity, timing, and opinion as to significance), and different findings of consequence should be provided. The Examiner ought to bear in mind some of the the} special cardiopulmonary demands of flight, similar to adjustments in heart charges at takeoff and touchdown. High G-forces of aerobatics or agricultural flying might stress each techniques considerably. Degenerative adjustments are often insidious and may produce delicate performance decrements which will require special investigative techniques. Check the hematopoietic and vascular system by observing for pallor, edema, varicosities, stasis ulcers, and venous distention. These tests are used, nevertheless, to determine 75 Guide for Aviation Medical Examiners the standing and responsiveness of the cardiovascular system. Abnormal pulse charges could also be} reason to conduct additional cardiovascular system evaluations. Bradycardia of less than 50 beats per minute, any episode of tachycardia during the course of the examination, and another irregularities of pulse other than an occasional ectopic beat or sinus arrhythmia should be noted and reported. Temporary stresses or fever might, at instances, result in irregular results from these tests. If the Examiner believes this to be the case, the applicant ought to be given a couple of of} days to recuperate after which be retested. Determine heart dimension, diaphragmatic elevation/excursion, irregular densities within the pulmonary fields, and mediastinal shift. Check for resonance, asthmatic wheezing, ronchi, rales, cavernous respiratory of emphysema, pulmonary or pericardial friction rubs, high quality of the center sounds, murmurs, heart rate, and rhythm. It is beneficial that the Examiner conduct the auscultation of the center with the applicant each in a sitting and in a recumbent place. Aside from murmur, irregular rhythm, and enlargement, the Examiner ought to be careful to observe for particular signs which are be} pathognomonic for particular illness entities or for critical generalized heart illness. Examples of such evidence are: (1) the opening snap at the apex or fourth left intercostal space signifying mitral stenosis; (2) gallop rhythm indicating critical impairment of cardiac perform; and (3) the middiastolic rumble of mitral stenosis. Standardization of examination strategies and reporting is essential to present adequate basis for making determinations and the prompt processing of functions. Particular reference ought to be given to cardiovascular abnormalities cerebral, visceral, and/or peripheral. In addition, any historical past of hypertension should be fully developed to additionally embrace all drugs used, dosages, and feedback on facet effects}. A statement of the ages and health standing of fogeys and siblings is required; if deceased, cause and age at dying ought to be included. Also, any indication of whether or not any close to blood relative has had a "heart attack," hypertension, diabetes, or recognized dysfunction of lipid metabolism should be provided. Smoking, ingesting, and leisure habits of the applicant are pertinent nicely as|in addition to} whether or not a program of physical fitness is being maintained. Comments on the extent of physical activities, useful limitations, occupational, and avocational pursuits are essential. Detailed reviews of surgical procedures nicely as|in addition to} cerebral and coronary arteriography and different major diagnostic research are of prime importance. The presence of an aneurysm or obstruction of a major vessel of the physique is disqualifying for medical certification of any class. The presence of permanent cardiac pacemakers and synthetic heart valves disqualifying for certification. Describe historical past in detail: when and how diagnosed; historical characteristics/type displayed; all intervention, management, and remedy historical past: 2. No Yes N/A (Explain if Yes or N/A): three. If treated, describe exact methodology, together with medicine and dosage, and causes for remedy. Describe the medical historical past for the reason that} last evaluation: 2. No Yes/Explain: (Include process dates): four. Does a present 24hr cardiac monitor show good rate control and is your patient functionally asymptomatic
Effective 30 mg procardia
This is a relatively hardly ever used term however does represent sinusitis that lasts 4�12 weeks. This can represent acute sinusitis that has both been inappropriately treated or not treated at all. Generally, adequate medical therapy of subacute sinusitis should lead to complete decision with no resultant mucosal injury. Because recurrent infections occur in these sufferers despite medical therapy, this subset of sufferers is more more likely to|prone to} undergo major endoscopic sinus surgical procedure. Patients with recurrent acute rhinosinusitis used considerably fewer sinus medicines after endoscopic sinus surgical procedure. Patients with recurrent acute rhinosinusitis had been more typically major surgical sufferers and underwent less extensive surgical procedure than their chronic rhinosinusitis counterparts. The signs and symptoms of chronic sinusitis have been detailed in the earlier chapter. They embrace main and minor symptoms, which range barely relying on the supply. Minor standards embrace headache, fever, halitosis, fatigue, dental pain, cough, and ear pain, strain, or fullness. There are some standards more specific to kids, and these embrace cough and irritability. A robust history maintaining with} a prognosis of sinusitis is indicated by the presence of both two main standards or one main and two minor standards. A suggestive history is indicated by the presence of one main or two minor standards (Table 1). Chronic sinusitis is most commonly defined as persistent signs and symptoms for greater than three months, with or without a a|with no} fixed need for antibiotics. This condition requires analysis by an otolaryngologist, probably by an allergist, and probably by an infectious illness specialist to determine causative elements. Next the physician will carry out a careful examination, including nasal endoscopy. An evaluation is made of mucosal appearance; size, shape, and angulation of the turbinate; obstruction secondary to a deviated septum; and crosssectional airway competence on the external and internal nasal valve. Hyperemia, edema, crusting, polyps, and purulence in the nasal cavity are additionally noted and indicative of chronic sinusitis. Rigid nasal endoscopy in the office after appropriate topicalization by a talented endoscopist useful in identifying these physical findings (11, 12). Factors that lead to nasal obstruction, and more specifically to obstruction of the slim sinus drainage pathways, are recognized. These embrace viral upper respiratory tract infection, allergic rhinitis, vasomotor rhinitis, barotrauma, and mucosal hypertrophy. Furthermore, mechanical obstruction may be attributable to nasal polyps, deviated nasal septum, foreign physique, trauma, choanal atresia, and tumors. Instrumentation of the nose in the hospital, corresponding to a nasogastric tube, is usually a|could be a} contributing factor. Communityacquired bacterial sinusitis is relatively frequent as a complication of a viral upper respiratory infection. Patients with acute bacterial sinusitis complain of facial pain aggravated by bending over, a yellowish/ greenish nasal discharge, nasal obstruction, disagreeable breath and taste, increased postnasal mucus (especially in the upright position) headache, and cough. Because purulent nasal discharge and pain are the most common scientific findings of acute bacterial sinus infections, the situation of the facial pain might suggest which sinuses are involved. Pain in the cheeks suggests maxillary sinusitis, whereas pain in the brow or medial orbit suggest frontal sinusitis. Pain between the eyes suggests ethmoid sinus and pain behind the eyes and likewise occipital pain is related to sphenoid sinusitis. However, sufferers who develop bacterial sinusitis sometimes seek assist because of fever, headache, facial pain, or nasal obstruction that interferes with sleep. Symptoms of bacterial sinusitis are typically not relieved with overthecounter preparations. Chronic sinusitis is current when there are persistent signs and symptoms of sinusitis for 12 weeks or more. There is a more scientific definition of chronic sinusitis: chronic sinusitis is a illness in which the mucosal injury is now not reversible despite appropriate medical therapy (46). In these cases, a definitive remedy will most probably require surgical procedure that addresses the "primary" sinus drainage pathways. Endoscopic examination enables the physician to determine specific areas of blockage, to detect the presence of polyps, and to obtain cultures at specific drainage sites. Endoscopic examination enables the physician to determine specific areas of blockage, to detect the presence of polyps, and to obtain cultures at specific drainage sites. The flexible fiberoptic endoscope is useful in sure circumstances because of|as a end result of} its flexibility allows examination of difficulttoexamine structures. Examination of the ear, nose, and throat all the way way|the method in which} the vocal cords may be undertaken with a versatile scope. The inflexible endoscopes are advocated for diagnostic purposes by most otolaryngologists. Spraying the nose with 1% phenylephrine and 2% tetracaine (pontocaine) typically is sufficient to make the affected person comfortable for an entire office examination with nasal endoscopy. If essential, additional consolation may be successfully achieved by placing a cotton pledget with 4% topical anesthetic agent into the nasal cavity for 5 minutes. After appropriate decongestion and topical anesthesia, the 4mm nasal endoscope with a 0� or 30� lens is handed into the nasal cavity. Proper prognosis of intranasal and sinus illness can solely be maximally achieved with sort of|this type of|this kind of} endoscopic examination (5, 1113). Also, sweat chloride testing carried out to rule out cystic fibrosis, particularly in kids with nasal polyps or chronic or recurrent sinusitis. These instruments are an immense enchancment over plain film sinus depiction and can give reliable reproducible info. This info includes the standing of the bony walls, the character of fabric inside the sinuses, and the standing of the adjacent regular structures corresponding to the eye, brain, and midface. The standing of the bony walls of the sinuses is essential both in benign sinus illness and likewise in sinus tumors. It takes newergeneration scanners solely minutes to present highresolution photographs of tissue slabs that are be} 36 just a few millimeters thick. Patients undergo medical therapy to tackle acute infections, shrink inflamed mucosal membranes, and scale back hyperplastic mucosa. These photographs are adequate for analysis of assorted densities inside the sinus contents, which may indicate fungal sinus illness or concretions in the sinuses. Although some clinicians advocate additional windowing to increase sensitivity for further 37 sinus pathology, this has not routine. It is notable that plain films of the sinuses in kids may be particularly deceptive. In kids, computer tomography will provide an improved sensitivity and specificity, but it has its drawbacks, particularly greater price, somewhat increased radiation exposure, and the frequent necessity of sedation to carry out these exams in kids. A "plain Xray" useful in evaluating the pediatric affected person suspected of getting acute sinusitis. With regard to radiation exposure, the lens of the eye and the thyroid gland are major organs of concern. Factors to which the nose might react embrace environmental pollution and allergy symptoms, temperature modifications, and probably stress and sure meals (26). In sufferers with hypersensitive sinus and nasal lining, these elements might trigger more marked irritation and swelling, secondary sinus obstruction, and poor clearance of mucus. Should secondary chronic infection develop subsequently, the issue is typically made worse, and the hyperreactivity then further increases. While many suppose that sinusitis means infection, infection of many causes of irritation of the sinuses. Signs of infection embrace fever, inexperienced and foulsmelling nasal drainage, and facial pain. Mechanical elements embrace choanal atresia, sinonasal polyps, deviated septum, foreign physique, trauma, tumor, nasogastric tube, turbinate hypertrophy, concha bullosa, adenoid hypertrophy. Medicationrelated causes embrace betablockers, contraception pills, antihypertensives, aspirin intolerance, rhinitis medicamentosa (overuse of topical decongestants), and cocaine abuse. Anatomic abnormalities that predispose to sinusitis are sometimes recognized by the sinus specialist and amenable to surgical correction. It is well known that viral infections destroy the cilia of the mucous membranes, and roughly 6 weeks are required for regeneration.
References:
- https://www.eurotimes.org/wp-content/uploads/2019/11/RIOL-Supplement.pdf
- https://atriumhealth.org/-/media/newsroom/Documents/2018-Annual-Report.pdf
- https://www.abacademies.org/articles/aeljvol19no12015.pdf
- https://www.aae.org/specialty/wp-content/uploads/sites/2/2018/04/TreatmentStandards_Whitepaper.pdf