.png)
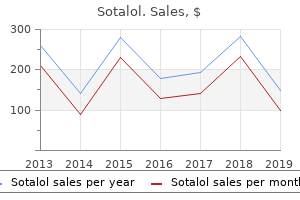
40mg sotalol
The distal nephron (including the cortical and medullary accumulating ducts), beneath the influence of aldosterone, reabsorbs the final amount of sodium and secretes hydrogen and potassium ions. The terminal accumulating ducts are influenced by antidiuretic hormone to permit water reabsorption and therefore lead to urinary focus. Many tubular problems are inherited and appear to contain the loss or formation of a defective transport protein ("provider") and symbolize an inborn error of transport. Because many of these transporter proteins and channels have been cloned, the exact genetic defect of a lot of thse conditions can now be understood more utterly. [newline]These conditions include (1) a single selective transport defect, (2) a class-specific defect. Luminal, intracellular, or peritubular elements of the web transport course of could be affected in each scenario. Several of the more usual transport defects of individual nephron segments are described right here. Urinary wastage of bulk quantities of these solutes implies a disorder of proximal tubular function. The renal glycosurias are attributable to inherited or acquired defects in proximal tubule glucose reabsorption such that glycosuria is clear at regular serum glucose concentrations. The quantity of glucose reabsorbed adjustments, depending on the filtered glucose load, till a maximal reabsorptive capacity, or Tm, is achieved. Before saturation, glucose reabsorption is incomplete and a "splay" is clear. The initial point within the splay represents that filtered glucose focus (the "threshold") at which reabsorption now not equals filtration and glucose appears within the urine. Normally, the threshold focus, 200 to 240 mg/dL, is way above the plasma values; thus, scant glucose (<125 mg/day) appears within the urine. The kinetics of D-glucose reabsorption have been compared with traditional enzyme kinetics. In the 2 primary types of renal glucosuria, both the capacity (type A, Vmax, or Km mutation) or the affinity (type B, K m, or extent-of-splay mutation) of glucose reabsorption is affected. In both type, the threshold is influenced in order that glucose is lost within the urine at a traditional plasma glucose focus. Inheritance is autosomal recessive, and heterozygotes have more marked glucosuria. Usually, however not at all times, Vmax and Km variants are inherited individually, as can be anticipated with two separate genes. Diagnosis should be based on finding glucosuria of greater than 500 mg/24 hr (on a food regimen containing 50% carbohydrate) without hyperglycemia (serum glucose <140 mg/dL). To verify the excreted sugar as glucose, the glucose oxidase method should be used; this can exclude other mellituric conditions (pentosuria, fructosuria, sucrosuria, maltosuria, galactosuria, and lactosuria). If desired, differentiation of the Vmax or Km variants could be made by glucose loading. The renal aminoacidurias symbolize inborn errors of renal tubular transport during which a single or group of amino acids is hyperexcreted and is usually accompanied by intestinal malabsorption of the same amino acid(s) (see Table 109-1). The 20 L-amino acids are predominantly reabsorbed by the proximal tubule at a fee of reabsorption exceeding 95 to 98% of the filtered load. Stereospecific amino acid transport happens across the luminal membrane of the proximal tubule, accompanied by sodium and driven by the lumen-to-cell sodium focus gradient. Specific: hypercystinuria, dibasic aminoaciduria (lysine, arginine, ornithine), lysinuria 2. Hematologic problems: hereditary elliptocytosis, sickle cell anemia, carbonic anhydrase I deficiency or alteration c. Non-selective Transport Defects: Generalized Distal Renal Tubular Acidosis, Hyperkalemia, and Renal Salt Wasting A. Tubulointerstitial nephropathies: methicillin, obstructive nephropathy, transplantation, sickle cell illness, cyclosporine c. Other Concentrating and Diluting Disorders glutamic acid; (3) impartial amino group-glycine, proline, hydroxyproline, and sarcosine; (4) impartial (Hartnup) group-alanine, serine, threonine, valine, leucine, isoleucine, phenylalanine, glutamine, histidine, asparagine, tyrosine, tryptophan, and citrulline; and (5) beta- amino acids-taurine, beta-alanine, and beta-aminoisobutyrate. Inherited dysfunction of a provider ends in urinary lack of the complete amino acid group: cystinuria (basic aminoaciduria), dicarboxylic aminoaciduria, Hartnup illness (neutral aminoaciduria), and iminoglycinuria. There are minimal of|no less than} 25 selective amino acid carriers that transport a single or few numbers of a given amino acid group. Human problems of these carriers lead to much more selective aminoaciduria: hypercystinuria, histidinuria, and lysinuria. This depicts each the normal pattern and the pattern within the two variants of renal glucosuria (type A and sort B). Many proximal nephron amino acid carriers are also expressed throughout the luminal (brush border) membrane of gastrointestinal epithelial cells. Defective intestine absorption happens concomitantly with renal hyperexcretion of the amino acid(s) in query. Di- and tripeptides could be absorbed usually by the intestine; therefore dietary issues arising from amino acid malabsorption are unusual. To diagnose a renal aminoaciduria, an elevated plasma level of the amino acids should be excluded. Whenever the filtered load of an amino acid exceeds the transport capacity of the renal tubule, an "overload" or "prerenal" aminoaciduria can occur. Most inborn errors of amino acid metabolism exhibit kind of|this sort of|this type of} aminoaciduria end result of|as a end result of} the plasma focus of individual amino acids which are be} poorly metabolized rises sharply. By contrast, the renal aminoacidurias are associated with low or regular levels of plasma amino acid concentrations, end result of|as a end result of} the aminoaciduria of} an inborn error of proximal tubule transport. Cystinuria is the term used to designate a group of renal transport problems which have in frequent the excessive excretion of the extremely insoluble amino acid cystine and the formation of urinary calculi. Cystine loss leads to cystine urolithiasis, which accounts for 1 to 2% of all urinary calculi. Stone formation normally turns into evident during the second and third decades of life, although presentation might occur from infancy to the ninth decade, and males are more severely affected. Cystine stones are radiopaque, can create staghorn calculi, and often type a nidus for calcium oxalate stone formation. Symptoms include renal colic, which may be associated with obstruction or infection or each. The analysis of cystinuria should be considered in any affected person with renal calculus, even when the stone is composed primarily of calcium oxalate. Typical hexagonal crystals acknowledged by urinalysis, notably in a concentrated, acidic, early-morning specimen. A helpful screening test is the cyanide-nitroprusside test, which detects a cystine focus of greater than seventy five to one hundred fifty mg/L. Because of false-positive test outcomes, a definitive analysis requires thin-layer or ion-exchange chromatography. Excretion ratios in an grownup of greater than 18 mg of cystine per gram of creatinine verify the analysis. Homozygous individuals normally excrete greater than 250 mg of cystine per gram of creatinine. Medical therapy for cystinuria is aimed at lowering the urinary focus below the solubility limit of 300 mg of cystine per liter. Because cystine excretion as excessive as 1 g/24 hr, a complete of 4 L of water should be ingested. The most effective technique of converting cystine to a more soluble compound follows the therapeutic administration of D-penicillamine, which means of|by means of|by the use of} a disulfide trade response produces cysteine-penicillamine. Hartnup illness, a impartial aminoaciduria, is a rare autosomal recessive disorder (1 in 26,000 births) during which the medical presentation is dominated by nicotinamide deficiency. Because up to as} 50% of nicotinamide is often supplied by metabolism of tryptophan, malabsorption and renal lack of tryptophan contribute to nicotinamide deficiency, especially when dietary nicotinamide is inadequate. Hence, this disorder demonstrates the significance of each the intestinal and renal transport defects. Clinical evidence of nicotinamide deficiency is intermittent and often worse in kids and includes pellagra in sun-exposed areas, cerebellar ataxia, and typically psychiatric disturbances. Hartnup illness should be suspected in a affected person with pellagra or cerebellar signs without a a|with no} historical past of niacin deficiency. Supplemental nicotinamide (40 to 250 mg per day) will prevent pellagra and neurologic issues. Less frequent aminoacidurias which are be} asymptomatic include iminoglycinuria, isolated hypercystinuria (without hyperexcretion of other primary amino acids), isolated glycinuria, and dicarboxylic aminoaciduria.
Safe sotalol 40 mg
Echocardiography (see Chapter 43) with exercise has a sensitivity and specificity minimal of|no much less than} equal to those of exercise electrocardiography. When performed after the infusion of dobutamine, stress echocardiography has been related to a sensitivity of 86 to 96% for diagnosing coronary disease and a specificity of sixty six to 95% for excluding it. Positron emission tomography can assess myocardial perfusion and metabolism and diagnose coronary disease with sensitivities and specificities that may strategy 95%. Continuous electrocardiographic monitoring allows detection of in any other case clinically silent ischemia. Many patients with symptomatic angina also have quantity of} extra episodes of asymptomatic ischemia with a total ischemic burden greater than suspected. Control of asymptomatic ischemia by approaches that rely on reduction of ischemic burden quite than consideration to} signs may enhance prognosis in some patients with episodes of silent ischemia. The mixture of multivessel disease and poor left ventricular function is related to a poor enough prognosis to think about a mechanical revascularization process (see later). Quite typically, segmental dysfunction may be caused by surprised myocardium (transient dysfunction due to of} acute ischemia) or hibernating myocardium (poorly functioning myocardium due to of} continual hypoperfusion). These circumstances ought to be recognized as a result of|as a result of} they are often reversible with appropriate treatment. When selecting a diagnostic test (Table 59-6), it is important to|it could be very important|you will need to} understand that the predictive worth of the test is dependent on the prevalence of the disease as determined by the Bayes theorem; thus, the post-test probability of coronary artery disease is influenced by the pretest prevalence of the disease. Other determinants of threat are older age, earlier bypass surgery, earlier myocardial infarction, and co-morbid circumstances such as diabetes mellitus, renal failure, and obstructive coronary disease. An extra indication to carry out provocative testing is to acquire insight into the severity of the disease for prognostic stratification. Considering the different yield of varied exams and the costs concerned, it is important to|it could be very important|you will need to} select the exams that will be most appropriate in different types of|several sorts of|various kinds of} patients (Table 59-6). Unstable angina is a heterogeneous syndrome with regard to causes, clinical manifestations, severity, and prognosis. The severity of the underlying coronary artery disease is also be|can be} variable: 5 to 10% may have left major vessel disease; 40%, three-vessel disease; 25%, two-vessel disease; 20%, one-vessel disease; and 10%, no important coronary artery stenoses. The analysis requires careful clinical recognition followed by stratification of patients into groups at excessive, intermediate, or low threat of subsequent problems (Table 59-7). More aggressive therapeutic methods are usually beneficial in higher-risk patients. Counseling is essential for instructing the nature and causes of the disease and its manifestations, dangers, therapeutic approaches, and medical follow-up. Aspirin is the most typical first selection, but clopidogrel, a thienopyridine by-product closely related to ticlopidine, is an alternate. Clopidogrel was related to fewer gastrointestinal unwanted effects effects}, barely extra cutaneous reactions, no extra whole bleeding, and no extra in leukopenia or thrombocytopenia compared with aspirin. Because of this favorable aspect effect profile, clopidogrel may be most well-liked over ticlopidine, which has additionally been proven helpful in secondary prevention of vascular occasions. Clopidogrel and ticlopidine are antagonists of the adenosine diphosphate receptors in platelets. Aspirin irreversibly inhibits platelet cyclooxygenase and prevents formation of thromboxane A2. Paradoxically, warfarin was proven helpful when added to aspirin in a major prevention trial in high-risk people. Effective antianginal therapy relieves myocardial ischemia by enhancing oxygen provide and/or reducing demand. Myocardial oxygen demand is decreased by beta-blockers, nitrates, and calcium antagonists. Nitroglycerin (Table 59-9) produces quick vasodilation; venous and arteriolar vasodilatation reduces preload and afterload on the center, and coronary vasodilatation relieves inappropriate coronary vasoconstriction. Long-acting nitrates administered orally or transdermally are efficient to stop angina and enhance tolerance to exercise. Nitroglycerin is exogenous nitric oxide and should overcome variety of the} problems related to deficient production within the dysfunctional endothelium. Calcium channel antagonists (Table 59-11) are potent vasodilators to relieve coronary artery spasm. They additionally scale back myocardial oxygen needs by a variable effect on heart fee, blood pressure, and contractility. Selection of the best agent for a person patient is influenced by many issues, including related disease and tolerance to the medicine. A controversy exists on attainable deleterious results on mortality for calcium antagonists, significantly short-acting nifedipine. Patients with hypertension will benefit from beta-blockers or calcium antagonists. Patients with heart failure will benefit from nitrates and low-dose beta-blockers. Active bronchospasm is a contraindication to beta-blockers; cardioselective beta-blockers may, however, be examined. The dihydropyridine calcium channel blockers advantageous when a bradyarrhythmia is current. Internal mammary artery grafts are clearly related to a better short- and long-term consequence. The treatment of unstable angina contains interventions to control ache, interventions that scale back myocardial oxygen demand, and interventions would possibly be} designed to improve myocardial oxygen provide. Intravenous or sublingual nitroglycerin (up to three sublingual nitroglycerin tablets at 5-minute intervals) is run for the relief of chest ache and is followed by an intravenous infusion of nitroglycerin (beginning at 5 to 10 g/min and rising by a lot as} 10 g/min every 5 minutes as needed and tolerated). The objective is to switch patients to oral or topical nitrates when they have been asymptomatic for 24 hours. Morphine given in doses of two to 5 mg intravenously, repeated once or twice after 15 to half-hour to relieve signs. Aspirin ought to be started immediately at an initial dose of a hundred and sixty to 325 mg followed by 80 to a hundred and sixty mg/day. Intravenous heparin ought to be started on all patients at excessive or intermediate threat immediately and be continued for 2 to 5 days until the patient has been free of chest ache for minimal of|no much less than} 24 hours or a coronary intervention process is performed. The beneficial dose is 80 units/kg as an intravenous bolus followed by eight units/kg/min by infusion to keep the activated partial thromboplastin time at one and one-half to two times control values. Low molecular-weight heparin (see Chapter 188), which may be most well-liked to commonplace heparin, may be administered subcutaneously to produce a sustained and reproducible anticoagulation response, without having for monitoring. Low-molecular-weight heparins have much less platelet results and solely not often trigger heparin-induced thrombocytopenia. Two recent trials have proven a superiority of subcutaneous enoxaparin (1 mg or one hundred anti-Factor X units per kilogram) administered twice daily for 48 hours to eight days after admission. Prolonged administration after hospital discharge was not related to extra benefit in these trials. Therapy is begun intravenously in patients with evolving ache and is followed by oral therapy to a goal of fifty to 60 beats per minute: metoprolol (5 mg by sluggish intravenous bolus repeated every 5 minutes for a total initial dose of 15 mg followed in 1 to 2 hours by 25 to one hundred mg orally every 12 hours); propranolol (0. Intra-aortic balloon counterpulsation is indicated as a bridge to revascularization within the unstable patient. The early aggressive strategy is related to much less angina and decrease charges of hospital readmission throughout follow-up. Correction of coronary threat components improves prognosis in patients with coronary artery disease and related to regression of the disease. An aggressive program for correction of threat components is subsequently mandated in patient administration. Indeed, in lots of} patients the long-term benefits may exceed those of revascularization procedures. The program should embody smoking cessation; control of blood ldl cholesterol, blood sugar, and hypertension; and physical fitness. The meta-analysis of a hundred forty five randomized trials of greater than one hundred,000 patients documented clearly the efficacy of antiplatelet therapy for the administration of the acute manifestations of coronary artery disease, for its secondary prevention, and, in some situations, for major prevention. The trial compared clopidogrel to aspirin for secondary prevention of cardiovascular occasions in patients with a earlier stroke, earlier myocardial infarction, or peripheral vascular disease. The randomized double-blind trial compared treatment with enoxaparin, a low-molecular-weight heparin, to unfractionated heparin in hospitalized patients with unstable angina or non- Q-wave myocardial infarction; aspirin was administered to all patients. The threat of demise, myocardial infarction, or recurrent angina was decreased with the low-molecular-weight heparin. Original description of angina pectoris revealed in 1772 stays up-to-date; it additionally accounts for the development from stable angina to unstable angina. Theroux P, Fuster V: Acute coronary syndromes: Unstable angina and non-Q wave myocardial infarction.
Diseases
- Lymphoma
- Secondary pulmonary hypertension
- Smith Magenis syndrome
- Akesson syndrome
- Recurrent peripheral facial palsy
- Contact dermatitis, irritant
Effective 40 mg sotalol
Optimal programming is important for many of} causes, together with minimizing affected person discomfort, reducing the prospect of syncope with an arrhythmia episode, maximizing the battery life of the heart beat|the heartbeat} generator, and preventing inappropriate shocks. Complications related to the implantation process embody pneumothorax, myocardial perforation, and an infection, all of which should have an incidence less than 1%. Complications related to the subcutaneous or submuscular pocket into which the system is positioned embody hematoma formation and erosion of the pocket. A, In this affected person, the stored electrogram demonstrates ventricular tachycardia, rate 300 beats per minute, indicating tht the shock was appropriate. He was handled with amiodarone to cut back the frequency of episodes of ventricular tachycardia. B, this affected person obtained shocks because of paroxysmal supraventricular tachycardia at a rate of 206 beats per minute, which exceeded the programmed rate cut-off of one hundred seventy beats per minute. He underwent radiofrequency ablation of the paroxysmal supraventricular tachycardia and obtained no additional inappropriate shocks. C, the stored electrograms on this affected person indicate that the affected person obtained inappropriate shocks that had been triggered by atrial fibrillation, rate one hundred eighty beats per minute. This affected person was trated with a beta-blocker to maintain the ventricular rate less than 150 beats per minute during atrial fibrillation. Other lead complications embody a fracture or insulation breakdown, either of which can result in a failure to defibrillate. However, pressing analysis is important if the affected person experiences flurries of discharges. Flurries of shocks could also be} triggered by atrial fibrillation with a fast ventricular response, by which case aggressive administration of the atrial fibrillation is indicated. In addition, flurries of shocks could also be} a manifestation of a lead fracture, by which case lead substitute is important. The radiofrequency vitality results in resistive heating of the tissue and irreversible tissue destruction when the tissue temperature exceeds 50� C. Diagnostic electrophysiologic testing (see Chapter 50) and radiofrequency ablation usually are performed during the identical process, commonly on an outpatient basis. Depending on kind of|the type of} tachycardia, sites in the coronary heart are focused for ablation primarily based on the results of mapping (see Chapter 50) or as guided by specific anatomic landmarks. Radiofrequency vitality is delivered, typically in purposes of 1 minute, at a power setting enough to result in sufficient tissue heating of 60 to 70� C. For gradual pathway ablation, which is the popular approach, target sites for ablation are located in the posteroseptal proper atrium, near the ostium of the coronary sinus. Slow pathway ablation has a success rate of 98 to one hundred pc and is related to a zero to 1. Left-sided accent pathways are ablated utilizing either a retrograde aortic or transseptal strategy, and people which might be} right-sided or septal are ablated utilizing a venous strategy. Detailed mapping of the accent pathway is crucial for identification of an appropriate ablation web site, and the ablation catheter is positioned either on the atrial or ventricular side of the mitral or tricuspid annulus. The success rate of accent pathway ablation is 90 to 98%, and the complication rate is 2 to 3%. Detailed mapping also is required to establish sites for ablation of atrial tachycardias (see Chapter 51). Most atrial tachycardias come up 252 in the proper atrium and are mapped utilizing a venous strategy, however left atrial tachycardias are mapped utilizing a transseptal strategy. Assuming that the atrial tachycardia is arising solely at one web site, the success rate of ablation is roughly 90%, and complications are rare. Type I atrial flutter (see Chapter 51) arises in the proper atrium and can be eliminated by radiofrequency ablation directed at a crucial isthmus in the low proper atrium, between the tricuspid annulus and the inferior vena cava. The success rate of this type of|this type of|this type of} ablation is roughly 90%, and the risk of a severe complication is less than 1%. Both types of procedures could also be} related to a late, 1 to 2% threat of sudden demise. Two other ablation procedures that will show to be helpful in patients with atrial fibrillation are the creation of linear lesions in the proper and/or left atrium to get rid of atrial fibrillation and ablation of a focal supply of paroxysmal atrial fibrillation, normally within one of the pulmonary veins. At present, ablation procedures are investigational, and their efficacy and safety remain to be decided. The sinus node, located in the excessive lateral proper atrium, is focused for ablation. The success rate is 90%, and 10% of patients require a pacemaker because of an inadequate atrial escape rate. At present, surgical accent pathway ablation could also be} indicated for the occasional affected person with the Wolff-Parkinson-White syndrome who has probably harmful arrhythmias and in whom radiofrequency catheter ablation is unsuccessful. When performed by an experienced surgeon, the success rate of surgical accent pathway ablation approaches one hundred pc and the risk of a severe complication is low. Intraoperative mapping is important to establish the location of the accent pathway, which then can be ablated either cryosurgically utilizing an epicardial strategy or by direct dissection utilizing an endocardial strategy. At centers experienced in this type of|this type of|this type of} operation, the success rate of subendocardial resection has been eighty five to 90%, and the operative mortality rate has been in the range of 5 to 10%. In the past few years, the Maze process has been developed in an try to treatment atrial fibrillation. A sequence of incisions are made in specific areas of the left and proper atria to subdivide the atria into parts too small to sustain atrial fibrillation, and an isthmus of tissue is left between the subdivisions to enable both for normal atrial activation by the sinus node and for restoration of atrial transport operate. With the latest refinements in the Maze process, the operative mortality rate has been 2%, greater than 90% of patients have had no recurrences of atrial fibrillation during long-term follow-up, and roughly 25% of patients have required a permanent pacemaker because of pre-existing or surgically induced chronotropic incompetence. Although these results are spectacular, many patients are reluctant to undergo an open-heart process related to a threat of demise to deal with a non-lethal arrhythmia. The most appropriate role for the Maze process right now could also be} as an adjunct to valve restore or substitute in patients with atrial fibrillation who require valve surgery. A detailed description of the indications for implantation of permanent pacemakers and implantable cardioverter-defibrillators. In mortality trials, profit has not been seen, and worsened mortality has been observed with several of} drugs. Therefore, care have to be taken in deciding the mode of remedy, or actually whether or not to deal with with drugs in any respect. Many antiarrhythmic brokers can be found right now, however no agent is totally effective for all patients, and every agent has the potential for causing severe toxicity. Drug choice is usually empirical, and known aspect effects} might prohibit the usage of} sure lessons of medicine for a particular affected person. Amiodarone might improve mortality in some patients, however the 253 d-isomer of sotalol will increase mortality after myocardial infarction. However, most antiarrhythmic drugs have multiple of} actions; hence their pharmacology is advanced and will differ in different cardiac tissues. Furthermore, many antiarrhythmic brokers have pharmacologically active metabolites whose manufacturing varies extensively inside the population and whose exercise could also be} fairly different than the father or mother compound. Drugs having Class I motion possess "local anesthetic" or "membrane-stabilizing" exercise by blocking of the quick inward sodium channel to produce a lower in the maximum depolarization rate, Vmax, of the motion potential (phase 0) and gradual intracardiac conduction. Because of the many limitations of the Vaughan Williams classification, "The Sicilian Gambit" classification system has been developed primarily based on the differential results of antiarrhythmic drugs on channels, receptors, and transmembrane pumps. Because antiarrhythmic drugs have a slender therapeutic index, variable metabolism and clearance usually cause clinical results. These individuals have markedly decreased clearance of mexiletine, flecainide, and propafenone. Lidocaine is very usually the drug of first choice for the acute suppression of ventricular arrhythmias. Figure 54-1 this determine is a modification of the Sicilian Gambit drug classification system and includes designation by the Vaughan Williams system. The sodium channel blockers are subdivided into the A, B, and C subgroups primarily based on their relative efficiency. The stable triangle signifies the biphasic results of bretylium initially to launch norepinephrine and act as an agonist and subsequently to block additional launch and act as an antagonist of adrenergic tone. The number of arrows and their course indicate the magnitude and course of effect of the drugs on coronary heart rate and left ventricular operate. Lidocaine has little effect on the electrophysiology of the normal conduction system; in patients with conduction system abnormalities, it has variable results. The time required to attain steady-state situations is 8 to 10 hours in normal individuals and up to as} 20 to 24 hours in some patients with coronary heart failure and/or liver illness, whose elimination half-life is much longer longer} than the 1. Single intravenous boluses will achieve solely transient therapeutic results outcome of|as a result of} the drug is rapidly distributed out of the plasma and myocardium.
Generic sotalol 40 mg
Tacrolimus (Prograf) is often substituted for cyclosporine in patients with persistent or recurrent rejection and can also be|can be} often utilized in girls and youngsters to keep away from the hirsutism associated with cyclosporine. Prednisone doses are tapered and, in some centers, discontinued if no vital rejection happens throughout tapering. In common, the azathioprine dose is lowered if the white blood cell depend persistently falls beneath 4000 to 5000 cells/mL. Mycophenolate mofetil (CellCept) additionally be} superior to azathioprine and is preferred in some centers. Routine use of influenza vaccine, though controversial, is of little risk and should supply some safety. Diltiazem can also be|can be} routinely used at many transplant centers, as it may also lower the chance of cardiac allograft rejection; diltiazem also increases cyclosporine levels, leading to reduced cyclosporine dosing and an total savings in drug prices. Cardiac rejection additionally be} cell mediated (cellular rejection), the commonest form, and/or antibody mediated (humoral rejection). Cellular rejection, which results in|which finally ends up in} substantive or persistent rejection, is characterised initially by a mononuclear infiltrate. Higher grades of rejection are categorised in accordance with the presence and extent of myocyte infiltration, myocyte necrosis, hemorrhage, and/or vasculitis. The incidence of cardiac rejection is highest early after transplantation and subsequently decreases to a low but fixed price. Symptoms and signs associated with rejection additionally be} nonspecific and embrace malaise, lethargy, fatigue, low-grade fever, and temper changes, or they may be cardiac-specific, corresponding to dyspnea, lower blood strain, jugular venous distention, model new} S3 or S4 gallop, or model new} supraventricular arrhythmia. Depressed cardiac perform after cardiac transplantation, with or with out hemodynamic changes, is often attributable to acute rejection. Surveillance endomyocardial biopsies, particularly throughout the first 6 months after transplantation, stay the standard for detecting early signs of rejection. About one third of patients develop a serious infection post-transplant (defined as requiring intravenous antibiotics and/or thought of to be life-threatening) during the first 12 months after transplant, and infection stays the commonest explanation for death in the first 12 months. Lung and bloodborne infections are commonest, accounting for 50% of significant infections. The incidence of rejection episodes, calculated because the number per one hundred patients occurring every month after transplant, is highest in the first month following transplantation (34 rejections per one hundred patient-months) and then rapidly declines over time. Cyclosporine-induced hypertension happens in more than 90% of heart transplant recipients throughout the first 12 months. Antihypertensive drug dosing ought to allow for diurnal blood strain changes, with dosing timed to have a peak impact in the morning. To control blood strain, vasodilators (direct and calcium channel blocking drugs) and angiotensin-converting enzyme inhibitors are equally efficient. If attainable, beta-adrenergic blocking medication ought to be avoided, outcome of|as a end result of} the denervated heart depends on circulating catecholamines to increase heart price and systolic perform with exercise. Cyclosporine commonly decreases glomerular filtration price and raises the serum creatinine. Acute nephrotoxicity may occur with the primary perioperative dose of cyclosporine (see Chapter a hundred and five. Cyclosporine also appears to have dose-dependent poisonous results on the renal tubules and can cause renal tubular acidosis. Hepatic dysfunction, which happens in as much as} 10% of patients following transplantation, additionally be} many causes, together with intraoperative or perioperative hepatic hypoperfusion, a response to cyclosporine or azathioprine, or viral hepatitis. Cyclosporine-induced hepatotoxicity is dose-dependent and often happens when serum levels are extraordinarily excessive. Cyclosporine decreases urate clearance by the kidney; hyperuricemia and gout commonly occur. Allopurinol is associated with a decrease in azathioprine metabolism, and azathioprine dosing must due to this fact be adjusted accordingly. Non-steroidal anti-inflammatory medication ought to be avoided, if attainable, because of their nephrotoxic results. Short-term colchicine additionally be} very useful, but long-term use can increase immunosuppression and cause bone marrow toxicity. Cyclosporine is metabolized by the cytochrome P-450 enzyme pathway and due to this fact interacts with numerous medications and substances which are be} metabolized by or that affect that enzyme system (including alcoholic beverages). Many medication, together with certain antibiotics, may instantly worsen the renal toxicity of cyclosporine. Corticosteroid use after transplantation may lead to or worsen glucose intolerance and hyperlipidemia and should precipitate osteoporosis and its issues (see Chapter 28). The commonest adverse impact associated with azathioprine is bone marrow toxicity, most commonly leukopenia and less commonly thrombocytopenia, megaloblastic anemia, pink cell aplasia, and reticulocytopenia, which often appears 7 to 14 days after preliminary dosing or elevations in dosing. Any drug that impacts the guts through either a change in vagal tone or a direct increase in sympathetic nerve exercise has little impact on the transplanted heart. However, it nonetheless has non-cardiac results corresponding to dry mouth, mydriasis, cycloplegia, constipation, and urinary retention. The denervated heart is, nonetheless, more delicate to both beta-adrenergic agonists. Isoproterenol, by virtue of its chronotropic impact, is used routinely to stimulate heart price in instances of sinus node dysfunction early after transplantation. The denervated heart is hypersensitive to adenosine; if adenosine is run to convert supraventricular tachycardia, it ought to be given at 25% of the same old} dose. Cardiac allograft vasculopathy impacts all vessels in the transplanted heart (including veins) and leads to vessel lumen obliteration. Depending on the means used to detect it, the incidence of the illness ranges from 10 to 50% at 1 12 months to 50 to 90% at 5 years after transplantation. Histologically, the illness manifests as hyperplasia of easy muscle cells, intimal proliferation, mononuclear cell infiltration of the intima, and the presence of lipid-laden macrophages in all areas of the vessel wall. The process is believed to be multifactorial in origin, but it most likely stems from an preliminary and/or ongoing immunologically mediated or infection-induced. The therapy of the illness includes coronary angioplasty, the location of intracoronary stents, and consideration of retransplantation. End-stage cardiac patients typically become depressed; after transplantation, early exhilaration followed by mild to average depression is widespread, possibly corticosteroid 378 use. Constant vigilance for signs suggestive of more vital or longer-term depression is required. About eighty to 85% of patients become bodily lively after cardiac transplantation, but solely 33 to 50% of patients return to work. Cardiac transplantation, generally, markedly improves the cardiovascular hemodynamics of the transplant recipient. However, the transplant recipient is commonly left with a slightly diminished maximal cardiac output owing to denervation (neural decentralization), limited atrial perform, decreased myocardial compliance, and donor-recipient measurement mismatch. Because parasympathetic influences that normally lower the guts price in regular hearts are absent after cardiac transplantation, the resting heart price is often 95 to 115 beats per minute. Furthermore, the lack of sympathetic innervation blunts the conventional increases in heart price and contractility that occur with exercise, with low cardiac filling pressures, and after vasodilation. The cardiac allograft increases cardiac output primarily by a rise in filling strain and secondarily in response to circulating catecholamines. Immediately after transplantation, the cardiac allograft reveals compliance abnormalities as evidenced by a restrictive hemodynamic sample. This sample often progressively improves over days to weeks, but 10 to 15% of recipients develop a persistent restrictive hemodynamic sample (see Chapter 64). A evaluate of the early publications of the Cardiac Transplant Research Database, which outlines strategies of outcomes analysis in the heart transplant inhabitants. A evaluate of use of presently available units as a bridge to cardiac transplantation. A comparatively quick overview of the historical past, physiology, and current status of heart transplantation directed to the non-transplant doctor. Turino the process of respiration consists of many structural and practical elements (see Chapter 73) along with the lungs, such because the nose, pharynx, sinuses, chest cage and musculature, pleura, diaphragm, extrathoracic airways, cerebral regulatory respiratory centers, and cardiovascular system. In addressing the patient with pulmonary illness, the doctor must preserve a circumspect approach to attainable pathogenic elements.
Cheap 40mg sotalol
The most common explanation for main tricuspid regurgitation is infective endocarditis, often stemming from drug abuse and unsterile injections. Other causes embrace carcinoid syndrome, rheumatic involvement of the tricuspid valve, myxomatous degeneration, right ventricular infarction, and mishaps throughout endomyocardial biopsy. The symptoms of tricuspid regurgitation are these of right-sided coronary heart failure, together with ascites, edema, and infrequently right higher quadrant pain. On bodily examination, tricuspid regurgitation produces jugular venous distention accentuated by a 336 giant v wave as blood is regurgitated into the proper atrium throughout systole. Regurgitation into the hepatic veins causes hepatic enlargement and liver pulsation. The definitive analysis of tricuspid regurgitation is made throughout echocardiography. Doppler interrogation of the tricuspid valve demonstrates systolic disturbance of the proper atrial blood pool. Echocardiography can also be|may additionally be|can be} used to determine the severity of pulmonary hypertension, to measure right ventricular dilatation, and to assess whether or not the valve itself is intrinsically normal or abnormal. The remedy for secondary tricuspid regurgitation is often aimed at trigger of|the purpose for} the lesion. Thus, if left ventricular failure has been responsible for right ventricular failure and tricuspid regurgitation, the standard remedy for bettering left ventricular failure (see Chapter 48) will decrease left ventricular filling strain, cut back secondary pulmonary hypertension, relieve some of the the} hemodynamic burden of the proper ventricle, and partially restore tricuspid valve competence. If pulmonary disease is the primary trigger, remedy is directed towards bettering lung function (see Chapter 75). Vasodilators, so useful in the remedy of left-sided coronary heart failure, are often ineffective in treating pulmonary hypertension itself. Thus, medical remedy directed at tricuspid regurgitation itself is often restricted to diuretic use. However, if other cardiac surgery is deliberate in a patient with severe tricuspid regurgitation, ring annuloplasty or tricuspid valve restore is usually attempted to guarantee postoperative tricuspid competence. Tricuspid valve alternative is usually not properly tolerated and is now rarely performed besides when severe deformity, as usually seen in endocarditis or carcinoid disease, precludes valve restore. It is often detected and corrected throughout childhood, however occasionally cases are recognized for the first time in adulthood. During bodily examination, the uncalcified valve in pulmonic stenosis produces an early systolic ejection click on on opening. [newline]During inspiration, the click diminishes or even disappears outcome of|as a result of} increased move into the proper side of the center throughout inspiration partially opens the pulmonic valve in diastole so systole causes less of a gap sound. The click on is followed by a systolic ejection murmur, which radiates to the bottom of the center. If the transvalvular gradient is severe, right ventricular hypertrophy develops and produces a parasternal raise. The analysis of pulmonic stenosis is confirmed throughout echocardiography, which quantifies the transvalvular gradient the diploma of right ventricular hypertrophy and dysfunction. In asymptomatic patients with a gradient of lower than 25 mm Hg, no remedy is required. If symptoms develop or the gradient exceeds 50 mm Hg, balloon commissurotomy is efficient in decreasing the gradient and relieving symptoms. After a prosthetic valve has been inserted, a baseline echocardiogram ought to be obtained to present a reference point ought to valve dysfunction be suspected at a later date. The major causes of valve dysfunction are infectious endocarditis, clot, and valve degeneration. Dysfunction is most commonly manifested by valvular regurgitation, however valvular stenosis can also occur with clot, vegetations, or degeneration, particularly degeneration of a bioprosthesis. Whenever a patient with a prosthetic coronary heart valve develops a temperature higher than 100�F, endocarditis must be excluded by blood culture; for fever with signs of sepsis, broad-spectrum antibiotics must be begun while awaiting culture outcomes. Whether prophylaxis is necessary for pulmonary autografts is currently unclear, however physicians often prescribe prophylaxis for such patients. Aspirin, at doses of 325 mg, is really helpful in addition to warfarin to cut back the danger of valve thrombosis in patients with mechanical prosthetic valves at greater risk for thromboembolic issues. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Management of Patients with Valvular Heart Disease). Consensus guidelines that present a useful approach to common valvular abnormalities. General usage, nonetheless, incessantly additionally includes the diffuse dilation and hypocontractility that may result from severe coronary artery disease and is termed ischemic cardiomyopathy. Elevated filling pressures at rest can cause orthopnea, supine cough, and paroxysmal nocturnal dyspnea (see Chapter 47). Right-sided congestion can cause discomfort throughout bending, abdominal discomfort, anorexia, and peripheral edema, though edema is usually absent, notably in younger patients. These symptoms are common in all types of cardiomyopathy and in reality are common to all cardiac illnesses when filling pressures become 337 elevated. The time period congestive coronary heart failure describes this syndrome of elevated filling pressures however not trigger of|the purpose for} coronary heart failure nor kind of|the sort of} cardiomyopathy. In some patients, tachyarrhythmias or bradyarrhythmias will be the presenting symptom of cardiomyopathy. Chest pain occurs in virtually one third of patients with cardiomyopathy regardless of normal epicardial coronary arteries and may result from pulmonary hypertension, pericardial involvement, microvascular ischemia, or unknown factors. Systemic emboli arising from dilated ventricles or atria and incessantly associated with atrial fibrillation are occasionally the first signal of cardiomyopathy. Although the myocardial pathology differs markedly, the scientific manifestations of elevated filling pressures and fluid retention characteristic prominently throughout this spectrum. Specific cardiac conditions similar to coronary artery disease or valvular coronary heart failure are often suggested by the history, bodily examination, and echocardiogram however might require cardiac catheterization for affirmation and quantification. Tachycardia-induced cardiomyopathy, most commonly observed in youngsters and young adults, adults from supraventricular or sluggish ventricular tachycardias when rates are chronically or incessantly above a hundred and twenty to 140 beats per minute and is completely reversible. If these other conditions are absent or insufficient to explain the cardiac dysfunction, the subsequent task is to distinguish among dilated, restrictive, and hypertrophic cardiomyopathy by echocardiography. Evidence from inhabitants screening suggests a higher frequency of asymptomatic disease than beforehand acknowledged. Etiology Dilated cardiomyopathy has many causes (Table 64-2) that result in the syndrome. A brief main injury similar to poisonous publicity fatal to some myocytes, after which the increased burden of strain and quantity stimulates hypertrophy in the surviving myocytes. This hypertrophy initially preserves world function however can ultimately result in progressive useful impairment. One mechanism resulting in progressive deterioration late after an initial injury will be the triggering of programmed cell demise, recognized as|often identified as} "apoptosis. Inflammatory myocarditis might combine irreversible cell demise with reversible despair from inflammatory mediators similar to cytokines. Many injuries may also result on} the collagen scaffolding of the myocardium, influencing stiffness and the potential for ventricular dilation. Most cardiomyopathies reflect the sum of irrevocable myocyte Figure 64-1 Initial approach to classification of cardiomyopathy. Although that is usually obvious from routine bodily examination, echocardiography serves to affirm cardiac disease and supplies clues to the presence of other cardiac disease, similar to focal abnormalities, suggesting main valve disease or congenital coronary heart disease. Having excluded these conditions, cardiomyopathy is generally considered to be dilated, restrictive, or hypertrophic, as proven in Figure 64-2. Patients with apparently normal cardiac structure and contraction are occasionally discovered to reveal abnormal intracardiac move patterns preserving with} diastolic dysfunction however also needs to|must also} be evaluated rigorously for other causes of their symptoms. Most patients with so-called diastolic dysfunction may also reveal at least of|no less than} borderline criteria for left ventricular hypertrophy, incessantly in the setting of continual hypertension and diabetes. A moderately decreased ejection fraction with out marked dilation or a sample of restrictive cardiomyopathy is typically referred to as "minimally dilated cardiomyopathy," which may either represent a distinct entity or a transition between acute and continual disease. Right-sided symptoms of systemic venous congestion: discomfort on bending, hepatic and abdominal distention, peripheral edema. Myocarditis Viral Myocarditis Most of our conception of viral myocarditis derives from murine animal fashions in which initial viral replication could be exacerbated by train and immunosuppression. Infected animals might die, recover, or develop dilated hearts with areas of fibrosis. Viruses are incessantly suspected however rarely isolated as the direct explanation for myocarditis in people.
Syndromes
- Coronary artery disease
- Chlorhexidine gluconate
- Valve repair: A small incision is made in the leg and the damaged valve is repaired.
- The severity of the infection and how well it response to treatment
- Allergic reactions to medicines
- What makes the problem worse? Better?
Proven sotalol 40mg
Bedside evaluation of the gastric transit of a bolus of isotonic saline additionally be} a useful and inexpensive screening test. After half-hour, the residual should be less than 40% of an oral quantity of 750 mL administered. A breath test measures both liquid and stable gastric emptying utilizing non-radioactive isotopes of carbon (13 C or 14 C) certain to octanoic acid. With an enteric neuropathy, the migrating motor complicated is absent, whereas with a myopathy, contractions are current but their amplitude is decreased. Small intestinal transit can be measured by breath checks to estimate small intestinal transit by reflecting the bacterial metabolism of non-absorbable carbohydrate marker to H2, or the bacterial launch of a radionuclide label from a bile salt conjugate, both of which improve within the breath after the substrates reach the colon. These checks are invalid if the patient has small intestinal bacterial overgrowth ensuing from the motility dysfunction or a blind loop of gut, outcome of|as a result of} the micro organism launch the marker proximal to the ileocecal valve. The appearance in the proper lower quadrant (cecum) of a radionuclide-labeled non-absorbable marker ingested with a meal also offers an estimate of small intestinal transit. Intraluminal pressures measured within the small gut could document abnormalities within the fasting migrating motor complicated and the postprandial motility response. As within the abdomen, concomitant use of transit and manometric research allows the contribution of the enteric nerves and smooth muscle to the motility disorder to be estimated objectively. Global colonic transit can be simply measured by orally administering radiopaque markers and measuring the distribution of the markers all through the colon 5 days later. In the constipated patient, localization of the markers to the rectosigmoid region suggests a rectoanal outlet dysfunction. If the markers are distributed all through the colon, a colonic motility disturbance exists. Once the motility defect has been localized to the colon, more particular transit and motility checks, measuring increases in intraluminal pressure and phase transit times with radionuclide markers, can be found in specialized centers. The absence of a postprandial improve in segmenting contractions suggests a neural lesion, whereas low amplitude or absent postprandial contraction suggests disturbed smooth muscle operate. Anorectal manometry exhibits whether or not the anal sphincter contributes to outlet dysfunction. Acute gastroparesis, which is most incessantly associated with an electrolyte disturbance, ketoacidosis, systemic an infection, or an acute abdominal insult, is managed by treating the underlying disease, not the gastric motility disorder. Delayed gastric emptying additionally be} associated with different systemic ailments or additionally be} a main dysfunction of the abdomen (Table 132-3). The typical signs of delayed gastric emptying embody early satiety, nausea, and vomiting. Phytobezoars sometimes occur in these patients as well, particularly if the migrating motor complicated is absent. Vagotomy, with the exception of the extremely selective vagotomy (parietal cell vagotomy), decreases fundic rest, antral contractions, and coordinated rest of the pylorus (Chapter 129). This complication is more likely to to|prone to} occur if the patient had gastric outlet obstruction caused by a main disease. Metoclopramide improves signs plenty of} patients with delayed gastric emptying after a vagotomy. The traditional dose of metoclopramide (10 mg orally, 4 times a day) may cause anxiousness, fatigue, or sedation or dyskinesia in about 15% of patients. Cisapride, which releases acetylcholine from the enteric neurons, additionally be} useful in gastroparesis. Erythromycin, a macrolide antibiotic, initiates phase 3 within the abdomen, improving gastroparesis signs. Roux-en-Y anastomoses after gastric resection sometimes trigger poor gastric emptying, particularly of solids. The migrating motor complicated and the postprandial motor response are abnormal within the roux limb. Delayed gastric emptying of solids is the major useful disturbance; liquid gastric emptying additionally be} regular. Patients with severe vomiting can be treated with subcutaneous bethanechol, additional gastric resection, or elimination of the roux loop. Leuprolide could scale back signs, and some patients could benefit from a near-total gastrectomy. Chronic delayed gastric emptying, associated with long-standing insulin-dependent diabetes mellitus, is a larger medical drawback. Such patients have frequent episodes of nausea and vomiting, which affect on} meals intake and complicate insulin necessities. Retinopathy, nephropathy, peripheral neuropathy, and different complications are generally current. Absence of the gastric migrating motor complicated, essential for emptying of non-digestible material greater than 1 mm, predisposes the diabetic patient to bezoars, inflicting abdominal discomfort, early satiety, and vomiting. Metoclopramide improves the signs of gastric stasis in patients with diabetes mellitus both by growing gastric emptying and decreasing the central nervous system recognition of nausea and distention. Bethanechol also stimulates a rise in gastric motility and improves signs in patients with diabetic gastric stasis. Erythromycin improves signs of gastroparesis by growing antral contractions and fundal tone. The gastric emptying of solids, but not of liquids, is slowed in patients with anorexia nervosa (see Chapter 227), but not in patients with bulimia. The delayed gastric emptying is associated with antral dysrhythmia, fundal hypotonia, decreased postprandial plasma concentrations of norepinephrine and neurotensin, and impaired autonomic operate (decreased resting diastolic blood pressure and skin conductance). Reversal of the underlying psychiatric disturbance seems essential for full resolution of signs. Delayed gastric emptying in progessive systemic sclerosis could exacerbate issues with esophageal reflux. The decreased gastric emptying associated with an acute viral an infection normally resolves shortly. Up to 25% of patients with reflux esophagitis, associated with an incompetent lower esophageal sphincter, have delayed gastric emptying, which must be corrected to deal with the reflux esophagitis adequately. Lesions such as tumors, infarction, or viral encephalitis that affect on} the vagal complicated within the medulla can delay gastric emptying. Rapid Gastric Emptying Rapid gastric emptying happens in some patients with duodenal ulcer disease and Zollinger-Ellison syndrome duodenal insensitivity to an acid load (Chapter 130). Rapid liquid emptying happens in patients with pancreatic insufficiency (Chapter 141) and possibly with celiac sprue due to poor suggestions inhibition of gastric motility by fat a maldigestion or malabsorption. Decreased intestinal motility displays both absent or fewer contractions of phase 3 of the migrating motor complicated throughout fasting or a minimal improve in postprandial motility within the completely different regions of the small bowel. Conversely, elevated motility is mirrored in elevated numbers of fasting migrating motor complexes or an augmented intraluminal pressure response to consuming. Uncoordinated intestinal motility can be caused by retrograde migrating motor complexes and clustered contractions. In patients with motility problems, qualitatively comparable transit patterns could result in completely different signs. For example, patients with constipation could have delayed small intestinal transit. In contrast, a patient with pseudo-obstruction could have a larger delay in intestinal transit that ends in diarrhea bacterial overgrowth. Diarrhea is generally speedy intestinal transit due to decreased time of contact of the luminal contents with the mucosa. Patients also could have maldigestion and malabsorption poor mixing of the dietary material with the digestive enzymes and bile salts. Patients with slow intestinal transit probably to|are inclined to} complain of nausea, vomiting, abdominal distention, and periumbilical abdominal cramps. Phase 3 of the migrating motor complex-in which micro organism and sloughed, dead epithelial cells are propelled from the small gut into the colon-is often absent or severely deranged by an enteric neuropathy. Bacterial overgrowth a diminished variety of migrating motor complicated contractions deconjugates bile salts, inflicting steatorrhea and diarrhea. The absence of postprandial motility impedes the traditional transit by way of the small gut.
Order sotalol 40 mg
Once alternate-day therapy has been realized, gradual reductions in glucocorticosteroids must be attempted. An alternate method is to attain a complete day by day dose of 30 mg/day and then cut back the drug on the low-dose day. These tapering schemes are possible only when comparatively short-acting glucocorticosteroids are used; longer-acting medication have biologic half-lives of greater than 24 hours, thereby negating the beneficial effects of an alternate-day regimen. Failures may occur if the try to start tapering is premature as a result of|as a end result of} the illness continues to be energetic, if the dose is lowered too rapidly, if the decrements in dose are too giant, if not enough prednisone is run on the "on" day, or if glucocorticosteroid "withdrawal" signs. In some instances, tapering may be facilitated by utilizing glucocorticosteroid-sparing medication that help management the primary illness as glucocorticosteroids are lowered. Clearly, nevertheless, these brokers may have associated toxicities that restrict utility. In many circumstances it may be acceptable to administer glucocorticosteroids domestically or to use systemic regimens which will cut back the probability of adverse effects. Topical and ophthalmic preparations can typically management cutaneous (see Chapters 521 and 522) and ocular (see Chapter 512) illness, respectively, with out appreciable systemic absorption of the preparation. Similarly, glucocorticosteroids administered nasally for allergic rhinitis (see Chapter 274), by inhalation for bronchial asthma or decrease airway illness (see Chapter 74), and intra-articularly or by delicate tissue injection for musculoskeletal inflammatory conditions may management the underlying illness with out the adverse effects of systemic therapy. However, these methods of delivering medication can even trigger native toxicity and must be used with caution. Deflazacort, an oral glucocorticosteroid preparation not currently obtainable in the United States, has been reported to have fewer adverse reactions, particularly osteoporosis, than conventional glucocorticosteroids. When native glucocorticosteroid therapy and even systemic day by day oral treatment are inadequate to management the underlying illness, intermittent, short-term, high-dose intravenous methylprednisolone can be utilized in inflammatory and immunologically mediated ailments, using 3- to 5-day regimens at 20 mg/kg/day or 1 g/m2 /day. The precise mechanism(s) of the beneficial actions of such "pulse" therapy is unclear, particularly as a result of|as a end result of} these protocols are sometimes efficacious even when superimposed on day by day glucocorticosteroid utilization. Pulse therapy has been related to arrhythmias and sudden death, most likely because of shifts in electrolytes in patients with underlying electrolyte abnormalities, conduction system disturbances, or diuretic therapy. In these settings, electrocardiographic monitoring is advisable whereas the drug is slowly administered over 1 to a number of} hours. Other reported adverse reactions with pulse therapy include seizures and systemic infections, but the precise relationship of the reactions to pulse glucocorticosteroids is unclear as a result of|as a end result of} the therapy is often given to critically unwell patients. Current indications for pulse regimens have included recrudescence of illness regardless of continual glucocorticosteroid therapy, a flare of illness exercise in the setting of glucocorticosteroid unwanted side effects}, the need to|the necessity to} management illness till one other modality. In basic, unwanted side effects} depend upon day by day dose, dosing frequency, and period of treatment, and emphasize the need to|the necessity to} deal with with alternate-day regimens or the bottom day by day dose attainable for as briefly as possible. Hypothalamic-pituitary-adrenal axis suppression may occur with less than 2 weeks of systemic therapy and additionally be} persistent regardless of cessation of the drug. The integrity of the hypothalamic-pituitary-adrenal axis in the setting of glucocorticosteroid therapy may be decided by measuring the change in serum cortisol degree after cosyntropin infusion (see Chapter 240). In basic, the most effective way of stopping or minimizing the adverse effects of glucocorticosteroids is to cut back their dosage; unfortunately, this may not all the time be possible. It is particularly essential to monitor patients intently for the event of an infection; typical signs of an infection additionally be} masked by glucocorticosteroid treatment. Glucocorticosteroid-induced osteoporosis (see Chapter 257) is especially problematic in older individuals, particularly those who are estrogen deficient. Complete abstract of the literature on supplemental, "stress" glucocorticoids in patients receiving continual therapy. On June 2, 1763, the Royal Society obtained a communication from Reverend Edward Stone of Chipping Norton in Oxfordshire. Its opening lines are most likely unmatched in scientific pharmacology: "Among the various helpful discoveries which this age has made, there are only a few which higher deserve the attention of than what I am going to lay earlier than your Lordship. There is a bark of an English tree, which I even have have} discovered by expertise to be a robust astringent and very efficacious in curing aguish and intermittent issues. Stone had discovered that salicylates lowered the fever and aches produced by a variety of|quite lots of|a wide selection of} acute, shiver-provoking illnesses, or agues. At its low doses (80 to 325 mg/day), acetylsalicylic acid is used to stop coronary and cerebral thrombosis by advantage of its antiplatelet impact. Intermediate, over-the-counter doses (650 mg to 3 g/day) are used as analgesics and antipyretics. Finally, for a hundred years very high doses (> 3 g/day) have been used to cut back the redness and swelling of joints in rheumatic fever, gout, and rheumatoid arthritis. Aspirin and other salicylates have a variety of|quite lots of|a wide selection of} other biologic effects, only some of which are related to their use in drugs at present. Salicylates can dissolve corns on the toes-a keratolytic impact; provoke loss of uric acid from the kidneys-their uricosuric property; and kill bacteria in vitro-their antiseptic action. But cell biologists additionally use aspirin and salicylates to inhibit anion transport throughout cell membranes, to intervene with the activation of white blood cells, and to uncouple oxidative phosphorylation by isolated mitochondria. Finally, molecular biologists use salicylates to activate genes that code for heat-shock proteins in the lampbrush chromosomes of Drosophila, to affect mitogen-activated protein kinases, and to induce ceramide-mediated apoptosis in most cancers cells. By 1828, at the Pharmacologic Institute of Munich, Buchner isolated a tiny quantity of the energetic glycoside, salicin, in the form of bitter-tasting yellow, needle-like crystals. Two years later, Leroux, in Paris, improved on the extraction procedure and obtained 1 ounce of salicin from 3 kilos of the bark. By 1838, Raffaele Pira of Pisa described how he obtained a pure substance from salicin by hydrolyzing the glycoside in a CrO3 -mediated oxidation via an aldehyde intermediate. Meadowsweet (Spiraea ulmaria) yielded ample quantities of an ether-soluble oil from which Spirsa ure, the same acide salicylique of Pira, was crystallized. Oil of wintergreen, a conventional remedy for aguish issues, additionally was shown to include the methyl ester of salicylic acid from which acide salicylique might be be} ready. Forced to compete with the French and British dye industries, which supplied their textile mills with pigments imported from abroad colonies, the Germans responded by inventing low-cost aniline dyes, creating in their train such large enterprises as I. In 1876, Stricker and Ries reported the first profitable treatment of acute rheumatism by sodium salicylate at doses of 5 to 6 g/day. Almost concurrently, Maclagan reported his results with salicylic acid and salicin at related dosage levels. Stricker and Ries and Maclagan discovered that salicylates cut back not only fever and ache but also redness and swelling. That anti-inflammatory property was subsequent used to benefit by the Parisian Germain See, who, in 1877, launched high-dose salicylates, both acid salicylique and salicin, as effective therapies for gout and "continual poly-arthritis. In 1898, Felix Hofmann, an aniline dye chemist at the Friedrich Bayer-Eberfeld division of I. Farben, searched for less acidic derivatives to keep away from gastric irritation and centered on acetyl derivatives of sodium salicylate. Competitors entered the sphere as markets expanded for other medication that might cut back fever and ache. Based on anecdotal accounts from Alsace that a product fashioned from aniline handled with vinegar made a helpful febrifuge, Karl Morner, in 1889, synthesized the material-acetanilide-and isolated its metabolites. Acetanilide itself, unfortunately, brought on bone marrow depression and anemias in a distinct variety of patients, so other derivatives had been sought. Acetanilide and the extensively used phenacetin are metabolized to N-acetyl- p-aminophenol, which by various anagramatic combos yields the generic names acetaminophen in the United States and paracetamol in the United Kingdom. In 1955, acetaminophen acquired a trade name in the United States that was to make it well-known: Tylenol-also from acetylp-aminophenol. The constitutive enzyme, cyclooxygenase 1, is a 70-kd homodimer localized to microsomal membranes. This enzyme catalyzes two reactions: the bis-dioxygenation 115 Figure 29-1 the inflammatory cascade. The endoperoxides, important for platelet perform, are transformed by platelets to a most potent vasoconstricting and platelet-aggregating substance, thromboxane A2 (TxA2). Because platelets make TxA2, which constricts the smooth muscle of blood vessels, and because blood vessel walls make prostacyclin I2, which powerfully relaxes blood vessels and inhibits platelet aggregation, the hunt was on for methods to inhibit the synthesis of thromboxane however not prostacyclin. Vane and his associates, in the Nineteen Seventies, had amassed convincing evidence that the prostaglandin speculation of aspirin action was largely appropriate. Vane argued that stable prostaglandins not only had been produced at websites of irritation but also, alone or in live performance with other mediators, may provoke all the cardinal signs of irritation. By comparability, acetaminophen ineffectively inhibits prostaglandin synthesis by enzyme preparations from a variety of|quite lots of|a wide selection of} tissues however is effective in opposition to the synthetase from brain. And although non-acetylated salicylates are roughly 1/10 as potent as aspirin in vitro, studies of urinary prostaglandin metabolites confirmed that sodium salicylate effectively diminishes excretion of those metabolites in people. Sodium salicylate additionally effectively reduces prostaglandin release in models of experimental irritation in animals.
Buy 40 mg sotalol
It is comparatively widespread, with an incidence of 1 in 2000 to 3000 whites; and roughly 30,000 persons in the United States are affected. The illness impacts quantity of} totally different organs, but most of present morbidity and ninety to 95% of mortality end result from persistent pulmonary infections. The first pathologic and clinical description got here in 1938, when the illness was called cystic fibrosis of the pancreas. Since then, marked improvements have occurred in prognosis, clinical management, understanding, and remedy of the illness. More than seven hundred different mutations and variations have been found in the gene, with only a handful accounting for greater than 1% of mutations. Thus, correction of the defective processing might present a novel method to remedy. At least some of the variability in the clinical illness may be defined by variations in the severity of the particular mutation. It appears doubtless that obstruction of the small ducts in the male genital tract also results in the atrophy, fibrosis, or absence of the vas deferens, tail and body of the epididymis, and seminal vesicles. Disruption of this process is assumed to produce thick, dehydrated intestinal contents that hinder the ileum in the new child, inflicting meconium ileus and producing meconium ileus-equivalent later in life. Normal lungs are protected against inhaled and aspirated bacteria by quantity of} protection methods, together with mucociliary clearance, phagocytic cells (such as macrophages and neutrophils), and the innate immune system, consisting of quantity of} antimicrobial elements. These elements embody lysozyme, lactoferrin, and small peptides, corresponding to beta-defensins. Inhibition of the antimicrobial activity of the innate immune system may give inhaled bacteria an advantage in colonizing the airway floor. The paracellular pathway between the cells via the tight junctions also exhibits some permeability to ions. Chronic an infection is associated with an intense inflammatory response with an abundance of neutrophils. A profusion of cytokines and proinflammatory stimuli also lead to submucosal gland hypertrophy and increased mucus output. The progressive inflammation and an infection injury the airways, resulting in bronchitis, progressive bronchiectasis, and respiratory failure. For instance, they might present as newborns with meconium ileus, as infants or children with failure to thrive, or from childhood to adulthood with recurrent respiratory tract infections. The cough is usually accompanied by wheezing, notably in infants and young children. Episodes of cough tend to to|are inclined to} persist longer than expected for an acute respiratory sickness and, with time, occur more and more incessantly. As the illness progresses, the cough turns into productive of thick, purulent, often green sputum. Patients might have symptoms of bronchitis for quantity of} years or even a a} decade or two. Eventually, nevertheless, exacerbations of cough and sputum manufacturing are accompanied by dyspnea, reduced appetite, and weight reduction. Acute exacerbations improve with intensive therapy but tend to to|are inclined to} improve in frequency and severity till the affected person develops symptoms of 403 bronchiectasis (see Chapter 77). However, with time Pseudomonas aeruginosa turns into very common, often as a mucoid species. Quantitative sputum cultures are sometimes of worth in evaluating the response to antibiotic therapy. With normal chest radiographs, hyperinflation may be the first finding, followed by peribronchial cuffing, which creates linear opacities. Impaction of mucus and changes preserving with} bronchiectasis are observed as the illness progresses. For causes that stay unknown, the proper higher lobe is commonly the primary and most severely concerned. The arterial P O2 tends to decrease with time ventilation-perfusion mismatching. The course of the illness and the response to therapy are often followed by serial measurement of spirometry, lung volumes, and oxygenation. Pneumothorax (see Chapter 86) is a well-recognized complication, and the incidence increases with age. Indications for chest tube placement are the identical as for pneumothorax from different causes. The price of recurrence is excessive; pleural sclerosis required to prevent recurrences. Massive hemoptysis occurs in roughly 1% of sufferers and is often associated with an exacerbation of the persistent respiratory an infection. Treatment is often directed at the underlying pulmonary illness; but when hemoptysis is life-threatening, surgery or bronchial artery embolization required. Hypertrophic pulmonary osteoarthropathy might occur in a lot as} 15% of sufferers, especially adolescents and adults; its symptoms might correlate with exacerbations of the pulmonary illness. Nasal polyps occur in 15 to 20% of sufferers and sometimes require resection to prevent nasal obstruction. Of note, epithelial cells isolated from resected nasal polyps are important in producing model methods used in research on pathogenesis and novel therapies. Although greater than 50% of sufferers have antibodies to Aspergillus fumigatus, only a small quantity develop allergic aspergillosis. Late in the illness, untreated hypoxemia and progressive lack of useful lung might produce pulmonary artery hypertension and right ventricular failure (see Chapter 56). Respiratory failure turns into more and more tough to manage as the illness worsens. Pancreatic Disease Failure of the exocrine pancreas (see Chapter 141) occurs in roughly 85% of sufferers. Obstruction of ducts, lack of acinar cells, and pancreatic enzyme deficiency lead to malabsorption of protein, fats, and fat-soluble vitamins. If left untreated, sufferers with pancreatic insufficiency might show a failure to thrive, weight reduction, and progress inhibition. Weight loss associated with severe respiratory illness and an increased work of respiration. Although the islets of Langerhans are relatively spared, destruction of the pancreas can cause endocrine pancreatic dysfunction in roughly 7% of all sufferers and is extra widespread in adults. If diabetes occurs, insulin therapy should be initiated oral agents are ineffective. Small bowel obstruction, "distal intestinal obstruction syndrome," occurs in roughly 3% of sufferers, and intermittent stomach pain, perhaps from partial obstruction, is far extra widespread. Another reason for stomach pain is intussusception, which often requires surgical intervention. Genitourinary Disease More than 95% of males are sterile because of atrophy of wolffian duct buildings. Spermatogenesis is undamaged, and retrieval of sperm has been used for in vitro fertilization. Women with severely compromised pulmonary and nutritional standing might show an accelerated deterioration during being pregnant. Hepatobiliary Disease Focal biliary cirrhosis appears to be growing as sufferers stay longer. The severity varies widely, with evidence plenty of} sufferers limited to an elevated alkaline phosphatase level. In severe 404 cases, sufferers develop hepatosplenomegaly, jaundice, ascites, and edema. Hematemesis from esophageal varices is a severe complication which will require endoscopy and sclerosis of affected vessels. Enlarged submandibular, sublingual, and submucosal glands are generally observed on physical examination. Adult sufferers might develop osteoporosis poor vitamin or vitamin deficiency. Psychosocial issues in coping with a lethal illness have to be acknowledged and treated appropriately.
Proven 40 mg sotalol
The lack of segmenting contractions to impede forward movement or transit could exacerbate the urgency. Increased concentrations of fecal bile salts contribute to the functional diarrhea by irritating colonic sensory nerves. In treating functional diarrhea, antidiarrheal brokers such because the opioid analogues, loperamide, and diphenoxylate lower signs. If excess bile salts contribute to the diarrhea, low doses of cholestyramine could lower the diarrhea. Surreptitious laxative abuse is a typical however troublesome to diagnose cause of functional diarrhea (see Chapter 227). Oxyphenisatin and bisacodyl stimulate increased numbers of propagating contractions and diarrhea. Patients could take these or other laxatives as a manifestation of a psychiatric dysfunction. Rapid transit of colonic contents and increased mucosal secretion occur in sufferers with active ulcerative colitis. As in the other colonic causes of diarrhea, propagating contractions are increased in number and propagate into the rectum, accounting for the significant incidence of fecal incontinence. The rapid transit improves because the mucosal irritation decreases after therapy for the underlying irritation. When some of these medication are used to treat other systemic diseases, they may precipitate gastrointestinal signs as a facet impact. Excitatory Agents Drugs that excite the gastrointestinal tract must be used to treat decreased motility when the smooth muscle can functionally contract. In basic, sufferers who profit from these brokers have an enteric neuropathy with decreased release of endogenous stimulatory neurotransmitters or an increased release of inhibitory neurotransmitters. When the smooth muscle is absent or severely broken, the prokinetic medication are hardly ever helpful. Acetylcholine analogues, corresponding to bethanechol, stimulate both longitudinal and round gastrointestinal clean muscle by directly binding to the M2 muscarinic receptor to release inositol triphosphate or to open receptor-operated or voltage-dependent calcium channels. Drugs that block acetylcholinesterase improve endogenous acetylcholine concentration on the myoneural junction. These medication have a theoretical benefit in regulating nicely as|in addition to} in increasing motility, because of|as a outcome of} the distribution of acetylcholine release is predetermined by the autonomic nervous system. Dopamine antagonists can variably improve motility throughout the gastrointestinal tract. Domperidone, a peripherally performing dopamine antagonist, mainly increases gastric emptying and has little therapeutic impact in small intestinal or colonic motility issues. It stimulates gastric emptying, increases small intestinal transit, and stimulates colonic contractility. Cisapride could improve signs in sufferers with decreased gastric emptying, small intestinal pseudo-obstruction, or colonic inertia. Acetylcholine analogues Excitatory Neostigmine Metoclopramide Domperidone Cisapride Macrolide antibiotics Octreotide (low dose) Leuprolide acetate Atropine Secoverine Papaverine Calcium channel blockers Nitrate compounds Peppermint oil Cholecytokinin antagonists Erythromycin stimulates migrating motor advanced exercise, which is absent plenty of} sufferers with neuropathic pseudo-obstruction, by binding on the motilin receptor on the small intestinal clean muscle cell. Low dose octreotide (<100 mug) initiates section 3 of the migrating motor advanced, which additionally makes it helpful in sufferers with pseudo-obstruction. Leuprolide acetate could improve signs secondary to functional disturbances of small intestinal motility. This drug is believed to work by decreasing the concentrations of the smooth muscle inhibitory hormones progesterone and relaxin. Inhibitory Agents Inhibitory medication must be most helpful for treating sufferers whose signs outcome from increased motility, which causes uncoordinated movement of the intestinal contents. The inhibitory medication could block the receptors for excitatory neurotransmitters or block the rise in intracellular calcium needed for normal clean muscle contraction. Anticholinergic medication, which inhibit muscarinic receptor stimulation, are generally effective for the small intestinal or colonic variants of the irritable bowel syndrome. The anticholinergics must be used with care in sufferers who could develop urinary retention. These utilized in some sufferers with increased small intestinal or colonic motility. Nitrate compounds inhibit clean muscle contraction, most likely by increasing the intracellular concentration of cyclic guanosine monophosphate and decreasing calcium inflow into the smooth muscle cell. Peppermint oil relaxes clean muscle, which improves signs in some sufferers with the irritable bowel syndrome. Cholecystokinin antagonists could prove helpful for treating gastrointestinal motility issues. Bueno L, Fioramonti J, Delvaux M, Frexinos J: Mediators and pharmacology of visceral sensitivity: From fundamental to medical investigations. Comprehensive evaluate of the pathophysiology of increased visceral ache; can serve as a information to therapy for abdominal ache. Excellent evaluate of motility issues of the higher gastrointestinal tract with rationalization of work-up. Cisapride has a therapeutic impact on sufferers with bowel dysmotility related to signs of the irritable bowel syndrome. Although people hardly ever cite increases in frequency alone because the definition of diarrhea, a lower in stool consistency (increased fluidity) and stools that cause urgency or abdominal discomfort are more likely to|prone to} be termed diarrhea. Consistency is defined because the ratio of fecal water to the water-holding capacity of fecal insoluble solids, that are made up of bacterial mass and dietary fiber. Because it is rather troublesome to measure stool consistency and because stool is predominantly (60-85%) water, stool weight turns into an inexpensive surrogate of consistency. Physicians typically define diarrhea as a physical signal, 24-hour stool excretion by weight or volume, somewhat than as a symptom. Daily stool weights of children and adults are less than 200 g, and greater stool weights are an goal definition of diarrhea; nonetheless, this definition will miss 20% of diarrheal signs in sufferers with free stools under this every day weight. There are three categories of persistent diarrheas: osmotic (malabsorptive) diarrhea, secretory diarrhea, and inflammatory diarrhea. The incidence of infant and baby diarrheal deaths in the United States decreased by 75% between 1968 and 1991 however remains greater than 500 deaths every year. In the United 703 States, diarrheal diseases are frequent and extreme sufficient to result in over 300,000 hospital admissions, 6 million visits to physicians, and 48 million episodes that final minimal of|no much less than} one full day and result in loss of time from school or work. Although enchancment in sanitation and training in the United States has decreased charges for infectious parasitic diarrheas, diarrheas ensuing from person-to-person contact. It is now clear, nonetheless, virtually all} diarrheal circumstances are due primarily to alterations of intestinal fluid and electrolyte transport and less to clean muscle perform. Each 24 hours 8 to 10 L of fluid enters the duodenum with 800 mEq sodium (Na+), seven-hundred mEq chloride (Cl-), and one hundred mEq potassium (K+). The food regimen provides 2 L of this fluid; the remainder comes from salivary, abdomen, liver, pancreatic, and duodenal secretions. Of the remaining fluid, the colon absorbs all however roughly one hundred mL, which incorporates 3, 8, and 2 of|and a pair of} mEq of Na+, K+, and Cl-, respectively. Diarrhea finish up} from decreased absorption or increased secretion by either the small intestine or the colon. If either deranged electrolyte transport or the presence of non-absorbable solutes in the intestinal lumen reduces the absorptive capacity of the small intestine by 50%, the volume of fluid (50% of 10 L, or 5 L) introduced every day to the conventional colon would exceed its maximum every day absorptive capacity of four L. Na+ transport by the epithelium from lumen to blood (by Na+:H+ exchange proteins in the small intestine and proximal colon and by amiloride-sensitive Na+ channels in the distal colon) create a good osmotic gradient for absorption. Na+ absorption in the small intestine could be enhanced by the glucose and galactose or by amino acids in the lumen due to the presence of Na+ -coupled sugar and amino acid transporters in the small bowel epithelium. Oral rehydration solutions, that are used extensively to exchange diarrheal fluid and electrolyte losses, are effective because of|as a outcome of} they contain Na+, sugars, and, typically, protein (amino acids). Active Cl- secretion or inhibited Na+ absorption additionally creates an osmotic gradient favorable for the movement of fluids from blood to lumen and is the premise of the secretory diarrheas. Agents that improve enterocyte cyclic adenosine monophosphate, cylic guanosine monophosphate, or intracellular ionized calcium (Ca2+) all inhibit Na+ absorption and stimulate Cl- secretion (Table 133-1). Classification of Diarrhea to perceive the three basic categories of diarrhea-malabsorption (osmotic diarrheas), secretory diarrheas, and inflammatory diarrheas-it is necessary to perceive how the conventional intestine handles fluid and solutes in well being and disease.
Safe sotalol 40mg
If the transit is too too|is merely too} sluggish, the mucosa can extract an excessive amount of} water and the stool turns into hard, resulting in constipation. Diarrhea attributable to colonic motility issues is low in quantity (<400 mL/day), end result of|as a end result of} most intestinal fluid is absorbed in the small intestine (see Chapter 133). Many of the systemic illnesses that result on} gastric and small intestinal motility also alter colonic motility. Either increased or decreased segmenting contractions can sluggish transit through the colon. The colonic contents also transfer slowly if colonic segmenting activity is decreased (colonic inertia). Propagating contractions are invariably absent in patients with sluggish colonic transit and constipation, suggesting that these contractions are necessary for internet ahead motion of feces into the distal rectosigmoid. Patients with diarrhea and rapid colonic transit have decreased colonic segmenting contractions and increased numbers of contractions propagating into the rectum. When these highly effective contractions carry the colonic contents into the rectum, the patient experiences urgency. Cramping abdominal pain referable to the colon happens predominantly in the decrease abdominal quadrants, however might be} felt wherever over the anatomic distribution of the colon. Although patients really feel bloated, ascribed to increased gastrointestinal gas, they actually have normal amounts of bowel gas. Tenesmus, a sense of incomplete evacuation, is related to rectosigmoid spasm. Most folks experience transient intervals of constipation throughout their lives; treatment is usually not necessary unless the signs last for a number of} months. Infrequent bowel actions (less than each different day) lead to hard fecal pellets, which require straining to get rid of, due to sluggish colonic transit and the ensuing desiccation of the stool. Fecal impactions, which rarely occur besides in elderly or sedentary patients, might trigger overflow diarrhea or bleeding from stercoral rectal ulcers. Although the pathophysiology of major constipation is poorly understood, most patients reply rapidly to increased fiber and water in their diets. The persistent use of stimulant laxatives has the potential to injury the myenteric plexus, inflicting an unresponsive "cathartic colon. Patients with constipation-predominant irritable bowel syndrome might have alterations in both smooth muscle and myenteric nerve perform. Therapy is aimed toward enhancing colonic motility and reducing the visceral hypersensitivity (see Chapter 131). Diverticular illness, mucosal outpouchings through the colonic wall that occur with getting older, leads to a spectrum of abnormalities extending from no signs to diverticulitis. Acquired diverticula, which occur most regularly in the left colon, end result from increased intraluminal strain pushing sleeves of mucosa through perivascular weaknesses in the wall of the colon juxtaposed to the taeniae coli (Chapter 136). Decreased dietary fiber and distal colonic smooth muscle hypertrophy contribute to elevation in distal colonic intraluminal strain. The signs of painful colonic diverticular illness are similar to those of irritable bowel syndrome however extra doubtless to|usually tend to} be localized in the left decrease quadrant. When diverticulitis happens as a complication, the patient might have fever, left decrease quadrant mass, leukocytosis, and occult blood in the stool (see Chapter 136). Narrowing diverticular irritation may be tough to differentiate from carcinoma of the colon. Painful diverticular illness of the colon is finest handled by reducing the intraluminal strain, similar to the remedy for the irritable bowel syndrome. Narcotics, especially morphine, must be 701 prevented due to an exaggerated improve in smooth muscle contraction. Constipation might end result from a disturbance in the elimination of stool through the anal sphincter. Elimination normally begins by the involuntary leisure of the internal anal sphincter after distention of the rectum. Voluntary controls open the rectoanal angle and loosen up the exterior anal sphincter. Several studies have localized the genetic defect to the chromosomal loci ret proto-oncogene, endothelin B, and endothelin three. Absence of nitric oxide synthase and the consequent absence of the inhibitory mediator nitric oxide might trigger the fixed contraction of the affected bowel. The severity of signs and the age at analysis are related to the size of the aganglionic phase. Involvement of the entire rectum or further elements of the colon leads to constipation or obstipation in infancy, requiring emergent resection of the aganglionic bowel and a pull-through anastomosis to the anus. If a short phase of the distal rectum is aganglionic, the patient might not current with signs until adolescence and even adulthood. Abnormalities in anal physiology are a big reason for constipation; impaired anal sphincter leisure happens relatively regularly in adults. Some patients have subtle histologic abnormalities in the myenteric plexus, suggesting that an acquired neuropathy may account for the abnormal sphincter response. In the spastic pelvic ground syndrome (animus), the exterior anal sphincter and the puborectalis loosen up poorly or the levator ani contracts poorly, leading to impaired opening of the rectoanal angle (Chapter 143). This acquired condition, which happens more usually in multiparous ladies, can prevent normal stool evacuation. Impaired internal anal sphincter leisure in an adult might respond to a posterior anal sphincter myomectomy. Slow Transit with Decreased Segmenting Contractions Patients with decreased segmenting contractions after stimulation have signs similar to those in patients with increased contractions. The colonic inertia form of the irritable bowel syndrome and primary colonic pseudo-obstruction a similar pathophysiologic disturbance. Postprandial increases in colonic motility are absent in both, however the colon is dilated in major intestinal pseudo-obstruction, explaining the increased incidence of abdominal distention. Constipation is current in many of} patients with persistent, insulin-requiring diabetes mellitus, progressive systemic sclerosis, or thoracic spinal wire lesions. In patients with diabetes or spinal wire lesions, colonic smooth muscle may be stimulated with exogenous drugs, suggesting a neural lesion, not a myopathy. In patients with neuropathy and normal smooth muscle perform, prokinetic drugs have had some success. Some patients have practical, painless diarrhea with fecal urgency however with no associated anatomic or histologic abnormality of the gastrointestinal tract. Lactose intolerance must be excluded either by history or by particular checks of lactose intolerance. The diarrhea is larger than that in the spastic irritable colon syndrome, and abdominal pain absent. Propagating contractions are increased and propagate into the rectum, presumably accounting for the increased urgency and fecal incontinence in these patients. The very permeable duodenum then renders the meal approximately isotonic with an electrolyte content similar to plasma by the point it reaches the proximal jejunum. In the colon, K+ is secreted, and the amiloride-sensitive Na+ transport mechanism of the colonocyte and the low epithelial permeability extract Na+ and fluid from the stool. As a end result, the Na+ content of stool drops to 30 to forty mmol/L, K+ increases from 5 to 10 mmol/L in the small bowel to seventy five to ninety mmol/L, and poorly absorbed divalent cations corresponding to Mg2+ and Ca2+ are concentrated in stool to values of 5 to a hundred mmol/L. The anion concentrations in the colon change drastically end result of|as a end result of} bacterial degradation of carbohydrate. At colonic pH, these are current as organic anions corresponding to acetate, propionate, and butyrate. This gap between stool osmolality and the sum of the electrolytes in the stool causes osmotic diarrhea. Inflammatory diarrheas are characterised by enterocyte injury and death, villous atrophy, and crypt hyperplasia. The enterocytes on rudimentary villi of the small intestine are immature cells with poor disaccharidase and peptide hydrolase activity, lowered or absent Na+ -coupled sugar or amino acid transport mechanisms, and lowered or absent NaCl absorptive transporters. If the irritation is severe, immune-mediated 704 vascular injury or ulceration permits protein to leak (exudate) from capillaries and lymphatics and contribute to the diarrhea. Lymphocyte and phagocyte activation releases numerous inflammatory mediators that induce intestinal secretion. Patients with infectious diarrhea usually complain of nausea, vomiting, and abdominal pain and have either watery, malabsorptive, or bloody diarrhea and fever (dysentery) (see Chapters 339 - 348). Many of the short-lived watery diarrheas ascribed to "viral gastroenteritis" are be mild, sporadic, food-borne bacterial infections. The incidence of food-borne illness in the United States is estimated to be 6 to eighty million circumstances per yr, including at least of|no less than} 9000 deaths annually.
References:
- http://www.eatoncommunityschools.org/userfiles/38/Classes/1598/the_bean_trees.pdf?id=19649
- https://www.opm.gov/healthcare-insurance/healthcare/plan-information/plan-codes/2021/brochures/71-006.pdf
- https://apps.who.int/iris/bitstream/handle/10665/327356/9789289051750-eng.pdf
- https://www.ncsbn.org/2013_NCLEX_RN_Detailed_Test_Plan_Educator.pdf